Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Comparison of High-Flow Nasal Cannula with Conventional Oxygen Therapy in Patients with Hypercapnic Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Authors Zhang L ![]() , Wang Y
, Wang Y ![]() , Ye Y, Gao J, Zhu F, Min L
, Ye Y, Gao J, Zhu F, Min L
Received 29 January 2023
Accepted for publication 30 April 2023
Published 16 May 2023 Volume 2023:18 Pages 895—906
DOI https://doi.org/10.2147/COPD.S402506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Lisha Zhang,1,* Yuxiu Wang,2,* Yaokun Ye,2 JunYin Gao,2 Fabei Zhu,1 Lingfeng Min2
1Department of Respiratory and Critical Care Medicine, The Yangzhou School of Clinical Medicine, Dalian Medical University, Yangzhou City, Jiangsu Province, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, Clinical Medical College, Yangzhou University, Yangzhou City, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lingfeng Min, Department of Respiratory and Critical Care Medicine, Clinical Medical College, Yangzhou University, Yangzhou City, Jiangsu Province, People’s Republic of China, Tel +86 19962595724, Email [email protected]
Purpose: This study aimed to evaluate the clinical outcomes of high-flow nasal cannula (HFNC) compared with conventional oxygen therapy (COT) in patients with hypercapnic chronic obstructive pulmonary disease (COPD), including arterial partial pressure of carbon dioxide (PaCO2), arterial partial pressure of oxygen (PaO2), respiratory rate (RR), treatment failure, exacerbation rates, adverse events and comfort evaluation.
Patients and Methods: PubMed, EMBASE and the Cochrane Library were retrieved from inception to September 30, 2022. Eligible trials were randomized controlled trials and crossover studies comparing HFNC and COT in hypercapnic COPD patients. Continuous variables were reported as mean and standard derivation and calculated by weighted mean differences (MD), while dichotomous variables were shown as frequency and proportion and calculated by odds ratio (OR), with the 95% confidence intervals (Cl). Statistical analysis was performed using RevMan 5.4 software.
Results: Eight studies were included, five with acute hypercapnia and three with chronic hypercapnia. In acute hypercapnic COPD, short-term HFNC reduced PaCO2 (MD − 1.55, 95% CI: − 2.85 to − 0.25, I² = 0%, p < 0.05) and treatment failure (OR 0.54, 95% CI: 0.33 to 0.88, I² = 0%, p< 0.05), but there were no significant differences in PaO2 (MD − 0.36, 95% CI: − 2.23 to 1.52, I² = 45%, p=0.71) and RR (MD − 1.07, 95% CI: − 2.44 to 0.29, I² = 72%, p=0.12). In chronic hypercapnic COPD, HFNC may reduce COPD exacerbation rates, but there was no advantage in improving PaCO2 (MD − 1.21, 95% CI: − 3.81 to 1.39, I² = 0%, p=0.36) and PaO2 (MD 2.81, 95% CI: − 1.39 to 7.02, I² = 0%, p=0.19).
Conclusion: Compared with COT, short-term HFNC reduced PaCO2 and the need for escalating respiratory support in acute hypercapnic COPD, whereas long-term HFNC reduced COPD exacerbations rates in chronic hypercapnia. HFNC has great potential for treating hypercapnic COPD.
Keywords: nasal high-flow oxygen therapy, conventional oxygen therapy, hypercapnia, chronic obstructive pulmonary disease, meta-analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is a worldwide cause of morbidity and mortality with a growing burden.1 The progression of COPD leads to hypercapnic respiratory failure, which is thought to be associated with exacerbation recurrence, poor disease prognosis, and high mortality.2 Noninvasive ventilation (NIV) can reduce the partial pressure of carbon dioxide in hypercapnic COPD patients; however discomfort and intolerance limit its widespread application.3
Therefore, conventional oxygen therapy (COT) is still the main method of respiratory support,4 but the maximum oxygen flow rate it can provide is limited. Previous study has reported a high risk of intubation and invasive mechanical ventilation (IMV) in acute mild acidosis COPD patients treated with COT.5 In addition, despite improved survival in COPD when treated with long-term oxygen therapy (LTOT), life expectancy is limited when accompanied by comorbidities and hypercapnia.6 Therefore there is a need to seek alternative strategies.
The high-flow nasal cannula (HFNC) is a new respiratory support technique that provides heated, humidified gas with adjustable oxygen fraction through a special large-bore nasal cannula, with a maximum flow rate of 60 liters per minute (L/min).7 The main mechanisms of HFNC include creating a low level of positive end-expiratory pressure (PEEP), washing out of nasopharyngeal dead space, decreasing inspiratory effort, and improving airway clearance.7 In the acute setting, short-term use of HFNC has been found to decrease respiratory rate (RR) and tissue carbon dioxide, and increase tidal volume in COPD patients compared to COT.8 HFNC has also been shown to reduce inspiratory effort and improve lung volume and compliance in patients with acute hypoxic respiratory failure.9 A meta-analysis found that HFNC reduced the risk of intubation or escalation of oxygen therapy for acute hypoxemic respiratory failure compared to COT.10 In the chronic setting, long-term HFNC are thought to enhance pulmonary mucosal cilia function and improve secretion clearance, primarily through humidification.2 A randomized controlled trial reported that long-term adjunct HFNC therapy reduced exacerbations and hospital readmission in COPD patients with hypoxic failure treated with LTOT.11
However, the effect of HFNC on physiological indicators and clinical outcomes in COPD patients with hypercapnia remains uncertain. A previous meta-analysis showed no statistic differences in arterial partial pressure of carbon dioxide (PaCO2) and arterial partial pressure of oxygen (PaO2) between the HFNC and COT.12 However, it only included four studies, and only half of patients being hypercapnia. After this, several studies with larger sample sizes were published,2,4,13,14 but findings were inconsistent. Therefore, we sought to perform a systematic review and meta-analysis, including recent data, to assess the role of HFNC in hypercapnic COPD compared to COT.
Material and Methods
The review protocol was registered at PROSPERO (CRD42022372244) and reported according to the PRISMA guidelines.15
Search Strategies
We conducted a systematic search of PubMed, EMBASE and the Cochrane Library from inception to September 30, 2022. A retrospective search was also performed on March 24, 2023. The references of relevant articles were also further reviewed to avoid missing any studies. The comprehensive search strategy included the following Medical Subject Headings (MeSH) terms and keywords: chronic obstructive pulmonary disease, COPD, High Flow Oxygen, High-Flow Nasal Cannula, High-flow nasal oxygen therapy, High-Flow Nasal Cannula Oxygen Therapy, High flow oxygen therapy, and randomized controlled trials. There were no limitations on language. The detailed search strategies are presented in Appendix 1.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: (1) Population: The research populations were COPD patients with hypercapnia. (2) Intervention measures: HFNC was used in the experimental group, and COT was used in the control group. (3) Outcomes: PaCO2, PaO2, RR, treatment failure (defined as meet the criteria for NIV or IMV), exacerbation rates, adverse events, and comfort evaluation. If multiple time points reported, we used the data of 24 hours after randomization for acute patients and longest available for chronic patients. (4) Study design: randomized controlled studies and crossover studies.
Exclusion criteria were as follows: (1) Patients younger than 18 years old. (2) Abstract publications, conference presentations, case reports, editorials or reviews. (3) Studies with incomplete data, which could not be extracted and included for synthesized analysis.
Two investigators independently screened the titles, abstracts, and full texts to determine eligible articles. Any disagreements were resolved by consensus with a third author.
Data Extraction
Two investigators independently extracted the relevant data and information from the eligible studies including authors, publication year, country, study design, sample size, hypercapnia type, interventions, controls, flow rate of HFNC, baseline of PH, PaCO2 and PaO2, outcomes and follow-up duration. Any disagreements were resolved through discussion or evaluation with a third author.
Quality Assessments
Two independent investigators evaluated the quality of included studies using Cochrane’s risk of bias assessment tool,16 including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of related outcomes assessment, incomplete outcome data, selective reporting bias, and other potential biases. Any disagreement was resolved through discussion or evaluation with a third author.
Statistical Analyses
Data for continuous variables were reported as mean and standard derivation (SD) and calculated by weighted mean differences (MD) with the 95% confidence intervals (CIs), while dichotomous variables were shown as frequency and proportion and calculated by odds ratio (OR) with the 95% CIs. If means and SD were not provided, we were estimated according to methods from Luo and Wan.17,18 Heterogeneity between studies was evaluated using the χ²-based Q test and quantified by using the I² test, with a significance value of at P<0.10 or I²≥50% respectively.19 If there was no significant heterogeneity, a fixed model was used; otherwise, a random model was used. Publication bias assessment and sensitivity analyses was not performed due to the limited number of studies (below 10) included in each analysis. Statistical analysis was performed using RevMan 5.4 software. P < 0.05 was considered to be statistically significant.
Results
Selected Studies and Characteristics
We identified 425 studies in our initial literature search, as shown in Figure 1. After duplicate studies (n = 141) and irrelevant topics (n = 244) were removed, forty potentially relevant literature were reserved. Eventually, eight studies were included in our meta-analysis.2,4,13,14,20–23
 |
Figure 1 Flow diagram of the study selection. |
The characteristics of the included studies and patients are shown in Table 1 and Table 2 respectively. A total of 1006 patients were included in our study, of which 488 patients treated with HFNC and 518 patients treated with COT. Five of the studies were of patients with acute hypercapnic COPD receiving HFNC for a short period of time (ranging from 30 minutes to several days),4,13,14,20,23 while three focused on patients with stable hypercapnia receiving HFNC for a long period of time (ranging from 6 weeks to 12 months).2,21,22
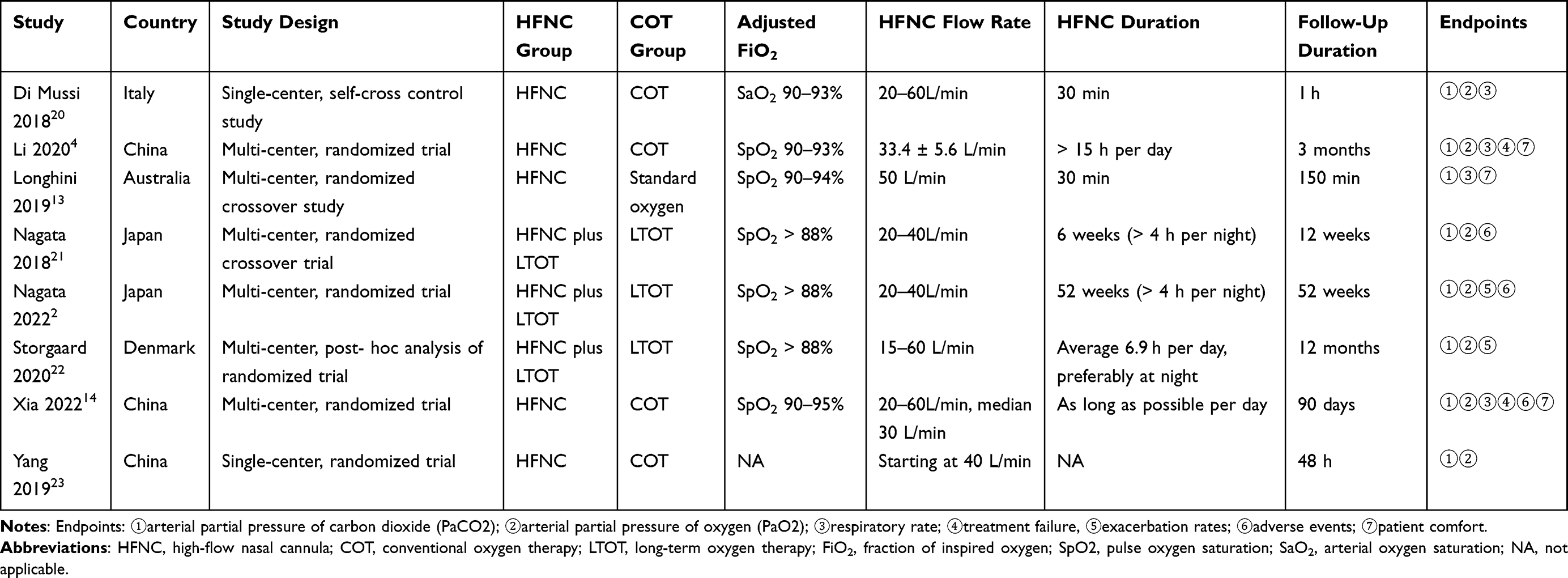 |
Table 1 Characteristic of Included Studies |
 |
Table 2 Characteristics of Patients in the Included Studies |
Quality Assessment
The results of the quality assessment are shown in Figure 2. All trials were at high risk of performance bias as blinding of patients to treatment assignment was not possible. Since most of the outcome indicators are objective, they would not have a significant impact on outcomes even if the patients were not blinded. With the exception of this field, one study was deemed to have a high risk of bias,20 and the remaining studies were considered to have a low or unclear risk of bias.
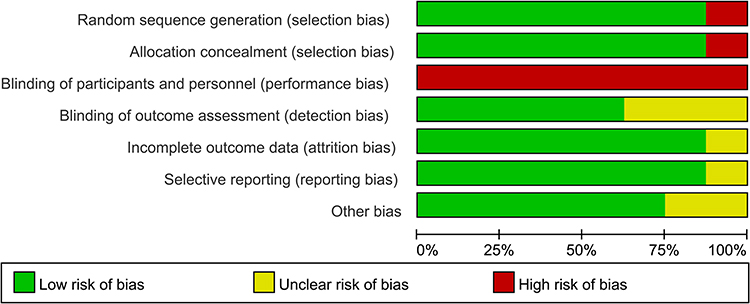 |
Figure 2 Quality assessment of bias graph. |
Outcome Analysis
PaCO2
Eight studies compared PaCO2,2,4,13,14,20–23 five of them concerning patients with acute hypercapnia COPD,4,13,14,20,23 and three on chronic hypercapnia.2,21,22 In acute patients, there was no heterogeneity among studies (I² = 0%, Q test P=0.49), so the fixed-effect model was used. Compared to COT, PaCO2 was lower in HFNC group (MD −1.55, 95% CI: −2.85 to −0.25, Z = 2.34, p =0.02), as shown in Figure 3A.
 |
Figure 3 Forest plot of PaCO2, (A) acute hypercapnia, (B) chronic hypercapnia. |
In chronic patients, there was no heterogeneity among studies (I² = 0%, Q test P=0.96), so the fixed-effect model was used. We observed no significant difference between the two groups in PaCO2 (MD −1.21, 95% CI: −3.81 to 1.39, Z = 0.91, p =0.36), as shown in Figure 3B.
PaO2
Seven studies compared PaO2,2,4,14,20–23 of which four concerning acute hypercapnia COPD patients,4,14,20,23 and three for chronic patients.2,21,22 In acute patients, there was no heterogeneity between the studies (I² = 45%, Q test P=0.14), so the fixed-effect model was used. Meta-analysis showed no statistical difference between HFNC and COT in terms of improvement in PaO2 (MD −0.36, 95% CI: −2.23 to 1.52, Z = 0.37, p=0.71), as shown in Figure 4A.
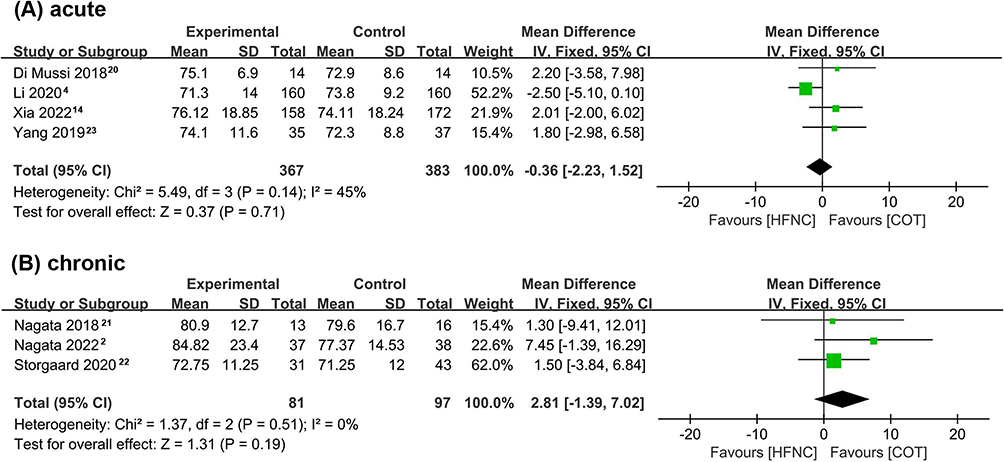 |
Figure 4 Forest plot of PaO2, (A) acute hypercapnia, (B) chronic hypercapnia. |
In chronic patients, there was no heterogeneity between the studies (I² = 0%, Q test P=0.51). Similarly, fixed-effects models showed no differences in PaO2 between the two groups (MD 2.81 95% CI: −1.39 to 7.02, Z =1.31, p=0.19), as shown in Figure 4B.
RR
Four studies about acute hypercapnia compared the RR.4,13,14,20 There was heterogeneity (I² = 72%, Q test P=0.01), so the random effect model was used. Meta-analysis showed no statistical difference between the two groups (MD −1.07, 95% CI: −2.44 to 0.29, Z = 1.54, p=0.12), as shown in Figure 5.
 |
Figure 5 Forest plot of respiratory rate. |
Treatment Failure
Two studies about acute hypercapnic COPD reported data on treatment failure.4,14 To obtain an accurate number of patients who met the criteria for escalation of ventilation, we excluded patients who received NIV due to intolerance. There was no heterogeneity (I² = 0%, Q test P=0.48), so the fixed effect model was used. The pooled results showed a lower rate of treatment failure in the HFNC group (OR 0.54, 95% CI: 0.33 to 0.88, Z = 2.48, p<0.05), as shown in Figure 6A.
 |
Figure 6 Forest plot of treatment failure in acute hypercapnia, (A) Treatment failure, (B) Actual upgraded to noninvasive ventilation. |
We also combined the results of the actual upgraded to NIV and found a lower proportion of patients in the HFNC group (OR 0.57, 95% CI: 0.35 to 0.94, Z = 2.23, p<0.05), as shown in Figure 6B. However, pooled analysis for IMV was not allowed due to the fact that only one study had patients experienced IMV and the number was too small,14 but the results showed no difference between the two groups (4/158 for HFNC group, 1/172 for COT group, p=0.198).
Exacerbation Rates
Two studies about chronic hypercapnic COPD compared exacerbation rates over one year.2,22 We were unable to pool the results because of different assessment methods. Storgaard reported that long-term HFNC stabilized the exacerbation rate, but COT did not.22 Specifically, compared with the year prestudy, the exacerbation rate for the control group increased by 2.2/year (P<0.001), while the HFNC group remained essentially stable with an increase of 0.15/year (p=0.661). Nagata’s study also showed that domiciliary HFNC can reduce moderate/severe COPD exacerbations,2 the adjusted ratios (95% CIs) of the mean exacerbation count in the COT group compared with that in the HFNC group was 2.85 (95% CIs 1.48–5.47, P =0.002).
Adverse Events
Three studies compared adverse events with insufficiently reported data,2,14,21 so we could only provide a description of their occurrence. In the studies by Xia and Nagata,14,21 no severe adverse events attributable to the randomized group occurred. In the study by Nagata,2 the most common adverse events in the HFNC/LTOT and LTOT groups were respiratory, thoracic, and mediastinal disorders (38.8% versus 42.0%), with no significant difference in the incidence between the two groups. Also, the overall incidence of severe adverse events was similar between the two groups (38.8% versus 32.0%).
Patient Comfort
Three studies compared comfort using different indicators.4,13,14 Two of the studies reported better comfort in the HFNC group,4,13 while one study found no difference between the two groups.14 The results from trials were summarized in Table S1.
Discussion
This systematic review and meta-analysis included eight studies to examine whether there were differences between HFNC therapy and COT in the treatment of hypercapnic COPD. In acute hypercapnic COPD, short-term HFNC reduced carbon dioxide retention and the need for higher respiratory support, but there were no significant differences in PaO2 and RR. In chronic hypercapnic COPD, HFNC may reduce COPD exacerbation rates, but there was no advantage in improving PaCO2 and PaO2.
A previous meta-analysis by Huang12 included four original studies and found no significant difference in PaCO2 reduction and PaO2 improvement between the HFNC and COT. Compared to it, our review focused on patients with hypercapnic COPD, included more studies and patients, evaluated more outcome indicators, and obtained different results.
Our study found that the effect of HFNC on PaCO2 was related to the duration of hypercapnia and the HFNC treatment period. In acute patients, short-term HFNC was more effective in reducing PaCO2 than COT. In fact, several randomized clinical studies have shown that the ability of HFNC to maintain PaCO2 was comparable to NIV in exacerbated COPD.24 Physiological studies have shown that HFNC can flush the upper airway and reduce anatomical dead space with the assistance of a positive airway pressure effect, allowing higher ventilation per minute to facilitate gas exchange.25 At the same time, HFNC also decreased inspiratory resistance and room air dilution effect by providing gas flow matching or higher than the peak inspiratory flow.25 Furthermore, HFNC could decrease neuroventilatory drive and work of breathing in COPD patients and alleviate muscle fatigue.20
However, in chronic patients, there was no significant difference in PaCO2 between long-term HFNC groups and COT groups. Persistent carbon dioxide retention leads to poor response of respiratory central chemoreceptors to carbon dioxide and patients become dependent on hypoxic drive, so a decrease in PaO2 may stimulate respiratory drive and reduce PaCO2.22 In the chronic hypercapnia studies we included, there was a tendency for PaO2 to decrease more in the COT group, which may be one of the explanatory mechanisms. Moreover, long-term follow-up may have reduced patient compliance and introduced other confounding factors, such as differences in prescribed medications and pulmonary rehabilitation. In fact, Nagata21 reported that when statistically controlling the time effect and allocation effect, the adjusted results showed lower PaCO2 in HFNC groups.
Our analysis found no statistical difference in PaO2 between the two groups, which requires further research. Sztrymf’s research has demonstrated the efficiency of HFNC in ameliorating oxygenation in patients with acute respiratory failure.26 Proper management of fraction of inspired oxygen (FiO2) and PEEP is the key to maintain adequate oxygenation.27 The HFNC is capable of providing high gas flow rates, creating a certain amount of PEEP, and providing more stable FiO2 than low-flow oxygen delivery.27 Theoretically, it has an advantage over COT in terms of improving oxygenation. However, our pooled results in patients with acute hypercapnic COPD did not support this, probably for the following reasons. First, since the cannula is part of an open system, pharyngeal pressure is limited. Airway pressure increased as flow increased,27 but pressure remained below 3 cmH2O even at 60 L/min flow,28 which is far from adequate for comparison with NIV. In our included clinical studies, most patients received oxygen flow rates significantly lower than 60 L/min,4,13,14,23 so HFNC produced an even lower PEEP. Moreover, FiO2 was dynamically adjusted with oxygenation in our included studies, and both patients with different oxygen therapy could be maintained to arterial oxygen saturation (SaO2) or pulse oxygen saturation (SpO2) levels by adjusting FiO2.4,13,14,20 Although PaO2 levels were comparable in both groups after treatment, there was no hypoxic respiratory failure in either group, indicating the potential benefit of HFNC in improving oxygenation.
In patients with chronic hypercapnia, our pooled results showed that the ability of HFNC to stabilize PaO2 is comparable to COT. There may be other explanations than the above mechanism. COPD patients have persistent inflammatory reactions in the airways, pulmonary parenchyma and pulmonary vessels, resulting in repeated airway remodeling, parenchymal destruction and pulmonary vessels abnormalities that contribute to a decrease in pulmonary gas exchange ability.29 These histopathological changes accumulate over the long-term duration of the disease and are difficult to reverse with HFNC treatment. Furthermore, the three included studies were designed to use HFNC mainly at night,2,21,22 but blood gas measurements were mostly evaluated in the daytime,2,21 several hours after HFNC cessation, which may lead to an underestimation of improvement in physiological parameters.
Similarly, RR was comparable between the two groups. Previous studies have found that HFNC can significantly reduce RR compared with COT in patients with dyspnea or acute respiratory failure,30,31 but the baseline RR in these studies was rapid, reaching 32–33.4 breaths/min compared to 21 breaths/min in our study. The mechanism is likely to be a reduction in anatomical dead space with HFNC, which resulting in improved ventilation and perfusion matching.32 However, given the high heterogeneity of pooled results, we need to be cautious and more original studies were required.
The need for treatment escalation is the main indicator to evaluate the treatment outcome of acute hypercapnic COPD patients. Our study found that HFNC reduced the need for escalated respiratory support, which is consistent with the study by Rochwerg10 in patients with acute hypoxic respiratory failure. The physiological mechanisms of HFNC may underlie its clinical benefit. Increased HFNC flow rate gradually may reduce inspiratory effort and minute ventilation; improve pulmonary ventilation, dynamic compliance, and oxygenation,33 thus decreasing the rates of intubation or NIV secondary to hypoxia. In addition, HFNC decreased the risk of self-inflicted lung injury by more fully matching the patient’s respiratory flow requirements.10 However, it is noteworthy that in the study by Xia,14 the length of hospital stay and hospital costs were significantly higher in the HFNC group than those in the COT group, which they suggest may be related to the delayed escalation of NIV in HFNC group. Therefore, we recommend that HFNC should be fully evaluated by experienced clinicians and that treatment strategies should be adjusted in time for patients who fail to improve with HFNC treatment.
Exacerbation rates were the main indicator to evaluate the treatment outcome of stable hypercapnic COPD patients. Our study found that long-term HFNC reduces exacerbations rate in patients with hypercapnic COPD. Previous studies have indicated that exacerbation history is the most important determinant of frequent exacerbations of COPD and is associated with increased severity.34 Therefore, it is of great importance to reduce acute exacerbations of COPD. In COPD chronic care, HFNC improves mucociliary function and promotes secretion clearance by providing heated and humidified gas, which will prevent the occurrence of atelectasis and improve the ventilation-perfusion ratio.27 Also the humidified gas can reduce the chronic airway inflammatory response caused by mucosal dryness.27 Besides, HFNC can relieve ventilator fatigue,20,35 and has a have long-term effects promoting respiratory muscle recovery.35 The above mechanisms may explain the reduction of COPD exacerbation by HFNC, but further mechanistic studies are still needed.
Our meta-analysis has several limitations. First, due to the nature of the interventions applied, blinding of patients was not possible, so all studies were at high risk of performance bias, but all the outcome indicators we assessed were objective except for comfort. Second, the timing and duration of HFNC treatment, as well as the length of follow-up, varied between studies. Third, the number of included studies was too small and included crossover studies. We performed a retrospective search on March 24, 2023, no updated articles were found, but several registered or ongoing clinical trials were noted (NCT05497986, NCT04640948, and NCT04840706). Fourth, there was a lack of sufficient data to perform relevant subgroup analyses to identify specific beneficiaries of HFNC use. Fifth, the medical cost is an important factor influencing clinical application, but only one article reported the cost of treatment, and later studies should focus on the issue of cost.
Conclusions
Our systematic review and meta-analysis suggests that compared with COT, short-term HFNC reduced PaCO2 and the need for escalating respiratory support in acute hypercapnic COPD, whereas long-term HFNC reduced COPD exacerbations rates in chronic hypercapnia. HFNC has great potential for treating hypercapnic COPD. Further large-scale studies are needed to confirm our results and identify specific beneficiaries of HFNC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China [Grant numbers 81870033]; the Six Talent Peaks Project of Jiangsu Province [Grant number WSN-106]; the Medical Scientific Research Foundation of Jiangsu Province of China [Grant numbers QNRC2016340]; and the Foundation for High-level Talents during the 13th Five-year Plan Period of Yangzhou, China [Grant numbers ZDRC201866].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Khakban A, Sin DD, FitzGerald JM, et al. The projected epidemic of chronic obstructive pulmonary disease hospitalizations over the next 15 years. a population-based perspective. Am J Respir Crit Care Med. 2017;195(3):287–291. doi:10.1164/rccm.201606-1162PP
2. Nagata K, Horie T, Chohnabayashi N, et al. Home high-flow nasal cannula oxygen therapy for stable hypercapnic COPD: a randomized trial. Am J Respir Crit Care Med. 2022;206(11):1326–1335. doi:10.1164/rccm.202201-0199OC
3. Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure. Eur Respir J. 2017;50(2):1602426. doi:10.1183/13993003.02426-2016
4. Li X, Tang X, Wang R, et al. High-flow nasal cannula for chronic obstructive pulmonary disease with acute compensated hypercapnic respiratory failure: a randomized, controlled trial. Int J Chron Obstruct Pulmon Dis. 2020;15:
5. Disease CRGoNMVfCOP. Early use of non-invasive positive pressure ventilation for acute exacerbations of chronic obstructive pulmonary disease: a multicentre randomized controlled trial. Chin Med J. 2005;118(24):2034–2040.
6. Ringbaek TJ, Lange P. Trends in long-term oxygen therapy for COPD in Denmark from 2001 to 2010. Respir Med. 2014;108(3):511–516. doi:10.1016/j.rmed.2013.10.025
7. Rittayamai N, Phuangchoei P, Tscheikuna J, Praphruetkit N, Brochard L. Effects of high-flow nasal cannula and non-invasive ventilation on inspiratory effort in hypercapnic patients with chronic obstructive pulmonary disease: a preliminary study. Ann Intensive Care. 2019;9(1):122. doi:10.1186/s13613-019-0597-5
8. Fraser JF, Spooner AJ, Dunster KR, Anstey CM, Corley A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue carbon dioxide while increasing tidal and end-expiratory lung volumes: a randomised crossover trial. Thorax. 2016;71(8):759–761. doi:10.1136/thoraxjnl-2015-207962
9. Mauri T, Turrini C, Eronia N, et al. Physiologic effects of high-flow nasal cannula in acute hypoxemic respiratory failure. Am J Respir Crit Care Med. 2017;195(9):1207–1215. doi:10.1164/rccm.201605-0916OC
10. Rochwerg B, Granton D, Wang DX, et al. High flow nasal cannula compared with conventional oxygen therapy for acute hypoxemic respiratory failure: a systematic review and meta-analysis. Intensive Care Med. 2019;45(5):563–572. doi:10.1007/s00134-019-05590-5
11. Storgaard LH, Hockey HU, Laursen BS, Weinreich UM. Long-term effects of oxygen-enriched high-flow nasal cannula treatment in COPD patients with chronic hypoxemic respiratory failure. Int J Chron Obstruct Pulmon Dis. 2018;13:1195–1205. doi:10.2147/COPD.S159666
12. Huang X, Du Y, Ma Z, et al. High-flow nasal cannula oxygen versus conventional oxygen for hypercapnic chronic obstructive pulmonary disease: a meta-analysis of randomized controlled trials. Clin Respir J. 2021;15(4):437–444. doi:10.1111/crj.13317
13. Longhini F, Pisani L, Lungu R, et al. High-flow oxygen therapy after noninvasive ventilation interruption in patients recovering from hypercapnic acute respiratory failure. Crit Care Med. 2019;47(6):E506–E511. doi:10.1097/CCM.0000000000003740
14. Xia J, Gu S, Lei W, et al. High-flow nasal cannula versus conventional oxygen therapy in acute COPD exacerbation with mild hypercapnia: a multicenter randomized controlled trial. Crit Care. 2022;26(1):109. doi:10.1186/s13054-022-03973-7
15. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
16. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
17. Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
18. Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018;27(6):1785–1805. doi:10.1177/0962280216669183
19. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
20. Di Mussi R, Spadaro S, Stripoli T, et al. High-flow nasal cannula oxygen therapy decreases postextubation neuroventilatory drive and work of breathing in patients with chronic obstructive pulmonary disease. Crit Care. 2018;22(1):180. doi:10.1186/s13054-018-2107-9
21. Nagata K, Kikuchi T, Horie T, et al. Domiciliary high-flow nasal cannula oxygen therapy for patients with stable hypercapnic chronic obstructive pulmonary disease. A multicenter randomized crossover trial. Ann Am Thorac Soc. 2018;15(4):
22. Storgaard L, Hockey H, Weinreich U. Development in PaCO 2 over 12 months in patients with COPD with persistent hypercapnic respiratory failure treated with high-flow nasal cannula—post-hoc analysis from a randomised controlled trial. BMJ Open Respir Res. 2020;7(1):e000712. doi:10.1136/bmjresp-2020-000712
23. Yang S, Guizhen Z, Zhen L, et al. Effect of high-flow nasal cannula oxygen therapy on diaphragmatic function in patients with acute exacerbation of chronic obstructive pulmonary disease: a prospective randomized controlled trial. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2019;31(5):551–555. doi:10.3760/cma.j.issn.2095-4352.2019.05.006
24. Pisani L, Astuto M, Prediletto I, Longhini F. High flow through nasal cannula in exacerbated COPD patients: a systematic review. Pulmonology. 2019;25(6):348–354. doi:10.1016/j.pulmoe.2019.08.001
25. Roca O, Hernández G, Díaz-Lobato S, Carratalá JM, Gutiérrez RM, Masclans JR. Current evidence for the effectiveness of heated and humidified high flow nasal cannula supportive therapy in adult patients with respiratory failure. Crit Care. 2016;20(1):109. doi:10.1186/s13054-016-1263-z
26. Sztrymf B, Messika J, Bertrand F, et al. Beneficial effects of humidified high flow nasal oxygen in critical care patients: a prospective pilot study. Intensive Care Med. 2011;37(11):1780–1786. doi:10.1007/s00134-011-2354-6
27. Nishimura M. High-flow nasal cannula oxygen therapy in adults. J Intens Care. 2015;3(1):15. doi:10.1186/s40560-015-0084-5
28. Parke R, McGuinness S, Eccleston M. Nasal high-flow therapy delivers low level positive airway pressure. Br J Anaesth. 2009;103(6):886–890. doi:10.1093/bja/aep280
29. Lyu R, Wang W, Wang W, Liu N, Xiao J, Li X. Effect of humidified high-flow nasal cannula oxygen therapy on respiratory function recovery in stable COPD patients. Am J Transl Res. 2022;14(6):4074–4081.
30. Ruangsomboon O, Dorongthom T, Chakorn T, et al. High-flow nasal cannula versus conventional oxygen therapy in relieving dyspnea in emergency palliative patients with do-not-intubate status: a randomized crossover study. Ann Emerg Med. 2020;75(5):615–626. doi:10.1016/j.annemergmed.2019.09.009
31. Azoulay E, Lemiale V, Mokart D, et al. Effect of high-flow nasal oxygen vs standard oxygen on 28-day mortality in immunocompromised patients with acute respiratory failure: the HIGH randomized clinical trial. JAMA. 2018;320(20):2099–2107. doi:10.1001/jama.2018.14282
32. Fu C, Liu X, Zhu Q, et al. Efficiency of high-flow nasal cannula on pulmonary rehabilitation in COPD patients: a meta-analysis. Biomed Res Int. 2020;2020:7097243. doi:10.1155/2020/7097243
33. Mauri T, Alban L, Turrini C, et al. Optimum support by high-flow nasal cannula in acute hypoxemic respiratory failure: effects of increasing flow rates. Intensive Care Med. 2017;43(10):1453–1463. doi:10.1007/s00134-017-4890-1
34. Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. doi:10.1056/NEJMoa0909883
35. Chen YH, Huang CC, Lin HL, Cheng SL, Wu HP. Effects of high flow nasal cannula on exercise endurance in patients with chronic obstructive pulmonary disease. J Formosan Med Assoc. 2022;121(1 Pt 2):381–387. doi:10.1016/j.jfma.2021.05.018
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Feng Z, Zhang L, Yu H, Su X, Shuai T, Zhu L, Chen D, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1987-1999
Published Date: 30 August 2022
Clinically Important Deterioration (CID) and Ageing in COPD: A Systematic Review and Meta-Regression Analysis According to PRISMA Statement
Manzetti GM, Ora J, Sepiacci A, Cazzola M, Rogliani P, Calzetta L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2225-2243
Published Date: 10 October 2023
Efficacy and Safety of Bisoprolol in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Feng Z, Zhang L, Wang Y, Guo H, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:3067-3083
Published Date: 23 December 2023
Comparison of the Application of Vibrating Mesh Nebulizer and Jet Nebulizer in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta‐analysis
Feng Z, Han Z, Wang Y, Guo H, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:829-839
Published Date: 28 March 2024
Impact of High-Flow Nasal Cannula for Chronic Obstructive Pulmonary Disease Exacerbation: A Systematic Review of Clinical and Physiological Outcomes
Al Nufaiei ZF, Hakeem JZ
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:593501
Published Date: 14 July 2026