Back to Journals » Clinical Ophthalmology » Volume 20
Comparison of Peripapillary and Submacular Choroidal Changes After Trabeculectomy and Phaco-Trabeculectomy in Open-Angle Glaucoma
Authors Eraydin B, Cakmak-Cengiz E ![]() , Arıtürk N
, Arıtürk N
Received 16 February 2026
Accepted for publication 1 June 2026
Published 18 June 2026 Volume 2026:20 603832
DOI https://doi.org/10.2147/OPTH.S603832
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sotiria Palioura
Bilge Eraydin,1 Esen Cakmak-Cengiz,2 Nurşen Arıtürk1
1Department of Ophthalmology, Ondokuz Mayıs University Faculty of Medicine, Samsun, Turkey; 2Department of Ophthalmology, Unye State Hospital, Ordu, Turkey
Correspondence: Esen Cakmak-Cengiz, Department of Ophthalmology, Unye State Hospital, Ordu, Turkey, Email [email protected]
Purpose: Choroidal vascular and structural alterations are increasingly recognized as relevant to intraocular pressure (IOP) regulation and glaucoma pathophysiology. Surgical IOP reduction induces hemodynamic and biomechanical changes that may affect choroidal thickness and perfusion, particularly in the peripapillary and submacular regions. Although trabeculectomy is known to cause early postoperative choroidal expansion, the additional impact of concomitant phacoemulsification remains unclear. We compared early regional choroidal responses after trabeculectomy (Trab) alone and phaco-trabeculectomy (Phaco-Trab) in eyes with open-angle glaucoma (OAG).
Patients and Methods: This retrospective study included patients with OAG who underwent Trab or combined Phaco-Trab after failure of maximal medical therapy. Preoperative and 1-month postoperative assessments included best-corrected visual acuity, Goldmann applanation tonometry, slit-lamp and fundus examinations, and enhanced depth imaging optical coherence tomography. Submacular and peripapillary choroidal parameters, including choroidal thickness (CT), luminal area (LA), stromal area (SA), total choroidal area (TCA), and choroidal vascularity index (CVI), were quantified using ImageJ software. Eyes with previous intraocular surgery, systemic vascular disease, media opacity, or postoperative complications were excluded. Intra- and intergroup comparisons were performed.
Results: Fifty-five eyes were analyzed (30 Trab, 25 Phaco-Trab). Both groups showed significant postoperative IOP reduction (p< 0.001). In the Trab group, submacular CT decreased significantly, whereas LA and TCA increased; CVI remained unchanged. In contrast, the Phaco-Trab group demonstrated significant increases in submacular CT, LA, TCA, and CVI at 1 month. In the peripapillary region, the Trab group showed increased temporal CVI, whereas the Phaco-Trab group demonstrated increased temporal LA. No significant correlation was found between IOP reduction and changes in choroidal parameters.
Conclusion: Early postoperative choroidal responses differed between procedures. Phaco-Trab induced greater structural and vascular choroidal changes, likely due to the combined effects of IOP reduction and inflammation associated with cataract surgery. These findings highlight the choroid’s dynamic role in postoperative recovery and warrant long-term investigation.
Keywords: glaucoma, trabeculectomy, phaco-trabeculectomy, choroid
Introduction
Cataracts and glaucoma are the leading causes of blindness worldwide and frequently coexist in the aging population. Epidemiological studies estimate that 10% of elderly individuals with cataracts have elevated intraocular pressure (IOP).1,2 In cases where IOP cannot be adequately controlled, and visual field loss progresses despite maximal medical therapy, surgical intervention becomes necessary. However, selecting the optimal surgical strategy in patients with coexisting cataract and glaucoma remains challenging, as the management of one condition may influence the course of the other. Trabeculectomy alone has been associated with accelerated cataract progression, with approximately 30% of patients requiring cataract surgery within the first postoperative year.3,4 Consequently, combined phaco-trabeculectomy has emerged as a practical approach in appropriately selected patients, allowing simultaneous visual rehabilitation and IOP control.
Beyond IOP reduction, increasing evidence highlights the role of vascular factors in glaucoma pathophysiology. Imaging-based studies have demonstrated reduced retinal, choroidal, and optic nerve head perfusion in glaucomatous eyes compared with healthy controls.5–7 Moreover, structural and functional changes can occur in the retinal and choroidal vasculature in response to decreases in IOP during surgery and the postoperative period. The choroid plays a key role in supplying blood to the prelaminar, laminar, and post-laminar regions of the optic nerve head, as well as to the outer retina, making it a key structure in both the development and progression of glaucomatous damage.8
Enhanced depth imaging optical coherence tomography (EDI-OCT) improves visualization of the choroid–scleral interface, facilitating quantitative assessment of submacular choroidal thickness (SMCT). However, because choroidal thickness may be influenced by physiological factors such as age, axial length, and diurnal variation, the choroidal vascularity index (CVI), a recently introduced parameter derived from image binarization, has emerged as a more stable marker of choroidal vascular status by separately quantifying luminal area (LA) and stromal area (SA).9,10
Although previous studies have reported postoperative increases in choroidal thickness following trabeculectomy, comparative data evaluating both structural and vascular choroidal changes between trabeculectomy (Trab) and phaco-trabeculectomy (Phaco-Trab) remain limited. Moreover, most studies have focused on either the macular or peripapillary region alone, and comprehensive regional analyses are scarce.
Therefore, the primary aim of this study was to compare early postoperative changes in both peripapillary and submacular choroidal parameters, including SMCT, CVI, LA, and SA, in patients with open-angle glaucoma undergoing Trab versus Phaco-Trab.11 The novelty of this study lies in its simultaneous evaluation of regional (peripapillary and submacular) structural and vascular choroidal changes using EDI-OCT–based quantitative biomarkers, providing a more comprehensive understanding of early postoperative choroidal remodeling following different surgical approaches.
Materials and Methods
This retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and approved by the Ethics Committee of the Ondokuz Mayıs University Hospital (Decision No: B.30.2.ODM.0.20.08/102). A detailed review of the medical records of patients followed at the institution’s Glaucoma Unit from January 2023 to May 2024 was performed. Patients diagnosed with open-angle glaucoma who required surgical intervention despite medical treatment were included in the study.
Indication for surgery was determined by failure to achieve target IOP despite maximally tolerated topical therapy or by objective progression demonstrated on OCT, visual field testing, and optic disc examinations. Progression was assessed using structural and functional indicators, including elevated IOP during long-term follow-up, diurnal pressure fluctuations, neuroretinal rim thinning, acquired optic cup formation, scotoma enlargement, and decreased visual acuity. Phaco-Trab was performed in patients with visually significant cataract and uncontrolled intraocular pressure, whereas isolated Trab was performed in those without cataract.
Trabeculectomy was performed using a standard fornix-based conjunctival flap with a partial-thickness scleral flap, followed by trabecular block excision and peripheral iridectomy. Intraoperative mitomycin C was applied. The scleral flap and conjunctiva were sutured with adjustable sutures to regulate aqueous outflow. In the Phaco-Trab group, after creation of the scleral flap, phacoemulsification with intraocular lens implantation was performed through the trabecular block site, followed by completion of trabeculectomy using the same filtration technique.12
The study included patients aged 18 years or older with open-angle glaucoma, signs of glaucomatous optic neuropathy, and high-quality preoperative and postoperative EDI-OCT images. To minimize the effect of diurnal variation, all EDI-OCT measurements for choroidal assessment were performed within the same time interval (between 9:00 AM and 12:00 PM) for all patients. Patients were excluded if they had a history of intraocular surgery; refractive error greater than ±6 diopters; ocular pathology other than glaucoma or cataracts; systemic vascular disease that could affect ocular perfusion; systemic medications that alter vascular tone; or media opacities that could compromise image quality. Patients who developed postoperative complications were also excluded.
Best-corrected visual acuity, IOP measured with a Goldmann applanation tonometer (AT900; Haag-Streit, Köniz, Switzerland), and findings from biomicroscopic and dilated fundus examinations were recorded for all patients preoperatively and at one month postoperatively. Demographic data (age, gender, glaucoma stage) were also evaluated.
For analysis of choroidal structures, OCT scans were performed with Spectralis (Heidelberg Engineering, Heidelberg, Germany) in enhanced depth imaging (EDI) mode. For submacular assessment, 1500 µm reference lines were placed from the foveola in nasal and temporal directions, while for peripapillary evaluation, 1000 µm lines were placed from the inner scleral ring in nasal and temporal directions, parallel to the retinal pigment epithelium. Image analysis was performed using ImageJ software (version 1.53, National Institutes of Health, Bethesda, MD, USA) following a previously described binarization protocol.10 Briefly, OCT images were first converted to 8-bit format, and the region of interest (ROI) corresponding to the choroid was manually delineated between the retinal pigment epithelium and the choroid–sclera interface. Subsequently, images were processed using the Niblack auto local thresholding method to differentiate luminal and stromal components. The luminal area was defined as the dark pixels, while the SA corresponded to the light pixels. Total choroidal area was calculated as the sum of LA and SA, and the CVI was defined as the ratio of LA to TCA. Submacular and peripapillary CT, LA, SA, and TCA were measured quantitatively (Figures 1 and 2).
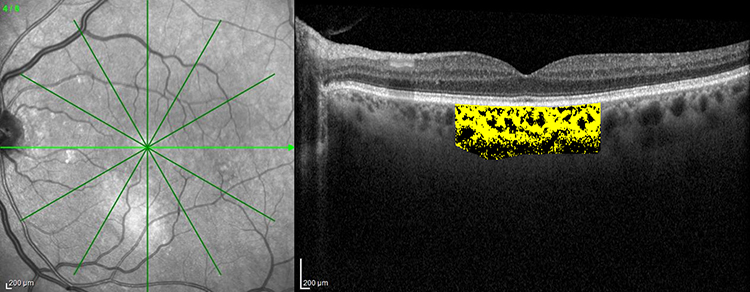 |
Figure 1 Representative enhanced depth imaging optical coherence tomography (EDI-OCT) image demonstrating fovea-centered choroidal analysis and binarization. The yellow highlighted area represents the selected subfoveal choroidal region used for quantitative analysis of luminal area (LA), total choroidal area (TCA), and choroidal vascularity index (CVI). Green radial lines and arrows indicate the scan orientations used for fovea-centered imaging. Abbreviations: EDI, enhanced depth imaging; OCT, optical coherence tomography. |
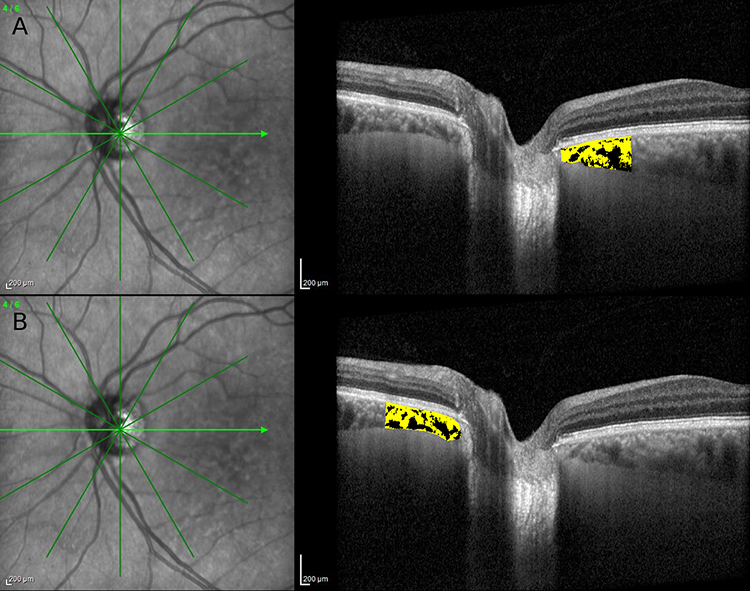 |
Figure 2 Representative enhanced depth imaging optical coherence tomography (EDI-OCT) images of the peripapillary optic disc region demonstrating choroidal structural analysis and binarization used for calculation of choroidal vascularity parameters. Green radial lines and arrows indicate the scan directions used for peripapillary choroidal imaging. The yellow highlighted areas represent the selected peripapillary choroidal regions used for binarization and quantitative analysis of luminal area (LA), total choroidal area (TCA), and choroidal vascularity index (CVI). The upper image (A) shows the temporal peripapillary optic disc scan, whereas the lower image (B) shows the nasal peripapillary optic disc scan. Abbreviations: EDI, enhanced depth imaging; OCT, optical coherence tomography. |
In this study, the early effects of surgery on choroidal structures were comprehensively evaluated by comparing preoperative and first-month postoperative measurements.
Statistical Analysis
All statistical analyses were conducted using SPSS v26.0 (IBM Corp., Armonk, NY, USA). Continuous variables are presented as mean ± standard deviation (SD), and categorical variables as frequencies and percentages. The Shapiro–Wilk test was used to assess normality of continuous variables. Depending on normality, within-group comparisons (preoperative vs 1-month postoperative) were performed using the paired t-test or the Wilcoxon signed-rank test, and between-group comparisons (Trab vs Phaco-Trab) were performed using the independent samples t-test or the Mann–Whitney U-test. Categorical variables (eg, sex distribution) were analyzed using the chi-square test or Fisher’s exact test when expected frequencies were low. Multiple comparisons were adjusted using Hedges’ correction. Statistically significant differences were defined as P < 0.05.
Results
A total of 55 eyes from 55 patients with open-angle glaucoma were enrolled, comprising 30 in the Trab group and 25 in the Phaco-Trab group. The baseline characteristics of the study population are presented in Table 1, and no significant differences were observed between the groups in demographic or clinical parameters. The preoperative mean IOP was 28.68±6.97 mmHg in the Trab group and 25.00±8.73 mmHg in the Phaco-Trab group. At one month postoperatively, the mean IOP was 15.45 ± 3.11 mmHg in the Trab group and 14.33 ± 4.71 mmHg in the Phaco-Trab group, with a statistically significant reduction in IOP at both time points (p<0.001) (Figure 1).
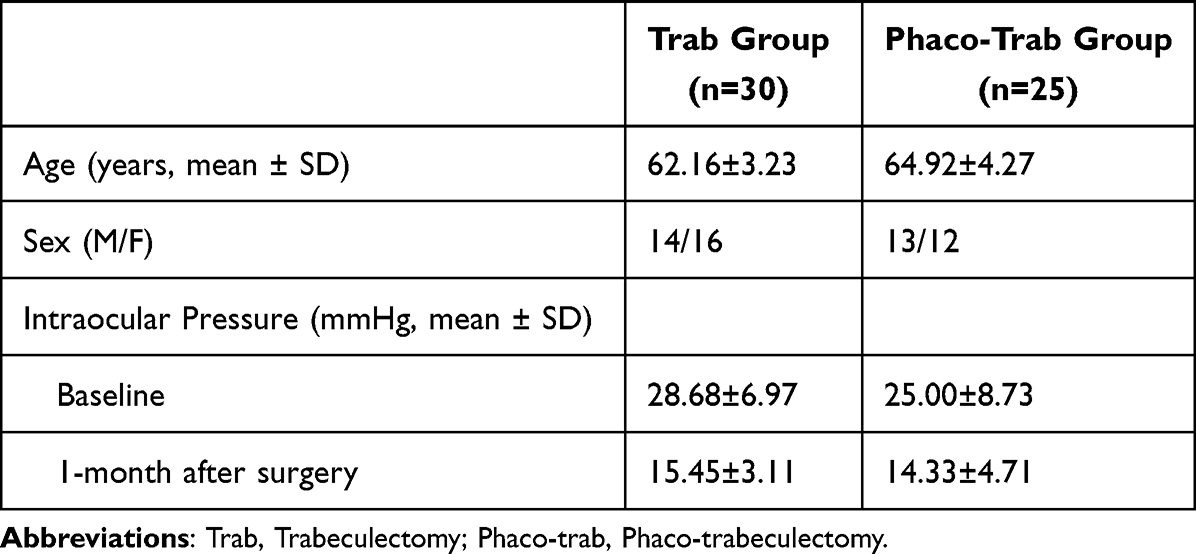 |
Table 1 Demographic Characteristics and Clinical Data of the Patients |
In the Trab group, SMCT 276.65±86.54 µm and 275.57±66.65 µm before and after surgery, respectively (p=0.007) showed a significant decrease, while LA 1.44±0.47 mm2 and 1.47±0.47 mm2 before and after surgery, respectively (p=0.030) and TCA 2.20±0.70 mm2 and 2.34±0.75 mm2 before and after surgery, respectively (p=0.014) showed a statistically significant increase, no statistical difference was found in the comparison of submacular CVI %64.79 ± 3.15 and %65.77 ± 7.50 before and after surgery, respectively (p=0.254).
In the Phaco-Trab group, SMCT increased significantly from 280.44 ± 55.96 µm to 303.77 ± 70.60 µm (P=0.006). Additionally, submacular CVI increased from 60.56% ± 4.15% to 63.83% ± 3.58% (P=0.39), LA increased from 1.49 ± 0.35 mm2 to 1.57 ± 0.33 mm2 (P=0.007), and TCA increased from 2.46 ± 0.50 mm2 to 2.47 ± 0.60 mm2 (P=0.03). In the Phaco-Trab group, the preoperative CVI was 60.56% ± 4.15%, increasing to 63.83% ± 3.58% postoperatively, representing a statistically significant improvement (P = 0.020). LA increased from 1.49 ± 0.35 mm2 preoperatively to 1.57 ± 0.33 mm2 postoperatively (P=0.007), and TCA increased from 2.46 ± 0.50 mm2 preoperatively to 2.47 ± 0.60 mm2 at 1 month postoperatively, which was a statistically significant increase (P=0.037).
Among peripapillary choroidal measurements in the Trab group, only the temporal peripapillary CVI showed a significant increase (%62.33 ± 6.73 and %64.86 ± 6.13 before and after surgery, respectively) (P=0.031). In the Phaco-Trab group, temporal peripapillary LA increased significantly, rising from 0.28 ± 0.07 mm2 to 0.32 ± 0.08 mm2 (P=0.030). However, no significant changes were noted in TCA (0.44 ± 0.10 mm2 to 0.48 ± 0.12 mm2, P=0.011), nasal peripapillary LA (0.28 ± 0.09 mm2 to 0.30 ± 0.08 mm2, P=0.13), or temporal CVI (63.53% ± 4.81% to 66.82% ± 6.21%, P=0.569) (Table 2). As a result, both groups showed a significant decrease in IOP and an increase in submacular LA and TCA levels at 1 month postoperatively. CVI increased significantly in the Phaco-Trab group, whereas no significant change was observed in the Trab group. Submacular CT increased in the Phaco-Trab group but decreased in the Trab group. No correlation was found between IOP measurements and choroidal changes in either group.
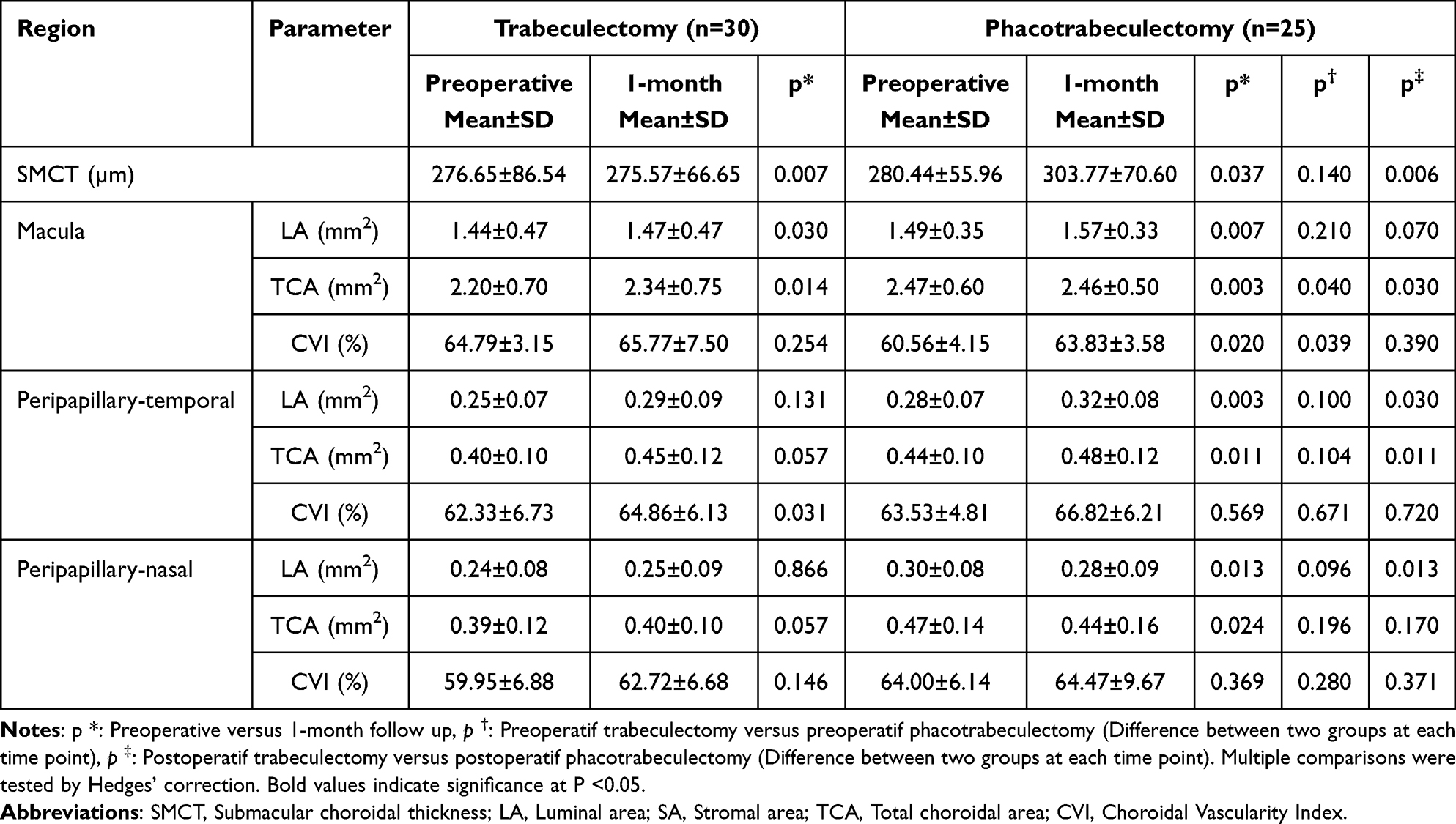 |
Table 2 Comparison of Preoperative and 1-Month Choroidal Parameters in the Submacular and Peripapillary Areas of the Trab and Phaco-Trab Groups |
Discussion
Glaucoma affects not only the retinal circulation but also the choroidal vasculature. Analyzing the structural susceptibility and associated factors of the optic nerve head and macula can provide valuable insights for predicting glaucoma progression. Portmann et al demonstrated that patients with primary open-angle glaucoma (POAG) and ocular hypertension had lower choroidal blood flow than healthy controls, suggesting a potential role for choroidal vascular dysregulation in glaucoma pathophysiology.13
Numerous studies have investigated CT in patients with glaucoma. A meta-analysis of 22 studies found no significant difference in macular or peripapillary CT between eyes with open-angle glaucoma and healthy controls.14 However, some studies have reported that the peripapillary choroid is thinner in eyes with normal-tension glaucoma compared to healthy individuals.15,16 In contrast, other studies have not supported this finding.17,18 Researches have also shown that CT is notably greater in individuals with primary angle-closure glaucoma than in those with primary open-angle glaucoma and healthy eyes. This suggests that increased CT may be a risk factor for angle-closure glaucoma.19–21
CVI distinguishes the LA and SA, providing a more accurate assessment of vascularity. This makes CVI a more sensitive marker than CT. Moghimi et al found that peripapillary CT (excluding the superotemporal, superonasal, and nasal quadrants) was significantly reduced in eyes with PEXG compared with healthy controls, and they reported that peripapillary CT decreased with PEXG severity.22 Although Li et al found a significant decrease in central submacular CT in the PEXG group compared with the control group, they reported a significant decrease only in the nasal inferior quadrant of peripapillary CT.21 In our study, a significant increase in TCA values was detected after surgery in both the Phaco-Trab and Trab groups. Previous studies have shown that CT increases during the first month after IOP-lowering surgery in POAG, and that this change correlates with both decreased IOP and increased ocular perfusion pressure. These studies also suggest that enhanced ocular blood flow following trabeculectomy may contribute to postoperative choroidal expansion.11,23 Consistent with this evidence, our study similarly demonstrated an increase in TCA, accompanied by more pronounced peripapillary and submacular changes in the Phaco-Trab group, likely reflecting the combined effects of IOP reduction and the observed increases in LA and TCA.
The significant increase in TCA and CVI observed in the Phaco-Trab group can be interpreted as choroidal expansion, reflecting not only the decrease in IOP but also the inflammatory response associated with phacoemulsification. Studies demonstrating significant increases in CT in the submacular and nasal regions after phacoemulsification suggest that these changes may reflect short-term hemodynamic and inflammatory effects of surgery.24
Numerous studies have evaluated choroidal structural changes after cataract surgery, but the exact mechanism remains unclear. One theory suggests that postoperative inflammation triggers the release of proinflammatory prostaglandins and cytokines during surgery, which are also implicated in the pathogenesis of macular edema after cataract surgery.25 The outer blood–retinal barrier has been shown to be disrupted as a consequence of post–cataract surgery inflammation. Hence, it can be speculated that an anterior-segment inflammatory response may lead to posterior-segment inflammation.26 Additionally, topical steroids are known to reduce postoperative inflammation and suppress the inflammatory response in the retina.25 In our study, participants were prescribed steroidal anti-inflammatory eye drops postoperatively. Statistical analysis of our study found a statistically significant increase in SFCT at 1 month in the Phaco-Trab group compared to the Trab group. Our study revealed that changes in CVI were not correlated with IOP across groups, suggesting that choroidal changes may be driven by inflammation.
In our study, a significant decrease in SFCT was observed in the first postoperative month in the Trab group. Results regarding the SFCT after Trab are mixed: some studies indicate an increase in CT at long-term follow-up (eg, six months postoperatively), whereas others report a decrease in central CT as early as the second week or first month. The decrease in SFCT and the corresponding increase in temporal peripapillary CVI observed in the Trab group suggest that the choroidal response after trabeculectomy may vary by region. Studies reporting significant changes in CT in the early postoperative period after trabeculectomy have shown that the biomechanical and hemodynamic remodeling accompanying IOP reduction may substantially affect the choroid.27,28
Studies examining peripapillary choroidal changes have reported a significant decrease in thickness in glaucomatous eyes compared to healthy eyes.9,21 In our study, this is supported by the observation of increases in CVI, LA, and SA in the peripapillary temporal choroidal area in the Trab and Phaco-Trab groups when the effect of high IOP was eliminated in the postoperative period. Usui et al measured postoperative peripapillary CT changes in open-angle glaucoma patients and found a significant increase in all four peripapillary quadrants.23 In our study, increases were found in CVI, LA, and SA in both groups. We believe that this situation will support optic nerve nutrition and regression of glaucomatous optic neuropathy, along with IOP reduction.
Park et al compared TCA and CVI in patients with primary open-angle glaucoma with and without microvascular loss detected by OCT-angiography. Although there was no significant difference in TCA, CVI was lower in eyes with microvascular loss, particularly in the temporal quadrant.29 Thinning of the peripapillary choroidal layer is associated with inadequate blood supply to the optic nerve and may result in glaucomatous optic neuropathy; therefore, an increase in peripapillary choroidal blood flow in the postoperative period may protect the optic nerve from further damage.2,30
TCA in Phaco-Trab eyes was significantly higher than in Trab eyes. Additionally, choroidal changes were more frequent in the Phaco-Trab group. Inflammatory responses following cataract surgery may be responsible for the choroidal differences between Phaco-Trab and Trab eyes. It suggests a potential role for structural choroidal changes in the pathogenesis of glaucoma, particularly in the peripapillary region that supplies the optic nerve head. The acute reduction in IOP may induce vascular structural changes in both the peripapillary and central macular regions of the choroid. To our knowledge, this is the first study to examine choroidal changes in Trab and Phaco-Trab eyes. The ultrastructural structure of choroidal changes can be evaluated with ImageJ software, and more sensitive results can be obtained for postoperative changes. The fact that choroidal changes were more common in the Phaco-Trab group supports the role of inflammation caused by cataract surgery.
This study has several limitations. First, choroidal changes after Trab and Phaco-Trab were evaluated only in the early postoperative period; therefore, the long-term persistence and clinical significance of these vascular and structural alterations remain uncertain. Second, choroidal measurements were obtained using manual image analysis, which may introduce observer-dependent variability despite standardized methodology. Third, the relatively small sample size may have limited statistical power and generalizability.
The present findings suggest that although both Trab and Phaco-Trab achieve effective intraocular pressure reduction, they may induce distinct early choroidal structural responses. The greater increases observed in CVI, LA, and CT following Phaco-Trab likely reflect a more pronounced vascular response driven by the combined effects of IOP reduction and postoperative inflammatory processes associated with cataract extraction. These changes may represent an early, adaptive increase in choroidal perfusion and vascular reactivity in the postoperative period.
To our knowledge, few studies have directly compared early postoperative choroidal responses between trabeculectomy and phaco-trabeculectomy using both structural and vascular OCT-derived parameters. From a clinical perspective, this differential response may be relevant for interpreting early postoperative imaging and could inform individualized follow-up strategies, particularly in eyes with advanced glaucoma or limited macular reserve, where vascular dynamics may influence functional outcomes.
Conclusion
In conclusion, phaco-trabeculectomy appears to elicit a more pronounced early choroidal vascular response compared with trabeculectomy alone, despite similar intraocular pressure reduction. This enhanced vascular reactivity may have implications for early postoperative assessment and risk stratification, highlighting the need for longitudinal studies to determine its impact on long-term visual and structural outcomes.
Abbreviations
OAG, open-angle glaucoma; IOP, intraocular pressure; OCT, optical coherence tomography; EDI-OCT, enhanced depth imaging optical coherence tomography; SMCT, submacular choroidal thickness; LA, luminal area; SA, stromal area; TCA, total choroidal area; CVI, choroidal vascularity index; Trab, trabeculectomy; Phaco-Trab, phacotrabeculectomy; BCVA, best-corrected visual acuity.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
All procedures involving human participants were performed in accordance with institutional and national ethical standards and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This retrospective study was approved by the Ethics Committee of Ondokuz Mayıs University Hospital (Decision No: B.30.2.ODM.0.20.08/102).
Informed Consent Statement
All participants gave written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for this article’s research, authorship, and/or publication.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Friedman DS, Wolfs RCW, O’Colmain BJ, et al. Prevalence of open-angle glaucoma among adults in the United States. Arch Ophthalmol. 2004;122(4):532–9. doi:10.1001/archopht.122.4.532
2. Gugleta K, Polunina A, Kochkorov A, et al. Association between risk factors and glaucomatous damage in untreated primary open-angle glaucoma. J Glaucoma. 2013;22(6):501–505. doi:10.1097/IJG.0b013e3182447d9b
3. Rajavi Z, Moezzi-Ghadim H, Kamrava K. The effect of trabeculectomy on cataract formation or progression. J Ophthalmic Vis Res. 2009;4(2):84. PMID: 23198053.
4. Hylton C, Congdon N, Friedman D, et al. Cataract after glaucoma filtration surgery. Am J Ophthalmol. 2003;135(2):231–232. doi:10.1016/s0002-9394(02)01919-0
5. Bengtsson B, Heijl A. Lack of visual field improvement after initiation of intraocular pressure reducing treatment in the early manifest glaucoma trial. Invest Ophthalmol Visual Sci. 2016;57(13):5611–5615. doi:10.1167/iovs.16-19389
6. Leske MC. Ocular perfusion pressure and glaucoma: clinical trial and epidemiologic findings. Curr Opin Ophthalmol. 2009;20(2):73–78. doi:10.1097/ICU.0b013e32831eef82
7. Lommatzsch C, Rothaus K, Koch J, et al. OCTA vessel density changes in the macular zone in glaucomatous eyes. Graefes Arch Clin Exp Ophthalmol. 2018;256:1499–1508. doi:10.1007/s00417-018-3965-1
8. Nickla DL, Wallman J. The multifunctional choroid. Prog Retin Eye Res. 2010;29(2):144–168. doi:10.1016/j.preteyeres.2009.12.002
9. Tan CS, Ouyang Y, Ruiz H, et al. Diurnal variation of choroidal thickness in normal, healthy subjects measured by spectral domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(1):261–266. doi:10.1167/iovs.11-8782
10. Agrawal R, Gupta P, Tan KA, et al. Choroidal vascularity index as a measure of vascular status of the choroid: measurements in healthy eyes from a population-based study. Sci Rep. 2016;6:21090. doi:10.1038/srep21090
11. Chen S, Wang W, Gao X, et al. Changes in choroidal thickness after trabeculectomy in primary angle closure glaucoma. Invest Ophthalmol Visual Sci. 2014;55(4):2608–2613. doi:10.1167/iovs.13-13595
12. Razeghinejad MR, Fudemberg SJ, Spaeth GL. The changing conceptual basis of trabeculectomy: a review of past and current surgical techniques. Surv Ophthalmol. 2012;57(1):1–25. doi:10.1016/j.survophthal.2011.07.005
13. Portmann N, Gugleta K, Kochkorov A, et al. Choroidal blood flow response to isometric exercise in glaucoma patients and patients with ocular hypertension. Invest Ophthalmol Vis Sci. 2019;52(10):7068–7073. doi:10.1167/iovs.11-7758
14. Zhang Z, Yu M, Wang F, et al. Choroidal thickness and open-angle glaucoma: a meta-analysis and systematic review. J Glaucoma. 2016;25(5):e446–54. doi:10.1097/IJG.0000000000000275
15. Hirooka K, Tenkumo K, Fujiwara A, et al. Evaluation of peripapillary choroidal thickness in patients with normal-tension glaucoma. BMC Ophthalmol. 2012;12:1–6. doi:10.1186/1471-2415-12-29
16. Park H-YL, Lee N-Y, Shin H-Y, et al. Analysis of macular and peripapillary choroidal thickness in glaucoma patients by enhanced depth imaging optical coherence tomography. J Glaucoma. 2014;23(4):225–231. doi:10.1097/IJG.0000000000000045
17. Mwanza J-C, Hochberg JT, Banitt MR, et al. Lack of association between glaucoma and macular choroidal thickness measured with enhanced depth-imaging optical coherence tomography. Invest Ophthalmol Visual Sci. 2011;52(6):3430–3435. doi:10.1167/iovs.10-6600
18. Suh W, Cho HK, Kee C. Evaluation of peripapillary choroidal thickness in unilateral normal-tension glaucoma. Jpn J Ophthalmol. 2014;58:62–67. doi:10.1007/s10384-013-0290-4
19. Arora KS, Jefferys JL, Maul EA, et al. The choroid is thicker in angle closure than in open angle and control eyes. Invest Ophthalmol Visual Sci. 2012;53(12):7813–7818. doi:10.1167/iovs.12-10483
20. Zhou M, Wang W, Huang W, et al. Is increased choroidal thickness association with primary angle closure? Acta Ophthalmol. 2014;92(7):e514–e520. doi:10.1111/aos.12403
21. Li F, Shang Q, Tang G, et al. Analysis of peripapillary and macular choroidal thickness in eyes with pseudoexfoliative glaucoma and fellow eyes. J Ophthalmol. 2020;2020(1):9634543. doi:10.1155/2020/9634543
22. Moghimi S, Mazloumi M, Johari M, et al. Evaluation of lamina cribrosa and choroid in nonglaucomatous patients with pseudoexfoliation syndrome using spectral-domain optical coherence tomography. Invest Ophthalmol Vis Sci. 2016;57(3):1293–1300. doi:10.1167/iovs.15-18312
23. Usui S, Ikuno Y, Uematsu S, et al. Changes in axial length and choroidal thickness after intraocular pressure reduction resulting from trabeculectomy. Clin Ophthalmol. 2013:1155–1161. doi:10.2147/OPTH.S44884
24. Aslan Bayhan S, Bayhan HA, Muhafiz E, et al. Evaluation of choroidal thickness changes after phacoemulsification surgery. Clin Ophthalmol. 2016;10:961–967. doi:10.2147/opth.S94096
25. Henderson BA, Kim JY, Ament CS, et al. Clinical pseudophakic cystoid macular edema: risk factors for development and duration after treatment. J Cataract Refract Surg. 2007;33(9):1550–1558. doi:10.1016/j.jcrs.2007.05.013
26. Xu H, Chen M, Forrester JV, et al. Cataract surgery induces retinal pro-inflammatory gene expression and protein secretion. Invest Ophthalmol Visual Sci. 2011;52(1):249–255. doi:10.1167/iovs.10-6001
27. Du S, Gao X, Zhang X, et al. Changes in retinal oxygen saturation, choroidal thickness, and retinal nerve fibre layer. Can J Ophthalmol. 2015;50(2):159–165. doi:10.1016/j.jcjo.2014.11.015
28. Kadziauskiene A, Kuoliene K, Asoklis R, et al. Changes in choroidal thickness after intraocular pressure reduction following trabeculectomy. Acta Ophthalmol. 2016;94(6):586–591. doi:10.1111/aos.13057
29. Park JW, Suh MH, Agrawal R, et al. Peripapillary choroidal vascularity index in Glaucoma-A comparison between spectral-domain OCT and OCT angiography. Invest Ophthalmol Vis Sci. 2018;59(8):3694–3701. doi:10.1167/iovs.18-24315
30. Jonas JB, Budde WM, Panda-Jonas S. Ophthalmoscopic evaluation of the optic nerve head. Surv Ophthalmol. 1999;43(4):293–320. doi:10.1016/s0039-6257(98)00049-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
Glaucoma Surgery and Ocular Blood Flow in Colour Doppler Imaging: Is There a Link?
Zarzecki M, Obuchowska I, Ustymowicz A, Konopińska J
Clinical Ophthalmology 2024, 18:49-60
Published Date: 6 January 2024
Compared to Trabeculectomy, Ex-Press® Surgery Significantly Decreased the Loss of Corneal Endothelial Cell Density in Low-Intraocular-Pressure Glaucoma: 3-Year Follow-Up
Otsuka M, Tojo N, Yamazaki H, Ueda-Consolvo T, Hayashi A
Clinical Ophthalmology 2024, 18:3009-3015
Published Date: 22 October 2024
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
Optimizing Filtration Surgery Procedures in African-Derived Populations: Trabeculectomy and Preserflo
Gazzard G, Kailani O, Muntasser H, Lim KS, Vig N, Yu J
Clinical Ophthalmology 2026, 20:570347
Published Date: 10 March 2026