Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Comprehensive Nursing Intervention Improves Polysomnography Success, Safety, and Patient Experience in Obstructive Sleep Apnea
Authors Feng X, Miao Y, Zheng C, Yuan S, Qin J
Received 22 October 2025
Accepted for publication 10 April 2026
Published 30 April 2026 Volume 2026:19 576138
DOI https://doi.org/10.2147/JMDH.S576138
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Xiaodong Feng,1 Yuqing Miao,2 Chenhai Zheng,3 Shuai Yuan,3 Jie Qin3
1Department of Hepatobiliary Pancreatic Spleen Thyroid Surgery, General Hospital of Northern Theater Command, Shenyang, 110016, People’s Republic of China; 2Department of Burn Plastic Surgery, General Hospital of Northern Theater Command, Shenyang, 110016, People’s Republic of China; 3Department of Otolaryngology, General Hospital of Northern Theater Command, Shenyang, 110016, People’s Republic of China
Correspondence: Jie Qin, Department of Otolaryngology, General Hospital of Northern Theater Command, No. 83 Wenhua Road, Shenhe District, Shenyang, 110016, People’s Republic of China, Email [email protected]; [email protected]
Background: Polysomnography (PSG) is the gold standard for diagnosing Obstructive Sleep Apnea Syndrome (OSAS); however, monitoring failure and patient discomfort can compromise diagnostic accuracy. This study evaluated whether comprehensive nursing interventions improved PSG monitoring success, clinical parameters, and patient outcomes.
Methods: This prospective observational cohort study included 100 patients with OSAS who underwent PSG. Participants were sequentially allocated to a control group (n=50) receiving standard care or an observation group (n=50) receiving comprehensive nursing intervention. The intervention integrated structured patient education, proactive technical management of monitoring equipment, cardiovascular risk assessment, and psychological support for patients. The primary outcomes were the PSG success rate and monitoring interruptions. Secondary outcomes included oxygen saturation, sleep architecture, cardiovascular events, and psychological status (anxiety and depression scores). Between-group comparisons were performed using independent t-tests, chi-square tests, and binary logistic regression to adjust for potential confounders.
Results: The observation group demonstrated a significantly higher monitoring success rate than the control group (96.0% vs. 82.0%, P=0.025; odds ratio [OR] = 5.27, 95% CI: 1.12– 24.84) and fewer monitoring interruptions (16.0% vs. 36.0%, P=0.023). The intervention group also showed significantly improved mean and lowest arterial oxygen saturation, reduced obstructive apneas and awakenings, and shortened sleep latency (all P< 0.0001). No statistically significant difference was observed in the Apnea-Hypopnea Index (AHI) between the groups (P=0.312), suggesting that the intervention did not alter the underlying OSAS severity. Furthermore, the incidence of abnormal blood pressure (4.0% vs. 20.0%, P=0.014) and arrhythmia (2.0% vs. 16.0%, P=0.014) was significantly lower. Post-intervention, the observation group reported significantly lower anxiety and depression scores (P< 0.0001).
Conclusion: A structured nursing intervention was associated with improved PSG technical success, reduced cardiovascular events during monitoring, and better psychological well-being of patients. These findings suggest that comprehensive nursing protocols may optimize diagnostic quality in sleep medicine, although multicenter randomized controlled trials are needed to confirm causality.
Plain Language Summary: Better Care Leads to Better Sleep Tests
Diagnosis of sleep apnea often involves an overnight sleep test (polysomnography [PSG]) with many wires and sensors. This can be uncomfortable and stressful, sometimes leading to failed tests that need to be repeated.
Our study compared a new, more supportive approach to nursing care during these tests with standard care. Nurses provided clearer explanations before the test, checked patients more often to fix any loose sensors, and offered reassurance to help reduce anxiety.
We found that this more thorough care was linked to important differences:Fewer failed tests: The success rate of the sleep test was 96% with comprehensive care compared with 82% with standard care.Safer for patients: Dangerous spikes in blood pressure and irregular heartbeats occurred less frequently.Less stress: Patients reported feeling less anxious and less depressed during the process.
These results suggest that a more attentive and supportive nursing approach may help sleep tests succeed more often, keep patients safer, and improve their experiences. Further research is required to confirm these findings in other hospitals.
Keywords: obstructive sleep apnea, polysomnography, nursing intervention, sleep monitoring, patient safety
Introduction
Obstructive sleep apnea syndrome (OSAS) is a prevalent sleep-related breathing disorder characterized by repetitive episodes of partial or complete upper airway obstruction during sleep, resulting in intermittent hypoxemia, sleep fragmentation, and daytime symptoms, including excessive sleepiness.1,2 The global incidence of OSAS continues to rise, with recent estimates suggesting that nearly one billion adults worldwide may be affected. There is a concerning trend toward a younger age at diagnosis, reflecting both increased awareness and rising obesity rates.3,4
The clinical significance of OSAS extends beyond sleep disruption, as chronic intermittent hypoxemia and sleep fragmentation contribute to multisystem complications, including cardiovascular disease, metabolic dysfunction, cardiac arrhythmias, and, in severe cases, sudden cardiac death during sleep.5,6 These associations underscore the critical importance of accurate diagnosis and timely interventions.
Polysomnography remains the gold standard for OSAS diagnosis, providing comprehensive physiological monitoring during sleep through the simultaneous recording of electroencephalography, electrocardiography, respiratory effort, airflow, oxygen saturation, and body position.7,8 However, the technical complexity of PSG presents practical challenges that may compromise its diagnostic accuracy. Multiple electrode connections and monitoring devices can cause physical discomfort, while an unfamiliar sleep environment and awareness of being monitored may alter natural sleep patterns, potentially leading to monitoring failure or non-representative results.9,10
Despite the diagnostic importance of PSG, limited attention has been given to optimizing the patient experience and monitoring success through structured nursing interventions. Prior studies have shown that patient-related factors, including anxiety about the diagnosis and discomfort with monitoring equipment, significantly influence PSG data quality.11 Emerging evidence suggests that nursing-led interventions in sleep laboratories, including structured patient education, technical quality assurance, and psychological preparation, can improve test completion rates and patient satisfaction.12,13 Furthermore, research in psychosocial nursing has demonstrated that pre-procedural anxiety reduction strategies and patient-centered communication improve cooperation and physiological stability during diagnostic procedures.14,15 However, systematic approaches that integrate technical, educational, and psychological support within a single comprehensive nursing protocol for PSG monitoring remain understudied.
Therefore, this study aimed to evaluate whether a comprehensive nursing intervention protocol specifically designed for PSG monitoring was associated with improved monitoring success rates, clinical parameters, and patient outcomes in patients with OSAS. We hypothesized that structured nursing support addressing both technical and psychological aspects of PSG monitoring would be associated with enhanced data quality and patient cooperation compared with standard care.
Materials and Methods
Study Design and Setting
This prospective observational cohort study evaluated the association between comprehensive nursing interventions and polysomnography (PSG) monitoring outcomes in patients with OSAS. The study was performed at the General Hospital of Northern Theater Command in Shenyang, China, from February 2022 to February 2024. The observational design allowed for a comparison of two standard clinical nursing approaches without experimental manipulation, reflecting real-world clinical practice conditions. However, the non-randomized, sequential allocation of participants to groups introduces potential selection bias and temporal confounding, which should be considered when interpreting these findings.
The study protocol was approved by the Medical Ethics Committee of the General Hospital of Northern Theater Command (Approval No. 2022020025-A) prior to participant enrollment. All participants provided written informed consent after receiving comprehensive information about the study objectives, procedures, and their right to withdraw at any time without affecting their clinical care. The study was conducted in accordance with the Declaration of Helsinki principles for medical research involving human subjects.
Study Population
One hundred consecutive patients diagnosed with OSAS who required PSG monitoring were enrolled in this study cohort. Recruitment was conducted through the Department of Otolaryngology during routine clinical visits (Figure 1). OSAS was diagnosed according to the diagnostic criteria outlined in the 2011 revised edition of the Guidelines for the Diagnosis and Treatment of Obstructive Sleep Apnea Hypoventilation Syndrome. All eligible patients presenting during the study period were approached for participation to minimize selection bias.
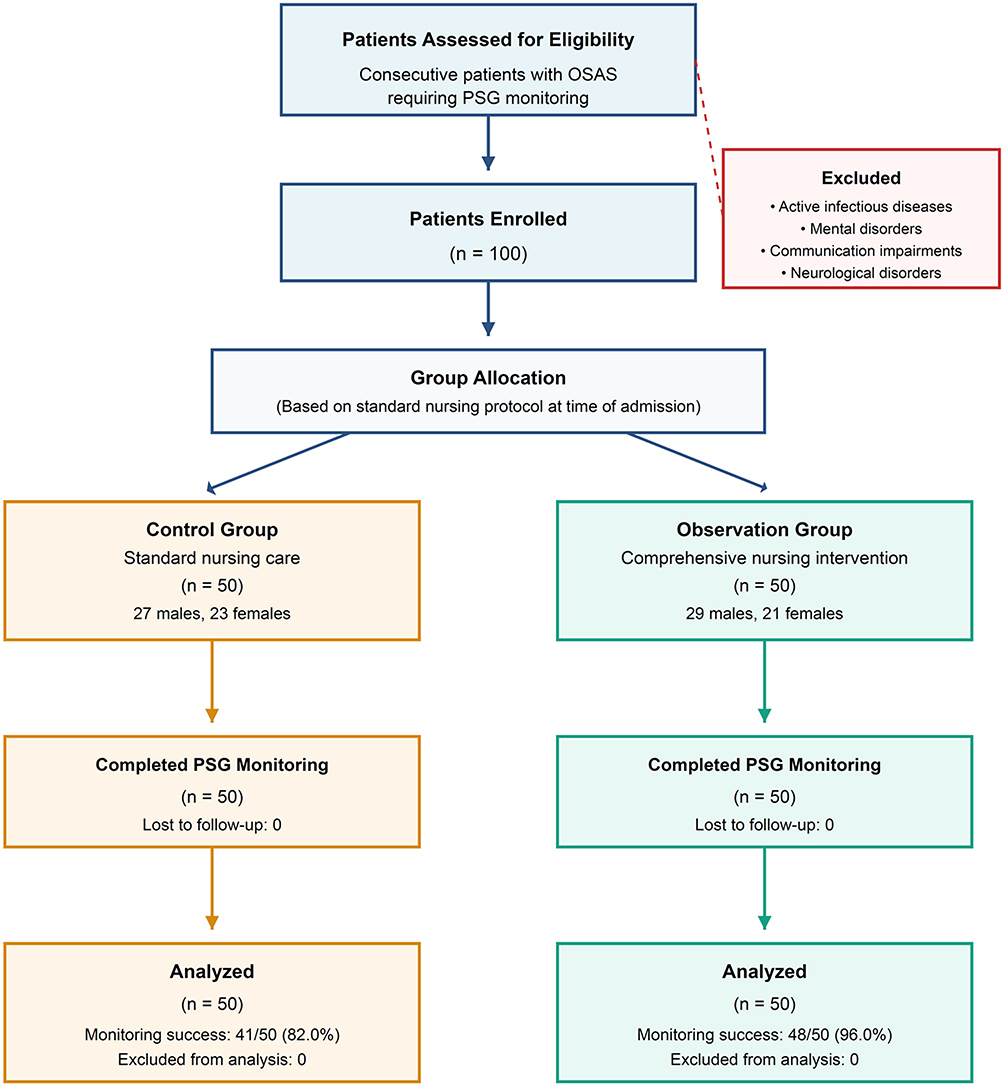 |
Figure 1 STROBE flow diagram showing participant enrollment, allocation, and analysis. This prospective observational cohort study enrolled 100 consecutive patients with obstructive sleep apnea syndrome (OSAS) requiring polysomnography (PSG) monitoring at the General Hospital of Northern Theater Command, Shenyang, China, from February 2022 to February 2024. Participants were sequentially allocated to either the control group (n=50) receiving standard nursing care or the observation group (n=50) receiving comprehensive nursing intervention, based on the nursing protocol available at the time of admission. All enrolled patients completed the study with no losses to follow-up, and no patients were excluded after enrollment due to missing data or protocol violations. |
Inclusion and Exclusion Criteria
Participants were included if they met the following criteria:
- Confirmed diagnosis of OSAS according to the 2011 revised guidelines
- Scheduled for PSG monitoring as part of clinical care
- Demonstrated adequate communication and comprehension abilities
- Provided written informed consent
Exclusion criteria were:
- Presence of active infectious diseases
- Mental disorders affecting normal communication
- Hearing or speech impairments preventing communication
- Withdrawal from the study before completion
- Concurrent neurological disorders
Group Allocation and Characteristics
Participants were allocated to two groups based on the standard nursing protocol available at the time of admission, with 50 patients receiving conventional nursing care (control group, CG) and 50 receiving enhanced PSG monitoring nursing intervention (observation group, OG). This allocation reflected the sequential implementation of the enhanced nursing protocol in our department, with the first cohort (February 2022 to approximately January 2023) receiving standard care and the subsequent cohort (approximately February 2023 to February 2024) receiving the enhanced intervention after the protocol development and staff training. We acknowledge that this sequential design may introduce temporal confounding (eg, from technology updates, seasonal variation, or staff experience changes over time), and the absence of randomization limits causal inference.
The demographic and clinical characteristics were well balanced between the groups. The control group comprised 27 men and 23 women with a mean age of 41.05 ± 1.03 years and a disease duration of 4.15 ± 0.35 months. Among them, 34 and 16 patients presented with moderate and severe OSAS, respectively. The observation group included 29 males and 21 females with a mean age of 41.08 ± 1.06 years and disease duration of 4.19 ± 0.31 months, with 33 moderate and 17 severe OSAS cases.
Intervention Protocols
Clarification Regarding the Scope of This Study
This study focused exclusively on the PSG diagnostic monitoring process and the quality of nursing care delivered during the process. This study was not designed to evaluate or initiate therapeutic interventions, such as positive airway pressure (PAP) therapy. In both groups, patients underwent PSG as a diagnostic procedure, and treatment decisions, including PAP initiation, were made by the treating physician after diagnostic results were obtained, as per standard clinical practice. Therefore, PAP therapy was not withheld, as it was outside the scope of this diagnostic monitoring study.
Standard Care Protocol (Control Group)
Patients in the control group received conventional nursing care during PSG monitoring, which encompassed environmental optimization to ensure quiet and comfortable sleeping conditions, basic nursing procedures, including vital sign monitoring and patient comfort measures, and standard health education regarding OSAS and the PSG monitoring process. This protocol represented the institutional standard of care established before the study period.
Enhanced PSG Monitoring Nursing Intervention (Observation Group)
The observation group received a comprehensive, structured nursing intervention specifically designed for PSG monitoring. All nursing staff delivering the intervention completed a standardized training program of approximately 20 h, which included didactic instruction on PSG monitoring principles, hands-on practice with electrode placement and troubleshooting, patient communication skills, and emergency response protocols. Intervention fidelity was monitored through regular supervisory observations and standardized checklists completed during each monitoring session.
Nurses applied multi-channel sleep monitor electrodes to predetermined locations on the patient’s head, neck, chest, and abdomen for continuous 7-hour overnight monitoring. The monitoring captured electroencephalogram, electrocardiogram, pulse oximetry, electromyogram, blood oxygen saturation, electrooculogram, and limb-movement data.
The enhanced intervention protocol comprised three integrated phases. During the monitoring preparation phase, the nursing staff provided detailed patient education about electrode placement locations, monitored parameters, and the clinical purpose of PSG monitoring to enhance patient understanding and cooperation. The educational materials were standardized and delivered using verbal explanations and visual aids. A comprehensive risk assessment was conducted for each patient, documenting underlying comorbidities and current medications to prepare appropriate emergency-response measures.
The monitoring nursing phase involved meticulous attention to electrode security before initiating PSG monitoring, considering potential movement-related displacement during sleep. Nurses positioned call devices within the easy reach of patients to facilitate the rapid communication of any discomfort. Throughout the monitoring period, nurses performed regular rounds (approximately every 30–60 min) to verify electrode attachment integrity and promptly reconnect any displaced electrodes to minimize data loss.
Cardiovascular vigilance was a specific component of the enhanced protocol. For patients identified as high-risk for cardiovascular events (based on the pre-monitoring risk assessment), pre-emptive consultation with the attending physicians was conducted to ensure that existing cardiovascular medications were appropriately timed and administered before the monitoring session. During monitoring, nurses maintained continuous observation of vital sign trends displayed on the monitoring system, with predefined thresholds for alerting the on-call physician (eg, blood pressure exceeding 160/120 mmHg, new-onset arrhythmia, or oxygen saturation falling below 80). This component was purely observational and preventive in nature. No new medications were initiated by the nursing staff during PSG monitoring, and all clinical decisions regarding acute management were made by the attending physician when consulted. All monitoring interruptions and interventions were documented in standardized nursing records.
Psychological support was integrated throughout the intervention, recognizing that patients often experience significant emotional distress following an OSAS diagnosis. The nursing staff maintained a warm and professional demeanor while introducing patients to the ward environment, available facilities, and the medical team. This psychological support component aimed to reduce anxiety-related sleep disruptions during monitoring.
Outcome Measures
Primary Outcome: Monitoring Success Rate
PSG monitoring success was defined as complete acquisition of all eight essential parameters within the specified monitoring period: electroencephalography, electrocardiography, electrooculogram, snoring detection, SpO2, nasal and oral airflow, body position, and chest and abdominal movements. These eight parameters were selected based on international PSG quality standards (American Academy of Sleep Medicine guidelines), which require simultaneous multi-channel recording for valid sleep study interpretation.16 Monitoring was classified as unsuccessful if any parameter was incompletely captured, as the absence of any single channel may render the study uninterpretable for diagnostic purposes. Partial monitoring failures (ie, brief signal interruptions that were corrected during nursing rounds and did not result in loss of interpretable data for the full monitoring period) were documented but classified as monitoring interruptions rather than failures, provided that the final dataset contained complete data for all eight parameters. The frequency of monitoring interruptions was documented as a secondary measure of monitoring quality.
Secondary Outcomes
Clinical parameters were assessed by measuring the mean arterial oxygen saturation (MSaO2) and least arterial oxygen saturation (LSaO2) during the PSG monitoring period. Sleep quality indicators included the quantification of obstructive apnea frequency, awakening frequency, sleep latency, hypoventilation frequency, and the Apnea-Hypopnea Index (AHI) during the monitoring period.
Safety outcomes were monitored throughout PSG recordings, with particular attention to cardiovascular events. Abnormal blood pressure was defined as readings exceeding 160/120 mmHg, and any cardiac rhythm disturbance was documented as an arrhythmia event. These thresholds were based on the established clinical guidelines for acute hypertensive episodes and clinically significant arrhythmias.
Psychological status was evaluated using validated instruments: the Self-Rating Depression Scale (SDS) and Self-Rating Anxiety Scale (SAS). Both scales comprise 20 items, with established cutoff scores for severity classification. For the SDS, scores of 53–62, 63–72, and >73 indicated mild, moderate, and severe depression, respectively. For the SAS, the corresponding severity categories were defined by scores of 50–59, 60–69, and >70 points.
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0. The sample size of 50 participants per group was determined to provide 80% power to detect a 15% difference in the monitoring success rate between groups, assuming a baseline success rate of 80% based on prior institutional audit data and using a two-sided test with α = 0.05.
Continuous variables were assessed for normality using the Shapiro–Wilk test, and the equality of variances was evaluated using Levene’s test. Variables conforming to a normal distribution with equal variances are expressed as mean ± standard deviation and compared between groups using independent samples t-tests. Categorical variables were presented as frequencies and percentages, with between-group comparisons performed using chi-square tests or Fisher’s exact tests when expected cell counts were below 5.
To account for potential confounding from baseline characteristics and the sequential allocation design, binary logistic regression was performed for the primary outcome (monitoring success), adjusting for age, sex, disease duration, and OSAS severity. Effect sizes were calculated as Cohen’s d for continuous outcomes and odds ratios (OR) with 95% confidence intervals (CI) for categorical outcomes. Given the multiple secondary outcome comparisons, the results were interpreted with consideration of the increased risk of Type I error, and Bonferroni-corrected significance thresholds were noted where applicable.
Correlation analyses between clinical parameters and psychological scores were conducted using Pearson’s correlation coefficients. Statistical significance was defined as P < 0.05 for all primary analyses.
Results
Baseline Characteristics and Group Comparability
The demographic and clinical characteristics of the participants demonstrated excellent balance between the control and observation groups, with no statistically significant differences observed in any baseline parameter (all P > 0.05, Table 1). This comparability in age distribution (41.05±1.03 vs. 41.08±1.06 years, P = 0.841), sex composition (46.0% vs. 42.0% male, P = 0.687), disease duration (4.15±0.35 vs. 4.19±0.31 months, P = 0.482), and OSAS severity distribution (68.0% vs. 66.0% moderate cases, P = 0.832) provided a foundation for comparing intervention effects, although the absence of randomization means that unmeasured confounders cannot be excluded.
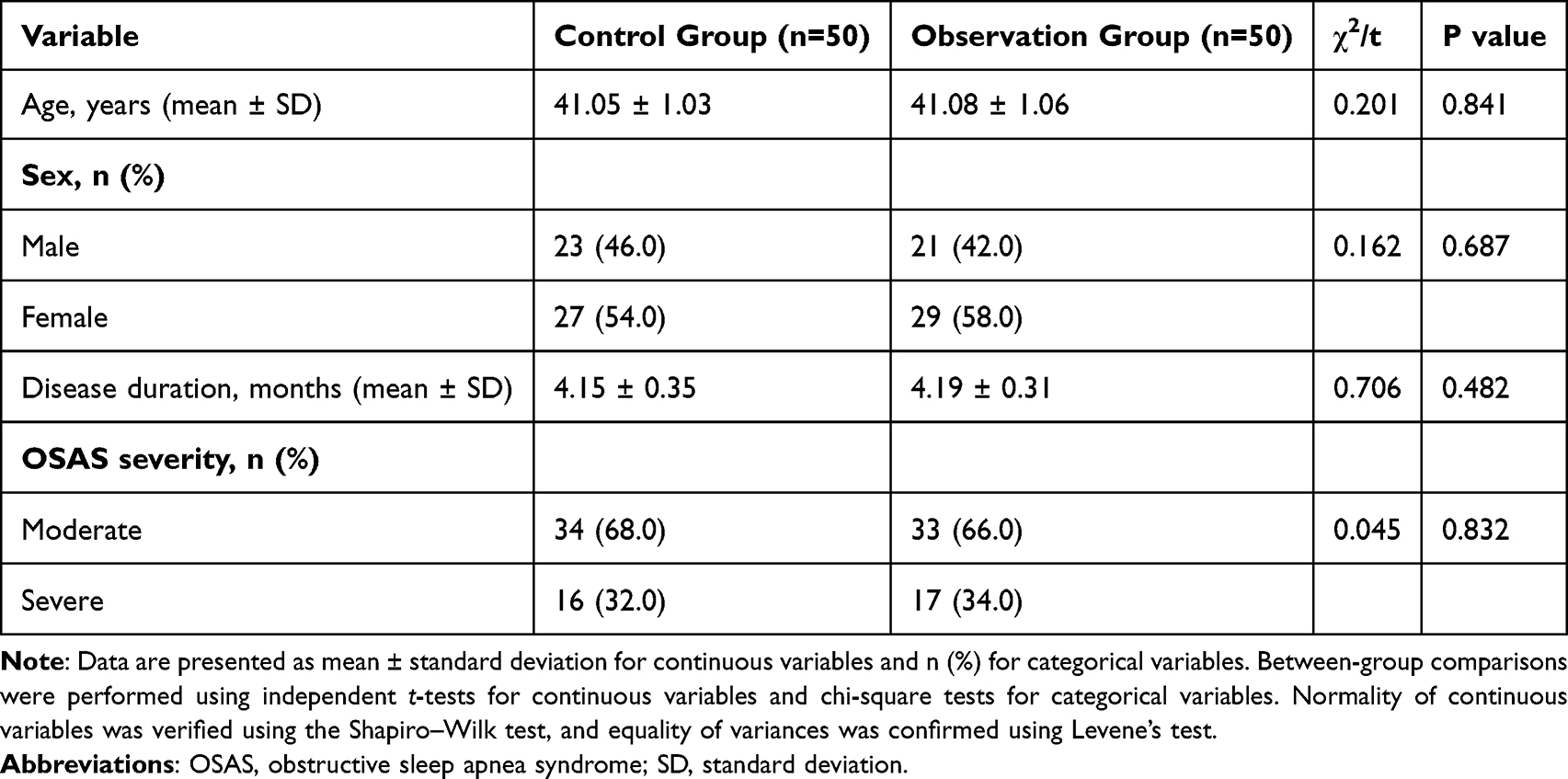 |
Table 1 Baseline Demographic and Clinical Characteristics of Study Participants |
Impact on PSG Monitoring Quality
The implementation of enhanced nursing interventions was associated with substantial improvements in PSG monitoring quality parameters (Table 2). The monitoring success rate in the observation group reached 96.0% (48/50), compared with 82.0% (41/50) in the control group (χ2 = 5.005, P = 0.025; OR = 5.27; 95% CI: 1.12–24.84). After adjusting for age, sex, disease duration, and OSAS severity in a binary logistic regression model, the association remained significant (adjusted OR = 5.41, 95% CI: 1.10–26.62, P = 0.038). This improvement was paralleled by a reduction in monitoring interruptions, which occurred in 16.0% of patients in the observation group compared to 36.0% in the control group (χ2 = 5.198, P = 0.023; OR = 0.34, 95% CI: 0.13–0.87).
 |
Table 2 Polysomnography Monitoring Outcomes and Failure Patterns |
Analysis of monitoring failure patterns revealed differences between the groups. In the control group, nine monitoring failures (18.0%) resulted from nasal airflow sensor detachment (n=2), environmental disturbances leading to insufficient sleep (n=2), nocturnal gastrointestinal symptoms (n=2), unresolved electrode detachment (n=1), and SpO2 signal loss (n=2). The observation group experienced only two failures (4.0%): one environmental disturbance and one instance of SpO2 signal loss. The individual causes of failure were not statistically compared because of the small cell sizes.
Clinical Oxygenation Parameters
The observation group demonstrated improved arterial oxygenation parameters compared with the control group during sleep monitoring (Figure 2A and B). Prior to the intervention, both groups exhibited comparable baseline oxygenation statuses, with no significant differences in MSaO2 or LSaO2 values (P > 0.05). Following the intervention period, the observation group showed significantly higher MSaO2 (effect size: Cohen’s d = 0.89, 95% CI: 0.48–1.30) and LSaO2 values (Cohen’s d = 0.95, 95% CI: 0.53–1.36) than the control group (both P < 0.0001; Supplementary Table S1). These improvements in oxygen saturation parameters may reflect several factors, including reduced sleep fragmentation, improved patient positioning through nursing-assisted adjustments, and more reliable sensor maintenance during the monitoring period.
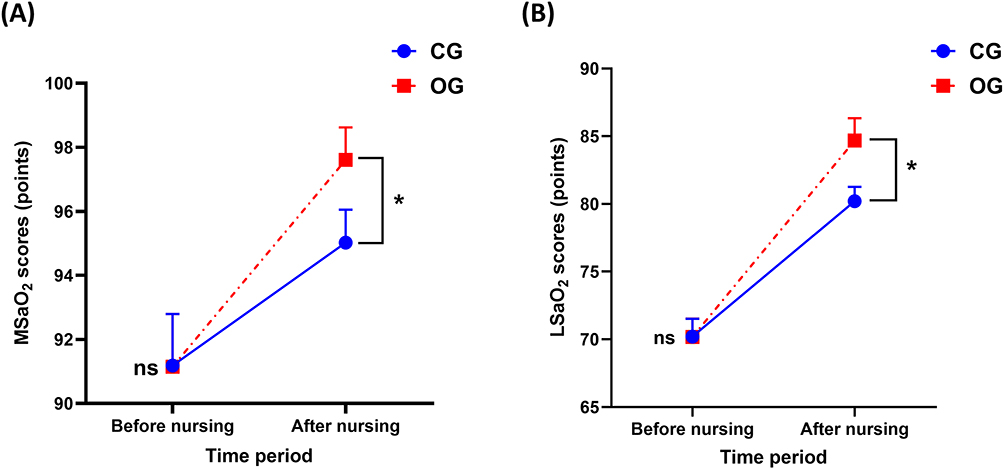 |
Figure 2 Arterial oxygen saturation parameters before and after nursing intervention. Comparison of (A) mean arterial oxygen saturation (MSaO2) and (B) least arterial oxygen saturation (LSaO2) between control group (CG, n=50) and observation group (OG, n=50) before and after implementation of nursing interventions. Data are presented as mean ± standard error of the mean. ns = not significant (P > 0.05); *P < 0.0001. |
Apnea-Hypopnea Index
No statistically significant difference was observed in the overall AHI between the observation and control groups (mean AHI: 38.4 ± 12.6 vs. 40.1 ± 13.2 events/hour, P = 0.312; Cohen’s d = 0.13) (Table 3). This finding is consistent with the expectation that a nursing intervention targeting monitoring quality would not alter the underlying severity of OSAS and supports the interpretation that observed differences in other parameters reflect improved monitoring conditions rather than a change in disease pathology.
 |
Table 3 Apnea-Hypopnea Index Comparison Between Groups |
Sleep Architecture and Respiratory Events
Analysis of the sleep quality parameters revealed differences favoring the enhanced nursing intervention across multiple domains (Figure 3A–D). The observation group showed reduced obstructive apnea frequency (Cohen’s d = 0.92, 95% CI: 0.50–1.33; P < 0.0001), fewer awakening episodes (Cohen’s d = 1.05, 95% CI: 0.62–1.47; P < 0.0001), shorter sleep onset latency (Cohen’s d = 0.87, 95% CI: 0.46–1.28; P < 0.0001), and lower hypoventilation frequency (Cohen’s d = 0.78, 95% CI: 0.37–1.18; P < 0.0001) than the controls. After applying the Bonferroni correction for four comparisons (adjusted α = 0.0125), all differences remained statistically significant (Supplementary Table S1).
 |
Figure 3 Sleep architecture parameters during polysomnography monitoring. Sleep quality indicators in control group (CG, n=50) versus observation group (OG, n=50) following nursing intervention. Four parameters were assessed: (A) Obstructive apnea frequency (events per hour), (B) Awakening frequency (events per hour), (C) Sleep onset latency (minutes), and (D) Hypoventilation frequency (events per hour). *P < 0.0001 for all comparisons. |
Safety Profile and Adverse Events
The enhanced nursing protocol was associated with reduced cardiovascular events during PSG monitoring (Table 4). Abnormal blood pressure episodes (>160/120 mmHg) occurred in 4.0% of observation group patients compared to 20.0% in the control group (χ2 = 6.061, P = 0.014; OR = 0.17, 95% CI: 0.03–0.80). Similarly, arrhythmia events were documented in 2.0% of observation group patients versus 16.0% of controls (χ2 = 5.983, P = 0.014; OR = 0.11, 95% CI: 0.01–0.88). These safety differences may reflect the proactive risk assessment and preventive measures incorporated into the enhanced nursing protocol, including pre-monitoring medication optimization and vigilance for early signs of cardiovascular instability, although the contribution of reduced patient anxiety and improved sleep quality to hemodynamic stability cannot be excluded.
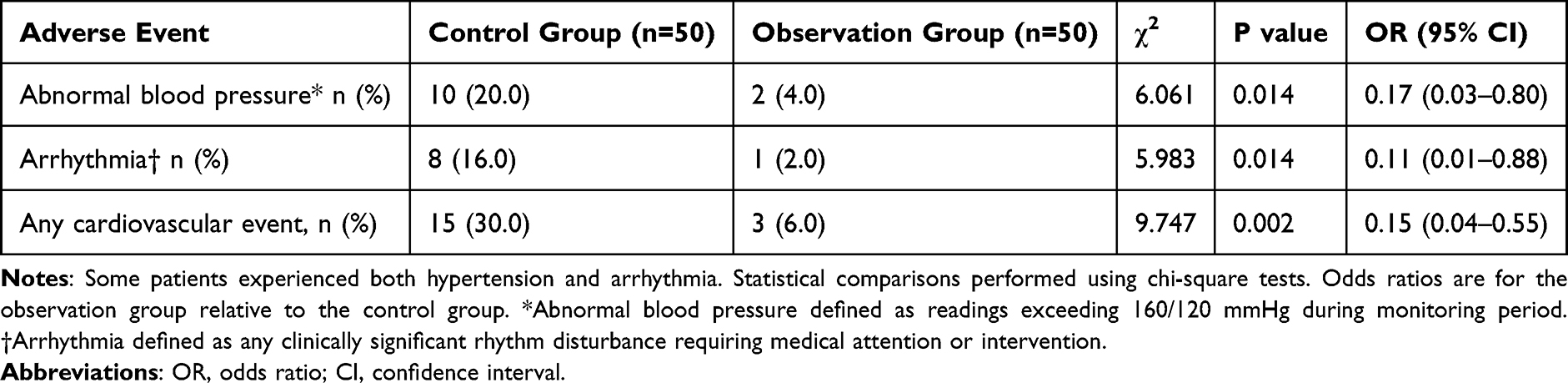 |
Table 4 Cardiovascular Adverse Events During Polysomnography Monitoring |
Psychological Outcomes
The psychological impact of the nursing intervention was evaluated using standardized anxiety and depression assessments (Figure 4A and B). Baseline psychological scores showed no significant differences between the groups (P > 0.05), indicating comparable emotional statuses at study entry. Following the intervention, the observation group exhibited significantly lower anxiety scores on the SAS (Cohen’s d = 1.12, 95% CI: 0.69–1.55; P < 0.0001) and reduced depression scores on the SDS (Cohen’s d = 0.98, 95% CI: 0.56–1.40; P < 0.0001) than the control group. However, it should be noted that the SAS and SDS are self-report instruments, and the absence of blinding may have influenced patient responses.
 |
Figure 4 Psychological outcomes assessed by standardized questionnaires. Changes in anxiety and depression scores between control group (CG, n=50) and observation group (OG, n=50) before and after nursing intervention. (A) Self-rating Anxiety Scale (SAS) scores, where scores of 50–59, 60–69, and ≥70 indicate mild, moderate, and severe anxiety, respectively. (B) Self-rating Depression Scale (SDS) scores, where scores of 53–62, 63–72, and ≥73 indicate mild, moderate, and severe depression, respectively. Data are presented as mean ± standard error of the mean. ns = not significant (P > 0.05); *P < 0.0001. |
Correlation Between Oxygenation and Psychological Status
Correlation analysis revealed significant inverse relationships between oxygenation parameters and psychological distress measures following the nursing intervention (Figure 5A–D). Both MSaO2 and LSaO2 values demonstrated strong negative correlations with SAS and SDS scores in both study groups (all P < 0.0001), indicating that patients with better oxygen saturation profiles reported less anxiety and depression. These correlations are cross-sectional and do not establish directionality; the observed associations may reflect shared, underlying mechanisms rather than a direct causal pathway.
 |
Figure 5 Correlation analysis between oxygenation parameters and psychological distress scores. Scatter plots demonstrating the relationship between arterial oxygen saturation parameters and psychological assessment scores following nursing intervention in both study groups (n=100 total). (A) Correlation between mean arterial oxygen saturation (MSaO2) and Self-rating Anxiety Scale (SAS) scores. (B) Correlation between MSaO2 and Self-rating Depression Scale (SDS) scores. (C) Correlation between least arterial oxygen saturation (LSaO2) and SAS scores. (D) Correlation between LSaO2 and SDS scores. Pearson correlation coefficients (r) and significance levels are shown for each analysis. All correlations were negative and statistically significant (P < 0.0001). |
Discussion
This prospective observational study found that a structured nursing intervention protocol was associated with improved PSG monitoring success rates from 82% to 96% in patients with OSAS. The intervention was also associated with fewer monitoring interruptions, reduced cardiovascular events during monitoring, and improved patient psychological well-being during the diagnostic process. These findings suggest that the quality of nursing care may influence the technical success of sleep studies and patient outcomes, although the observational design limits the causal inference.
The 14% absolute improvement in the monitoring success rate represents a notable enhancement in diagnostic reliability. Our success rate of 96% compares favorably with previously reported rates, which typically range from 70% to 85% in routine clinical practice.17 The near elimination of electrode detachment and patient-related monitoring failures in the observation group suggests that regular nursing rounds and proactive electrode maintenance may effectively prevent the common causes of PSG failure. This improvement has practical implications, as failed studies require repeat testing, increasing healthcare costs, and delaying diagnosis and treatment initiation.
The reduction in cardiovascular events during monitoring deserves particular attention. We observed lower rates of hypertensive episodes and arrhythmias in the intervention group compared with the control group. While OSAS patients inherently carry cardiovascular risk, the stress of unfamiliar monitoring environments and equipment discomfort may exacerbate hemodynamic instability.18 The enhanced protocol’s emphasis on pre-monitoring risk assessment, medication optimization, and continuous observation may have contributed to mitigating these risks. However, it is important to acknowledge that the Hawthorne effect, whereby patients may behave differently or report differently when they know they are receiving enhanced attention, could partially account for some observed differences, particularly in subjective outcomes.
The improved oxygenation parameters in the intervention group warrant careful interpretation of the results. Notably, the overall AHI did not differ significantly between the groups (P = 0.312), indicating that the nursing intervention was not associated with a change in the underlying severity of OSAS. Therefore, the observed improvements in MSaO2 and LSaO2 likely reflect improved monitoring conditions rather than a therapeutic effect on the airway pathology. Several mechanisms may contribute to this finding. First, more frequent nursing rounds and sensor maintenance may have ensured more reliable and continuous pulse oximetry readings, as sensor displacement or poor contact can lower recorded oxygen saturation values. Second, patients experiencing less anxiety and fewer technical disruptions may have achieved better-quality sleep, resulting in more stable breathing patterns and reduced transient desaturation events. Third, nursing-assisted positioning adjustments during the monitoring period may have optimized airway patency in some patients. We acknowledge that distinguishing between true physiological improvement and improved measurement accuracy is not possible within this study design, which represents an important limitation.
An additional finding was the strong inverse correlation between oxygenation parameters and psychological distress. While we cannot establish causality from our observational design, this relationship suggests that patients’ emotional states during PSG may be related to physiological measurements. Previous studies have documented a high prevalence of anxiety and depression in OSAS patients,19 but our findings raise the possibility that psychological factors may influence the quality of diagnostic testing. The structured psychological support component of our intervention, including patient education and emotional reassurance, was associated with significantly reduced anxiety and depression scores. However, these outcomes were measured using self-report instruments in an unblinded study, and temporal effects, including natural adaptation to the hospital environment over time and environmental differences between the two study periods, could also have contributed to the observed differences.
Our findings should be interpreted in the context of prior research on nursing interventions in sleep medicine. While the concept of nursing-led quality improvement in sleep laboratories is not entirely new, the integration of technical, educational, and psychological support components within a single structured protocol represents an advancement over interventions targeting individual components in isolation.20,21 Patient-centered care frameworks have shown benefits across various diagnostic and therapeutic settings, and our results extend this evidence to the sleep laboratory context.22,23 The intervention’s effectiveness likely stems from addressing multiple failure points simultaneously rather than any single component being solely responsible for the improvements observed.
The practical implementation of our protocol requires consideration of resource allocations. While the intervention demanded additional nursing time and training, the reduction in failed studies and adverse events may offset these costs. Each failed PSG requires rescheduling, repeated resource utilization, and a delayed treatment initiation. Future cost-effectiveness analyses should quantify these trade-offs to guide institutional policy-making.
This study has several important limitations that should be considered. First, the observational design and sequential group allocation prevent definitive causal conclusions about the intervention’s effectiveness. Because the control group was enrolled first and the observation group second, improvements in the observation group could partly reflect temporal factors such as accumulated staff experience, equipment upgrades, or seasonal variations in patient characteristics, rather than the intervention alone. Second, the absence of randomization means that despite balanced baseline characteristics, unmeasured confounders may have influenced the results. Third, neither participants nor assessors were blinded to group assignment, which could introduce bias, particularly for subjective outcomes such as anxiety and depression scores. Fourth, the single-center setting in a tertiary hospital may limit generalizability to community sleep laboratories with different staffing levels and resources. Fifth, we did not assess long-term outcomes such as treatment adherence or clinical improvement following diagnosis, which would strengthen the argument for enhanced nursing protocols. Sixth, we did not employ multivariate analyses for all secondary outcomes, and the potential for Type I error from multiple comparisons should be considered when interpreting secondary findings. Finally, the possibility of a Hawthorne effect, whereby enhanced attention itself, rather than the specific intervention components, produced improvements, cannot be excluded.
Future research should address these limitations through multicenter randomized controlled trials with appropriate blinding, where feasible. Future studies should examine which components of the comprehensive intervention are most critical for success, potentially allowing for streamlined protocols that maintain effectiveness while minimizing resource requirements. Investigating patient characteristics that predict greater benefits from enhanced nursing support could enable targeted intervention strategies. Long-term follow-up examining whether improved initial PSG experiences translate to better treatment acceptance and adherence would provide valuable insights into the downstream effects of nursing care.
In conclusion, implementing a structured nursing intervention protocol during PSG monitoring was associated with improved monitoring success rates, reduced adverse events, and enhanced patient well-being in patients with OSAS. The multifaceted approach of the intervention, which addressed the technical, safety, and psychological aspects of PSG, was associated with better outcomes than standard care across all measured domains. These findings provide preliminary evidence supporting the integration of comprehensive nursing protocols in sleep laboratories and highlight the need for confirmation through multicenter randomized controlled trials with appropriate blinding and longer follow-up to establish the generalizability and causal impact of such interventions on sleep quality.
Data Sharing Statement
The datasets generated and analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Medical Ethics Committee of the General Hospital of Northern Theater Command (Approval No. 2022020025-A). This study was conducted in accordance with the Declaration of Helsinki principles for medical research involving human subjects. All participants provided written informed consent prior to enrollment after receiving comprehensive information about the study objectives, procedures, and their right to withdraw at any time without affecting their clinical care.
Author Contributions
All authors made significant contributions to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Suri TM, Bhargava S, Akshara KT, et al. Postnatal growth trajectories and risk of obstructive sleep apnea in middle age: a cohort study. Pediatr Pulmonol. 2025;60(1):e27396. doi:10.1002/ppul.27396
2. Lee K. Influence of the partner’s obstructive sleep apnea on metabolic syndrome in couples. Maturitas. 2024;191:108147. doi:10.1016/j.maturitas.2024.108147
3. Knowlden AP, Winchester LJ, MacDonald HV, Geyer JD, Higginbotham JC. Associations among cardiometabolic risk factors, sleep duration, and obstructive sleep apnea in a southeastern us rural community: cross-sectional analysis from the SLUMBRx-PONS study. JMIR Form Res. 2024;8:e54792. doi:10.2196/54792
4. Breitkopf M, Ahrens E, Herrmann ML, et al. Preoperative hypoxic biomarkers and postoperative delirium in patients with obstructive sleep apnea. J Anesth. 2024. doi:10.1007/s00540-024-03417-2
5. Maeda H, Matsuno K, Tamura Y, Sogabe S, Yoshida KI. Postmorterm computed tomography and autopsy to confirm sudden death due to tracheal compression by mediastinal fat tissue in a young man with obesity. Cureus. 2023;15(1):e33322. doi:10.7759/cureus.33322
6. Zhu W, Xiang L, Long Y, Xun Q, Kuang J, He L. Cluster analysis of clinical phenotypic heterogeneity in obstructive sleep apnea assessed using photoplethysmography. Sleep Med. 2023;102:134–15. doi:10.1016/j.sleep.2022.12.023
7. Sukharom R, Tovichien P, Udomittipong K, Tiamduangtawan P, Chotinaiwattarakul W. Polysomnographic features of children with obesity: body mass index predict severe obstructive sleep apnea in obese children? Clin Exp Pediatr. 2024;68:80–90. doi:10.3345/cep.2024.00066
8. Garcia-Vicente C, Gutierrez-Tobal GC, Vaquerizo-Villar F, Martin-Montero A, Gozal D, Hornero R. SleepECG-Net: explainable deep learning approach with ECG for pediatric sleep apnea diagnosis. IEEE J Biomed Health Inform. 2024. doi:10.1109/jbhi.2024.3495975
9. Nosetti L, Zaffanello M, Simoncini D, et al. Prioritising polysomnography in children with suspected obstructive sleep apnoea: key roles of symptom onset and sleep questionnaire scores. Children. 2024;11(10):1228. doi:10.3390/children11101228
10. Park MJ, Choi JH, Kim SY, Ha TK. A deep learning algorithm model to automatically score and grade obstructive sleep apnea in adult polysomnography. Digit Health. 2024;10:20552076241291707. doi:10.1177/20552076241291707
11. Dimitri F, Islind AS, Ólafsdóttir KA, et al. Feasibility and usability of three consecutive nights with self-applied, home polysomnography. J Sleep Res. 2024;34(2):e14286. doi:10.1111/jsr.14286
12. Ritmala‐Castren M, Salanterä S, Holm A, Heino M, Lundgrén‐Laine H, Koivunen M. Sleep improvement intervention and its effect on patients’ sleep on the ward. J Clin Nurs. 2022;31(1–2):275–282. doi:10.1111/jocn.15906
13. Kapur VK, Johnston JC, Rueschman M, et al. Patient satisfaction with sleep study experience: findings from the sleep apnea patient-centered outcomes network. Sleep. 2018;41(8):zsy093. doi:10.1093/sleep/zsy093
14. Agüero‐Millan B, Abajas‐Bustillo R, Ortego‐Maté C. Efficacy of nonpharmacologic interventions in preoperative anxiety: a systematic review of systematic reviews. J Clin Nurs. 2023;32(17–18):6229–6242. doi:10.1111/jocn.16755
15. Oliveira P, Pires R, Silva R, Sequeira C. Design of a nursing psychoeducation program to reduce preoperative anxiety in adults. Front Public Health. 2024;12:1391764. doi:10.3389/fpubh.2024.1391764
16. Berry RB, Brooks R, Gamaldo C, et al. AASM scoring manual updates for 2017 (version 2.4). J Clin Sleep Med. 2017;13:665–666.
17. Bozkurt F, Uçar MK, Bilgin C, Zengin A. Sleep-wake stage detection with single channel ECG and hybrid machine learning model in patients with obstructive sleep apnea. Phys Eng Sci Med. 2021;44(1):63–77. doi:10.1007/s13246-020-00953-5
18. Wang W, Pang J, Zhang YX, Mo YM, Zhang J, Wei ZH. Clinical effect of personalized adjustable mandibular advancement device on obstructive sleep apnea. Br J Hosp Med. 2024;85(8):1–17. doi:10.12968/hmed.2024.0189
19. Wu M, Xue P, Yan J, Benedict C. Association between age and comorbid insomnia and sleep apnea. Sleep Med. 2024;124:659–661. doi:10.1016/j.sleep.2024.11.011
20. Kamdar BB, Yang J, King LM, et al. Developing, implementing, and evaluating a multifaceted quality improvement intervention to promote sleep in an ICU. Am J Med Qual. 2014;29(6):546–554. doi:10.1177/1062860613509684
21. Huang D, Li Y, Ye J, Liu C, Shen D, Lv Y. Different nursing interventions on sleep quality among critically ill patients: a systematic review and network meta-analysis. Medicine. 2023;102(52):e36298. doi:10.1097/MD.0000000000036298
22. Rathert C, Wyrwich MD, Boren SA. Patient-centered care and outcomes: a systematic review of the literature. Med Care Res Rev. 2013;70(4):351–379. doi:10.1177/1077558712465774
23. Handley SC, Bell S, Nembhard IM. A systematic review of surveys for measuring patient-centered care in the hospital setting. Medical Care. 2021;59(3):228–237. doi:10.1097/MLR.0000000000001474
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Ring Pulse Oximetry Using Reflective Photoplethysmography and PSG in the Detection of OSA in Chinese Adults: A Pilot Study
Zhao R, Xue J, Zhang X, Peng M, Li J, Zhou B, Zhao L, Penzel T, Kryger M, Dong XS, Gao Z, Han F
Nature and Science of Sleep 2022, 14:1427-1436
Published Date: 18 August 2022
New Metrics from Polysomnography: Precision Medicine for OSA Interventions
Guo J, Xiao Y
Nature and Science of Sleep 2023, 15:69-77
Published Date: 9 March 2023
Association Between Sleep Efficiency and Hypertension in Chinese Obstructive Sleep Apnea Patients
Xia N, Wang H, Chen Y, Fan XJ, Nie XH
Nature and Science of Sleep 2023, 15:79-88
Published Date: 10 March 2023
Waiting for in-Lab Polysomnography May Unnecessarily Prolong Treatment Start in Patients with Moderate or Severe OSA at Home Sleep Apnea Testing
Pordzik J, Seifen C, Ludwig K, Ruckes C, Huppertz T, Matthias C, Gouveris H
Nature and Science of Sleep 2024, 16:1881-1889
Published Date: 5 December 2024
Association Between Nocturnal Hypoxemia Parameters and Coronary Microvascular Dysfunction: A Cross-Sectional Study
Feng L, Zhao X, Song J, Yang S, Xiang J, Zhang M, Tu C, Song X
Nature and Science of Sleep 2024, 16:2279-2288
Published Date: 28 December 2024