Back to Journals » Clinical Ophthalmology » Volume 18
Compared to Trabeculectomy, Ex-Press® Surgery Significantly Decreased the Loss of Corneal Endothelial Cell Density in Low-Intraocular-Pressure Glaucoma: 3-Year Follow-Up
Authors Otsuka M ![]() , Tojo N, Yamazaki H, Ueda-Consolvo T, Hayashi A
, Tojo N, Yamazaki H, Ueda-Consolvo T, Hayashi A ![]()
Received 3 September 2024
Accepted for publication 16 October 2024
Published 22 October 2024 Volume 2024:18 Pages 3009—3015
DOI https://doi.org/10.2147/OPTH.S494422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mitsuya Otsuka, Naoki Tojo, Hitoshi Yamazaki, Tomoko Ueda-Consolvo, Atsushi Hayashi
Department of Ophthalmology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, Toyama, Japan
Correspondence: Atsushi Hayashi, Department of Ophthalmology, Graduate School of Medicine and Pharmaceutical Sciences, University of Toyama, 2630 Sugitani, Toyama City, 930-0194, Japan, Tel +81-76-434-7363, Fax +81-76-434-5037, Email [email protected]
Purpose: We compared the corneal endothelial cell loss between trabeculectomy (Trab) and Ex-Press® surgery (EXP) for low-intraocular pressure (IOP) glaucoma patients.
Patients and Methods: This was a single-facility retrospective study. We analyzed the cases of patients with primary open-angle glaucoma (POAG) and pre-operative IOP ≤ 21 mmHg who had undergone Trab or EXP surgery and were followed for > 3 years. Noncontact specular microscopy was used to determine the corneal endothelial cell density (CED) before and after Trab or EXP surgery. We measured the CED at 12, 24, and 36 months post-surgery. We compared the CED values and CED survival ratio after both surgeries using paired t-tests.
Results: We included 39 eyes that underwent Trab and 36 eyes that underwent EXP surgery. In the Trab group, the mean CED value had decreased from 2333 ± 399 at baseline to 2066 ± 587 cells/mm2 after 3 years. In the EXP group, the mean CED value had decreased from 2320 ± 393 at baseline to 2229 ± 460 cells/mm2 after 3 years. The survival ratio of CED at > 3 years was 89.3 ± 14.2% (Trab group) and 95.6 ± 11.1% (EXP group); compared to the Trab surgery, the EXP surgery thus significantly decreased the CED loss (p = 0.037). No case resulted in bullous keratopathy.
Conclusion: Compared to trabeculectomy, Ex-Press® surgery appears to be a safer surgical method with regard to the endothelial cell loss risk.
Keywords: Ex-Press, glaucoma, corneal endothelial cell, trabeculectomy
Introduction
Normal tension glaucoma accounts for ~90% of all glaucoma cases in Japan.1 Glaucoma patients with progressive visual field aggravation despite low intraocular pressure (IOP) are more common in Japan compared to some other populations. There are many options for the surgical treatment of glaucoma, but minimally invasive glaucoma surgery (MIGS) results in mid-teen values of the mmHg range, and it might be difficult to achieve a successful outcome of MIGS for patients with a low preoperative IOP value.2 Tube shunt surgery is also difficult for patients with low preoperative IOP, due to the risk of hypotony.3 For these reasons, there are limited surgical options for glaucoma patients with low preoperative IOP.
Trabeculectomy is the most common glaucoma surgery for patients with low IOP,4 and trabeculectomy was reported to be effective for low-IOP glaucoma.5,6 Another surgical option for patients with low preoperative IOP is Ex-Press® surgery (Alcon Laboratories, Fort Worth, TX, USA); several studies have indicated that Ex-Press surgery is effective for patients with low preoperative IOP.7–9 The Ex-Press is a glaucoma filtration device designed for use in glaucoma surgery, and it was approved in Japan in December 2011. The Ex-Press surgery is similar to a trabeculectomy as filtration surgery, but Ex-Press surgery has the advantages of not requiring the removal of the trabecular meshwork or a resection of the iris. The surgical outcomes of trabeculectomy and Ex-Press surgery have been compared, and most of these studies described similar surgical outcomes.10–12 A single investigation reported that Ex-Press surgery resulted in fewer postoperative complications compared to trabeculectomy.13
The cornea’s endothelial cells have the function of maintaining the transparency of the cornea. Persistent corneal edema (also called “bullous keratopathy”) due to a reduction of corneal endothelial cell density (CED) is one of the serious possible complications of filtration surgery.14 Arimura et al stated that Ex-Press surgery decreased their patients’ CED faster compared to a trabeculectomy, and they proposed that Ex-Press surgery should not be considered for eyes with compromised corneal function.15 As noted by Ishida et al, Ex-Press surgery had the disadvantages of loss of the CED compared to trabeculectomy.16 However, Omatsu et al observed that the CED of their patients who underwent Ex-Press surgery was decreased by only 0.8% at 2 years postsurgery, and they concluded that Ex-Press surgery was beneficial for patients who have a low CED.17 There are thus reports with different opinions regarding the effect of trabeculectomy and Ex-Press surgery on CED. Possible reasons for the discrepant opinions include the lack of long-term data and the coexistence of various glaucoma types.18
We conducted the present study to investigate the effects of these two surgical techniques on CED, limited to patients with primary open-angle glaucoma (POAG). We compared the CED values and the CED reduction ratio between patients with POAG who underwent a trabeculectomy and those who underwent Ex-Press surgery.
Patients and Methods
Patients
This was a retrospective single-facility study. We included consecutive POAG patients who underwent a trabeculectomy (the Trab group) or Ex-Press surgery (the EXP group) for the first time at Toyama University Hospital and were followed for >3 years. We excluded patients with glaucoma types other than POAG, such as pseudo-exfoliation glaucoma and secondary glaucoma. We also excluded patients with a preoperative IOP value ≥22 mmHg while under treatment with glaucoma medication. We excluded patients who had a history of conventional trabeculectomy, laser iridotomy, peripheral iridotomy, or keratoplasty. Since the aim of this study was to evaluate the reduction of CED affected by these filtration surgeries, we excluded patients who had undergone additional glaucoma surgery. We included patients with a history of cataract surgery, trabeculotomy (TLO), selective laser trabeculoplasty (SLT), or vitrectomy before their filtration surgery.
We analyzed 39 eyes (36 patients) that underwent a trabeculectomy during the period from May 2018 to January 2020 and 36 eyes (34 patients) that underwent an EXP surgery during the period from May 2013 to April 2018. We used binocular data for the patients who underwent trabeculectomy or Ex-Press surgery in both eyes. Ex-Press surgery was chosen for all cases before April 2018, and trabeculectomy was chosen for all cases after May 2018. Since this study’s design was retrospective, we did not define a distinct surgical indication for glaucoma or cataracts. The indication for surgery was determined based on the judgment of one glaucoma specialist (N.T).
The study’s research protocol was approved by the Institutional Review Board of the University of Toyama (IRB No. R2023254), and the procedures used conformed to the tenets of the Declaration of Helsinki. After the nature and possible consequences of the study were explained to the patients, written informed consent was obtained from all individual participants included in the study.
Surgical Techniques
All surgeries were performed by one surgeon (N.T) who has abundant experience conducting both trabeculectomy and Ex-Press surgery. The Ex-Press surgical method was as follows. The surgery was performed with the patient under retrobulbar anesthesia. A fornix-based conjunctival incision was made, and a single 3.5-mm2 scleral flap was created. Mitomycin C (MMC) 0.04 mg/mL was applied below the conjunctiva and scleral flap for 4 min and washed out with approx. 100 mL of balanced saline solution. In the case of simultaneous cataract surgery, the cataract surgery was performed at this time. Phacoemulsification was performed with a WhiteStar Signature system (Johnson and Johnson, New Brunswick, NJ), and an intraocular lens (IOL) was implanted from the clear temporal cornea. Cataract surgery was performed based on the operator’s judgment. A 25-ga. guide needle was inserted into the anterior chamber parallel to the iris at the trabecular meshwork, and an Ex-Press shunt (model p50, Alcon Laboratories, Fort Worth, TX) was then inserted into the anterior chamber. The scleral flap was sutured using 10–0 nylon with two stitches. The conjunctiva was sutured closed with 10–0 nylon to prevent leakage.
Although the trabeculectomy surgical method has many of the same steps as the Ex-Press surgery, the differences from the Ex-Press surgery are as follows: (i) the trabecular meshwork is excised, (ii) the peripheral iris is incised, and (iii) the scleral flap is sutured with four stitches.
Postoperative Treatment
The postoperative treatment protocol was same in both groups. The postoperative treatments consisted of topical steroids, antibiotics, and non-steroidal anti-inflammatory drugs (NSAIDs). The antibiotics were applied the 4–6 weeks. The steroid and NSAIDs were reduced over a 12-week period after the interventions. After surgeries, glaucoma medications were stopped in all cases.
Immediately after surgery, laser suture-lysis was performed as necessary, aiming for an IOP of 10 or less. If IOP was high even after all suture-lysis were performed, we reduced IOP by needling. We used a bleb knife for needling and did not use antimetabolite such as MMC. Glaucoma medications were added at the discretion of the physicians. We counted a compounding agent as two medications.
Evaluation of the Rate of CED Reduction
As the measurement method, we used the EM-3000 specular microscope (Tomey Corp., Nagoya, Japan) to observe the CED at the center of the cornea a single time and used the value to automatically calculate it. The patient’s CED was measured once preoperatively and every 12 months postoperatively. We defined the ratio of CED survival as the ratio of the post-operative CED to the pre-operative CED.
Statistical Analyses
We used a paired t-test for comparisons between the Trab and EXP groups. JMP Pro 14 software (SAS, Cary, NC) was used for all of the statistical analyses. Significance was defined as a p-value <0.05.
Results
Final totals of 39 (Trab group) eyes and 36 eyes (EXP group) were analyzed. The patients’ ophthalmic data are summarized in Table 1, and their post-operative IOP values and glaucoma medications are provided in Tables 2 and 3. In Trab group, there were significantly fewer patients who had undergone TLO (p = 0.0287). We could not make an equal comparison. Both the trabeculectomy and Ex-Press surgeries significantly decreased the patients’ IOP values and number of glaucoma medications. There was no significant between-group difference in the patients’ postoperative IOP (p = 0.918) or number of medications (p = 0.951). Table 4 presents the two groups’ mean CED values and CED survival ratios. No case in either group resulted in persistent corneal edema. At >3 years postsurgery, the CED survival ratio was 89.3% in the Trab group and 95.6% in the EXP group. The patients who underwent the Ex-Press surgery thus had a significantly lesser decrease in CED compared to the patients who received a trabeculectomy (p = 0.037).
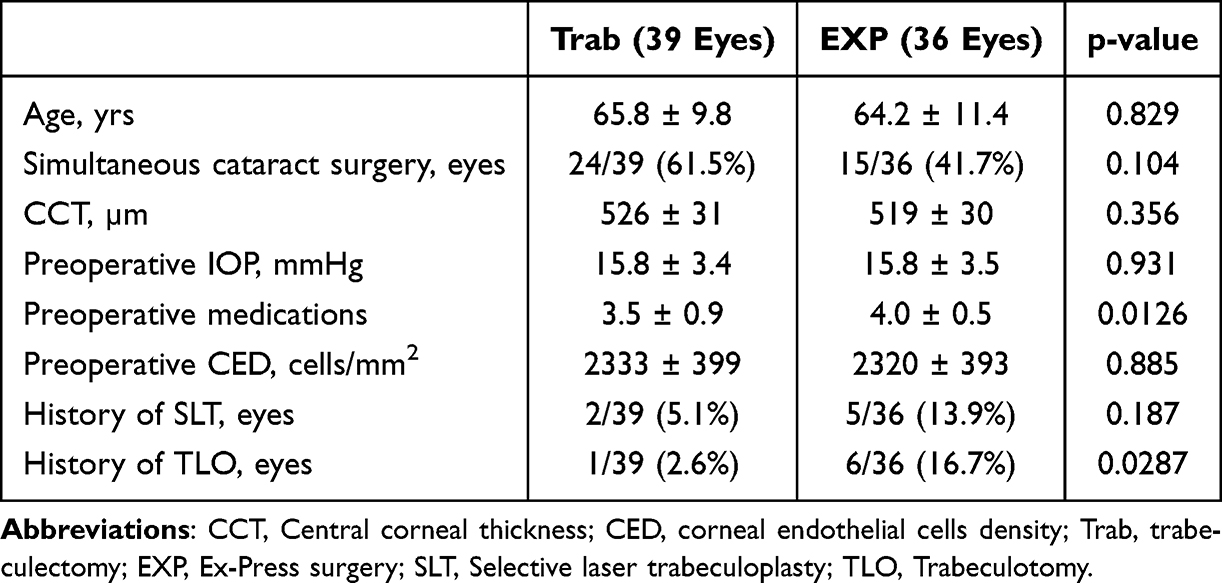 |
Table 1 Patients’ Characteristics |
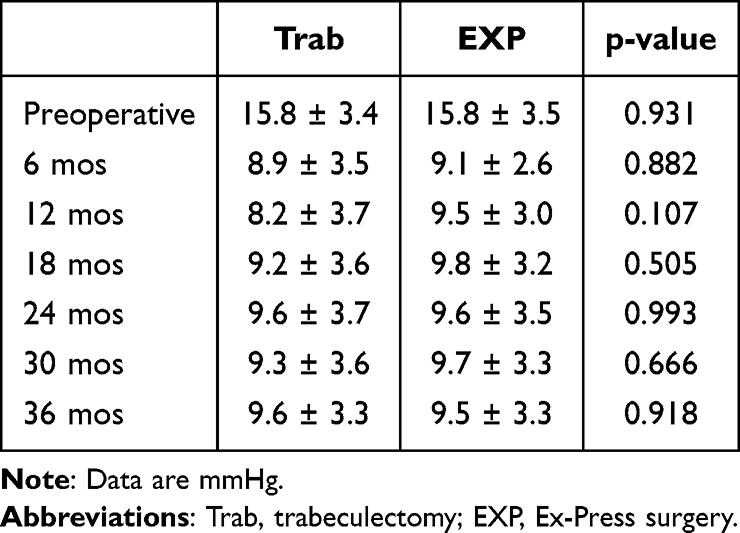 |
Table 2 Comparison of Postoperative IOP Between Ex-Press and Trabeculectomy |
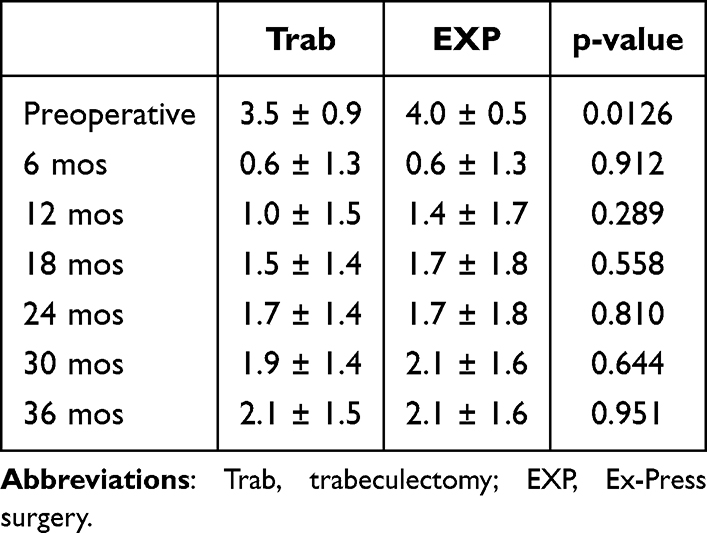 |
Table 3 The Number of Postoperative Glaucoma Medications |
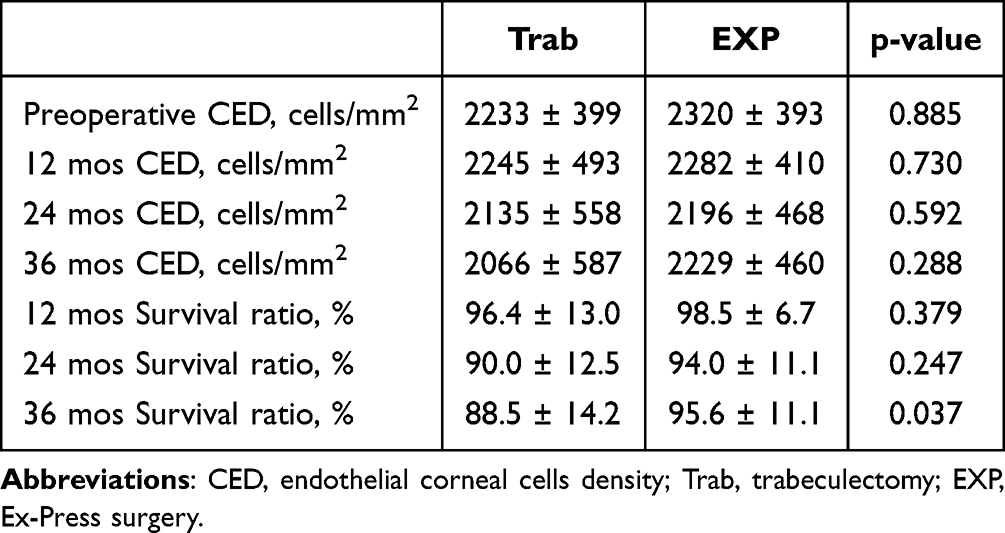 |
Table 4 Corneal Endothelial Cell Density and Survival Rate |
As an additional analysis, we compared the survival rates of CED between patients who underwent simultaneous cataract surgery and those who underwent glaucoma surgery alone. The results are shown in Table 5. Our results showed that simultaneous cataract surgery did not play a significant role in CED loss.
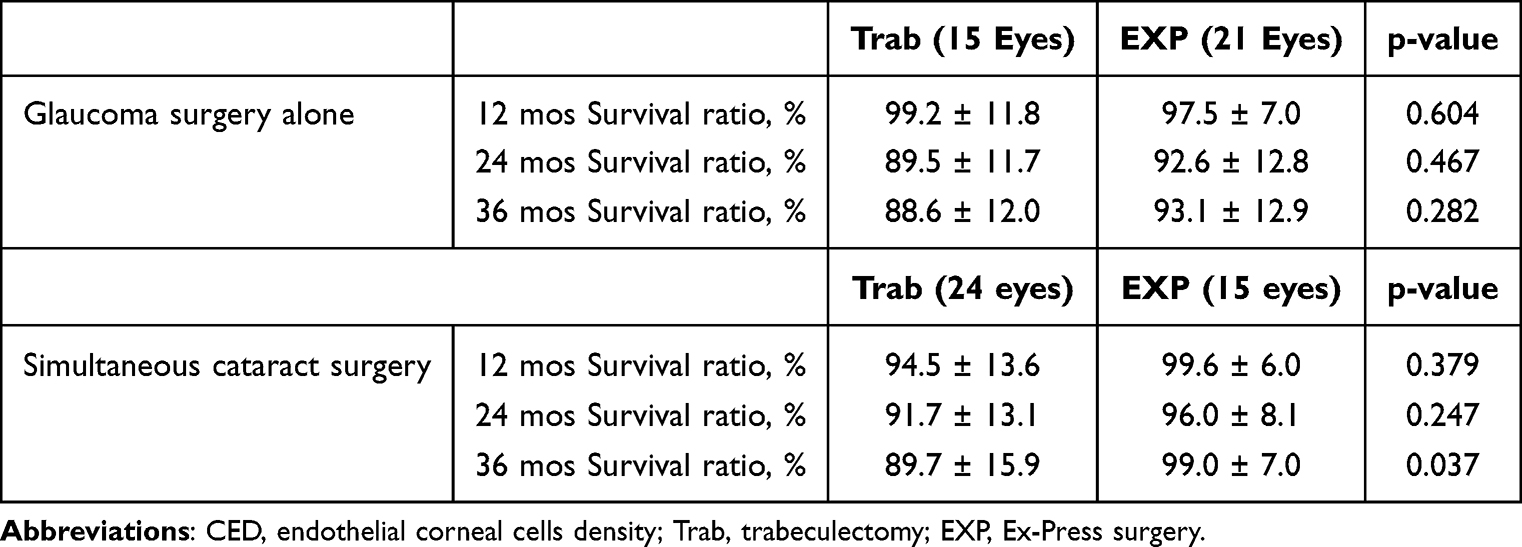 |
Table 5 Comparison of Corneal Endothelial Cell Survival Rate Between Glaucoma Surgery Alone and Simultaneous Cataract Surgery |
Discussion
The results of our present analyses of 75 eyes that underwent a trabeculectomy or Ex-Press surgery demonstrated that both surgeries significantly decreased the patients’ IOP; at >3 years postsurgery, the mean postoperative IOP was 9.6 mmHg in the Trab group and 9.6 mmHg in the EXP group. There are multiple reports that the postoperative IOP results of trabeculectomy and Ex-Press surgery were equivalent.10–13 Our present results are similar. It has been reported that the postoperative IOP was 13.1–14.7 mmHg after Ex-Press surgery and 13.1–13.9 after trabeculectomy.5,10,12 Our surgical outcomes included IOP values that are lower compared to those of the previous reports. However, clinicians need to aim for postoperative IOP values that are even lower than low preoperative IOP values. In our present investigation, we excluded the cases of patients who underwent additional glaucoma surgery, and we thus used data only from cases in which the surgery was successful.
The central cornea as the measurement site for the CED was not exactly the same site in all cases, and a measurement error may certainly have occurred. Our results also showed that in the EXP group, the CED values at 3 years post-surgery were further increased compared to the values at 2 years.
The mean CED survival ratios after 3 years of follow-up were 88.5% in the Trab group and 95.6% in the EXP group. In other words, the CED reduction ratio was 11.5% in the Trab group and 4.4% in the EXP group. There are few reports of long-term CED outcomes after a trabeculectomy or Ex-Press surgery.18 According to a study by Higashide et al, trabeculectomy decreased the CED of POAG patients by 4.8% after 2 years.15 Arimura et al noted that at 2 years post-surgery, the use of trabeculectomy had decreased the CED by 2.2% and the use of Ex-Press surgery had decreased the CED by 18.0%; they concluded that Ex-Press surgery resulted in a greater CED loss compared to trabeculectomy.15
On the other hand, several research groups reported that trabeculectomy caused a greater CED loss than Ex-Press surgery. Omatsu et al stated that at 2 years post-surgery, trabeculectomy had decreased the CED from 2505 ± 280 to 2277 ± 385 cells/mm,2 and Ex-Press surgery had decreased the CED from 2377 ± 389 to 2317 ± 449 cells/mm2.17 The mean CED reduction ratio at 12 months post-surgery in a study by Lee et al was 18.2 ± 13.3% in their trabeculectomy group and 10.0 ± 7.0% in their Ex-Press surgery group.19 The reduction ratio of CED varies widely among existing studies, especially among patients who underwent Ex-Press surgery. One of the reasons for this large variation might be due to the insertion site used in Ex-Press surgery. In one of our group’s earlier studies, we compared the CED loss between cornea insertion and trabecular meshwork insertion, and we observed that the mean CED reduction ratio was 5.2% in the trabecular meshwork insertion group and 15.1% in the corneal insertion group.20
It is well known that glaucoma filtration surgery decreases the CED. The mechanisms that underlie the loss of CED after filtration surgery might be multifactorial. Factors such as the effects of MMC, inflammatory cytokines, and the abnormal aqueous humor flow might also be involved.21–23 Although trabeculectomy decreased CED year by year, Ex-press surgery decreased less CED in long-term. The application of an iridectomy might be a major reason why the CED decreases faster in trabeculectomy compared to Ex-Press surgery. Trabeculectomy requires iridectomy, whereas Ex-press surgery does not require iridectomy. It has been reported that an iridectomy decreased the CED.24,25 Another possible effect of an iridectomy is the secretion of inflammatory cytokines. Macdonald et al reported that inflammatory cytokines decreased the CED.23 The chronic inflammation might persist in the eye after iridectomy for long time.
This study has some limitations to address. There are many causes for the decrease in corneal endothelial cells, including the effects of previous surgery or laser treatment, the severity of postoperative inflammation, peripheral anterior synechia formation, postoperative shallow anterior chamber, and postoperative treatment. It is difficult to quantify and compare all of this information, and this study did not perform a multifactorial analysis. We did not consider potential confounding factors that might influence long-term outcomes, such as systemic diseases, medication use, and smoking other than filtration surgery. For this reason, this study only evaluated a portion of the cause of the CED loss.
This study focused on EXP and Trab and was considered under the assumption that these two groups underwent the same conditions. In fact, there are some different conditions in the comparison between the two groups. For example, we included patients who had undergone cataract surgery, TLO, or SLT, and these surgeries affect the loss of the CED.26–28 Simultaneous cataract surgery did not affect CED loss significantly in this study. The number of patients with a history of TLO differed significantly between the two groups. Postoperative shallow anterior chamber is a factor in corneal endothelial cell loss.29 There were two cases in each group that occurred a shallow anterior chamber after surgery (p = 0.934). The mean of survival ratio of CED after 3 years was 74.3 ± 21.3% in Trab group and 81.5 ± 23.0% in EXP group. In this study, the CED with postoperative shallow anterior chamber decreases rapidly.
The patients’ CED was measured only once. It is desirable to measure the CED several times and use the average value to avoid measurement error. In this study, the EM-3000 we used cannot automatically measure the coefficient of variation and hexagonality. We only evaluated the mean cell density. The number of patients in this investigation may also have been too small to evaluate the CED loss.
In conclusion, our results suggest that compared to trabeculectomy, Ex-Press surgery might be a factor preventing endothelial cell loss over a long period of term.
Data Sharing Statement
The datasets in our study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
All procedures were performed in accordance with the 1964 helsinki Declaration and its later amendments or comparable ethical standards. Ethical approval is approved by the Institutional Review Board of the University of Toyama (IRB No. R2023254). A written informed consent form was obtained from all patients.
Consent for Publication
We consent for publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received.
Disclosure
No potential conflict of interest was reported by the authors.
References
1. Iwase A, Suzuki Y, Araie M, et al. The prevalence of primary open-angle glaucoma in Japanese: the Tajimi Study. Ophthalmology. 2004;111(9):1641–1648. doi:10.1016/j.ophtha.2004.03.029
2. Lavia C, Dallorto L, Maule M, Ceccarelli M, Fea AM. Minimally-invasive glaucoma surgeries (MIGS) for open angle glaucoma: a systematic review and meta-analysis. PLoS One. 2017;12(8):e0183142. doi:10.1371/journal.pone.0183142
3. Coleman AL, Hill R, Wilson MR, et al. Initial clinical experience with the Ahmed glaucoma valve implant. Am J Ophthalmol. 1995;120(1):23–31. doi:10.1016/S0002-9394(14)73755-9
4. Iverson SM, Schultz SK, Shi W, Feuer WJ, Greenfield DS. Effectiveness of single-digit IOP targets on decreasing global and localized visual field progression after filtration surgery in eyes with progressive normal-tension glaucoma. J Glaucoma. 2016;25(5):408–414. doi:10.1097/IJG.0000000000000240
5. Schultz SK, Iverson SM, Shi W, Greenfield DS. Safety and efficacy of achieving single-digit intraocular pressure targets with filtration surgery in eyes with progressive normal-tension glaucoma. J Glaucoma. 2016;25(2):217–222. doi:10.1097/IJG.0000000000000145
6. Naito T, Fujiwara M, Miki T, et al. Effect of trabeculectomy on visual field progression in Japanese progressive normal-tension glaucoma with intraocular pressure <15 mmHg. PLoS One. 2017;12(8):e0184096. doi:10.1371/journal.pone.0184096
7. Aihara M, Kuwayama Y, Miyata K, et al. Twelve-month efficacy and safety of glaucoma filtration device for surgery in patients with normal-tension glaucoma. Jpn J Ophthalmol. 2019;63(5):402–409. doi:10.1007/s10384-019-00682-7
8. Kato N, Takahashi G, Kumegawa K, Kabata Y, Tsuneoka H. Indications and postoperative treatment for Ex-PRESS® insertion in Japanese patients with glaucoma: comparison with standard trabeculectomy. Clin Ophthalmol. 2015;9:1491–1498. doi:10.2147/OPTH.S86504
9. Yuasa Y, Sugimoto Y, Hirooka K, et al. Effectiveness of trabeculectomy with mitomycin C for glaucomatous eyes with low intraocular pressure on treatment eye drops. Acta Ophthalmol. 2020;98(1):e81–e7. doi:10.1111/aos.14195
10. Gonzalez-Rodriguez JM, Trope GE, Drori-Wagschal L, Jinapriya D, Buys YM. Comparison of trabeculectomy versus Ex-PRESS: 3-year follow-up. Br J Ophthalmol. 2016;100(9):1269–1273. doi:10.1136/bjophthalmol-2015-307161
11. Chen G, Li W, Jiang F, Mao S, Tong Y. Ex-PRESS implantation versus trabeculectomy in open-angle glaucoma: a meta-analysis of randomized controlled clinical trials. PLoS One. 2014;9(1):e86045. doi:10.1371/journal.pone.0086045
12. Netland PA, Sarkisian SR Jr, Moster MR, et al. Randomized, prospective, comparative trial of EX-PRESS glaucoma filtration device versus trabeculectomy (XVT study). Am J Ophthalmol. 2014;157(2):433–40e3. doi:10.1016/j.ajo.2013.09.014
13. Liu JH, Lin HY, Tzeng SH, Chao SC. Comparison of trabeculectomy with Ex-PRESS shunt implantation in primary-open-angle-glaucoma patients: a retrospective study. Taiwan J Ophthalmol. 2015;5(3):120–123. doi:10.1016/j.tjo.2015.04.004
14. Higashide T, Nishino T, Sakaguchi K, Yamada Y, Sugiyama K. Determinants of corneal endothelial cell loss after trabeculectomy with mitomycin C. J Glaucoma. 2019;28(1):61–67. doi:10.1097/IJG.0000000000001108
15. Arimura S, Miyake S, Iwasaki K, et al. Randomised clinical trial for postoperative complications after Ex-PRESS Implantation versus trabeculectomy with 2-year follow-up. Sci Rep. 2018;8(1):16168. doi:10.1038/s41598-018-34627-w
16. Ishida K, Moroto N, Murata K, Yamamoto T. Effect of glaucoma implant surgery on intraocular pressure reduction, flare count, anterior chamber depth, and corneal endothelium in primary open-angle glaucoma. Jpn J Ophthalmol. 2017;61(4):334–346. doi:10.1007/s10384-017-0512-2
17. Omatsu S, Hirooka K, Nitta E, Ukegawa K. Changes in corneal endothelial cells after trabeculectomy and EX-PRESS shunt: 2-year follow-up. BMC Ophthalmol. 2018;18(1):243. doi:10.1186/s12886-018-0913-0
18. Aoyama Y, Sakata R, Fujishiro T, Honjo M, Shirato S, Aihara M. Changes in corneal endothelial cell density after initial Ex-PRESS drainage device implantation and its relating factors over 3 years. Eye. 2023;37(1):69–74. doi:10.1038/s41433-021-01888-1
19. Lee GY, Lee CE, Lee KW, Seo S. Long-term efficacy and safety of ExPress implantation for treatment of open angle glaucoma. Int J Ophthalmol. 2017;10(9):1379–1384. doi:10.18240/ijo.2017.09.08
20. Otsuka M, Tojo N, Hayashi A. Corneal endothelial cell loss after EX-PRESS surgery depends on site of insertion, cornea or trabecular meshwork. Int Ophthalmol. 2023;43(10):3471–3477. doi:10.1007/s10792-023-02752-9
21. Wu KY, Wang HZ, Hong SJ. Mechanism of mitomycin-induced apoptosis in cultured corneal endothelial cells. Mol Vis. 2008;14:1705–1712.
22. Macdonald JM, Geroski DH, Edelhauser HF. Effect of inflammation on the corneal endothelial pump and barrier. Curr Eye Res. 1987;6(9):1125–1132. doi:10.3109/02713688709034885
23. McDermott ML, Swendris RP, Shin DH, Juzych MS, Cowden JW. Corneal endothelial cell counts after Molteno implantation. Am J Ophthalmol. 1993;115(1):93–96. doi:10.1016/S0002-9394(14)73530-5
24. Kaji Y, Oshika T, Usui T, Sakakibara J. Effect of shear stress on attachment of corneal endothelial cells in association with corneal endothelial cell loss after laser iridotomy. Cornea. 2005;24(8 Suppl):S55–S8. doi:10.1097/01.ico.0000178735.27674.52
25. Lim LS, Ho CL, Ang LP, Aung T, Tan DT. Inferior corneal decompensation following laser peripheral iridotomy in the superior iris. Am J Ophthalmol. 2006;142(1):166–168. doi:10.1016/j.ajo.2006.01.070
26. Soro-Martinez MI, Villegas-Perez MP, Sobrado-Calvo P, Ruiz-Gomez JM, Miralles de Imperial Mora-Figueroa J. Corneal endothelial cell loss after trabeculectomy or after phacoemulsification, IOL implantation and trabeculectomy in 1 or 2 steps. Graefes Arch Clin Exp Ophthalmol. 2010;248(2):249–256. doi:10.1007/s00417-009-1185-4
27. Kasahara M, Shoji N, Matsumura K. The influence of trabectome surgery on corneal endothelial cells. J Glaucoma. 2019;28(2):150–153. doi:10.1097/IJG.0000000000001128
28. Leahy KE, Madigan MC, Sarris M, Watson SL, McCluskey P, White AJ. Investigation of corneal endothelial changes post selective laser trabeculoplasty. Clin Exp Ophthalmol. 2018;46(7):730–737. doi:10.1111/ceo.13172
29. Yamamoto Y, Uno T, Joko T, Shiraishi A, Ohashi Y. Effect of anterior chamber depth on shear stress exerted on corneal endothelial cells by altered aqueous flow after laser iridotomy. Invest Ophthalmol Vis Sci. 2010;51(4):1956–1964. doi:10.1167/iovs.09-4280
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
Glaucoma Surgery and Ocular Blood Flow in Colour Doppler Imaging: Is There a Link?
Zarzecki M, Obuchowska I, Ustymowicz A, Konopińska J
Clinical Ophthalmology 2024, 18:49-60
Published Date: 6 January 2024
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
Effectiveness of Trabeculectomy in Primary Open-Angle Glaucoma with Low Preoperative Intraocular Pressure
Katayama H, Tojo N, Toyoda N, Hayashi A
Clinical Ophthalmology 2026, 20:586125
Published Date: 17 February 2026
Optimizing Filtration Surgery Procedures in African-Derived Populations: Trabeculectomy and Preserflo
Gazzard G, Kailani O, Muntasser H, Lim KS, Vig N, Yu J
Clinical Ophthalmology 2026, 20:570347
Published Date: 10 March 2026