Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Comparative Evaluation of CT and MRI in Detecting Intracranial and Extracranial Manifestations of Tuberous Sclerosis Complex
Authors He J, Deng LH ![]() , Wang K, Deng C
, Wang K, Deng C ![]() , Lai YM, Zeng Y
, Lai YM, Zeng Y
Received 3 August 2025
Accepted for publication 10 January 2026
Published 4 February 2026 Volume 2026:22 558051
DOI https://doi.org/10.2147/NDT.S558051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Jun He,1,* Li-Hua Deng,1,2,* Kang Wang,1 Chao Deng,1 Yuan-Mei Lai,1 Yan Zeng3
1Department of Radiology, The First People’s Hospital of Neijiang, Neijiang, Sichuan, People’s Republic of China; 2 7T Magnetic Resonance Imaging Translational Medical Center, Department of Radiology, Southwest Hospital, Army Medical University (Third Military Medical University), Chongqing, People’s Republic of China; 3Department of Ultrasound, The First People’s Hospital of Neijiang, Neijiang, Sichuan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Zeng, Department of Ultrasound, The First People’s Hospital of Neijiang, Neijiang, Sichuan, People’s Republic of China, Email [email protected]
Background: Tuberous sclerosis complex (TSC) is an autosomal dominant genetic disorder characterized by the formation of benign tumors in multiple organs. Neuroimaging plays a pivotal role in diagnosis and surveillance of intracranial and extracranial manifestations.
Objective: To evaluate and compare the diagnostic performance of CT and MRI in detecting intracranial and extracranial lesions associated with TSC.
Methods: A retrospective analysis was conducted on imaging data from 57 patients diagnosed with TSC. Cranial CT and routine MRI findings were reviewed and compared. In addition, abdominal and thoracic CT findings were evaluated for renal, hepatic, pulmonary, and skeletal involvement.
Results: Subependymal calcified nodules were observed in 51/57 (89.5%) patients, with a CT detection rate of 100% (46/46), significantly higher than routine MRI (68.4%, 13/19; P < 0.001). Cortical dysplasia lesions were found in 19/57 (33.3%) patients, with significant difference between CT (10/46, 21.7%) and routine MRI (16/19, 84.2%; P < 0.001). Subependymal giant cell astrocytoma (SEGA) lesions were detected in 11/19 (19.3%) cases with no statistical difference between CT (7/46, 15.2%) and routine MRI (6/19, 31.6%; P = 0.250). Cerebral fissure malformation and cranial bone dysplasia were detected in 3/57 (5.3%) and 2/57 (3.5%) patients, respectively. Extracranially, renal angiomyolipoma (AML) lesions were detected in 12/21 (57.1%) patients, hepatic AMLs in 5/21 (23.8%), multifocal micronodular pneumocyte hyperplasia (MMPH) lesions in 5/15 (33.3%), pulmonary lymphangioleiomyomatosis (LAM) lesions in 3/15 (20.0%), and multifocal bone sclerosis in 13/36 (36.1%) by CT.
Conclusion: CT and routine MRI demonstrated lesion-specific, complementary roles in TSC. CT preferentially identified calcified lesions and delineated extracranial multisystem involvement, whereas MRI offered an advantage in the detection of cortical dysplasia and other soft-tissue abnormalities. Integrating intracranial and extracranial imaging within a single cohort, this study supported a practical, modality-tailored CT–MRI approach for comprehensive assessment and risk-adapted surveillance in TSC.
Keywords: tuberous sclerosis complex, CT, MRI, comparative evaluation
Introduction
Tuberous Sclerosis Complex (TSC) is a rare autosomal dominant neurocutaneous syndrome, and currently, there is no radical cure available.1,2 The pathogenic genes associated with TSC are primarily TSC1 and TSC2, with approximately 12% of patients exhibiting TSC1 mutations and 73% having TSC2 mutations. Notably, around 15% of patients do not have identifiable mutations in TSC-related genes.3,4 It is generally accepted that mutations in TSC2 tend to more severe clinical phenotypes compared to TSC1 mutations.5,6 TSC affects multiple systems, including the central nervous system (CNS), liver, kidney, skin, lung, bone, heart and so on, leading to highly heterogeneous clinical presentations.7 Classic symptoms include epileptic seizure, intellectual disability, and facial angiofibroma, which are collectively as Vogt’s triad.8 The incidence rate of TSC is approximately 1/10,000, with about one-third of patients having a positive family history.9 The disease typically manifests before the age of 10, and tends to progress with age, making imaging crucial for early diagnosis, monitoring, and therapeutic evaluation.10–13
According to the 2021 Updated International Tuberous Sclerosis Complex Diagnostic Criteria and Surveillance and Management Recommendations,14 the diagnosis of TSC is categorized into clinical and genetic diagnosis, further highlighting the essential role of neuroimaging. Within this framework, imaging is central not only to achieving a definitive diagnosis through detailed lesion assessment but also to tracking lesion evolution, evaluating therapeutic efficacy, and detecting complications associated with increased morbidity.15 Accordingly, an imaging strategy that supports both intracranial evaluation and extracranial surveillance is essential in routine care.
In clinical practice, TSC may first present with neurological symptoms such as seizures, intellectual disability/developmental delay, or with extracranial manifestations related to renal, pulmonary, or skeletal involvement.16 Because clinically important complications can arise in different organs and at different ages, clinicians require imaging modalities that are accessible, repeatable, and informative for both diagnosis and follow-up. Computed tomography (CT) and magnetic resonance imaging (MRI) are the two most widely used cross-sectional techniques in TSC evaluation. However, their diagnostic yield may vary by organ system and lesion composition (eg, calcified versus non-calcified lesions and soft-tissue characterization), which creates a practical need to clarify how these modalities should be deployed and integrated in everyday management.
The imaging of TSC commonly demonstrates cortical/subcortical tubers, subependymal calcified nodules, cortical dysplasia, and subependymal giant cell astrocytoma (SEGA), whereas extracranial imaging may reveal renal and hepatic angiomyolipoma (AML), pulmonary lymphangioleiomyomatosis (LAM) or multifocal micronodular pneumocyte hyperplasia (MMPH), and sclerotic bone lesions.17–19 Despite these well-recognized imaging features, prior reports have often focused on isolated intracranial abnormalities or single-organ disease,17,20,21 and an integrated assessment spanning both intracranial and extracranial manifestations within a single cohort remains limited. Moreover, evidence that translates imaging findings into a practical, complementary CT–MRI strategy across lesion types and organ systems is still lacking. Therefore, in this retrospective study of 57 clinically diagnosed TSC patients, we innovatively applied both CT and MRI to systematically characterize multisystem involvement-including intracranial and extracranial manifestations in the same cohort, thereby evaluating the complementary roles and practical application patterns of these modalities in clinical assessment.
Materials and Methods
Clinic Data
Diagnostic Criteria
We performed a retrospective analysis of imaging data from 57 patients diagnosed with TSC between January 2021 and December 2024. All patients fulfilled the diagnostic criteria set forth by the 2012 International TSC Consensus Conference and were definitively diagnosed based on their clinical presentation, genetic testing results, or characteristic findings observed in imaging studies. Specifically, the diagnostic criteria are as follows:14,22 1) Two major features (such as cortical/subcortical tubers, subependymal nodules, renal AML, SEGA, cardiac rhabdomyomas, facial angiofibroma, shagreen patches); 2) One major feature and two minor features (such as hypomelanotic macules, skeletal lesions, multiple bone sclerosis, pulmonary LAM, retinal hamartomas, dental enamel pits); 3) A pathogenic mutation in TSC1 or TSC2 confirmed by genetic testing. Genetic testing for TSC1/TSC2 mutations was performed in a subset of patients when clinically indicated but was not routinely available for all cases and therefore was not systematically analyzed in this study.
Inclusion and Exclusion Criteria
Inclusion criteria were as follows: 1) patients who fulfilled the diagnostic criteria for TSC; 2) availability of cranial CT and/or routine brain MRI data of sufficient image quality for analysis; 3) complete clinical and imaging records.
Exclusion criteria included: 1) patients with incomplete or poor-quality imaging data that precluded reliable interpretation; 2) patients with intracranial lesions unrelated to TSC (eg, traumatic brain injury, infection, or other neoplastic diseases); 3) patients who had undergone prior neurosurgical intervention or treatment that significantly altered the native imaging appearance of TSC-related lesions.
Image Acquisition
CT Scanning
Cranial, thoracic, or abdominal CT scans were performed based on clinical indications, with or without contrast enhancement as needed. All examinations were conducted using a 64-slice, 128-detector row spiral CT scanner (SOMATOM Definition, Siemens Healthineers, Germany). Scanning parameters were set as follows: slice thickness of 5mm, pitch of 5.0, and reconstruction interval of 1.2mm. For contrast-enhanced scans, iopromide (300mgI/mL) was administered intravenously at a dosage of 1.5–2.0mL/kg, with an injection rate of 3.0–3.5mL/s.
MRI Scanning
MRI examinations were performed using a 3.0-T superconducting MRI system (MAGNETOM Skyra, Siemens Healthineers, Germany) with a standard head coil. The imaging protocol consisted of axial T1-weighted imaging (TR/TE = 2080/9.7ms), axial T2-weighted imaging (TR/TE = 4150/95ms), axial T2-FLAIR (TR/TE = 2300/97ms), diffusion-weighted imaging (TR/TE = 5200/89ms; b = 1000s/mm2), and sagittal T1-weighted imaging (TR/TE = 250/2.46ms). Slice thickness was 5mm with an interslice gap of 1.5mm. The acquisition matrix was 320 × 292, and the field of view was 24 × 24 cm. Contrast-enhanced imaging was performed using gadopentetate dimeglumine (Gd-DTPA) administered intravenously at a dose of 0.1mmol/kg.
Image Analysis and Measurement
All images were retrospectively reviewed by two senior radiologists, and consensus was reached regarding the interpretation of imaging features. The assessment criteria included: 1) Cranial findings: presence of subependymal calcified nodules, cortical dysplasia, SEGA, cerebral fissure malformation, cranial bone dysplasia; 2) Abdominal findings: number, size, and distribution of renal and hepatic AML, as well as other associated characteristics; 3) pulmonary findings: number, size, and distribution of pulmonary LAM and MMPH; 4) multifocal sclerotic lesions involving the vertebral bodies and appendages of the thoracolumbar spine.
Statistical Analysis
All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Categorical variables were expressed as n (%). Positive rates between CT and MRI for various intracranial lesions were compared using either the chi-square test or Fisher’s exact test, as appropriate. A P value < 0.05 was considered statistically significant.
Results
Patients’ Data
A total of 57 patients with clinically diagnosed TSC were enrolled. Of these, 33/57 (57.9%) were male and 24/57 (42.1%) were female. Age ranged from 4 months to 59 years, with a mean of 23.5 years. 6/57 (10.5%) patients were younger than 5 years, 32/57 (56.1%) were aged 5–18 years, and 19/57 (33.3%) were older than 18 years. Clinical characteristics and imaging examinations were summarized in Table 1.
 |
Table 1 Clinical Features and Imaging Examinations in TSC Patients (n = 57) |
Intracranial Findings
The features of intracranial lesions detected by cranial CT and/or routine MRI in 57 TSC patients were summarized in Table 2. Subependymal calcified nodules (Figure 1A–C), which presented as multiple calcified nodules, predominantly located in the body, atrium, and foramen of Monro regions of the lateral ventricles and measuring 2–10 mm, were observed in 51/57 cases (89.5%). On cranial CT, the detection rate was 100% (46/46), significantly higher than routine MRI (13/19, 68.4%; P < 0.001).
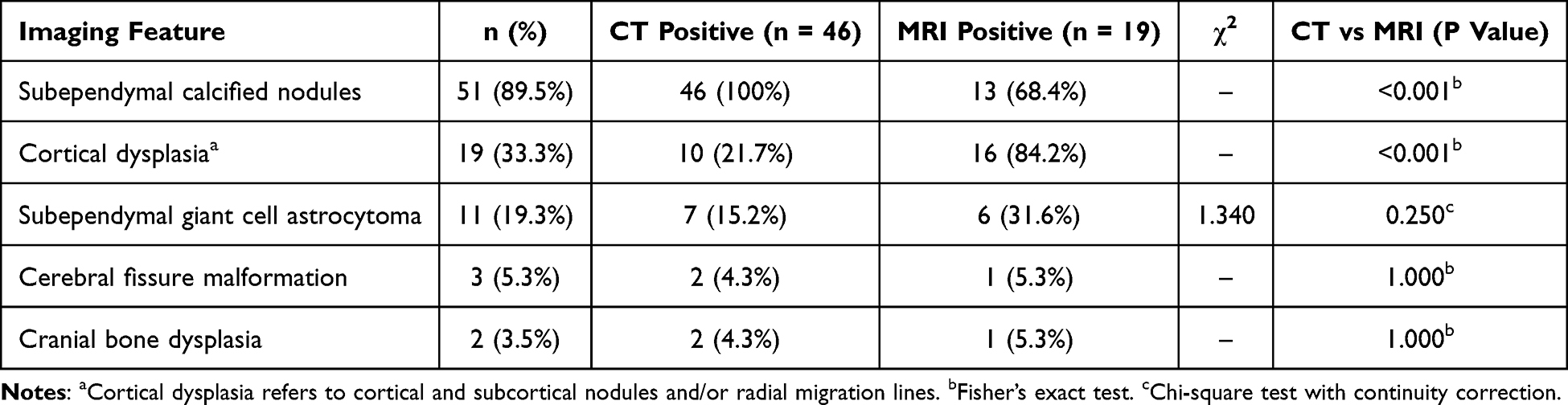 |
Table 2 Comparison Imaging Features of CT and MRI in TSC Patients |
 |
Figure 1 Subependymal calcified nodules shown on CT and/or MRI. (A) Calcified nodule in subependymal region of the lateral ventricle shown on CT (white arrow); (B–C) Subependymal calcified nodules (black arrow) shown by MRI T1WI (B) and T2WI (C). |
Cortical dysplasia lesions (Figure 2A–C), which typically manifested as cortical/subcortical nodules and/or radial migration lines, were observed in 19/57 (33.3%) patients. MRI detected these lesions in 16/19 (84.2%) patients, significantly higher than CT (10/46, 21.7%; P < 0.001).
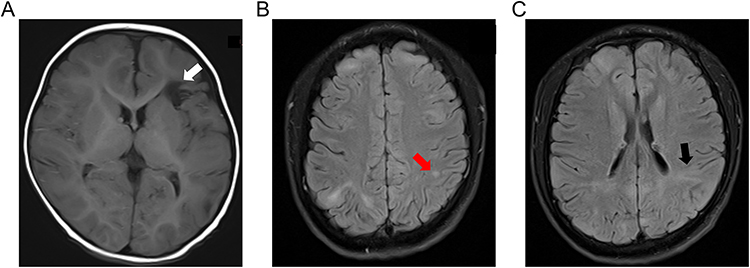 |
Figure 2 Cortical dysplasia and cerebral fissure malformation shown by MRI. (A–C) Cerebral fissure malformation (A, white arrow), cortical and subcortical nodule (B, red arrow), and radial migration line (C, black arrow) shown by MRI. |
Furthermore, 11/57 (19.3%) patients were diagnosed with SEGA (Figure 3A–C), which were predominantly presented as irregularly lobulated masses projecting into the lateral ventricles at the anterior horn and/or foramen of Monro with marked enhancement when contrast was used. But the enhancement pattern became markedly heterogeneous, when internal calcification or cystic degeneration presented. CT detected SEGAs in 7/46 (15.2%) patients and routine MRI in 6/19 (31.6%) patients, without a statistically significant difference (P = 0.250).
 |
Figure 3 Subependymal giant cell astrocytoma and cranial bone dysplasia shown by MRI. (A–C) Subependymal giant cell astrocytoma (red arrow) in the left anterior ventricle and cranial bone dysplasia of the left frontoparietal temporal bone (white arrow), shown by MRI T1WI (A), T2WI (B) and contrast-enhanced T1WI (C). |
Additionally, cerebral fissure malformations (Figure 2A) were presented in 3/57 (5.3%) patients: two cases located in the left frontal lobe (associated with focal subarachnoid space enlargement and calcified nodules), and one case located in the left parietal lobe which communicated with the posterior body of the left lateral ventricle. Finally, cranial bone dysplasia lesions (Figure 3B), manifesting as focal calvarial thickening with patchy sclerosis, were identified in 2/57 (3.5%) patients.
Extracranial Findings
Among the 21 patients who underwent abdominal CT scan (including 9 contrast-enhanced cases), multiple bilateral renal AMLs (Figure 4A) of varying size were found in 12/21 (57.1%) patients. The masses with < −20 HU on unenhanced CT were characteristic of AMLs and typically appeared as macroscopic fat with varying degrees of enhancement in the soft-tissue and dysmorphic vascular components. Some of the larger lesions were complicated by intralesional aneurysms and hemorrhage. Additionally, hepatic AMLs (Figure 4B) were observed in 5/21 (23.8%) patients, showing heterogeneous enhancement after contrast administration, similar to renal AMLs.
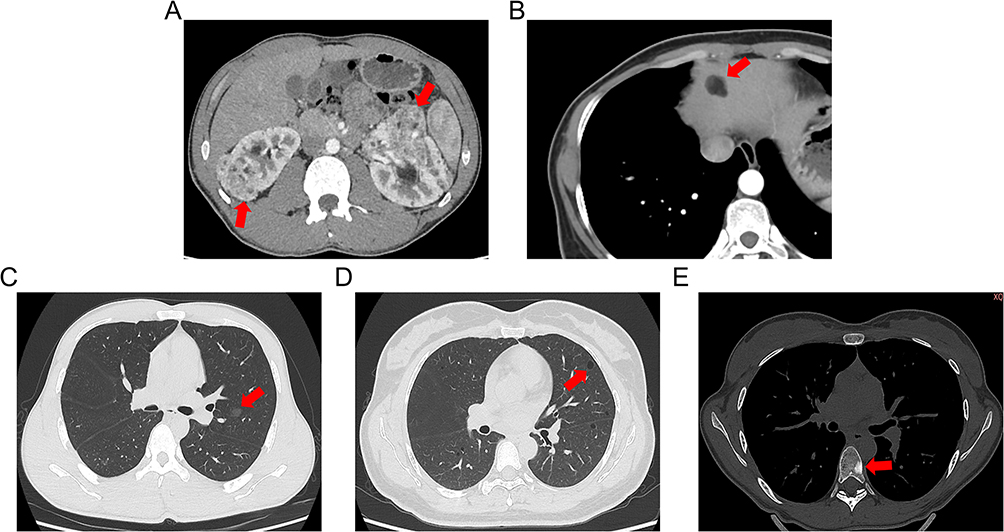 |
Figure 4 Abdominal and thoracic CT findings in TSC. (A) Multiple renal AMLs shown on contrast-enhanced abdominal CT (red arrow). (B) AML of hepatic S4 shown on contrast-enhanced abdominal CT (red arrow). (C) Multiple MMPHs in both lungs shown on thoracic unenhanced CT (red arrow). (D) Multiple pulmonary LAMs in both lungs shown on thoracic unenhanced CT (red arrow). (E) Sclerotic bone lesions of thoracic vertebra shown on thoracic unenhanced CT (red arrow). |
Thoracic unenhanced CT was performed in 15 patients. MMPHs (Figure 4C), manifesting as multiple bilateral ground-glass opacities, were identified in 5/15 (33.3%) patients. Pulmonary LAMs (Figure 4D), characterized by multiple, variably sized, thin-walled cysts with smooth margins, were detected in 3/15 (20.0%) patients. Among the patients with LAMs, one developed recurrent bilateral spontaneous pneumothoraces and a left-sided chylothorax.
Among the 36 patients who underwent thoracic and/or abdominal CT scan that permitted evaluation of the visualized spine, multiple sclerotic bone lesions (Figure 4E) were identified in 13/36 (36.1%) patients. Radiologically, these lesions appeared as ivory-like sclerotic foci involving the thoracic and lumbar vertebral bodies and posterior elements.
Discussion
This study evaluated the imaging manifestations of TSC and compared CT and routine MRI for detecting key intracranial lesions. We found that CT identified subependymal calcified nodules more frequently than routine MRI, whereas MRI was more sensitive for soft-tissue lesions, like cortical dysplasia and SEGAs. Extracranial CT further demonstrated common multisystem involvement, including renal/hepatic AMLs, pulmonary lesions, and sclerotic bone changes. Collectively, these results supported a complementary, modality-tailored imaging strategy for comprehensive diagnosis and surveillance in TSC.
Consistent with previous results,14,23 CT has been shown a clear advantage over routine MRI in depicting calcifications, particularly subependymal calcified nodules. On CT, calcifications could be confidently identified along the ventricular walls, most commonly involving the body and atrium of the lateral ventricles and the foramen of Monro region, where small, often millimeter-sized hyperdense nodules are readily visualized.19,24,25 By comparison, routine MRI sequences, including T1-weighted, T2-weighted, and FLAIR imaging, showed limited sensitivity and specificity for calcification, which may appear variably as signal voids and could be obscured by other susceptibility-related effects.25 Although susceptibility-based sequences, such as susceptibility-weighted imaging (SWI)/Gradient Recalled Echo(GRE), can improve the detection of calcifications, these sequences are not universally included in routine brain MRI protocols and are less commonly performed solely for calcification depiction in real clinical practice.26 Pathologically, subependymal calcified nodules in TSC correspond to hamartomatous lesions composed of dysplastic glioneuronal elements and giant cells,27 where calcification is typically dystrophic, and reflects long-standing lesion evolution rather than active tumor growth.27–29 This propensity for chronic degeneration and calcium deposition provides a biological explanation for the performance advantage of CT, an imaging modality intrinsically suited to depicting mineralization, in detecting these lesions compared with routine MRI.28
In TSC, both cortical dysplasia lesions and SEGAs represent key neuropathological manifestations that share a common molecular basis. Loss-of-function mutations in TSC1 or TSC2 result in constitutive activation of the mTORC1 signaling pathway, which plays a critical role during embryonic and early postnatal brain development. Dysregulated mTORC1 activity interferes with neural progenitor cell proliferation and differentiation, neuronal migration, and cortical lamination, leading to focal cortical architectural disorganization and the formation of cortical tubers.30,31 Increasing evidence supports a somatic second-hit mechanism, whereby localized biallelic inactivation of TSC genes in subsets of neural precursor cells accounts for the multifocal yet regionally confined distribution of cortical lesions and their close association with epilepsy and neuropsychiatric manifestations.32 In parallel, sustained activation of the mTOR signaling pathway is thought to promote abnormal cellular growth within the subependymal region, contributing to the development of SEGAs.33 These lesions are generally slow-growing and may form intraventricular masses, most commonly near the foramen of Monro, where they can be associated with cerebrospinal fluid obstruction, hydrocephalus, and neurological morbidity, particularly in pediatric patients.33 Collectively, these lesions underscore the central biological role of mTOR dysregulation in the neurodevelopmental, epileptic, and neuropsychiatric phenotypes of TSC and place the disorder within the broader spectrum of mTORopathies, which provides a strong rationale for mTOR-targeted therapeutic strategies.
From an imaging perspective, MRI offered distinct advantages over CT in the evaluation of CNS involvement in TSC, owing to its superior gray-white matter contrast and sensitivity to subtle microstructural abnormalities. Specifically, T2-weighted and FLAIR sequences more reliably demonstrated cortical thickening, subcortical white matter signal abnormalities, radial migration lines, as well as the non-calcified components of SEGAs. These imaging characteristics supported MRI as the preferred modality for comprehensive assessment and longitudinal monitoring of TSC-related brain lesions, especially in the context of neurodevelopmental abnormalities and disease progression.34
Beyond intracranial evaluation, CT also plays an important role in the assessment of extracranial involvement in TSC, further demonstrating that TSC is a typical disease involving multiple systems. In the present cohort, extracranial CT demonstrated a broad range of organ involvement, including renal and hepatic AMLs, pulmonary manifestations (LAM and/or MMPH), as well as sclerotic bone lesions. Although these extracranial manifestations may remain clinically silent in the early stages, disease progression or the development of complications, such as hemorrhage from renal AMLs or pneumothorax related to LAM, can substantially affect patient prognosis.35,36 Therefore, systematic imaging assessment and follow-up of the thorax, abdomen, and skeletal system are of great significance. In the extracranial assessment, CT has several practical advantages, including rapid acquisition, broad anatomic coverage, and suitability for standardized follow-up across multiple organ systems. If the radiation exposure can be fully taken into account and the scanning protocols can be optimized, extracranial CT can serve as a valuable complement to cranial MRI for the ongoing monitoring and management of multisystem involvement in TSC.
Building on the established complementary roles of CT and routine MRI in the assessment of both intracranial and extracranial involvement in TSC, ongoing developments in imaging technology are expected to further enhance lesion evaluation and support more individualized clinical management. Functional imaging with PET-CT, for instance, has been increasingly explored for identifying epileptogenic regions in patients with drug-resistant epilepsy and may offer additional information for presurgical decision-making.37 In the context of SEGA, emerging data indicate that non–contrast-enhanced 3D T1-WI can achieve diagnostic performance similar to that of contrast-enhanced MRI, potentially reducing the need for gadolinium administration, particularly in pediatric patients and those with impaired renal function.38 Advances in MRI acceleration techniques, including approaches that combine Wave-CAIPI and MULTIPLEX, have also improved acquisition efficiency while preserving multiparametric image quality, which may facilitate more comprehensive imaging protocols in clinical practice.39 Furthermore, studies using ultra–high-field MRI have reported abnormal iron deposition in deep gray matter nuclei in patients with TSC, which may uncover the links between cortical lesions and alterations in cerebral vascular or metabolic pathways.40 Although not yet routinely implemented, these advanced imaging modalities highlight promising directions for future research aimed at optimizing imaging-based evaluation and long-term monitoring in TSC.
Alongside advancements in imaging technologies, there has been notable progress in the identification of molecular biomarkers that provide insight into the complex pathophysiology of TSC. Beyond the well-established mutations in TSC1 and TSC2, emerging transcriptomic research has introduced potential new markers, such as PDPN and lipid metabolism-related genes (including ALOX12B, CPT1C, and others), which may be associated with epileptogenesis and neuroinflammation.41,42 Additionally, elevated levels of peripheral biomarkers, such as glial fibrillary acidic protein (GFAP) and pro-inflammatory cytokines like IL-1β, CXCL8, and EGF, have shown promise as non-invasive indicators of neuroglial activation.43 When these molecular findings are integrated with radiological imaging results, they offer new opportunities for more personalized monitoring and targeted treatment strategies. The combination of advanced imaging techniques with molecular profiling thus holds significant potential to improve precision diagnostics and optimize long-term management in TSC.
Several limitations of this study should be acknowledged. First, the retrospective design and single-center setting may have introduced selection and information bias, which could affect the generalizability of the results. Second, the MRI protocols mainly consisted of conventional sequences, and SWI was not systematically included, potentially limiting the detection of calcifications and subtle lesions such as microbleeds. Third, extracranial imaging was not uniformly performed, as thoracic and abdominal CT examinations were obtained according to clinical indications and contrast-enhanced scans were used in a limited number of cases. As a result, the extent of extracranial involvement may have been underestimated. Finally, the absence of longitudinal follow-up and outcome data precluded analysis of the relationship between imaging findings and key clinical endpoints, including seizure control, renal function, hemorrhagic events, and pulmonary complications.
Based on our findings, imaging evaluation in TSC should follow a stage- and lesion-type–oriented strategy. At initial presentation, brain MRI should be the first-line modality to comprehensively assess non-calcified parenchymal lesions and establish a baseline for follow-up; cranial CT can be added when calcification characterization is required or when MRI-SWI is limited. During follow-up, MRI should remain the mainstay, with particular attention to growth of subependymal lesions near the foramen of Monro and the risk of hydrocephalus. Extracranial assessment should be organ- and risk-based, using thoracic/abdominal and skeletal CT to detect and monitor key manifestations such as AMLs, LAM/MMPH-related pulmonary changes, and sclerotic bone lesions. Looking ahead, integration of ultra-high-field MRI (eg, 7T) and quantitative approaches such as radiomics may enable more comprehensive assessment, improved risk stratification, and more individualized surveillance decisions.
Conclusion
In this retrospective study of clinically diagnosed TSC patients, CT and routine MRI exhibited complementary strengths in detecting intracranial lesions. CT was more effective in identifying subependymal calcified nodules, while routine MRI was more sensitive in detecting soft-tissue lesions. Extracranial CT also revealed common multisystem involvement, including renal, pulmonary, and skeletal lesions. These findings support a modality-tailored imaging approach, with MRI as the primary tool for CNS evaluation and CT as a valuable complement for detecting calcifications and extracranial lesions. Emerging imaging techniques and molecular biomarkers—including TSC1/TSC2 mutations and inflammatory markers—may further enhance individualized care. These findings support a multimodal, risk-adapted imaging approach to optimize diagnosis, surveillance, and neuropsychiatric management in patients with TSC.
Ethics Approval and Consent to Participate
This study received approval from the Ethics Committee of the First People’s Hospital of Neijiang (No. 2025-87) and was conducted in line with the ethical standards outlined in the Declaration of Helsinki. As this was a retrospective study using de-identified data, informed consent was waived. All patient information was anonymized prior to analysis, and confidentiality was maintained throughout the study.
Funding
This work was supported by the Neijiang Municipal Science and Technology Program (Grant No. Z2025041 and Z2025036).
Disclosure
The authors declare that they have no competing interests.
References
1. Uysal SP, Sahin M. Tuberous sclerosis: a review of the past, present, and future. Turk J Med Sci. 2020;50(7):1665–10. doi:10.3906/sag-2002-133
2. Annear NMP, Appleton RE, Bassi Z, et al. Tuberous Sclerosis Complex (TSC): expert recommendations for provision of coordinated care. Front Neurol. 2019;10:1116. doi:10.3389/fneur.2019.01116
3. Meng Y, Yu C, Chen M, et al. Mutation landscape of TSC1/TSC2 in Chinese patients with tuberous sclerosis complex. J Hum Genet. 2021;66(3):227–236. doi:10.1038/s10038-020-00839-0
4. Yu T, He Y, Li N, et al. Novel TSC1 and TSC2 gene mutations in Chinese patients with tuberous sclerosis complex. Clin Neurol Neurosurg. 2017;154:104–108. doi:10.1016/j.clineuro.2017.01.015
5. Ogórek B, Hamieh L, Hulshof HM, et al. TSC2 pathogenic variants are predictive of severe clinical manifestations in TSC infants: results of the EPISTOP study. Genet Med. 2020;22(9):1489–1497. doi:10.1038/s41436-020-0823-4
6. Wang F, Xiong S, Wu L, Chopra M, Hu X, Wu B. A novel TSC2 missense variant associated with a variable phenotype of tuberous sclerosis complex: case report of a Chinese family. BMC Med Genet. 2018;19(1):90. doi:10.1186/s12881-018-0611-z
7. Rosengren T, Nanhoe S, De Almeida LGD, et al. Mutational analysis of TSC1 and TSC2 in Danish patients with tuberous sclerosis complex. Sci Rep. 2020;10(1):9909. doi:10.1038/s41598-020-66588-4
8. Toyoshima M, Ohno K, Katsumoto T et al. Cellular senescence of angiofibroma stroma cells from patients with tuberous sclerosis. Brain Dev. 1999;21(3):184–91 doi:10.1016/s0387-7604(99)00008-x.
9. Northrup H. Tuberous sclerosis complex: genetic aspects. J Dermatol. 1992;19(11):914–919. doi:10.1111/j.1346-8138.1992.tb03805.x
10. Purbasari U, Prihartono NA, Helda N, Audita FR, Dharmawan BS. Challenges of siblings with tuberous sclerosis showing various manifestations and severe complications. Radiol Case Rep. 2024;19(6):2566–2573. doi:10.1016/j.radcr.2024.03.002
11. Kori H, Tobino K. Expanding the radiological spectrum of Lymphangioleiomyomatosis: a case with Unique imaging findings. Respir Investig. 2025;63(5):800–804. doi:10.1016/j.resinv.2025.06.015
12. Campanario Da Silva Pereira C, Gomes Dantas FD, Da Rosa Baratela WA, Antunes Da Costa F, Tavares Lucato L, Kok F. Tuberous sclerosis complex: clinical, genetic and 7T-MRI neuroimaging findings. Brain Dev. 2025;47(4):104386. doi:10.1016/j.braindev.2025.104386
13. Verma Saluja K, Sangar P, Pillai D, Suman CP. Tuberous sclerosis complex: one disorder, three generations and an assortment of radiological and clinical presentations. BMJ Case Rep. 2025;18(1):e261774. doi:10.1136/bcr-2024-261774
14. Northrup H, Aronow ME, Bebin EM, et al. Updated international tuberous sclerosis complex diagnostic criteria and surveillance and management recommendations. Pediatr Neurol. 2021;123:50–66. doi:10.1016/j.pediatrneurol.2021.07.011
15. Ellingson BM, Sanvito F, Cloughesy TF, et al. A neuroradiologist’s guide to operationalizing the response assessment in Neuro-Oncology (RANO) criteria version 2.0 for gliomas in adults. Am J Neuroradiol. 2024;45(12):1846–1856. doi:10.3174/ajnr.A8396
16. Boggarapu S, Rushing G, Pounders A, Roberds SL, Beresford E. Cutaneous manifestations-associated with tuberous sclerosis complex and the use of topical rapamycin in the United States: a sub-analysis of an international survey of caregivers and patients. Orphanet J Rare Dis. 2025;20(1):455. doi:10.1186/s13023-025-03653-z
17. Mekahli D, Müller R, Marlais M, et al. Clinical practice recommendations for kidney involvement in tuberous sclerosis complex: a consensus statement by the ERKNet working group for autosomal dominant structural kidney disorders and the ERA genes & kidney working group. Nat Rev Nephrol. 2024;20(6):402–420. doi:10.1038/s41581-024-00818-0
18. Hu S, Hu D, Zhu W, Wang L, Wang Z. Tuberous sclerosis complex: imaging characteristics in 11 cases and review of the literature. J Huazhong Univer SciTechnol. 2016;36(4):601–606. doi:10.1007/s11596-016-1632-5
19. Arredondo KH, Jülich K, Roach ES. Tuberous sclerosis complex: diagnostic features, surveillance, and therapeutic strategies. Semin Pediatr Neurol. 2024;51:101155. doi:10.1016/j.spen.2024.101155
20. Sun H, Yan Z, Gao J, et al. Improved pre-surgical localization of epileptogenic tubers in pediatric tuberous sclerosis complex using mean apparent propagator MRI. Neurosurg Rev. 2025;48(1):344. doi:10.1007/s10143-025-03495-0
21. Li W, Sha L, Zhu J, Long F, Chen L. Prediction of epileptogenicity in patients with tuberous sclerosis complex using multimodal cerebral MRI. Eur J Radiol. 2024;181:111800. doi:10.1016/j.ejrad.2024.111800
22. Northrup H, Krueger DA, Northrup H. International TSCC. Tuberous sclerosis complex diagnostic criteria update: recommendations of the 2012 International Tuberous Sclerosis Complex Consensus Conference. Pediatr Neurol. 2013;49(4):243–254. doi:10.1016/j.pediatrneurol.2013.08.001
23. van der Bie J, Berghout BP, Budde RPJ, Gutierrez J, van Straten M, Bos D. Intracranial calcification detection; a comparison between Micro-CT, conventional CT and ultra-high-resolution photon-counting detector CT. Acad Radiol. 2025;32(6):3599–3607. doi:10.1016/j.acra.2025.01.028
24. Wataya-Kaneda M. Tuberous sclerosis complex. Keio J Med. 2025;74(1):42–51. doi:10.2302/kjm.2023-0011-IR
25. Go JL, Zee CS. Unique CT imaging advantages. Hemorrhage and calcification. Neuroimaging Clin N Am. 1998;8(3):541–558.
26. Jaafari O, Salih S, Alkatheeri A, et al. Appropriate incorporation of susceptibility-weighted magnetic resonance imaging into routine imaging protocols for accurate diagnosis of traumatic brain injuries: a systematic review. J Med Life. 2024;17(3):273–280. doi:10.25122/jml-2023-0487
27. Crino PB, Nathanson KL, Henske EP. The tuberous sclerosis complex. New Engl J Med. 2006;355(13):1345–1356. doi:10.1056/NEJMra055323
28. von Ranke FM, Faria IM, Zanetti G, Hochhegger B, Souza ASJ, Marchiori E. Imaging of tuberous sclerosis complex: a pictorial review. Radiologia brasileira. 2017;50(1):48–54. doi:10.1590/0100-3984.2016.0020
29. Aronica E, Crino PB. Epilepsy related to developmental tumors and malformations of cortical development. Neurotherapeutics. 2014;11(2):251–268. doi:10.1007/s13311-013-0251-0
30. Crino PB, Aronica E, Baltuch G, Nathanson KL. Biallelic TSC gene inactivation in tuberous sclerosis complex. Neurology. 2010;74(21):1716–1723. doi:10.1212/WNL.0b013e3181e04325
31. Feliciano DM. The neurodevelopmental pathogenesis of Tuberous Sclerosis Complex (TSC). Front Neuroanat. 2020;14:39. doi:10.3389/fnana.2020.00039
32. Curatolo P, Specchio N, Aronica E. Advances in the genetics and neuropathology of tuberous sclerosis complex: edging closer to targeted therapy. Lancet Neurol. 2022;21(9):843–856. doi:10.1016/S1474-4422(22)00213-7
33. Curatolo P, Moavero R, de Vries PJ. Neurological and neuropsychiatric aspects of tuberous sclerosis complex. Lancet Neurol. 2015;14(7):733–745. doi:10.1016/S1474-4422(15)00069-1
34. Takanashi J, Sugita K, Fujii K, Niimi H. MR evaluation of tuberous sclerosis: increased sensitivity with fluid-attenuated inversion recovery and relation to severity of seizures and mental retardation. Am J Neuroradiol. 1995;16(9):1923–1928.
35. Dun S, Wang Y, Wan L, et al. Sirolimus can promote the disappearance of renal angiomyolipoma associated with tuberous sclerosis complex: a prospective cohort study. World J Pediatr. 2024;20(6):602–610. doi:10.1007/s12519-023-00751-5
36. Nasir K, Ahmad A. Giant renal angiomyolipomas and pulmonary lymphangioleiomyomatosis: follow-up report after more than a decade. Saudi J Kidney Dis Transplant. 2023;34(6):671–675 doi:10.4103/sjkdt.sjkdt_324_21.
37. Wang Z, Li Y, He Z, et al. Predictive model for epileptogenic tubers from all tubers in patients with tuberous sclerosis complex based on 18F-FDG PET: an 8-year single-centre study. BMC Med. 2023;21(1):500. doi:10.1186/s12916-023-03121-0
38. Gaillard A, Crombé A, Jecko V, et al. Magnetic resonance imaging diagnosis of subependymal giant cell astrocytomas in follow-up of children with tuberous sclerosis complex: should we always use contrast enhancement? Pediatr Radiol. 2020;50(10):1397–1408. doi:10.1007/s00247-020-04707-z
39. Liu C, Ye Y, Guo Y, et al. Wave‐CAIPI multiparameter MR imaging in neurology. NMR Biomed. 2025;38(3):e5322. doi:10.1002/nbm.5322
40. Sun K, Cui J, Xue R, et al. New imaging features of tuberous sclerosis complex: a 7 T MRI study. NMR Biomed. 2021;34(9):e4565. doi:10.1002/nbm.4565
41. Sun Y, Ji H, Xu L, et al. Screening for biomarkers of tuberous sclerosis complex-associated epilepsy: a bioinformatics analysis. Transl Pediatr. 2024;13(7):1190–1200. doi:10.21037/tp-24-211
42. Weiliang W, Yinghao R, Weiliang H, et al. Identification of hub genes significantly linked to tuberous sclerosis related-epilepsy and lipid metabolism via bioinformatics analysis. Front Neurol. 2024;15:1354062. doi:10.3389/fneur.2024.1354062
43. Balthazard R, Drouin-Engler R, Bertrand S, et al. Distinct peripheral pro-inflammatory profile associated with tuberous sclerosis complex and epilepsy. Epilepsia. 2025;66(4):1288–1303. doi:10.1111/epi.18261
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Advances in Multimodal Imaging Techniques for Evaluating and Predicting the Efficacy of Immunotherapy for NSCLC
Liu J, Xie M, Shen J, Yao J, Lin X, Bao X, Zhang X, Liang Y, Yang Y, Jiang G, Diao X, Han W, Du H, Xue X, Wu J
Cancer Management and Research 2025, 17:1073-1086
Published Date: 7 June 2025
HIV Complicated with Talaromyces Marneffei Multisystem Infection: A Case Report and Literature Review
Zhang G, Wu G, Xu Y, Yang L, Yang W
Infection and Drug Resistance 2025, 18:3561-3568
Published Date: 21 July 2025
Imaging Evaluation of Bone Tumors in the Cervical Spine: A Comprehensive Review
Sun M, Meng X, Wu M, Wang Z
International Journal of General Medicine 2025, 18:7785-7798
Published Date: 25 December 2025
A Novel Nomogram for Predicting Osteoporotic Vertebral Compression Fractures with Hounsfield Unit and Vertebral Bone Quality: A Retrospective Cohort Study
Zhuang C, Yang X, Wang H, Wang Z, Bao F, Yan Z, Lin H
Clinical Interventions in Aging 2026, 21:600367
Published Date: 18 June 2026