Back to Journals » Clinical Ophthalmology » Volume 20
Optimizing Filtration Surgery Procedures in African-Derived Populations: Trabeculectomy and Preserflo
Authors Gazzard G ![]() , Kailani O, Muntasser H, Lim KS, Vig N, Yu J
, Kailani O, Muntasser H, Lim KS, Vig N, Yu J
Received 25 September 2025
Accepted for publication 19 February 2026
Published 10 March 2026 Volume 2026:20 570347
DOI https://doi.org/10.2147/OPTH.S570347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Gus Gazzard,1,2 Obeda Kailani,3,4 Hussameddin Muntasser,5 Kin Sheng Lim,4,6 Niten Vig,7 Jonathan Yu8
1Glaucoma Service, Moorfields Eye Hospital NHS Foundation Trust, London, UK; 2Glaucoma Service, UCL Institute of Ophthalmology, London, UK; 3Glaucoma Service, King’s Ophthalmology Research Unit, King’s College Hospital NHS Foundation Trust, London, UK; 4Glaucoma Service, King’s College London, London, UK; 5St. Paul’s Eye Unit, Liverpool University Hospital NHS Foundation Trust, Liverpool, UK; 6Glaucoma Service, Guy’s and St Thomas’ NHS Foundation Trust, London, UK; 7Glaucoma Service, Western Eye Hospital, Imperial College Healthcare NHS Trust, London, UK; 8Glaucoma Service, Manchester Royal Eye Hospital, Manchester, UK
Correspondence: Gus Gazzard, Glaucoma Service, Moorfields Eye Hospital, NHS Foundation Trust, London, EC1V 2PD, UK, Tel +4407973303149, Email [email protected]
Background: African-derived populations are disproportionately affected by primary open-angle glaucoma (POAG) and face increased risks of surgical failure due to anatomical and genetic factors. This report identifies challenges in glaucoma care and strategies to optimize surgical outcomes in patients from African-derived backgrounds.
Methods: Six UK-based consultant ophthalmic glaucoma surgeons with extensive experience in diverse patient populations convened to discuss challenges and key approaches for optimising glaucoma filtration surgery outcomes in African-derived populations. Their opinions were supplemented by published literature to propose tailored recommendations and address some of the known challenges in this important patient group.
Results: Surgical treatment of glaucoma among African-derived populations includes challenges such as Tenon’s thickness, variable wound healing, and an increased risk of scarring. Preoperatively, outcomes can be improved through patient education, counselling and ocular surface optimisation, including reduction of preservative exposure. Intraoperatively, surgeons may consider the use of general anaesthesia or conscious sedation in younger patients, higher or prolonged mitomycin C exposure tailored to individual risk, and separate closure of Tenon’s capsule and conjunctiva to reduce bleb failure. Proactive postoperative care should include intensified steroid regimens and 5-fluorouracil use when indicated.
Conclusion: These insights support the delivery of culturally informed, evidence-based glaucoma care tailored to patients from African-derived backgrounds. By adopting a personalised and proactive approach, healthcare professionals may achieve more consistent and favourable surgical outcomes in this high-risk group.
Keywords: PreserFlo MicroShunt, African-derived populations, glaucoma, trabeculectomy, mitomycin C, bleb morphology, postoperative care, surgical optimisation, efficacy
Introduction
Glaucoma, commonly associated with elevated intraocular pressure (IOP), causes progressive optic neuropathy and is the second leading cause of blindness in Europe.1,2 Primary open angle glaucoma (POAG), the most common subtype, affected about 53 million people aged 40–80 years globally in 2020, with numbers projected to rise to 76 million by 2040.3,4
To prevent visual impairment, national and international clinical guidelines from the National Institute of Health Care and Excellence (NICE), the European Glaucoma Society and the American Academy of Ophthalmology recommend laser trabeculoplasty, topical medications, and surgical procedures aimed at reducing IOP.2,3,5 Surgical options include trabeculectomy, a well-established procedure for reducing IOP. In recent times, evidence supporting less invasive procedures such as the PreserFlo MicroShunt (PFMS; InnFocus/Santen, Miami, FL, USA), have become well-established.6 The PFMS glaucoma drainage system is intended for reduction of IOP in eyes of patients with POAG where IOP remains uncontrollable while on maximum tolerated medical therapy and/or where glaucoma progression warrants surgery.7 Introduced in Europe in 2019, this biocompatible subconjunctival ab-externo device offers an alternative to trabeculectomy for patients whose medical treatments no longer control IOP.8,9 As the use of PFMS grows, clinical and anecdotal experiences highlight differences in surgical techniques compared with trabeculectomy, particularly in high-risk populations.6,9–12
Risk factors for all patients with POAG include older age, elevated IOP, a family history of glaucoma and ethnicity.2,3 It is well-documented that glaucoma disproportionally affects patients from African-derived backgrounds.2,13 Research has shown that people of African ancestry are not only at increased risk of being affected by glaucoma, but also likely to experience more advanced glaucoma, a greater progression of visual field loss, and visual impairment or even blindness.10,14,15 A genome-wide association study involving 11,275 people of African ancestry identified 46 loci out of 174 known unique risk loci associated with POAG.15
Despite advancements in surgical techniques, patients from African-derived backgrounds consistently experience lower surgical success rates following glaucoma surgery compared to White populations.8,14 In a retrospective case-controlled study involving African ancestry patients, trabeculectomy achieved a success rate of only 46% without additional medication, with nearly a third of procedures failing within a year.14 Lower success rates of glaucoma surgery among patients from African-derived backgrounds are attributed to a combination of factors such as younger patient age at surgery, low pre-operative visual acuity and genetic predisposition for increased post-operative scarring.14,16
Studies also suggest that African-derived populations tend to have smaller trabecular meshwork height, thus reducing outflow facility.17,18 Additionally, they often have a thinner central corneal thickness, potentially contributing to the development of POAG.17,19,20 Darker skin tones correlate with increased scarring, identified at the genetic level, requiring a proactive and aggressive postoperative treatment regimen to mitigate complications.21,22 Furthermore, patients from African-derived backgrounds often have thicker and more prominent Tenon’s tissue.23 This may risk more frequent postoperative obstruction to the subconjunctival outflow pathway if it is not immobilised in the correct anatomical position.
Socio-cultural differences can also contribute to treatment outcomes following glaucoma surgery in addition to the anatomical and genetic variations.14,16 African-derived populations encounter significant non-clinical barriers, including systemic healthcare inequalities and racial biases. A recent survey indicated that the majority of respondents from African-derived backgrounds experienced racism from healthcare professionals, potentially undermining trust and patient outcomes.24
In response to these challenges, a group of UK-based consultant ophthalmic surgeons convened at a workshop to identify challenges and exchange insights on glaucoma filtration surgery, including PFMS and trabeculectomy across preoperative, intraoperative, and postoperative stages among patients from African-derived backgrounds. This perspective represents the first structured consensus addressing perioperative optimisation in African-derived populations, that aims to highlight the panel’s experience and recommendations on the technical aspects of trabeculectomy and PFMS surgery and peri-operative care in this high-risk population specifically, and identify areas requiring improvement to bridge the gaps in current practice.
Methods
A two-step approach was used to develop this article.
Literature Review
First, a comprehensive literature review was conducted using PubMed and Google Scholar, to identify previous practices, clinical outcomes, and recent advancements in the management of glaucoma specifically affecting patients from African-derived backgrounds. PubMed and Google Scholar were systematically searched from 1 January 2015 to 1 January 2025 to identify relevant peer-reviewed articles. Search terms included: “glaucoma”, “African”, “trabeculectomy”, “Preserflo”, “filtration surgery”, and additional related keywords. Articles were initially screened based on title and abstract, and duplicates, non-English language studies, and studies involving non-human subjects were excluded (Figure 1). The remaining articles underwent full-text review to extract insights on clinical practices, treatment outcomes, complications, and specific management strategies. These insights informed and enriched the discussion topics explored during the expert workshop.
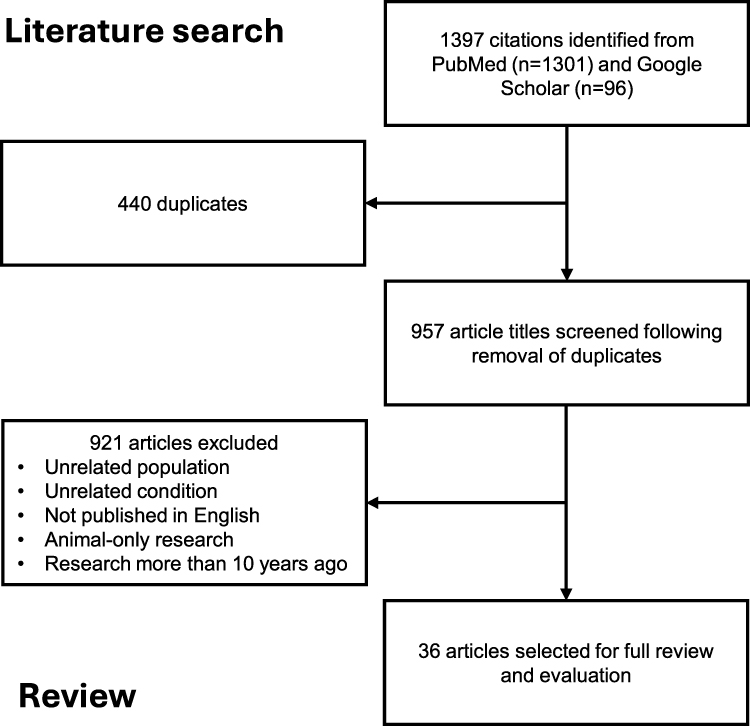 |
Figure 1 Literature analysis. |
Expert Panel Workshop
Secondly, a structured round-table discussion was convened involving six consultant ophthalmic surgeons based in the UK. The expert panel was selected based on a minimum of 20 years’ clinical experience in ophthalmology, a collective portfolio of over 200 peer-reviewed publications, and direct involvement in managing more than 2,000 patients of African-derived backgrounds undergoing glaucoma surgery. During the round-table meeting, moderated discussions explored barriers to effective glaucoma management, specific challenges related to surgical procedures and peri-operative management strategies tailored to African-derived populations. Expert opinions were sought on best practices, potential modifications to standard surgical techniques, and specific perioperative care recommendations. The discussion was audio-recorded and transcribed. The transcript was examined to identify recurring ideas, patterns or themes. Those themes were then combined into a clear descriptive summary of the expert panel’s shared conclusions or advice and thematically analysed to synthesise the collective recommendations. The resulting consensus recommendations from this meeting were integrated with findings from the literature review to inform practical guidance and optimise glaucoma surgical outcomes for patients from African-derived backgrounds, with particular focus on PFMS and trabeculectomy procedures.
Although the sponsors formally reviewed a penultimate draft, the opinions expressed are those of the authors and may not necessarily reflect those of the study sponsors. All co-authors approved the final version of the manuscript. Medical writing and/or editorial assistance was funded by Santen UK Ltd.
Results
The insights and recommendations presented in this section reflect the outcomes of the expert advisory board discussion, informed by both clinical experience and supporting literature in the context of treating patients from African-derived backgrounds with glaucoma. In the absence of robust comparative clinical trial data, the guidance presented reflects expert opinion integrated with the current evidence base.
Considerations for Glaucoma Filtration Surgery
Trabeculectomy remains the most performed surgical procedure for lowering IOP in glaucoma patients.25 Its efficacy in achieving low target pressures, especially in patients with advanced disease, is well-documented.25 The procedure also allows for postoperative flexibility, such as suture manipulation and bleb needling, to modulate outcomes.25 However, compared with PFMS surgery,26 trabeculectomy is associated with a high burden of postoperative management, increased risk of both early and late complications including bleb leaks, hypotony, and patient discomfort particularly due to the positioning and morphology of the bleb. These challenges are particularly pronounced in patients at high risk of surgical failure, such as those of African descent.
All surgeons agreed that PFMS can demonstrate several short-term advantages over trabeculectomy in the postoperative period.6,12 Based on the literature, stable IOP is often achieved sooner, leading to better early pressure outcomes than with trabeculectomy.27 Patients benefit from a more manageable intensity of follow-up, with fewer required visits (the surgeons typically schedule visits on Day 1, Week 1, Week 4, and Week 8 or 12), making postoperative care more economically predictable and logistically feasible for some patients.28 Additionally, PFMS is associated with fewer postoperative complications and improved visual comfort compared with trabeculectomy.26 Patients often experience quicker visual recovery with potentially reduced astigmatism.26 Whilst these latter points in particular would benefit all patients, they may be considered especially advantageous in younger patients such as those often seen in African-derived populations. In addition to clinical outcomes, resource utilisation and cost have been considered in other settings, with some cost analyses suggesting potential savings associated with PFMS compared with trabeculectomy.26
PFMS diverts aqueous humour and forms blebs more posteriorly than trabeculectomy.9,29 This posterior positioning has been quantified by anterior segment optical coherence tomography (OCT) imaging, which demonstrated a significantly greater distance from the limbus in PFMS blebs.29 Due to this difference in positioning, PFMS blebs are associated with fewer complications such as conjunctival cysts, which are more common in trabeculectomy blebs located closer to the limbus.29 PFMS blebs have also been shown to be more lower-lying, with a shallower episcleral lake than trabeculectomy blebs.29 This morphology likely contributes to a lower incidence of complications that can cause discomfort.29 Although the lower risk of sight threatening complications, such as bleb-related endophthalmitis from filtration surgery may be of more clinical impact. While further studies are needed to directly correlate these anatomical features with patient-reported outcomes, the reduction in discomfort and bleb-related complications is likely to be clinically meaningful and was consistently reported by the expert panel.
There had been initial reluctance among some surgeons to use PFMS in patients from African-derived backgrounds. Despite understanding that filtration surgery can be less effective in African-derived populations, many surgeons favour trabeculectomy due to their familiarity with the procedure, and the belief that it yields better outcomes. However, an increasing number of surgeons are gaining experience with PFMS in this patient population and observing results that are often comparable to those achieved with trabeculectomy.6,12 To optimise outcomes in these patients, it is crucial for surgeons to be confident not only in performing the PFMS procedure but also tailoring their approach to pre-, intra- and post-operative care.
Strategies and Approaches Preoperatively for Patients from African-Derived Backgrounds
The expert panel provided several tailored strategies aimed at optimising glaucoma surgical outcomes specifically for patients from African-derived backgrounds during the preoperative phase. These strategies focused on patient consent, education, ocular surface preparation, and specific surgical considerations, reflecting the need to address both clinical and non-clinical challenges, which are commonly observed within this patient population.
Patient Education and Communication
The consultant ophthalmic surgeons emphasised the important role of patient education, ensuring clear communication about potential postoperative scenarios to foster trust and strengthen the surgeon-patient partnership for all patients (Table 1). The expert panel suggested discussing scenarios such as “numerical” hypotony, defined as IOP below 6 mmHg without accompanying anatomical complications, that typically resolves spontaneously. Ensuring patients understand possible outcomes may help with managing their expectations and facilitating more open discussions about postoperative care, thereby potentially improving patient adherence to follow-up regimens.
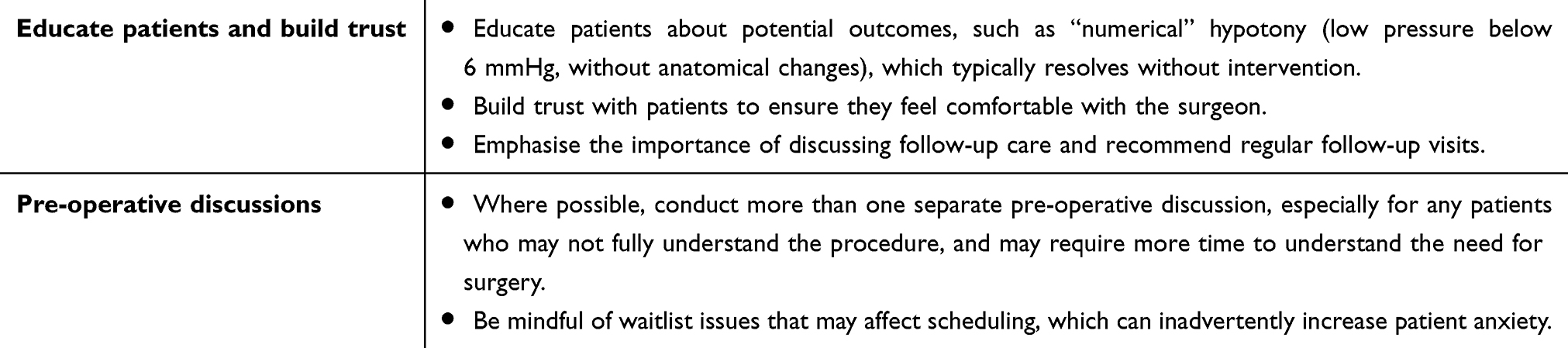 |
Table 1 Recommendations to Improve Consent and Education of Patients from African-Derived Backgrounds with Glaucoma |
Furthermore, the expert panel recommended conducting an additional preoperative consultation to address any concerns whenever possible and advised of the need to remain mindful of delays or issues with surgical scheduling, as prolonged waiting periods can inadvertently heighten patient anxiety.
Ocular Surface Optimisation
Optimising the ocular surface prior to surgery was highlighted to improve surgical outcomes (Table 2). Conjunctival inflammation, often exacerbated by topical medications, was identified as a significant risk factor for poorer outcomes in glaucoma filtration surgery. Therefore, it was recommended that medications causing inflammation should be discontinued at least two weeks before surgery, where feasible. Some experts also recommended switching patients to preservative-free medications in specific cases to further reduce ocular surface inflammation, although this practice lacks support from randomised controlled trials. Topical corticosteroids with limited intraocular penetration prescribed a week prior to surgery were also suggested as beneficial, although based on the literature, caution was advised due to the potential for steroid-induced IOP elevations in case of unexpected delays before surgery.28
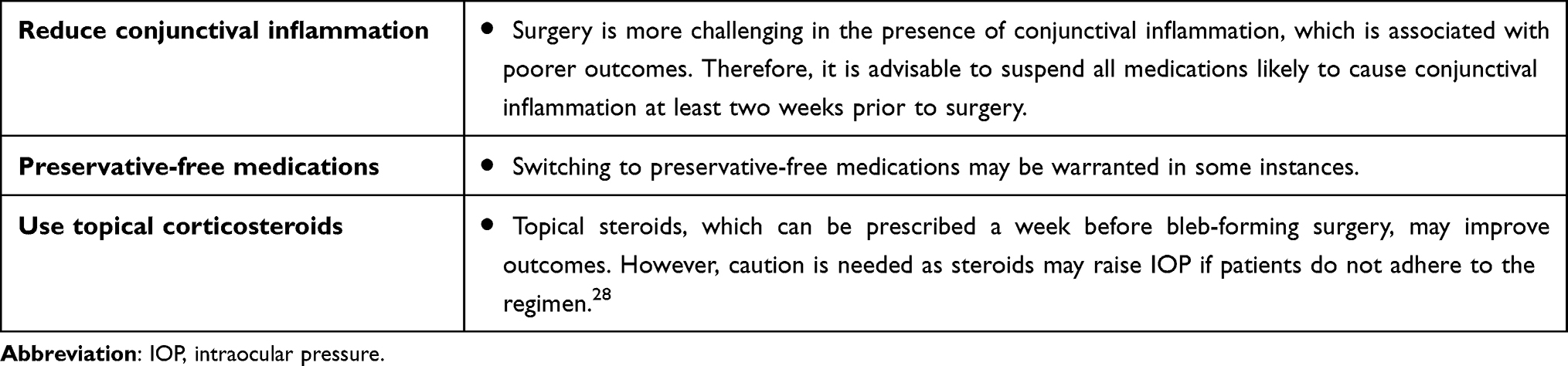 |
Table 2 Recommendations to Optimise the Ocular Surface in Preparation for Glaucoma Surgery in Patients from African-Derived Backgrounds |
Additional Pre-Surgical Considerations
Further presurgical considerations specific to patients from African-derived backgrounds were outlined (Table 3). It was recommended to avoid combining bleb-forming glaucoma surgeries with cataract surgery to reduce the risk of postoperative scarring. While the optimal interval between cataract surgery and filtration surgery remains uncertain, laser flare photometry studies indicate subclinical inflammation can persist beyond 30 days post-cataract surgery, potentially affecting the surgical success rates of subsequent glaucoma surgery.30 In contrast, the experts advised that performing surgery 3–6 months after a cataract operation generally avoids significant flare-ups. Therefore, carefully timing the sequence of procedures may enhance surgical outcomes.
 |
Table 3 Other Pre-Surgical Considerations to Take into Account in Patients from African-Derived Backgrounds with Glaucoma |
Intraoperative Strategies and Approaches
Intraoperative management of glaucoma surgery in African-derived populations requires particular attention to surgical planning and execution due to anatomical and clinical characteristics. Several strategies were identified by the expert panel, covering anaesthesia choice, bleeding control, use of mitomycin C (MMC), structural techniques, and adjunctive treatments.
Anaesthesia
Anaesthetic strategy is an important consideration in this population. Patients from African-derived backgrounds often present at a younger age, which may necessitate the use of general anaesthesia or conscious sedation to improve surgical conditions (Table 4). Furthermore, sickle cell disease is more prevalent in African-derived populations, and low oxygen tension can trigger red-cell sickling, so careful avoidance of peri-operative hypoxia is particularly important when operating in African-derived populations who may have undiagnosed sickle hemoglobinopathies.31
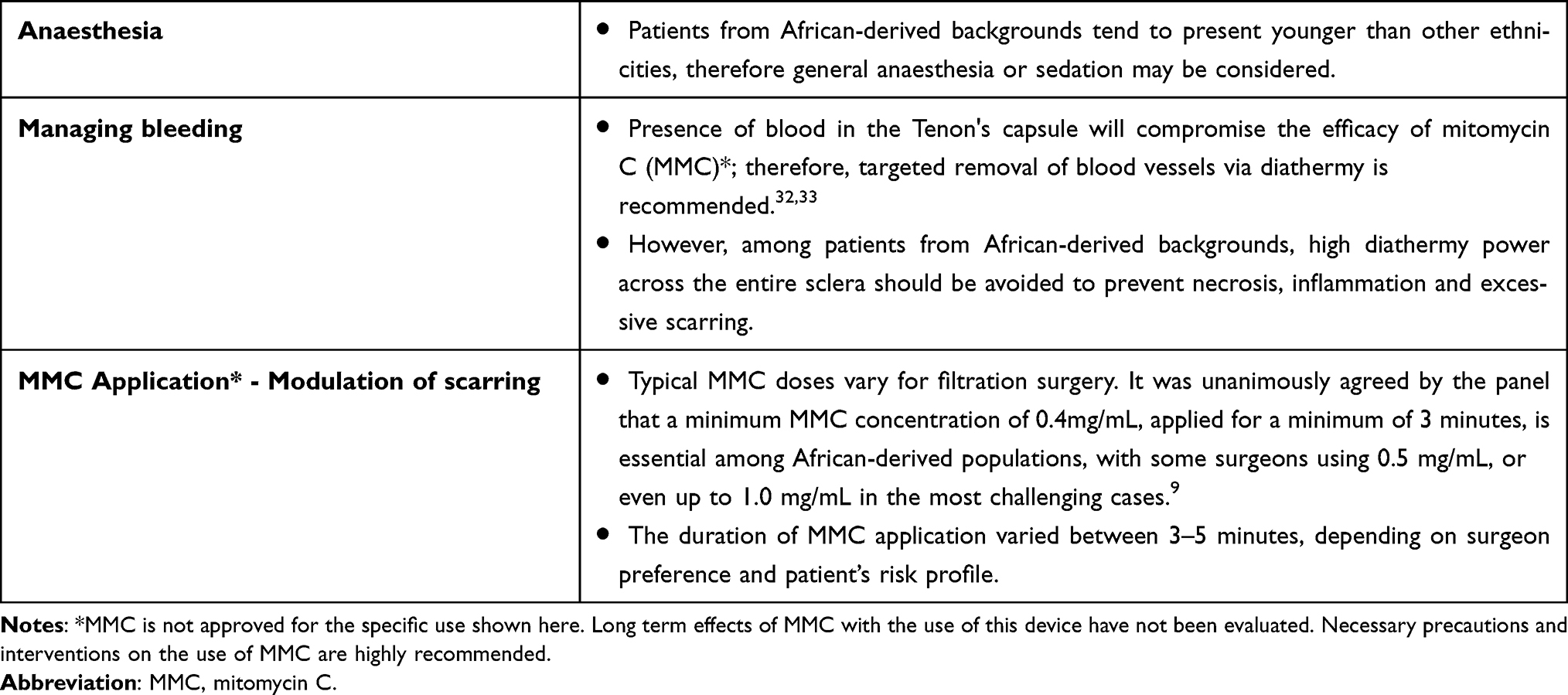 |
Table 4 Recommendations for Intraoperative Management in Patients from African-Derived Backgrounds Undergoing Glaucoma Surgery |
Intraoperative Haemostasis
Controlling bleeding during surgery is critical, especially since blood in the Tenon’s capsule can compromise the effectiveness of MMC. The surgeons recommended the use of targeted diathermy to remove blood vessels selectively. However, it was cautioned that high diathermy power across the entire sclera should be avoided due to increased risk of tissue necrosis, inflammation, and excessive postoperative scarring.32,33 The panel advised that liberal use of topical adrenalin perioperatively may significantly reduce bleeding. Furthermore, sympathomimetic agents, such as apraclonidine, can also be utilised for their vasoconstrictive properties, but their impact on pupillary mydriasis must be observed.
Use of Mitomycin-C
A minimum concentration of 0.4 mg/mL MMC applied for at least 3 minutes is commonly suggested, with application times ranging from 3 to 5 minutes based on individual patient risk profiles.9 In very high-risk or repeat surgical cases, one surgeon used MMC concentrations up to 1.0 mg/mL. However, there was no consensus on an upper level, with most using 0.4 mg/mL and two surgeons recommending 0.5 mg/mL.
Surgical Techniques
Techniques can also be adapted during surgery to the needs of patients from African-derived backgrounds (Table 5). In cases where stenting is used to prevent hypotony, the expert panel advised timely removal, usually within 1 to 3 weeks, as delayed removal may contribute to suboptimal bleb formation. This is particularly critical given the heightened risk of fibrosis and the risk of adverse bleb morphology in this population.
 |
Table 5 Recommendations Regarding Structural Techniques During Glaucoma Surgery in Patients from African-Derived Backgrounds |
Tenon’s capsule management was another area of focus. The surgeons emphasised the importance of locating and repositioning retracted Tenon’s tissue prior to conjunctival closure. In some cases, a two-layer closure technique – suturing the Tenon’s and conjunctiva separately, was preferred to ensure all Tenon’s tissue was secured, which might help reduce the incidence of limbal cystic blebs, postoperative scarring and bleb failure. There is limited evidence discussing Tenon excision in this population, but the panel’s experience supports Tenon preservation to achieve good posterior flow of aqueous humour and bleb formation. Furthermore, one surgeon advised that PFMS, compared with trabeculectomy, resulted in a low rate of bleb-related complications. However, subconjunctival injection of MMC may increase the risk.
Adjunctive Treatments
Adjunctive intraoperative medications were considered to support surgical outcomes (Table 6). Although the use of intracameral Avastin (bevacizumab) at the end of surgery remains off-label and only weakly supported by clinical evidence,34 two surgeons on the expert panel reported using it in high-risk patients, including patients from African-derived backgrounds, to potentially limit scarring. Orbital floor steroids were more widely accepted although not universally used for patients with poor compliance to topical treatments.
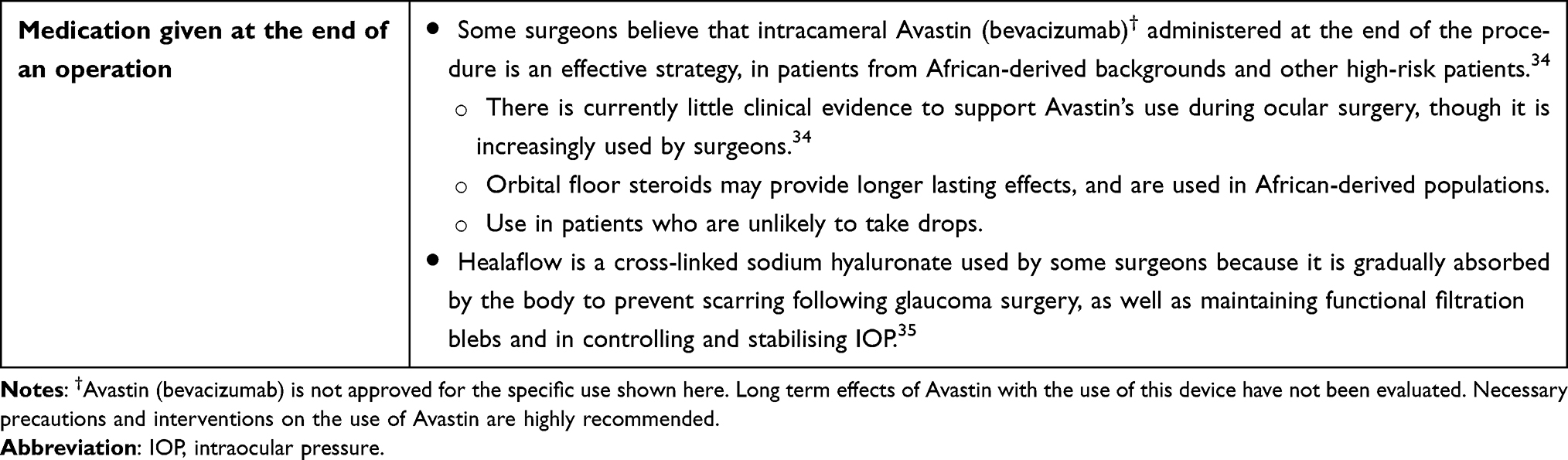 |
Table 6 Recommendations Regarding the Postoperative Transition Period After Glaucoma Surgery in Patients from African-Derived Backgrounds |
Healaflow, a cross-linked sodium hyaluronate gel, was used by one surgeon on the expert panel as a space-maintaining and anti-scarring agent. It is slowly absorbed and can support filtration bleb function while helping to stabilise IOP.35
These intraoperative adaptations may improve outcomes in African-derived populations who face higher surgical risks. Further research to validate the effectiveness of these tailored approaches is warranted, particularly for adjunctive agents like Avastin and Healaflow.34
Postoperative Considerations for African-Derived Populations
Several postoperative strategies were proposed by the expert panel to enhance postoperative outcomes in African-derived populations. (Table 7). A key recommendation was the implementation of very intensive steroid eye drop regimens aimed at suppressing the postoperative inflammatory response. The surgeons recommended initiating steroid drops as frequently as every 1–2 hours during the first postoperative week, followed by a gradual taper to six times daily over the following three weeks. For patients from African-derived backgrounds, the total duration of steroid therapy may be extended beyond the usual 3–4 months of standard practice, and in some cases, continuing for up to a year or longer at lower maintenance doses (eg, four times daily) to address the propensity for fibrotic healing in this population, particularly if pseudophakic.
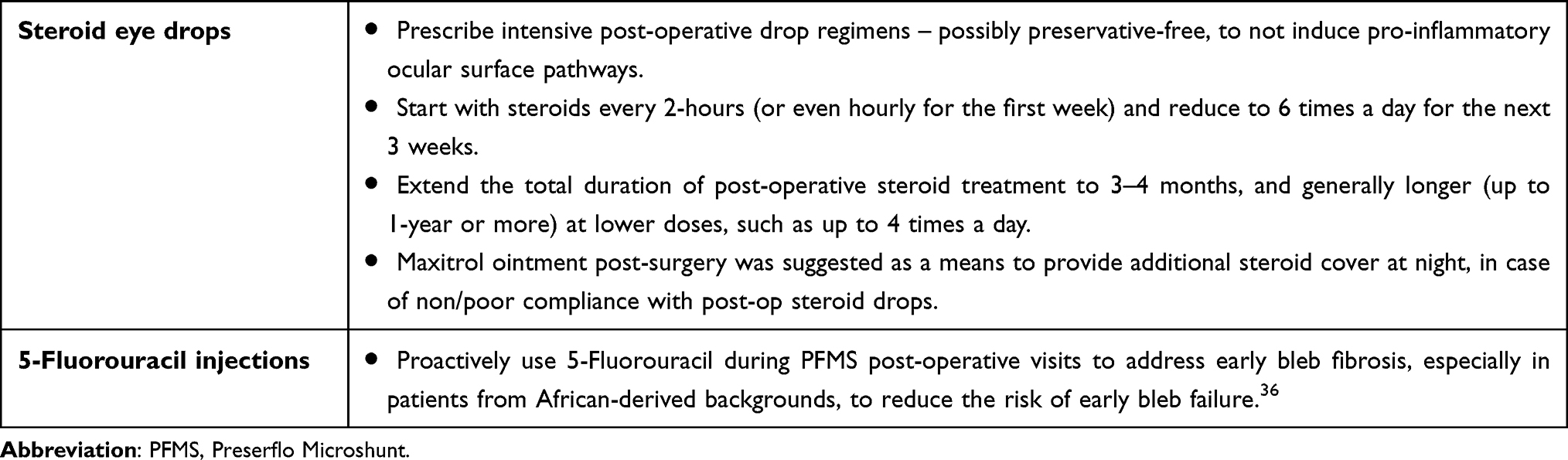 |
Table 7 Recommendations Regarding Pharmacological Treatments in Patients from African-Derived Backgrounds with Glaucoma |
A viscous ointment-based antibiotic-steroid combination was suggested by the panel as an additional overnight steroid delivery method to ensure continuous anti-inflammatory coverage during the healing period, although some surgeons restricted this to patients with suboptimal compliance to drop regimens. In addition to steroid therapy, the use of 5-fluorouracil injections during postoperative visits was endorsed by all experts.36 These injections were recommended to be used proactively in patients from African-derived backgrounds, rather than reactively, to prevent early bleb fibrosis. According to the literature early application of 5-fluorouracil can modulate fibroblast activity and improve the long-term success of bleb function by preventing excessive scarring at the filtration site.36
These pharmacological strategies aim to reduce the incidence of postoperative complications and improve long-term surgical success. Further studies are needed to determine the optimal duration and dosing of these treatments, specifically in African-derived populations.
Strengths and Limitations
A strength of this article is the use of expert consensus to provide clinically relevant guidance and offer practical insights in an area where population-specific evidence is only gradually expanding. However, reliance on expert opinion also represents a limitation in the absence of robust comparative clinical evidence evaluating surgical outcomes specifically in African-derived populations. These recommendations should therefore be viewed as provisional and highlight the need for more targeted, population-focused research. We also acknowledge that restricting the literature search to PubMed and Google Scholar may have excluded studies indexed in other databases, although these databases remain a comprehensive and widely used source for peer-reviewed ophthalmic research.
Conclusions
The primary goal of glaucoma surgery is to preserve patients’ vision, as untreated disease progression can ultimately lead to blindness. Glaucoma disproportionately affects patients from African-derived backgrounds, who face increased risks of disease progression and surgical failure due to genetic and anatomical factors, as highlighted by the expert panel and published evidence. The insights and experiences from the surgeons emphasise targeted surgical modification, intensified anti-scarring strategies, and proactive postoperative management including a prolonged topical steroid regimen, and 5-fluorouracil injections to suppress fibrosis to achieve favourable surgical outcomes in this high-risk group. In conclusion, by implementing carefully adapted strategies in this population, healthcare professionals may achieve better surgical success and improve the overall health of their patients when performing glaucoma filtration surgery procedures.
Data Sharing Statement
This publication does not include datasets, therefore there are no additional data for distribution.
Acknowledgments
Medical writing support was provided by Szonja Spanyol BSc, and Sara Shaw PhD CMPP of Mearns & Pike, funded by Santen UK Ltd, according to Good Publication Practice guidelines.37 The responsibility for opinions, conclusions, and data interpretation lies with the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funding for this research was provided by Santen UK Ltd.
Disclosure
Gus Gazzard is a consultant for Alcon Laboratories, Allergan, AbbVie, Balance, Belkin Vision, Ciliatech, Equinox, Essential Pharma, Genentech/Roche, Elios Vision, Glaukos, iStar Medical, Ivantis, McKinsey Consulting, Rayner Ltd, Reichert, Regeneron, Ripple Therapeutics, Santen, Sight Sciences, Thea Pharmaceuticals, Vialase, Visufarma, and Zeiss; reports fees for medical lectures with Alcon Laboratories, Allergan, AbbVie, Bausch & Lomb, Belkin Vision, Elios Vision, Glaukos, Haag-Streit Group; Lumenis, Lumibird, Quantel, Ellex Medical, Merck & Co, Reichert, Santen, Thea Pharmaceuticals, Vialase, Visufarma, and Zeiss; receives research support from Alcon Laboratories, Belkin Vision, Elios Vision, iStar Medical, Ivantis, Oertii, and Sight Sciences. Obeda Kailani is a consultant for Santen and Sight Sciences; and receives fees for medical lectures from Thea Pharmaceuticals. Kin Sheng Lim is a consultant for Santen; receives fees for medical lectures from Santen; and receives research grants from Santen, Thea Pharmaceuticals and Alcon. Hussameddin Muntasser reports honoraria from Santen. Niten Vig reports fees for medical lectures from Santen and Thea Pharmaceuticals. Jonathan Yu is a consultant for Santen and Sight Sciences; has lecture roles with Alcon and Bausch & Lomb; and reports fees for medical lectures from Santen. The authors report no other conflicts of interest in this work.
References
1. Glaucoma | health topics A to Z | CKS | NICE. Available from: https://cks.nice.org.uk/topics/glaucoma/.
2. BMJ Publishing Group Ltd. European glaucoma society terminology and guidelines for glaucoma, 5th Edition. Br J Ophthalmol. 2021;105(Suppl 1):1–11. doi:10.1136/bjophthalmol-2021-egsguidelines
3. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):71–150. doi:10.1016/j.ophtha.2020.10.022
4. Tham Y-C, Li X, Wong TY, Quigley HA, Aung T, Cheng C-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081–2090. doi:10.1016/j.ophtha.2014.05.013
5. Recommendations | glaucoma: diagnosis and management | guidance | NICE. 2017. Available from: https://www.nice.org.uk/guidance/ng81/chapter/recommendations#treatment.
6. Kuet M-L, Azuara-Blanco A, Barton K, King AJ. Will the PRESERFLO™ MicroShunt impact the future of trabeculectomy practice? A UK and Éire glaucoma society national survey. Eye. 2023;37(11):2252–2256. doi:10.1038/s41433-022-02326-6
7. NHS. PreserFlo MicroShunt information for use for glaucoma. 2025.
8. Jamke M, Herber R, Haase MA, Jasper CS, Pillunat LE, Pillunat KR. PRESERFLO ™ MicroShunt versus trabeculectomy: 1-year results on efficacy and safety. Graefes Arch Clin Exp Ophthalmol. 2023;261(10):2901–2915. doi:10.1007/s00417-023-06075-4
9. Armstrong JJ, De Francesco T, Ma J, Schlenker MB, Ahmed IIK. Ab externo SIBS microshunt with mitomycin C for open-angle glaucoma: three-year results as a primary surgical intervention. Ophthalmol Glaucoma. 2023;6(5):480–492. doi:10.1016/j.ogla.2023.04.002
10. Swampillai AJ, Nagar A, Sherman T, et al. Primary glaucoma surgery for African and African-Caribbean patients (PEACE): a pilot randomised controlled trial. Invest Ophthalmol Visual Sci. 2023;64(8):4278.
11. Zweifel LAB, Storp JJ, Vietmeier FE, et al. Preserflo MicroShunt versus trabeculectomy: efficacy and surgical success within a heterogenous patient cohort. Life. 2024;14(9):9. doi:10.3390/life14091171
12. Governatori L, Oliverio L, Mermoud A, et al. PreserFlo MicroShunt versus trabeculectomy: an updated meta-analysis and systematic review. Graefes Arch Clin Exp Ophthalmol. 2024;263:885–899. doi:10.1007/s00417-024-06649-w
13. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi:10.1136/bjo.2005.081224
14. Mamidipaka A, Shi A, Addis V, et al. Outcomes of trabeculectomy and predictors of success in patients of African ancestry with primary open angle glaucoma. J Glaucoma. 2025;34(2):127–135. doi:10.1097/IJG.0000000000002503
15. Verma SS, Gudiseva HV, Chavali VRM, et al. A multi-cohort genome-wide association study in African ancestry individuals reveals risk loci for primary open-angle glaucoma. Cell. 2024;187(2):464–480.e10. doi:10.1016/j.cell.2023.12.006
16. Bowman RJ, Kirupananthan S. How to manage a patient with glaucoma in Africa. Community Eye Health. 2006;19(59):38–39.
17. Zhang N, Wang J, Li Y, Jiang B. Prevalence of primary open angle glaucoma in the last 20 years: a meta-analysis and systematic review. Sci Rep. 2021;11(1):13762. doi:10.1038/s41598-021-92971-w
18. Chen RI, Barbosa DT, Hsu C-H, Porco TC, Lin SC. Ethnic differences in trabecular meshwork height by optical coherence tomography. JAMA Ophthalmology. 2015;133(4):437–441. doi:10.1001/jamaophthalmol.2014.5864
19. La Rosa FA, Gross RL, Orengo-Nania S. Central corneal thickness of Caucasians and African Americans in glaucomatous and nonglaucomatous populations. Arch Ophthalmol. 2001;119(1):23–27
20. Gordon MO, Beiser JA, Brandt JD, et al. The ocular hypertension treatment study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120(6):714–720. doi:10.1001/archopht.120.6.714
21. Klopot A, Baida G, Kel A, Tsoi LC, Perez White BE, Budunova I. Transcriptome analysis reveals intrinsic proinflammatory signaling in healthy African American skin. J Invest Dermatol. 2022;142(5):1360–1371.e15. doi:10.1016/j.jid.2021.09.031
22. Garg SP, Williams T, Taritsa IC, et al. Evaluating skin colour diversity in the validation of scar assessment tools. Wound Repair Regener. 2023;31(6):731–737. doi:10.1111/wrr.13120
23. Freedman J. Supra–tenon capsule placement of original molteno vs molteno 3 tube implants in black patients with refractory glaucoma: a single-surgeon experience. Arch Ophthalmol. 2011;129(8):993–997. doi:10.1001/archophthalmol.2011.183
24. Iacobucci G. Most black people in UK face discrimination from healthcare staff, survey finds. BMJ. 2022;378:o2337. doi:10.1136/bmj.o2337
25. Wagner FM, Schuster AK, Kianusch K, Stingl J, Pfeiffer N, Hoffmann EM. Long-term success after trabeculectomy in open-angle glaucoma: results of a retrospective cohort study. BMJ Open. 2023;13(2):e068403. doi:10.1136/bmjopen-2022-068403
26. Van Lancker L, Saravanan A, Abu-Bakra M, et al. Clinical outcomes and cost analysis of PreserFlo versus Trabeculectomy for glaucoma management in the United Kingdom. Ophthalmology Glaucoma. 2023;6(4):342–357. DOI:10.1016/j.ogla.2022.11.006
27. Gambini G, Carlà MM, Giannuzzi F, et al. Early post-operative anterior segment parameters modifications induced by PreserFlo MicroShunt in primary open-angle glaucoma. Int Ophthalmol. 2023;43(9):3035–3044. doi:10.1007/s10792-023-02697-z
28. Breusegem C, Spielberg L, Ginderdeuren RV, et al. Preoperative nonsteroidal anti-inflammatory drug or steroid and outcomes after trabeculectomy: a randomized controlled trial. Ophthalmology. 2010;117(7):1324–1330. doi:10.1016/j.ophtha.2009.11.038
29. Hasan SM, Theilig T, Meller D. Comparison of bleb morphology following PRESERFLO® MicroShunt and trabeculectomy using anterior segment. Diagnostics. 2023;13(21):3373. doi:10.3390/diagnostics13213373
30. Cagini C, Boni N, Bonifazi T, Fruttini D, Della Lena F, Contreras I. Efficacy and safety of PreserFlo MicroShunt implantation and its effects on intraocular inflammation through laser flare photometry. J Ophthalmol. 2024;2024(1):2447721. doi:10.1155/2024/2447721
31. Elendu C, Amaechi DC, Alakwe-Ojimba CE, et al. Understanding sickle cell disease: causes, symptoms, and treatment options. Medicine. 2023;102(38):e35237. doi:10.1097/MD.0000000000035237
32. Sakata R, Aihara M, Shirato S. Transient hyphema associated with PRESERFLO® MicroShunt surgery using a double-step knife in patients with glaucoma. Sci Rep. 2024;14(1):28457. doi:10.1038/s41598-024-80093-y
33. van Overdam KA, Kilic E, Verdijk RM, Manning S. Intra-ocular diathermy forceps. Acta Ophthalmol. 2018;96(4):420–422. doi:10.1111/aos.13619
34. Ramji S, Tan JCK, Jarrar ZA, Hamid S, Gazzard G, Ansari AS. Trabeculectomy augmented with anti-VEGF improves surgical outcomes in glaucoma: a systematic review and meta-analysis. Am J Ophthalmol. 2025;277:184–202. doi:10.1016/j.ajo.2025.05.005
35. Wu L, Liu J, Chang X, Zheng Y. The therapeutic effect of Healaflow in glaucoma surgery. Am J Transl Res. 2021;13(8):9729–9735.
36. The Fluorouracil Filtering Surgery Study Group. Fluorouracil filtering surgery study one-year follow-up. Am J Ophthalmol. 1989;108(6):625–635. doi:10.1016/0002-9394(89)90853-2
37. DeTora LM, Toroser D, Sykes A, et al. Good publication practice (GPP) guidelines for company-sponsored biomedical research: 2022 update. Ann Intern Med. 2022;175(9):1298–1304. doi:10.7326/M22-1460
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Statistical Analysis of Factors Affecting Surgically Induced Astigmatism Following Trabeculectomy
Shiratori N, Nakamoto K, Nishio Y, Takano Y, Arima T, Kunishige T, Suzuki H, Igarashi T, Takahashi H
Clinical Ophthalmology 2022, 16:3833-3839
Published Date: 21 November 2022
Glaucoma Surgery and Ocular Blood Flow in Colour Doppler Imaging: Is There a Link?
Zarzecki M, Obuchowska I, Ustymowicz A, Konopińska J
Clinical Ophthalmology 2024, 18:49-60
Published Date: 6 January 2024
Compared to Trabeculectomy, Ex-Press® Surgery Significantly Decreased the Loss of Corneal Endothelial Cell Density in Low-Intraocular-Pressure Glaucoma: 3-Year Follow-Up
Otsuka M, Tojo N, Yamazaki H, Ueda-Consolvo T, Hayashi A
Clinical Ophthalmology 2024, 18:3009-3015
Published Date: 22 October 2024
Trends in Glaucoma Fellowship Surgical Experience
Creagmile J, Chen N, Yee P, Lin K, Fox A, Smith A, Kwan C, Mosaed S
Clinical Ophthalmology 2025, 19:2719-2727
Published Date: 12 August 2025
Safety and Efficacy of Preserflo Microshunt in Different Subtypes of Glaucoma
Al Habash A, Alshaibani AK
Clinical Ophthalmology 2025, 19:3215-3226
Published Date: 4 September 2025