Back to Journals » Psychology Research and Behavior Management » Volume 19
Comparative Efficacy of Exercise Interventions for Anxiety Disorders: A Bayesian Network Meta-Analysis
Authors Liu J, Wang H, Lan Y, Yuan D, Du B, Zhou Y, Zhang W ![]() , Ke XW, Jiang Q, Wang F
, Ke XW, Jiang Q, Wang F ![]() , Cao S, Sun J
, Cao S, Sun J ![]()
Received 1 October 2025
Accepted for publication 28 December 2025
Published 17 February 2026 Volume 2026:19 570270
DOI https://doi.org/10.2147/PRBM.S570270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Jiahui Liu,1,* Hengchang Wang,2,* Yi Lan,1 Dian Yuan,1,3 Bin Du,4 Yifan Zhou,1 Weihao Zhang,1 Xiong-Wen Ke,1,5 Qingqing Jiang,2,6 Furong Wang,6,7 Shiyi Cao,2 Jian Sun1,3
1Wushu College, Wuhan Sports University, Wuhan, Hubei, People’s Republic of China; 2School of Public Health, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 3Northeast China Ethnic Traditional Sports Research Center, Wuhan Sports University, Wuhan, Hubei, People’s Republic of China; 4The School of Physical Education, Central China Normal University, Wuhan, Hubei, People’s Republic of China; 5Rochester Institute of Technology, Rochester, NY, USA; 6School of Nursing, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 7Department of Neurology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Sun, Wushu College, Wuhan Sports University, 461 Luoyu Road, Hongshan District, Wuhan, Hubei, People’s Republic of China, Email [email protected] Shiyi Cao, Email [email protected]
Purpose: The objective of this study is to conduct a Bayesian multilevel network meta-analysis to compare the effectiveness of various exercise modalities on anxiety symptoms and to assess how exercise and individual characteristics moderate these effects.
Methods: A comprehensive search of Web of Science, PubMed, Embase, and Cochrane databases identified randomized controlled trials (RCTs) on exercise and anxiety. Literature screening, data extraction, and analysis were conducted independently by two researchers. A Bayesian-based network meta-analysis was applied, and the Confidence in Network Meta-Analysis (CINeMA) tool assessed evidence quality.
Results: Forty-five studies (97 groups, 2643 participants) were included. Compared to control groups, meditation (Hedges’ g = − 0.72, 95% CI: − 1.20 to − 0.24), yoga (Hedges’ g = − 0.59, 95% CI: − 0.93 to − 0.27), and tai chi/qigong (Hedges’ g = − 0.52, 95% CI: − 0.88 to − 0.17) had the strongest effects. Resistance training (Hedges’ g = − 0.40), aerobic exercise (Hedges’ g = − 0.40), and walking/jogging (Hedges’ g = − 0.39) were also effective. However, mixed aerobic exercise did not achieve statistical significance.
Conclusion: Static, breath-focused exercises (eg, meditation, yoga, tai chi/qigong) and dynamic exercises (eg, resistance training, walking/jogging) may be effective interventions for anxiety reduction, with broad applicability across populations.
Keywords: anxiety disorders, exercise, meta-analysis
Background
Anxiety disorders are among the most common psychiatric conditions globally, with ~14% prevalence.1,2 They occur more frequently among women than men.1 As a frequent comorbidity with chronic illnesses—including cardiovascular disease, cancer, and depressive disorders—anxiety substantially worsens clinical trajectories and quality of life.3 Epidemiological data show that anxiety has a high lifetime prevalence among adults, with symptoms that are often persistent and prone to relapse.4 In severe cases, anxiety can lead to comorbidities such as depression and cardiovascular diseases, further compounding patients’ medical burden and creating a vicious cycle.5 For instance, anxiety and heart disease share a bidirectional relationship, and metabolic disorders such as diabetes and obesity are closely associated with anxiety.6,7
Conventional treatments of the anxiety disorder normally consist of pharmacotherapy and psychotherapy.8,9 Despite the effectiveness of these methods, some patients fail to respond to treatment or have problems with accessing timely care because of economic and social factors, especially in low- and middle-income countries where coverage of treatments does not meet the expectations.10 Also, pharmacotherapy can be associated with unwanted effects and prolonged dependency, and psychotherapies, such as cognitive-behavioural therapy, even though effective, can only be administered by mental health professionals, which are usually not available in resource-constrained regions.11 Thus, evidence-based alternative or complementary treatment methods are urgently required in order to enhance the quality of life and health outcomes of anxiety patients.
In recent years, exercise has gained increasing attention as a low-cost, easily implementable intervention in the field of anxiety treatment.12 It can be used not only as a supplement to pharmacotherapy and psychotherapy but also as a standalone alternative.13 A large body of research indicates that exercise can enhance mental health, improve physical health, boost immunity, and enhance cognitive function.13 For example, studies have shown that regular exercise can reduce the severity of anxiety symptoms.14 Furthermore, regular physical activity promotes the release of neurotransmitters such as serotonin and dopamine, which help alleviate stress and improve mood.15 Despite these promising mechanisms, the specific effects of different types, intensities, frequencies, and durations of exercise remain unclear.
Traditional pairwise meta-analyses have limitations in evaluating the overall effect of exercise interventions, as they generally compare a specific exercise type with a control group, potentially overlooking other exercise types.16 In addition, existing meta-analyses tend to focus on specific populations (eg, older adults), resulting in conclusions that lack generalizability and are difficult to apply to broader populations with anxiety.17 Many studies also fail to systematically consider exercise dosage (eg, frequency, intensity, duration, and type) and its influence on intervention outcomes, limiting their ability to provide specific guidance on optimal exercise regimens.18 More importantly, many meta-analyses have not adequately explored how individual characteristics (eg, baseline anxiety levels) modulate the effects of exercise interventions, potentially leading to significant differences in outcomes across populations and limiting the effectiveness of personalized interventions.19
To address these gaps, we extend the current evidence by (1) applying a Bayesian multilevel network meta-analysis to compare multiple exercise modalities on a common effect-size scale, (2) standardizing exercise dose using MET-min/week to evaluate dose–response patterns, and (3) assessing potential moderators such as age, sex, and baseline symptom severity. This study conducted a comprehensive network meta-analysis of the effects of exercise on anxiety disorders, aiming to identify the optimal type and dosage of exercise. By analyzing various exercise interventions, we seek to determine the most suitable form of exercise for individuals with anxiety. Furthermore, this study explored the moderating effects of participant characteristics (eg, gender, age, baseline anxiety level) on the effectiveness of exercise interventions, thereby revealing differential responses to exercise among different groups. Through this comprehensive network meta-analysis, we aim to provide more reliable and scientific evidence for the treatment of anxiety disorders, assisting clinicians in developing personalized and effective exercise intervention plans to improve the quality of life and overall health of individuals with anxiety.
Methods
The study adhered to the guidelines for systematic review and meta-analysis, as required by international standards. This study has been registered with the PROSPERO International Prospective Register of Systematic Reviews (https://www.crd.york.ac.uk/PROSPERO/) under the registration number CRD42024580590.
Inclusion and Exclusion Criteria
Inclusion Criteria
We included randomized controlled trials (RCTs) evaluating the effects of exercise interventions on anxiety symptoms. Eligible participants were individuals meeting clinical diagnostic criteria for anxiety disorders, determined either through clinician diagnosis or by exceeding established thresholds on validated self-report instruments, such as GAD-7 ≥ 7, BAI ≥ 8, HADS-A ≥ 8, or SAS ≥ 50.20 Studies were required to include at least one exercise intervention arm, including mixed aerobic activities, aerobic exercise, resistance training, walking or jogging, meditation, tai chi/qigong, or yoga. Both single-session and long-term interventions were eligible to permit comparisons of short- versus long-term effects. Trials were required to report at least one anxiety-related outcome measure. To enhance generalizability, studies including participants with comorbidities (eg, depression or cancer) were also eligible.
Exclusion Criteria
Studies were excluded when insufficient quantitative data were available to calculate effect sizes or when anxiety outcomes were not reported. Non-primary research (eg, reviews, protocols, conference abstracts) and non-exercise interventions were also excluded to ensure the reliability and accuracy of the overall analysis.
Search Strategy
We searched CENTRAL, PubMed, WOS, and Embase using Cochrane-based strategies with MeSH and free-text terms (eg, tai chi, aerobic, resistance, mixed exercise, yoga, Tai Chi/Qigong, and meditation). No filters or date limits were applied. Searches ran from October 10, 2024, to July 16, 2025 (Supporting Information P1).
Literature Screening
Two researchers independently screened and extracted data, achieving 96.58% agreement using Excel. Interventions were classified (aerobic, resistance, mixed, yoga, tai chi/qigong, meditation; Table). Discrepancies were resolved by a third researcher, missing data sought from authors, and triangulation ensured accuracy and completeness, enhancing reliability and rigor.
Data Extraction
In this study, baseline details were collected, including study title, first author, nationality, year, and approval number. Pre- and post-intervention means (Mean) and standard deviations (SD) were obtained, along with exercise frequency, intensity, type, and duration. To quantify exercise dose, the Compendium of Physical Activities21 was used to calculate energy expenditure in metabolic equivalents of task (METs), allowing comparisons across interventions.
Included trials used diverse comparators: established treatments (eg, cognitive-behavioral therapy), active controls (eg, usual care, stretching, health education), and waitlist controls. Additional descriptive data from randomized controlled trials (RCTs) included concurrent treatments and control conditions. Participant characteristics—age, gender, comorbidities, and baseline anxiety severity—were documented to assess differential effects. Funding sources for each trial were also recorded to evaluate study quality and ensure scientific rigor and reliability.
Risk of Bias Assessment
Two researchers assessed the risk of bias through Cochrane risk-of-bias 2.0 randomised controlled trial (RCT) tool. The evaluation was based on seven areas, which include random sequence generation, allocation concealment, participant and staff blinding, outcome assessment blinding, incomplete outcome data, selective reporting, and other possible biases. The domains were divided into low risk, unclear risk and high risk. The two researchers carried out the evaluations independently and in case of disagreements, they discussed the matter with the third researcher.22
Statistical Analysis
A Bayesian random-effects multilevel network meta-analysis was conducted to evaluate the effects of exercise on anxiety, following the analytical framework described in prior work.23 Standardized mean change (Hedges’ g) was used as the summary measure, calculated from pre- to post-intervention change scores within each study arm. Hedges’ g incorporates a small-sample correction, allowing effect sizes from different anxiety scales to be compared on a common metric, where more negative values indicate greater symptom improvement. Multiple anxiety scales were harmonized by aligning the direction of improvement; for instance, STAI-S scores were multiplied by –1 to ensure that more negative values indicated greater symptom reduction, and all scales were standardized to maintain comparability across instruments.24 The model assumed a normal likelihood for observed effect sizes and incorporated a random intercept for between-study heterogeneity and a nested random effect for multiple outcomes within the same study. In statistical terms, effect sizes were modeled as

where  represents the absolute mean change associated with treatment t. Weakly informative priors were used for all parameters (Normal (0,1) for fixed effects and Half-Student-t (3,0,0.5) for heterogeneity). Sampling was implemented in the brms package in R with four chains, 4000 iterations per chain (1000 warmup), adapt_delta = 0.95, and max_treedepth = 15. Model convergence was confirmed using
represents the absolute mean change associated with treatment t. Weakly informative priors were used for all parameters (Normal (0,1) for fixed effects and Half-Student-t (3,0,0.5) for heterogeneity). Sampling was implemented in the brms package in R with four chains, 4000 iterations per chain (1000 warmup), adapt_delta = 0.95, and max_treedepth = 15. Model convergence was confirmed using  < 1.01 and visual inspection of trace plots and posterior predictive checks.
< 1.01 and visual inspection of trace plots and posterior predictive checks.
Active control groups (eg, usual care, stretching, health education) were combined when their effects were comparable, whereas waitlist controls were modeled as a distinct comparator because of their consistently poorer outcomes in anxiety trials. Multi-arm trials were handled using a multivariate parameterization to avoid unit-of-analysis errors and to preserve the correlation structure across arms. Consistency and transitivity were evaluated using design-by-treatment tests and node-splitting methods.
Moderator analyses were conducted within the same multilevel framework to examine whether age, sex, baseline severity, comorbidities, intervention duration, diagnostic characteristics (clinical diagnosis vs self-reported symptoms) and weekly exercise dose (MET-min/week) influenced treatment effects.25 Dose–response relationships were further explored using spline-based meta-regression when appropriate. Sensitivity analyses were performed by excluding studies at high risk of bias, applying alternative prior specifications, and re-estimating models with alternative outcome scaling. The credibility of the network estimates was assessed using the CINeMA tool across its six domains of certainty.26
For interpretive purposes only—and not for model estimation—we compared posterior effect sizes against a prespecified minimal clinically important difference (MCID) of |g| = 0.31, representing the threshold generally considered clinically meaningful for anxiety improvement. Full model code and data-processing scripts are provided in the Supporting Information to ensure reproducibility.
Credibility Assessment
In order to compare the credibility of each exercise intervention compared to the active control conditions, we applied the CINeMA tool that was created by the Cochrane Multiple Interventions Group.27 Network meta-analysis grading can be supported by CINeMA, and a thorough assessment of credibility across many dimensions is possible. First, on bias, we critically evaluated the quality of each research to limit the effects of bias on the analysis outcome. Reporting bias was detected using funnel plots to identify potential negative results, reducing the influence of publication bias. For indirectness, we focused on adults with anxiety disorders; if the study participants were primarily of a particular gender, had comorbidities, or belonged to specific age groups, indirectness could be an issue. Imprecision was evaluated using the width of the 95% credible intervals and whether they crossed zero. Separately, we used Hedges’ g = –0.31 as a threshold for identifying clinically important differences, reflecting the minimum effect size generally considered meaningful for anxiety reduction. Heterogeneity was evaluated by examining whether prediction intervals crossed the equivalence region, identifying consistency in intervention effects across studies. Incoherence was assessed by evaluating the consistency between direct and indirect evidence, ensuring that the network analysis did not violate the transitivity assumption. These evaluation methods enabled a more comprehensive understanding and assessment of the credibility of each exercise intervention.
Results
Literature Search Results
A total of 26,477 records were identified through searches in the WOS, PubMed, Embase, and Cochrane databases. After importing the records into Endnote and removing 6841 duplicates, two reviewers independently screened 19,636 titles and abstracts. Following the screening process, 19,303 irrelevant records and 32 unobtainable records were excluded. The remaining 313 records were further screened, and based on the inclusion and exclusion criteria, 47 records were excluded for not meeting outcome criteria, 88 for being non-randomized controlled trials, 21 for having interventions not aligned with the study scope, 26 for being conference reviews, 48 for having unavailable data, and 38 for not specifying anxiety symptoms, resulting in a total of 265 exclusions. Ultimately, 45 studies comprising 97 groups and 2643 participants were included in the analysis (Figure 1 and List of key excluded documents, Supporting information P16).
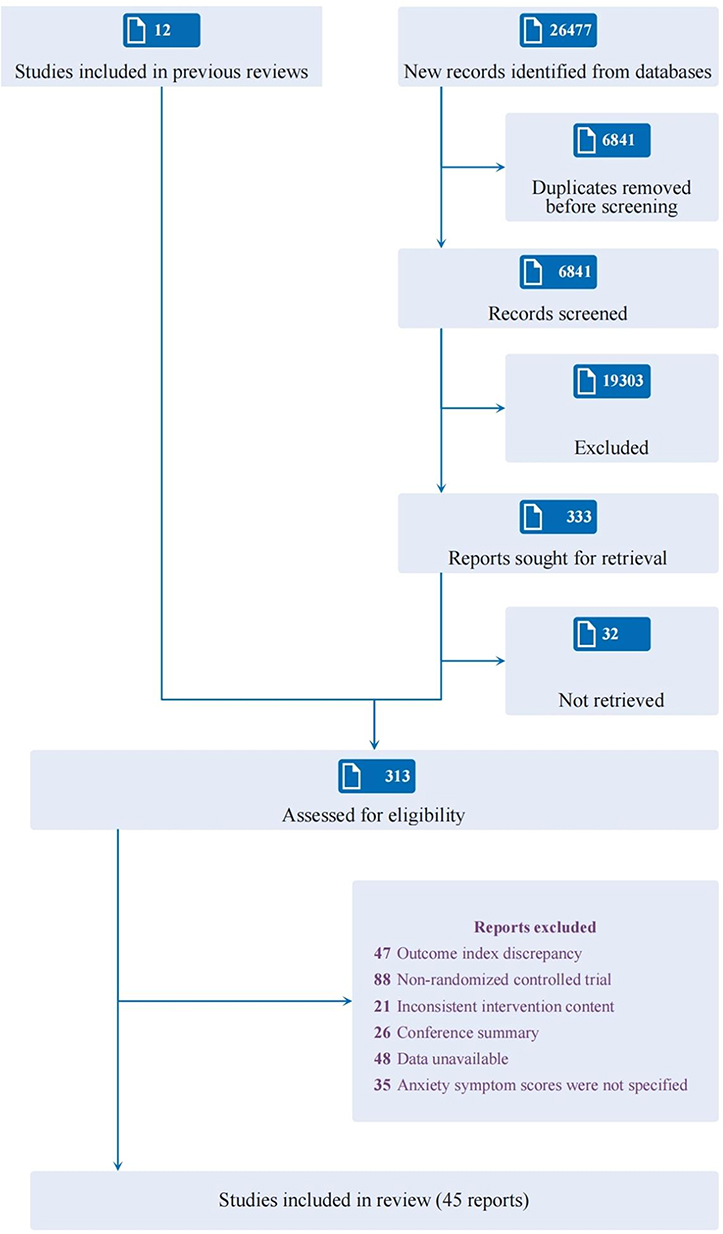 |
Figure 1 Flow of studies through review. |
The 45 included studies encompassed a variety of exercise interventions, including aerobic exercise, resistance training, yoga, Tai Chi, and mixed exercise. The intervention frequency ranged from once to seven times per week, with durations spanning from a single week to 24 weeks, allowing for the assessment of both short-term and long-term effects. Participants were recruited from various countries and regions, including the United States, the United Kingdom, Australia, China, Germany, and Brazil, ensuring sample diversity and enhancing the cross-cultural generalizability of the findings. The age range of participants was broad, including adolescents, adults, and older adults, with a relatively balanced gender distribution. Most studies used standardized scales, such as the Generalized Anxiety Disorder scale (GAD-7), the Hospital Anxiety and Depression Scale-Anxiety subscale (HADS-A), and the Beck Anxiety Inventory (BAI), to assess changes in anxiety symptoms. Supporting information P2 provides detailed information and characteristics of the included studies.28–66
Network Geometry
The network geometry (Figure 2) showed that most exercise interventions were compared with at least five nodes, forming a dense structure. The global design-by-treatment test was not significant (χ2 = 14.783, df = 24, P = 0.927), supporting transitivity and overall consistency. Network splitting identified inconsistency in only 2 of 45 comparisons (eg, aerobic vs resistance training). Although participant characteristics differed across groups (eg, yoga more common in females; Supporting Information P3), indirectness was incorporated into credibility ratings. Overall, no significant violations of transitivity were detected, indicating high model consistency and reliable evidence for comparing exercise interventions.
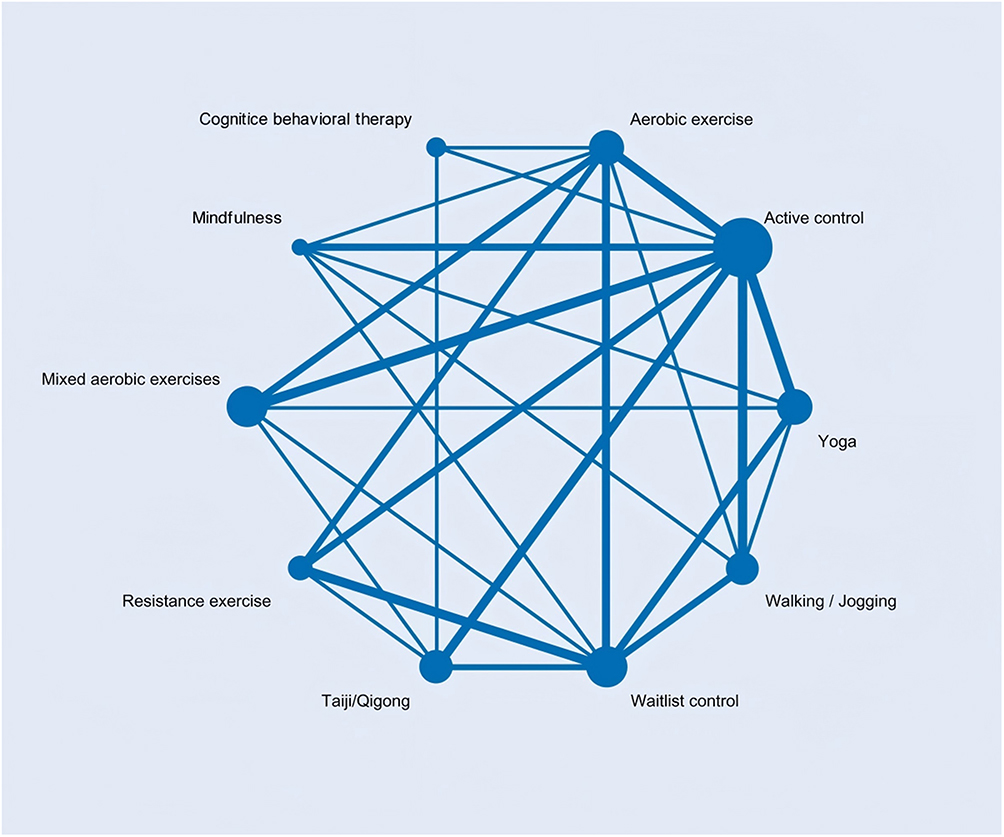 |
Figure 2 Network diagram. |
Risk of Bias in Included Studies
In this network meta-analysis, we comprehensively assessed risk of bias (Figure 3). Most studies lacked participant and personnel blinding, yielding unclear or high bias ratings that may have introduced expectancy effects. Sensitivity analyses showed that, despite variability in bias risk, effect sizes remained stable within credible intervals, supporting the robustness and reliability of the findings (Supporting information P4 and P5).
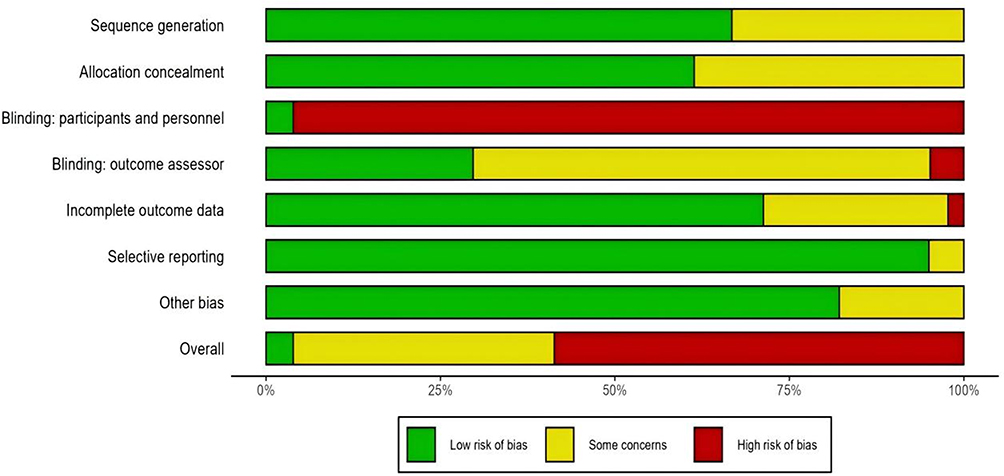 |
Figure 3 Risk of bias summary plot. |
Intervention Outcomes
This study systematically evaluated the effects of exercise interventions on anxiety through a network meta-analysis, providing predicted effects against active controls (Supporting Information P6 and Figure 4). Results showed substantial variation across exercise types, with meditation, yoga, and tai chi/qigong producing the strongest effects.
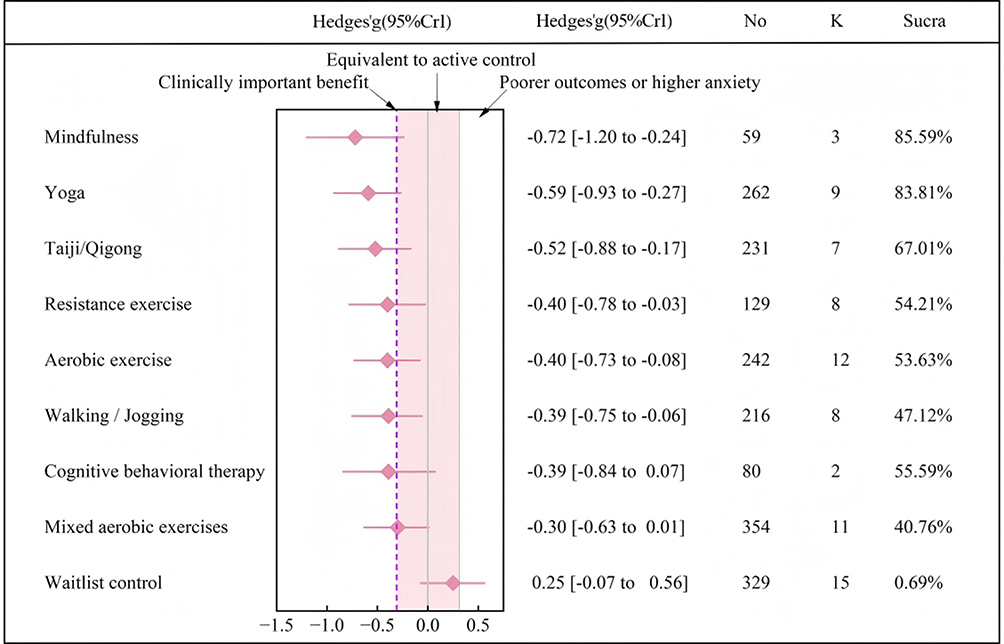 |
Figure 4 Predictive effects of exercise vs active control group. |
Meditation (k = 3, n = 59) yielded Hedges’ g = −0.72 (95% CI: −1.20 to −0.24), yoga (k = 9, n = 262) g = −0.59 (95% CI: −0.93 to −0.27), and tai chi/qigong (k = 7, n = 231) g = −0.52 (95% CI: −0.88 to −0.17). All exceeded the minimal clinically important difference (g = −0.31), highlighting their practical relevance. Among dynamic forms, resistance training (k = 8, n = 129) showed g = −0.40 (95% CI: −0.78 to −0.03), aerobic training (k = 12, n = 242) g = −0.40 (95% CI: −0.73 to −0.08), and walking/jogging (k = 8, n = 216) g = −0.39 (95% CI: −0.75 to −0.06). These moderate effects, while smaller than meditation, yoga, and tai chi/qigong, remained clinically meaningful. In contrast, mixed aerobic exercise (k = 11, n = 354) produced g = −0.30 (95% CI: −0.63 to 0.01), failing to reach statistical significance.
SUCRA rankings placed intervention efficacy as: meditation > yoga > tai chi/qigong > resistance training > aerobic exercise > walking/jogging (Figure 4). When compared with cognitive behavioral therapy (CBT), exercise—particularly static, breathing-focused activities such as yoga, meditation, and tai chi/qigong—demonstrated effects that, in some aspects, were not inferior, though findings should not replace systematic reviews.
Credibility Assessment
In the credibility assessment of this study, we analyzed the risk of bias of different interventions and its impact on the study results. Overall, the credibility of the interventions was rated as “low,” primarily due to limitations related to within-study bias and imprecision. Additionally, the majority of studies lacked direct comparisons with active control groups, and sample sizes were often fewer than ten, making it difficult to assess reporting bias, which limited the generalizability of the results. Notably, most studies showed high consistency between direct and indirect evidence, providing some support for the reliability of the overall findings (Supporting information P7).
Moderating Effects of Participant Characteristics
The study showed that age, gender, and comorbidity significantly moderated the effects of different interventions. Compared to the model including only exercise modalities (R2= 0.78), the addition of interaction variables such as gender (R2= 0.79), age (R2= 0.81), comorbidity (R2= 0.81), reporting (R2= 0.80), and funding support (R2= 0.79) increased the explanatory power of the model, indicating that these factors play an important role in moderating the effects of exercise interventions (Supporting information P8).
Specifically, gender significantly moderated the effects of exercise interventions. The results indicated that meditation had a more pronounced effect on anxiety reduction in females, whereas aerobic exercise, tai chi or qigong, resistance training, and yoga showed better effects in males. Furthermore, walking or jogging exhibited similar effects across genders, providing stable anxiety relief for both males and females (Figure 5). In terms of age, intervention effects also showed notable differences. Yoga, due to its low intensity and emphasis on breath regulation, was particularly suitable for older adults, helping reduce anxiety while also promoting physical and mental balance. Among younger individuals, resistance training and meditation showed more pronounced effects, suggesting adaptive differences in exercise intervention preferences between age groups (Figure 5).
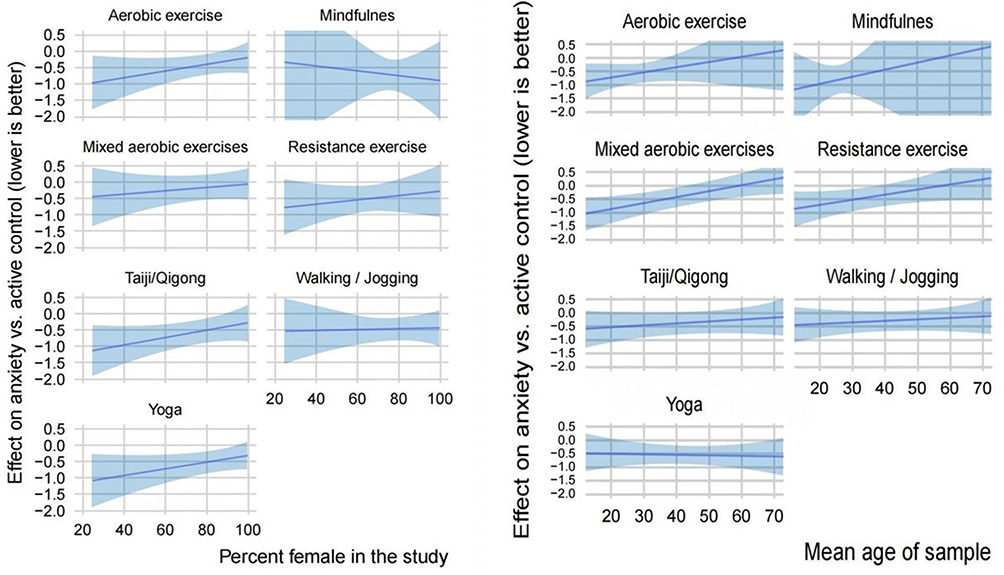 |
Figure 5 Effects of interventions versus active control on anxiety disorders (lower is better) by sex and age. Shading represents 95% credible intervals. |
In addition, comorbidity significantly influenced the effects of exercise interventions. Due to the wide confidence intervals and high variability in the effect of meditation, it was excluded from the comorbidity moderation analysis to provide a more accurate evaluation of other groups. The findings showed that exercise interventions were more effective for patients without comorbidities (g = −0.437, 95% CI = −0.871 to −0.017) compared to those with comorbidities (g = −0.22, 95% CI = −0.637 to 0.189). However, the effects of different exercise types varied in relation to whether comorbidities were reported (Supporting information P9). In groups without reported comorbidities, aerobic exercise, resistance training, and walking/jogging showed more substantial effects, with higher negative effect sizes, suggesting that these forms of exercise may be particularly effective in alleviating anxiety disorders in the absence of comorbidities. Furthermore, although the overall intervention effects for participants with comorbidities were lower, some forms of exercise, such as yoga and tai chi/qigong, still showed potential benefits, indicating that these interventions may be suitable for a broader population.
However, some uncertainty remained in the study results, particularly in certain subgroups (eg, yoga interventions among male participants), where relatively small sample sizes may have affected the accuracy of effect estimates for specific sub-populations. This statistical uncertainty, due to insufficient sample sizes, was more pronounced in smaller or specific subgroups, potentially impacting the reliability of these intervention effects.
Moderating Effects of Intervention and Design Characteristics
In this study, we examined moderating effects of intervention and design characteristics on anxiety reduction through network meta-analysis. Smaller exercise doses were effective (g = −0.673, 95% CI: −1.09 to −0.215), with modest increases at moderate levels (eg, 300 METs/week, g = −0.77, 95% CI: −1.06 to −0.499). Within the WHO-recommended range (600–1000 MET-min/week), exercise interventions showed stronger effects than active controls (g = −0.839, 95% CI: −1.143 to −0.568). However, higher doses produced no substantial additional benefits and even decreased effects (eg, 1500 METs/week, g = −0.817, 95% CI: −1.423 to −0.133) (Figure 6). Exercise intensity demonstrated a dose–response relationship, but effects remained below the threshold of clinical importance, with only slight gains at higher intensities (Supporting Information P10).
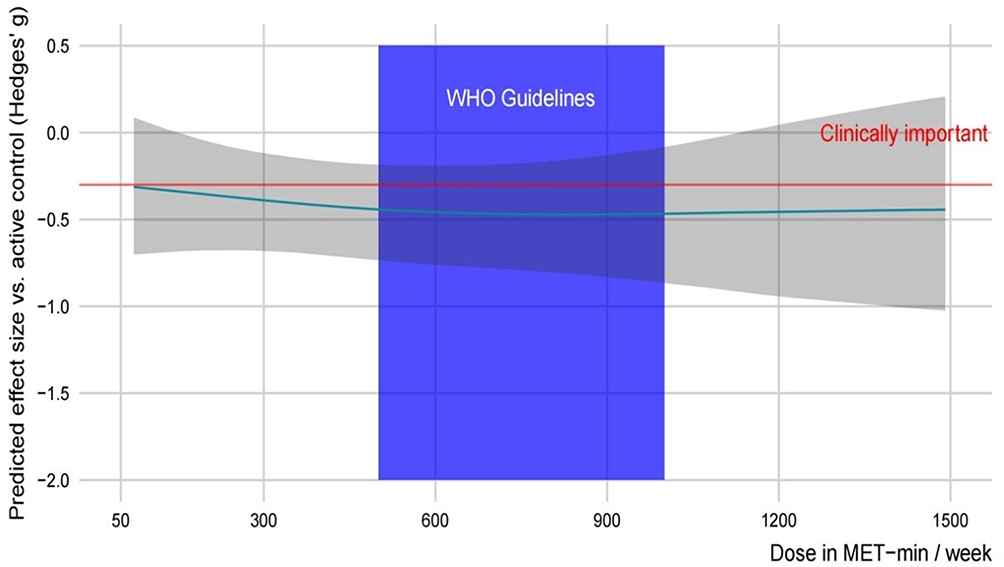 |
Figure 6 Dose in MET−min/week. |
Intervention duration was also influential: longer programs (12 weeks, g = −0.60, 95% CI: −0.70 to −0.11) were superior to shorter ones (3 weeks, g = −0.30, 95% CI: −0.76 to −0.03), indicating cumulative benefits with sustained engagement (Supporting Information P11). Funded trials (g = −0.455, 95% CI: −0.792 to −0.111) showed stronger effects than unfunded trials (g = −0.272, 95% CI: −0.777 to 0.253) (Supporting Information P12). Measurement methods mattered, as self-reported outcomes (g = −0.593, 95% CI: −1.055 to −0.15) exceeded clinician-reported outcomes (g = −0.181, 95% CI: −0.556 to 0.201) (Supporting Information P13).
Although anxiety severity (R2 = 0.63) and intervention type (R2 = 0.57) explained limited variance, moderation analyses revealed that interventions were more effective for mild anxiety (g = −0.774, 95% CI: −1.313 to −0.221) than for moderate (g = −0.103, 95% CI: −0.666 to 0.447) or severe cases (g = −0.119, 95% CI: −0.721 to 0.419). Individual exercise (g = −0.904, 95% CI: −1.453 to −0.456) outperformed group exercise (g = −0.717, 95% CI: −1.062 to −0.284), though group-based practices such as yoga, tai chi, qigong, and meditation achieved notable effects in specific contexts (Supporting Information P14).
Sensitivity Analysis
Supporting information P15 presents funnel plots for all exercise interventions compared with active control conditions. Overall, the funnel plots show a certain degree of asymmetry, suggesting potential publication bias. However, the pooled effect remained statistically significant after excluding high-risk studies. This indicates that, although publication bias may have some impact on the results, the overall robustness of the conclusions is maintained.
Discussion
Summary of Evidence
This study conducted a systematic review and network meta-analysis of randomized controlled trials to evaluate exercise interventions for anxiety disorders. Overall, exercise showed significant effects, with yoga, tai chi, and walking/jogging demonstrating the strongest outcomes. Meditative exercises (yoga, tai chi/qigong) produced the largest effects, while dynamic forms such as aerobic exercise and resistance training were effective in mild-to-moderate anxiety. Mixed aerobic exercise was not statistically significant except in isolated cases. Walking/jogging showed consistent effects across sexes, whereas meditation was more effective in females, and tai chi, qigong, and yoga in males. Older adults responded best to yoga, while younger individuals benefited more from aerobic exercise and meditation. Across varying doses and intensities, exercise remained beneficial, with the most favorable effects within the WHO-recommended range of 600–1000 MET-minutes/week. Benefits were consistent regardless of intensity, comorbidities, or baseline severity, supporting exercise as a broadly applicable and evidence-based intervention for individualized anxiety management.
The findings of this study are consistent with numerous previous studies, further substantiating the effectiveness of exercise interventions in alleviating anxiety symptoms. Several prior studies have demonstrated that static interventions, such as yoga, tai chi, and meditation, show significant efficacy in reducing anxiety.18,67–69 G Kirkwood reported that yoga help significantly reduce anxiety levels by promoting mental relaxation and emotional regulation, which aligns closely with the conclusions drawn from the current network meta-analysis. This provides additional support for the applicability of meditation, yoga, and tai chi as effective interventions for anxiety disorders.70 Furthermore, for adults diagnosed with anxiety or experiencing significant anxiety symptoms, high-intensity physical activity has been shown to be significantly more effective than low-intensity activity in alleviating anxiety, consistent with Aylett, who highlighted the substantial improvement associated with high-intensity exercise.71 Thus, this study not only validates previous research findings but also offers a comprehensive comparison and ranking of various exercise interventions, reinforcing the pivotal role of exercise in anxiety management.
Potential Mechanisms Underlying the Observed Associations
While the findings demonstrated significant effects of various forms of exercise in reducing anxiety disorders, the underlying causal mechanisms remain insufficiently established. As the present systematic review and network meta-analysis cannot establish causal relationships, the following discussion is limited to potential mechanisms suggested by previous experimental and theoretical literature. As previous research has suggested, the impact of exercise on mental health is often mediated through multiple physiological and psychological pathways, which may intertwine to create a complex intervention effect.72
The alleviation of anxiety disorders through exercise may result from a combination of factors, including social support, enhanced self-efficacy, immersion in natural environments, regulation of neurobiological mechanisms, and increased levels of brain-derived neurotrophic factor (BDNF).73–75 Each of these factors is closely linked to anxiety reduction, but a single exercise modality may not encompass all of these mechanisms. Therefore, different types of exercise may improve mental health through distinct pathways, with the interaction of multiple mechanisms potentially yielding greater overall effects.
Different forms of exercise alleviate anxiety through various mechanisms, each with its unique attributes. Meditative exercises (eg, yoga, tai chi) help create a relaxed mental state, enhancing self-efficacy, guiding participants to focus on the present moment, promoting mental relaxation, and improving stress-coping abilities.76 Resistance training, on the other hand, fosters confidence and self-efficacy through overcoming physical challenges, thereby increasing an individual’s confidence in coping with life’s stressors.77 Aerobic exercises (eg, running, swimming) primarily enhance cardiorespiratory fitness through physiological mechanisms and promote the secretion of endorphins and dopamine, resulting in a sense of exhilaration and alleviating emotional stress.78 Additionally, aerobic exercise may increase BDNF levels, promote neuronal growth, and enhance neuroplasticity, which can have positive effects on anxiety and other mood disorders.79
The effect of mixed aerobic exercise was relatively limited and did not reach statistical significance. One possible reason for this is that mixed aerobic exercise includes a variety of activities, and participants may find certain types unappealing or unsuitable, resulting in reduced adherence. Lower adherence can lead to insufficient exercise frequency and intensity, thereby affecting the efficacy of the intervention. Although mixed aerobic exercise may offer some benefits for anxiety in individual cases, it did not demonstrate statistically significant improvements overall.
Overall, meditative exercises and resistance training tend to exert their effects through psychological mechanisms, making them suitable for individuals seeking internal relaxation.80 Conversely, more vigorous exercises activate neurotransmitters and increase BDNF levels, providing rapid emotional relief, which may be preferable for those seeking immediate mood improvement.81 Based on these physiological and psychological mechanisms, different forms of exercise have distinct applicability for alleviating anxiety.
Therefore, future research should aim to explore “why” exercise is effective for reducing anxiety, rather than merely determining “if” it is effective. Understanding the specific mechanisms underlying the effects of different types of exercise on anxiety could help tailor individualized exercise prescriptions for individuals with anxiety, thereby more effectively alleviating symptoms and improving quality of life.
Strengths, Limitations and Future Directions
This study conducted a network meta-analysis to evaluate the efficacy of exercise interventions for anxiety disorders. Findings suggest that meditative forms of exercise (eg, yoga, meditation) show stronger anxiolytic effects, though evidence remains limited by small samples and restricted populations. Methodological challenges such as the difficulty of blinding in exercise trials may have introduced expectancy effects, and although publication bias was addressed, effect sizes may still be over- or underestimated. Also, The included studies encompassed heterogeneous populations, ranging from clinically diagnosed anxiety disorders to self-reported anxiety symptoms, which may influence responsiveness to exercise interventions. Future research should integrate unpublished data to enhance objectivity and employ individual patient data meta-analyses to clarify moderating factors such as age and gender, thereby enabling more personalized interventions. In addition, combining exercise-focused analyses with evidence from psychotherapeutic or pharmacological treatments would provide a more comprehensive picture of comparative effectiveness.
Conclusion
This network meta-analysis provides robust evidence that exercise interventions, across both meditative (eg, yoga, tai chi) and dynamic modalities (eg, aerobic and resistance training), demonstrated potentially beneficial effects on anxiety symptoms, particularly when practiced regularly and in moderation. Although the overall benefits were consistent, confidence in the effects of specific modalities remained low, underscoring the need for large-scale, high-quality trials to strengthen both internal and external validity.
Importantly, moderating effects of gender and age suggest that individualized prescriptions may optimize outcomes. Yoga appeared particularly beneficial for older men, while resistance training and aerobic exercise were more effective in younger women. Walking and jogging showed stable benefits across all groups, offering a flexible and safe option for self-management.
In conclusion, exercise should be incorporated as a core treatment strategy for anxiety. Beyond serving as an alternative to pharmacotherapy and psychotherapy, it can function as an adjunctive therapy to enhance treatment efficacy. Clinically, individualized exercise prescriptions not only alleviate anxiety but also improve overall health, reduce long-term risks, and substantially enhance quality of life.
Data Sharing Statement
The data that support the findings of this study are available in Figshare, reference number 10.6084/m9.figshare.28003526.
Acknowledgments
We extend our gratitude to Dr. Shaofeng Wang for his invaluable contributions to language editing. All content related to meta-analyses in this study was conducted in strict accordance with the guidelines of the *Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)*. The complete 27-item PRISMA checklist has been filled out (see Supplementary Materials for details).
Funding
This work was supported by the Excellent Young and Middle-aged Science and Technology Innovation Team Program of Universities in Hubei Province, focusing on “Sports Cultural Heritage and Health China” [grant numbers T201925). Additional funding was provided by the Fundamental Research Funds for the Central Universities, Huazhong University of Science and Technology [grant numbers 2024WKYXQN008), the Key Research and Development Program of Hubei Province [grant numbers 2020BCA089), the Major Project of Philosophy and Social Science Research of Hubei Provincial Department of Education, titled “Research on Effective Protection and Resource Exploitation and Utilization of Intangible Cultural Heritage of Jingchu Traditional Sports” [grant numbers 17ZD035]; the Guiding Project of Scientific Research Plan of Education Department of Hubei Province, focusing on “Historical Progress and Future Construction of Taijiquan Health Engineering Research” [grant numbers B2017228]; the Research Project supported by Young Teachers Research Fund of Wuhan Physical Education University, titled “Research on Inheritance of Jingchu Traditional Sports Culture and Effective Protection of Intangible Cultural Heritage” [grant numbers 2016QS11]; the Donghu Scholars Program of Wuhan Physical Education University (2018); and the Wuhan Sports University 2021 Young and Middle-aged Research Team, titled “National Traditional Sports and Health Promotion Innovation Team” [grant numbers 21KT12].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Penninx BW, Pine DS, Holmes EA, Reif A. Anxiety disorders. Lancet. 2021;397(10277):914–16. PubMed PMID: 33581801; PubMed Central PMCID: PMC9248771. doi:10.1016/s0140-6736(21)00359-7
2. Yang X, Fang Y, Chen H, et al. Global, regional and national burden of anxiety disorders from 1990 to 2019: results from the Global Burden of Disease Study 2019. Epidemiol Psychiatr Sci. 2021;30:e36. doi:10.1017/S2045796021000275
3. Szuhany KL, Simon NM. Anxiety disorders: a review. JAMA. 2022;328(24):2431–2445. PubMed PMID: 36573969. doi:10.1001/jama.2022.22744
4. DeGeorge KC, Grover M, Streeter GS. Generalized anxiety disorder and panic disorder in adults. Am Fam Physician. 2022;106(2):157–164. PubMed PMID: 35977134.
5. Daré LO, Bruand PE, Gérard D, et al. Co-morbidities of mental disorders and chronic physical diseases in developing and emerging countries: a meta-analysis. BMC Public Health. 2019;19(1):304. PubMed PMID: 30866883; PubMed Central PMCID: PMC6417021. doi:10.1186/s12889-019-6623-6
6. Chauvet-Gelinier JC, Bonin B. Stress, anxiety and depression in heart disease patients: a major challenge for cardiac rehabilitation. Ann Phys Rehabil Med. 2017;60(1):6–12. PubMed PMID: 27771272. doi:10.1016/j.rehab.2016.09.002
7. Strachan LP, Hyett MP, McEvoy PM. Imagery rescripting for anxiety disorders and obsessive-compulsive disorder: recent advances and future directions. Curr Psychiatry Rep. 2020;22(4):17. PubMed PMID: 32076845. doi:10.1007/s11920-020-1139-4
8. Wang Z, Whiteside SPH, Sim L, et al. Comparative effectiveness and safety of cognitive behavioral therapy and pharmacotherapy for childhood anxiety disorders: a systematic review and meta-analysis. JAMA Pediatr. 2017;171(11):1049–1056. PubMed PMID: 28859190; PubMed Central PMCID: PMC5710373. doi:10.1001/jamapediatrics.2017.3036
9. Slee A, Nazareth I, Bondaronek P, Liu Y, Cheng Z, Freemantle N. Pharmacological treatments for generalised anxiety disorder: a systematic review and network meta-analysis. Lancet. 2019;393(10173):768–777. PubMed PMID: 30712879. doi:10.1016/s0140-6736(18)31793-8
10. Choi NG, Choi BY, Marti CN, Kunik ME. Depression/anxiety symptoms and self-reported difficulty managing medication regimen among community-dwelling older adults. Gen Hosp Psychiatry. 2022;78:50–57. PubMed PMID: 35853418. doi:10.1016/j.genhosppsych.2022.07.005
11. Merz J, Schwarzer G, Gerger H. Comparative efficacy and acceptability of pharmacological, psychotherapeutic, and combination treatments in adults with posttraumatic stress disorder: a network meta-analysis. JAMA Psychiatry. 2019;76(9):904–913. PubMed PMID: 31188399; PubMed Central PMCID: PMC6563588. doi:10.1001/jamapsychiatry.2019.0951
12. Noetel M, Sanders T, Gallardo-Gómez D, et al. Effect of exercise for depression: systematic review and network meta-analysis of randomised controlled trials. BMJ. 2024;384:e075847. PubMed PMID: 38355154; PubMed Central PMCID: PMC10870815. doi:10.1136/bmj-2023-075847
13. Smith PJ, Merwin RM. The role of exercise in management of mental health disorders: an integrative review. Annu Rev Med. 2021;72:45–62. PubMed PMID: 33256493; PubMed Central PMCID: PMC8020774. doi:10.1146/annurev-med-060619-022943
14. Özkan SA, Kücükkelepce DS, Korkmaz B, Yılmaz G, Bozkurt MA. The effectiveness of an exercise intervention in reducing the severity of postpartum depression: a randomized controlled trial. Perspect Psychiatr Care. 2020;56(4):844–850. PubMed PMID: 32187390. doi:10.1111/ppc.12500
15. Marques A, Marconcin P, Werneck AO, et al. Bidirectional association between physical activity and dopamine across adulthood-a systematic review. Brain Sci. 2021;11(7):829. PubMed PMID: 34201523; PubMed Central PMCID: PMC8301978. doi:10.3390/brainsci11070829
16. Lin Y, Gao W. The effects of physical exercise on anxiety symptoms of college students: a meta-analysis. Front Psychol. 2023;14:1136900. PubMed PMID: 37063553; PubMed Central PMCID: PMC10100500. doi:10.3389/fpsyg.2023.1136900
17. Kazeminia M, Salari N, Vaisi-Raygani A, et al. The effect of exercise on anxiety in the elderly worldwide: a systematic review and meta-analysis. Health Qual Life Outcomes. 2020;18(1):363. PubMed PMID: 33176811; PubMed Central PMCID: PMC7656765. doi:10.1186/s12955-020-01609-4
18. Martínez-Calderon J, Casuso-Holgado MJ, Muñoz-Fernandez MJ, Garcia-Muñoz C, Heredia-Rizo AM. Yoga-based interventions may reduce anxiety symptoms in anxiety disorders and depression symptoms in depressive disorders: a systematic review with meta-analysis and meta-regression. Br J Sports Med. 2023;57(22):1442–1449. PubMed PMID: 37369553. doi:10.1136/bjsports-2022-106497
19. McDowell CP, Cook DB, Herring MP. The effects of exercise training on anxiety in fibromyalgia patients: a meta-analysis. Med Sci Sports Exerc. 2017;49(9):1868–1876. PubMed PMID: 28419024. doi:10.1249/mss.0000000000001290
20. Julian LJ. Measures of anxiety: State-Trait Anxiety Inventory (STAI), Beck Anxiety Inventory (BAI), and Hospital Anxiety and Depression Scale-Anxiety (Hads-A). Arthritis Care Res. 2011;63(Suppl 11):S467–72. PubMed PMID: 22588767; PubMed Central PMCID: PMC3879951. doi:10.1002/acr.20561
21. Ainsworth BE, Haskell WL, Herrmann SD, et al. 2011 compendium of physical activities: a second update of codes and MET values. Med Sci Sports Exerc. 2011;43(8):1575–1581. PubMed PMID: 21681120. doi:10.1249/MSS.0b013e31821ece12
22. Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. 2019;10(10):Ed000142. PubMed PMID: 31643080; PubMed Central PMCID: PMC10284251. doi:10.1002/14651858.Ed000142
23. Lin L, Zhang J, Hodges JS, Chu H. Performing arm-based network meta-analysis in R with the pcnetmeta Package. J Stat Softw. 2017;80. PubMed PMID: 28883783; PubMed Central PMCID: PMC5584882. doi:10.18637/jss.v080.i05
24. Dias S, Welton NJ, Sutton AJ, Ades AE. NICE decision support unit technical support documents. NICE DSU technical support document 2: a generalised linear modelling framework for pairwise and network meta-analysis of randomised controlled trials. London: National Institute for Health and Care Excellence (NICE); 2014.
25. Li X, Dusseldorp E, Su X, Meulman JJ. Multiple moderator meta-analysis using the R-package Meta-CART. Behav Res Methods. 2020;52(6):2657–2673. PubMed PMID: 32542441; PubMed Central PMCID: PMC7725699. doi:10.3758/s13428-020-01360-0
26. Papakonstantinou T, Nikolakopoulou A, Higgins JPT, Egger M, Salanti G. CINeMA: software for semiautomated assessment of the confidence in the results of network meta-analysis. Campbell Syst Rev. 2020;16(1):e1080. doi:10.1002/cl2.1080
27. Nikolakopoulou A, Higgins JPT, Papakonstantinou T, et al. CINeMA: an approach for assessing confidence in the results of a network meta-analysis. PLoS Med. 2020;17(4):e1003082. PubMed PMID: 32243458; PubMed Central PMCID: PMC7122720. doi:10.1371/journal.pmed.1003082
28. Abedi P, Nikkhah P, Najar S. Effect of pedometer-based walking on depression, anxiety and insomnia among postmenopausal women. Climacteric. 2015;18(6):841–845. PubMed PMID: 26100101. doi:10.3109/13697137.2015.1065246
29. Abrantes AM, Brown RA, Strong DR, et al. A pilot randomized controlled trial of aerobic exercise as an adjunct to OCD treatment. Gen Hosp Psychiatry. 2017;49:51–55. PubMed PMID: 29122148; PubMed Central PMCID: PMC5726421. doi:10.1016/j.genhosppsych.2017.06.010
30. Ahmadi A, Arastoo AA, Nikbakht M, Zahednejad S, Rajabpour M. Comparison of the effect of 8 weeks Aerobic and Yoga training on ambulatory function, fatigue and mood status in MS patients. Iran Red Crescent Med J. 2013;15(6):449–454. PubMed PMID: 24349740; PubMed Central PMCID: PMC3840829. doi:10.5812/ircmj.3597
31. Aidar FJ, Jaco de Oliveira R, Gama de Matos D, et al. A randomized trial of the effects of an aquatic exercise program on depression, anxiety levels, and functional capacity of people who suffered an ischemic stroke. J Sports Med Phys Fitness. 2018;58(7–8):1171–1177. PubMed PMID: 28488825. doi:10.23736/S0022-4707.17.07284-X
32. Arcos-Carmona IM, Castro-Sanchez AM, Mataran-Penarrocha GA, Gutierrez-Rubio AB, Ramos-Gonzalez E, Moreno-Lorenzo C. [Effects of aerobic exercise program and relaxation techniques on anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia: a randomized controlled trial]. Med Clin. 2011;137(9):398–401. PubMed PMID: 21345470. doi:10.1016/j.medcli.2010.09.045
33. Armat MR, Emami Zeydi A, Mokarami H, Nakhlband A, Hojjat SK. The impact of laughter yoga on depression and anxiety among retired women: a randomized controlled clinical trial. J Women Aging. 2022;34(1):31–42. PubMed PMID: 32552530. doi:10.1080/08952841.2020.1774225
34. Broman-Fulks JJ, Berman ME, Rabian BA, Webster MJ. Effects of aerobic exercise on anxiety sensitivity. Behav Res Ther. 2004;42(2):125–136. PubMed PMID: 14975776. doi:10.1016/S0005-7967(03)00103-7
35. Broman-Fulks JJ, Kelso K, Zawilinski L. Effects of a single bout of aerobic exercise versus resistance training on cognitive vulnerabilities for anxiety disorders. Cogn Behav Ther. 2015;44(4):240–251. PubMed PMID: 25789738. doi:10.1080/16506073.2015.1020448
36. Broocks A, Bandelow B, Pekrun G, et al. Comparison of aerobic exercise, clomipramine, and placebo in the treatment of panic disorder. Am J Psychiatry. 1998;155(5):603–609. PubMed PMID: 9585709. doi:10.1176/ajp.155.5.603
37. Caldwell KL, Bergman SM, Collier SR, et al. Effects of tai chi chuan on anxiety and sleep quality in young adults: lessons from a randomized controlled feasibility study. Nat Sci Sleep. 2016;8:305–314. PubMed PMID: 27895522; PubMed Central PMCID: PMC5118018. doi:10.2147/NSS.S117392
38. Chan SHW, Chan WWK, Chao JYW, Chan PKL. A randomized controlled trial on the comparative effectiveness of mindfulness-based cognitive therapy and health qigong-based cognitive therapy among Chinese people with depression and anxiety disorders. BMC Psychiatry. 2020;20(1):590. PubMed PMID: 33317481; PubMed Central PMCID: PMC7734764. doi:10.1186/s12888-020-02994-2
39. Chen HM, Tsai CM, Wu YC, Lin KC, Lin CC. Randomised controlled trial on the effectiveness of home-based walking exercise on anxiety, depression and cancer-related symptoms in patients with lung cancer. Br J Cancer. 2015;112(3):438–445. PubMed PMID: 25490525; PubMed Central PMCID: PMC4453645. doi:10.1038/bjc.2014.612
40. Cheng D, Wang X, Hu J, et al. Effect of Tai Chi and resistance training on cancer-related fatigue and quality of life in middle-aged and elderly cancer patients. Chin J Integr Med. 2021;27(4):265–272. PubMed PMID: 33420583. doi:10.1007/s11655-021-3278-9
41. Crombie KM, Cisler JM, Hillard CJ, Koltyn KF. Aerobic exercise reduces anxiety and fear ratings to threat and increases circulating endocannabinoids in women with and without PTSD. Ment Health Phys Act. 2021;20:100366. PubMed PMID: 34149867; PubMed Central PMCID: PMC8208522. doi:10.1016/j.mhpa.2020.100366
42. Davis K, Goodman SH, Leiferman J, Taylor M, Dimidjian S. A randomized controlled trial of yoga for pregnant women with symptoms of depression and anxiety. Complement Ther Clin Pract. 2015;21(3):166–172. PubMed PMID: 26256135. doi:10.1016/j.ctcp.2015.06.005
43. Edwards MK, Rosenbaum S, Loprinzi PD. Differential experimental effects of a short bout of walking, meditation, or combination of walking and meditation on state anxiety among young adults. Am J Health Promot. 2018;32(4):949–958. PubMed PMID: 29216745. doi:10.1177/0890117117744913
44. Falsafi N. A randomized controlled trial of mindfulness versus yoga: effects on depression and/or anxiety in college students. J Am Psychiatr Nurses Assoc. 2016;22(6):483–497. PubMed PMID: 27566622. doi:10.1177/1078390316663307
45. Ferreira RM, Alves W, de Lima TA, et al. The effect of resistance training on the anxiety symptoms and quality of life in elderly people with Parkinson’s disease: a randomized controlled trial. Arq Neuropsiquiatr. 2018;76(8):499–506. PubMed PMID: 30231121. doi:10.1590/0004-282X20180071
46. Field T, Diego M, Delgado J, Medina L. Tai chi/yoga reduces prenatal depression, anxiety and sleep disturbances. Complement Ther Clin Pract. 2013;19(1):6–10. PubMed PMID: 23337557; PubMed Central PMCID: PMC3730281. doi:10.1016/j.ctcp.2012.10.001
47. Gaudlitz K, Plag J, Dimeo F, Strohle A. Aerobic exercise training facilitates the effectiveness of cognitive behavioral therapy in panic disorder. Depress Anxiety. 2015;32(3):221–228. PubMed PMID: 25515221. doi:10.1002/da.22337
48. Gordon BR, McDowell CP, Lyons M, Herring MP. Resistance exercise training for anxiety and worry symptoms among young adults: a randomized controlled trial. Sci Rep. 2020;10(1):17548. PubMed PMID: 33067493; PubMed Central PMCID: PMC7567848. doi:10.1038/s41598-020-74608-6
49. Hardoerfer K, Jentschke E. Effect of yoga therapy on symptoms of anxiety in cancer patients. Oncol Res Treat. 2018;41(9):526–532. PubMed PMID: 30086538. doi:10.1159/000488989
50. Herring MP, Jacob ML, Suveg C, Dishman RK, O’Connor PJ. Feasibility of exercise training for the short-term treatment of generalized anxiety disorder: a randomized controlled trial. Psychother Psychosom. 2012;81(1):21–28. PubMed PMID: 22116310. doi:10.1159/000327898
51. Hovland A, Nordhus IH, Sjobo T, et al. Comparing physical exercise in groups to group cognitive behaviour therapy for the treatment of panic disorder in a randomized controlled trial. Behav Cogn Psychother. 2013;41(4):408–432. PubMed PMID: 22874661; PubMed Central PMCID: PMC3675676. doi:10.1017/S1352465812000446
52. Javnbakht M, Hejazi Kenari R, Ghasemi M. Effects of yoga on depression and anxiety of women. Complement Ther Clin Pract. 2009;15(2):102–104. PubMed PMID: 19341989. doi:10.1016/j.ctcp.2009.01.003
53. Jazaieri H, Goldin PR, Werner K, Ziv M, Gross JJ. A randomized trial of MBSR versus aerobic exercise for social anxiety disorder. J Clin Psychol. 2012;68(7):715–731. PubMed PMID: 22623316; PubMed Central PMCID: PMC4136448. doi:10.1002/jclp.21863
54. Kuvacic G, Fratini P, Padulo J, Antonio DI, De Giorgio A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: a randomized controlled trial. Complement Ther Clin Pract. 2018;31:262–267. PubMed PMID: 29705466. doi:10.1016/j.ctcp.2018.03.008
55. Kwok JYY, Kwan JCY, Auyeung M, et al. Effects of mindfulness yoga vs stretching and resistance training exercises on anxiety and depression for people with Parkinson disease: a randomized clinical trial. JAMA Neurol. 2019;76(7):755–763. PubMed PMID: 30958514; PubMed Central PMCID: PMC6583059. doi:10.1001/jamaneurol.2019.0534
56. Loh KP, Kleckner IR, Lin PJ, et al. Effects of a home-based exercise program on anxiety and mood disturbances in older adults with cancer receiving chemotherapy. J Am Geriatr Soc. 2019;67(5):1005–1011. PubMed PMID: 31034591; PubMed Central PMCID: PMC6544022. doi:10.1111/jgs.15951
57. O’Sullivan D, Gordon BR, Lyons M, Meyer JD, Herring MP. Effects of resistance exercise training on depressive symptoms among young adults: a randomized controlled trial. Psychiatry Res. 2023;326:115322. PubMed PMID: 37429171; PubMed Central PMCID: PMC12309288. doi:10.1016/j.psychres.2023.115322
58. Parker AG, Hetrick SE, Jorm AF, et al. The effectiveness of simple psychological and physical activity interventions for high prevalence mental health problems in young people: a factorial randomised controlled trial. J Affect Disord. 2016;196:200–209. PubMed PMID: 26926659. doi:10.1016/j.jad.2016.02.043
59. Philippot A, Dubois V, Lambrechts K, et al. Impact of physical exercise on depression and anxiety in adolescent inpatients: a randomized controlled trial. J Affect Disord. 2022;301:145–153. PubMed PMID: 35007642. doi:10.1016/j.jad.2022.01.011
60. Rosenbaum S, Sherrington C, Tiedemann A. Exercise augmentation compared with usual care for post-traumatic stress disorder: a randomized controlled trial. Acta Psychiatr Scand. 2015;131(5):350–359. PubMed PMID: 25443996. doi:10.1111/acps.12371
61. Ruiz-Comellas A, Valmana GS, Catalina QM, et al. Effects of physical activity interventions in the elderly with anxiety, depression, and low social support: a clinical multicentre randomised trial. Healthcare. 2022;10(11):2203. PubMed PMID: 36360543; PubMed Central PMCID: PMC9690598. doi:10.3390/healthcare10112203
62. Shavaisi F, Heydarpour S, Jalilian N, Jalali A, Rezaei M. The effects of positive psychology and physical activity on depression, anxiety, and stress among students with premenstrual syndrome: a single-blind, randomized controlled trial. BMC Womens Health. 2024;24(1):499. PubMed PMID: 39256784; PubMed Central PMCID: PMC11385119. doi:10.1186/s12905-024-03333-3
63. Smits JA, Berry AC, Rosenfield D, Powers MB, Behar E, Otto MW. Reducing anxiety sensitivity with exercise. Depress Anxiety. 2008;25(8):689–699. PubMed PMID: 18729145. doi:10.1002/da.20411
64. Steptoe A, Edwards S, Moses J, Mathews A. The effects of exercise training on mood and perceived coping ability in anxious adults from the general population. J Psychosom Res. 1989;33(5):537–547. PubMed PMID: 2795526. doi:10.1016/0022-3999(89)90061-5
65. Whitworth JW, Nosrat S, SantaBarbara NJ, Ciccolo JT. Feasibility of resistance exercise for posttraumatic stress and anxiety symptoms: a randomized controlled pilot study. J Trauma Stress. 2019;32(6):977–984. PubMed PMID: 31743507. doi:10.1002/jts.22464
66. Zhang J, Gao T, Li Y, et al. The effect of Bafa Wubu of Tai Chi on college students’ anxiety and depression: a randomized, controlled pilot study. Front Physiol. 2023;14:1036010. PubMed PMID: 36760533; PubMed Central PMCID: PMC9905723. doi:10.3389/fphys.2023.1036010
67. Saeed SA, Cunningham K, Bloch RM. Depression and anxiety disorders: benefits of exercise, yoga, and meditation. Am Fam Physician. 2019;99(10):620–627. PubMed PMID: 31083878.
68. Gonzalez M, Pascoe MC, Yang G, et al. Yoga for depression and anxiety symptoms in people with cancer: a systematic review and meta-analysis. Psychooncology. 2021;30(8):1196–1208. PubMed PMID: 33763925. doi:10.1002/pon.5671
69. Song Y, Lindquist R. Effects of mindfulness-based stress reduction on depression, anxiety, stress and mindfulness in Korean nursing students. Nurse Educ Today. 2015;35(1):86–90. PubMed PMID: 25066651. doi:10.1016/j.nedt.2014.06.010
70. Kirkwood G, Rampes H, Tuffrey V, Richardson J, Pilkington K. Yoga for anxiety: a systematic review of the research evidence. Br J Sports Med. 2005;39(12):
71. Aylett E, Small N, Bower P. Exercise in the treatment of clinical anxiety in general practice - a systematic review and meta-analysis. BMC Health Serv Res. 2018;18(1):559. PubMed PMID: 30012142; PubMed Central PMCID: PMC6048763. doi:10.1186/s12913-018-3313-5
72. Paluska SA, Schwenk TL. Physical activity and mental health: current concepts. Sports Med. 2000;29(3):167–180. PubMed PMID: 10739267. doi:10.2165/00007256-200029030-00003
73. St Clair Gibson A, Swart J, Tucker R. The interaction of psychological and physiological homeostatic drives and role of general control principles in the regulation of physiological systems, exercise and the fatigue process - The Integrative Governor theory. Eur J Sport Sci. 2018;18(1):25–36. PubMed PMID: 28478704. doi:10.1080/17461391.2017.1321688
74. Liu M, Shi B. The effect of physical exercise on the anxiety of college students in the post-pandemic era: the mediating role of social support and proactive personality. Front Psychol. 2023;14:1128748. PubMed PMID: 37008871; PubMed Central PMCID: PMC10056215. doi:10.3389/fpsyg.2023.1128748
75. Holmes PV. Trophic mechanisms for exercise-induced stress resilience: potential role of interactions between BDNF and Galanin. Front Psychiatry. 2014;5:90. PubMed PMID: 25120496; PubMed Central PMCID: PMC4112800. doi:10.3389/fpsyt.2014.00090
76. Brown RP, Gerbarg PL. Sudarshan Kriya yogic breathing in the treatment of stress, anxiety, and depression: part I-neurophysiologic model. J Altern Complement Med. 2005;11(1):189–201. PubMed PMID: 15750381. doi:10.1089/acm.2005.11.189
77. Zhang F, Wang Z, Su H, et al. Effect of a home-based resistance exercise program in elderly participants with osteoporosis: a randomized controlled trial. Osteoporos Int. 2022;33(9):1937–1947. PubMed PMID: 35704055. doi:10.1007/s00198-022-06456-1
78. Schoenfeld TJ, Swanson C. A Runner’s high for new neurons? Potential role for endorphins in exercise effects on adult neurogenesis. Biomolecules. 2021;11(8):1077. PubMed PMID: 34439743; PubMed Central PMCID: PMC8392752. doi:10.3390/biom11081077
79. Mang CS, Campbell KL, Ross CJ, Boyd LA. Promoting neuroplasticity for motor rehabilitation after stroke: considering the effects of aerobic exercise and genetic variation on brain-derived neurotrophic factor. Phys Ther. 2013;93(12):1707–1716. PubMed PMID: 23907078; PubMed Central PMCID: PMC3870490. doi:10.2522/ptj.20130053
80. Herbert C. Enhancing mental health, well-being and active lifestyles of university students by means of physical activity and exercise research programs. Front Public Health. 2022;10:849093. PubMed PMID: 35548074; PubMed Central PMCID: PMC9082407. doi:10.3389/fpubh.2022.849093
81. Cotman CW, Berchtold NC. Exercise: a behavioral intervention to enhance brain health and plasticity. Trends Neurosci. 2002;25(6):295–301. PubMed PMID: 12086747. doi:10.1016/s0166-2236(02)02143-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Exercise Rehabilitation an Effective Adjuvant to Clinical Treatment for Myofascial Trigger Points? A Systematic Review and Meta-Analysis
Zhou Y, Lu J, Liu L, Wang HW
Journal of Pain Research 2023, 16:245-256
Published Date: 28 January 2023
Comparison of Mobile Health-Based Exercise vs Traditional Exercise for Chronic Neck Pain: A Systematic Review and Meta-Analysis
He X, Zhou H, Jiang YS, Liu DC, Qi F, Wang Z
Journal of Pain Research 2025, 18:4639-4649
Published Date: 7 September 2025
Efficacy of Cognitive Behavioral Therapy Combined with Exercise in Patients with Chronic Pain: A Systematic Review and Meta-Analysis
Zhang YZ, Yang B, Jiang CH, Guo YX, Lai XX, Zhang WQ, Zhang H
Journal of Pain Research 2026, 19:599315
Published Date: 23 April 2026
Exercise Training Improves Depression and Anxiety in Patients with COPD: A Dose-Response Meta-Analysis of Randomized Controlled Trials
Chen S, Shang B, Bi Y, Xu R, Li Q, Zhang W, Yang Y, Hu S
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:578054
Published Date: 6 May 2026