Back to Journals » Nature and Science of Sleep » Volume 14
Comparison of Ring Pulse Oximetry Using Reflective Photoplethysmography and PSG in the Detection of OSA in Chinese Adults: A Pilot Study
Authors Zhao R, Xue J ![]() , Zhang X, Peng M
, Zhang X, Peng M ![]() , Li J, Zhou B, Zhao L, Penzel T
, Li J, Zhou B, Zhao L, Penzel T ![]() , Kryger M, Dong XS, Gao Z, Han F
, Kryger M, Dong XS, Gao Z, Han F ![]()
Received 24 March 2022
Accepted for publication 27 July 2022
Published 18 August 2022 Volume 2022:14 Pages 1427—1436
DOI https://doi.org/10.2147/NSS.S367400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Rui Zhao,1 Jianbo Xue,1 Xueli Zhang,1 Maohuan Peng,1 Jing Li,1 Bing Zhou,1 Long Zhao,1 Thomas Penzel,2 Meir Kryger,3 Xiao Song Dong,1 Zhancheng Gao,1 Fang Han1
1Department of Pulmonary and Critical Care Medicine, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Sleep Medicine Center, Charité-Universitätsmedizin, Berlin, Germany; 3Division of Pulmonary, Critical Care and Sleep Medicine, Yale School of Medicine, New Haven, CT, USA
Correspondence: Xiao Song Dong; Zhancheng Gao, Department of Pulmonary and Critical Care Medicine, Peking University People’s Hospital, No. 11 Xizhimen Nandajie, Xicheng District, Beijing, 100044, People’s Republic of China, Email [email protected]; [email protected]
Objective: A novel ring-worn oximeter (Circul) uses reflective photoplethysmography and automated signal processing to calculate oxygen desaturations. We evaluated the ability of Circul to detect obstructive sleep apnea in Chinese adults.
Methods: We recruited 207 Chinese Han subjects: 70% males, mean age 48.2± 14.7 years, mean BMI 27.6± 4.8 kg/m2 and mean AHI 28.6± 25.2 events/h. All participants underwent simultaneous polysomnography (PSG) and Circul testing in a sleep laboratory. Oxygen desaturation index (ODI), mean oxygen saturation (MSpO2), cumulative time at SpO2< 90% (CT90), cumulative percentage of sleep time spent with SpO2< 90% (CT90/TST) were derived and compared for the Circul and the PSG.
Results: The ODI was 25.3± 24.5 events/h using PSG and 22.2± 24.5 events/h using Circul (P< 0.0001), with an intraclass correlation coefficient (ICC) of 0.884. CT90 and CT90/TST between the two methods were not different; the MSpO2 level calculated by PSG was slightly lower than Circul, 95.0% (93.0– 96.0%) vs 95.3% (93.9– 96.6%), P< 0.0001. Circul-ODI had a good correlation (r=0.91, p< 0.0001) and close agreement with PSG-AHI (Bland-Altman analysis: Mean Difference 6.4, 95% CI − 14.8 to 27.5 events/h). Using a threshold of AHI ≥ 5 events/h, the Circul had 87% sensitivity, 83% specificity, 5.09 positive likelihood ratio (LR+), 86% accuracy, and 0.929 area under the curve (AUC).
Conclusion: Circul ring pulse oximetry can detect OSA with reasonable reliability. The Circul system is a reliable and comfortable choice for OSA assessment.
Keywords: obstructive sleep apnea, reflective photoplethysmography, pulse oximetry, polysomnography
Introduction
Obstructive sleep apnea (OSA) is a chronic disorder that negatively impacts cardio-cerebrovascular and metabolic diseases, cognitive impairment, traffic accidents, and mortality.1–4 It is estimated that almost 1 billion adults aged 30–69 years are affected by OSA, and 425 million have moderate to severe OSA.5 However, OSA remains significantly underdiagnosed and undertreated all over the world. In-laboratory attended polysomnography (PSG) is the gold standard for diagnosing OSA. However, the capacity for performing PSG is limited. Pulse oximetry is an accessible, simple, cost-effective technique routinely used in many clinical settings. It is the most common single-channel portable monitor (PM) device for detecting OSA and has been widely validated in adults and pediatrics.6–8 Oxygen desaturation index (ODI), a reliable indicator of hypoxia, is always coupled with airflow, respiratory effort, and heart rate in most type III PMs, which has been recommended in out-of-center sleep testing (OCST).9 In previous studies evaluating the utility of overnight oximetry as a diagnostic tool for OSA, underestimation of apnea–hypopnea index (AHI) and decreased negative predictive value (NPV) were found.10,11 Traditional pulse oximeters use transmissive photo-plethysmography (tPPG) sensors, which are usually placed on fingertips, toes, or earlobes. The most commonly used is finger-worn pulse oximetry, but wearing a finger-worn probe overnight may be uncomfortable for subjects.
Pulse oximetry probes that use reflectance technology have been developed. For example, Circul, a novel ring pulse oximetry (Megahealth Medical, Inc. Zhejiang, China) based on reflective PPG (rPPG), is designed to monitor SpO2, pulse rate, and movement. This device uses automated signal processing, feature extraction, and pattern recognition by an algorithm inside the ring. In this study, we evaluated the accuracy of this ring-pulse oximetry and its clinical utility in the assessment of OSA.
Methods
Participants
Two hundred and seven subjects with suspected sleep apnea were recruited from the Sleep Disorders Clinic at the Peking University People’s Hospital, Beijing, China. Eligible participants were between the ages of 18 to 80 years and had no previous sleep testing or treatment. Individuals were excluded from the study for the following reasons: 1) overnight oxygen use, ventilatory support; 2) prior diagnosis of chronic heart failure, pacemaker insertion, chronic obstructive pulmonary disease, or obesity hypoventilation syndrome; 3) finger deformity, history of peripheral vascular disease; 4) prior diagnosis of other sleep disorders, such as narcolepsy, parasomnia, rapid eye movement behavior disorder, jet lag or shift worker by history over the past three months. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Peking University People’s Hospital. Informed consent was obtained from all patients.
Circul System
Circul is a novel wearable device for oxygen saturation and heart rate monitoring, movement measurement, and sleep/wake analysis, based on photo-plethysmography (PPG) techniques, 3-axis accelerometer signals, advanced automated-signal processing, and sleep pattern recognition. The Circul incorporates all required components for calculating and measuring oxygen saturation, heart pulse rate, and body movement. The device features an adjustable fit (using multiple ring sizes and a patented spring fit) for comfort and can be worn continuously (Figure 1A). Circul uses a reflectance PPG technology whereby a tiny sensor is placed on the proximal phalangeal radialis finger (Figure 1B) that can operate during sleep and physical activity. Typical motion artifacts have been compensated for within the system algorithms. Circul is designed to measure SpO2 with a high resolution of 0.1% and sampling frequency of one sample per second with an averaging time of 1s. There is a built-in 3.7v rechargeable lithium-ion battery in the ring that can operate the total system for at least 16 hours. The acquired data signal was processed automatically by an algorithm inside the ring. Circul can output measurement data to the analyzing application installed on a smartphone or tablet using Bluetooth. When Circul is connected to the smart device, the data could be downloaded from the instrument’s built-in memory to the smart device to analyze and display data graphically and generate a report.
 |
Figure 1 Circul and its working principle. (A) Circul and the accessory charger. (B) An example of Circul ring which uses the reflective SpO2 measuring method with embedded red and infra-red (IR) PPG. (C) Schematic diagram of the oxygen desaturation events detection and ODI calculation algorithm in the Circul. |
The schematic diagram of oxygen desaturation events detection and ODI calculation by Circul is shown in Figure 1C. Mean oxygen saturation (MSpO2), cumulative time at SpO2<90% (CT90), and cumulative percentage of sleep time spent with SpO2<90% (CT90/TST) were derived from an automated algorithm of the Circul oximetry. An example of the Circul’s reflective SpO2 signal, traditional tPPG SpO2 signal versus PSG sum channel, epoch by epoch analysis demonstrating a series of oxygen desaturation events is displayed in Figure 2.
 |
Figure 2 An example of a comparison of the nocturnal oxygen saturation signal of Circul, Pulsox 300i, and the polysomnographic (PSG) sum signal, demonstrating a series of hypoxia events in a subject with severe OSA. The amplitude of all signals has been normalized. |
Before routine in-laboratory PSG sleep testing, the sleep technician helped the subjects apply the Circul onto the index finger, middle finger or third finger (Figure 1B). The sleep technician chose the appropriate ring size and finger for each participant to optimize oximetry signal quality. The start and stop of recording of ring oximetry monitoring were defined as the same as lights off and lights on time during PSG testing. All the data from Circul testing and the PSG study were conducted simultaneously.
Pulsox 300i: Pulse Oximetry Using a Finger Probe
The Pulsox 300i (Konica Minolta, Inc., Osaka, Japan) obtained oxygen saturation (SpO2) and pulse rate information using a finger probe using the transmissive PPG technique. The Pulsox 300i can collect SpO2 data continuously, extract oxygen desaturation events, and calculate ODI. The overnight Pulsox SpO2 data was downloaded the next morning via a USB connection to DS-5 data analysis software, and the oxygenation parameters (MSpO2, ODI, CT90, CT90/TST) were generated automatically by software. All data were processed and collected by a technician blinded to the clinical data for the PSG study and the Circul study.
Polysomnography
Trained sleep technicians performed polysomnography (PSG) according to the recommendations of the American Academy of Sleep Medicine (AASM).12,13 All physiologic data were collected and stored using the Alice 6 digital PSG system (Philips Respironics, Inc, Murrysville, Pennsylvania, USA). Channels recorded included: electroencephalogram (F3M2, F4M1, C3M2, C4M1, O1M2, and O2M1), electrooculogram, bilateral anterior tibialis electromyograms, chin muscle electromyogram, oronasal thermistor, nasal pressure, rib cage, and abdominal movement, electrocardiogram, snoring, body position, and heart rate and oxygen saturation by finger-worn pulse oximetry. Using the AASM scoring criteria,13 PSG was scored manually with the aid of computer software by an experienced sleep technologist without knowledge of the results of the Circul oximetry. Apneas were scored when there was ≥ 90% reduction in airflow from baseline for at least 10 seconds on the oronasal thermistor signal. Hypopneas were defined by a ≥30% reduction in a respiratory signal for at least 10 seconds associated with a ≥3% reduction in oxygen saturation or an arousal. AHI on PSG was calculated as the average number of apneas and hypopneas per hour of scored sleep.
In addition, all desaturations of ≥3% from the baseline oxygen saturation were quantified independently for these three recording systems. The 3% desaturations scored for the Circul and Pulsox-300i were scored and extracted the next morning, automatically using analysis software. Data were processed by two technicians who were blinded to the PSG study outcomes. The ODI was calculated as the total number of desaturations divided by the total sleep time or total analyzed time.
Statistical Analysis
Statistical analyses were performed using MedCalc Version 19.0.5 (MedCalc Software, Ostend, Belgium) and MATLAB (MathWorks, Natick, Massachusetts, USA) to assess the clinical accuracy of Circul in determining the presence of OSA. Normally distributed data are presented as mean ± standard deviation (SD), and non-normally distributed data are presented as the median and interquartile range (IQR). A Chi-square analysis was conducted to assess differences in proportion. To test for differences, a paired Student’s t-test was performed for normally distributed data, and a Wilcoxon rank test was used for non-normally distributed data. Correlation coefficients and Bland-Altman plots were done to validate the correlation and agreement between Circul and PSG.14 Sensitivity, specificity, positive predictive value, negative predictive value, and Cohen’s kappa coefficient were calculated at the AHI thresholds of ≥ 5, ≥ 15 and ≥ 30 events/h, respectively. Receiver-operator characteristics (ROC) curves were determined for different PSG diagnostic thresholds to identify the cutoff values of the Circul. Values of P < 0.05 were considered statistically significant for all analyses.
Results
Demographic and Clinical Data
A cohort of 207 Chinese Han subjects was studied with simultaneous PSG and Circul. 145 (70%) were male and had a mean age of 48.2±14.7 years, a mean BMI of 27.6±4.8 kg/m2, a mean total sleep time (TST) of 395.8±58.5 min, and a mean AHI of 28.6±25.2 events/h. A subsample of 141 participants, in addition, was monitored simultaneously with a Pulsox-300i. The characteristics of the sample and sub-sample were summarized in Table S1.
Comparison Between Circul, PSG, and Pulsox 300i
Table 1 summarizes the main parameters observed in PSG and Circul oximetry. A significant difference was observed between PSG-ODI and Ring-ODI (25.3±24.5 events/h vs 22.2±24.5 events/h, P<0.0001). The Circul underestimated overall ODI using the 3% rule, but with good correlation, intraclass correlation coefficient value with 0.884. CT90 and CT90/TST between the two methods were not different. The MSpO2 level of Circul was slightly higher than PSG, but the magnitudes of the differences were relatively small and unlikely to be of clinical significance.
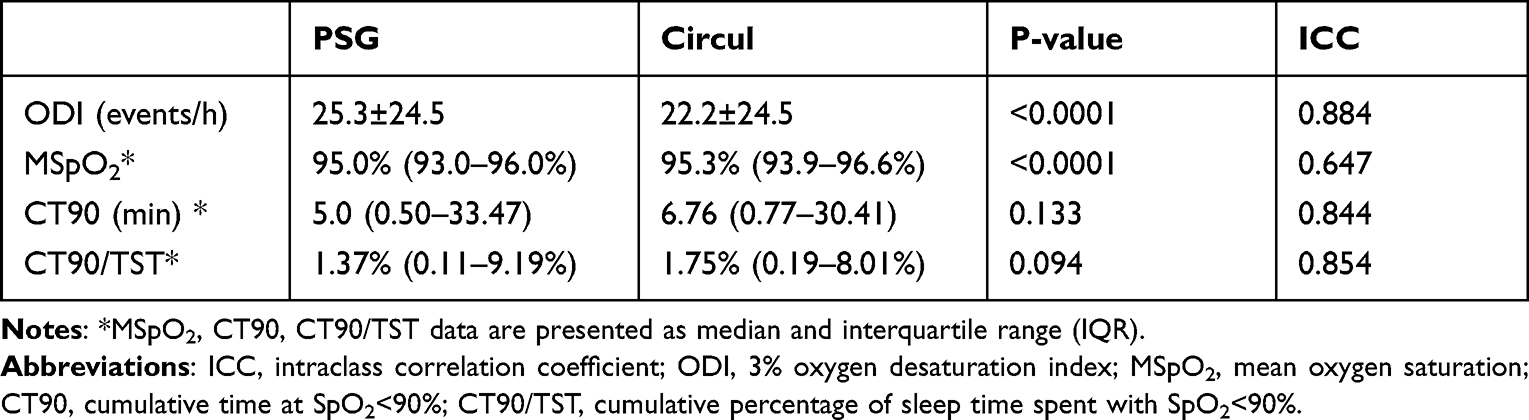 |
Table 1 Comparison of Parameters Observed in PSG and Simultaneous in-Lab Circul Oximetry (n=207) |
Among the total of 207 subjects, the sub-sample of 141 also underwent Pulsox 300i oximetry simultaneously; the performance of the two oximeters (Circul with rPPG and Pulsox with tPPG technique) was investigated (Table S2). The result showed that the rPPG-ODI and tPPG-ODI both had underestimated PSG-ODI with a statistically significant difference, 23.4±25.5 events/h for rPPG-ODI, 23.7±21.5 events/h for tPPG-ODI and 26.6±25.4 events/h for PSG-ODI. But the ODI between the rPPG and tPPG devices were not significantly different, indicating this rPPG method in detecting oxygen desaturation is comparable to transmissive finger probe oximetry.
Correlation and Agreement Between the Circul Oximetry and PSG
The ODI calculated from the Circul device significantly correlated with the PSG-AHI (Pearson r=0.91, p<0.0001), and the scatter plot is shown in Figure 3A. The Bland-Altman analysis demonstrated a mean difference of 6.4, with limits of agreement ranging from −14.8 to 27.5 events/h (Figure 3B). After calculation, 93.7% of the points were within the limits of agreement and the 95% CI. As shown in Figure 3C and D, the Ring-ODI was highly correlated with PSG-ODI (Pearson r=0.89, p<0.001); the Bland-Altman analysis of PSG-ODI and Ring-ODI showed a mean difference of 3.1, limits of agreement ranging from −19.4, 25.5 events/h.
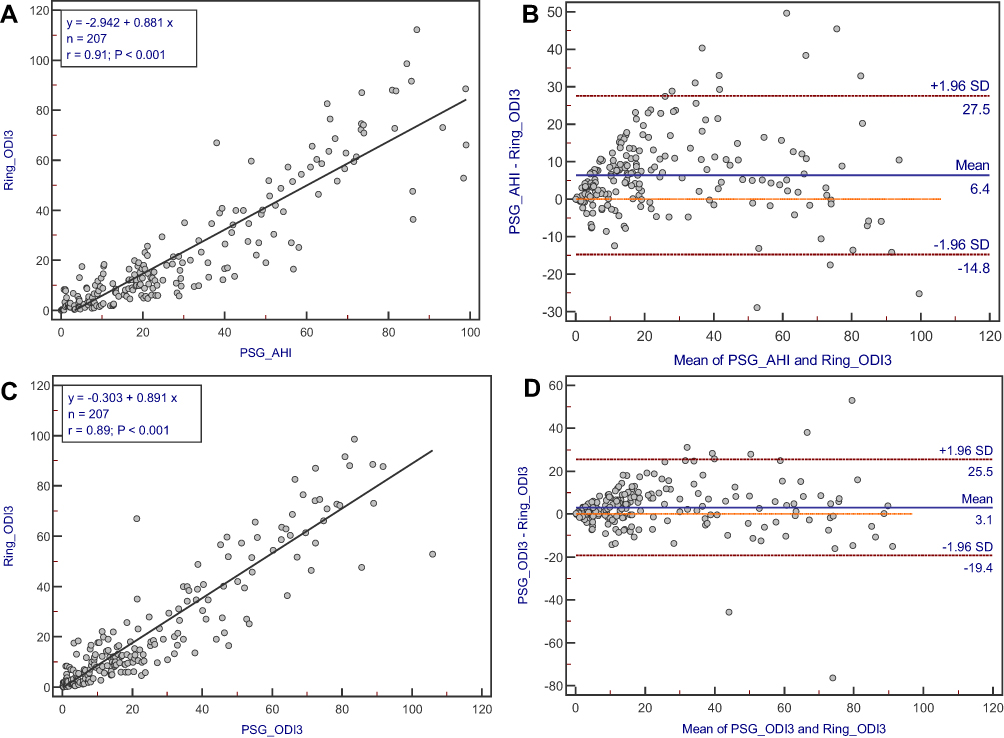 |
Figure 3 Comparison of automatically calculated ODI on Circul and manual-edited PSG-AHI. (A) Scatter plot of AHI on PSG compared to Ring-ODI. (B) Bland-Altman plot of AHI on PSG compared to in-laboratory Ring-ODI. (C) Scatter plot of ODI on PSG compared to Ring-ODI. (D) Bland-Altman plot of ODI on PSG compared to in-laboratory Ring-ODI. |
Diagnostic Efficiency of Circul Oximetry
Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), positive likelihood ratio (LR+), negative likelihood ratio (LR-), accuracy, and Cohen’s kappa coefficient for the Ring-ODI for different AHI thresholds were shown in Table 2. For example, when using Ring-ODI ≥ 5 events/h to identify OSA, the Circul oximetry had 87% sensitivity, 83% specificity, 5.09 LR+, 0.15 LR-, and 86% accuracy. Using Ring-ODI ≥ 15 events/h to recognize moderate-severe OSA, we found a specificity of 96%, sensitivity of 66%, and 76% accuracy. Using Ring-ODI ≥ 30 events/h to diagnose severe OSA, the Circul oximetry had 74% sensitivity, 100% specificity, and 91% accuracy. The kappa coefficient of agreement for AHI≥ 5, ≥ 15, and ≥ 30 events/h were 0.574, 0.544, and 0.784, respectively.
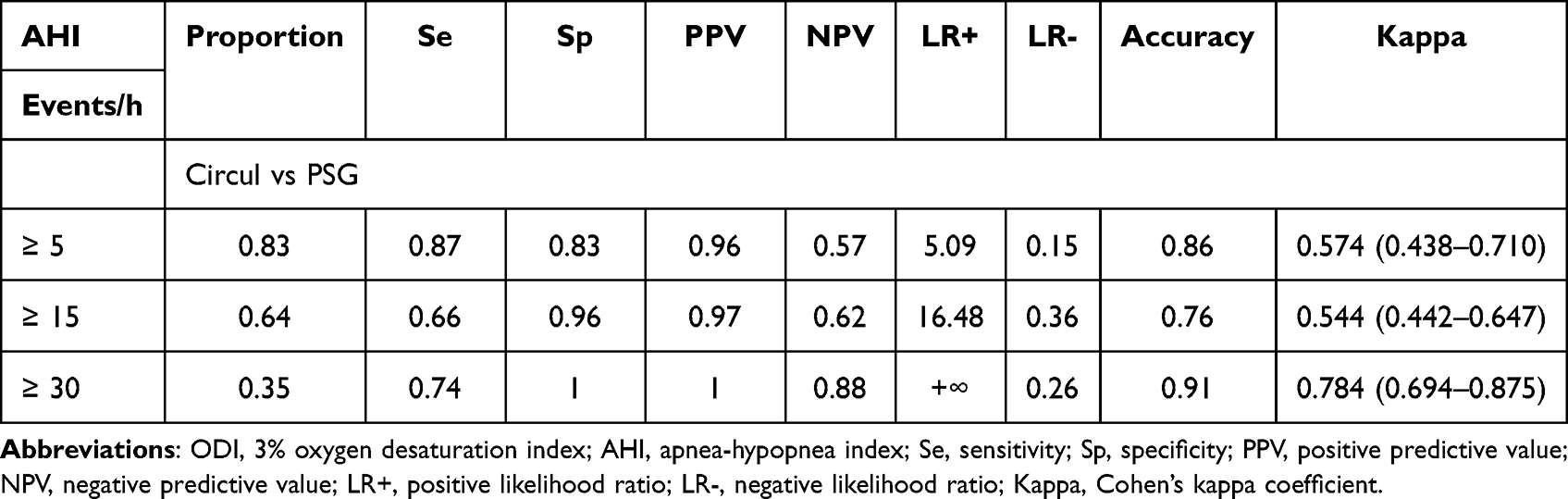 |
Table 2 Diagnostic Comparison of the ODI Derived from Circul with PSG-AHI |
ROC analysis was used to assess the sensitivity and specificity of Circul oximetry in different thresholds of AHI (Figure 4). Using a threshold of AHI ≥5 events/, when the optimal diagnostic cutoff value from Ring-ODI was 5 events/h, with 87.2% sensitivity, 82.8% specificity, 96.2% PPV, 58% NPV, and 0.929 area under the curve (AUC). When the cutoff value of Ring-ODI was lowered to ≥3.2 events/h, Circul oximetry had 91.2% sensitivity and 74.3% specificity to identify OSA-negative or OSA-positive. With a threshold of AHI ≥30 events/h, and a 21.9 cutoff value of Ring-ODI, the diagnostic efficiency improved with 84.7% sensitivity, 97.8% specificity, 95.3% PPV, 92.3% NPV and 0.973 AUC.
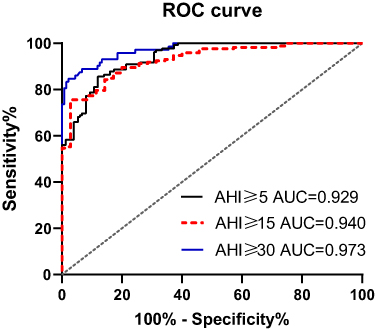 |
Figure 4 ROC curve for the Circul calculated ODI versus the PSG AHI. The three curves refer to a diagnostic threshold of the expert annotated of AHI ≥5; AHI≥15 and AHI≥30 events/h. |
The classification of subjects by referenced PSG against the classification of cases by Circul was shown in Figure 5. The data demonstrate that among 207 participants, 158 (76.3%) subjects in this study can be accurately classed by Circul using binary classification as AHI<15 or AHI ≥15. Considerable underestimation of OSA severity by Circul was found, forty-six subjects of 127 (34.8%) in the group of AHI≥15 events/h were scored as ODI <15 events/h by Circul testing. 3 (4.0%) subjects with AHI<15 were overestimated by Circul as ODI >15 events/h.
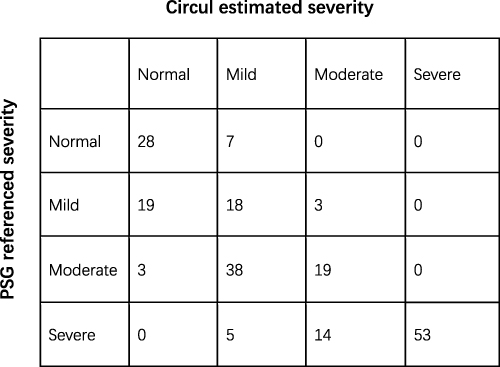 |
Figure 5 The error matrix of OSA severity classes obtained from referenced PSG and Circul using the canonical threshold (AHI<5; AHI ≥5; AHI≥15 and AHI≥30 events/h). |
Discussion
Portable oximetry-based monitors are widely used for assessment and management of OSA. However, ring pulse oximetry with rPPG is a relatively new technology which still needs validation. This pilot study validated the accuracy of Circul compared with simultaneous PSG recording in a Chinese clinic-based sample. The results demonstrated that the performance of the Circul system is capable of providing a reliable detection of OSA on Han Chinese. A close correlation and agreement were found between ODI calculated from Circul oximetry and manual-scored AHI, with Pearson r=0.91, limits of agreement of −14.8 to 27.5 events/h. The Circul system screens OSA with high sensitivity and specificity. When using Ring-ODI ≥ 5 events/h to identify OSA, Circul oximetry can reach 87% sensitivity, 83% specificity, 5.09 positive likelihood ratio (LR+) and 86% accuracy; and using Ring-ODI ≥ 15 events/h to screen moderate-severe OSA, we found the specificity can reach 96%.
The main blood oxygen parameters comparison showed that the Circul correlated with PSG oximetry with ICC 0.884 in ODI. A significant difference was observed between PSG-ODI and Ring-ODI (25.3±24.5 events/h vs 22.2±24.5 events/h, P<0.0001), Circul underestimated ODI as −3.2 events/h in mean difference between Ring-ODI and PSG-ODI. Our study compared rPPG and tPPG, both located on the finger in the detection of oxygen desaturation; Ring-ODI was not statistically different than Pulsox-ODI (23.4±25.5 vs 23.7±21.5), showing this rPPG based oximetry is comparable to traditional finger-probe oximetry (Table S2). Schallom et al15 compared forehead rPPG oximetry and two finger-probe oximeters with tPPG technique, they found over a simultaneous 24-hour measurement in critically ill participants who were at risk of peripheral hypoperfusion, rPPG measurement had a superior correlation and agreement with SaO2 obtained by atrial blood gas analysis. Pertzov et al16 also found significant delay in the detection of desaturation between finger tPPG and earlobe rPPG oximetry during fiberoptic bronchoscopy, showing a centrally located rPPG was more accurate and allows earlier identification of desaturation. These studies displayed an improvement of rPPG technique.
The positive correlation and close agreement of rPPG-estimated respiratory event index (REI) and PSG-derived AHI were also found in other portable oximetry-based monitors,17–19 indicating the reliability of wearable PPG sensors in respiratory event detection. Belun Ring study17 and NightOwl study19 using REI to estimate PSG-AHI, the bias of REI between PSG-AHI is smaller than Circul oximetry, but the positive correlation is inferior to Circul oximetry. Circul oximetry, other rPPG-based oximetry17,19,20 and tPPG-based oximetry18,21 systems were reported to underestimate PSG-AHI. Respiratory event induced oxygen desaturation is determined by the duration of apnea/hypopnea, type of respiratory event, functional residual capacity and basic SaO2 level.22,23 First, apnea could be scored by airflow signals (cessation of breath for 10 secs or more) without oxygen desaturation in PSG. This is important in younger population with no significant comorbidities, and those with low BMI, as they may have a higher incidence of apneas without oxygen desaturations. Decreased airflow in short duration may not have more than 3% oxygen desaturation, the lack of electroencephalogram signals on portable oximetry prevents detection of arousals, resulting in hypopneas with arousals but not desaturations were also missed by oximetry, so that ODI underestimated the AHI as well. Second, AHI could be underestimated because artifacts and noise would affect the signal quality of PPG, which might be incorrectly discarded by automatic algorithms, so that potential respiratory events coupled with movements were missed by a portable PPG-based device, as Massie et al and Papini et al reported.19,20 Thus, Circul could miss oxygen desaturation events and underestimate ODI in this situation.
The utility of Circul in detection for OSA was further illustrated by the ROC, with an area under the curve of 0.929. Using the threshold of Ring-ODI ≥5 events/h, Circul displayed a sensitivity of 87%, a specificity of 83% in the diagnosis of OSA, when using the threshold of Ring-ODI ≥30 events/h, the specificity can reach 100%, and the sensitivity lowered to 74%. Relative to other PPG-based devices, Circul oximetry performed well overall (Table 3): Belun Ring (95% sensitivity, 29% specificity, AUC 0.934 compared with PSG),17 Morpheus Ox (80% sensitivity, 86% specificity, AUC 0.909 with PSG),18 wrist-worn rPPG (72% sensitivity, 71% specificity, AUC of 0.8).20 With PAT-devices, as reported by Ayas et al, when a threshold of AHI≥10 events/h was used, Watch-PAT can reach a sensitivity of 82.6%, and a specificity of 71.4%.21 Using a threshold of in-lab AHI ≥5 events/h, the Circul had 87% sensitivity, 83% specificity, 5.09 positive likelihood ratio (LR+), and 86% accuracy, and 0.929 area under the curve (AUC), which meet the criteria of AASM-guidelines for validation of Out-of-Center devices recommendation.24 The overall specificity of Circul oximetry is good and the underestimation of AHI with Circul caused the relative lower sensitivity, however, when decreased the cutoff value as Ring-ODI ≥3.2 events/h, the Circul oximetry identified OSA with 91.2% sensitivity and 74.3% specificity using the threshold of AHI≥ 5 events/h, this may complement the utility of the Circul oximetry in clinical settings to identify OSA-negative or OSA-positive. The Circul oximetry recognized moderate-severe OSA with 96% specificity and 66% sensitivity at the cutoff of 15 events/h; thus, a positive Circul result is highly suggestive of high-risk OSA. This good specificity of Circul oximetry allows accurate identification of moderate-to-severe OSA, helping to stratify high-risk patients and thus help allocate medical resources such as CPAP intervention. The main advantage of Circul oximetry is that it is more comfortable, convenient, and easy to wear, which requires little training to use properly.
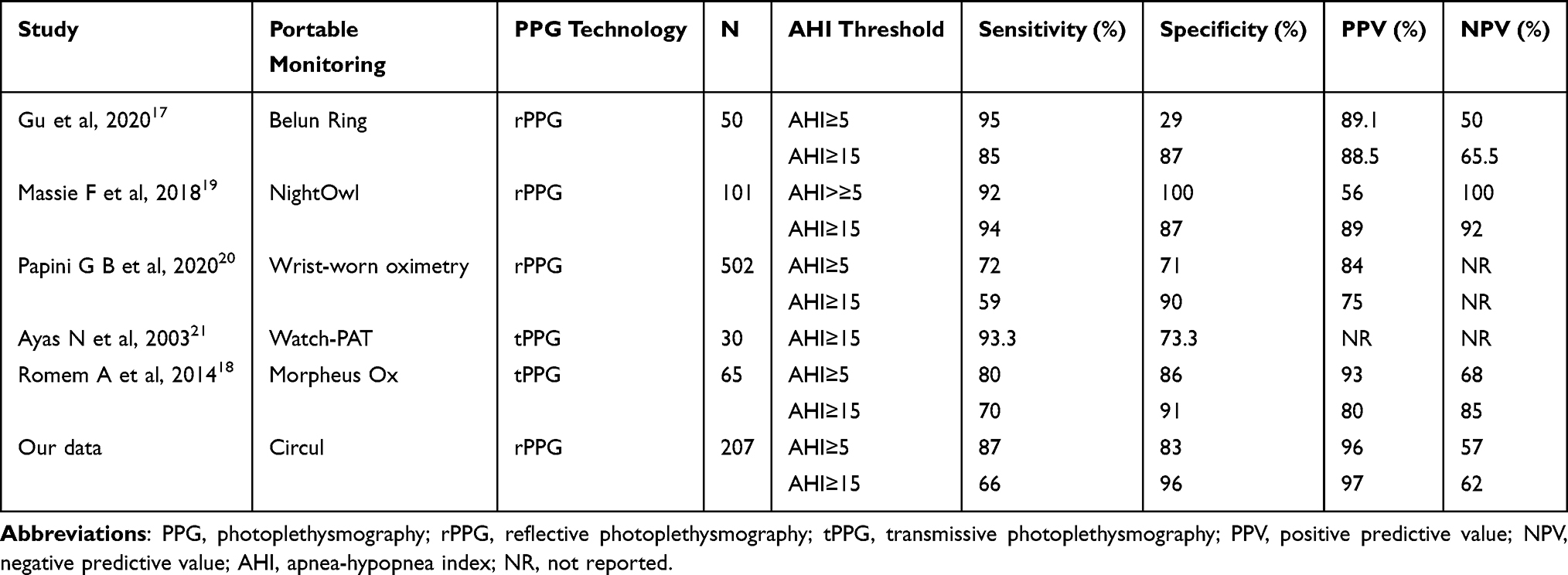 |
Table 3 The Performance of Reported PPG Based Oximetry for Sleep Apnea Testing in Detecting Suspected OSA |
This study is a large cohort study in patients suspected of having OSA. However, it has several limitations. Firstly, the study population is recruited from a sleep disorder clinic, and many who were referred were suspected of having OSA. So the clinical application of this system in a community-based population needs to be evaluated further. Secondly, this study excluded patients with cardiopulmonary disease which may have a potential impact, such as those with chronic obstructive pulmonary disease, chronic heart failure, obesity hypoventilation syndrome, or those on supplemental oxygen. Thirdly, this study focused on Chinese Han adults with relatively lower BMI and lighter skin pigmentation, and the generalization of the findings from the current report to other people with greater BMI or dark skin pigmentation remain to be studied. Also, the measurement accuracy of Circul in children is unclear; further testing is needed to assess its utility in children.
Conclusion
This pilot study evaluated Circul oximetry in detecting obstructive sleep apnea in the Chinese Han population with suspected OSA. Circul ring pulse oximetry can detect OSA with reasonable reliability compared with simultaneous PSG. The Circul system is a reliable and comfortable choice for OSA assessment and complementary for PSG with less interruption of sleep. Future studies should focus on the obese and the subjects with cardiopulmonary comorbidities, its HSAT utility for OSA is also needed.
Abbreviations
AASM, American Academy of Sleep Medicine; AHI, apnea-hypopnea index; AUC, area under the curve; BMI, body mass index; CI, confidence interval; CPAP, continuous positive airway pressure; HSAT, home sleep apnea testing; ICC, intraclass correlation coefficient; IQR, interquartile range; LR+, positive likelihood ratio; LR-, negative likelihood ratio; MSpO2, mean oxygen saturation; NPV, negative predictive value; OCST, out-of-center devices for sleep apnea testing; ODI, oxygen desaturation index; OSA, obstructive sleep apnea; OSAHS, obstructive sleep apnea hypopnea syndrome; PM, portable monitor; PPV, positive predictive value; PSG, polysomnogram; RDI, respiratory disturbance index; REI, respiratory event index; ROC, receiver-operator curve; PPG, photoplethysmography; SD, standard deviation; CT90, cumulative time at SpO2<90%; CT90/TST, cumulative percentage of sleep time spent with SpO2<90%; TST, total sleep time.
Acknowledgments
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper was supported by Research and Development Fund of Peking University People's Hospital (PTU2021-01).
Disclosure
Dr Thomas Penzel reports Research grants by Cidelec, Novartis, Löwenstein Medical. Consultation fees by Bayer Healthcare, Cerebra, National Sleep Foundation. Speaker fee and travel support by Jazz Pharma, Löwenstein Medical, Neuwirth Medical, Somnico. Owns shares from Advanced Sleep Research, The Siestagroup GmbH, Nukute. Dr Meir Kryger reports On Scientific advisory board for Bodimetrics, Wesper and Dormotech, outside the submitted work. All of the authors have indicated no financial conflicts of interest. Megahealth Medical, Inc. provided the Circul oximeter devices and the dedicated software, had no other involvement in the study.
References
1. Newman AB, Nieto FJ, Guidry U, et al. The relationship of sleep disordered breathing to cardiovascular disease risk factors: the sleep heart health study. Am J Epidemiol. 2001;54:50–59. doi:10.1093/aje/154.1.50
2. Redline S, Yenokyan G, Gottlieb DJ, et al. Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Am J Resp Crit Care. 2010;182:269–277. doi:10.1164/rccm.200911-1746OC
3. Teran-Santos J, Jimenez-Gomez A, Cordero-Guevara J. The association between sleep apnea and the risk of traffic accidents. Cooperative Group Burgos-Santander. N Engl J Med. 1999;340:847–851. doi:10.1056/NEJM199903183401104
4. Punjabi NM, Caffo BS, Goodwin JL, et al. Sleep-disordered breathing and mortality: a prospective cohort study. PLoS Med. 2009;6(8):e1000132. doi:10.1371/journal.pmed.1000132
5. Benjafield A, Ayas N, Eastwood P, et al. Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis. Lancet Resp Med. 2019;7(8):687–698. doi:10.1016/S2213-2600(19)30198-5
6. Hang LW, Wang HL, Chen JH, et al. Validation of overnight oximetry to diagnose patients with moderate to severe obstructive sleep apnea. BMC Pulm Med. 2015;15:24. doi:10.1186/s12890-015-0017-z
7. Hornero R, Kheirandish-Gozal L, Gutiérrez-Tobal GC, et al. Nocturnal oximetry–based evaluation of habitually snoring children. Am J Respir Crit Care Med. 2017;196(12):1591–1598. doi:10.1164/rccm.201705-0930OC
8. Chung F, Liao P, Elsaid H, et al. Oxygen desaturation index from nocturnal oximetry: a sensitive and specific tool to detect sleep-disordered breathing in surgical patients. Anesth Analg. 2012;114(5):993–1000. doi:10.1213/ANE.0b013e318248f4f5
9. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(3):479–504. doi:10.5664/jcsm.6506
10. Rofail LM, Wong KK, Unger G, et al. Comparison between a single-channel nasal airflow device and oximetry for the diagnosis of obstructive sleep apnea. Sleep. 2010;33(8):1106–1114. doi:10.1093/sleep/33.8.1106
11. Wiltshire N, Kendrick AH, Catterall JR. Home oximetry studies for diagnosis of sleep apnea/hypopnea syndrome: limitation of memory storage capabilities. Chest. 2001;120(2):384–389. doi:10.1378/chest.120.2.384
12. Kushida CA, Littner MR, Morgenthaler T, et al. Practice parameters for indications for polysomnography and related procedures: an update for 2005. Sleep. 2005;28(4):499–521. doi:10.1093/sleep/28.4.499
13. Berry RB, Brooks R, Gamaldo CE, et al. For the American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. Version 2.6. Darien, IL: American Academy of Sleep Medicine; 2020.
14. Flemons WW, Littner MR. Measuring agreement between diagnostic devices. Chest. 2003;124(4):1535–1542. doi:10.1378/chest.124.4.1535
15. Schallom L, Sona C, McSweeney M, et al. Comparison of forehead and digit oximetry in surgical/trauma patients at risk for decreased peripheral perfusion. Heart Lung. 2007;36(3):188–194. doi:10.1016/j.hrtlng.2006.07.007
16. Pertzov B, Brachfeld E, Unterman A, et al. Significant delay in the detection of desaturation between finger transmittance and earlobe reflectance oximetry probes during fiberoptic bronchoscopy: analysis of 104 cases. Lung. 2019;197(1):67–72. doi:10.1007/s00408-018-0180-0
17. Gu W, Leung L, Kwok KC, et al. Belun ring platform: a novel home sleep apnea testing system for assessment of obstructive sleep apnea. J Clin Sleep Med. 2020;16(9):1611–1617. doi:10.5664/jcsm.8592
18. Romem A, Romem A, Koldobskiy D, et al. Diagnosis of obstructive sleep apnea using pulse oximeter derived photoplethysmographic signals. J Clin Sleep Med. 2014;10(3):285–290. doi:10.5664/jcsm.3530
19. Massie F, Almeida DMD, Dreesen P, et al. An evaluation of the nightowl home sleep apnea testing system. J Clin Sleep Med. 2018;14(10):1791–1796. doi:10.5664/jcsm.7398
20. Papini GB, Fonseca P, Gilst M, et al. Wearable monitoring of sleep-disordered breathing: estimation of the apnea–hypopnea index using wrist-worn reflective photoplethysmography. Sci Rep. 2020;10(1):13512. doi:10.1038/s41598-020-69935-7
21. Ayas NT, Pittman S, Macdonald M, et al. Assessment of a wrist-worn device in the detection of obstructive sleep apnea. Sleep Med. 2003;4(5):435–442. doi:10.1016/S1389-9457(03)00111-4
22. Yılmaz Durmaz D, Güneş A. Which is more important: the number or duration of respiratory events to determine the severity of obstructive sleep apnea? Aging Male. 2020;23(2):119–124. doi:10.1080/13685538.2019.1630062
23. Kulkas A, Duce B, Leppänen T, et al. Severity of desaturation events differs between hypopnea and obstructive apnea events and is modulated by their duration in obstructive sleep apnea. Sleep Breath. 2017;21(4):829–835. doi:10.1007/s11325-017-1513-6
24. Collop NA, Tracy SL, Kapur V, et al. Obstructive sleep apnea devices for out-of-center (OOC) testing: technology evaluation. J Clin Sleep Med. 2011;7(5):531–548. doi:10.5664/JCSM.1328
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
New Metrics from Polysomnography: Precision Medicine for OSA Interventions
Guo J, Xiao Y
Nature and Science of Sleep 2023, 15:69-77
Published Date: 9 March 2023
Association Between Sleep Efficiency and Hypertension in Chinese Obstructive Sleep Apnea Patients
Xia N, Wang H, Chen Y, Fan XJ, Nie XH
Nature and Science of Sleep 2023, 15:79-88
Published Date: 10 March 2023
Waiting for in-Lab Polysomnography May Unnecessarily Prolong Treatment Start in Patients with Moderate or Severe OSA at Home Sleep Apnea Testing
Pordzik J, Seifen C, Ludwig K, Ruckes C, Huppertz T, Matthias C, Gouveris H
Nature and Science of Sleep 2024, 16:1881-1889
Published Date: 5 December 2024
Association Between Nocturnal Hypoxemia Parameters and Coronary Microvascular Dysfunction: A Cross-Sectional Study
Feng L, Zhao X, Song J, Yang S, Xiang J, Zhang M, Tu C, Song X
Nature and Science of Sleep 2024, 16:2279-2288
Published Date: 28 December 2024
Association Between Fractional Exhaled Nitric Oxide (FeNO) and Cognitive Function in Patients with Obstructive Sleep Apnea
Zhu Q, Huang L, Zhu L, Zhang X, Ji H, Niu D, Ji W, Ma Q, Chen R, Shi H, Wang Y, Xu L
Nature and Science of Sleep 2025, 17:1603-1614
Published Date: 12 July 2025