Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Comparative Performance of Stereotactic Body Radiotherapy and Lenvatinib in Unresectable Hepatocellular Carcinoma Complicated by Portal Vein Tumor Thrombosis: A Propensity Score-Matched Cohort Analysis
Authors Huang J, Liu FC, Yang Y, Yuan SX, Gu FM, Jiang BG, Pan ZY
Received 26 December 2025
Accepted for publication 5 June 2026
Published 15 June 2026 Volume 2026:13 589137
DOI https://doi.org/10.2147/JHC.S589137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Jian Huang, Fu-Chen Liu, Yun Yang, Sheng-Xian Yuan, Fang-Ming Gu, Bei-Ge Jiang, Ze-Ya Pan
The Third Department of Hepatic Surgery, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, Shanghai, 201805, People’s Republic of China
Correspondence: Ze-Ya Pan, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, No. 700, Moyu North Road, Jiading, Shanghai, People’s Republic of China, Tel +86-13391236437, Email [email protected] Bei-Ge Jiang, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, No. 700, Moyu North Road, Jiading, Shanghai, People’s Republic of China, Tel +86-13764561303, Email [email protected]
Purpose: To investigate whether adding stereotactic body radiotherapy (SBRT) to lenvatinib improves outcomes for patients with unresectable hepatocellular carcinoma (uHCC) and portal vein tumor thrombosis (PVTT).
Methods: This retrospective cohort study enrolled 133 cases of uHCC with PVTT treated with either lenvatinib plus SBRT (n = 65) or lenvatinib alone (n = 68) between 2021 and 2023. To minimize baseline imbalances, 1:1 propensity score matching (PSM, caliper width, 0.02) was performed. The primary endpoints were overall survival (OS) and progression-free survival (PFS).
Results: Across the full study population, patients receiving lenvatinib in combination with SBRT experienced significantly longer median OS relative to those who received lenvatinib alone (24.7 vs 16.4 months; HR=0.521, 95% CI: 0.338– 0.802, p = 0.003). A similar advantage was observed for PFS (13.0 vs 8.6 months; HR=0.494, 95% CI: 0.335– 0.728, p < 0.0001). These findings remained consistent after PSM, with hazard ratios of 0.589 for OS and 0.540 for PFS. The objective response rate was also substantially higher in the combination arm than in the monotherapy arm (55.4% vs 30.9%, p = 0.004). Subgroup analyses revealed that the survival advantage was confined to patients with Cheng’s type I–II PVTT, whereas no significant benefit was observed in those with type III–IV disease. Furthermore, salvage hepatectomy was an independent protective factor for survival in 33 cases (24.8%), with a significantly higher conversion rate in the combined treatment group (30.8%). Both treatment groups had comparable and manageable safety profiles.
Conclusion: Lenvatinib in combination with SBRT confers meaningful advantages in both survival and tumor response over lenvatinib monotherapy in individuals with uHCC and PVTT, particularly among those with Cheng’s type I–II involvement. Moreover, this multimodal approach appears to be an effective strategy for achieving tumor downstaging and enabling subsequent salvage hepatectomy.
Keywords: hepatocellular carcinoma, portal vein tumor thrombus, lenvatinib, stereotactic body radiotherapy, survival
Introduction
As the sixth most common disease to be diagnosed and the third-ranking cause of cancer-associated mortality, hepatocellular carcinoma (HCC) remains a significant global health burden.1 Portal vein tumor thrombosis (PVTT) is detected in approximately 44–62.2% of HCC cases at diagnosis.2 The occurrence of PVTT contributes to the development of portal hypertension and progressive hepatic dysfunction. Moreover, it provides a key pathway for intrahepatic tumor spread, resulting in a median survival between 2.7 and 4.0 months when untreated.3
There is ongoing discussion on the best course of treatment for HCC complicated by PVTT. These cases are considered advanced-stage disease according to the Barcelona Clinic Liver Cancer (BCLC) system, and systemic therapy is recommended.4 In comparison, guidelines in the Asia-Pacific region support a more aggressive, multidisciplinary treatment strategy that may include transarterial chemoembolization (TACE), radiotherapy, and even surgical resection in some cases.5 With the advent of molecularly targeted treatments, lenvatinib, a multi-kinase inhibitor, has been recognized as a first-line standard therapy following the pivotal REFLECT trial, which showed non-inferior overall survival (OS) and a significantly higher objective response rate (ORR) compared with sorafenib.6 In patients with macrovascular invasion, however, the therapeutic gains achieved with systemic monotherapy are frequently limited, and ORR remain unsatisfactory. In addition, although TACE is commonly applied, its effectiveness against PVTT is constrained by the thrombus’s dual blood supply. At the same time, ischemia-triggered increases in vascular endothelial growth factor (VEGF) levels may paradoxically promote tumor progression.7,8
Moreover, HCC with PVTT can now be effectively treated locoregionally with stereotactic body radiation therapy (SBRT). By administering high, ablative radiation doses with steep dose fall-off, SBRT can promote portal vein recanalization and achieve favorable local tumor control while minimizing injury to surrounding normal liver tissue.9 Recent evidence suggests that, in carefully selected patients, SBRT can provide survival outcomes comparable to and in some cases better than those achieved with sorafenib or lenvatinib monotherapy.10,11 From a mechanistic perspective, combining lenvatinib with SBRT is supported by a strong biological rationale: SBRT promotes immunogenic tumor cell death and reduces local tumor burden, whereas lenvatinib normalizes tumor vasculature and inhibits the angiogenic rebound triggered by radiation, thereby potentially producing synergistic anti-tumor effects.12
Despite its strong theoretical rationale, robust clinical evidence directly comparing the combined use of lenvatinib and SBRT with lenvatinib alone, particularly in real-world settings that incorporate TACE-based comprehensive treatment, remains limited. Furthermore, the effectiveness of this combined approach in achieving tumor downstaging and facilitating subsequent salvage hepatectomy remains unclear. Therefore, this retrospective cohort study was performed to compare survival outcomes, tumor response, and treatment-related safety between lenvatinib plus SBRT and lenvatinib monotherapy in cases of unresectable HCC (uHCC) with PVTT.
Materials and Methods
Participants
Individuals with uHCC and PVTT who had undergone treatment at the Eastern Hepatobiliary Surgery Hospital between January 2021 and December 2023 were enrolled in this retrospective cohort study. Inclusion criteria: (1) aged ≥ 18 years; (2) clinical or pathological diagnosis of HCC based on the EASL or Chinese clinical guidelines for the management of hepatocellular carcinoma; (3) disease considered unresectable at initial evaluation by a multidisciplinary team, due to tumor burden, vascular invasion, insufficient future liver remnant, inadequate hepatic reserve, or technical infeasibility of curative resection; (4) presence of uHCC with PVTT confirmed through independent imaging assessments by two radiologists; (5) a minimum of one lesion measurable by the modified Response Evaluation Criteria in Solid Tumors (mRECIST);13 (6) an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1; and (7) maintained hepatic function, which is classified as Child-Pugh class A without refractory ascites or hepatic encephalopathy. Exclusion criteria: (1) presence of extrahepatic spread, including invasion of adjacent organs, lymph node involvement, or distant metastasis; (2) a current or prior diagnosis of another malignancy; (3) previous exposure to systemic therapy for HCC; (4) Child–Pugh class B or C liver function, ECOG performance status >1, or severe comorbidities precluding the planned treatment; (5) a history of prior radiotherapy to the liver; or (6) incomplete clinical data or failure to complete follow-up. The Declaration of Helsinki’s (1964) ethical guidelines and its subsequent amendments were followed for conducting the study. The Institutional Review Board of Eastern Hepatobiliary Surgery Hospital (Shanghai) granted ethical approval for this study (No. EHBHKY2020-K-010). All participants signed written informed consent forms. A detailed research flowchart is presented in Figure 1.
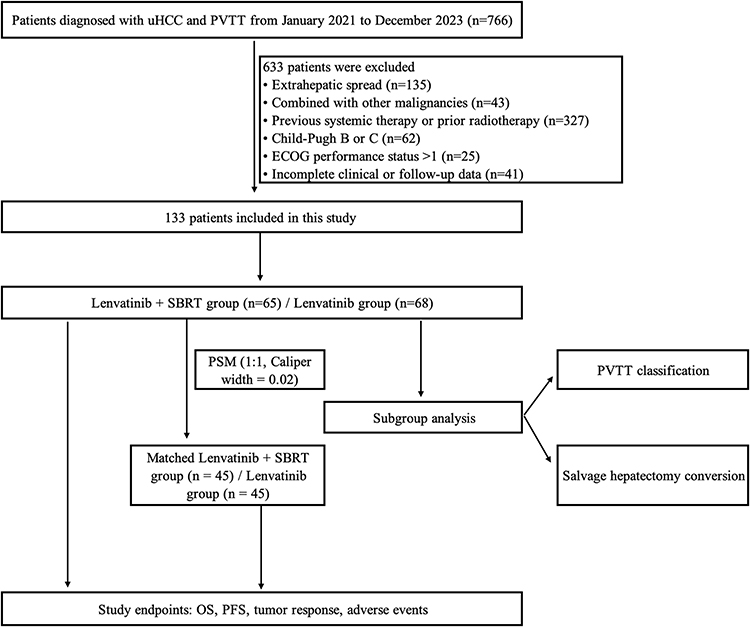 |
Figure 1 Research flowchart of the study. Abbreviations: uHCC, unresectable hepatocellular carcinoma; PVTT, portal vein tumor thrombosis; SBRT, stereotactic body radiotherapy; PSM, propensity score matching; OS, overall survival; PFS, progression-free survival; ECOG, Eastern Cooperative Oncology Group. |
Data Collection
Before treatment initiation, baseline patient information was systematically collected. Recorded variables included: (1) demographic data, comprising age and sex; (2) clinical characteristics, including the underlying etiology of liver disease and the presence of cirrhosis; (3) virological indicators, namely hepatitis B surface antigen and DNA; (4) tumor biomarkers, including serum alpha-fetoprotein (AFP) and protein induced by vitamin K absence or antagonist-II (PIVKA-II); and (5) hepatic function, evaluated using the albumin–bilirubin (ALBI) score, calculated as (log10 bilirubin [μmol/L] × 0.66) + (albumin [g/L] × −0.085),14 along with other routine biochemical parameters.
Two radiologists independently confirmed the diagnosis of PVTT based on distinctive features on contrast-enhanced computed tomography (CT) or magnetic resonance imaging (MRI). The degree of PVTT was classified using Cheng’s system,15 specifically: type I, involvement of the segmental branches of the portal vein or more distal vessels; type II, thrombus within the right or left portal vein; type III, extension into the main portal vein trunk; and type IV, invasion of the superior mesenteric vein.
Lenvatinib Treatment
All patients received oral lenvatinib once daily at weight-adjusted doses in accordance with the REFLECT trial protocol: 8 mg for those < 60 kg and 12 mg for those > 60 kg.6 Dose reductions were applied in response to treatment-related toxicities until adverse events (AEs) were mitigated or resolved. When AEs persisted despite dose modification, lenvatinib was temporarily discontinued until clinical improvement occurred. In addition, a subset of patients was treated with concurrent programmed death-1 (PD-1) inhibitors administered every three weeks, based on decisions reached through multidisciplinary team (MDT) discussions.
TACE Procedures
TACE represents a cornerstone of multidisciplinary therapy for advanced HCC.16 In the present study, patients with hypervascular tumors and no contraindications routinely received TACE as an initial intervention. To further strengthen local tumor control, SBRT was subsequently combined with TACE based on a comprehensive evaluation of PVTT classification, hepatic functional reserve, and overall tumor burden. A catheter was introduced into the hepatic artery via the femoral artery and progressed selectively or superselectively into the tumor-feeding arteries to execute TACE using the Seldinger technique. An emulsion containing appropriate doses of chemotherapy drugs (fluorouracil, epirubicin, and a platinum compound) and embolic materials (Lipiodol and gelatin sponge) was then infused through the catheter. Chemotherapy dosing was individually tailored according to tumor characteristics, body surface area (BSA), and the patient’s general condition.
SBRT Treatment
TACE was generally administered before SBRT as initial locoregional therapy, and the interval between TACE and SBRT was determined by liver function recovery and multidisciplinary assessment. SBRT was subsequently delivered to the PVTT and/or primary lesion to enhance local control.
SBRT was delivered using the CyberKnife robotic radiosurgery system with 6-MV photons. During treatment, patients were positioned supine with their arms alongside their bodies and immobilized using a vacuum-based fixation system. For radiation planning, contrast-enhanced CT images were obtained at a slice thickness of 1.5 mm. The target volumes and organs at risk (OARs) were contoured by radiation oncologists. MRI, 18F-FDG PET-CT, or contrast-enhanced CT was used to calculate the gross tumor volume (GTV). In this investigation, the standard GTV included both the thrombus within the portal vein and the primary HCC lesion.
However, in patients with extensive tumor burden, advanced cirrhosis, or multiple intrahepatic metastases, the GTV was limited to the PVTT alone. The GTV was enlarged by 3–5 mm laterally and anteroposteriorly to establish the planning target volume (PTV), with modifications made to reduce exposure to nearby OARs. Treatment planning and dose determination were customized for each patient by senior radiation oncologists. Over five to ten fractions, the total recommended radiation dose ranged from 30 to 58 Gy. In view of the established association between higher biologically effective dose (BED) and improved local tumor control, the treatment strategy aimed to administer the highest safely tolerable dose while strictly complying with the OAR dose limits recommended by the American Association of Physicists in Medicine (AAPM) TG-101 guidelines.17
End Point
Progression-free survival (PFS) and OS were the primary outcomes. PFS represented the interval between the start of treatment to death (all-cause) or radiographically verified disease progression, as determined by RECIST version 1.1, while OS was considered the interval between start of treatment and death (all-cause). Secondary outcome measures focused on tumor response, categorized as complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The ORR represented the proportion of patients achieving either CR or PR, whereas the disease control rate (DCR) included patients with CR, PR, or SD. The Common Terminology Criteria for Adverse Events (CTCAE) version 5.0 was used to assess and grade treatment-related AEs.18
Follow-Up
Tumor response was evaluated at 6–8-week intervals using CT or MRI, with additional imaging performed whenever clinical manifestations suggested possible disease progression. Every follow-up visit included routine laboratory testing, and serum tumor indicators, including AFP and PIVKA-II, were routinely checked. Patients who fulfilled the criteria for tumor downstaging subsequently underwent radical surgical resection followed by postoperative adjuvant therapy after providing informed consent. Lenvatinib was stopped for one week, and PD-1 inhibitors for one month prior to and following surgery to improve perioperative safety. The final follow-up for the entire cohort was completed in September 2024.
Statistical Analysis
Data were analyzed using SPSS 26.0 and R software (version 4.2.2). Moreover, graphs were produced using GraphPad Prism version 9.0. Categorical variables are summed up as counts and percentages, while continuous data are displayed as medians with matching ranges. Categorical variables were compared using Pearson’s chi-square test (with Yates’ continuity correction applied for 2×2 tables) or Fisher’s exact test, as appropriate. Kaplan-Meier curves and Log rank tests were applied to evaluate and compare survival data. Univariate and multivariate Cox proportional hazards regression was utilized to investigate potential prognostic factors. Specifically, due to its critical clinical significance and the high proportion of utilization (57.9%), the concurrent use of PD-1 inhibitors (ICIs) was forced into the multivariate Cox models to adjust for potential confounding effects. Propensity score matching (PSM) was performed in R using a 1:1 optimal matching without replacement and a caliper width of 0.02 to reduce selection bias arising from baseline confounding variables. A p-value < 0.05 was regarded as statistically significant, and tests were two-sided.
Results
Baseline Features of Patients with PVTT Who Have Incurable HCC
One hundred and thirty-three individuals with HCC and PVTT were enrolled; Table 1 summarizes their baseline characteristics. The cohort was overwhelmingly male (93.2%), and most patients (76.7%) were 60 years of age or younger. In a total of 86.5% of instances of liver disease, infection by hepatitis B virus (HBV) was the cause, with 28.6% of patients having an HBV DNA level ≥2000IU/mL. Liver cirrhosis was documented in 52.6% of the population, while 39.8% showed preserved hepatic function classified as ALBI grade 1. Regarding tumor biomarkers, elevated serum AFP levels (≥400μg/L) were observed in 73 patients (54.9%), and increased PIVKA-II levels (>400mAU/mL) were detected in 86 patients (64.7%). Regarding tumor burden, 52.6% of patients presented with a solitary lesion, and 36.8% had tumors exceeding 10 cm in diameter. According to Cheng’s classification, type I–II PVTT constituted 75.9% of all cases. The majority of patients (90.2%) received TACE, and 77 individuals (57.9%) were treated with PD-1 inhibitors at the treating physician’s discretion. After conversion therapy, 33 patients (24.8%) achieved successful downstaging and subsequently underwent salvage hepatectomy.
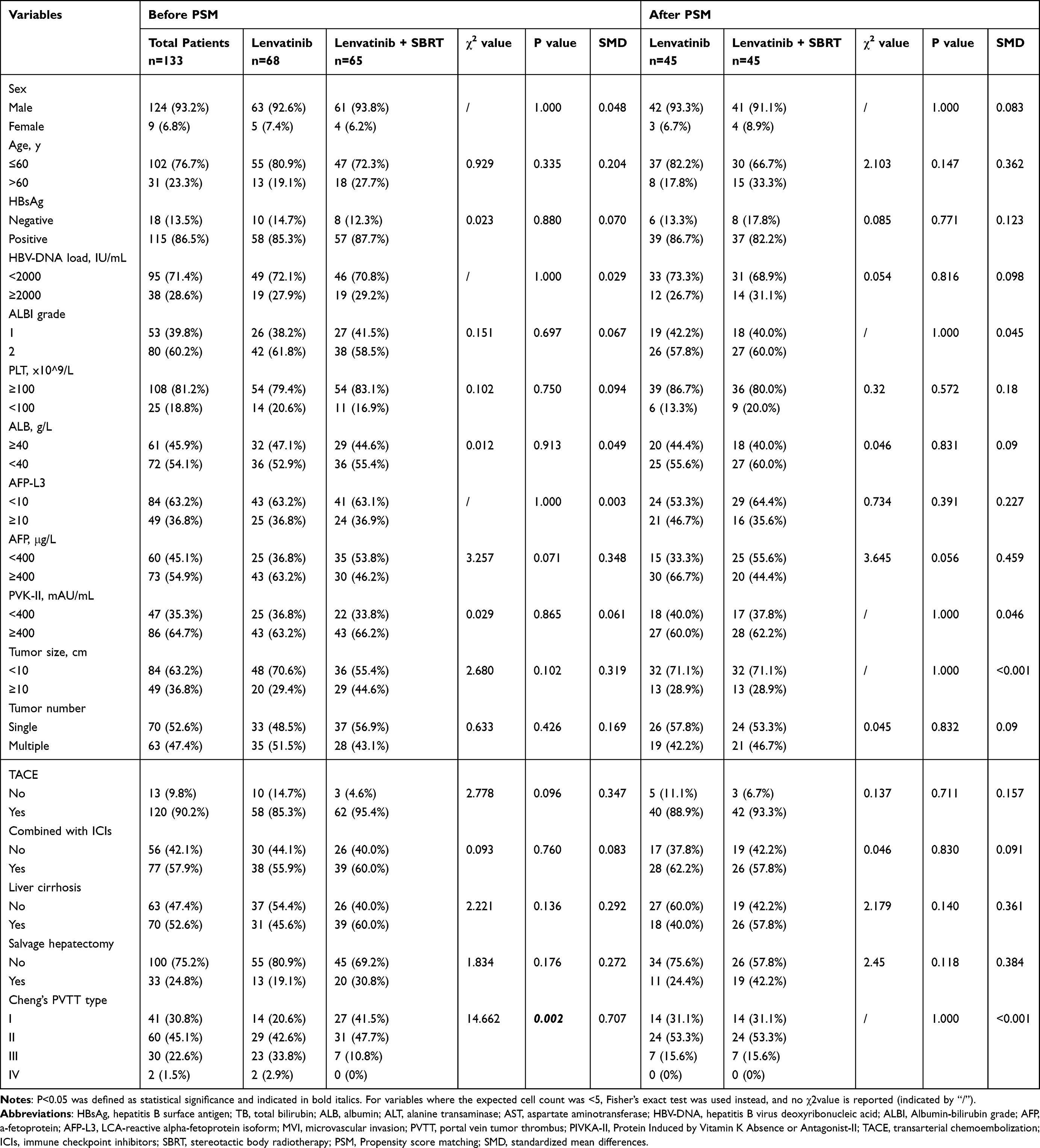 |
Table 1 Baseline Characteristics of Unresectable HCC Patients with PVTT |
Before PSM, 65 participants received lenvatinib combined with SBRT, whereas 68 received lenvatinib alone. Except for Cheng’s PVTT classification, baseline clinical characteristics, such as TACE use and PD-1 inhibitor use, were largely similar between the two groups. In particular, relative to those receiving monotherapy, the combination group contained a higher proportion of individuals with type I and II PVTT and a lower percentage with type III and IV disease. To minimize potential confounding, a 1:1 PSM was subsequently applied. After matching, there were 45 patients in the combination group and 45 in the lenvatinib monotherapy group. The baseline features of the groups were comparable, as detailed in Table 1.
Treatment Response
Across the full cohort, CR was observed in 13 patients (9.8%), PR in 44 patients (33.1%), SD in 30 patients (22.6%), and PD in 46 patients (34.6%). Accordingly, the ORR was 42.9% (n = 57), and the DCR reached 65.4% (n = 87, Table 2).
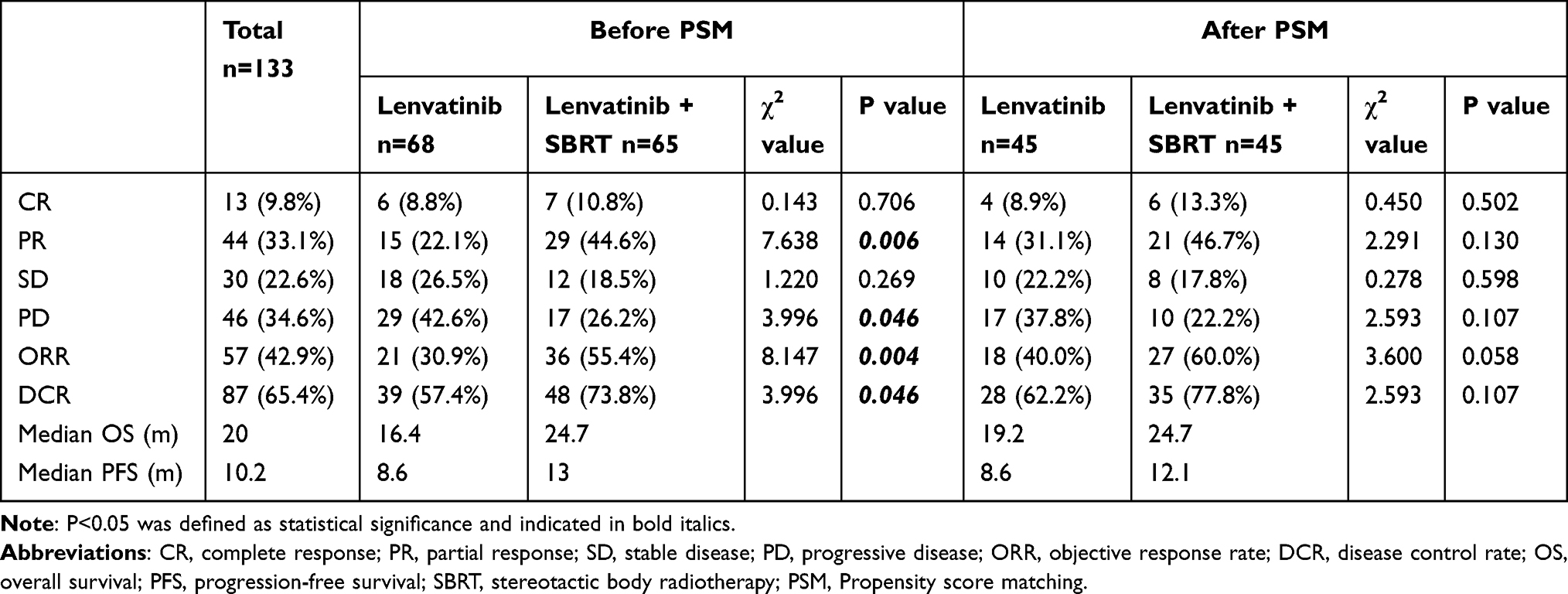 |
Table 2 Best Tumor Response in All Patients |
The ORR was considerably greater in the lenvatinib and SBRT group than in the lenvatinib monotherapy group in subgroup analyses carried out before PSM (55.4% vs 30.9%, p = 0.004). Similarly, the DCR was substantially higher in the combination group than in the monotherapy group (73.8% vs 57.4%, p = 0.046). On the other hand, treatment with lenvatinib alone was linked to higher PD incidence relative to the combined regimen (42.6% vs 26.2%, p = 0.046). After PSM, although the combination group maintained a numerically higher ORR (60.0% vs 40.0%), the difference did not reach statistical significance (p=0.058). Likewise, no significant differences were observed in DCR or PD rates between the two groups post-matching (both p=0.107).
Survival Outcomes
The median follow-up of the overall cohort was 31 months (range: 2–45 months). The cumulative 1-, 2-, and 3-year OS rates for the entire cohort were 74.3%, 40.7%, and 15.3%, respectively; the corresponding PFS rates were 42.2%, 15.8%, and 12.8% (Figure 2A and Figure 2B). For both cohorts, the median OS and PFS rates were 20.0 and 10.2 months, respectively.
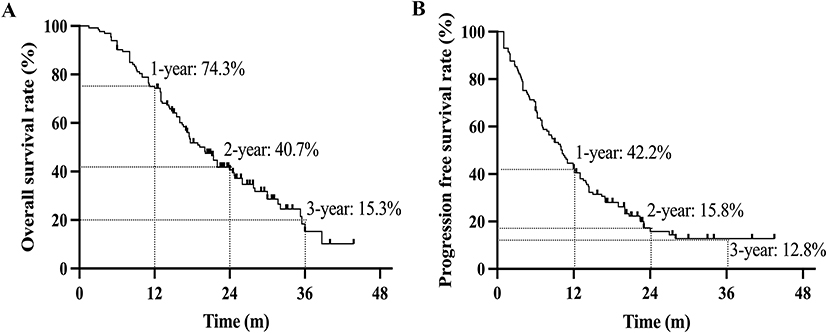 |
Figure 2 Kaplan-Meier analysis of survival in the overall cohort of patients with uHCC and PVTT. (A) Overall survival (OS). (B) Progression-free survival (PFS). Abbreviations: uHCC, unresectable hepatocellular carcinoma; PVTT, portal vein tumor thrombus. |
Participants who received combined lenvatinib and SBRT demonstrated markedly superior survival outcomes relative to those receiving lenvatinib alone. The median OS in the combination cohort was 24.7 months, substantially longer than the 16.4 months observed in the monotherapy group. The 1-, 2-, and 3-year OS rates were 81.5%, 48.6%, and 36.8% in the combination arm, versus 67.3%, 31.4%, and 3.7% in the monotherapy arm (HR = 0.521, 95% CI: 0.338–0.802, p = 0.003; Figure 3A). Consistent advantages were also observed in PFS, with a median PFS of 13.0 months in the combination group relative to 8.6 months in the monotherapy group. The 1-, 2-, and 3-year PFS rates were 54.7%, 26.9%, and 23.5% for patients receiving lenvatinib plus SBRT, compared with 29.4%, 5.4%, and 2.7% for those treated only with lenvatinib (HR = 0.494, 95% CI: 0.335–0.728, p < 0.0001; Figure 3B).
 |
Figure 3 Survival outcomes comparing lenvatinib plus SBRT versus lenvatinib monotherapy. Kaplan-Meier curves for (A) overall survival (OS) and (B) progression-free survival (PFS) in the full cohort before propensity score matching (PSM). Kaplan-Meier curves for (C) OS and (D) PFS in the cohort after PSM. Abbreviation: SBRT, stereotactic body radiotherapy. |
After PSM to adjust for baseline imbalances, the survival advantage associated with the combined regimen remained robust. The lenvatinib plus SBRT group continued to demonstrate significantly superior OS (HR = 0.589, 95% CI: 0.355–0.978, p = 0.040; Figure 3C) and PFS (HR = 0.540, 95% CI: 0.334–0.860, p = 0.008; Figure 3D) in the matched cohort.
OS and PFS Independent Risk Factors for the Whole Cohort
To rigorously address potential confounders, particularly the concurrent administration of PD-1 inhibitors, multivariate Cox proportional hazards modeling was performed. Multivariate analysis for OS demonstrated that Cheng’s classification of PVTT was an independent adverse prognostic factor (HR = 1.573, 95% CI: 1.156–2.141, p = 0.004). In contrast, both salvage hepatectomy and SBRT were independently associated with favorable survival outcomes (HR = 0.502, 95% CI: 0.284–0.888, p = 0.018; and HR = 0.613, 95% CI: 0.389–0.967, p = 0.035, respectively). Notably, although forced into the model due to its clinical relevance, the concurrent use of ICIs did not emerge as an independent prognostic factor for OS (HR = 1.151, 95% CI: 0.736–1.801, p = 0.537). Cheng’s PVTT type remained independently predictive of PFS, with a similar pattern (HR = 1.521, 95% CI: 1.165–1.985, p = 0.002). Conversely, salvage hepatectomy (HR = 0.585, 95% CI: 0.363–0.945, p = 0.029) and SBRT (HR = 0.613, 95% CI: 0.406–0.926, p = 0.020) were confirmed as independent factors protecting against progression, even after adjusting for ICIs use (HR = 1.107, 95% CI: 0.745–1.645, p = 0.615) (Table 3).
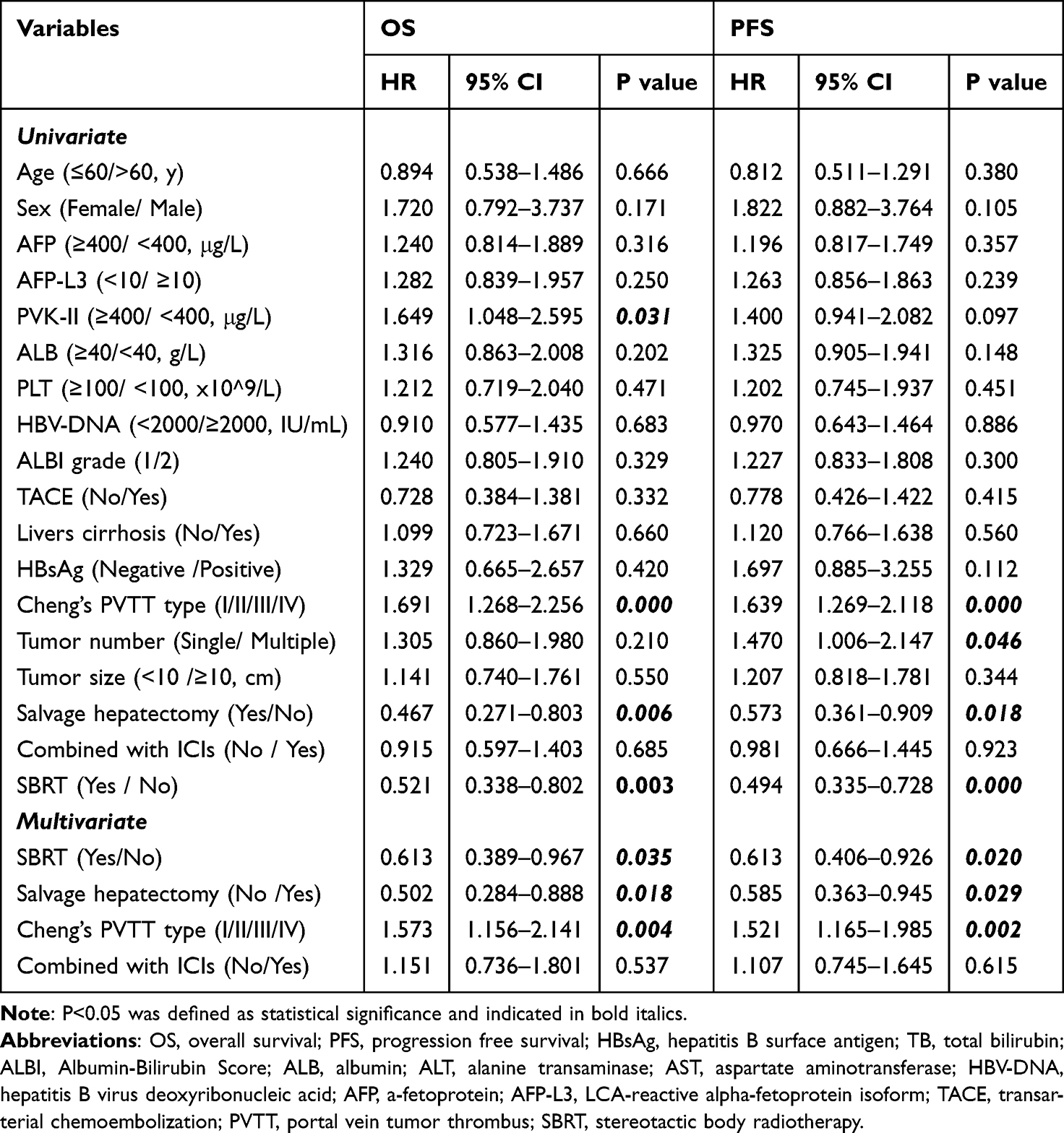 |
Table 3 Univariate and Multivariate Analysis of the Total Patients for OS and PFS |
AE Assessment
The overall safety profile was acceptable, as outlined in Table 4. All treatment-associated AEs could be managed, and no treatment-linked mortality was observed. The most commonly reported AEs of any grade were hepatic dysfunction (36.8%), fever (19.5%), loss of appetite (16.5%), hypertension (13.5%), cutaneous rash (10.5%), and abdominal pain (9.8%). Overall, 16.5% of individuals had grade 3 or higher toxicities; the most common serious events were hepatic dysfunction (4.5%), gastrointestinal hemorrhage (3.0%), hypertension (2.3%), and proteinuria (2.3%). Importantly, no significant difference in AEs incidence was observed between the lenvatinib plus SBRT group and the lenvatinib monotherapy group.
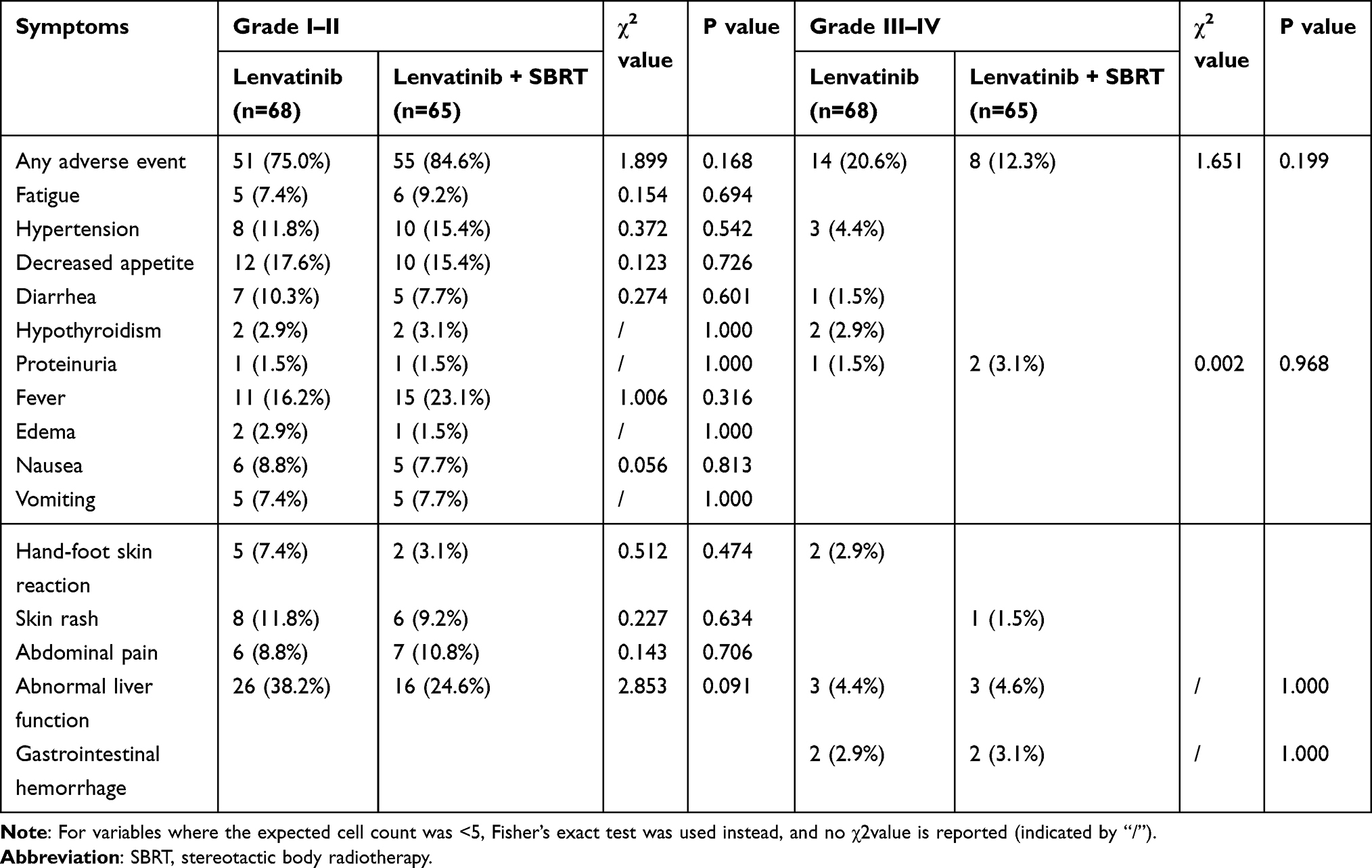 |
Table 4 Adverse Events |
Survival Analysis by Tumor Response
Prognostic outcomes were further analyzed according to tumor response status. Patients who attained an objective response in the lenvatinib + SBRT cohort showed markedly longer OS and PFS than those with no response to therapy (both p < 0.001; Figure 4A and B). A similar pattern was noted in the lenvatinib monotherapy group, in which responders similarly showed significantly superior survival outcomes compared with non-responders (both p < 0.05; Figure 5A and B).
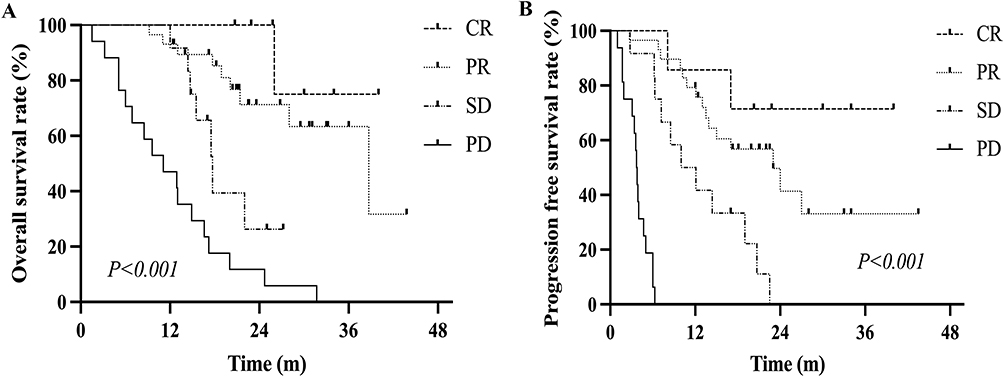 |
Figure 4 Survival outcomes stratified by tumor response in the lenvatinib plus SBRT group. (A) Overall survival (OS). (B) Progression free survival (PFS). |
 |
Figure 5 Survival outcomes stratified by tumor response in the lenvatinib monotherapy group. (A) Overall survival (OS). (B) Progression free survival (PFS). |
Subgroup Analysis by PVTT Classification
Multivariate modeling confirmed Cheng’s classification of PVTT as independently predictive of unfavorable prognosis. In the Cheng’s type I–II PVTT subgroup, individuals treated with lenvatinib plus SBRT showed markedly longer OS relative to those receiving lenvatinib alone (26.0 vs 19.2 months; HR = 0.521, 95% CI: 0.319–0.853), along with superior median PFS (13.9 vs 9.6 months; HR = 0.547, 95% CI: 0.344–0.871) (Figure 6A and B). On the other hand, neither the median OS (13.0 vs 11.0 months; HR = 0.903, 95% CI: 0.345–2.368) nor the median PFS (4.0 vs 6.5 months; HR = 0.608, 95% CI: 0.259–1.429) of individuals with Cheng’s type III–IV PVTT (Figure 6C and D).
 |
Figure 6 Subgroup analysis of survival outcomes based on Cheng’s classification of PVTT. (A) Overall survival (OS) and (B) progression-free survival (PFS) in patients with Cheng’s type I–II PVTT. (C) OS and (D) PFS in patients with Cheng’s type III–IV PVTT. Abbreviation: PVTT, Portal Vein Tumor Thrombus. |
Survival Outcomes of Salvage Hepatectomy
Overall, 33 patients proceeded to salvage hepatectomy after a median duration of 4.0 months (range, 2.2–7.7 months) from the start of conversion therapy. The median OS and RFS for this surgery subgroup were 30.0 and 10.2 months, respectively. The comparable 1- and 2-year RFS rates were 44.7% and 25.8%, respectively, whereas the cumulative 1-, 2-, and 3-year OS rates were 87.9%, 62.3%, and 13.2% (Figure 7A and B).
 |
Figure 7 Survival outcomes for patients who underwent salvage hepatectomy. (A) Overall survival (OS). (B) Recurrence free survival (RFS). |
Among the 33 patients who underwent salvage hepatectomy, 20 (30.8%) were in the lenvatinib plus SBRT cohort, and 13 (19.1%) were in the lenvatinib monotherapy cohort. In the combination therapy arm, individuals who received salvage hepatectomy had substantially longer survival than those who did not (p = 0.039; Figure 8A). In comparison, within the lenvatinib monotherapy group, survival outcomes did not differ between individuals who received salvage hepatectomy and those who did not (Figure 8B).
 |
Figure 8 Overall survival (OS) after salvage hepatectomy, stratified by initial treatment. Kaplan-Meier curves for patients initially treated with (A) lenvatinib plus SBRT or (B) lenvatinib monotherapy. |
Discussion
In patients with incurable HCC complicated by PVTT, we compared the safety profile and therapeutic efficacy of lenvatinib plus SBRT to lenvatinib alone in this retrospective investigation. Compared with monotherapy, the data clearly show that the combined regimen was associated with significant improvements in both OS and PFS. In addition, patients receiving lenvatinib plus SBRT achieved higher objective response and disease control rates, and these advantages in survival and tumor response remained consistent after PSM. Importantly, multivariate analyses confirmed SBRT and subsequent salvage hepatectomy as independent protective factors for survival. At the same time, advanced PVTT (Cheng’s type III–IV) emerged as a strong independent indicator of unfavorable prognosis.
The synergistic interaction between SBRT and lenvatinib may be explained by several complementary biological mechanisms. As a multi-kinase inhibitor, lenvatinib suppresses angiogenic and oncogenic signaling pathways mediated by VEGFR1–3, FGFR1–4, PDGFR, RET, and KIT.19 Beyond direct anti-angiogenic effects, lenvatinib has also been shown to remodel the tumor immune microenvironment by reducing tumor-associated macrophages and enhancing CD8+ T-cell infiltration, thereby potentially improving antitumor immune activation.20,21
SBRT, in contrast, provides highly conformal ablative irradiation with steep dose fall-off, allowing potent local tumor destruction while sparing surrounding liver parenchyma. In patients with HCC complicated by PVTT, this local effect is particularly important because PVTT is a major driver of intrahepatic dissemination, portal hypertension, and hepatic functional deterioration. Beyond direct cytotoxicity, radiotherapy can induce immunogenic tumor cell death, promote the release of tumor-associated antigens and damage-associated molecular patterns, enhance antigen presentation, and facilitate T-cell priming, thereby potentially converting an immunologically “cold” tumor microenvironment into a more inflamed and treatment-responsive state.22
The combination of SBRT and lenvatinib may therefore create a reciprocal and reinforcing therapeutic interaction. On one hand, lenvatinib-mediated vascular normalization may improve tumor oxygenation and radiosensitivity. On the other hand, radiotherapy may induce compensatory upregulation of VEGF and other pro-angiogenic mediators, which can promote tumor revascularization, regrowth, and metastatic spread after irradiation.23 Lenvatinib may counteract this radiation-induced angiogenic rebound, thereby sustaining the local tumor control achieved by SBRT. In addition, lenvatinib-mediated immune microenvironment remodeling may further amplify radiotherapy-induced antitumor immunity. This mechanistic rationale is consistent with the broader development of combination strategies in HCC. Tong et al recently summarized that HCC is characterized by poor immune cell infiltration and a strongly immunosuppressive tumor microenvironment, which limits the efficacy of immune checkpoint inhibitor monotherapy. They further emphasized that combination approaches integrating immune checkpoint inhibitors with targeted therapy and local treatment modalities represent a promising strategy to overcome immune resistance and enhance antitumor activity.24 In this context, the survival benefit observed in our cohort may reflect not only improved local control of PVTT by SBRT but also a broader therapeutic interaction among radiotherapy, lenvatinib-mediated vascular and immune modulation, and, in some patients, concurrent PD-1 blockade.
Our clinical findings are consistent with this mechanistic framework. The combination group achieved a markedly higher ORR than the lenvatinib monotherapy group before PSM (55.4% vs 30.9%) and maintained a numerically higher ORR after PSM (60.0% vs 40.0%). Moreover, even after adjusting for clinically relevant confounders, including concurrent use of ICIs, SBRT remained an independent protective factor for both OS and PFS. These results support the hypothesis that adding SBRT to lenvatinib provides clinically meaningful benefit through enhanced local tumor control and potential systemic biological synergy.
Importantly, in the current treatment landscape of advanced HCC, immunotherapy has become a cornerstone of comprehensive management. In our real-world cohort, a substantial proportion of patients (57.9%) received concurrent PD-1 inhibitors, and this use was well-balanced between the two groups. By incorporating ICI administration into our multivariate Cox regression models, we confirmed that the survival advantage conferred by SBRT is an independent prognostic factor, rather than a mere reflection of confounding from immunotherapy. This finding is highly relevant to the broader context of modern oncology, underscoring that even in the era of potent systemic and immune combinations, robust locoregional interventions like SBRT remain crucial for managing disease drivers such as PVTT and maximizing overall survival.
Our survival data further underscore the clinical value of incorporating radiotherapy into the treatment paradigm for advanced HCC. Systemic monotherapy for HCC with macrovascular invasion has historically been associated with poor efficacy; the sub-analysis of the REFLECT trial revealed a median OS of approximately 13.6 months with Lenvatinib.6 Our study’s median OS in the monotherapy arm of 16.4 months is in line with this earlier data. Importantly, the addition of SBRT markedly prolonged median OS to 24.7 months, a result consistent with several recent investigations. For instance, a meta-analysis by Li et al indicated that, as compared to tyrosine kinase inhibitors (TKIs) monotherapy, the combination of radiation plus TKIs led to substantially enhanced OS and PFS in individuals with advanced HCC.25 Similarly, in patients with HCC and PVTT, lenvatinib plus SBRT offered better survival advantages than lenvatinib alone, with tolerability, according to another comparative trial.26 Collectively, our findings confirm that, even in the current era in which lenvatinib is established as first-line therapy, integrating SBRT into a multidisciplinary treatment strategy that includes TACE continues to yield meaningful survival advantages in real-world clinical practice.
A crucial finding of our study is the differential benefit of combination therapy based on PVTT extent. Moreover, subgroup analyses demonstrated that the survival benefit associated with SBRT was confined to individuals with Cheng’s type I–II PVTT and was not evident in those with type III–IV disease. Here, it was found that the degree of vascular invasion is critical in determining therapeutic efficacy. In cases of limited PVTT, SBRT can precisely target and recanalize the thrombus, restore portal venous flow, and achieve sustained local control,26,27 thereby enhancing the systemic effectiveness of lenvatinib. In comparison, when thrombi extend into the main portal vein trunk or the superior mesenteric vein (type III–IV), the tumor burden may exceed the effective range of SBRT, or the required radiation field may pose an unacceptable risk of radiation-induced liver injury.28 This observation highlights the need for appropriate patient selection. It suggests the existence of a “therapeutic ceiling” for locoregional interventions in the setting of extensive disease, a conclusion consistent with prior studies identifying main portal vein invasion as a major adverse prognostic factor.29
The clinical relevance of our findings lies in demonstrating that an intensive combined treatment approach can effectively act as a bridge to potentially curative surgical intervention. In our series, 24.8% of patients were successfully downstaged and proceeded to salvage hepatectomy. Importantly, the survival advantage associated with surgery was observed exclusively in the lenvatinib plus SBRT group. This suggests that the robust local tumor control achieved by SBRT, together with the systemic anti-tumor effects of lenvatinib, creates more favorable conditions for complete surgical resection and improved long-term postoperative outcomes. This observation was further supported by multivariate analysis, which identified salvage hepatectomy as independently protective for both OS (HR = 0.519, p = 0.022) and PFS (HR = 0.599, p = 0.033). These results are in line with an expanding body of evidence indicating that conversion from unresectable to resectable HCC represents one of the most effective strategies for achieving durable long-term survival.30,31
The study has several limitations. Initially, the retrospective structure and single-center setting fundamentally introduce the potential for selection bias, despite the application of strict inclusion criteria. Second, the therapeutic strategy was not fully standardized, as TACE and PD-1 inhibitor administration were determined by clinical judgment, resulting in treatment heterogeneity. Although such an approach reflects real-world practice, it complicates the precise isolation of the therapeutic contribution attributable specifically to the lenvatinib–SBRT combination. Given that most patients received TACE as part of comprehensive treatment, we cannot fully exclude a potential synergistic effect between TACE and SBRT. However, TACE use was balanced between groups, and the survival advantage associated with adding SBRT persisted after adjustment for baseline confounders, suggesting that SBRT contributed independently to the observed benefit. In addition, the SBRT target volume was not fully uniform across the combination group, because in some patients the GTV included both the primary tumor and PVTT, whereas in others it was limited to PVTT alone due to extensive disease burden or limited hepatic reserve. This heterogeneity may have influenced local treatment intensity and complicates interpretation of the treatment effect attributable to SBRT. Another important limitation is the lack of translational correlative analyses. Because this was a retrospective real-world study, tumor tissue, peripheral immune cell profiling, cytokine levels, PD-L1 expression, and angiogenesis-related biomarkers were not systematically collected. Therefore, we were unable to directly validate the proposed immunologic and angiogenic mechanisms underlying the synergy between SBRT and lenvatinib. Future prospective studies should incorporate serial biomarker assessment and immune profiling to clarify the biological basis of this combined strategy. Third, the overall sample size, particularly in subgroup analyses, was limited, potentially reducing statistical power in detecting differences among cases with Cheng’s type III–IV PVTT. Finally, although treatment-related toxicities were generally manageable and no unexpected safety signals were observed, long-term adverse effects, especially radiation-induced liver disease (RILD), warrant further evaluation through extended follow-up.
Conclusion
For participants with unresectable HCC complicated by PVTT, especially those with Cheng’s type I–II involvement, this study offers strong real-world evidence that lenvatinib plus SBRT provides definite advantages over lenvatinib alone. This combined strategy not only enhances tumor response and prolongs survival but also successfully downstages a meaningful proportion of patients, thereby creating an opportunity for curative-intent salvage hepatectomy. Collectively, these findings advocate for a more intensive, multidisciplinary treatment approach in appropriately selected patients with advanced HCC and highlight the necessity for future prospective, randomized trials to validate these results and further refine patient selection.
Abbreviations
uHCC, Unresectable hepatocellular carcinoma; PVTT, portal vein tumor thrombosis; SBRT, stereotactic body radiotherapy; OS, overall survival; PFS, progression-free survival; BCLC, Barcelona Clinic Liver Cancer; TACE, Transarterial chemoembolization; ORR, objective response rate; VEGF, vascular endothelial growth factor; mRECIST, modified Response Evaluation Criteria in Solid Tumors; ECOG, Eastern Cooperative Oncology Group; AFP, alpha-fetoprotein; PIVKA-II, protein induced by vitamin K absence or antagonist-II; ALBI, albumin–bilirubin; CT, computed tomography; MRI, magnetic resonance imaging; AEs, adverse events; PD-1, programmed death-1 inhibitors; MDT, multidisciplinary team; GTV, gross tumor volume; PFS, progression-free survival; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease; DCR, disease control rate; PSM, propensity score matching; TKIs, tyrosine kinase inhibitors; RILD, radiation-induced liver disease.
Data Sharing Statement
Research data are not shared, owing to the privacy or ethical restrictions.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Eastern Hepatobiliary Surgery Hospital (No. EHBHKY2020-K-010), and all patients signed informed documents.
Consent for Publication
Written informed consent for publication was obtained from all participants.
Acknowledgments
Thank all the staff authors for their contributions in this study.
Funding
This study was supported by grants from the Open Project Program of Key Laboratory of Minimally Invasive Techniques & Rapid Rehabilitation of Digestive System Tumor of Zhejiang Province (21SZDSYS05), Youth Startup Fund Project of Naval Medical University (2022QN096) and Tengfei Project (TF2024XSYJ06).
Disclosure
The author reports no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–17. doi:10.3322/caac.21660
2. Lu J, Zhang XP, Zhong BY, et al. Management of patients with hepatocellular carcinoma and portal vein tumour thrombosis: comparing east and west. Lancet Gastroenterol Hepatol. 2019;4(9):721–730. doi:10.1016/S2468-1253(19)30178-5
3. Tao ZW, Cheng BQ, Zhou T, Gao YJ. Management of hepatocellular carcinoma patients with portal vein tumor thrombosis: a narrative review. Hepatobiliary Pancreat Dis Int. 2022;21(2):134–144. doi:10.1016/j.hbpd.2021.12.004
4. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
5. Xie DY, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2020;9(4):452–463. doi:10.21037/hbsn-20-480
6. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
7. Minagawa M, Makuuchi M. Treatment of hepatocellular carcinoma accompanied by portal vein tumor thrombus. World J Gastroenterol. 2006;12(47):7561–7567. doi:10.3748/wjg.v12.i47.7561
8. Han K, Kim JH. Transarterial chemoembolization in hepatocellular carcinoma treatment: barcelona clinic liver cancer staging system. World J Gastroenterol. 2015;21(36):10327–10335. doi:10.3748/wjg.v21.i36.10327
9. Bujold A, Massey CA, Kim JJ, et al. Sequential Phase I and II trials of stereotactic body radiotherapy for locally advanced hepatocellular carcinoma. J Clin Oncol. 2013;31(13):1631–1639. doi:10.1200/JCO.2012.44.1659
10. Ji X, Zhang A, Duan X, Wang Q. Stereotactic body radiotherapy versus lenvatinib for hepatocellular carcinoma with portal vein tumor thrombosis: a propensity matching score analysis. Radiat Oncol. 2024;19(1):143. doi:10.1186/s13014-024-02527-1
11. Chang WI, Kim BH, Kim YJ, Yoon JH, Jung YJ, Chie EK. Role of radiotherapy in Barcelona clinic liver cancer stage C hepatocellular carcinoma treated with sorafenib. J Gastroenterol Hepatol. 2022;37(2):387–394. doi:10.1111/jgh.15722
12. Zhu XD, Li KS, Sun HC. Adjuvant therapies after curative treatments for hepatocellular carcinoma: current status and prospects. Genes Dis. 2020;7(3):359–369. doi:10.1016/j.gendis.2020.02.002
13. Lencioni R, Llovet JM. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010;30(1):52–60. doi:10.1055/s-0030-1247132
14. Toyoda H, Johnson PJ. The ALBI score: from liver function in patients with HCC to a general measure of liver function. JHEP Rep. 2022;4(10):100557. doi:10.1016/j.jhepr.2022.100557
15. Chen ZH, Wang K, Zhang XP, et al. A new classification for hepatocellular carcinoma with hepatic vein tumor thrombus. Hepatobiliary Surg Nutr. 2020;9(6):717–728. doi:10.21037/hbsn.2019.10.07
16. Villanueva A. Hepatocellular Carcinoma. N Engl J Med. 2019;380(15):1450–1462. doi:10.1056/NEJMra1713263
17. Benedict SH, Yenice KM, Followill D, et al. Stereotactic body radiation therapy: the report of AAPM task group 101. Med Phys. 2010;37(8):4078–4101. doi:10.1118/1.3438081
18. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the common terminology criteria for adverse events (CTCAE - Version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr (Engl Ed). 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
19. Chen Y, Dai S, Cheng CS, Chen L. Lenvatinib and immune-checkpoint inhibitors in hepatocellular carcinoma: mechanistic insights, clinical efficacy, and future perspectives. J Hematol Oncol. 2024;17(1):130. doi:10.1186/s13045-024-01647-1
20. Kato Y. Lenvatinib enhances antitumor immunity of anti-PD-1 antibody. Int J Clin Oncol. 2025;30(4):666–673. doi:10.1007/s10147-025-02721-5
21. Kato Y, Tabata K, Kimura T, et al. Lenvatinib plus anti-PD-1 antibody combination treatment activates CD8+ T cells through reduction of tumor-associated macrophage and activation of the interferon pathway. PLoS One. 2019;14(2):e0212513. doi:10.1371/journal.pone.0212513
22. Formenti SC, Demaria S. Combining radiotherapy and cancer immunotherapy: a paradigm shift. J Natl Cancer Inst. 2013;105(4):256–265. doi:10.1093/jnci/djs629
23. Kioi M, Vogel H, Schultz G, Hoffman RM, Harsh GR, Brown JM. Inhibition of vasculogenesis, but not angiogenesis, prevents the recurrence of glioblastoma after irradiation in mice. J Clin Invest. 2010;120(3):694–705. doi:10.1172/JCI40283
24. Tong J, Tan Y, Ouyang W, Chang H. Targeting immune checkpoints in hepatocellular carcinoma therapy: toward combination strategies with curative potential. Exp Hematol Oncol. 2025;14(1):65. doi:10.1186/s40164-025-00636-5
25. Li H, Wu Z, Chen J, et al. External radiotherapy combined with sorafenib has better efficacy in unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Clin Exp Med. 2023;23(5):1537–1549. doi:10.1007/s10238-022-00972-4
26. Ji X, Xu Z, Sun J, Li W, Duan X, Wang Q. Lenvatinib with or without stereotactic body radiotherapy for hepatocellular carcinoma with portal vein tumor thrombosis: a retrospective study. Radiat Oncol. 2023;18(1):101. doi:10.1186/s13014-023-02270-z
27. Lee SM, Choi JH, Yoon JH, et al. Efficacy and safety of image-guided hypofractionated radiotherapy for hepatocellular carcinoma with portal vein tumor thrombosis: a retrospective, multicenter study. BMC Cancer. 2025;25(1):736. doi:10.1186/s12885-025-13739-3
28. Roquette I, Bogart E, Lacornerie T, et al. Stereotactic body radiation therapy for the management of hepatocellular carcinoma: efficacy and safety. Cancers (Basel). 2022;14(16):3892. doi:10.3390/cancers14163892
29. Chang Y, Yu SJ, Kim HC, et al. Reappraisal of portal vein tumor thrombosis as a prognostic factor for patients with hepatocellular carcinoma. Gut Liver. 2024;18(1):156–164. doi:10.5009/gnl230057
30. Zhu XD, Huang C, Shen YH, et al. Downstaging and resection of initially unresectable hepatocellular carcinoma with tyrosine kinase inhibitor and Anti-PD-1 antibody combinations. Liver Cancer. 2021;10(4):320–329. doi:10.1159/000514313
31. Zhu XD, Huang C, Shen YH, et al. Hepatectomy after conversion therapy using tyrosine kinase inhibitors plus anti-PD-1 antibody therapy for patients with unresectable hepatocellular carcinoma. Ann Surg Oncol. 2023;30(5):2782–2790. doi:10.1245/s10434-022-12530-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of the Efficacy and Safety of Transarterial Chemoembolization with or without Lenvatinib for Unresectable Hepatocellular Carcinoma: A Retrospective Propensity Score–Matched Analysis
Chen YX, Zhang JX, Zhou CG, Liu J, Liu S, Shi HB, Zu QQ
Journal of Hepatocellular Carcinoma 2022, 9:685-694
Published Date: 1 August 2022
Lenvatinib Induces Immunogenic Cell Death and Triggers Toll-Like Receptor-3/4 Ligands in Hepatocellular Carcinoma

Zhou C, Yang ZF, Sun BY, Yi Y, Wang Z, Zhou J, Fan J, Gan W, Ren N, Qiu SJ
Journal of Hepatocellular Carcinoma 2023, 10:697-712
Published Date: 24 April 2023
Application and Resistance Mechanisms of Lenvatinib in Patients with Advanced Hepatocellular Carcinoma
Tao M, Han J, Shi J, Liao H, Wen K, Wang W, Mui S, Li H, Yan Y, Xiao Z
Journal of Hepatocellular Carcinoma 2023, 10:1069-1083
Published Date: 10 July 2023
Lymphocyte-to-C Reactive Protein Ratio is an Independent Predictor of Survival Benefits for Hepatocellular Carcinoma Patients Receiving Radiotherapy
Shi Z, Zhu S, Jin Y, Qi L, Zhou M, Zhou Z, Zhang J, Liu B, Shen J
Journal of Hepatocellular Carcinoma 2024, 11:305-316
Published Date: 8 February 2024
Feasibility and Safety of the Clinical Outcomes of TACE Combined with Lenvatinib and PD-1 Blockades in the Treatment of Hepatocellular Carcinoma with Portal Vein Tumor Thrombus: A Retrospective Exploratory Study
Sun W, Liu Y, Wang L
International Journal of General Medicine 2024, 17:3627-3640
Published Date: 21 August 2024