Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Clinically Important Deterioration (CID) and Ageing in COPD: A Systematic Review and Meta-Regression Analysis According to PRISMA Statement
Authors Manzetti GM ![]() , Ora J
, Ora J ![]() , Sepiacci A, Cazzola M
, Sepiacci A, Cazzola M ![]() , Rogliani P
, Rogliani P ![]() , Calzetta L
, Calzetta L ![]()
Received 15 June 2023
Accepted for publication 1 October 2023
Published 10 October 2023 Volume 2023:18 Pages 2225—2243
DOI https://doi.org/10.2147/COPD.S396945
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Gian Marco Manzetti,1 Josuel Ora,1 Arianna Sepiacci,1 Mario Cazzola,1 Paola Rogliani,1 Luigino Calzetta2
1Department of Experimental Medicine, Unit of Respiratory Medicine, University of Rome “Tor Vergata”, Rome, Italy; 2Department of Medicine and Surgery, Respiratory Disease and Lung Function Unit, University of Parma, Parma, Italy
Correspondence: Luigino Calzetta, Department of Medicine and Surgery, Respiratory Disease and Lung Function Unit, University of Parma, Parma, Italy, Email [email protected]
Purpose: Clinically important deterioration (CID) is a composite endpoint developed to quantify the impact of pharmacological treatment in clinical trials for Chronic Obstructive Pulmonary Disease (COPD), also showing a prognostic value. CID is defined as any of the following condition: forced expiratory volume in 1 s decrease ≥ 100 mL from baseline, and/or St. George’s Respiratory Questionnaire total score increase ≥ 4-unit from baseline, and/or the occurrence of a moderate-to-severe exacerbation of COPD. Although most COPD patients experience a clinical worsening as they get older, to date, no specific studies assessed the correlation between ageing and CID in COPD. Therefore, the aim of this study was to investigate the impact of ageing on CID in COPD patients.
Patients and Methods: Data obtained from 55219 COPD patients were extracted from 17 papers, mostly post-hoc analyses. A pairwise meta-analysis and a meta-regression analysis were performed according to PRISMA-P guidelines to quantify the impact of pharmacological therapy on CID and to determine whether ageing might modulate the risk of CID in COPD patients.
Results: Inhaled treatments resulted generally effective in reducing the risk of CID in COPD (relative risk: 0.81, 95% confidence interval 0.79– 0.84; P < 0.001). The meta-regression analysis indicated a trend toward significance (P = 0.063) in the linear relationship between age and the risk of CID. Of note, age significantly (P < 0.05) increased the risk of CID when associated with lower post-bronchodilator FEV1. These results were not affected by a significant risk of bias.
Conclusion: This quantitative synthesis suggests that inhaled therapy is effective in reducing the risk of CID in COPD, although such a protective effect may be affected in older patients with impaired lung function. Further studies specifically designed on CID in COPD are needed to confirm these results.
Keywords: ageing, clinically important deterioration, chronic obstructive pulmonary disease, elderly, meta-analysis, inhaled therapy
Introduction
Chronic obstructive pulmonary disease (COPD) is defined by the latest Global Initiative for Chronic Obstructive Lung Disease (GOLD) report as a heterogeneous lung condition characterized by chronic respiratory symptoms and a persistent, often progressive, airflow obstruction.1 The need for a multi-dimensional approach, assessing lung function, acute exacerbations, and quality of life of COPD patients, led to the development of the composite clinically important deterioration (CID) endpoint in 2016.2 In its original formulation, a CID was defined as any of the following: a decrease of ≥100 mL from baseline in forced expiratory volume in 1 s (FEV1) and/or a ≥4-unit increase from baseline in St. George’s Respiratory Questionnaire (SGRQ) total score and/or the occurrence of a moderate-to-severe exacerbation of COPD (AECOPD). AECOPD was defined as an acute worsening of COPD symptoms requiring the use of additional treatment.2
The CID concept has proven itself as a reliable tool to quantify the impact of pharmacological treatment in several post-hoc analyses of randomized controlled trials (RCTs),3 overcoming the exclusive effect on FEV1, which might correlate weakly with patient reported outcomes (PRO).4 Throughout the years, the composite CID endpoint also showed a prognostic value5 and alternative definitions, including, among the others, the COPD Assessment test (CAT) score6 and the Transition Dyspnea Index (TDI),7 were developed.
COPD patients can experience a rather fast decline in lung function over the years, ranging from 33 to 66 mL/year in FEV1 according to different studies.8,9 However, this annual rate is below the 100 mL decrease considered by the original CID definition, which is indeed intended to be greater than the expected functional decline; for this reason, this value is considered the minimal clinically important difference (MCID) for FEV1 in COPD.10
According to the well-known Fletcher–Peto curve11 and to more recent retrospective evidence, the FEV1 decrease could accelerate with ageing.12 As a matter of fact, this trend can be identified also in healthy subjects, where the median FEV1 decline is 22.4 mL/year, ranging from 3 mL/year in the 40–49 years decade to 34 mL/year in the 70–79 years decade, as reported by a recent systematic review.13
Likewise, older COPD patients have a higher risk of future AECOPD and a higher mortality for acute exacerbations,14,15 showing an age-related dysfunction of the immune system.16 Moreover, elderly COPD patients are more likely to suffer from comorbidities,17 that per se increase the risk of moderate and severe AECOPD.18
Conversely, ageing does not seem to affect health-related quality of life (HRQL) in COPD patients, since younger patients, aged 50–64 years, actually score higher in SGRQ than patients aged 65–80 years, probably due to a higher impact of dyspnea.19
Despite this evidence, to date, no specific studies have been carried out to assess the correlation between ageing and CID in COPD patients.
The meta-regression analysis is a statistical method which usually follows a traditional meta-analysis: on one hand, it is mainly used to identify possible confounding factors in a meta-analysis, on the other hand, meta-regression analysis can also be used as a tool to investigate if and how a specific variable, such as ageing, may modulate certain outcomes.20–23
Therefore, the aim of this systematic review and meta-regression analysis was to investigate the impact of ageing on CID in COPD patients, according to the current PRISMA statement.24
Materials and Methods
Search Strategy and Study Eligibility
This systematic review and meta-regression analysis was performed according to PRISMA-P guidelines.24 The PRISMA 2020 flow diagram is shown in Figure 1. The PRISMA-P checklist is reported in Table S1.24
 |
Figure 1 PRISMA 2020 flow diagram for the identification of the studies included in the systematic review. Abbreviation: PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses. Notes: PRISMA figure adapted from Page MJ, McKenzie JE et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.25 |
A comprehensive literature search was carried out for Phase III RCTs or post-hoc analyses of RCTs written in English and assessing CID in COPD patients.
The patient problem, intervention, comparison, and outcome (PICO) framework were used for the literature search.26 The “Patient problem” included COPD; the ‘Intervention’ regarded inhaled therapy; the ‘Comparison’ was performed vs placebo (PCB) or across different inhaled drugs; the ‘Outcome’ was the association between CID and ageing.
The search was performed in MEDLINE and Scopus to find relevant studies published up to February 9th, 2023.
The following search string was used in the database was: ((clinically important deterioration) OR CID) AND COPD. References of previous high-quality reviews were checked to identify further RCTs, if any.5
Eppi-Reviewer 4 (EPPI-Centre Software. London, UK) was used to manage data in literature and facilitate the collaboration across reviewers for the selection of the studies.
Study Selection
Phase III RCTs or post-hoc analyses of RCTs that analyzed CID in COPD patients were included in the systematic review and meta-regression analysis. Trials not including at least FEV1 decline, SGRQ increase, and AECOPD in the CID definition were excluded from the analysis. Two reviewers (GMM and LC) independently checked for study selection and any difference in opinion was resolved by consensus.
Data Extraction
Data from the Phase III or RCTs post-hoc analyses included in this systematic review and meta-regression analysis were extracted from journal articles, and/or Supplementary Data Files, and/or the ClinicalTrials.gov database.
Data were checked for reference, clinical trial ID, duration and characteristics of the study, number of analyzed patients, treatments administered including the doses of medications, regimen of administration, main inclusion criteria, age, gender, smoking habit, post-bronchodilator FEV1, AECOPD, SGRQ, COPD assessment test (CAT), modified medical research council dyspnea scale (mMRC), and Jadad Score.27
Data were extracted according to the DECiMAL recommendations.28 Cohen’s Kappa score was used to assess the inter- and intra-rater reliability for data abstraction (≥0.80: excellent agreement; ≥0.61 and <0.80: substantial agreement; ≥0.41 and <0.61 moderate agreement; <0.41 poor agreement).29
Endpoint
The primary endpoint of systematic review and meta-regression analysis was to assess the risk of CID according to ageing.
Data Synthesis and Analysis
A pairwise meta-analysis was carried out to quantify the risk of CID in COPD patients enrolled in RCTs. Obtained results were reported as relative risk (RR) and 95% confidence interval (95% CI).
A common effect size cannot be assumed because data were extracted from a series of studies performed by investigators operating independently. Therefore, the binary DerSimonian-Laird random-effects model was used to balance the study weights and correctly assess the effect estimates and relative 95% CI. Subgroup analyses were carried out according to specific inhaled treatments.
A meta-regression analysis via random-effect method was also performed to investigate whether ageing, alone or in association with other potential effect modifiers, might modulate the risk of CID in COPD. The meta-regression analysis was carried out by plotting the outcome variables obtained from the pairwise meta-analysis with the explanatory variables reported in the included studies.20–23 The resulting regression coefficient indicates how strongly the explanatory variables may modify the effect induced by a specific treatment.22 The meta-regression analysis reports a positive or negative correlation between the effect estimates and the potential effect modifiers for statistically significant regression coefficient. In this study, meta-regression analysis was used to investigate the impact of ageing on CID.
Study Quality, Bias, and Quality of Evidence
The risk of bias for the included studies was quantified via Jadad score, ranging from 1 to 5 (score ≤2: low quality; score = 3: medium quality; score ≥4: high quality).27
Heterogeneity (I2) was assessed to analyze the between-study dissimilarity, as previously reported.20
Funnel plot and Egger’s test were performed to investigate the origin and risk of publication bias related to significant and/or substantial (I2>50%) level of heterogeneity if more than 10 studies were included in the meta-analysis.30–33
The quality of the evidence was assessed according to GRADE system (++++: high quality; +++: moderate quality; ++: low quality; +: very low quality).34
Two reviewers (GMM and LC) independently assessed the study quality, bias, and quality of evidence and any difference in opinion was resolved by consensus.
Software and Statistical Significance
Open-MetaAnalyst Was Used to Perform
The pairwise meta-analysis and meta-regression analysis were analyzed via Open-MetaAnalyst software20 and the quality of evidence assessed via the GRADEpro GDT software.34 The statistical significance was identified for P value <0.05.
Results
Study Characteristics
Of the 332 potentially relevant records identified in the initial search, 17 studies were deemed eligible for qualitative and quantitative syntheses.2,6,7,35–48 Full-text papers were published between 2016 and 2021.
Data obtained from 55219 COPD patients were extracted from 15 post-hoc analyses of RCTs, a subgroup analysis of a RCT,40 and a RCT prospectively assessing the CID composite endpoint.42 The duration of the studies ranged from 3 to 48 months and the age of the COPD populations enrolled in the studies ranged from 62.8 to 65.3 years.
A certain level of study population overlap was detected across the post-hoc analyses. Namely, the SHINE trial49 was analyzed in both the studies by D’Urzo et al45 and Anzueto et al,7 the ZEP117115 trial50 was included in both the post-hoc analyses by Maleki-Yazdi et al48 and Singh et al,2 the study by Chen et al40 was a subgroup analysis of the PINNACLE-4 trial,51 which was also included in the post-hoc analysis by Zheng et al.39
Different treatments were analyzed as following: long-acting bronchodilators (LABD) vs PCB,2,37–40,45,47 long-acting muscarinic antagonist (LAMA) vs long-acting β2-adrenoceptor agonist (LABA),2,40 dual bronchodilation vs PCB,2,39,40,47 dual bronchodilation vs LABD,2,7,36,39,40,42,47,48 dual bronchodilation vs inhaled corticosteroid (ICS)/LABA,35,46 ICS/LABA vs LABD,41 triple combination vs LABD,43 triple combination vs dual bronchodilation,35,43 triple combination vs ICS/LABA.6,35,43,44
The main characteristics of the studies included in the systematic review and meta-regression analysis are reported in Table 1, whereas Table 2 shows the different CID definitions for study.
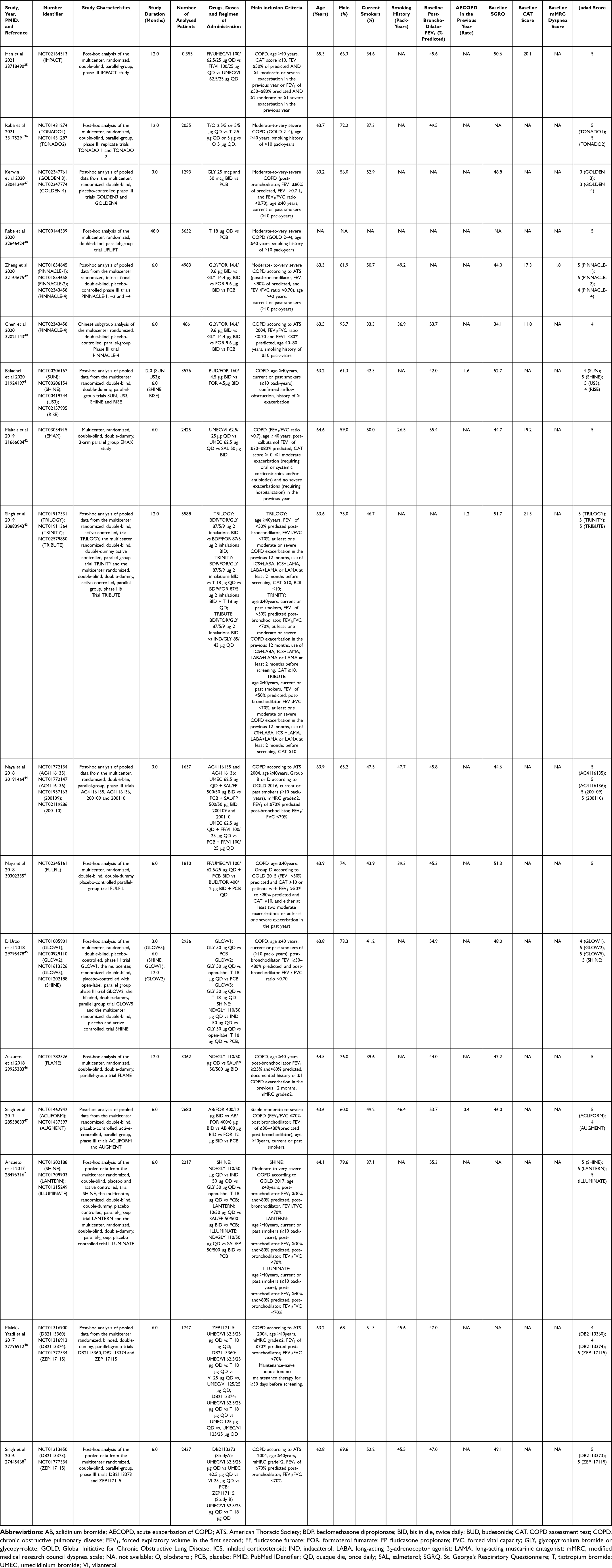 |
Table 1 Main Characteristics of the Studies Included in the Systematic Review and Meta-Regression Analysis |
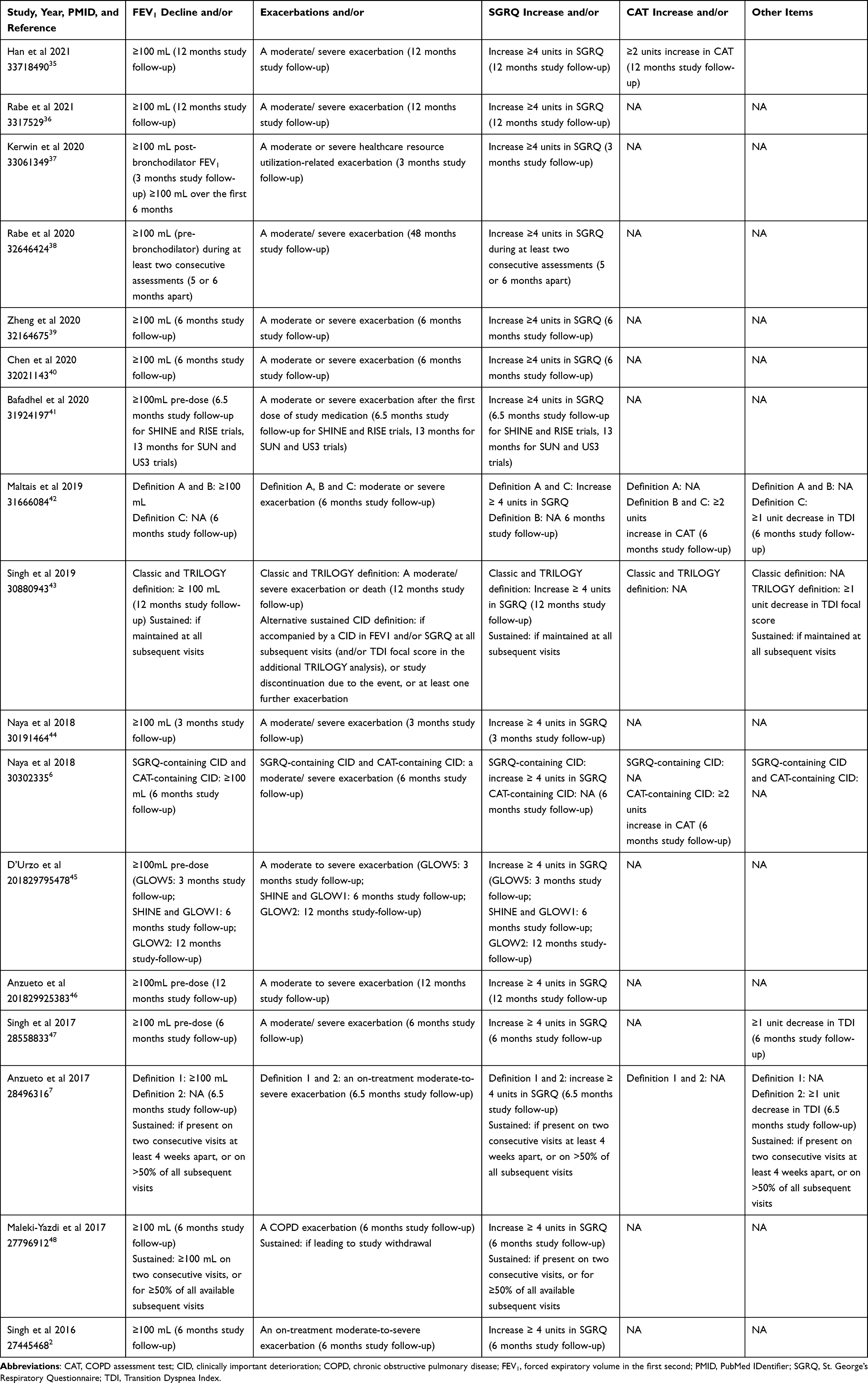 |
Table 2 Different CID Definitions Used in the Studies Included in the Systematic Review and Meta-Regression Analysis |
Pairwise Meta-Analysis
The overall pairwise meta-analysis indicated that the pharmacological treatment of COPD is effective in reducing the risk of CID in COPD (RR: 0.81, 95% CI 0.79–0.84; P < 0.001, GRADE +++) (Figure 2). The effect estimates were affected by high and significant heterogeneity (I2 92.28%, P < 0.001).
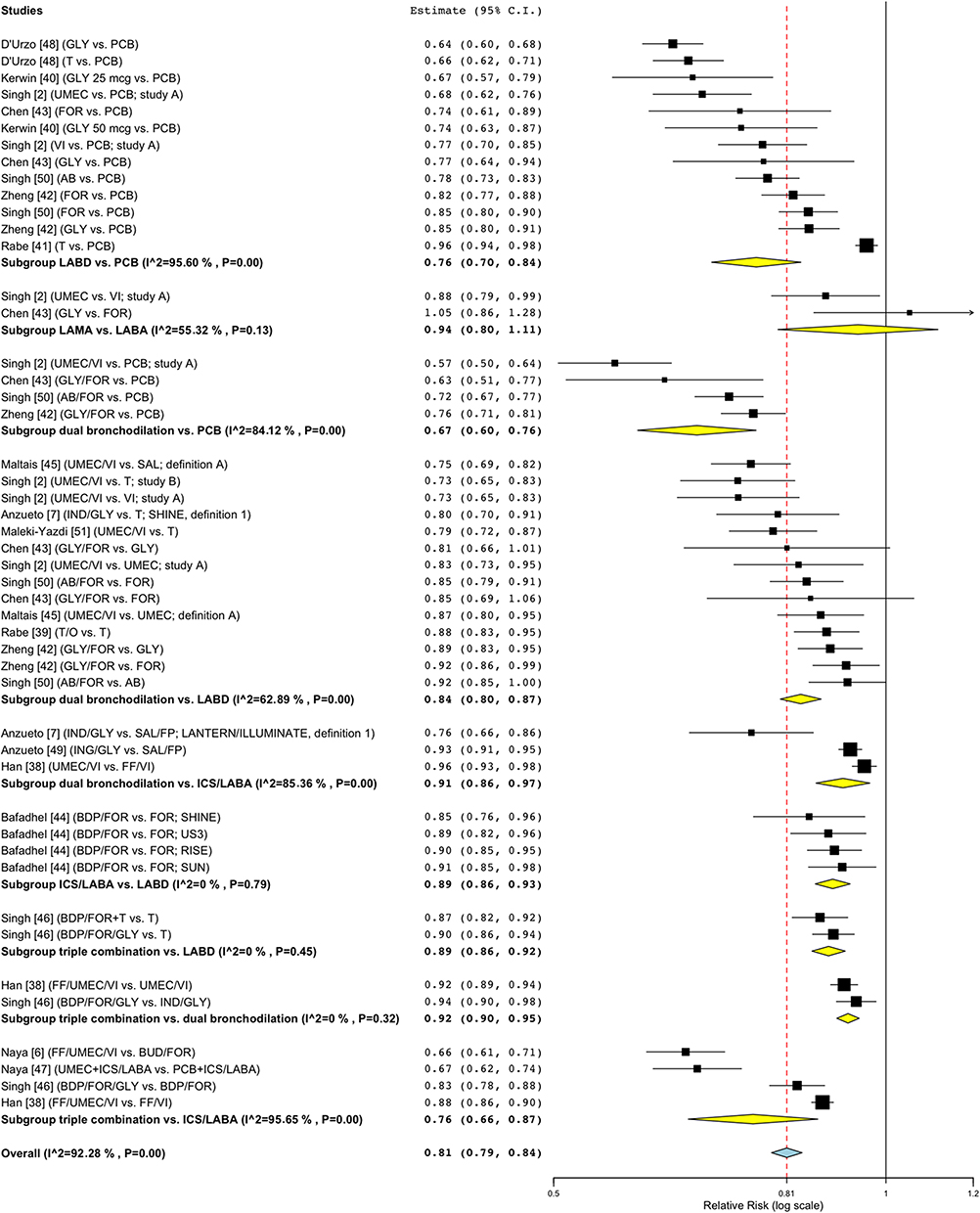 |
Figure 2 Forest plot of meta-analysis concerning the impact of pharmacological treatment on the risk of CID in COPD. Abbreviations: AB, aclidinium bromide; BUD, budesonide; CID, clinically important deterioration; COPD, chronic obstructive pulmonary disease; FF, fluticasone furoate; FOR, formoterol fumarate; FP, fluticasone propionate; GLY, glycopyrronium bromide or glycopyrrolate; ICS, inhaled corticosteroid; IND, indacaterol; LABA, long-acting β2-adrenoceptor agonist; LABD, long-acting bronchodilators; LAMA, long-acting muscarinic antagonist; O, olodaterol; PCB, placebo; SAL, salmeterol; T, tiotropium bromide; UMEC, umeclidinium bromide; VI, vilanterol. Notes: The subgroup and overall effect estimates resulting from the meta-analysis are reported in bold; the red-dashed line indicates the average relative risk resulting for the overall effect estimate. |
More specifically, when compared to PCB, LABD and dual bronchodilation significantly (P < 0.001) reduced the risk of CID (RR: 0.76, 95% CI 0.70–0.84, GRADE +++ and RR: 0.67, 95% CI 0.60–0.76, GRADE +++, respectively). When compared to LABD, dual bronchodilation, ICS/LABA and triple combination significantly (P < 0.001) reduced the risk of CID (RR: 0.84, 95% CI 0.80–0.87, GRADE +++, RR: 0.89, 95% CI 0.86–0.93, GRADE ++++ and RR: 0.89, 95% CI 0.86–0.92, GRADE ++++, respectively). Triple combination significantly (P < 0.001) reduced the risk of CID (RR: 0.92, 95% CI 0.90–0.95, GRADE ++++) compared to dual bronchodilation. When compared to ICS/LABA, dual bronchodilation and triple combination significantly reduced the risk of CID (RR: 0.91, 95% CI 0.86–0.97, P < 0.01, GRADE +++ and RR: 0.76, 95% CI 0.66–0.87, P < 0.001, GRADE +++, respectively). Only the comparison between LAMA and LABA did not significantly modulate in the risk of CID (RR: 0.94, 95% CI 0.80–1.11, P > 0.05, GRADE +++).
The study arms comparing the same treatment groups were excluded from the pairwise meta-analysis. Namely, the study by Zheng et al, Maltais et al and Singh et al39,42,47 included a subgroup comparing a long-acting muscarinic antagonist (LAMA) and a LABA, both belonging to the LABDs. The post-hoc analysis by Singh et al43 included the TRINITY trial,52 comparing two different triple combinations, while the study by D’Urzo et al47 compared different LAMAs.
Meta-Regression Analysis
An overall meta-regression analysis was performed for age, to assess whether it might modulate the risk of CID in COPD patients. Although age was not a significant (P > 0.05) potential effect modifier, it resulted a trend toward significance (P = 0.063) in the linear relationship with respect to the RR of CID (slope: 0.051, Figure 3).
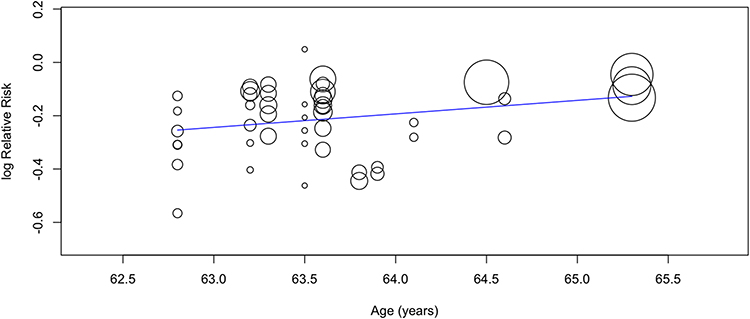 |
Figure 3 Graphical representation of the meta-regression analysis for age with respect to the risk of CID. Abbreviation: CID, clinically important deterioration. Note: The size of the circles is proportional to the sample weights. |
When considering specific treatment subgroups, age was a significant (P < 0.05) potential effect modifier for CID only for dual bronchodilation vs PCB and dual bronchodilation vs ICS/LABA subgroups (slope: 0.268 and 0.103, respectively).
The impact of age on CID was also analyzed in association with other characteristics of the study population, namely, gender, smoking habit, post-bronchodilator FEV1, AECOPD, SGRQ, CAT, and mMRC. Only when associated with post-bronchodilator FEV1, age significantly modulated the risk of CID (P = 0.027, slope = 0.061), indicating that the pharmacological treatment of COPD is less effective in older patients with reduced lung function. When associated with the other population characteristics, age did not result in a significant modulating factor (P > 0.05).
Among the study characteristics, the duration of the trials represented a significant (P < 0.001) albeit modest potential effect modifier for the risk of CID in COPD (slope: 0.008, Figure S1), suggesting a greater impact of pharmacological treatment in shorter-term studies.
Bias and Quality of Evidence
All studies (100.0%) were ranked as being of medium- to high-quality in agreement with Jadad score (Table 1). One study was of medium quality (Jadad score = 3),37 and all the others were of high quality (Jadad score >3).
The assessment of the quality of evidence carried out via the GRADE system reported a general moderate (+++) to high-quality (++++) of evidence.
The visual inspection of the funnel plot confirmed the presence of overall heterogeneity, with data reported in an apparent symmetric way. Nevertheless, Egger’s test indicated that the overall effect estimates resulting from this meta-analysis were not affected by significant bias and confirmed symmetry for the reported data. Details on the funnel plots and Egger’s test analyses are reported in Figure 4.
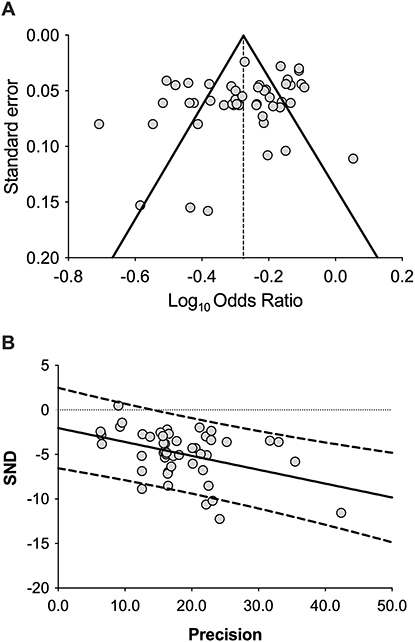 |
Figure 4 Funnel plot (A) and graphical representations of Egger’s test (B). Abbreviation: SND, standard normal deviate. Notes: Funnel plot represents a visual approach to check for the existence of publication bias by assessing the symmetry of study distribution, whereas Egger’s test is a regression assay that permits to statistically quantify the extent of Funnel plot asymmetry; dotted lines in the Egger’s test represent 90% prediction bands. |
Discussion
The findings of this quantitative synthesis indicate with moderate-to-high quality of evidence that the pharmacological treatment of COPD significantly reduces the risk of CID in the overall study population.
Moreover, three specific treatment subgroups, namely, LABD vs PCB, dual bronchodilation vs PCB, and triple combination vs ICS/LABA reached the minimal clinically important difference in the risk of CID, according to a detected RR value ≤0.75, as previously reported.53,54 As expected, LAMA vs LABA did not modulate the risk of CID. Although data reported a certain level of heterogeneity, Egger’s test excluded that results were affected by significant bias.
Thus, the findings of this quantitative synthesis support the use of CID as an outcome for pharmacological trials in COPD, as already suggested in previous narrative reviews.3,5
Of note, the meta-regression analysis indicated that age may represent a potential effect modifier for the impact of pharmacological treatment against the risk of CID in COPD, although just a trend towards significance was detected. As a matter of fact, despite the limited range of age between 62.5 and 65.5 years of the investigated population, it resulted that older patients may have a numerical greater risk of CID. Such a narrow age range is related to the intrinsic characteristics of the COPD populations enrolled in the primary RCTs, which evidently appear to differ from the broader demographic diversity detectable among real-life COPD patients. Therefore, it is expected that the impact of ageing could have a significant and detrimental impact on the risk of CID when considering a wider range of age in a real-life setting.
Interestingly, when the meta-regression analysis for age was carried out along with lung function, age significantly modulated the risk of CID when associated with post-bronchodilator FEV1. On the other hand, the latter evidence suggests that older COPD patients with a larger impairment in lung function may experience a higher risk of CID.
In this regard, the Age, Dyspnea and airflow Obstruction (ADO) index was reported to be a prognostic factor in COPD.55 Further evidence indicated that the ADO index may be a predictor of 3-year mortality in COPD.56 It is important to underline that also the occurrence of a CID in the natural history of COPD patients correlates with all-cause mortality,14,57 supporting the existence of a correlation between CID and age, especially when associated with lower FEV1.
The evidence that older patients with impaired lung function are more prone to undergo a CID may have a substantial impact on daily clinical practice. In this respect, since the general population ageing is increasing as well as the age at death in COPD patients, and FEV1 decline is greater in older patients,9,58 it is expected that the prevalence of elderly COPD patients with poor clinical condition will increase in the future (Figure 5). This COPD population is per se characterized by a higher burden of comorbidities17,59 that need to be managed properly, especially on the cardiovascular disease counterpart.60,61 In this scenario, elderly COPD patients not only need to be screened and treated for comorbidities but might also benefit from a tight functional follow-up and an early pharmacological therapy in order to reduce the risk of CID.
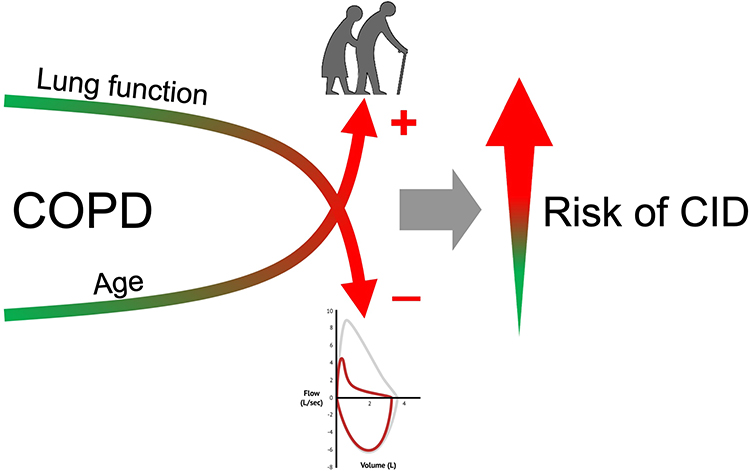 |
Figure 5 CID risk increases in older patients with worse lung function. Abbreviation: CID, clinically important deterioration; COPD, chronic obstructive pulmonary disease; FEV1, forced expiratory volume in the first second. Notes: The meta-regression analysis suggested that age significantly modulates the risk of CID when associated with lower post-bronchodilator FEV1. |
The main limitations to this study are intrinsic to the quantitative synthesis methods, which are based on large sample approximations, and to the intrinsic weakness of the included studies.62,63 Indeed, most of the studies were post-hoc analyses of RCTs, and only one was an RCT prospectively assessing the CID composite endpoint. Moreover, the studies spanned a duration ranging from 3 to 48 months, introducing a certain level of temporal heterogeneity that could potentially act as an effect modifier, suggesting greater efficacy of pharmacological treatment in shorter-term studies. Finally, also the limited age range may represent a limitation of our analysis.
Conclusion
This systematic review and meta-regression analysis indicates that inhaled therapy is effective in reducing the risk of CID in COPD, although such a protective effect may be affected in older patients with reduced lung function. Certainly, further studies designed to directly assess the impact of ageing on CID are needed to confirm these findings in COPD.
Abbreviations
AB, aclidinium bromide; ADO, Age, Dyspnea and airflow Obstruction; AECOPD, acute exacerbation of COPD; ATS, American Thoracic Society; BDP, beclomethasone dipropionate; BID, bis in die, twice daily; BUD, budesonide; CAT, COPD assessment test; CI, confidence interval; CID, clinically important deterioration; COPD, chronic obstructive pulmonary disease; DECiMAL, Data Extraction for Complex Meta-anALysis; FEV1, forced expiratory volume in the first second; FF, fluticasone furoate; FOR, formoterol fumarate; FP, fluticasone propionate; FVC, forced vital capacity; GLY, glycopyrronium bromide or glycopyrrolate; GOLD, Global Initiative for Chronic Obstructive Lung Disease; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; HRQL, health-related quality of life; ICS, inhaled corticosteroid; IND, indacaterol; LABA, long-acting β2-adrenoceptor agonist; LAMA, long-acting muscarinic antagonist; MCID, minimal clinically important difference; mMRC, modified medical research council dyspnea scale; NA, not available; O, olodaterol; PICO, Patient problem, Intervention, Comparison, and Outcome; PCB, placebo; PMID, PubMed Identifier; PRISMA-P, Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols; PRO, patient-reported outcome; QD, quaque die, once daily; RCT, randomized controlled trial; RR, relative risk; SABA, short-acting β2-adrenoceptor agonist; SAL, salmeterol; SAMA, short-acting muscarinic antagonist; SGRQ, St. George’s Respiratory Questionnaire; T, tiotropium bromide; TDI, Transition Dyspnea Index; UMEC, umeclidinium bromide; VI, vilanterol.
Acknowlegments
No sponsor had a role in the design of the study, the collection and analysis of the data, or in the preparation of the manuscript.
Author Contributions
All the authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was not funded.
Disclosure
GMM, JO and AS report no conflicts of interest in this work. MC has participated as a faculty member and advisor in scientific meetings and courses under the sponsorship of Almirall, AstraZeneca, Biofutura, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini Group, Lallemand, Mundipharma, Novartis, Pfizer, Verona Pharma, and Zambon, and is or has been a consultant to ABC Farmaceutici, AstraZeneca, Chiesi Farmaceutici, Edmond Pharma, Lallemand, Novartis, Ockham Biotech, Verona Pharma, and Zambon. His department was funded by Almirall. PR report grants and personal fees from Almirall, AstraZeneca, Biofutura, Boehringer Ingelheim, Chiesi Farmaceutici, GlaxoSmithKline, Menarini Group, MSD, Mundipharma, and Novartis, and participated as a lecturer and advisor in scientific meetings sponsored by Almirall, AstraZeneca, Biofutura, Boehringer Ingelheim, Chiesi Farmaceutici, Edmond Pharma, GlaxoSmithKline, Menarini Group, Mundipharma, and Novartis. Her department was funded by Almirall, Boehringer Ingelheim, Chiesi Farmaceutici, Novartis, and Zambon. LC participated as an advisor in scientific meetings sponsored by Boehringer Ingelheim and Novartis, received non-financial support from AstraZeneca, a research grant partially funded by Chiesi Farmaceutici, Boehringer Ingelheim, Novartis, and Almirall, and is or was a consultant to ABC Farmaceutici, MSD, Recipharm, Zambon, Verona Pharma and Ockham Biotech. His department was funded by Almirall, Boehringer Ingelheim, Chiesi Farmaceutici, Novartis and Zambon.
References
1. 2023 GOLD report - global initiative for chronic obstructive lung disease - GOLD. Available from: https://goldcopd.org/2023-gold-report-2/.
2. Singh D, Maleki-Yazdi MR, Tombs L, Iqbal A, Fahy WA, Naya I. Prevention of clinically important deteriorations in COPD with umeclidinium/vilanterol. Int J COPD. 2016;11(1). doi:10.2147/COPD.S101612
3. Cazzola M, Matera MG. Clinically important deterioration: a composite tool for managing patients with COPD. Respir Med. 2022;205. doi:10.1016/j.rmed.2022.107054
4. O T, N K, T M, S S, H T, M M. Longitudinal deteriorations in patient reported outcomes in patients with COPD. Respir Med. 2007;101(1):1.
5. Singh D, Criner GJ, Naya I, et al. Measuring disease activity in COPD: is clinically important deterioration the answer? Respir Res. 2020;21(1). doi:10.1186/s12931-020-01387-z
6. Naya I, Compton C, Ismaila AS, et al. Preventing clinically important deterioration with single-inhaler triple therapy in COPD. ERJ Open Res. 2018;4(4):00047–2018. doi:10.1183/23120541.00047-2018
7. Anzueto AR, Vogelmeier CF, Kostikas K, et al. The effect of indacaterol/glycopyrronium versus tiotropium or salmeterol/fluticasone on the prevention of clinically important deterioration in COPD. Int J COPD. 2017;2017:12–1325. doi:10.2147/COPD.S133307
8. Vestbo J, Edwards LD, Scanlon PD, et al. Changes in forced expiratory volume in 1 second over time in COPD. N Engl J Med. 2011;365(13):1184–1192. doi:10.1056/nejmoa1105482
9. Rosso A, Egervall K, Elmståhl S. Annual decline rate in FEV1s in community-dwelling older adults diagnosed with mild to moderate COPD. NPJ Prim Care Respir Med. 2022;32(1). doi:10.1038/s41533-022-00292-w
10. Donohue JF. Minimal clinically important differences in COPD lung function. COPD. 2005;2(1):111–124. doi:10.1081/COPD-200053377
11. Fletcher C, Peto R. The natural history of chronic airflow obstruction. Bull Int Union Tuberc. 1978;53(2):1.
12. Kim SJ, Lee J, Park YS, et al. Age-related annual decline of lung function in patients with COPD. Int J COPD. 2015:11. doi:10.2147/COPD.S95028
13. Thomas ET, Guppy M, Straus SE, Bell KJL, Glasziou P. Rate of normal lung function decline in ageing adults: a systematic review of prospective cohort studies. BMJ Open. 2019;9(6):e028150. doi:10.1136/bmjopen-2018-028150
14. Hurst JR, Han MLK, Singh B, et al. Prognostic risk factors for moderate-to-severe exacerbations in patients with chronic obstructive pulmonary disease: a systematic literature review. Respir Res. 2022;23(1). doi:10.1186/s12931-022-02123-5
15. Spannella F, Giulietti F, Cocci G, et al. Acute exacerbation of chronic obstructive pulmonary disease in oldest adults: predictors of in-hospital mortality and need for post-acute care. J Am Med Dir Assoc. 2019;20(7):893–898. doi:10.1016/j.jamda.2019.01.125
16. Cho WK, Lee CG, Kim LK. COPD as a disease of immunosenescence. Yonsei Med J. 2019;60(5):407. doi:10.3349/ymj.2019.60.5.407
17. Cavaillès A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. doi:10.1183/09059180.00008612
18. Mülazimoglu DD, Ayöz S. Are comorbidities related to frequent severe exacerbations of COPD? Eur Respir J. 2019;54:1.
19. Martinez CH, Diaz AA, Parulekar AD, et al. Age-related differences in health-related quality of life in COPD: an analysis of the COPDGene and SPIROMICS Cohorts. Chest. 2016;149(4):927–935. doi:10.1016/j.chest.2015.11.025
20. Wallace BC, Dahabreh IJ, Trikalinos TA, Lau J, Trow P, Schmid CH. Closing the gap between methodologists and end-users: r as a computational back-end. J Stat Softw. 2012;49. doi:10.18637/jss.v049.i05
21. Viechtbauer W, Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1–48. doi:10.18637/jss.v036.i03
22. Haggins GSR. Cochrane handbook for systematic reviews of interventions version 5.1.0. Cochrane Database Syst Rev. 2020;2020(2):1.
23. Borenstein M, Hedges LV. Introduction to Meta‐Analysis; 2009.
24. Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Rev Esp Nutr Hum Diet. 2016;20(2). doi:10.1186/2046-4053-4-1
25. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
26. Schardt C, Adams MB, Owens T, Keitz S, Fontelo P. Utilization of the PICO framework to improve searching PubMed for clinical questions. BMC Med Inform Decis Mak. 2007;7:16. doi:10.1186/1472-6947-7-16
27. Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12. doi:10.1016/0197-2456(95)00134-4
28. Pedder H, Sarri G, Keeney E, Nunes V, Dias S. Data extraction for complex meta-analysis (DECiMAL) guide. Syst Rev. 2016;5(1):212. doi:10.1186/s13643-016-0368-4
29. Gianinazzi ME, Rueegg CS, Zimmerman K, Kuehni CE, Michel G. Swiss paediatric oncology G. Intra-rater and inter-rater reliability of a medical record abstraction study on transition of care after childhood cancer. PLoS One. 2015;10(5):e0124290. doi:10.1371/journal.pone.0124290
30. Sterne JAC, Gavaghan D, Egger M. Publication and related bias in meta-analysis: power of statistical tests and prevalence in the literature. J Clin Epidemiol. 2000;53(11):1119–1129. doi:10.1016/S0895-4356(00)00242-0
31. Sterne JAC, Egger M. Funnel plots for detecting bias in meta-analysis: guidelines on choice of axis. J Clin Epidemiol. 2001;54(10):1046–1055. doi:10.1016/S0895-4356(01)00377-8
32. Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Br Med J. 1997;315(7109):629–634. doi:10.1136/bmj.315.7109.629
33. 10.4.3.1 Recommendations on testing for funnel plot asymmetry. Available from: https://handbook-5-1.cochrane.org/chapter_10/10_4_3_1_recommendations_on_testing_for_funnel_plot_asymmetry.htm.
34. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
35. Han MK, Criner GJ, Dransfield MT, et al. Prognostic value of clinically important deterioration in COPD: impact trial analysis. ERJ Open Res. 2021;7(1):00663–2020. doi:10.1183/23120541.00663-2020
36. Rabe KF, Chalmers JD, Miravitlles M, et al. Tiotropium/olodaterol delays clinically important deterioration compared with tiotropium monotherapy in patients with early COPD: a post hoc analysis of the TONADO® trials. Adv Ther. 2021;38(1):579–593. doi:10.1007/s12325-020-01528-2
37. Kerwin EM, Murray L, Niu X, Dembek C. Clinically important deterioration among patients with chronic obstructive pulmonary disease (COPD) treated with nebulized glycopyrrolate: a post hoc analysis of pooled data from two randomized, double-blind, placebo-controlled studies. Int J COPD. 2020;15. doi:10.2147/COPD.S267249
38. Rabe KF, Halpin DMG, Han MK, et al. Composite endpoints in COPD: clinically important deterioration in the UPLIFT trial. Respir Res. 2020;21(1). doi:10.1186/s12931-020-01431-y
39. Zheng J, Xu JF, Jenkins M, Assam PN, Wang L, Lipworth BJ. Glycopyrrolate/formoterol fumarate metered dose inhaler for maintenance-naïve patients with chronic obstructive pulmonary disease: a post-hoc analysis of the randomized PINNACLE trials. Respir Res. 2020;21(1). doi:10.1186/s12931-020-1332-3
40. Chen R, Zhong N, Wang HY, et al. Efficacy and safety of glycopyrrolate/formoterol fumarate metered dose inhaler (GFF MDI) formulated using co-suspension delivery technology in Chinese patients with COPD. Int J COPD. 2020;15. doi:10.2147/COPD.S223638
41. Bafadhel M, Singh D, Jenkins C, et al. Reduced risk of clinically important deteriorations by ICS in COPD is eosinophil dependent: a pooled post-hoc analysis. Respir Res. 2020;21(1). doi:10.1186/s12931-020-1280-y
42. Maltais F, Bjermer L, Kerwin EM, et al. Efficacy of umeclidinium/vilanterol versus umeclidinium and salmeterol monotherapies in symptomatic patients with COPD not receiving inhaled corticosteroids: the EMAX randomised trial. Respir Res. 2019;20(1). doi:10.1186/s12931-019-1193-9
43. Singh D, Fabbri LM, Vezzoli S, Petruzzelli S, Papi A. Extrafine triple therapy delays COPD clinically important deterioration vs ICS/LABA, LAMA, or LABA/LAMA. Int J COPD. 2019;14. doi:10.2147/COPD.S196383
44. Naya IP, Tombs L, Lipson DA, Compton C. Preventing clinically important deterioration of COPD with addition of umeclidinium to inhaled corticosteroid/long-acting β2-agonist therapy: an integrated post hoc analysis. Adv Ther. 2018;35(10):1626–1638. doi:10.1007/s12325-018-0771-4
45. Durzo A, Bader G, Shen S, Goyal P, Altman P. Comparison of glycopyrronium versus tiotropium on the time to clinically important deteriorations in patients with COPD: a post-hoc analysis of randomized trials. NPJ Prim Care Respir Med. 2018;28(1). doi:10.1038/s41533-018-0084-8
46. Anzueto AR, Kostikas K, Mezzi K, et al. Indacaterol/glycopyrronium versus salmeterol/fluticasone in the prevention of clinically important deterioration in COPD: results from the FLAME study. Respir Res. 2018;19(1). doi:10.1186/s12931-018-0830-z
47. Singh D, D’Urzo AD, Chuecos F, Muñoz A, Garcia Gil E. Reduction in clinically important deterioration in chronic obstructive pulmonary disease with Aclidinium/formoterol. Respir Res. 2017;18(1). doi:10.1186/s12931-017-0583-0
48. Maleki-Yazdi MR, Singh D, Anzueto A, Tombs L, Fahy WA, Naya I. Assessing short-term deterioration in maintenance-naïve patients with COPD receiving umeclidinium/vilanterol and tiotropium: a pooled analysis of three randomized trials. Adv Ther. 2017;33(12):2188–2199. doi:10.1007/s12325-016-0430-6
49. Bateman ED, Ferguson GT, Barnes N, et al. Dual bronchodilation with QVA149 versus single bronchodilator therapy: the SHINE study. Eur Respir J. 2013;42(6):1484–1494. doi:10.1183/09031936.00200212
50. Maleki-Yazdi MR, Kaelin T, Richard N, Zvarich M, Church A. Efficacy and safety of umeclidinium/vilanterol 62.5/25 mcg and tiotropium 18 mcg in chronic obstructive pulmonary disease: results of a 24-week, randomized, controlled trial. Respir Med. 2014;108(12):1752–1760. doi:10.1016/j.rmed.2014.10.002
51. Lipworth BJ, Collier DJ, Gon Y. Improved lung function and patient-reported outcomes with co-suspension delivery technology glycopyrrolate/formoterol fumarate metered dose inhaler in COPD: a randomized phase III study conducted in Asia, Europe, and the USA. Int J Chron Obstruct Pulmon Dis. 2018;13:2969–2984. doi:10.2147/COPD.S171835
52. Vestbo J, Papi A, Corradi M, et al. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (TRINITY): a double-blind, parallel group, randomised controlled trial. Lancet. 2017;389(10082):1919–1929. doi:10.1016/S0140-6736(17)30188-5
53. Guyatt GH, Oxman AD, Kunz R, et al. GRADE guidelines 6. Rating the quality of evidence--imprecision. J Clin Epidemiol. 2011;64(12):1283–1293. doi:10.1016/J.JCLINEPI.2011.01.012
54. Calzetta L, Cazzola M, Matera MG, Rogliani P. Adding a LAMA to ICS/LABA therapy: a meta-analysis of triple combination therapy in COPD. Chest. 2019;155(4):758–770. doi:10.1016/j.chest.2018.12.016
55. Puhan MA, Garcia-Aymerich J, Frey M, et al. Expansion of the prognostic assessment of patients with chronic obstructive pulmonary disease: the updated BODE index and the ADO index. Lancet. 2009;374(9691):704–711. doi:10.1016/S0140-6736(09)61301-5
56. Puhan MA, Hansel NN, Sobradillo P, et al. Large-scale international validation of the ADO index in subjects with COPD: an individual subject data analysis of 10 cohorts. BMJ Open. 2012;2(6):e002152. doi:10.1136/bmjopen-2012-002152
57. Naya IP, Tombs L, Muellerova H, Compton C, Jones PW. Long-term outcomes following first short-term clinically important deterioration in COPD. Respir Res. 2018;19(1). doi:10.1186/s12931-018-0928-3
58. James GD, Donaldson GC, Wedzicha JA, Nazareth I. Trends in management and outcomes of COPD patients in primary care, 2000–2009: a retrospective cohort study. NPJ Prim Care Respir Med. 2014;24. doi:10.1038/npjpcrm.2014.15
59. Matera M, Calzetta L, Rogliani P, Cesario A, Cazzola M. New treatments for COPD in the elderly. Curr Pharm Des. 2014;20(38):5968–5982. doi:10.2174/1381612820666140314154331
60. Matera MG, Calzetta L, Rinaldi B, Cazzola M. Treatment of COPD: moving beyond the lungs. Curr Opin Pharmacol. 2012;12(3):315–322. doi:10.1016/j.coph.2012.04.001
61. Cazzola M, Calzetta L, Rinaldi B, et al. Management of chronic obstructive pulmonary disease in patients with cardiovascular diseases. Drugs. 2017;77(7):721–732. doi:10.1007/s40265-017-0731-3
62. Rogliani P, Cavalli F, Chetta A, Cazzola M, Calzetta L. Potential drawbacks of ICS/LABA/LAMA triple fixed-dose combination therapy in the treatment of asthma: a quantitative synthesis of safety profile. J Asthma Allergy. 2022;15:565–577. doi:10.2147/JAA.S283489
63. Curran-Everett D, Milgrom H. Post-hoc data analysis: benefits and limitations. Curr Opin Allergy Clin Immunol. 2013;13(3):223–224. doi:10.1097/ACI.0b013e3283609831
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Feng Z, Zhang L, Yu H, Su X, Shuai T, Zhu L, Chen D, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1987-1999
Published Date: 30 August 2022
Comparison of High-Flow Nasal Cannula with Conventional Oxygen Therapy in Patients with Hypercapnic Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Zhang L, Wang Y, Ye Y, Gao J, Zhu F, Min L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:895-906
Published Date: 16 May 2023
Barriers and Facilitators to Exercise Compliance for Community Elders with COPD: A Cross-Sectional Study
Xia J, Yang J, Yang X, Zhang S, Guo H, Zhang C
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1965-1974
Published Date: 8 September 2023
Efficacy and Safety of Bisoprolol in Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Feng Z, Zhang L, Wang Y, Guo H, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:3067-3083
Published Date: 23 December 2023
Comparison of the Application of Vibrating Mesh Nebulizer and Jet Nebulizer in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta‐analysis
Feng Z, Han Z, Wang Y, Guo H, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:829-839
Published Date: 28 March 2024