Back to Journals » Clinical Ophthalmology » Volume 19
Trends in Glaucoma Fellowship Surgical Experience
Authors Creagmile J, Chen N ![]() , Yee P, Lin K
, Yee P, Lin K ![]() , Fox A, Smith A
, Fox A, Smith A ![]() , Kwan C, Mosaed S
, Kwan C, Mosaed S
Received 4 March 2025
Accepted for publication 16 July 2025
Published 12 August 2025 Volume 2025:19 Pages 2719—2727
DOI https://doi.org/10.2147/OPTH.S526259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jack Creagmile, Natalie Chen, Philina Yee, Ken Lin, Austin Fox, Andrew Smith, Claire Kwan, Sameh Mosaed
Department of Ophthalmology, Glaucoma Division, University of California - Irvine, Irvine, CA, USA
Correspondence: Jack Creagmile, Email [email protected]
Purpose: To evaluate trends in fellow exposure to trabeculectomy, tube shunt, and minimally invasive glaucoma surgery (MIGS) procedures during glaucoma fellowship training.
Methods: We analyzed fellowship surgical logs from 2013 to 2024 from the Association of University Professors of Ophthalmology (AUPO) Fellowship Compliance Committee to determine the frequency of trabeculectomy, tube shunt, and MIGS procedures within glaucoma fellowship programs.
Results: Our analysis revealed a 55.9% decrease with significant correlative decline (r = − 0.89, p = 0.0002) over the 11-year study period in total trabeculectomy exposure (primary and assistant surgeon), while total tube shunt surgeries underwent a modest 7.3% decrease with significant correlative decline (r = − 0.80, p = 0.003) over the 11-year study period, and MIGS procedures showed a marked 128.6% increase with significant correlative increase (r = +0.72, p = 0.02) from 2016 to 2024.
Conclusion: The declining exposure to trabeculectomy surgery, both as primary and assistant surgeon raises concerns about glaucoma fellowship graduate proficiency with this fundamental procedure. This may limit access to qualified care for specific glaucoma populations that may benefit most from this intervention, and for the continued care of patients that have previously undergone trabeculectomy surgery. These findings highlight the need to maintain proficiency in trabeculectomy to ensure optimal care for diverse glaucoma patient populations.
Keywords: glaucoma, trabeculectomy, glaucoma drainage implant, minimally invasive glaucoma surgery, MIGS, fellowship training, surgical trends, ophthalmology
Introduction
Glaucoma, a leading cause of irreversible blindness worldwide, has seen significant advancements in surgical management over the past few decades.1 While medical and laser therapy is frequently the foundation of treatment, surgery is often required in refractory cases. The major categories of surgical interventions currently employed to control IOP in refractory or advanced cases are traditional glaucoma surgeries, such as trabeculectomy and aqueous tube shunt surgery, as well as emerging minimally invasive glaucoma surgery (MIGS) or minimally invasive bleb surgery (MIBS). Along with these advancements come shifts in clinical practices with recent years demonstrating an overall decline in traditional glaucoma surgeries performed and an overall increase in MIGS/MIBS performed.2 According to Medicare and Medicaid Services Part B Database, there has been an overall 176.66% increase in glaucoma surgeries performed nationally from 2011 to 2021.3 However, despite this increase, there was an overall 58.5% decline in trabeculectomies performed and a fluctuating but eventual 18.69% decline in glaucoma tube shunt surgeries during this time. In contrast, MIGS and MIBS demonstrated an overall 513.4% increase with the iStent MIGS alone accounting for 46.8% of all glaucoma surgeries by 2011. This trend is also reflected in the AAO Ophthalmology Intelligent Research in Sight (IRIS) registry, which reported a 422.92% increase in MIGS and MIBS performed and a 15.5% decline in traditional glaucoma surgeries.4 This trend may be explained by the technical difficulty of traditional glaucoma surgeries, the comparatively lower risk profile of MIGS and MIBS surgeries, and the reimbursement policies of the United States healthcare system which discourage interventions that have an involved postoperative period.
Prior studies on glaucoma fellowship training have taken note of this trend but found trabeculectomy and glaucoma tube shunt surgery exposure to remain fairly stable in training despite an increase in MIGS/ MIBS exposure. However, our study provides an important update on the surgical trends in fellowship training utilizing the most recent data from the Association of University Professors of Ophthalmology (AUPO) Fellowship Compliance Committee (aupofcc.org), which demonstrates a notable decline in overall exposure to trabeculectomy (as primary and assistant surgeon) and a clear increase in MIGS/ MIBS performed by glaucoma fellows nationally. This trend in fellowship is concerning as the lack of exposure in training as both primary and assistant surgeon perpetuates a cycle of underutilization in subsequent practice and even less exposure for future trainees. Our study brings to light these findings in order to reinforce the importance of maintaining proficiency in traditional glaucoma surgeries in fellowship, ultimately to ensure optimal care of our diverse glaucoma patient populations.
Materials and Methods
To assess trends in surgical training, we analyzed AUPO’s database of all surgical case logs from 2013 to 2024 submitted by glaucoma fellowship programs. All AUPO FCC compliant glaucoma fellowship programs across the United States are included in this database and the total number of fellows included each academic year is noted in Tables 1–3. This dataset provided information on the number of cases and types of glaucoma surgeries performed by fellows (both as primary surgeon and as assistant surgeon) and is populated from surgical logs submitted by fellows during their exit questionnaire at the time of fellowship completion. We categorized the appropriate surgical procedures into three main groups: trabeculectomy, tube shunt surgery, and MIGS. Only primary trabeculectomies and tube shunt surgeries were included in this study, revisions were excluded. Tube shunt surgeries were not further specified by the type of glaucoma drainage implant device in the database, so this information was not available for review. For the purposes of this study, MIGS includes MIBS and will not be further delineated. The type of MIGS specified in this database included Gonioscopy Assisted Transluminal Trabeculotomy (GATT), Hydrus (Alcon), Istent (Glaukos), Xen Gel Stent (AbbVie), PreserFlo (Santen), Suprachoroidal Stents, Canaloplasty, and Endocyclophotocoagulation (ECP). Of note, consistent formal reporting of MIGS was not recorded by the AUPO until the 2016–2017 fellowship year. Surgeries that were not pertinent to a glaucoma fellowship training specifically (eg cataract surgery, globe repair, exam under anesthesia)) and in-office procedures (transscleral cyclophotocoagulation, laser iridotomy, laser capsulotomy) were excluded from the analysis. Mean annual totals for each procedure type were calculated, both as primary surgeon and as assisting surgeon, and trends were analyzed over the 2013–2024 period. Statistical analysis and linear regression were done by computing a Pearson correlation coefficient (r) to assess the relationship between fellowship year and mean glaucoma surgery cases per fellow with p < 0.05 considered statistically significant. The proposed study was submitted to UCI IRB for review but was found to meet the criteria for Non-Human Subjects Research (NHSR) and approved for IRB exemption.
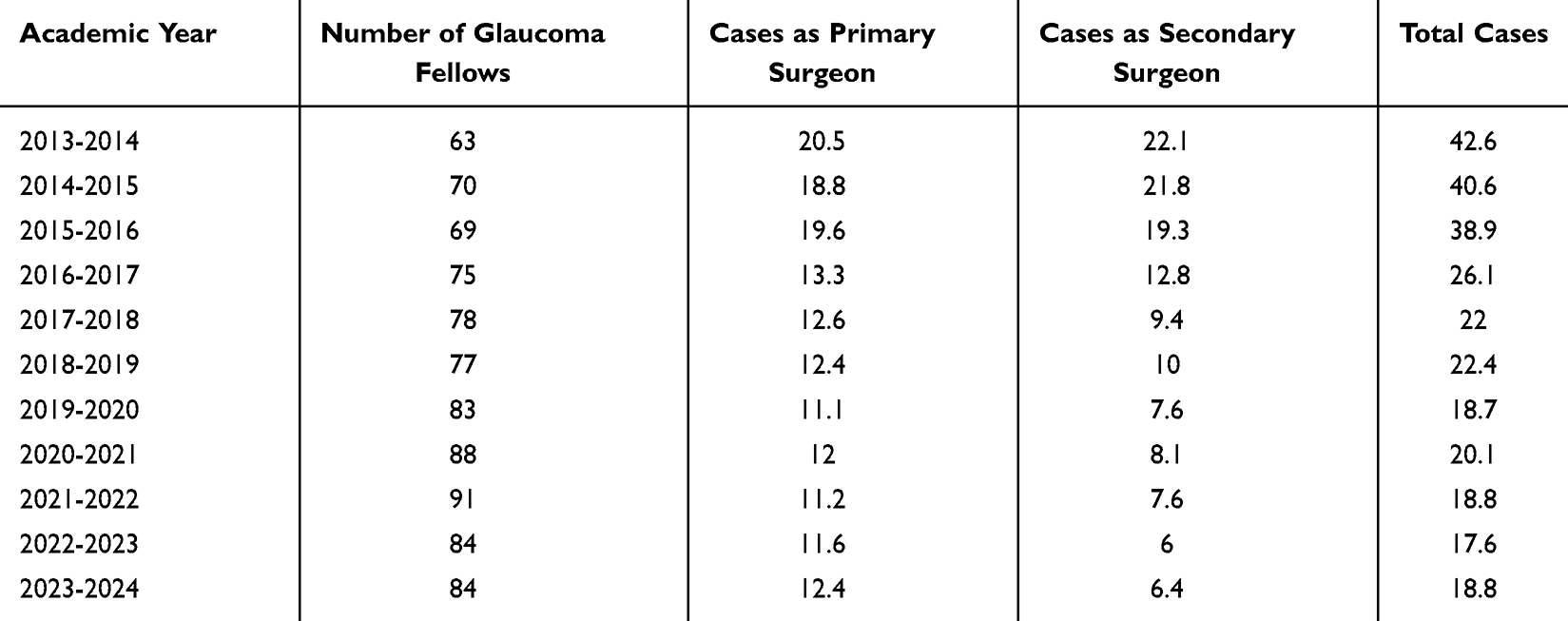 |
Table 1 AUPO Case Log: Average Number of Trabeculectomy Surgeries per Glaucoma Fellow Annually from 2013 - 2024 |
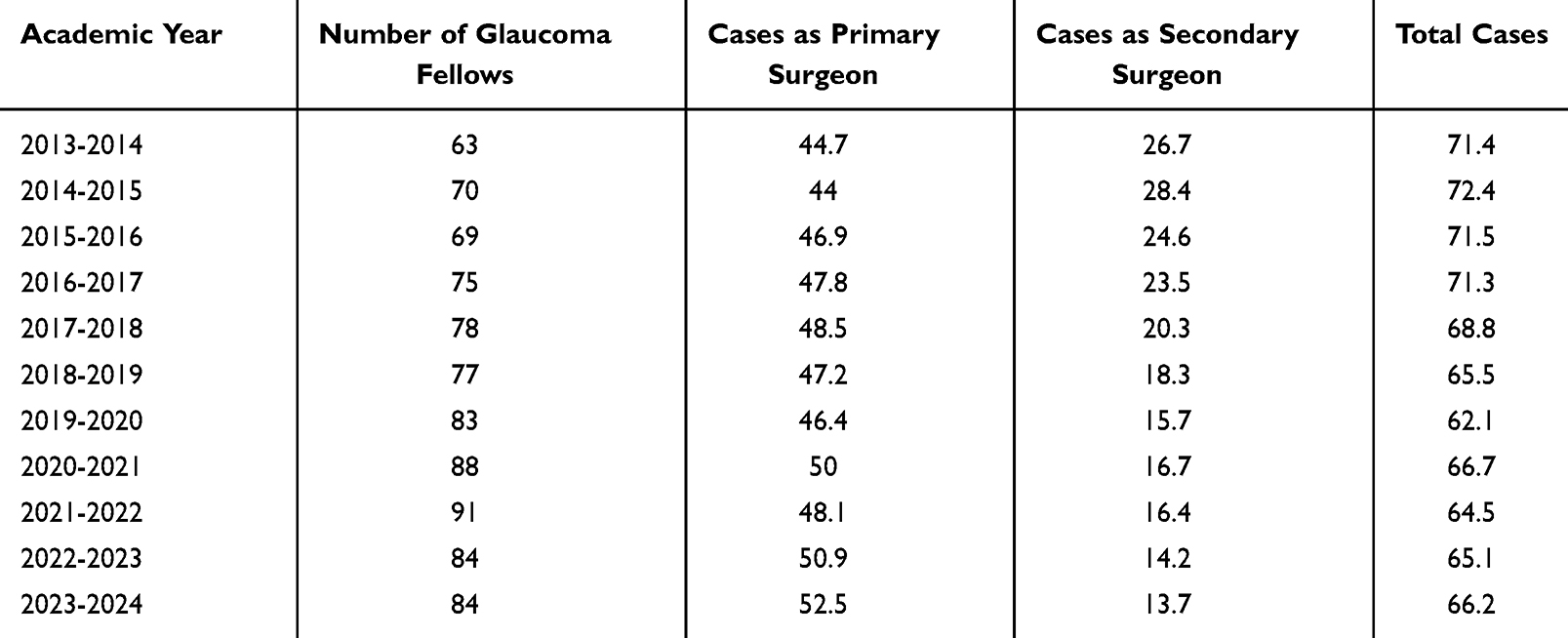 |
Table 2 AUPO Case Log: Average Number of Tube Shunt Surgeries per Glaucoma Fellow Annually from 2013 - 2024 |
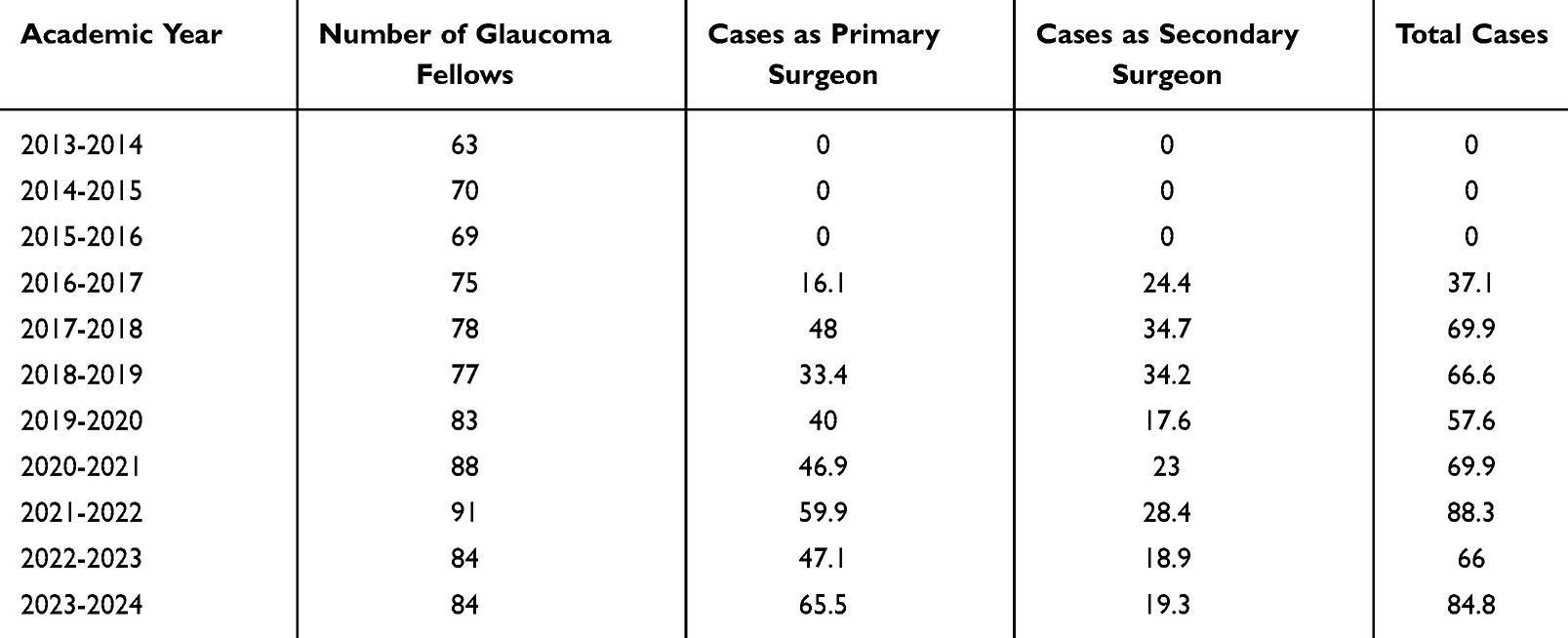 |
Table 3 AUPO Case Log: Average Number of Minimally Invasive Glaucoma Surgeries (MIGS) per Glaucoma Fellow Annually from 2013 - 2024 |
Results
Our analysis revealed significant shifts in surgical experience by glaucoma fellows from 2013 to 2024. Total trabeculectomy exposure in fellowship training (sum of primary and assist cases) showed a significant correlative decline over this 11-year period (r = −0.89, p = 0.0002, Figure 1) with a 55.9% decrease in cases between 2013 and 2024 (Table 1). Total tube shunt exposure in fellowship training (sum of primary and assist cases) showed a significant correlative decline over this 11-year period (r = −0.80, p = 0.003, Figure 2) with 7.3% decrease in cases between 2013 and 2024 (Table 2). Total MIGS exposure in fellowship training (sum of primary and assist cases) showed a significant correlative increase over this 11-year period (r = +0.72, p = 0.02, Figure 3) with a marked 128.6% increase in cases between 2013 and 2024 (Table 2). These results indicate a clear shift in glaucoma fellow surgical exposure, with a significant decrease in trabeculectomy experience paired with a concurrent rise in MIGS procedures.
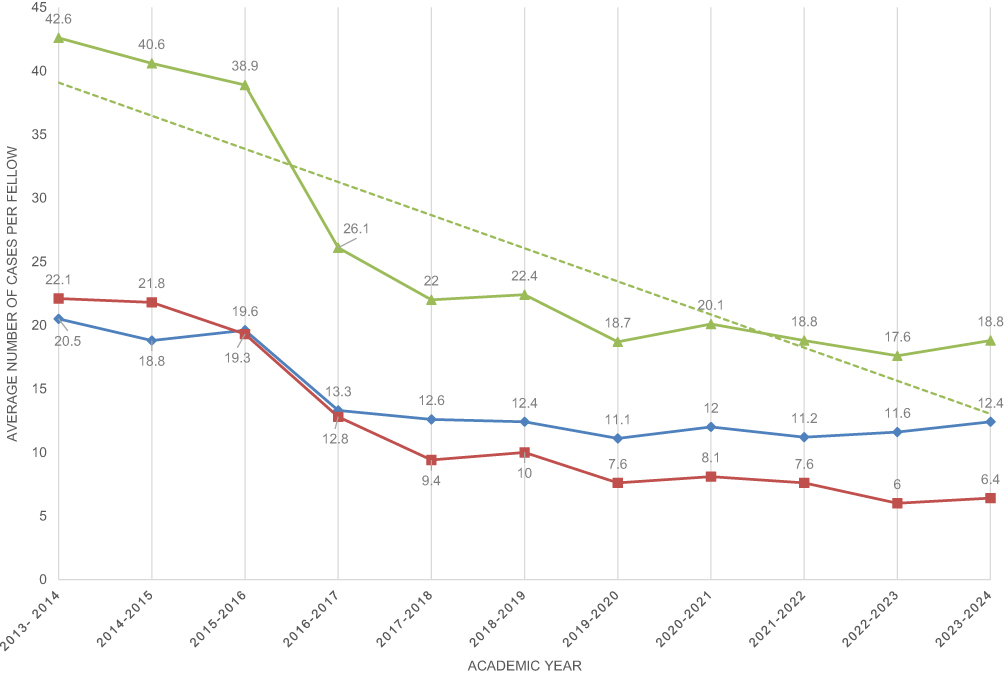 |
Figure 1 Average number of trabeculectomy surgeries per fellow per year from 2013–2024 (triangle) with an overlaying trendline demonstrating a significant downward trend over the years (r = −0.89, p = 0.0002). Further stratified by the fellow’s role in the case as primary surgeon (diamond) or secondary surgeon (square). |
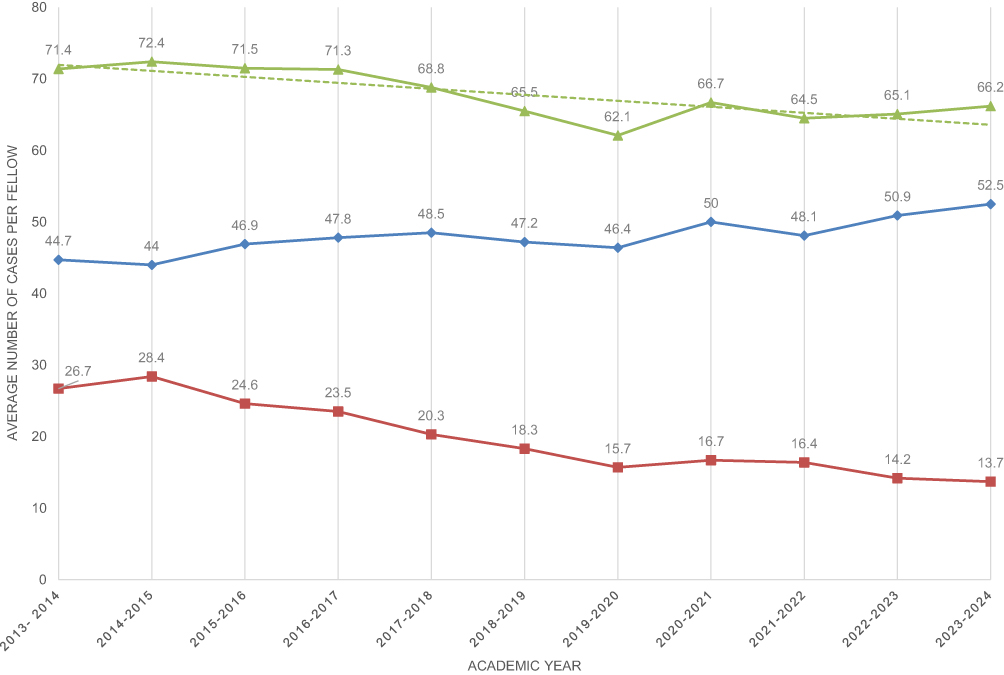 |
Figure 2 Average number of tube shunt surgeries per fellow per year from 2013–2024 (triangle) with an overlaying trendline demonstrating a significant downward trend over the years (r = −0.80, p = 0.003). Further stratified by the fellow’s role in the case as primary surgeon (diamond) or secondary surgeon (square). |
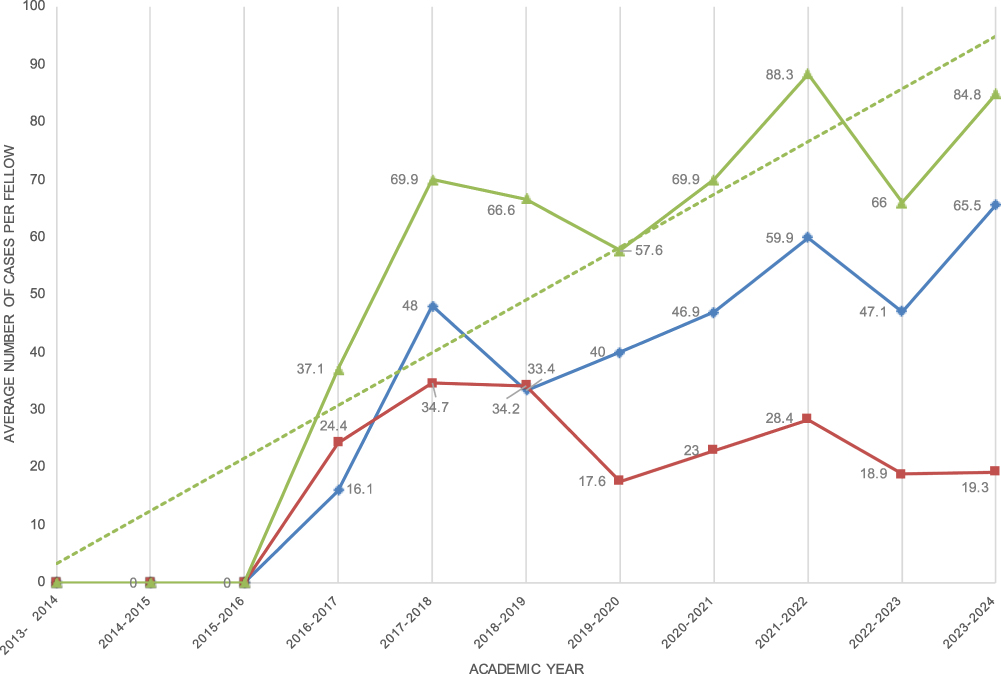 |
Figure 3 Average number of minimally invasive glaucoma surgeries (MIGS) per fellow per year from 2013–2024 (triangle) with an overlaying trendline demonstrating a significant upward trend over the years (r = +0.72, p = 0.02). Further stratified by the fellow’s role in the case as primary surgeon (diamond) or secondary surgeon (square). |
Discussion
Trabeculectomy, first described by Cairns in 1968, has long been considered the gold standard in glaucoma filtration surgery.5,6 This procedure involves creating a partial-thickness scleral flap and a full-thickness sclerostomy to allow aqueous humor to flow from the anterior chamber to the subconjunctival space, forming a filtering bleb. Over the years, modifications such as the use of antimetabolites (eg, mitomycin C and 5-fluorouracil) have improved its success rates and longevity.7–10 This procedure has several key steps, none of which are standardized, and are essentially up to the surgeon’s preference. These steps include the choice of anesthesia, conjunctival incision (fornix based or limbal based), the method and concentration of antimetabolite application (sponges v injected) the size and shape of the scleral flap, the size of the sclerostomy, the method of scleral flap closure (releasable v interrupted sutures), the preferred degree of flap closure (watertight v immediate filtration), and the method of conjunctival closure.11–18 This lack of standardization with a technically challenging surgery illustrates the need for repeated exposure with a skilled mentor to adequately hone the necessary surgical skills that cannot be otherwise easily replicated. A previous study analyzed the types of glaucoma surgeries performed by trainees from 2008 to 2016, which showed that trabeculectomy surgery among trainees fluctuated slightly from year to year but was largely stable at that time.7 A more recent 2023 study looking at cases performed by glaucoma trainees from 2013 to 2018 found that MIGS procedures (including trabectome, goniotomy, iStent, GATT, Trabeculotomy 360/OMNI and cypass) were increasing while tube shunt and trabeculectomy numbers were fairly stable.19 This study provides an important update on surgical trends to include more recent data, but importantly includes fellowship experience both as the primary and assisting surgeon, which is a more comprehensive view of overall trabeculectomy exposure during training.
Aqueous tube shunts, also known as glaucoma drainage devices, were developed to provide an alternative to trabeculectomy, especially in cases with a high risk of failure or in refractory glaucoma.7,20–22 The surgical technique for implanting aqueous shunts do allow for some minor variations, however the basic concept involves opening the conjunctiva, suturing the tubes with permanent sutures a minimum distance behind the limbus, entering the anterior chamber or scleral sulcus with a needle, and inserting the tube. This is then covered with a patch grafting material (sclera or corneal graft). While the surgical variations in tube shunt surgery mainly involve the choice of implant (valved v non-valved), the steps of the procedure are more uniform than trabeculectomy. To underscore the facility with which trainees can adopt this technique, a study by Thangamathesvaran et al showed no difference in outcomes of tube shunt surgery when performed by trainees as compared to attending surgeons.23
The results of numerous randomized controlled trials indicate that the IOP reductions seen following implantation of tube shunts are not superior to the trabeculectomy, and indeed more medications were required to achieve similar results to the trabeculectomy.24–27 However, many of these studies found that there were more complications seen after trabeculectomy, highlighting the fact that trabeculectomy outcomes are highly unpredictable, and that surgical technique may be particularly impactful on these outcomes.
MIGS procedures represent the latest evolution in glaucoma surgery, aiming to provide a safer, less invasive approach with faster recovery times.28 The current literature indicates that IOP outcomes following these procedures are modest, with typical post-operative IOP in the mid teens.29–32 Patients often need topical glaucoma medications to achieve these results, and MIGS procedures are typically performed on patients with only mild to moderate disease, often in combination with phacoemulsification. There is a paucity of data regarding the use of MIGS in advanced disease. While there is a learning curve for MIGS, many surgeons have adopted MIGS surgery into their practice without a glaucoma fellowship, and indeed a large proportion of MIGS procedures in the US are not performed by sub-specialists.33 A recent study by Smith et al showed no difference in ab-interno canaloplasty and trabeculotomy outcomes in cases performed by trainees as compared to seasoned glaucoma specialists.34 These findings confirm that the learning curve for MIGS is manageable by most trainees and non-glaucoma trained ophthalmologists without the need for extensive mentorship.
There are numerous options for ophthalmologists learning to perform MIGS procedures and aqueous tube shunt surgery outside of institutional training. Nearly every manufacturer of MIGS devices and instruments has developed surgical simulation models for training surgeons on their novel technique. Industry leaders have been quite successful in developing anatomically similar representations of the angle, particularly the trabecular meshwork and Schlemm’s canal, where the majority of MIGS procedures are focused. For aqueous tube shunt surgery, surgeons have long used porcine models to successfully mirror the in vivo anatomical behavior of the human eye for the relevant portions of the procedure. Conversely, no such model has yet to be devised for surgical training of the trabeculectomy. Without the ability to adequately hone the surgical skills necessary for trabeculectomy outside of the operating room, there is currently no viable alternative to fellowship training to learn trabeculectomy surgery. Trabeculectomy skill is solely acquired through observation of a skilled mentor, repetition of the key elements of surgery on a variety of eyes with inherently differing conjunctival and scleral anatomy, and intensive post-operative exposure to the myriad ways in which trabeculectomy outcomes present in the early and late-post operative period.35
There are numerous potential contributing factors for the observed decline in trabeculectomy utilization. First, the development of MIGS devices has provided surgeons with less invasive options that offer quicker recovery times and potentially fewer short-term complications. The perceived lower risk profile of MIGS procedures may make them more appealing to patients and their surgeons. This may compel surgeons to favor MIGS over trabeculectomy even when the treatment may be suboptimal and may have a higher risk of long-term treatment failure due to insufficient IOP lowering. Second, the decrease in trabeculectomy procedures during fellowship training may perpetuate a cycle of reduced utilization in subsequent practice. If trainees receive inadequate or limited experience with trabeculectomy during training, they may be less likely to routinely employ the procedure in practice. This carries forward when these newly-trained glaucoma specialists pursue careers in academia, and very well may already be a factor contributing to declining trabeculectomy numbers in fellowship programs that include junior faculty members. Lastly, the reimbursement policies of the healthcare system in the United States financially discourage interventions that require intensive care during the 90-day global postoperative period, as none of these visits are compensated. Trabeculectomy, even with impeccable surgeon performance, requires frequent and time-intensive clinic visits during this period.36 These visits are crucial to the long-term success of the surgery, and often require injection of antimetabolite into the surgical site to prevent fibrosis and encapsulation of the filtering bleb, and laser/mechanical suture lysis to titrate proper flow through the scleral flap.37 Given the well-documented effects of reimbursement on surgeon choice of intervention in the glaucoma space, the United States’ financial reimbursement of trabeculectomy is a likely deterrent to its utilization.38
Implications of Decreased Trabeculectomy Utilization
The declining rates of trabeculectomy in fellowship training raise several concerns. Reduced exposure to trabeculectomy during training may lead to a phenomenon of skill erosion, where subsequent generations of surgeons are less adept with the technically demanding procedure of trabeculectomy. This, in turn, could potentially impact surgical outcomes if and when it is performed. Studies have previously shown increased rates of postoperative complications when trainees performed trabeculectomy surgery in comparison to attending physicians, highlighting the challenging learning curve and emphasizing the importance of intensive surgical training under expert supervision and guidance.39
As surgeons become less experienced with trabeculectomy, there may be a tendency to opt for alternative procedures due to unfamiliarity with the procedure. Even in cases where trabeculectomy would be the optimal choice, surgeon lack of experience with trabeculectomy may limit their surgical options for the comprehensive range of surgical cases. The trend towards MIGS procedures, which are often more expensive and may have more limited insurance coverage, could exacerbate existing health disparities in glaucoma care. In addition to the costs of the surgical devices used in most MIGS procedures, the increased need for long-term topical medications in patients treated with these less effective modalities results in considerable cost burden, perpetuating health disparities.40,41
The deferment of trabeculectomy in favor of MIGS, laser treatments, or tube shunts results in increased medication reliance.42 Increased topical medication necessity in turn leads to increased ocular surface inflammation and decreased conjunctival health, thusly increasing the risk of trabeculectomy failure if and when the patient ultimately is referred for trabeculectomy.43–45 Despite the recent trends in declining utilization of trabeculectomy for surgical treatment of glaucoma, there are hundreds of thousands of patients that have undergone trabeculectomy surgery in the United States that necessitate continued active management.46 These patients may transfer care to another ophthalmologist during their lifetime, and it is imperative that they are under the care of providers that are equipped to manage both routine care and management of late post-surgical complications of trabeculectomy. Long-term complications from trabeculectomy continue to arise even years following the procedure, and it is imperative that we train surgeons comfortable in this space in order to manage the complexities of these complications.47–49
Our results indicate a 55.9% decrease (p = 0.0002) in overall trabeculectomy exposure during fellowship training from 2013 to 2024. With trainees performing 3–4 times as many tubes and MIGS, the current trajectory suggests that many trainees will not have sufficient exposure to the variations in trabeculectomy technique and post-operative manipulations to achieve good outcomes, and to feel comfortable continuing to offer this treatment through the trajectory of their careers.
There are two main limitations to the data in this study. First, fellowship surgical entry data is self-reported by outgoing glaucoma fellows. This inherently can lead to some level of inaccuracy if fellows have been cursory in their duties of surgical case logs, both in terms of overall case numbers, and in the proper classification of primary or assisting surgeon as defined by the AUPO. Second, the categories available for fellows to sort their surgical data into has been imperfect during the study period. The most notable of these imperfections was the lack of a clear classification for the Xen gel stent until recent years. Fellows may have logged these as trabeculectomy or MIGS prior to more recent AUPO updated surgical logsheets. Although this would indicate that the decline in trabeculectomy surgery is even more pronounced in reality than as observed in the data, it nevertheless may somewhat degrade the quality of the data from which the study derives its conclusions.
Our findings confirm that overall trabeculectomy exposure during training has fallen to a critically low level, a concern shared by thought-leaders in the field, and active efforts need to be made to increase the trabeculectomy experience in fellowship training to ensure its survival.37,50 These concerns highlight the importance of maintaining proficiency in a full range of glaucoma surgical techniques, including trabeculectomy, to ensure that all patients have access to the most appropriate treatment for their specific needs.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet. 2004;363(9422):1711–1720. doi:10.1016/S0140-6736(04)16257-0
2. Schwartz GF, Patel A, Naik R, Lunacsek O, Ogbonnaya A, Campbell J. Characteristics and treatment patterns of newly diagnosed open-angle glaucoma patients in the United States: an administrative database analysis. Ophthalmol Glaucoma. 2021;4(2):117–125. doi:10.1016/j.ogla.2020.09.002
3. Jayaram RH, Maheshwari A, Sarrafpour S, Liu J, Teng C. Trends for glaucoma surgeries in the United States from 2011 and 2021 – a national study. Invest Ophthalmol Vis Sci. 2024;65(7):4641.
4. Yang SA, Mitchell W, Hall N, et al. Trends and usage patterns of minimally invasive glaucoma surgery in the United States: IRIS® registry analysis 2013–2018. Ophthalmol Glaucoma. 2021;4(6):558–568. doi:10.1016/j.ogla.2021.03.012
5. Cairns JE. Trabeculectomy: preliminary report of a new method. Am J Ophthalmol. 1968;66(4):673–679. doi:10.1016/0002-9394(68)91288-9
6. Rao A, Cruz RD. Trabeculectomy: does it have a future? Cureus. 2022;14(8).
7. Wilkins M, Indar A, Wormald R. Intraoperative mitomycin C for glaucoma surgery. Cochrane Database Syst Rev. 2005;2010(4). doi:10.1002/14651858.CD002897.pub2
8. Chadha N, Warren JL, Liu J, Tsai JC, Teng CC. Seven-and eight-year trends in resident and fellow glaucoma surgical experience. Clin Ophthalmol. 2019;13:303. doi:10.2147/OPTH.S185529
9. Islamaj E, Wubbels RJ, de Waard PW. Primary baerveldt versus trabeculectomy study after 5 years of follow‐up. Acta ophthalmologica. 2020;98(4):400–407. doi:10.1111/aos.14265
10. Cabourne E, Clarke JC, Schlottmann PG, Evans JR. Mitomycin C versus 5‐Fluorouracil for wound healing in glaucoma surgery. Cochrane Database Syst Rev. 2015;2015(11). doi:10.1002/14651858.CD006259.pub2
11. Jones E, Clarke J, Khaw PT. Recent advances in trabeculectomy technique. Curr Opin Ophthalmol. 2005;16(2):107–113. doi:10.1097/01.icu.0000156138.05323.6f
12. Lee MJ, Bajaj RP, Mihailovic A, Iyer JV, Jampel HD, Friedman DS. Outcomes of a modified trabeculectomy closure technique. J Glaucoma. 2019;28(7):584–587. doi:10.1097/IJG.0000000000001263
13. Wang Q, Nauheim J, Kolomeyer NN, Pro MJ, Pro MJ. Fornix-based trabeculectomy conjunctival closure: winged sutures versus modified wise closure. Ophthalmol Glaucoma. 2019;2(4):251–257. doi:10.1016/j.ogla.2019.04.005
14. Al-Haddad CE, Abdulaal M, Al-Moujahed A, Ervin AM, Ismail K. Fornix-based versus limbal-based conjunctival trabeculectomy flaps for glaucoma: findings from a Cochrane systematic review. Am J Ophthalmol. 2017;174:33–41. doi:10.1016/j.ajo.2016.10.006
15. Zhou M, Wang W, Huang W, Zhang X. Trabeculectomy with versus without releasable sutures for glaucoma: a meta-analysis of randomized controlled trials. BMC Ophthalmol. 2014;14:1–8. doi:10.1186/1471-2415-14-41
16. Vandewalle E, Van de Veire S, Renier C, Stalmans I, Zeyen T. Trabeculectomy with or without anterior chamber maintainer and adjustable sutures. J Glaucoma. 2014;23(2):95–100. doi:10.1097/IJG.0b013e318269806a
17. Duman F, Faria B, Rutnin N, et al. Comparison of 3 different releasable suture techniques in trabeculectomy. Eur J Ophthalmol. 2016;26(4):307–314. doi:10.5301/ejo.5000718
18. He M, Wang W, Zhang X, Huang W. Ologen implant versus mitomycin C for trabeculectomy: a systematic review and metaanalysis. PLoS One. 2014;9(1):e85782. doi:10.1371/journal.pone.0085782
19. Nipp GE, Aref AA, Stinnett SS, Muir KW. Glaucoma Fellows-in-Training Recent Surgery Trends. Ophthalmol Glaucoma. 2023;6(6):651–656. doi:10.1016/j.ogla.2023.06.006
20. Minckler DS, Francis BA, Hodapp EA, et al. Aqueous shunts in glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2008;115(6):1089–1098. doi:10.1016/j.ophtha.2008.03.031
21. Tseng VL, Coleman AL, Chang MY, Caprioli J. Aqueous shunts for glaucoma. Cochrane Database Syst Rev. 2017;2017(7). doi:10.1002/14651858.CD004918.pub3
22. Chopra V, Takusagawa HL, Rosdahl JA, et al. Aqueous shunts with extraocular reservoir for open-angle adult glaucoma: a report by the American Academy of Ophthalmology. Ophthalmology. 2024;131(2):227–239. doi:10.1016/j.ophtha.2023.10.007
23. Thangamathesvaran L, Crane E, Modi K, Khouri AS. Outcomes of resident-versus attending-performed tube shunt surgeries in a United States residency program. J Curr Glaucoma Pract. 2018;12(2):53. doi:10.5005/jp-journals-10028-1245
24. Gedde SJ, Herndon LW, Brandt JD, Budenz DL, Feuer WJ, Schiffman JC, Tube Versus Trabeculectomy Study Group. Postoperative complications in the Tube Versus Trabeculectomy (TVT) study during five years of follow-up. Am J Ophthalmol. 2012;153(5):804–814. doi:10.1016/j.ajo.2011.10.024
25. Edmunds B, Thompson JR, Salmon JF, Wormald RP. The national survey of trabeculectomy. III. Early and late complications. Eye. 2002;16(3):297–303. doi:10.1038/sj.eye.6700148
26. Jampel HD, Musch DC, Gillespie BW, Lichter PR, Wright MM, Guire KE, Collaborative Initial Glaucoma Treatment Study Group. Perioperative complications of trabeculectomy in the collaborative initial glaucoma treatment study (CIGTS). Am J Ophthalmol. 2005;140(1):16–22. doi:10.1016/j.ajo.2005.02.013
27. Sarkisian SR Jr. Tube shunt complications and their prevention. Curr Opin Ophthalmol. 2009;20(2):126–130. doi:10.1097/ICU.0b013e328323d519
28. Saheb H, Ahmed II. Micro-invasive glaucoma surgery: current perspectives and future directions. Curr Opin Ophthalmol. 2012;23(2):96–104. doi:10.1097/ICU.0b013e32834ff1e7
29. Chan PP, Larson MD, Dickerson JE Jr, et al. Minimally invasive glaucoma surgery: latest developments and future challenges. Asia-Pacific J Ophthalmol. 2023;12(6):537–564. doi:10.1097/APO.0000000000000646
30. Balas M, Mathew DJ. Minimally invasive glaucoma surgery: a review of the literature. Vision. 2023;7(3):54. doi:10.3390/vision7030054
31. Lim R. The surgical management of glaucoma: a review. Clin Experiment Ophthalmol. 2022;50(2):213–231. doi:10.1111/ceo.14028
32. Cantor L, Lindfield D, Ghinelli F, et al. Systematic literature review of clinical, economic, and humanistic outcomes following minimally invasive glaucoma surgery or selective laser trabeculoplasty for the treatment of open-angle glaucoma with or without cataract extraction. Clin Ophthalmol. 2023;Volume 17:85–101. doi:10.2147/OPTH.S389406
33. Rathi S, Andrews CA, Greenfield DS, Stein JD. Trends in glaucoma surgeries performed by glaucoma subspecialists versus nonsubspecialists on medicare beneficiaries from 2008 through 2016. Ophthalmology. 2021;128(1):30–38. doi:10.1016/j.ophtha.2020.06.051
34. Smith AK, Kwan CC, Fox A, et al. Prospective study of canaloplasty and trabeculotomy performed by trainees. Clin Ophthalmol. 2024;31:17–26. doi:10.1097/00004397-199103140-00005
35. Taube AB, Niemelä P, Alm A. Trabeculectomy with an active postoperative regimen: results and resource utilization. Acta ophthalmologica. 2009;87(5):524–528. doi:10.1111/j.1755-3768.2008.01249.x
36. Singh K, Sherwood MB, Pasquale LR. Trabeculectomy must survive! Ophthalmol Glaucoma. 2021;4(1):1–2. doi:10.1016/j.ogla.2020.08.009
37. Williams PJ, Hussain Z, Paauw M, et al. Glaucoma surgery shifts among medicare beneficiaries After 2022 reimbursement changes in the United States. J Glaucoma. 2024;33(1):59–64. doi:10.1097/IJG.0000000000002294
38. Walkden A, Huxtable J, Senior M, et al. Trabeculectomy training in England: are we safe at training? Two year surgical outcomes. Eye. 2018;32(7):1253–1258. doi:10.1038/s41433-018-0059-6
39. Atik A, Fahy ET, Rhodes LA, Samuels BC, Mennemeyer ST, Girkin CA. Comparative cost-effectiveness of trabeculectomy versus MicroShunt in the US medicare system. Ophthalmology. 2022;129(10):1142–1151. doi:10.1016/j.ophtha.2022.05.016
40. Shabaninejad H, Homer T, Kernohan A, et al. Is primary trabeculectomy cost-effective for patients with advanced primary open angle glaucoma? Results from the treatment of advanced glaucoma study economic model. Br J Ophthalmol. 2024;108(9):1210–1215. doi:10.1136/bjo-2023-323390
41. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL, Tube versus Trabeculectomy Study Group. Treatment outcomes in the Tube Versus Trabeculectomy (TVT) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803. doi:10.1016/j.ajo.2011.10.026
42. Broadway DC, Grierson I, O’Brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication: II. The outcome of filtration surgery. Arch Ophthalmol. 1994;112(11):1446–1454. doi:10.1001/archopht.1994.01090230060021
43. Lee S, Park DY, Huh MG, Cha SC. Influence of preoperative glaucoma medication on long-term outcomes of trabeculectomy. Sci Rep. 2024;14(1):28341. doi:10.1038/s41598-024-79637-z
44. Wong JK, Leung TK, Lai JS, Chan JC. Evaluation of adverse effects of topical glaucoma medications on trabeculectomy outcomes using the glaucoma medications intensity index. Ophthalmol Ther. 2022;11(1):387–401. doi:10.1007/s40123-021-00447-x
45. Ma AK, Lee JH, Warren JL, Teng CC. GlaucoMap–distribution of glaucoma surgical procedures in the United States. Clin Ophthalmol. 2020;Volume 14:2551–2560. doi:10.2147/OPTH.S257361
46. Cardakli N, Weinreb SF, Quigley HA, Quigley HA. Long-term functional outcomes of trabeculectomy revision surgery. Ophthalmol Glaucoma. 2019;2(4):240–250. doi:10.1016/j.ogla.2019.04.003
47. Chen PP, Moeller KL. Smaller-incision revision of trabeculectomy with mitomycin: long-term outcomes and complications. J Glaucoma. 2019;28(1):27–31. doi:10.1097/IJG.0000000000001129
48. Zahid S, Musch DC, Niziol LM, Lichter PR, Collaborative Initial Glaucoma Treatment Study Group. Risk of endophthalmitis and other long-term complications of trabeculectomy in the Collaborative Initial Glaucoma Treatment Study (CIGTS). Am J Ophthalmol. 2013;155(4):674–680. doi:10.1016/j.ajo.2012.10.017
49. Walkden A, Au L, Fenerty C. Trabeculectomy training: review of current teaching strategies. Adv Med Edu Pract. 2020;Volume 11:31–36. doi:10.2147/AMEP.S168254
50. Rabiolo A, Dean WH, Ferris J, et al. Trabeculectomy must survive!(Ophthalmology Glaucoma. 2021; 4: 1-2). Ophthalmol Glaucoma. 2021;4(3):e8–9. doi:10.1016/j.ogla.2021.03.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Proportion of Glaucoma Types and Surgeries Among Young, Pre-Old, Old, and Oldest-Old Age Groups or Different Sex Groups
Tanito M, Matsuoka Y
Clinical Ophthalmology 2022, 16:1815-1819
Published Date: 7 June 2022
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
The Link Between Gastrointestinal Microbiome and Ocular Disorders
Alfuzaie R
Clinical Ophthalmology 2023, 17:2133-2140
Published Date: 25 July 2023
Glaucoma Surgery and Ocular Blood Flow in Colour Doppler Imaging: Is There a Link?
Zarzecki M, Obuchowska I, Ustymowicz A, Konopińska J
Clinical Ophthalmology 2024, 18:49-60
Published Date: 6 January 2024
Six-Month Outcomes of Goniotomy Performed with a Trapezoidal Dual Blade in Combination with Cataract Surgery
Meyer AD, Huggins D, Nwokeji I, Provencher LM
Clinical Ophthalmology 2024, 18:2619-2625
Published Date: 19 September 2024