Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Impact of High-Flow Nasal Cannula for Chronic Obstructive Pulmonary Disease Exacerbation: A Systematic Review of Clinical and Physiological Outcomes
Authors Al Nufaiei ZF ![]() , Hakeem JZ
, Hakeem JZ
Received 3 January 2026
Accepted for publication 7 May 2026
Published 14 July 2026 Volume 2026:21 593501
DOI https://doi.org/10.2147/COPD.S593501
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Ziyad F Al Nufaiei,1,2 Jameel Zaid Hakeem1,2
1Respiratory Therapy Department, College of Applied Medical Sciences, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 2King Abdullah International Medical Research Center, Jeddah, Saudi Arabia
Correspondence: Ziyad F Al Nufaiei, Respiratory Therapy Department, College of Applied Medical Sciences-Jeddah, King Saud bin Abdulaziz University for Health Sciences, P.O.Box.9515, Jeddah, 21423, Kingdom of Saudi Arabia, Tel +966551600060, Ext: 46125, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) caused 3.72 million deaths in 2021. Exacerbations drive morbidity and hospital admissions. Conventional oxygen therapy (COT) offers limited support, while non-invasive ventilation (NIV) improves outcomes but is often poorly tolerated. High-flow nasal cannula (HFNC) delivers heated, humidified oxygen at high flow rates, improving gas exchange and comfort. This systematic review (PRISMA-guided) examines HFNC use in acute and chronic hypercapnic COPD compared with COT and NIV.
Methods: Systematic searches of MEDLINE, Embase and CENTRAL (to 2025) identified 14 primary studies (7 randomized trials, 7 observational cohorts). Physiological, clinical and patient-reported outcomes were extracted. Risk of bias was evaluated using RoB 2 and ROBINS-I.
Results: In acute settings, HFNC consistently improved PaCO2 and reduced respiratory effort versus COT, lowering treatment failure (10.0% vs 19.4%, p=0.026). However, HFNC failed non-inferiority versus NIV for treatment failure (25.7% vs 14.3%) and showed higher intubation (14.2% vs 5.4%, p=0.026). Domiciliary HFNC reduced annual exacerbations and improved quality of life (SGRQ mean difference − 8.12).
Conclusion: HFNC provides physiological benefits and lowers short-term failure versus COT and reduces home exacerbations. However, it is less effective than NIV for severe hypercapnic failure. HFNC should be reserved for mild-to-moderate exacerbations or NIV-intolerant patients, with close monitoring and predefined escalation criteria.
Keywords: chronic obstructive pulmonary disease, high-flow nasal cannula, non-invasive ventilation, conventional oxygen therapy, exacerbations, hypercapnic respiratory failure
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading global cause of death and disability. The Global Burden of Disease Study estimated 3.72 million COPD-related deaths in 2021, with an age-standardized mortality rate of 45.2 per 100,000 persons.1 Exacerbations—acute episodes of worsening respiratory symptoms requiring additional treatment—occur approximately 2.4 times per year and are strongly linked to lung function decline and poor quality of life.2 Hospitalization for an acute exacerbation carries a one-year mortality approaching 40% when mechanical ventilation is required, rising to 49% by three years.3
Standard respiratory support relies on low-flow conventional oxygen therapy (COT) and non-invasive ventilation (NIV). Low-flow oxygen often fails to meet inspiratory demand, whereas NIV, though effective in reducing intubation and mortality, is frequently limited by patient intolerance.4 Current guidelines from GOLD recommend NIV as first-line ventilatory support for acute hypercapnic respiratory failure, but do not endorse HFNC as a replacement.4
High-flow nasal cannula (HFNC) therapy has emerged as an alternative, delivering heated, humidified oxygen at flow rates up to 60 L/min with precise FiO2 control.5 HFNC can flush anatomical dead space, reduce CO2 rebreathing, generate mild positive airway pressure (approximately 2–5 cmH2O), and ease breathing effort.6–8 Despite these physiological benefits, evidence remains mixed: while studies show improved gas exchange and comfort, benefits for intubation, treatment failure, or mortality are inconsistent.9,10 A clear knowledge gap exists regarding whether HFNC can safely replace NIV in acute settings or should be reserved for specific subgroups.
This review examines the current evidence for HFNC in COPD exacerbations across three distinct settings: (1) acute in-hospital hypercapnic exacerbations, (2) post-extubation support, and (3) chronic domiciliary use. We focus on its clinical efficacy, safety, and comparative role alongside COT and NIV, with explicit attention to patient severity—mild-to-moderate versus severe hypercapnic respiratory failure—as outcomes differ substantially across these groups.
Methodology
Search Strategy and Selection
A structured literature search was conducted across MEDLINE, Embase and the Cochrane Central Register of Controlled Trials (CENTRAL) through 2025. The full search strategy with Boolean operators and controlled vocabulary was as follows: (“high-flow nasal cannula” OR HFNC OR “nasal high flow” OR “heated humidified high-flow nasal cannula”) AND (“COPD exacerbation” OR “acute exacerbation of COPD” OR AECOPD OR “chronic obstructive pulmonary disease” OR “hypercapnic respiratory failure”) AND (“non-invasive ventilation” OR NIV OR “oxygen therapy” OR “conventional oxygen therapy” OR COT OR “post-extubation” OR “domiciliary oxygen”). Reference lists of identified papers were screened to capture additional relevant studies. Preprint servers were not included in this search.
Eligibility Criteria
Included reports comprised randomized controlled trials, randomized crossover physiologic studies, and prospective or retrospective observational cohorts examining HFNC in acute or chronic hypercapnic COPD. Eligible comparisons included NIV or COT. Studies without quantifiable outcomes or original data (eg, case reports, editorials, systematic reviews, meta-analyses, device descriptions) were excluded (Figure 1).
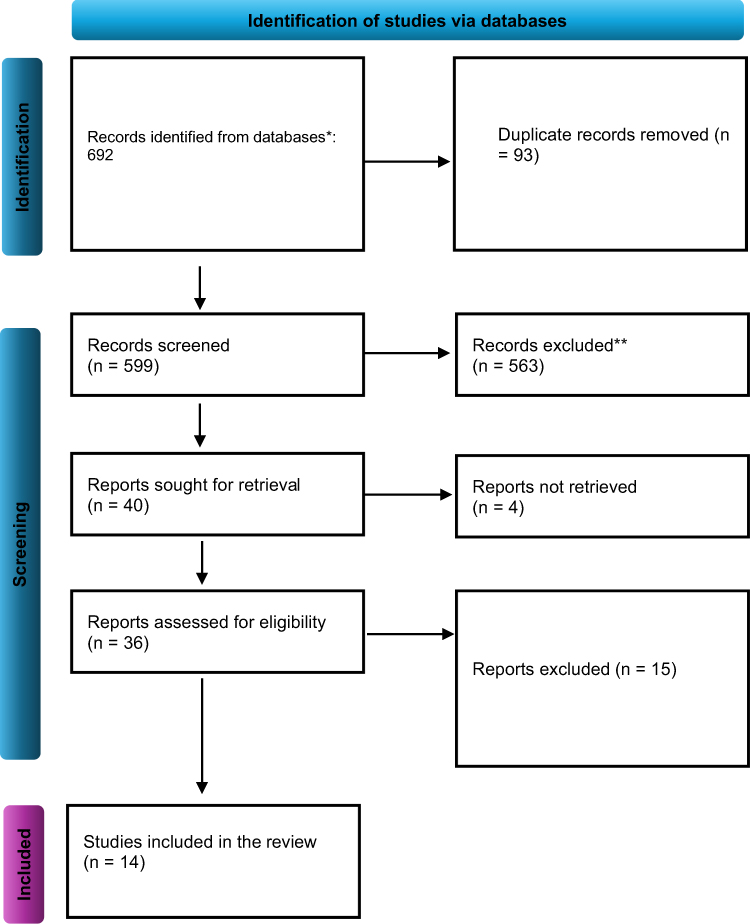 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram illustrating the studies’ selection process. Notes: This figure was adapted from Page, Matthew J., et al “The PRISMA 2020 statement: an updated guideline for reporting systematic reviews”. bmj 372 (2021). https://doi.org/10.1136/bmj.n71. * The studies were identified from the databases. ** The studies were excluded after the initial screening. |
Data Extraction
Two reviewers independently extracted prespecified fields: study design, setting, sample size, inclusion criteria, HFNC settings, comparator, follow-up and quantitative outcomes (PaCO2, pH, intubation, treatment failure, length of stay, exacerbation rate, quality of life). Discrepancies were resolved by consensus (Table 1).
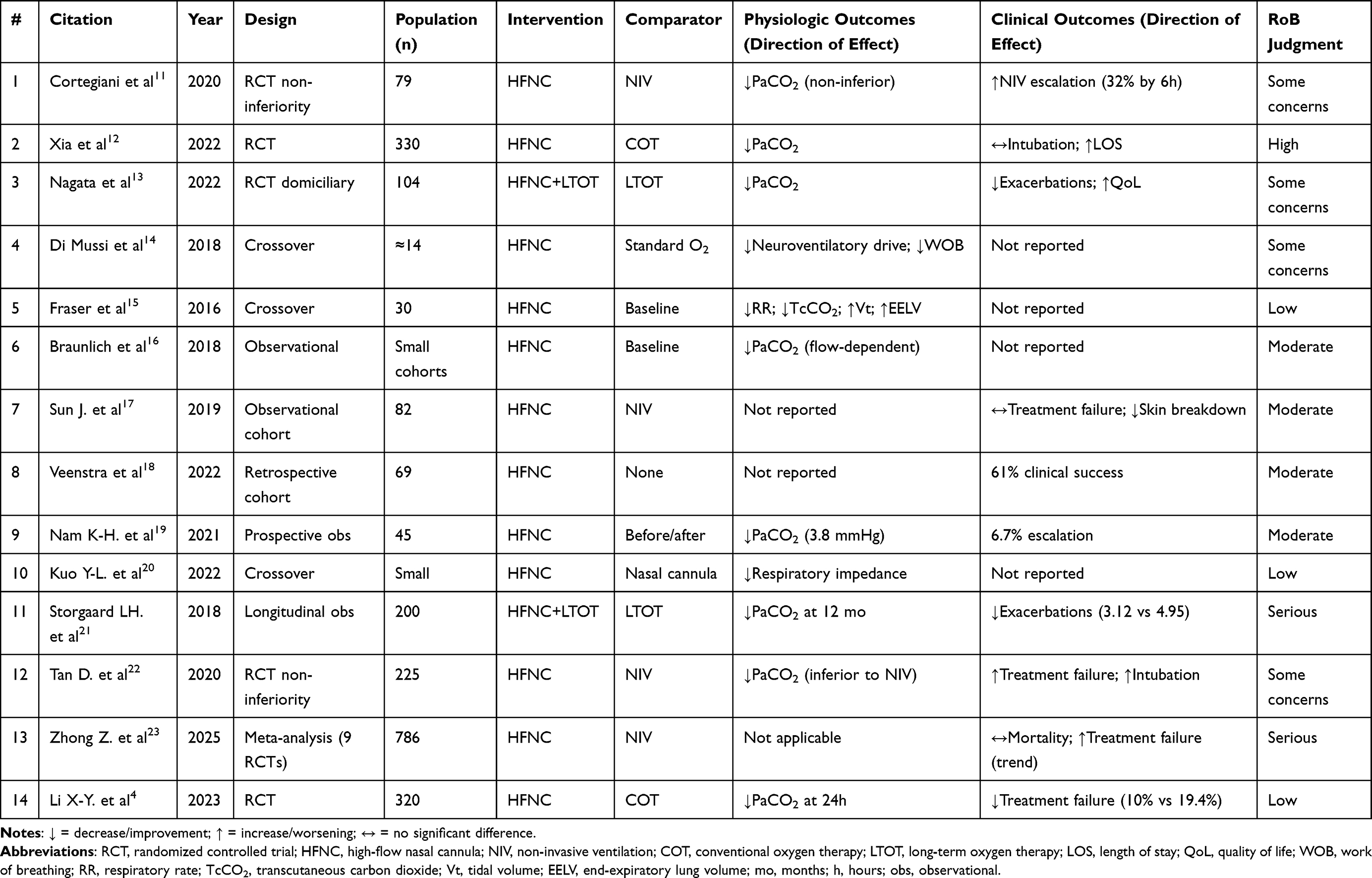 |
Table 1 Characteristics of Included Studies on High-Flow Nasal Cannula (HFNC) in COPD Exacerbation |
Risk of Bias Assessment
Design-appropriate tools were applied. Randomized trials were evaluated using Cochrane RoB 2, crossover trials with RoB 2-crossover, and non-randomized studies with ROBINS-I. Each study received a global judgment as low, some concerns, moderate, serious, or high risk of bias (Table 2).
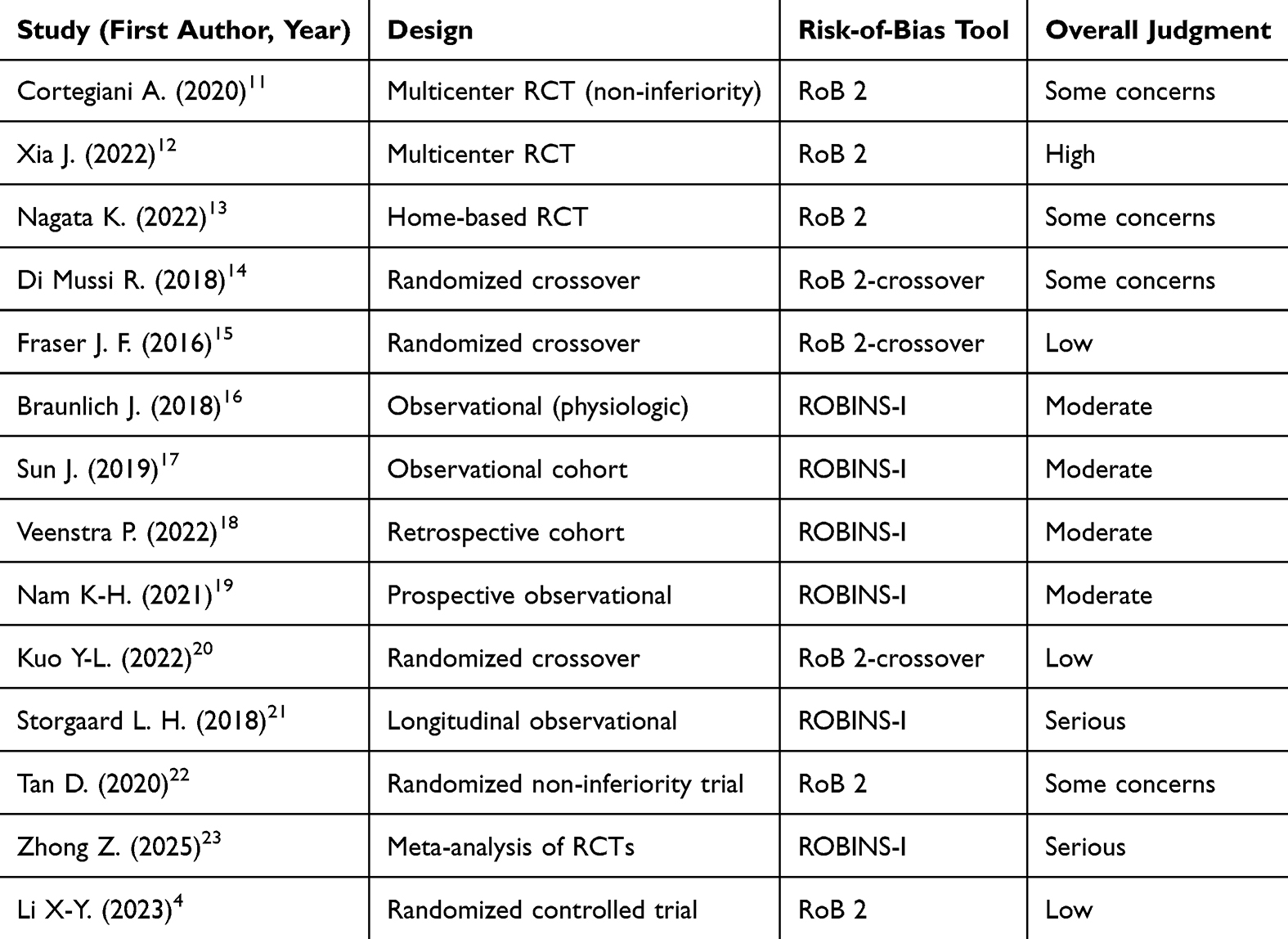 |
Table 2 Risk of Bias of Included Studies (n=14) |
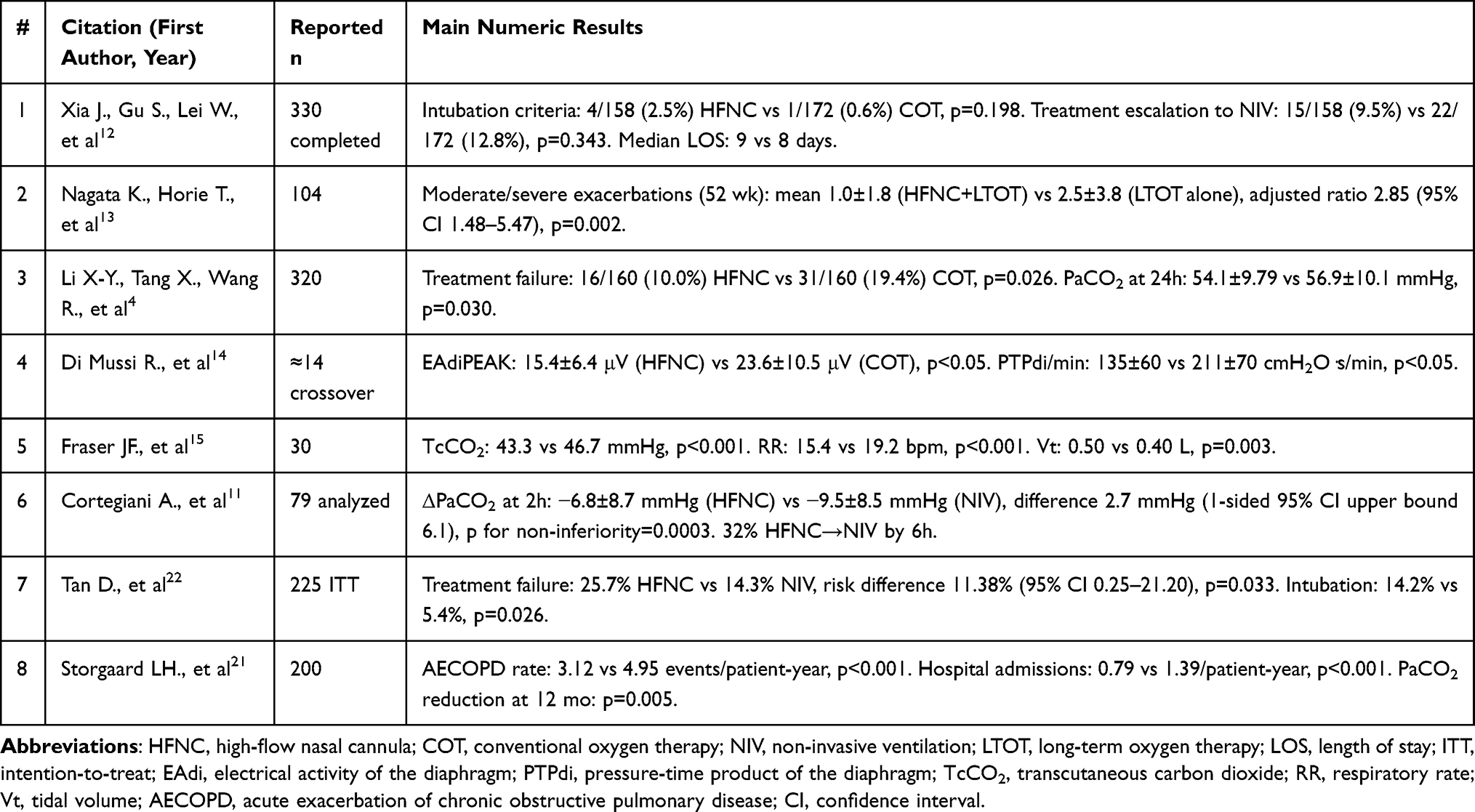 |
Table 3 Primary Findings of Selected Studies |
Data Synthesis and Analysis
Given heterogeneity in disease severity, HFNC protocols and comparators, formal meta-analysis was not performed. Reported pooled estimates from existing reviews are summarized. Studies were stratified by setting: (1) acute in-hospital COPD exacerbation, (2) post-extubation support, and (3) domiciliary long-term therapy. Quantitative emphasis was placed on direction and magnitude of physiological change (PaCO2, respiratory rate, end-expiratory lung volume [EELV]) and on clinically relevant outcomes: treatment failure, intubation, and exacerbation frequency. Sensitivity appraisal prioritized randomized evidence and crossover physiology studies (Table 3).
Methodological Limitations
Open-label designs, short follow-up intervals, and heterogeneous HFNC settings limit causal interpretation. Observational data are subject to confounding by indication, while underpowered RCTs constrain precision. These weaknesses informed a conservative synthesis and highlight the need for larger, protocol-standardized multicenter trials.
Results
Across fourteen studies, seven were randomized or crossover trials and seven observational (Table 1). Sample sizes ranged from small physiologic groups (n=10) to large multicenter trials (n>300). Most studies addressed acute or post-extubation hypercapnic COPD, while a smaller group examined long-term domiciliary use. Only two small physiologic trials met a low risk-of-bias standard. The larger randomized studies were often open-label, short in duration, and statistically underpowered. Observational work suffered from selection effects and inconsistent reporting.
Acute In-Hospital Studies: Physiologic Outcomes
High-flow nasal cannula (HFNC) shows consistent short-term physiologic benefit in COPD. Physiologic trials report reproducible reductions in CO2 and work of breathing. In a randomized crossover trial, Fraser et al15 found transcutaneous CO2 decreased from 46.7 to 43.3 mmHg (p<0.001), respiratory rate fell from 19.2 to 15.4 breaths per minute (p<0.001), tidal volume rose from 0.40 to 0.50 L (p=0.003), and EELV increased markedly (p<0.001). Di Mussi et al14 showed neuroventilatory drive (EAdi peak) fell from 23.6±10.5 μV to 15.4±6.4 μV and PTPdi/min fell from 211±70 to 135±60 cmH2O·s/min (p<0.05 for both).
Acute In-Hospital Studies: Clinical Outcomes
Clinical trials produce heterogeneous results that hinge on setting and patient severity. In controlled comparisons versus COT, Li et al4 reported reduced treatment failure at 24 hours with HFNC (16/160 [10.0%] versus COT 31/160 [19.4%], p=0.026) and lower PaCO2 at 24 hours (54.1±9.79 vs 56.9±10.1 mmHg, p=0.030). Xia et al12 enrolling patients with milder hypercapnia, found no significant reduction in intubation criteria during hospitalization (4/158 versus 1/172, p=0.198), and HFNC was associated with longer median length of stay (9 vs 8 days).
Comparisons with Non-Invasive Ventilation
Comparisons with NIV show caution is necessary. Cortegiani et al11 met a physiological non-inferiority margin for PaCO2 at two hours. Mean ΔPaCO2 was −6.8±8.7 mmHg with HFNC versus −9.5±8.5 mmHg with NIV. The absolute difference (2.7 mmHg) satisfied the prespecified non-inferiority bound (p for non-inferiority = 0.0003), but 32% of HFNC patients switched to NIV by six hours. Tan et al22 produced a larger randomized dataset. Treatment failure occurred in 25.7% with HFNC versus 14.3% with NIV. The risk difference (11.38%, 95% CI 0.25 to 21.20, p=0.033) exceeded the non-inferiority margin, so HFNC failed to demonstrate non-inferiority. Intubation rates were higher with HFNC (14.2% versus 5.4% with NIV, p=0.026).
Domiciliary HFNC
Domiciliary HFNC yields more consistent clinical advantages for chronic hypercapnic COPD. Nagata et al13 and Storgaard et al21 reported reduced exacerbation rates and improved quality of life (St. George’s Respiratory Questionnaire [SGRQ] mean difference −8.12, 95% CI −13.30 to −2.95). The meta-analysis by Pitre et al24 confirmed a pooled relative risk reduction in exacerbations (RR 0.77, 95% CI 0.66–0.89) and improvements in dyspnoea indices.
Discussion
The current body of evidence on HFNC in acute exacerbations of COPD (AECOPD) reveals a field in transition—from physiologic promise to cautious clinical application. Physiological studies consistently support HFNC’s capacity to improve ventilation mechanics, reduce inspiratory effort, and enhance carbon dioxide clearance compared with COT.14,15 The consistent reduction in transcutaneous CO2, diaphragmatic pressure-time product, and respiratory rate observed in crossover studies14,15 confirms that high-flow nasal cannula generates meaningful physiological unloading. These improvements are not merely statistical; the increased end-expiratory lung volume and reduced neuroventilatory drive indicate effective counteraction of dynamic hyperinflation, the core pathophysiological defect in acute exacerbations of COPD. By flushing anatomical dead space and providing low-level positive pressure, high-flow nasal cannula reduces the work of breathing at a level detectable by both electrical diaphragmatic activity and ventilatory pattern analysis, establishing a clear mechanistic rationale for clinical application. Short physiologic crossover trials provide a controlled signal supporting HFNC’s mechanistic effect. In randomized crossover settings, where each patient serves as their own control, HFNC consistently reduced transcutaneous CO2, respiratory rate, and diaphragmatic effort within hours of application.14,15 These short-duration studies isolate device-specific effects from disease variability and confirm that the observed improvements in ventilation and work of breathing are directly attributable to high-flow therapy rather than clinical progression. However, their brief time horizon and small sample sizes limit extrapolation to sustained clinical outcomes such as intubation or mortality, reinforcing that physiologic benefit alone is insufficient to establish equivalence with NIV in more severe exacerbations.
Despite these mechanistic advantages, the translation to clinically significant outcomes is inconsistent. Meta-analyses demonstrate modest mean PaCO2 reduction and a reduction in treatment failure versus COT, yet they fail to show meaningful benefit in mortality or intubation.12–19,24–26 The lack of statistical difference despite physiologic improvement suggests that HFNC is most effective in borderline cases—patients with mild hypercapnia or moderate exacerbations who do not yet need ventilatory assistance.4
In contrast, when compared with NIV, HFNC demonstrates both its clinical limits and its patient-centered strengths. NIV remains superior for controlling hypercapnia and preventing intubation in moderate to severe exacerbations.22 Data demonstrate that HFNC’s physiologic benefit does not equate to ventilatory efficacy. NIV remains the intervention of choice for acute hypercapnic respiratory failure, while HFNC serves as a comfort-oriented adjunct, suitable when NIV is contraindicated, poorly tolerated, or being weaned.11
Comfort, tolerance, and patient interface outcomes are consistently superior with HFNC. Yang et al25 found that HFNC reduced interface-related skin breakdown by nearly half compared with NIV (RR 0.52, 95% CI 0.39–0.69). Sun et al17 corroborated this, reporting fewer airway interventions and lower rates of pressure injury with HFNC. Improved tolerance allows longer continuous use, potentially stabilizing patients who would otherwise fail COT. However, this comfort advantage must be weighed against delayed escalation risk—patients may appear clinically stable while ventilation deteriorates.
Beyond acute management, HFNC demonstrates a more consistent role in chronic or domiciliary settings. Long-term studies indicate that nightly HFNC use reduces the frequency of moderate and severe exacerbations and improves quality-of-life scores.13–21,24–26 The chronic benefit likely arises from sustained washout of anatomical dead space, reduced CO2 retention during sleep, and improved mucociliary clearance—mechanisms less dependent on immediate ventilatory drive.27–29
Limitations
Several limitations must be acknowledged. At the study level, most included trials had small sample sizes, short follow-up durations (often 24–72 hours for acute studies), and heterogeneous HFNC settings (flow rates ranging 30–60 L/min, variable FiO2 titration protocols). Open-label designs are common due to the inability to blind patients and clinicians to device type, introducing performance bias. Observational studies are subject to confounding by indication, where sicker patients may preferentially receive NIV. At the review level, we did not perform a meta-analysis due to substantial clinical and methodological heterogeneity across studies. Furthermore, the absence of standardized outcome definitions—particularly for “treatment failure” and “escalation criteria”—limits comparability across trials. Ongoing controversies remain regarding optimal patient selection, flow titration protocols, and long-term safety, which await resolution in larger, adequately powered multicenter RCTs.
Conclusion
In summary, HFNC holds a defined but selective place in COPD management. It is superior to COT for mild-to-moderate exacerbations, offering physiological relief and improved comfort. It does not, however, match the efficacy of NIV in severe hypercapnic episodes and should not be used as its substitute in that context. Safety considerations require close monitoring of PaCO2 and work of breathing, with predefined escalation criteria to prevent delayed intubation. Its most promising role appears to be in domiciliary therapy for stable, chronically hypercapnic COPD, where it meaningfully reduces exacerbations and improves patient well-being. Further large-scale randomized trials are needed to identify patient profiles that benefit most and to standardize its application in both acute and chronic settings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang Z, Lin J, Liang L, et al. Global, regional, and national burden of chronic obstructive pulmonary disease and its attributable risk factors from 1990 to 2021: an analysis for the global burden of disease study 2021. Respir Res. 2025;26(1):2. doi:10.1186/s12931-024-03051-2
2. Fettal N. The impact of exacerbations COPD on respiratory function and quality of life. Res Rev. 2024. doi:10.52845/CMRO/2024/7-5-6
3. Roberto C, Valdés P, Lenoir A, Nicod L, Perez C. COPD exacerbation and prevention. Cardiovasc Med. 2017;20(02):38–8.
4. Li XY, Tang X, Wang R, et al. High-flow nasal cannula versus conventional oxygen therapy in acute exacerbation of COPD: a randomized controlled trial. Crit Care. 2023;27(1):112. doi:10.1186/s13054-023-04388-8
5. Sharma S, Danckers M, Sanghavi DK, Chakraborty RK. High-flow nasal cannula. StatPearls. 2023.
6. Zantah M, Pandya A, Jacobs MR, Criner GJ. The mechanisms of benefit of high-flow nasal therapy in stable COPD. J Clin Med. 2020;9(12):3832. doi:10.3390/jcm9123832
7. Piquilloud L, Olivier PY, Richard JC, et al. High flow nasal cannula improves breathing efficiency and ventilatory ratio in COPD patients recovering from an exacerbation. J Crit Care. 2022;69:154023. doi:10.1016/j.jcrc.2022.154023
8. Bruni A, Garofalo E, Procopio D, et al. Current practice of high flow through nasal cannula in exacerbated COPD patients. Healthcare. 2022;10(3):536. doi:10.3390/healthcare10030536
9. Rittayamai N, Phuangchoei P, Tscheikuna J, Praphruetkit N, Brochard L. Effects of high-flow nasal cannula and non-invasive ventilation on inspiratory effort in hypercapnic patients with COPD. Ann Intensive Care. 2019;9(1):122. doi:10.1186/s13613-019-0597-5
10. Cong L, Zhou L, Liu H, Wang J. Outcomes of high-flow nasal cannula versus non-invasive positive pressure ventilation for patients with acute exacerbations of COPD. Int J Clin Exp Med. 2019;12(8):10863–10867.
11. Cortegiani A, Longhini F, Madotto F, et al. High-flow nasal therapy versus noninvasive ventilation as initial ventilatory strategy in COPD exacerbation: a multicenter non-inferiority randomized trial. Crit Care. 2020;24:692. doi:10.1186/s13054-020-03409-0
12. Xia J, Gu S, Lei W, et al. High-flow nasal cannula versus conventional oxygen therapy in acute COPD exacerbation with mild hypercapnia: a multicenter randomized controlled trial. Crit Care. 2022;26:109. doi:10.1186/s13054-022-03973-7
13. Nagata K, Horie T, Chohnabayashi N, et al. Home high-flow nasal cannula oxygen therapy for stable hypercapnic COPD: a randomized clinical trial. Am J Respir Crit Care Med. 2022;206:1326–1335. doi:10.1164/rccm.202201-0199OC
14. Di Mussi R, Spadaro S, Stripoli T, et al. High-flow nasal cannula oxygen therapy decreases post-extubation neuroventilatory drive and work of breathing in patients with chronic obstructive pulmonary disease. Crit Care. 2018;22:180. doi:10.1186/s13054-018-2107-9
15. Fraser JF, Spooner AJ, Dunster KR, Anstey CM, Corley A. Nasal high flow oxygen therapy in patients with COPD reduces respiratory rate and tissue CO2 while increasing tidal and end-expiratory lung volumes: a randomized crossover trial. Thorax. 2016;71(8):759–761. doi:10.1136/thoraxjnl-2015-207962
16. Bräunlich J, Mauersberger F, Wirtz H. Effectiveness of nasal high-flow in hypercapnic COPD patients is flow- and leakage-dependent. BMC Pulm Med. 2018;18:14. doi:10.1186/s12890-018-0576-x
17. Sun J, Wang Y, Ling B, et al. High-flow nasal cannula oxygen therapy versus non-invasive ventilation for chronic obstructive pulmonary disease with acute-moderate hypercapnic respiratory failure. Int J Chron Obstruct Pulmon Dis. 2019;14:1229–1237. doi:10.2147/COPD.S206567
18. Veenstra P, Veeger NJGM, Koppers RJH, Duiverman ML, van Geffen WH. High-flow nasal cannula oxygen therapy for admitted COPD-patients: a retrospective cohort study. PLoS One. 2022;17(10):e0272372. doi:10.1371/journal.pone.0272372
19. Nam K-H, Kang HK, Lee SS, et al. Effects of high-flow nasal cannula in patients with mild to moderate hypercapnia: a multicentre prospective observational study. Acute Crit Care. 2021;36(3):249–255. doi:10.4266/acc.2020.01102
20. Kuo YL, Chien CL, Ko HK, et al. High-flow nasal cannula improves respiratory impedance evaluated by impulse oscillometry in COPD patients: a randomised controlled trial. Sci Rep. 2022;12(1):6981. doi:10.1038/s41598-022-10873-x
21. Storgaard LH, et al. Long-term effects of high-flow nasal cannula in COPD patients with chronic hypoxemic respiratory failure. Randomized Trial. 2018.
22. Tan D, Walline JH, Ling B, et al. High-flow nasal cannula oxygen therapy versus non-invasive ventilation for COPD patients after extubation: a multicenter, randomized controlled trial. Crit Care. 2020;24(1):489. doi:10.1186/s13054-020-03214-9
23. Zhong Z, Zhao L, Zhao Y, Li R, Xia S. Comparison of clinical outcomes between high-flow nasal cannula and non-invasive ventilation in acute exacerbation of COPD: a meta-analysis of randomized controlled trials. BMC Pulm Med. 2025;25(1):405. doi:10.1186/s12890-025-03873-w
24. Pitre T, Abbasi S, Su J, Mah J, Zeraatkar D. Home high-flow nasal cannula for chronic hypercapnic respiratory failure in COPD: a systematic review and meta-analysis. Respir Med. 2023;219:107420. doi:10.1016/j.rmed.2023.107420
25. Yang H, Huang D, Luo J, et al. The use of high-flow nasal cannula in patients with chronic respiratory disease — systematic review. Heart Lung. 2023;60:116–126. doi:10.1016/j.hrtlng.2023.02.016
26. Zhang L, Li S, Ye Y, et al. Comparison of high-flow nasal cannula with conventional oxygen therapy in patients with hypercapnic COPD: systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2023;18:895–906. doi:10.2147/COPD.S402506
27. Qin J, Wang G, Liao Y, Shang W, Han D. High flow nasal therapy versus noninvasive ventilation for AECOPD with acute hypercapnic respiratory failure: a meta-analysis of randomized controlled trials. Ann Intensive Care. 2025;15(1):64. doi:10.1186/s13613-025-01480-w
28. Colaianni-Alfonso N, Herrera F, Flores D, et al. Physiological effects and clinical evidence of high-flow nasal cannula during acute exacerbation in COPD patients: a narrative review. J Intensive Med. 2024;5(2):127–133. doi:10.1016/j.jointm.2024.10.005
29. Sabir L, Wharton L, Goodacre S. Retrospective single-centre descriptive study of the characteristics, management and outcomes of adult patients with suspected sepsis in the emergency department. Emerg Med J. 2022;39(4):272–278. doi:10.1136/emermed-2020-211111
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
High-Flow Nasal Cannula Oxygen Therapy versus Non-Invasive Ventilation for AECOPD Patients After Extubation: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Feng Z, Zhang L, Yu H, Su X, Shuai T, Zhu L, Chen D, Liu J
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1987-1999
Published Date: 30 August 2022
Comparison of High-Flow Nasal Cannula with Conventional Oxygen Therapy in Patients with Hypercapnic Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Zhang L, Wang Y, Ye Y, Gao J, Zhu F, Min L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:895-906
Published Date: 16 May 2023