Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Common Biomarkers and Pathogenesis of Inflammatory Bowel Disease and Breast Cancer: Mendelian Randomization and Multi-Omics Studies
Authors Zhang D, Guan Y, Tang H, Xue Q, Li X, Bin X, You F
Received 11 June 2025
Accepted for publication 26 November 2025
Published 8 December 2025 Volume 2025:17 Pages 1183—1197
DOI https://doi.org/10.2147/BCTT.S546371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Daqing Zhang,1 Yongjun Guan,1 Haitao Tang,2 Qingze Xue,2 Xiaoqiang Li,2 Xu Bin,3 Faping You2
1Department of General Surgery, Beijing Friendship Hospital, Capital Medical University,State Key Lab of Digestive Health,National Clinical Research Center for Digestive Diseases, Beijing, People’s Republic of China; 2Department of Breast Surgery, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China; 3Department of Pathology, Shengli Oilfield Central Hospital, Dongying, Shandong, People’s Republic of China
Correspondence: Faping You, Email [email protected] Xu Bin, Email [email protected]
Background: Inflammatory bowel disease (IBD) and breast cancer represent significant global health burdens. Although epidemiological studies have suggested a potential link between them, the causal relationship and underlying molecular mechanisms remain unclear. This study employed Mendelian randomization (MR) and multi-omics approaches to investigate the causal association between IBD and breast cancer and to explore shared genetic biomarkers and pathological pathways.
Methods: A two-sample MR analysis was performed using genome-wide association study (GWAS) data. Shared genes were identified and validated using the GEO and TCGA databases. THBS3 expression was further verified in human breast cancer tissues via immunohistochemistry and RT-PCR. Immune infiltration analysis, drug sensitivity assessment, molecular docking, ceRNA network construction, and pathway enrichment analyses (GSEA and GSVA) were conducted to explore the functional role of THBS3.
Results: MR analysis indicated that IBD significantly increases the risk of breast cancer. THBS3 was identified as a commonly overexpressed gene in both diseases and was associated with poor prognosis. THBS3-high breast cancer patients exhibited resistance to Dinaciclib, Daporinad, and Rapamycin. Molecular docking and dynamics simulations confirmed a strong binding affinity between THBS3 and Rapamycin. A ceRNA network linked THBS3 to miR-423-5p and chemotherapy resistance-related lncRNAs. Pathway analyses revealed THBS3 involvement in extracellular matrix receptor interaction and proteasome pathways.
Conclusion: This study provides genetic evidence supporting IBD as a risk factor for breast cancer and highlights THBS3 as a key shared biomarker. THBS3 may promote breast cancer progression through immune regulation, ECM remodeling, and drug resistance mechanisms, suggesting its potential as a therapeutic target. These findings support enhanced breast cancer screening in IBD patients.
Keywords: IBD, Crohn’s disease, ulcerative colitis, breast cancer, Mendelian randomization
Introduction
Inflammatory bowel disease (IBD) includes Crohn’s disease and ulcerative colitis.1,2 The pathogenesis of IBD is highly complex, making it difficult to cure completely, and its incidence is gradually increasing. Meanwhile, breast cancer ranks among the most common cancers in women worldwide.3 Despite differences in incidence rates, some epidemiological studies suggest that patients with IBD may be more susceptible to developing breast cancer compared to the general population. Furthermore, some studies have found a higher proportion of breast cancer patients who also have IBD.4–6 However, other research has found no association between IBD and breast cancer, leading to controversy in the epidemiological data.7 These observational studies are susceptible to various confounding factors, such as disease activity, during implementation, making it challenging to determine the relationship between IBD and breast cancer. Mendelian randomization (MR) employs summary data from genome-wide association studies (GWAS) to identify single nucleotide polymorphisms (SNPs) that are strongly correlated with the traits of interest, using them as instrumental variables for genetic prediction. This approach minimizes the impact of confounding factors and helps mitigate reverse causality.8 While epidemiological studies suggest an association between IBD and breast cancer, a critical knowledge gap persists in the field: no study has systematically explored the shared genetic drivers and immune-mediated pathways linking these diseases through an integrated MR and multi-omics analytical approach. THBS3, as an extracellular matrix protein, acts as an adhesion molecule and participates in various biological processes, including tissue remodeling, angiogenesis, and tumorigenesis.9,10 It is highly expressed in multiple tumors and is associated with poor prognosis.11–13 Specifically, the bridging role of the THBS3-mediated immunoregulatory mechanism remains unelucidated. We hypothesize that IBD may causally increase breast cancer risk via immune dysregulation through shared genetic loci, with the THBS3-mediated ceRNA network serving as a critical hub for cross-disease immune regulation. Our findings provide a basis for early breast cancer screening in IBD patients (Figure 1).
 |
Figure 1 Flow chart of the study. |
Materials and Methods
MR Analysis
We obtained data from the GWAS database (https://www.ebi.ac.uk/gwas/home). The GWAS ID for IBD is ebi-a-GCST004131, and for breast cancer, it is ieu-a-1131. Data related to IBD were obtained from a GWAS study conducted by de Lange KM et al, including 25,042 European cases and 34,915 European ancestry controls. Data related to breast cancer were obtained from a GWAS study conducted by de Michailidou K et al, including 14910 European cases and 17588 European ancestry controls (Table 1). All data utilized in this study were obtained from publicly available databases, eliminating the requirement for further ethical approval.
 |
Table 1 Basic Information About the Exposure Group and the Outcome Group in the Study |
We performed MR analysis to explore the causal link between IBD and breast cancer, using techniques such as Inverse Variance Weighted (IVW), MR-Egger, Weighted Median (WME), and Weighted Mode (WM). We selected SNPs strongly associated with IBD and breast cancer at genome-wide significance (P < 5×10−8). We performed linkage disequilibrium (LD) pruning (r2 < 0.001, kb = 10,000) and excluded SNPs correlated with potential confounders. We evaluated instrument strength using the F statistic (all SNPs had F > 10), excluding weak instrument bias. We obtained causal estimates using IVW, MR-Egger, WME, and WM. We assessed horizontal pleiotropy via MR-Egger intercept and funnel plots, and heterogeneity via Cochran’s Q test and leave-one-out sensitivity analysis. We conducted all analyses using the Two Sample MR package in R (version 4.4.1). A schematic of SNP selection and quality control is in Supplementary figure 1.
Analysis of IBD and Breast Cancer-Associated Genes
We used MR to analyze genes associated with IBD and breast cancer. We employed the “Venn Diagram” package to extract common genes, depicted using Venn diagrams and forest plots.
TCGA Database
The Cancer Genome Atlas (TCGA) is an open-access database that provides comprehensive data on 33 cancer types, including RNA-Seq gene expression (HTSeq-FPKM), clinical information, survival statistics, mRNA-based stemness scores (RNAss), and DNA methylation (DNAss) data.14 We analyzed THBS3 expression in 33 cancers via Sangerbox 3.0 (http://sangerbox.com/).
GEO Database
The Gene Expression Omnibus (GEO) database is managed and curated by the National Center for Biotechnology Information (NCBI). Since its establishment in 2000, GEO has collected gene expression data from research institutions worldwide, encompassing tumor and non-tumor samples, chips, NGS, differential analysis, and molecular validation, among other areas, as a freely accessible public database.15 IBD dataset (GSE179285) and breast cancer dataset (GSE70947) were downloaded separately from the GEO database.
Human Samples
Human samples were exclusively collected for breast cancer analysis. Pathological sections of 20 cases of breast cancer were collected from Shengli Oilfield Central Hospital (Dongying City, Shandong Province) from April 2024 to September 2024. We removed normal tissue adjacent to the primary tumor, ensuring a margin >2 cm from the tumor site. Demographic and clinicopathological characteristics were as follows: median age 59 years (range: 53–79 years); tumor stage distribution—Stage I (n = 2), Stage II (n = 17), Stage III (n =1) based on AJCC 8th edition; histological subtype—all are invasive ductal carcinomas (n = 20). None of the 20 breast cancer patients had IBD.
Ethics Statement
We conducted all human subjects were carried out in compliance with the ethical guidelines and protocols sanctioned by the Ethics Committee of Shengli Oilfield Central Hospital (Approval no. YXLL202406301). We obtained written informed consent from all patients.
Immunohistochemistry
We detected THBS3 expression in breast cancer tissues using an antibody from Abmart (1:200, Rabbit, Shanghai, China), as described previously.16
RT-PCR
We extracted total RNA from breast cancer and adjacent normal tissues using Trizol, reverse-transcribed RNA into cDNA, and performed qPCR on a BIO-RAD system with SYBR Premix Ex Taq™ II (Takara, Dalian, China). Primer sequences: THBS3 forward: CTCGGCAGATGGTAGCTGTG, reverse: TGGATAAGAGGTAGATGTCCCCA; GAPDH forward: GGAAGCTTGTCATCAATGGAAATC, reverse: TGATGACCCTTGGCTCCC. We quantified relative THBS3 expression using the 2−ΔΔCt method.17
Immune Infiltration Analysis and Its Correlation with THBS3
We used the CIBERSORT algorithm to quantify 22 immune cell types in IBD and breast cancer. We visualized results with the vioplot package in R, generated a correlation matrix, and performed Spearman correlation analysis between hub gene expression and immune cell abundance.
Drug Sensitivity Analysis
Based on the GDSC database (www.cancerrxgene.org),18 the association between THBS3 expression and the half-maximal inhibitory concentration (IC50) of chemotherapeutic drugs was evaluated using regression analysis.
Molecular Docking Method
We performed molecular docking was performed using PyRx/Vina to analyze the binding energy and interaction patterns between THBS3 and the drugs, utilizing the predicted structure of THBS3 (Uniprot ID: P49746) and drug data from PubChem. We resolved protein-ligand interactions were resolved using LigPlus, and results were visualized with PyMOL.
GSEA and GSVA
For GSEA, THBS3 expression levels were divided into high and low groups, and gene set enrichment analysis was performed using the “GSEA” function from the clusterProfiler package in R. The reference gene set was c2.cp.kegg.Hs.symbols.gm. A false discovery rate (FDR) < 0.25 was adopted as the statistical cutoff, in line with the Broad Institute GSEA guidelines, to balance sensitivity and specificity in exploratory pathway discovery.19 P-values < 0.05 were also considered significant. GSVA was conducted using the Molecular Signatures Database gene sets, applying the gsva package with default Gaussian kernel estimation.
Construct the ceRNA Network
We predicted THBS3-targeting miRNAs using miRanda, miRDB, and TargetScan, selecting miRNAs present in all three databases. We used spongeScan to predict lncRNA-miRNA interactions and identified miRNA-lncRNA pairs. We constructed the ceRNA network with Cytoscape.
Results
MR Analysis Results
Our MR analysis demonstrated a causal relationship between IBD and breast cancer. Both the weighted median and IVW methods yielded statistically significant results. The Weighted median analysis indicated a positive association (OR = 1.060, 95% CI: 0.985–1.141; P = 0.053), and the IVW results similarly showed this relationship (OR = 1.053, 95% CI: 1.021–1.086; P = 0.001). Since the β values of the other three methods aligned with IVW, we conclude that IBD increases breast cancer risk (Table 2, Figure 2A).
 |
Table 2 MR Analysis Results of Association Between Inflammatory Bowel Disease and Breast Cancer |
 |
Figure 2 (A) Inflammatory bowel disease and breast cancer: Mendelian randomization effect size. (B) Inflammatory bowel disease and breast cancer two sample Mendelian randomization funnel plot. (C) Scatter plot of the results of the Mendelian randomization study on inflammatory bowel disease and breast cancer. (D) Sensitivity analysis results of inflammatory bowel disease and breast cancer. |
Heterogeneity and Pleiotropy Analysis
The Cochran Q test showed no heterogeneity (MR-Egger Q = 103.516, P = 0.680; IVW Q = 103.552, P = 0.703). The MR-Egger regression indicated no horizontal pleiotropy (Egger intercept = −0.00088, SE = 0.0046, P = 0.84938) (Table 3). Funnel plot analysis confirmed symmetry in causal effect estimates, supporting the absence of pleiotropy (Figure 2B and C).
 |
Table 3 Heterogeneity Statistics |
Sensitivity Analysis Results
The leave-one-out test results indicated that after systematically excluding each SNP, the IV analysis outcomes for the remaining SNPs were consistent with those obtained when all SNPs were included. No single SNP was found to have a significant impact on the estimated causal association between IBD and breast cancer (Figure 2D). This consistency indicates a lack of heterogeneity, further validating the robustness of the results.
Genes Associated with IBD and Breast Cancer
Using five MR methods, we identified 332 IBD-related and 562 breast cancer-related genes. We found 5 common highly expressed genes and 15 low expressed genes (Figure 3A and B). Forest plots showed that FCGRT, METTL27, THBS3, MAGEF1, and ANXA6 are high-risk genes (Figure 3C), while KCTD7, SLC9A3-AS1, HLA-F, SLC22A5, SLC22A4, TRIM64B, UBE2F, SETD9, ATG10, INPP5E, CTSK, PRDM15, PRR5L, OSER1, and IL18R1 are low-risk genes (Figure 3D).
 |
Figure 3 (A) Identify differentially expressed genes between two diseases through intersection filtering (high expression); blue is breast cancer, purple is IBD. (B) Identify differentially expressed genes between two diseases through intersection filtering (Low expression); blue is breast cancer, purple is IBD. (C) The forest plot shows genes associated with inflammatory bowel disease (P-values of less than 0.05 are shown in bold). (D) The forest plot shows genes associated with breast cancer (P-values of less than 0.05 are shown in bold). |
Validation of Gene Expression Using the GEO Database
We validated gene expression in IBD (GSE179285) and breast cancer (GSE70947) datasets. The results showed differential expression of METTL27, MAGEF1, ATG10, SETD9, SLC22A5, THBS3, ANXA6, IL18R1, CTSK, UBE2F, and HLA-F in the IBD dataset (GSE179285) (Supplementary figure 2A), with significant correlations observed among these genes (Supplementary figure 2B). In the breast cancer dataset (GSE70947), FCGRT, THBS3, MAGEF1, ANXA6, PRR5L, PRDM15, ATG10, SLC22A4, and KCTD7 were differentially expressed, and significant correlations were also found among these genes (Supplementary figure 2C and D). The intersection of the significantly expressed genes from the IBD dataset (GSE179285) and the breast cancer dataset (GSE70947) identified THBS3, MAGEF1, ANXA6, and ATG10 as genes co-expressed in both IBD and breast cancer (Supplementary figure 2E). Among them, THBS3 was highly expressed in both IBD and breast cancer but had low expression in normal groups. Previous research has identified that THBS3 plays a pivotal role in tumor development.11,12,20 Therefore, we will further analyze the function of THBS3 in IBD and breast cancer.
Expression of THBS3 Gene in IBD and Breast Cancer
We analyzed THBS3 expression in 33 cancers via Sangerbox3.0 and found overexpression in 16 types, including breast cancer (Figure 4A). Immunohistochemistry confirmed elevated THBS3 in breast cancer (Figure 4B and C). Both IHC and RT-PCR showed significantly higher THBS3 levels in cancer tissues than in adjacent normal tissues (Figure 4D). Similarly, in the GEO database, THBS3 is highly expressed in both ulcerative colitis and Crohn’s disease (Supplementary figure 3A and B).
 |
Figure 4 (A) The expression of THBS3 in 33 cancers and normal groups was analyzed by TCGA database. (B and C) The expression of THBS3 in breast cancer and adjacent tissues was analyzed by immunohistochemistry. (D) The expression of THBS3 in breast cancer and adjacent tissues was analyzed by RT-PCR; *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001, ns P >0.05. |
Association Between THBS3 and Immune Infiltration
We analyzed immune infiltration in IBD (GSE179285) and breast cancer (GSE70947) using CIBERSORT. In IBD, memory B cells, plasma cells, CD8⁺ T cells, CD4⁺ naïve T cells, activated memory CD4⁺ T cells, follicular helper T cells, Tregs, gamma delta T cells, M0, M1, and M2 macrophages, and resting dendritic cells were more abundant than in normal tissue (P < 0.05) (Supplementary figure 4A and B), with correlations among cells (Supplementary figure 4C). In breast cancer, memory B cells, plasma cells, CD8⁺ T cells, CD4⁺ naïve T cells, activated memory CD4⁺ T cells, follicular helper T cells, Tregs, gamma delta T cells, M0 and M1 macrophages were more abundant (P < 0.05) (Supplementary figure 5A and B), with correlations (Supplementary figure 5C).THBS3 expression in the IBD dataset (GSE179285) and the breast cancer dataset (GSE70947) was divided into high-expression and low-expression groups, and the immune cell profiles of the two groups were analyzed. In the IBD cohort, beyond CD4⁺ T subsets, naïve B cells and Tregs were enriched in the THBS3-high group and positively correlated with THBS3, whereas activated CD4 memory T cells showed a negative correlation and resting CD4 memory T cells a positive correlation (Supplementary figure 6A and B). In breast cancer, beyond CD4⁺ T subsets, CD8⁺ T cells were enriched in the THBS3-high group and positively correlated with THBS3, while both activated and resting CD4 memory T cells were negatively correlated (Supplementary figure 6C and D).
THBS3 and Drug Sensitivity Analysis
We divided THBS3 into high and low expression groups and compared IC50 values. We found that Dinaciclib, Daporinad, and Rapamycin had significantly higher IC50 in the THBS3-high group (P < 0.05) (Figure 5A–C).
 |
Figure 5 (A) Expression of THBS3 and its sensitivity to Daporinad. (B) Expression of THBS3 and its sensitivity to Dinaciclib. (C) Expression of THBS3 and its sensitivity to Rapamycin. (D) Molecular docking of THBS3 with Daporinad. (E) Molecular docking of THBS3 with Dinaciclib. (F) Molecular docking of THBS3 with Rapamycin. |
Molecular Docking Results
Molecular docking was conducted to assess the binding affinity between the target drugs and THBS3 (Figure 5D–F). Each candidate drug is connected to THBS3 via visible hydrogen bonds and strong electrostatic interactions. Rapamycin demonstrated the lowest binding energy (−7.884 kcal/mol), indicating a highly stable interaction (Table 4). To further analyze the role of THBS3 in the context of Dinaciclib, Daporinad, and Rapamycin, we conducted molecular dynamics simulations. Integrated analysis employing molecular dynamics simulations and energy calculations revealed that the Rapamycin-formed complex exhibits the greatest stability and the tightest binding to the THBS3 protein (Supplementary Figure 7, Supplementary Figure 8). This complex demonstrated minimal structural fluctuations, highest compactness, and the greatest number of hydrogen bonds. In contrast, Daporinad and Dinaciclib exhibited weaker binding and greater structural flexibility, resulting in less stable complexes (Supplementary Table 1). The detailed methodologies and corresponding results are presented in Supplementary Materials 1 and 2.
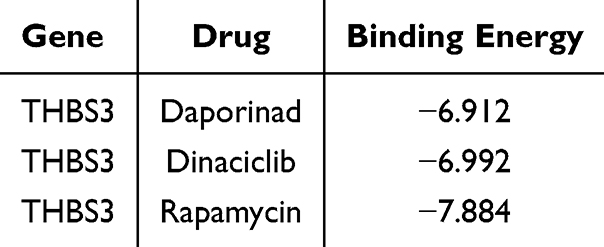 |
Table 4 The Docking Results of Small Molecules |
Construction of the ceRNA Network
The miRanda, miRDB, and TargetScan databases were utilized to predict target genes, and miRNAs interacting with THBS3 were analyzed. The intersection with differentially expressed miRNAs identified 10 interacting miRNAs (Supplementary table 2). Furthermore, the spongeScan database was employed to predict lncRNAs that interact with these differentially expressed miRNAs, and their overlap with differentially expressed lncRNAs revealed 22 interacting lncRNAs (Supplementary table 3). The mRNA-miRNA-lncRNA interaction network was then integrated into the ceRNA framework, with hsa-miR-423-5p and hsa-miR-185-3p interacting with multiple lncRNAs (Supplementary table 4, Figure 6A).
 |
Figure 6 (A) Construction of the ceRNA network. Red nodes represent mRNAs, yellow nodes represent miRNAs, and blue nodes represent lncRNAs. Each line indicates interactions between mRNAs and miRNAs, as well as between miRNAs and lncRNAs. (B) GSEA analysis in IBD. (C) GSEA analysis in breast cancer. (D) GSVA analysis in IBD. (E) GSVA analysis in breast cancer. |
GSEA and GSVA
GSEA analysis revealed that in IBD, THBS3 is associated with focal adhesion, ECM receptor interaction, leukocyte transendothelial migration, vascular smooth muscle contraction, and FC gamma R-mediated phagocytosis (Figure 6B, Table 5). In breast cancer, THBS3 is associated with ECM receptor interaction, hypertrophic cardiomyopathy (HCM), focal adhesion, dilated cardiomyopathy, and arrhythmogenic right ventricular cardiomyopathy (Figure 6C, Supplementary table 5). Notably, both IBD and breast cancer are related to ECM receptor interaction.GSVA analysis showed that in IBD (Figure 6D), THBS3 is associated with proteasome, cysteine and methionine metabolism, sphingolipid metabolism, interactions in vesicular transport, and DNA replication. In breast cancer (Figure 6E), THBS3 is associated with proteasome, basal transcription factors, ascorbate and aldarate metabolism, citrate cycle (TCA cycle), pyruvate metabolism, and propanoate metabolism, with both IBD and breast cancer being linked to the proteasome pathway.
 |
Table 5 The GSEA Analysis Results of IBD |
Discussion
We gathered datasets on IBD and breast cancer from public repositories and investigated their causal relationship using two-sample MR. The IVW method revealed that IBD increases breast cancer risk. Tests for heterogeneity, pleiotropy, and sensitivity confirmed the robustness of these findings. In previous studies, conflicting evidence regarding the relationship between IBD and breast cancer was observed, such as in Hovde et al.4 Riegle et al5 and Pellino et al.6 While these studies provided insightful data, they were limited by confounding factors like disease progression and treatment biases. In contrast, our MR approach minimizes such biases by using genetic data as natural randomization, providing stronger evidence of causality between IBD and breast cancer. However, a meta-analysis by Gong’s et al7 found no significant effect, highlighting ongoing debate. We used MR to clarify this relationship, as it reduces confounding and allows more accurate causal assessment.
Shared susceptibility genes may link IBD and breast cancer.21 We validated these genes using GEO data and found consistent THBS3 overexpression in both IBD and breast cancer. TCGA analysis showed THBS3 overexpression in 16 cancers, including breast cancer. IHC and RT-PCR confirmed this in breast cancer tissues. Thus, THBS3 is integral to both diseases. As an extracellular matrix protein, THBS3 acts as an adhesion molecule involved in tissue remodeling, angiogenesis, and tumorigenesis,9,10,12 and is associated with poor prognosis.11–13
The pathophysiological mechanisms linking IBD and breast cancer remain unclear but may involve inflammatory mediators,22 immune abnormalities,23 genetic factors, and intestinal flora.24,25 Gut flora and immune dysregulation may be key, as both diseases are linked to chronic inflammation and immune dysfunction. Studies show that germ-free conditions prevent intestinal inflammation in susceptible mice, and IBD is most prevalent in areas with high bacterial abundance.26 The intestinal microbiota can significantly influence tumor initiation and progression by modulating cancer cell metabolism, altering the microenvironment, and inducing genetic toxicity. It is essential in the progression and management of multiple cancers, such as gastrointestinal tumors, lung cancer, and hematological malignancies. Additionally, it is important in the context of breast cancer.24,25,27
Immune dysregulation is recognized as a significant contributor to the onset and progression of breast cancer, and individuals with IBD frequently exhibit abnormalities in their immune systems.23,28 Studies found that the immune system of IBD patients may be in a hyperactive state, leading to excessive inflammatory responses.29,30 Abnormal activation of the immune system may also increase the risk of breast cancer. We found THBS3 significantly associated with CD4⁺ T cells in both diseases, which are known to be involved.31,32 Thus, immune regulation may be a key factor in IBD-related breast cancer risk.
LncRNAs and miRNAs play key regulatory roles in gene expression at both transcriptional and post-transcriptional levels. Studies indicate that they influence the development of IBD and breast cancer by modulating tumor growth, invasion, and metastasis, making miRNAs potential diagnostic biomarkers. For instance, miR-149-3p promotes IBD progression and affects tumor development.33 Using multiple databases, we predicted THBS3-associated miRNAs and lncRNAs and constructed a ceRNA network, which revealed interactions between THBS3 and several miRNAs, including hsa-miR-423-5p—known to impair intestinal barrier function by targeting claudin-5 and aggravating IBD.34 Additionally, Lnc00707 competitively binds miR-423-5p, upregulating MARCH2 and promoting triple-negative breast cancer via the PI3K/AKT/mTOR pathway.35 In our network, lncRNA SNHG14 interacted with hsa-miR-185-3p; SNHG14 promotes breast cancer progression and chemoresistance,36,37 though its role in IBD is unknown.
Surgery and chemotherapy are mainstays for breast cancer, with drug resistance being a critical issue. Identifying predictive markers can improve outcomes and reduce burden. Although THBS3 has not been previously linked to drug sensitivity, its family member THBS1 is associated with immunity and chemoresistance in gastric cancer.38 We analyzed the GDSC database and found THBS3 associated with sensitivity to Dinaciclib, Rapamycin, and Daporinad. Molecular docking and dynamics simulations showed strong THBS3-Rapamycin binding, suggesting THBS3 as a potential chemotherapy response indicator.
Further analysis of the potential mechanisms of THBS3 in IBD and breast cancer using GSEA and GSVA revealed that the Focal Adhesion and ECM Receptor Interaction pathways were associated with both IBD and breast cancer in the GSEA analysis. The GSVA analysis revealed a notable association between the Proteasome pathway and both IBD and breast cancer. Previous studies have shown that THBS3 is highly expressed in gastric cancer (GC) and colorectal cancer (CRC), binds to integrins (such as ITGA3/ITGB1, ITGA5), promotes cell-matrix adhesion, and affects tumor migration and invasion.20,39 In the research of renal cell carcinoma, THBS3 was incorporated into the core prognostic marker network of the ECM-receptor interaction pathway (KEGG hsa04512), and its expression was co-expressed with ECM genes such as COL1A2 and FN1, and it indirectly regulated ITGA5 through miR-32-5p.39 In addition, adjacent genes of THBS3 (such as A2M and ADAMTS families) are significantly enriched in the proteasome degradation pathway (GO:0006511), indicating that THBS3 may affect proteasome activity by regulating ECM degrading enzymes.13 It is suggested that TBHS3 may maintain the dynamic balance of the tumor microenvironment by regulating the degradation and renewal of ECM-related proteins. These functions reflect the specific regulatory role of THBS3 in the ECM-receptor interaction and proteasome pathway.40,41
THBS3-targeted therapeutic strategies could involve small-molecule inhibitors or RNA interference approaches. Small-molecule inhibitors could block the pro-inflammatory and pro-angiogenic activities of THBS3, which are crucial for tumor progression and immune evasion. RNA interference strategies, such as siRNAs or miRNAs targeting THBS3, might downregulate its expression in patients at high risk for breast cancer. However, challenges exist, including the potential for off-target effects in normal tissues. Careful design of delivery mechanisms, such as nanoparticle-based systems, will be crucial to minimize systemic toxicity and achieve targeted tissue modulation without harming healthy cells.
Conclusion
Our study confirms IBD as a breast cancer risk factor, potentially linked to THBS3 expression and immune abnormalities. However, the exact mechanisms remain unclear, requiring further research to develop better screening and prevention strategies for IBD patients. Our research has several advantages, including the first use of MR to analyze the impact of IBD on breast cancer and an in-depth analysis of the underlying mechanisms. However, it also has limitations. The research population is entirely of European descent, which may introduce bias and limit promotion. Furthermore, our immunohistochemical and RT-PCR analyses were based on a small sample of breast cancer tissue. MR Also cannot explain the interaction between genes and the environment, such as diet or lifestyle, which may affect the relationship between ibd and breast cancer. Future research should address these factors and expand the research population. Furthermore, this study did not distinguish the subtypes of breast cancer; Further research is needed to verify the role of THBS3 in specific subtypes.
Data Sharing Statement
The data supporting the results in the manuscript can be obtained from the corresponding author based on reasonable request.
Ethics Approval and Consent to Participate
All procedures performed in this study were in accordance with the ethical standards of the Helsinki Declaration. The approved number by the Institutional Review Board at Shengli Oilfield Central Hospital is YXLL202406301. Informed consent was obtained from all participants.
Acknowledgment
Thanks to GWAS, TCGA, GEO, Sangerbox, and Shengxin self-study network for providing open data and analysis platform.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Bruner LP, White AM, Proksell S. Inflammatory bowel disease. Prim Care. 2023;50(3):411–427. doi:10.1016/j.pop.2023.03.009
2. Flynn S, Eisenstein S. Inflammatory bowel disease presentation and diagnosis. Surg Clin North Am. 2019;99(6):1051–1062. doi:10.1016/j.suc.2019.08.001
3. Wilkinson L, Gathani T. Understanding breast cancer as a global health concern. Br J Radiol. 2022;95(1130):20211033. doi:10.1259/bjr.20211033
4. Hovde Ø, Høivik ML, Henriksen M, Solberg IC, Småstuen MC, Moum BA. Malignancies in patients with inflammatory bowel disease: results from 20 years of follow-up in the IBSEN study. J Crohns Colitis. 2017;11(5):571–577. doi:10.1093/ecco-jcc/jjw193
5. Riegler G, Caserta L, Castiglione F, et al. Increased risk of breast cancer in first-degree relatives of Crohn’s disease patients. An IG-IBD study. Dig Liver Dis. 2006;38(1):18–23. doi:10.1016/j.dld.2005.07.006
6. Pellino G, Sciaudone G, Patturelli M, et al. Relatives of Crohn’s disease patients and breast cancer: an overlooked condition. Int J Surg. 2014;12 Suppl 1:S156-158. doi:10.1016/j.ijsu.2014.05.022
7. Gong C, Xu R, Zou P, Zhang Y, Wang X. Inflammatory bowel disease and risk of breast cancer: a meta-analysis of cohort studies. Eur J Cancer Prev. 2022;31(1):54–63. doi:10.1097/cej.0000000000000667
8. Luo J, Xu Z, Noordam R, van Heemst D, Li-Gao R. Depression and inflammatory bowel disease: a bidirectional two-sample mendelian randomization study. J Crohns Colitis. 2022;16(4):633–642. doi:10.1093/ecco-jcc/jjab191
9. Vos HL, Devarayalu S, de Vries Y, Bornstein P. Thrombospondin 3 (Thbs3), a new member of the thrombospondin gene family. J Biol Chem. 1992;267(17):12192–12196. doi:10.1016/S0021-9258(19)49823-2
10. Liu X, Xu D, Liu Z, et al. THBS1 facilitates colorectal liver metastasis through enhancing epithelial-mesenchymal transition. Clin Transl Oncol. 2020;22(10):1730–1740. doi:10.1007/s12094-020-02308-8
11. Wang G, Qu F, Zhou J, Zhu B, Gao Y. Elevated THBS3 predicts poor overall survival for clear cell renal cell carcinoma and identifies LncRNA/RBP/THBS3 mRNA networks. Cell Cycle. 2023;22(3):316–330. doi:10.1080/15384101.2022.2117910
12. Dalla-Torre CA, Yoshimoto M, Lee CH, et al. Effects of THBS3, SPARC and SPP1 expression on biological behavior and survival in patients with osteosarcoma. BMC Cancer. 2006;6(1):237. doi:10.1186/1471-2407-6-237
13. Chen X, Lin J, Chen M, Chen Q, Cai Z, Tang A. Identification of adhesion-associated extracellular matrix component thrombospondin 3 as a prognostic signature for clear cell renal cell carcinoma. Investig Clin Urol. 2022;63(1):107–117. doi:10.4111/icu.20210273
14. Tomczak K, Czerwińska P, Wiznerowicz M. The cancer genome atlas (TCGA): an immeasurable source of knowledge. Contemp Oncol. 2015;19(1A):A68–77. doi:10.5114/wo.2014.47136
15. Barrett T, Wilhite SE, Ledoux P, et al. NCBI GEO: archive for functional genomics data sets--update. Nucleic Acids Res. 2013;41(D1):D991–995. doi:10.1093/nar/gks1193
16. Zhang Y, Xu J, Qiu Z, et al. STK25 enhances hepatocellular carcinoma progression through the STRN/AMPK/ACC1 pathway. Cancer Cell Int. 2022;22(1):4. doi:10.1186/s12935-021-02421-w
17. Chen Y, Meng H, Meng X, Yan Z, Wang J, Meng F. Correlation between low THBS3 expression in peripheral blood and acute myocardial infarction. Front Biosci. 2022;27(10):291. doi:10.31083/j.fbl2710291
18. Yang W, Soares J, Greninger P, et al. Genomics of drug sensitivity in cancer (GDSC): a resource for therapeutic biomarker discovery in cancer cells. Nucleic Acids Res. 2013;41(D1):D955–961. doi:10.1093/nar/gks1111
19. Hänzelmann S, Castelo R, Guinney J. GSVA: gene set variation analysis for microarray and RNA-seq data. BMC Bioinf. 2013;14(1):7. doi:10.1186/1471-2105-14-7
20. Deng LY, Zeng XF, Tang D, Deng W, Liu HF, Xie YK. Expression and prognostic significance of thrombospondin gene family in gastric cancer. J Gastrointest Oncol. 2021;12(2):355–364. doi:10.21037/jgo-21-54
21. Zhou S, Yu J. Crohn’s disease and breast cancer: a literature review of the mechanisms and treatment. Intern Emerg Med. 2023;18(5):1303–1316. doi:10.1007/s11739-023-03281-0
22. Pierce BL, Ballard-Barbash R, Bernstein L, et al. Elevated biomarkers of inflammation are associated with reduced survival among breast cancer patients. J Clin Oncol. 2009;27(21):3437–3444. doi:10.1200/jco.2008.18.9068
23. Dieci MV, Miglietta F, Guarneri V. Immune infiltrates in breast cancer: recent updates and clinical implications. Cells. 2021;10(2):223. doi:10.3390/cells10020223
24. Kwa M, Plottel CS, Blaser MJ, Adams S. The intestinal microbiome and estrogen receptor-positive female breast cancer. J Natl Cancer Inst. 2016;108(8). doi:10.1093/jnci/djw029
25. Nishida A, Inoue R, Inatomi O, Bamba S, Naito Y, Andoh A. Gut microbiota in the pathogenesis of inflammatory bowel disease. Clin J Gastroenterol. 2018;11(1):1–10. doi:10.1007/s12328-017-0813-5
26. Qiu P, Ishimoto T, Fu L, Zhang J, Zhang Z, Liu Y. The gut microbiota in inflammatory bowel disease. Front Cell Infect Microbiol. 2022;12:733992. doi:10.3389/fcimb.2022.733992
27. Zhao Y, Liu Y, Li S, et al. Role of lung and gut microbiota on lung cancer pathogenesis. J Cancer Res Clin Oncol. 2021;147(8):2177–2186. doi:10.1007/s00432-021-03644-0
28. Santa-Maria CA, Park SJ, Jain S, Gradishar WJ. Breast cancer and immunology: biomarker and therapeutic developments. Expert Rev Anticancer Ther. 2015;15(10):1215–1222. doi:10.1586/14737140.2015.1086270
29. Zhang YZ, Li YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. 2014;20(1):91–99. doi:10.3748/wjg.v20.i1.91
30. Chen Y, Cui W, Li X, Yang H. Interaction between commensal bacteria, immune response and the intestinal barrier in inflammatory bowel disease. Front Immunol. 2021;12:761981. doi:10.3389/fimmu.2021.761981
31. Zhang H, Qin G, Yu H, Han X, Zhu S. Comprehensive genomic and immunophenotypic analysis of CD4 T cell infiltrating human triple-negative breast cancer. Cancer Immunol Immunother. 2021;70(6):1649–1665. doi:10.1007/s00262-020-02807-1
32. Gomez-Bris R, Saez A, Herrero-Fernandez B, Rius C, Sanchez-Martinez H, Gonzalez-Granado JM. CD4 T-Cell Subsets and the Pathophysiology of Inflammatory Bowel Disease. Int J Mol Sci. 2023;24. doi:10.3390/ijms24032696
33. Cao Y, Wang Z, Yan Y, et al. Enterotoxigenic bacteroidesfragilis promotes intestinal inflammation and malignancy by inhibiting exosome-packaged miR-149-3p. Gastroenterology. 2021;161(5):1552–1566.e1512. doi:10.1053/j.gastro.2021.08.003
34. Wang M, Guo J, Zhao YQ, Wang JP. IL-21 mediates microRNA-423-5p /claudin-5 signal pathway and intestinal barrier function in inflammatory bowel disease. Aging. 2020;12(16):16099–16110. doi:10.18632/aging.103566
35. Li H, Liu Q, Hu Y, Yin C, Zhang Y, Gao P. Linc00707 regulates autophagy and promotes the progression of triple negative breast cancer by activation of PI3K/AKT/mTOR pathway. Cell Death Discov. 2024;10(1):138. doi:10.1038/s41420-024-01906-7
36. Wang B, Xing AY, Li GX, Liu L, Xing C. SNHG14 promotes triple-negative breast cancer cell proliferation, invasion, and chemoresistance by regulating the ERK/MAPK signaling pathway. IUBMB Life. 2024;76(12):1295–1308. doi:10.1002/iub.2910
37. Zhang D, Ding X, Peng M. LncRNA SNHG14 accelerates breast cancer progression through sponging miR-543 and regulating KLF7 expression. Arch Gynecol Obstet. 2022;305(6):1507–1516. doi:10.1007/s00404-021-06300-7
38. Zhang X, Huang T, Li Y, Qiu H. Upregulation of THBS1 is related to immunity and chemotherapy resistance in gastric cancer. Int J Gen Med. 2021;14:4945–4957. doi:10.2147/ijgm.S329208
39. Nersisyan S, Novosad V, Engibaryan N, Ushkaryov Y, Nikulin S, Tonevitsky A. ECM-receptor regulatory network and its prognostic role in colorectal cancer. Front Genet. 2021;12:782699. doi:10.3389/fgene.2021.782699
40. Catalgol B. Proteasome and cancer. Prog Mol Biol Transl Sci. 2012;109:277–293. doi:10.1016/B978-0-12-397863-9.00008-0
41. Han D, Wang L, Jiang S, Yang Q. The ubiquitin-proteasome system in breast cancer. Trends Mol Med. 2023;29:599–621. doi:10.1016/j.molmed.2023.05.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Stem Cell Therapy in Inflammatory Bowel Disease: A Review of Achievements and Challenges

Tian CM, Zhang Y, Yang MF, Xu HM, Zhu MZ, Yao J, Wang LS, Liang YJ, Li DF
Journal of Inflammation Research 2023, 16:2089-2119
Published Date: 16 May 2023
A Multicentre Study of the Clinical and Epidemiological Profile of Inflammatory Bowel Disease in Northeast Brazil
Brito CAA, Celani LMS, Araújo MVTD, Lucena MT, Vasconcelos GBS, Lima GAS, Nóbrega FJF, Diniz GTN, Lucena-Silva N, Toneto GT, Falcão JVDC, Barbosa PM, Oliveira PRFD, Dantas LSX, Fernandes LKC, Araújo SAD, Martinelli VF
Clinical and Experimental Gastroenterology 2023, 16:87-99
Published Date: 21 June 2023
Cytomegalovirus Pneumonia in Inflammatory Bowel Disease: Literature Review and Clinical Recommendations
Ren K, Yong C, Wang Y, Wei H, Zhao K, He B, Cui M, Chen Y, Wang J
Infection and Drug Resistance 2023, 16:6195-6208
Published Date: 13 September 2023
Dissecting Innate and Adaptive Immunity in Inflammatory Bowel Disease: Immune Compartmentalization, Microbiota Crosstalk, and Emerging Therapies

Yue N, Hu P, Tian C, Kong C, Zhao H, Zhang Y, Yao J, Wei Y, Li D, Wang L
Journal of Inflammation Research 2024, 17:9987-10014
Published Date: 29 November 2024
Challenges in the Management of Inflammatory Bowel Disease in Children: A Narrative Review
Hathagoda W, Rajindrajith S, Niriella MA
Clinical and Experimental Gastroenterology 2025, 18:259-275
Published Date: 1 November 2025