")
Back to Journals » Infection and Drug Resistance » Volume 16
Cytomegalovirus Pneumonia in Inflammatory Bowel Disease: Literature Review and Clinical Recommendations
Authors Ren K, Yong C, Wang Y, Wei H, Zhao K, He B, Cui M, Chen Y, Wang J
Received 7 May 2023
Accepted for publication 22 August 2023
Published 13 September 2023 Volume 2023:16 Pages 6195—6208
DOI https://doi.org/10.2147/IDR.S420244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Keyu Ren,1 Chunming Yong,2 Yanting Wang,1 Hongyun Wei,1 Kun Zhao,1 Baoguo He,1 Mingjuan Cui,1 Yunqing Chen,3 Jin Wang4
1Department of Gastroenterology, Affiliated Hospital of Qingdao University, Qingdao, Shandong, 266000, People’s Republic of China; 2Department of Emergency, Affiliated Hospital of Qingdao University, Qingdao, Shandong, 266000, People’s Republic of China; 3Department of Pathology, Affiliated Hospital of Qingdao University, Qingdao, Shandong, 266000, People’s Republic of China; 4Department of Pathology, School of Basic Medicine, Qingdao University, Qingdao, Shandong, 266000, People’s Republic of China
Correspondence: Jin Wang, Department of Pathology, School of Basic Medicine, Qingdao University, No. 308, Ningxia Road, Qingdao, Shandong, 266000, People’s Republic of China, Email [email protected]
Aim: The objective was to elucidate the correlation between CMVP and immunosuppressive therapy in IBD patients, we hope this review could expand on the significance of CMV as an opportunistic pathogen and the potential impact on morbidity and mortality in IBD patients.
Methods: Records and clinical trajectories linked to CMVP in IBD patients were extracted from the PubMed database, irrespective of language barriers. The reference lists incorporated in these studies were manually inspected. Conclusions were generated using straightforward descriptive analysis.
Results: In total, 18 IBD patients, including Crohn’s disease (CD, 67%) and Ulcerative Colitis (UC, 33%), affected by CMVP were identified from 17 published articles. A minority of these patients (17%) exhibited active disease, whereas the majority (83%) presented with quiescent disease. Fever (100%) and dyspnea (44%) emerged as the most prevalent clinical symptoms. All the patients had undergone immunosuppressive therapy. A significant proportion, up to 89%, had received thiopurine treatment prior to the CMVP diagnosis. Interestingly, none of the patients were subjected to biological therapy. Half of the patients manifested with Hemophagocytic Lymphohistiocytosis (HLH). Almost all patients (94%) were administered antiviral treatment and a substantial 83% experienced full recovery. Immunosuppressive agents were either tapered or discontinued altogether. A subset of patients, 17%, suffered fatal outcomes.
Conclusion: Our findings underscore the need for heightened suspicion of CMVP in IBD patients who exhibit symptoms such as fever and dyspnea. During the COVID-19 pandemic, CMVP should be considered a potential differential diagnosis. It was observed that CMVP primarily transpires during CD remission. Azathioprine emerged as the predominant immunosuppressant linked to CMV reactivation. The prompt application of effective antiviral therapy can substantially enhance patient outcomes. CMV vaccine might serve as a viable prevention strategy.
Keywords: CMV, cytomegalovirus pneumonia, inflammatory bowel disease, ulcerative colitis, Crohn’s disease
Introduction
Cytomegalovirus (CMV) is a double-stranded DNA virus, part of the Herpesviridae family, and commonly infects humans. This virus can establish a lifelong latent state in healthy individuals, with potential for reactivation leading to either subclinical or clinical infection. While CMV infection often presents as asymptomatic in immunocompetent individuals, it can lead to severe clinical complications in those who are immunocompromised. This is particularly observed in individuals receiving steroids or immunosuppressive therapy, as these treatments can facilitate CMV reactivation.1,2
The gastrointestinal tract is a frequently involved system in Cytomegalovirus (CMV) infections. It has been noted that patients diagnosed with Inflammatory Bowel Disease (IBD) exhibit a heightened risk ratio for CMV reactivation. Roughly 34.5% of patients diagnosed with IBD exhibit CMV colitis as confirmed by quantitative real-time PCR.3 CMV infection is also a potential contributor to instances of therapy-resistant IBD.4 According to recent guidelines published by the European Crohn’s and Colitis Organisation (ECCO),5 CMV colitis is linked to a higher risk of surgical intervention and mortality among patients with active IBD. Implementing effective antiviral therapy can significantly improve patient outcomes. Multiple risk factors are widely recognized for this increase, including extensive usage of immunosuppressants6,7 and impaired T-cell immunity. T-cell responses are critical in controlling CMV,8 and the activation of CMV-specific T-cells may lead to unchecked viral replication.9 Furthermore, the propensity of CMV to target sites of inflammation is another significant factor.10 CMV reactivation is often induced and sustained by inflamed mucosa.
The lungs are among the most frequently involved organs in CMV infections.11 CMV may initially seed in the oropharyngeal cavity before infecting the lungs. Its primary mode of spread is via cell-to-cell infection through innate immune cells, which aids in establishing latency within the host.12 Beyond inhalation of infectious body fluids, systemic CMV infection can also lead to pneumonia in the lungs.13 The lungs and the gastrointestinal tract share the same embryological origin, tracing back to the ancestral intestine.14 The similarities in immune systems between the lungs and intestines might facilitate pulmonary involvement.15 Current evidence suggests that the prevalence of CMV pneumonia (CMVP) in immunocompromised hosts can reach up to 60%, which could be attributed to severe immunosuppression.16 Indeed, symptomatic CMVP infections are more commonly identified in immunocompromised patients.17
Over the past decade, there has been a surfeit of therapeutic advancements in the treatment of IBD. These developments have revolutionized IBD management, enabling the induction of intestinal mucosal healing and potentially altering disease progression. Despite the high mortality associated with CMVP in patients with IBD, there is scant information about the manifestation of CMVP in IBD patients who are subjected to immunosuppressive therapy.18,19 The optimal treatment strategy has yet to be definitively determined, indicating a clear need for additional data and research to address this knowledge gap.
The primary objective of this study is to scrutinize the existing literature, aiming to delineate the clinical characteristics, diagnostic procedures, and treatment approaches pertinent to CMV infections among IBD patients. Through this comprehensive review, we anticipate extending our understanding of the implications of CMV as an opportunistic pathogen, as well as providing pragmatic clinical recommendations for the prevention and management of CMV infections in patients with IBD.
Methods
This study adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines.20 A comprehensive search of the PubMed database was performed, collecting pertinent literature up to September 2022. The search terms utilized included “Cytomegalovirus” or “CMV” and “inflammatory bowel disease” or “Crohn’s disease” or “ulcerative colitis” or “IBD”.
First, titles and abstracts were screened to identify potentially relevant papers. Studies not meeting inclusion criteria were excluded. Second, we read them in their entirety to assess their appropriateness for inclusion. Articles selected for inclusion met specific criteria, namely, they provided detailed information on IBD patients with CMVP. In addition, the references cited in these articles were reviewed to discover potentially relevant studies. The retrieved studies were manually scrutinized to assess their suitability for inclusion. Conversely, non-relevant articles were excluded based on the following criteria: (1) cases with underlying congenital CMV infections, (2) IBD patients without CMVP, (3) patients with CMVP but not arising from IBD, and (4) those with unavailable or incomplete data.
CMVP was diagnosed according to specific criteria: (1) Symptoms including, but not limited to, dyspnea, fever, cough, and hypoxia; (2) Radiological or post-mortem findings of pneumonia; (3) The presence of pp65 antigenemia and/or CMV DNA in the blood and/or respiratory samples, as well as anti-CMV antibodies of IgM and IgG titers; (4) CMV inclusion bodies found in lung specimen histopathology; (5) Positive CMV cultures in lung and/or respiratory samples; and (6) Positive CMV in situ hybridization on lung specimens.21,22
Statistical analysis was performed with data summarized using descriptive statistics, including frequency and means. Calculations were conducted using Microsoft Excel.
Results
The initial literature search yielded a total of 810 articles. We screened these preliminary results for relevance based on two key criteria: topical relevance and descriptions of patient cases. This step resulted in 32 pertinent articles. Furthermore, in all the remaining articles, CMVP was confirmed based on predefined criteria. Ultimately, 17 articles comprising 18 case reports met the predetermined inclusion criteria. The process of literature search and evaluation is illustrated in Figure 1. All extracted clinical data are presented in Table 1.
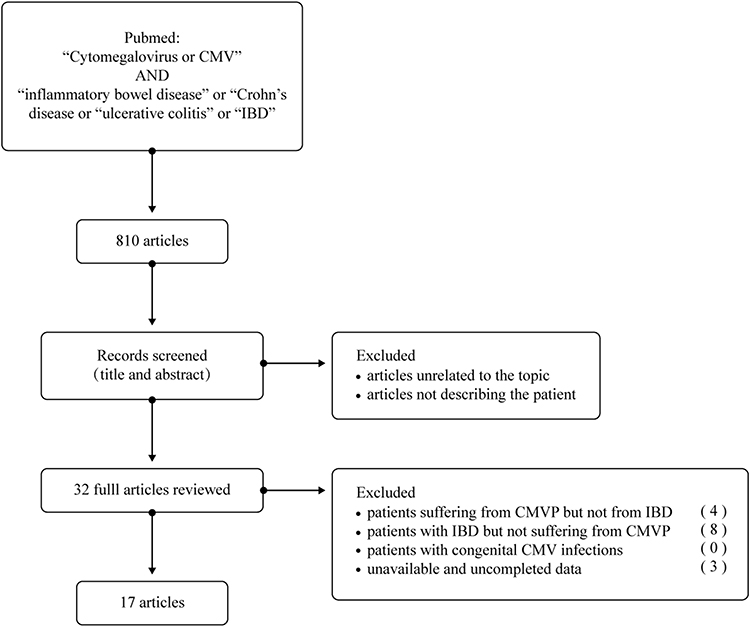 |
Figure 1 Flow chart of the literature search. The search led to 17 articles describing patient cases of CMVP. In total, 18 patient cases were included from literature. |
 |
Table 1 Main Characteristics, Therapy, and Outcome of IBD Patients with CMV Pneumonia |
The patient cohort predominantly comprised females (72%) with a median age of 37 years (range: 18–77 years). Among the patients, 67% had Crohn’s Disease (CD), and 33% suffered from Ulcerative Colitis (UC). Notably, 17% (UC=2, CD=1) of the patients had active disease, while 83% (UC=4, CD=11) presented with quiescent disease. Among the three patients with confirmed active IBD, characteristic cytomegalic cells were identified in the colonic autopsy specimens of a UC patient. All patients had received immunosuppressants such as prednisone (22%), 6-mercaptopurine (6-MP) (11%), azathioprine (AZA) (78%), and/or cyclosporine A (CSA) (11%) prior to the CMV onset. Notably, 89% of patients were administered thiopurines in combination with either glucocorticoids (n=2) or 5-aminosalicylates (n=6), with no patients receiving biologics.
The most frequently reported symptoms were fever (100%), varied degrees of dyspnea (44%), and cough (33%). Additional non-specific symptoms included breathlessness (11%) and pharyngeal discomfort (17%), while approximately one-fourth of the patients (23%) experienced no respiratory symptoms.
Serological tests were predominantly employed for diagnosing CMV infection, with 94% of the patients being CMV seropositive. The Bronchoalveolar lavage fluid (BALF)CMV DNA and blood CMV DNA were positive in 34% and 50% of the patients, respectively. BALF CMV DNA test serves as a valuable complement to CMV serological diagnosis, substantially enhancing diagnostic accuracy. Radiographic findings indicated pulmonary lesions manifesting as bilateral interstitial infiltrates (78%), ground-glass opacity (17%), and consolidation (17%). As for the treatment regimen, ganciclovir was administered to nearly all patients (94%) immediately after the diagnosis of CMVP, only one patient recovered in the absence of antiviral treatment. The average course of antiviral therapy was 22 days (5–42 days). Concurrent immunosuppressive therapy (100%) was either tapered (glucocorticoid) or discontinued (AZA,6-MP, or CsA). Notably, half of the patients (50%) developed complications from Hemophagocytic Lymphohistiocytosis (HLH). Regrettably, the mortality rate was 17%, with three patients succumbing to organ failure.
Discussion
Patients with Inflammatory Bowel Disease (IBD) present an increased susceptibility to Cytomegalovirus (CMV) infection, with 45 to 100% of IBD patients harboring latent CMV infections.40 It is widely acknowledged that immunologic dysregulation plays a significant role in the pathogenesis of IBD,41 thus predisposing these patients to opportunistic infections such as CMV, either via primary infection or reactivation of latent virus under immunocompromised states.
Despite the heterogeneous immunotypes associated with different IBD subtypes, it remains uncertain whether these variations influence the incidence of CMV Pneumonia (CMVP). The present study indicates that Crohn’s Disease (CD) is the subtype most frequently associated with CMVP, aligning with a prior systematic review.18 This review involved 13 IBD patients, out of which 10 were diagnosed with CD concurrent with CMVP. This trend may be attributed to the increased odds of CD patients to immunosuppressive therapy. Existing epidemiological data reveal that approximately 76.6% of Ulcerative Colitis (UC) patients experience a mild to moderate disease course.42 As such, 5-aminosalicylic acid (5-ASA) serves as the first-line treatment for this patient group, exerting no significant impact on immunity.43 Meta-analyses have corroborated the safety and efficacy of 5-ASA in mitigating the risk of CMV reactivation,44 which may explain the lower incidence of CMVP among UC patients.
Nevertheless, contradictory evidence exists in the literature. For instance, Romkens et al suggested that UC patients might exhibit a higher susceptibility to CMV-associated infections and intestinal diseases than those with CD.19 CMV reactivation in these patients is often facilitated by compromised intestinal immune barriers and immunosuppression.45 From an immunological perspective, UC is associated with increased production of pro-inflammatory cytokines in response to gut microbes.46 It is well-documented that CMV activation occurs in monocytes and dendritic cells under the influence of TNF and IFN.47 Consequently, interactions between CMV and inflammation exacerbate intestinal damage.48 These observations necessitate further research to elucidate the underlying mechanisms.
The prevailing evidence suggests that CMVP predominantly transpires during the remission phase in IBD patients, an observation that aligns with prior studies.18,49 Interestingly, intestinal inflammation does not appear to be related to the risk of CMVP onset. Notably, a significantly elevated incidence of CMVP was identified in patients with inactive IBD who were under thiopurine monotherapy, suggesting that advanced immunosuppression is a primary driver of increased CMVP incidence.50
Clinically, CMVP primarily affects the lung interstitium. Radiological signs of CMVP can often be atypical, encompassing a spectrum from diffuse interstitial infiltrates and ground-glass opacities to small nodules or a crazy-paving pattern on computed tomography.51,52 Pulmonary pathology in IBD patients lacks consensus and has been ascribed to drug toxicity, immune-related causes, or an obscure inflammatory association with gut disease. Nevertheless, it is crucial to bear in mind that authentic IBD-associated interstitial lung disease is infrequent. The history of drug usage should always be scrutinized in the management of IBD patients presenting with interstitial lung disease characteristics.53 Certain medications, including sulfasalazine,54 mesalamine,54 thiopurines,55 methotrexate,56 as well as the biologic,57,58 can induce lung injury if utilized for IBD treatment. Differentiating between lung disease stemming from IBD and that caused by medications remains a formidable challenge. Despite the difficulties in procuring pathological evidence of CMVP, a diagnosis typically necessitates the combination of positive CMV serostatus and viral DNA in blood and/or bronchoalveolar lavage samples. Lung biopsy may facilitate the direct detection of CMV infection via immunohistopathology.
CMVP symptoms can range from being asymptomatic to nonspecific, including manifestations such as dry cough, breathlessness, exertional dyspnea, and fevers.59 Respiratory symptoms are typically insidious and progressive.54 In the current study, prolonged fever emerged as the most prominent symptom. Intriguingly, in some instances, patients displayed no cough or respiratory symptoms, while bilateral basilar patchy/interstitial infiltrates predominantly appeared on chest radiographs. The presenting signs and symptoms of CMVP are usually nonspecific, often leading to delayed diagnosis due to their uncharacteristic nature. From our perspective, we assert that CMVP should be contemplated in the differential diagnosis for immunosuppressed patients presenting with fever and dyspnea. Further, more diagnostic modalities such as high-resolution lung CT and fiberoptic bronchoscopy should be deployed. Importantly, in the context of the ongoing COVID-19 pandemic, COVID-19 should be incorporated into the differential diagnosis as its clinical symptoms and imaging findings bear similarity to those of CMVP.60
Immunosuppression induced by medications paves the way for viral reactivation. Pharmaceuticals frequently employed in managing IBD, such as biological agents, glucocorticoids, and azathioprine, have been shown to maintain the body in a state of immune inhibition.5 CMV disease can manifest when host immunity is compromised. It is widely accepted that recent exposure to corticosteroids or thiopurines, but not anti-TNF agents, constitutes a significant risk factor.61 The protracted use of high-dose corticosteroid therapy elevates the risk of CMVP.62 Studies have reported that steroids can stimulate the transcription of immediate-early (IE) genes while downregulating the activity of lymphocytes and monocytes, in parallel with CMV reactivation implicated in steroid resistance.63 The potential mechanism encompasses a marked increase in pro-inflammatory cytokines and altered glucocorticoid receptor expression, which may exacerbate ulcerative colitis (UC). In contrast, combination therapies for IBD have been associated with a higher risk of severe infection, especially when corticosteroids are used in conjunction with TNF antagonists.64 A greater prednisolone dosage (>32 mg/d) used in combination with immunosuppressants can potentially shorten the duration of CMV reactivation and serve as a predictor of CMVP.65
In this study, we discerned a strong correlation between thiopurines and CMV infection. The most frequently observed adverse effects of AZA/6-MP are opportunistic infections.66 Although reports of CMV reactivation exist, a definitive causal relationship remains unestablished. Prior literature suggests that thiopurines augment the risk of viral infections67 and severe systemic CMV infection when on immunosuppressive medication,68 a scenario potentially attributable to thiopurine-induced lymphopenia.69 Thiopurines may induce apoptosis of activated T-cells70 and mitigate the T-cell response to infectious agents. For patients receiving thiopurine therapy, viral infections like cytomegalovirus, Epstein-Barr (EB) virus, and herpes simplex virus pose a significant concern.71 A systematic review reported a worse prognosis in CMVP patients with IBD;18 even a minimal dose of azathioprine could induce significant CMVP by facilitating sufficient immunosuppression, a phenomenon attributed to slow drug metabolism.38 Consequently, in clinical practice, screening for thiopurine methyltransferase (TPMT) and Nudix hydrolase (NUDT15) genetic polymorphisms prior to initiating azathioprine can enhance patient therapeutic response while minimizing side effects.72 Miechowiecki et al73 described a case of acute CMV infection in a patient with Crohn’s disease (CD) in remission under azathioprine therapy who recovered following antiviral and symptomatic therapy. This finding indicates that IBD patients undergoing long-term thiopurine therapy may be more vulnerable to severe CMV disease.
Recent studies have illuminated a decline in CMV infections among IBD patients, indicative of a transition from conventional corticosteroid-based therapies to more effective agents with desirable safety profiles and minimal side effects.74 Biologic drugs have emerged as a prevalent and often essential therapeutic option in IBD management. Beyond TNF-α inhibitors, integrin receptor antagonists and IL-12 and IL-23 antagonists are comparably utilized.75 Our review of the literature yielded no instances of CMVP related to biologics. The association between TNF-α inhibitors and CMV infections has not been systematically explored. However, it is recognized that TNF-α plays a vital role in controlling viral infection, eliciting CMV from latency to active infection, with the risk of CMV disease correlating with TNF-a levels.76,77 Theoretically, TNF-blockade treatment could promote viral reactivation through TNF depletion.77 Nevertheless, numerous instances have demonstrated that CMV activation remains unaffected by anti-TNF therapy.78,79 Reports suggest that TNF-α inhibitors could mitigate CMV viral load via TNF-α reduction.80 TNF-α inhibitors might also be effective in treating the underlying disease activity that accompanies inflammation-induced CMV replication in colon tissue.81 Short-term infliximab treatment (<14w) exerts minimal influence on the risk of latent CMV reactivation.82 Therefore, TNF-α inhibitors like infliximab and adalimumab may be suitable for severe ulcerative colitis in the context of CMV infection.44 Likewise, anti-TNF monotherapy has been linked with a lower risk of opportunistic viral infections compared to thiopurine monotherapy.67
Anti-integrin monoclonal antibodies, such as vedolizumab, are acknowledged to be efficacious in the treatment of IBD. Despite respiratory tract infections being the most common adverse events (AEs), there is no definitive evidence linking them to vedolizumab.83,84 Generally, gut-selective mechanisms underpin its safety profile.85,86 Vedolizumab demonstrates commendable biosafety during IBD flare-ups associated with CMV infection.87,88 Hommel et al reported a patient with active UC and colonic CMV reactivation who, following treatment with ganciclovir and vedolizumab, achieved clinical remission and experienced a reduction in gut viral load.89 In vivo, vedolizumab inhibits the recruitment of CMV-infected monocytes to the mucosa and modulates leukocyte trafficking.90 Moreover, it can be safely administered to IBD patients with severe COVID-19 infections, further highlighting its robust safety.91 However, one single-center clinical study noted a heightened risk of CMV reactivation in CMV seropositive UC patients administered vedolizumab compared to those receiving TNF-α inhibitors, yet the observation remained unelucidated.92 Data on CMV infection and vedolizumab use are, to date, still scarce.
Ustekinumab, a fully human monoclonal antibody targeting interleukin-12/23p40, is deemed a cornerstone in inducing and maintaining remission in moderate to severe IBD patients. Long-term follow-up studies have corroborated the effectiveness and safety of ustekinumab in UC and CD patients.93,94 Adverse effects are well-tolerated with ustekinumab, and its profile mirrors that of the placebo. The most frequently encountered adverse reactions include nasopharyngitis and upper respiratory tract infections.94 Tuberculosis infections have not been reported. Discontinuation of ustekinumab in patients with pneumonia is not requisite.95 Ustekinumab appears to be safe in situations of induced or exacerbated infection. Recently, Despotes et al described a CD patient with interstitial lung disease secondary to ustekinumab.96 In this case, pneumonia was attributed to ustekinumab following the ruling out of infections. The patient’s lung function recovered post high-dose steroid treatment. In summary, the safety of newer non-TNF-α biologics warrants more comprehensive scrutiny.
Hemophagocytic lymphohistiocytosis (HLH) represents a multisystem inflammatory syndrome induced by secondary immune disorders. The most frequent cause of secondary HLH is infection, with CMV and EBV infections being considered the most common triggers for HLH.97 It has been documented that IBD is the most prevalent comorbidity (20 out of 35 cases) in CMV-associated HLH patients.98 In our study, HLH was persistently observed in approximately half of the patient population, corroborating the argument that immunosuppressive treatments and immune-related comorbidities significantly escalate the risk. The high incidence of HLH could potentially explain the unfavorable prognosis of CMVP in patients suffering from IBD. Following antiviral treatment, most patients experienced favorable outcomes, evidenced by high survival rates, underscoring the cruciality of early diagnosis and intervention. Interestingly, we acknowledge recent reports concerning HLH induced by COVID-19, where even a mild COVID-19 infection could hyperactivate the immune response and trigger HLH.99 In the era of COVID-19, HLH should be considered in patients presenting with signs of liver injury and high fever subsequent to COVID-19 infection.
The necessity of antiviral drugs for CMVP is a well-recognized concept, with first-line treatment typically involving the intravenous administration of ganciclovir or its prodrug, valganciclovir, for 2–3 weeks. Symptomatic disseminated viral infections, encompassing pneumonia, mandate antiviral therapy alongside the tapering of all immunosuppressants.81 Given the severe impact of immunosuppression on systemic immunity in IBD patients, cessation of immunosuppressives, particularly azathioprine, warrants strong consideration, especially in cases where intestinal symptoms are not pronounced. Although TNF-α inhibitors exhibit a sound biosafety profile, the management of novel biological agents such as Vedolizumab and Ustekinumab remains an area of uncertainty, calling for additional research. Therefore, expedited treatment with ganciclovir coupled with the discontinuation of immunosuppressive therapy may enhance IBD symptomatology and avert complications and mortality in the majority of patients.
CMV infection imposes a considerable disease burden on immunocompromised individuals. Given the deleterious side effects and potential resistance encountered with antiviral agents, the use of neutralizing antibodies emerges as an appealing strategy for conferring protection, and as potential therapeutics and prophylactics against CMV.100 There is a pressing need for an effective human CMV vaccine, which could substantially prevent CMV infection and associated diseases, thereby mitigating numerous severe and disabling consequences, particularly in newborns and immunocompromised individuals.101 As far back as the 1970s, efforts to develop HCMV vaccines commenced. Despite the absence of a licensed HCMV vaccine, trials persist.102 Multiple candidate vaccines, including live-attenuated vaccines, chimeric peptidic vaccines, and recombinant subunit vaccines, have demonstrated favorable biosafety profiles and promising clinical results in trials.103 Even though IBD patients have not been incorporated into clinical trials,104 novel vaccine technologies, analogous to those effective against COVID-19, may facilitate the creation of a therapeutic vaccine against CMV, leading to improvements in the health of immunocompromised patients, inclusive of those with IBD.
Conclusion
In conclusion, cytomegalovirus pneumonia (CMVP) poses a grave complication in immunocompromised IBD patients undergoing thiopurine treatment, associated with elevated morbidity and mortality rates. Diagnosing CMVP in clinical settings proves arduous due to its potential to manifest with nonspecific clinical and radiological features akin to those of drug-induced or COVID-19 pneumonia. Hence, CMV infection should be contemplated as a differential diagnosis in IBD patients who exhibit respiratory symptoms. Prompt diagnosis and assertive antiviral intervention ameliorate the prognosis. Nevertheless, our understanding of CMV infection in the context of novel biological agents remains sparse, necessitating additional data and research to bridge this knowledge gap. This underscores the need for future research and could offer valuable insights for subsequent studies.
Acknowledgments
The authors would like to thank Hao Yuan for his advice on the web interface.
Funding
This work was supported by the Intramural Research Program of the Affiliated Hospital of Qingdao University [grant number 4020] to Keyu Ren and the Shandong Province Natural Science Foundation [General Program, Grant No. ZR2022MH204] to Jin Wang.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Griffiths P, Reeves M. Pathogenesis of human cytomegalovirus in the immunocompromised host. Nat Rev Microbiol. 2021;19(12):759–773. doi:10.1038/s41579-021-00582-z
2. Ran Z, Wu K, Matsuoka K, et al. Asian Organization for Crohn’s and Colitis and Asia Pacific Association of gastroenterology practice recommendations for medical management and monitoring of inflammatory bowel disease in Asia. J Gastroenterol Hepatol. 2021;36(3):637–645. doi:10.1111/jgh.15185
3. Wang W, Chen X, Pan J, Zhang X, Zhang L. Epstein-Barr Virus and human cytomegalovirus infection in intestinal mucosa of Chinese patients with inflammatory bowel disease. Front Microbiol. 2022;13:915453. doi:10.3389/fmicb.2022.915453
4. Liu CC, Ji S, Ding Y, Zhou L, Liu X, Li W. Cytomegalovirus infection and steroid-refractory inflammatory bowel disease: possible relationship from an updated meta-analysis. Ir J Med Sci. 2018;187(4):935–942. doi:10.1007/s11845-018-1752-y
5. Kucharzik T, Ellul P, Greuter T, et al. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis. 2021;15(6):879–913. doi:10.1093/ecco-jcc/jjab052
6. Oh SJ, Lee CK, Kim YW, et al. True cytomegalovirus colitis is a poor prognostic indicator in patients with ulcerative colitis flares: the 10-year experience of an academic referral inflammatory bowel disease center. Scand J Gastroenterol. 2019;54(8):976–983. doi:10.1080/00365521.2019.1646798
7. Zabana Y, Rodriguez L, Lobaton T, et al. Relevant infections in inflammatory bowel disease, and their relationship with immunosuppressive therapy and their effects on disease mortality. J Crohns Colitis. 2019;13(7):828–837. doi:10.1093/ecco-jcc/jjz013
8. Zangger N, Oxenius A. T cell immunity to cytomegalovirus infection. Curr Opin Immunol. 2022;77:102185. doi:10.1016/j.coi.2022.102185
9. Nowacki TM, Bettenworth D, Ross M, Heidemann J, Lehmann PV, Lugering A. Cytomegalovirus (CMV)-specific perforin and granzyme B ELISPOT assays detect reactivation of CMV infection in inflammatory bowel disease. Cells. 2012;1(2):35–50. doi:10.3390/cells1020035
10. Vega R, Bertran X, Menacho M, et al. Cytomegalovirus infection in patients with inflammatory bowel disease. Am J Gastroenterol. 1999;94(4):1053–1056. doi:10.1111/j.1572-0241.1999.01013.x
11. Cunha BA. Cytomegalovirus pneumonia: community-acquired pneumonia in immunocompetent hosts. Infect Dis Clin North Am. 2010;24(1):147–158. doi:10.1016/j.idc.2009.10.008
12. Jackson JW, Sparer T. There is always another way! Cytomegalovirus’ multifaceted dissemination schemes. Viruses. 2018;10(7):383. doi:10.3390/v10070383
13. Salomon N, Perlman DC. Cytomegalovirus pneumonia. Semin Respir Infect. 1999;14(4):353–358.
14. MacDermott RP, Nash GS, Nahm MH. Immunology and immunopathology of the intestines: antibody secretion by human intestinal mononuclear cells from normal controls and inflammatory bowel disease patients. Immunol Invest. 1989;18(1–4):449–457. doi:10.3109/08820138909112255
15. Lu DG, Ji XQ, Liu X, Li HJ, Zhang CQ. Pulmonary manifestations of Crohn’s disease. World J Gastroenterol. 2014;20(1):133–141. doi:10.3748/wjg.v20.i1.133
16. Saksirisampant G, Kawamatawong T, Promsombat K, et al. A Prospective Study of plasma and bronchoalveolar lavage fluid CMV DNA load quantification for the diagnosis and outcome of CMV pneumonitis in immunocompromised hosts. J Clin Virol. 2022;155:105243. doi:10.1016/j.jcv.2022.105243
17. Kanika A, Soldera J. Pulmonary cytomegalovirus infection: a case report and systematic review. World J Meta-Anal. 2023;11(5):151–166. doi:10.13105/wjma.v11.i5.151
18. Cascio A, Iaria C, Ruggeri P, Fries W. Cytomegalovirus pneumonia in patients with inflammatory bowel disease: a systematic review. Int J Infect Dis. 2012;16(7):e474–e479. doi:10.1016/j.ijid.2012.03.008
19. Romkens TE, Bulte GJ, Nissen LH, Drenth JP. Cytomegalovirus in inflammatory bowel disease: a systematic review. World J Gastroenterol. 2016;22(3):1321–1330. doi:10.3748/wjg.v22.i3.1321
20. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
21. Dioverti MV, Razonable RR, Hayden RT, Wolk DM, Carroll KC, Tang Y-W. Cytomegalovirus. Microbiol Spectr. 2016;4(4). doi:10.1128/microbiolspec.DMIH2-0022-2015
22. Restrepo-Gualteros SM, Gutierrez MJ, Villamil-Osorio M, Arroyo MA, Nino G. Challenges and clinical implications of the diagnosis of cytomegalovirus lung infection in children. Curr Infect Dis Rep. 2019;21(7):24. doi:10.1007/s11908-019-0681-x
23. Sijpkens YW, Allaart CF, Thompson J, et al. Fever and progressive pancytopenia in a 20-year-old woman with Crohn’s disease. Ann Hematol. 1996;72(4):286–290. doi:10.1007/s002770050174
24. Papadakis KA, Tung JK, Binder SW, et al. Outcome of cytomegalovirus infections in patients with inflammatory bowel disease. Am J Gastroenterol. 2001;96(7):2137–2142. doi:10.1111/j.1572-0241.2001.03949.x
25. Hookey LC, Depew W, Boag A, Vanner S. 6-mercaptopurine and inflammatory bowel disease: hidden ground for the cytomegalovirus. Can J Gastroenterol. 2003;17(5):319–322. doi:10.1155/2003/824547
26. Sato S, Kobayashi H, Saito R, et al. A case of steroid-refractory ulcerative colitis complicated with cytomegalovirus pneumonia. Fukushima J Med Sci. 2007;53(1):27–32. doi:10.5387/fms.53.27
27. Piton G, DuPont-Gossart AC, Weber A, et al. Severe systemic cytomegalovirus infections in patients with steroid-refractory ulcerative colitis treated by an oral microemulsion form of cyclosporine: report of two cases. Gastroenterol Clin Biol. 2008;32(5 Pt 1):460–464. doi:10.1016/j.gcb.2007.10.010
28. de Boer NK, van Bodegraven AA, de Graaf P, van der Hulst RW, Zoetekouw L, van Kuilenburg AB. Paradoxical elevated thiopurine S-methyltransferase activity after pancytopenia during azathioprine therapy: potential influence of red blood cell age. Ther Drug Monit. 2008;30(3):390–393. doi:10.1097/FTD.0b013e31816c20b3
29. Wolschke C, Fiedler W, Habermann RC, Janka-Schaub GE, Kluge S. 28-year old female patient with respiratory insufficiency, elevated liver enzymes, pancytopenia and fever. Internist. 2010;51(11):1434–1438. doi:10.1007/s00108-010-2650-1
30. Presti MA, Costantino G, Della Torre A, Belvedere A, Cascio A, Fries W. Severe CMV-related pneumonia complicated by the hemophagocytic lymphohistiocytic (HLH) syndrome in quiescent Crohn’s colitis: harmful cure? Inflamm Bowel Dis. 2011;17(11):E145–E146. doi:10.1002/ibd.21828
31. van Langenberg DR, Morrison G, Foley A, Buttigieg RJ, Gibson PR. Cytomegalovirus disease, haemophagocytic syndrome, immunosuppression in patients with IBD: ‘a cocktail best avoided, not stirred’. J Crohns Colitis. 2011;5(5):469–472. doi:10.1016/j.crohns.2011.04.010
32. N’Guyen Y, Baumard S, Salmon JH, et al. Cytomegalovirus associated hemophagocytic lymphohistiocytosis in patients suffering from Crohn’s disease treated by azathioprine: a series of four cases. Inflamm Bowel Dis. 2011;17(9):E116–E118. doi:10.1002/ibd.21770
33. Abbey A, Elsmore AC. Shortness of breath in a patient with inflammatory bowel disease. BMJ Case Rep. 2014;2014(oct09 1):bcr2014205269. doi:10.1136/bcr-2014-205269
34. Stack R, Parihar V, Ryan B, Alakkari A. CMV pneumonitis in an immunosuppressed Crohn’s disease patient. QJM. 2016;109(8):553–554. doi:10.1093/qjmed/hcw082
35. Divithotawela C, Garrett P, Westall G, Bhaskar B, Tol M, Chambers DC. Successful treatment of cytomegalovirus associated hemophagocytic lymphohistiocytosis with the interleukin 1 inhibitor - anakinra. Respirol Case Rep. 2016;4(1):4–6. doi:10.1002/rcr2.137
36. Vakkalagadda CV, Cadena-Semanate R, Non LR. Cytomegalovirus-associated hemophagocytic syndrome in a 59-year-old woman with ulcerative colitis. Am J Med. 2017;130(7):e305–e306. doi:10.1016/j.amjmed.2017.02.018
37. Cockbain BC, Mora Peris B, Abbara A, So CW, Cooke G. Disseminated CMV infection and HLH in a patient with well-controlled HIV and ulcerative colitis. BMJ Case Rep. 2019;12(2):e227916. doi:10.1136/bcr-2018-227916
38. Hawthorne TZ, Shellien R, Chambers L, Devereux G. CMV pneumonitis in a patient with Crohn’s disease taking azathioprine. BMJ Case Rep. 2021;14(4):e241256. doi:10.1136/bcr-2020-241256
39. Voet M, Calon T, Hendriks M, Schreuder RM. Severe complication of thiopurine treatment in a young woman with Crohn’s disease. Eur J Case Rep Intern Med. 2021;8(3):002350. doi:10.12890/2021_002350
40. Kandiel A, Lashner B. Cytomegalovirus colitis complicating inflammatory bowel disease. Am J Gastroenterol. 2006;101(12):2857–2865. doi:10.1111/j.1572-0241.2006.00869.x
41. Zhou J, Huang S, Wang Z, et al. Targeting EZH2 histone methyltransferase activity alleviates experimental intestinal inflammation. Nat Commun. 2019;10(1):2427. doi:10.1038/s41467-019-10176-2
42. Li X, Song P, Li J, et al. The disease burden and clinical characteristics of inflammatory bowel disease in the Chinese population: a systematic review and meta-analysis. Int J Environ Res Public Health. 2017;14(3):238.
43. Ye B, van Langenberg DR. Mesalazine preparations for the treatment of ulcerative colitis: are all created equal? World J Gastrointest Pharmacol Ther. 2015;6(4):137–144. doi:10.4292/wjgpt.v6.i4.137
44. Qin Y, Wang G, Kong D, et al. Risk factors of cytomegalovirus reactivation in ulcerative Colitis patients: a meta-analysis. Diagnostics. 2021;11(11):1952. doi:10.3390/diagnostics11111952
45. Henmi Y, Kakimoto K, Inoue T, et al. Cytomegalovirus infection in ulcerative colitis assessed by quantitative polymerase chain reaction: risk factors and effects of immunosuppressants. J Clin Biochem Nutr. 2018;63(3):246–251. doi:10.3164/jcbn.18-14
46. Gullett JC, Nolte FS. Quantitative nucleic acid amplification methods for viral infections. Clin Chem. 2015;61(1):72–78. doi:10.1373/clinchem.2014.223289
47. Rossini G, Cerboni C, Santoni A, et al. Interplay between human cytomegalovirus and intrinsic/innate host responses: a complex bidirectional relationship. Mediators Inflamm. 2012;2012:607276. doi:10.1155/2012/607276
48. Jentzer A, Veyrard P, Roblin X, et al. Cytomegalovirus and Inflammatory Bowel Diseases (IBD) with a special focus on the link with Ulcerative Colitis (UC). Microorganisms. 2020;8(7):1078. doi:10.3390/microorganisms8071078
49. Watanabe Y, Hayashi K, Terai S. A rare case of Ulcerative Colitis with severe pneumocystis jirovecii Pneumonia and Cytomegalovirus Colitis: a case report and literature review. Intern Med. 2022;61(3):339–344. doi:10.2169/internalmedicine.7953-21
50. Lee SO, Razonable RR. Current concepts on cytomegalovirus infection after liver transplantation. World J Hepatol. 2010;2(9):325–336. doi:10.4254/wjh.v2.i9.325
51. Omeri AK, Okada F, Takata S, et al. Comparison of high-resolution computed tomography findings between Pseudomonas aeruginosa pneumonia and Cytomegalovirus pneumonia. Eur Radiol. 2014;24(12):3251–3259. doi:10.1007/s00330-014-3326-3
52. Moon JH, Kim EA, Lee KS, Kim TS, Jung KJ, Song JH. Cytomegalovirus pneumonia: high-resolution CT findings in ten non-AIDS immunocompromised patients. Korean J Radiol. 2000;1(2):73–78. doi:10.3348/kjr.2000.1.2.73
53. Casella G, Villanacci V, Di Bella C, Antonelli E, Baldini V, Bassotti G. Pulmonary diseases associated with inflammatory bowel diseases. J Crohns Colitis. 2010;4(4):384–389. doi:10.1016/j.crohns.2010.02.005
54. Foster RA, Zander DS, Mergo PJ, Valentine JF. Mesalamine-related lung disease: clinical, radiographic, and pathologic manifestations. Inflamm Bowel Dis. 2003;9(5):308–315. doi:10.1097/00054725-200309000-00004
55. Ananthakrishnan AN, Attila T, Otterson MF, et al. Severe pulmonary toxicity after azathioprine/6-mercaptopurine initiation for the treatment of inflammatory bowel disease. J Clin Gastroenterol. 2007;41(7):682–688. doi:10.1097/01.mcg.0000225577.81008.ee
56. Imokawa S, Colby TV, Leslie KO, Helmers RA. Methotrexate pneumonitis: review of the literature and histopathological findings in nine patients. Eur Respir J. 2000;15(2):373–381. doi:10.1034/j.1399-3003.2000.15b25.x
57. Lee HS, Jo KW, Shim TS, et al. Six cases of lung injury following anti-tumour necrosis factor therapy for inflammatory bowel disease. J Crohns Colitis. 2015;9(11):1053–1057. doi:10.1093/ecco-jcc/jjv135
58. Fabiszewska S, Derda E, Szymanska E, Osiecki M, Kierkus J. Safety and effectiveness of vedolizumab for the treatment of pediatric patients with very early onset inflammatory bowel diseases. J Clin Med. 2021;10(13):2997. doi:10.3390/jcm10132997
59. Rafailidis PI, Mourtzoukou EG, Varbobitis IC, Falagas ME. Severe cytomegalovirus infection in apparently immunocompetent patients: a systematic review. Virol J. 2008;5(1):47. doi:10.1186/1743-422X-5-47
60. Lee JH, Koh J, Jeon YK, Goo JM, Yoon SH. An integrated radiologic-pathologic understanding of COVID-19 Pneumonia. Radiology. 2023;306(2):e222600. doi:10.1148/radiol.222600
61. Shukla T, Singh S, Tandon P, McCurdy JD. Corticosteroids and thiopurines, but not tumor necrosis factor antagonists, are associated with cytomegalovirus reactivation in inflammatory bowel disease: a systematic review and meta-analysis. J Clin Gastroenterol. 2017;51(5):394–401. doi:10.1097/MCG.0000000000000758
62. Li L, Hsu SH, Gu X, et al. Aetiology and prognostic risk factors of mortality in patients with pneumonia receiving glucocorticoids alone or glucocorticoids and other immunosuppressants: a retrospective cohort study. BMJ Open. 2020;10(10):e037419. doi:10.1136/bmjopen-2020-037419
63. Wang S, Dou Y, Yang H, Ni A, Zhang R, Qian J. Alteration of glucocorticoid receptors and exacerbation of inflammation during lytic cytomegalovirus infection in THP-1 cells. FEBS Open Bio. 2017;7(12):1924–1931. doi:10.1002/2211-5463.12334
64. Singh S, Facciorusso A, Dulai PS, Jairath V, Sandborn WJ. Comparative risk of serious infections with biologic and/or immunosuppressive therapy in patients with inflammatory bowel diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2020;18(1):69–81 e63. doi:10.1016/j.cgh.2019.02.044
65. Xue Y, Jiang L, Wan WG, Chen YM, Zhang J, Zhang ZC. Cytomegalovirus Pneumonia in patients with rheumatic diseases after immunosuppressive therapy: a Single Center Study in China. Chin Med J. 2016;129(3):267–273. doi:10.4103/0366-6999.174490
66. Massart A, Hunt DP. Pulmonary manifestations of inflammatory bowel disease. Am J Med. 2020;133(1):39–43. doi:10.1016/j.amjmed.2019.07.007
67. Kirchgesner J, Lemaitre M, Carrat F, Zureik M, Carbonnel F, Dray-Spira R. Risk of serious and opportunistic infections associated with treatment of inflammatory bowel diseases. Gastroenterology. 2018;155(2):337–346 e310. doi:10.1053/j.gastro.2018.04.012
68. Gomollon F, Dignass A, Annese V, et al. 3rd European evidence-based consensus on the diagnosis and management of Crohn’s Disease 2016: part 1: diagnosis and medical management. J Crohns Colitis. 2017;11(1):3–25. doi:10.1093/ecco-jcc/jjw168
69. Vogelin M, Biedermann L, Frei P, et al. The impact of azathioprine-associated lymphopenia on the onset of opportunistic infections in patients with inflammatory bowel disease. PLoS One. 2016;11(5):e0155218. doi:10.1371/journal.pone.0155218
70. Tiede I, Fritz G, Strand S, et al. CD28-dependent Rac1 activation is the molecular target of azathioprine in primary human CD4+ T lymphocytes. J Clin Invest. 2003;111(8):1133–1145. doi:10.1172/JCI16432
71. Mallick B, Malik S. Use of azathioprine in Ulcerative Colitis: a comprehensive review. Cureus. 2022;14(5):e24874. doi:10.7759/cureus.24874
72. Dubinsky MC, Reyes E, Ofman J, Chiou CF, Wade S, Sandborn WJ. A cost-effectiveness analysis of alternative disease management strategies in patients with Crohn’s disease treated with azathioprine or 6-mercaptopurine. Am J Gastroenterol. 2005;100(10):2239–2247. doi:10.1111/j.1572-0241.2005.41900.x
73. Miechowiecki J, Stainer W, Wallner G, et al. Severe complication during remission of Crohn’s disease: hemophagocytic lymphohistiocytosis due to acute cytomegalovirus infection. Z Gastroenterol. 2018;56(3):259–263. doi:10.1055/s-0043-123999
74. Hissong E, Chen Z, Yantiss RK. Cytomegalovirus reactivation in inflammatory bowel disease: an uncommon occurrence related to corticosteroid dependence. Mod Pathol. 2019;32(8):1210–1216. doi:10.1038/s41379-019-0258-0
75. Rawla P, Sunkara T, Raj JP. Role of biologics and biosimilars in inflammatory bowel disease: current trends and future perspectives. J Inflamm Res. 2018;11:215–226. doi:10.2147/JIR.S165330
76. Forte E, Swaminathan S, Schroeder MW, Kim JY, Terhune SS, Hummel M. Tumor necrosis factor alpha induces reactivation of human cytomegalovirus independently of myeloid cell differentiation following posttranscriptional establishment of latency. mBio. 2018;9(5). doi:10.1128/mBio.01560-18
77. Docke WD, Prosch S, Fietze E, et al. Cytomegalovirus reactivation and tumour necrosis factor. Lancet. 1994;343(8892):268–269. doi:10.1016/S0140-6736(94)91116-9
78. Fakhreddine AY, Frenette CT, Konijeti GG. A practical review of cytomegalovirus in gastroenterology and hepatology. Gastroenterol Res Pract. 2019;2019:6156581. doi:10.1155/2019/6156581
79. D’Ovidio V, Vernia P, Gentile G, et al. Cytomegalovirus infection in inflammatory bowel disease patients undergoing anti-TNFalpha therapy. J Clin Virol. 2008;43(2):180–183. doi:10.1016/j.jcv.2008.06.002
80. Deng J, Xiao J, Lv L, et al. Immunosuppressive therapy alleviates murine cytomegalovirus recurrence by reducing TNF-alpha post cell transplantation with lethal GVHD. Antiviral Res. 2016;133:130–139. doi:10.1016/j.antiviral.2016.06.015
81. Jena A, Mishra S, Singh AK, Sekar A, Sharma V. Cytomegalovirus in ulcerative colitis: an evidence-based approach to diagnosis and treatment. Expert Rev Gastroenterol Hepatol. 2022;16(2):109–120. doi:10.1080/17474124.2022.2032662
82. Lavagna A, Bergallo M, Daperno M, et al. Infliximab and the risk of latent viruses reactivation in active Crohn’s disease. Inflamm Bowel Dis. 2007;13(7):896–902. doi:10.1002/ibd.20131
83. Fang S, Song Y, Zhang C, Wang L. Efficacy and safety of vedolizumab for pediatrics with inflammatory bowel disease: a systematic review. BMC Pediatr. 2022;22(1):175. doi:10.1186/s12887-022-03229-x
84. Bye WA, Jairath V, Travis SPL. Systematic review: the safety of vedolizumab for the treatment of inflammatory bowel disease. Aliment Pharmacol Ther. 2017;46(1):3–15. doi:10.1111/apt.14075
85. Colombel JF, Sands BE, Rutgeerts P, et al. The safety of vedolizumab for ulcerative colitis and Crohn’s disease. Gut. 2017;66(5):839–851. doi:10.1136/gutjnl-2015-311079
86. Bressler B, Yarur A, Silverberg MS, et al. Vedolizumab and anti-tumour necrosis factor alpha real-world outcomes in biologic-naive inflammatory bowel disease patients: results from the EVOLVE Study. J Crohns Colitis. 2021;15(10):1694–1706. doi:10.1093/ecco-jcc/jjab058
87. Yeh H, Kuo CJ, Wu RC, et al. Vedolizumab in Crohn’s disease with rectal fistulas and presacral abscess: a case report. World J Gastroenterol. 2021;27(5):442–448. doi:10.3748/wjg.v27.i5.442
88. Rawa-Golebiewska A, Lenarcik M, Zagorowicz E. Resolution of CMV infection in the bowel on vedolizumab therapy. J Crohns Colitis. 2019;13(9):1234–1235. doi:10.1093/ecco-jcc/jjz033
89. Hommel C, Pillet S, Rahier JF. Comment on: ‘resolution of CMV infection in the bowel on vedolizumab therapy’. J Crohns Colitis. 2020;14(1):148–149. doi:10.1093/ecco-jcc/jjz108
90. Zeissig S, Rosati E, Dowds CM, et al. Vedolizumab is associated with changes in innate rather than adaptive immunity in patients with inflammatory bowel disease. Gut. 2019;68(1):25–39. doi:10.1136/gutjnl-2018-316023
91. Agrawal M, Zhang X, Brenner EJ, Ungaro RC, Kappelman MD, Colombel JF. The impact of vedolizumab on COVID-19 outcomes among adult IBD patients in the SECURE-IBD registry. J Crohns Colitis. 2021;15(11):1877–1884. doi:10.1093/ecco-jcc/jjab071
92. Hommel C, Roblin X, Brichet L, Bihin B, Pillet S, Rahier J-F. P579 risk of CMV reactivation in UC patients with previous history of CMV infection following infliximab or vedolizumab treatments. J Crohns Colitis. 2018;12(supplement_1):S400–S400. doi:10.1093/ecco-jcc/jjx180.706
93. Hanauer SB, Sandborn WJ, Feagan BG, et al. IM-UNITI: three-year efficacy, safety, and immunogenicity of ustekinumab treatment of Crohn’s disease. J Crohns Colitis. 2020;14(1):23–32. doi:10.1093/ecco-jcc/jjz110
94. Abreu MT, Rowbotham DS, Danese S, et al. Efficacy and safety of maintenance ustekinumab for Ulcerative Colitis through 3 years: UNIFI long-term extension. J Crohns Colitis. 2022;16(8):1222–1234. doi:10.1093/ecco-jcc/jjac030
95. Chaparro M, Garre A, Iborra M, et al. Effectiveness and safety of ustekinumab in Ulcerative Colitis: real-world evidence from the ENEIDA registry. J Crohns Colitis. 2021;15(11):1846–1851. doi:10.1093/ecco-jcc/jjab070
96. Despotes KA, Vigeland CL. Stelara struck: a case of noninfectious pneumonitis secondary to ustekinumab. BMC Pulm Med. 2022;22(1):280. doi:10.1186/s12890-022-02066-z
97. Rolsdorph LA, Mosevoll KA, Helgeland L, Reikvam H. Concomitant hemophagocytic lymphohistiocytosis and cytomegalovirus disease: a case based systemic review. Front Med. 2022;9:819465. doi:10.3389/fmed.2022.819465
98. Brambilla B, Barbosa AM, Scholze CDS, et al. Hemophagocytic lymphohistiocytosis and inflammatory bowel disease: case report and systematic review. Inflamm Intest Dis. 2020;5(2):49–58. doi:10.1159/000506514
99. Soldera J, Bosi GR. Haemophagocytic lymphohistiocytosis following a COVID-19 infection: case report. J Infect Dev Ctries. 2023;17(3):302–303. doi:10.3855/jidc.16983
100. Sandonis V, Garcia-Rios E, McConnell MJ, Perez-Romero P. Role of neutralizing antibodies in CMV infection: implications for new therapeutic approaches. Trends Microbiol. 2020;28(11):900–912. doi:10.1016/j.tim.2020.04.003
101. La Rosa C, Diamond DJ. The immune response to human CMV. Future Virol. 2012;7(3):279–293. doi:10.2217/fvl.12.8
102. Pantaleo G, Correia B, Fenwick C, Joo VS, Perez L. Antibodies to combat viral infections: development strategies and progress. Nat Rev Drug Discov. 2022;21(9):676–696. doi:10.1038/s41573-022-00495-3
103. Scarpini S, Morigi F, Betti L, Dondi A, Biagi C, Lanari M. Development of a vaccine against human cytomegalovirus: advances, barriers, and implications for the clinical practice. Vaccines. 2021;9(6):551. doi:10.3390/vaccines9060551
104. Hu X, Wang HY, Otero CE, Jenks JA, Permar SR. Lessons from acquired natural immunity and clinical trials to inform next-generation human cytomegalovirus vaccine development. Annu Rev Virol. 2022;9(1):491–520. doi:10.1146/annurev-virology-100220-010653
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.