Back to Journals » Journal of Inflammation Research » Volume 19
Clinical Value of Inflammatory Indexes in Predicting Post-Transplantation Prognosis in Hepatocellular Carcinoma: A Retrospective Cohort Study
Authors Wang HX, Ye XY, Jiang T, Lyu SC, He Q ![]() , Ji ZL
, Ji ZL ![]() , Lang R
, Lang R
Received 20 March 2026
Accepted for publication 18 June 2026
Published 3 July 2026 Volume 2026:19 610101
DOI https://doi.org/10.2147/JIR.S610101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Fatih Türker
Han-xuan Wang1,2,*, Xiao-yong Ye1,2,*, Tao Jiang1,2, Shao-cheng Lyu1,2, Qiang He1,2, Zhi-li Ji1,2, Ren Lang1,2
Division of Hepatobiliary and Pancreaticosplenic Surgery, Department of General Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Clinical and Research Center for Pancreatic Cancer, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ren Lang, Division of Hepatobiliary and Pancreaticosplenic Surgery, Department of General Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected]; Zhi-li Ji, Division of Hepatobiliary and Pancreaticosplenic Surgery, Department of General Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, 100020, People’s Republic of China, Email [email protected]
Background: Liver transplantation (LT) is an effective treatment for hepatocellular carcinoma (HCC), and inflammatory indexes are accessible, non-invasive prognostic biomarkers for HCC patients. This study aims to systematically evaluate the clinical value of various preoperative inflammatory indexes in predicting post-LT outcomes to optimize the stratification of suitable HCC patients that can benefit from LT.
Methods: This retrospective study included 239 HCC patients who underwent LT from April 2013 to July 2023 and their inflammatory biomarkers were calculated. Univariate and multivariate analysis were applied to identify independent risk factors for postoperative prognosis. Subgroup analysis was used to evaluate the predictive value in different sub-populations. Prediction models based on preoperative indexes were established using multiple machine-learning model. Mediating effect analysis was utilized to elucidate potential mediating factors.
Results: Inflammation biomarkers were significantly different in patients with different postoperative prognosis. Lymphocyte-to-monocyte ratio (LMR, RR: 0.806, 95% CI: 0.675– 0.962, P=0.017) served as an independent predictor for early tumor recurrence, with an optimal cutoff of 2.03. The systemic immune-inflammation index served as an independent risk factor for both overall survival (HR: 3.472, 95% CI: 1.322– 9.119, P=0.012) and disease-free survival (HR: 2.604, 95% CI: 1.012– 6.698, P=0.047), with an optimal cutoff value of 155.19. The prognostic value of SII was robust across nearly all clinical subgroups, while the predictive value of LMR was limited to certain subgroups. The random survival forest model, incorporating alpha-fetoprotein and SII as its most important variables, achieved apparent and bootstrap-corrected C-indexes of 0.814 and 0.754 and apparent and bootstrap-corrected area under receiver characteristic curve of 0.854 and 0.788, demonstrating the optimal predictive accuracy in all established models. Mediating analysis indicated that tumor T stage significantly mediated the correlation between SII and postoperative survival outcomes, while liver function and tumor burden (T stage and tumor number) exerted significantly suppression and mediating effect on correlation between LMR and early tumor recurrence.
Conclusion: Preoperative LMR and SII are associated with early tumor recurrence and long-term prognosis in HCC patients after LT. A random survival forest model that integrated these inflammatory indexes with other preoperative variables may serve as a potential complementary tool for early risk stratification in the future after verified by further external validation.
Keywords: hepatocellular carcinoma, liver transplantation, prognosis, inflammatory index, lymphocyte-to-monocyte ratio, systemic immune-inflammation index
Background
Hepatocellular carcinoma (HCC) has always been the most lethal cancer type worldwide, especially in China due to the prevalence of hepatitis B virus (HBV) infection.1 As the effort of controlling HBV infection and progression in HCC management, the incidence of HCC in China gradually decreased while the prognosis of HCC patients improved significantly in recent years.2 However, since the atypical initial symptoms of HCC and the cirrhosis background, the treatment options of some HCC patients were rather limited due to unresectable tumor stage or poor liver function. Liver transplantation (LT) is an important therapy for these patients because it simultaneously eliminates the entire tumor burden and cures the underlying end-stage cirrhotic liver.3 For highly selected patients, particularly those meeting strict criteria, LT offers superior long-term survival and represents an ideal curative option.4
However, despite rigorous pre-transplant evaluations, the outcomes for some recipients remained unsatisfying. According to researches, 16% of HCC patients developed post-transplantation recurrence, among which nearly 50% of patients met the Milan criteria.5 Moreover, about 70% of post-transplantation recurrence developed in the first 2 year after surgery, which significantly impacted the post-LT prognosis.6 Therefore, accurately stratifying risk and identifying patients prone to poor prognosis is of clinical importance to optimize individualized management and improve overall survival (OS).
In recent years, accumulating evidence has highlighted that systemic inflammation can be induced by malignancy and subsequently reshape local tumor micro-environment, thereby exerting protumor effect.7 Previous researches have confirmed that sustained systemic inflammation can significantly impact post-resection prognosis of HCC, highlighting the close relationship between systemic inflammation and HCC outcomes.8 Therefore, researchers gradually focused on the impact of the systemic inflammatory status on post-transplantation prognosis of HCC patients. In clinical practice, routine blood test-derived inflammatory indexes, such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), lymphocyte-to-monocyte ratio (LMR), have emerged as non-invasive, cost-effective, and easily accessible biomarkers, and were validated as effective predictors for clinical outcomes in HCC after LT.9–11 However, despite their proven utility, a comprehensive and systematic evaluation of the prognostic value of these inflammatory indexes specifically in HCC patients after LT remains limited. Therefore, we intend to conduct this study to systematically investigate the clinical value of various blood routine-derived inflammatory indexes in predicting post-transplantation survival and recurrence in HCC patients, aiming to provide robust evidence for optimizing prognostic models and guiding clinical decision-making.
Methods
Study Design and Reporting Guideline
This study adopted a retrospective cohort study design and adhered to the REporting of studies Conducted using Observational Routinely collected health Data (RECORD) guidelines.12 The access to retrospective data was approved by the Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University (Granted No. 2020-D.-303). The written inform consent from patients was waived by the Ethics Committee of Beijing Chao-Yang Hospital, Capital Medical University due to the retrospective study design.
Patient Selection
HCC patients who received orthotopic LT in Beijing Chao-Yang Hospital, Capital Medical University from April 2013 to July 2023 were retrospectively included in our research and were further screened according to the inclusion and exclusion criteria:
Inclusion criteria:
- Received orthotopic LT without surgical contraindications;
- Postoperative pathological examination indicated HCC.
Exclusion criteria:
- Complicated with hypersplenism or other acute infectious disease;
- Perioperative death;
- Loss of follow-up.
Collection of Included Data
All investigators had direct access to the institutional electronic medical record system to identify eligible patients and extract data. The preoperative general data (sex, age, medical history, model of end-stage liver disease (MELD) score, preoperative treatment), preoperative laboratory test (white blood cell (WBC), neutrophil (NEUT), lymphocyte (LYM), monocyte (MONO), platelet (PLT), hemoglobin (HB), red blood cell distribution width (RDW), albumin (ALB), high-density lipoprotein cholesterol (HDL-c), total bilirubin (TB), alpha fetoprotein (AFP)), intraoperative surgical condition (operation time, anhepatic phase, blood loss, blood transfusion), postoperative pathological examination (tumor differentiation, tumor diameter, tumor number, microvascular invasion (MVI), capsule invasion) and follow-up condition (tumor recurrence, mortality) were retrospectively obtained from the electronic medical record system of our hospital. All preoperative laboratory tests were based on the latest results obtained within one week before the surgery. All included inflammatory biomarkers were calculated by the formula shown in supplementary Table 1. The MELD score was calculated using the formula of MELD score = 3.8×ln(bilirubin[mg/dL]) + 11.2 × ln(INR) + 9.6×ln(creatinine [mg/dL]) + 6.4× (etiology: 0 if cholestatic or alcoholic, 1 otherwise).13 The anhepatic phase was defined as the time from the physical removal of the liver from the recipient to portal vein reperfusion of the graft.14 MVI was defined as a nest of malignant cells in vessels lined with endothelial cells only detectable under a microscope. It can be further categorized into M0 (no MVI), M1 (MVI <5 vessels and ≤1 cm away from the adjacent peritumoural liver tissue) and M2 (MVI >5 vessels or >1 cm away from the adjacent peritumoural liver tissue), among which M1 and M2 were considered to have MVI.15 Capsule invasion was defined as cancer cells penetrating to the liver parenchyma through the fibrous capsule.16
Follow-Up Schedule
All included patients were followed up during postoperative period by the follow-up specialist in our department via telephone or outpatient visit. All patients were first followed at postoperative 1 and 3 months. Then the frequency of follow-up was set as 3 months within the first 2 year after surgery, and 6 months thereafter. The result of postoperative laboratory and imaging examination, treatment regimen and survival condition were collected during each follow-up. The primary endpoint of follow-up in our study was postoperative mortality, and the secondary endpoint of follow-up was postoperative tumor recurrence. OS time was defined as the time from surgery to postoperative death from any cause, while disease-free survival (DFS) was defined as the time from surgery to postoperative recurrence. Post-transplantation early recurrence was defined as tumor recurrence within 1 years after liver transplantation according to previous research.17
Determination and Validation of Cutoff Value
For OS and DFS, the optimal cutoff for indexes was calculated using maximally selected rank statistics using the “survminer” package. For early tumor recurrence, the optimal cutoff of indexes was determined using Youden’s index from receiver operating characteristic (ROC) analysis. Since optimal cutoffs for continuous indexes were determined using data‑driven methods, we performed internal validation to mitigate overfitting risk. Bootstrap resampling (B=500) was used to re-calculate optimal cutoffs, and a cutoff was considered stable if selected in ≥80% of bootstraps or if ≥70% of bootstrapped cutoffs fell within ± 10% of the original. For early recurrence, bootstrap (B=500) was applied to a univariate logistic regression model to obtain optimism-corrected odds ratios (ORs). Ten-fold cross-validation was performed on the logistic model to estimate the mean area under the ROC curve (AUC); folds containing only one class in the validation set were excluded, and the average AUC across evaluable folds was reported. For survival outcomes, bootstrap (B=500) was also applied to the final multivariate Cox model to obtain optimism-corrected hazard ratios. Ten-fold cross-validation was performed to estimate discriminative ability by calculating C-index. All procedures used “boot”, “survminer” and “caret” packages.
Identification of Independent Risk Factors
For early postoperative recurrence, least absolute shrinkage and selection operator (LASSO) regression was first applied to screen out potential risk factors. Features selected through LASSO regression were further included in multivariate logistic regression to determine independent predictors of early tumor recurrence. For OS and DFS, Kaplan–Meier method was utilized to calculate survival curves and Log rank test was used to compare the differences in survival rates between groups by “survminer” package. Variables that were statistically significant in Log rank tests were considered as potential risk factors and included in multivariate analysis. Multivariable Cox regression was then applied to identify independent risk factors for postoperative OS and DFS.
Establishment and Visualization of Prediction Models
Prediction model for postoperative overall survival were established by including preoperative predictors including age, sex, diabetes history, primary liver disease, liver cirrhosis, MELD score, albumin, TB, AFP, PLR, SII, SIRI, AISI. Six machine learning survival models including random survival forest (RSF), CoxBoost, eXtreme gradient boosting (XGBoost), partial least-squares regression for Cox models (plsRcox), survival support vector machine (SurvivalSVM) and supervised principal components (SuperPC) were built on the entire dataset using “randomForestSRC”, “CoxBoost”, “xgboost”, “plsRcox”, “survivalsvm”, and “superpc” packages, respectively. Hyperparameters for each algorithm were tuned on the full cohort prior to final model fitting: RSF used grid search over ntree ∈ {500, 1000, 2000} and nodesize ∈ {5, 10, 15} guided by the OOB C-index; CoxBoost optimized its regularization penalty via optimCoxBoostPenalty and boosting steps by 10-fold cross-validation; XGBoost used 5-fold cross-validation with early stopping over eta, max_depth, and gamma minimizing the Cox negative log-likelihood; SurvivalSVM used 5-fold cross-validation over gamma.mu maximizing the C-index; SuperPC selected the feature-score threshold by 10-fold cross-validation; and plsRcox determined the number of components via cv.plsRcox. To address overfitting in this moderate-sized cohort, bootstrap internal validation (B = 500) was performed following the Harrell optimism-correction framework. In each iteration, each model was refit on a bootstrap resample and evaluated on both the resample and the original cohort; optimism-corrected performance was obtained as apparent performance minus mean optimism across iterations, applied to the C-index and time-dependent AUC at following timepoints including 12, 18, 24, 30, 36, 42, 48, 54 and 60 months, with 95% confidence intervals derived from bootstrap percentiles. The best model was selected by optimism-corrected C-index. Calibration was assessed by calibration curve using “rms” package. Decision curve analysis (DCA) analysis was performed to evaluate the clinical utility using “rmda” package. SHapley additive explanation (SHAP) was applied to visualise feature importance and dependence using “kernalshap” and “shapviz” package.
Statistical Analysis
Quantitative data that conform to normal distribution were expressed as the  , while non-normally distributed data were expressed as the M (Q1, Q3). t-tests were used to compare normally distributed quantitative data, and rank sum tests were applied to compare non-normally distributed quantitative data. Chi-Square test was used to compare categorical data. Quantitative variables with missing rate less than 20% was imputed by the multiple imputation, while quantitative variables with missing rate more than 20% or categorical data with missing rate were excluded. The number and proportion of missing values for each variable were shown in supplementary Table 2. Multicolinear diagnostic analysis was applied to evaluate the colinearity among indexes. Subgroup analysis was performed by “jstable” package. Firth Logistic and Cox regression analysis were utilized when complete or quasi-complete separation was observed in certain subgroups using “logistf” and “coxphf” package. Correlation between non-normally distributed data was evaluated by Spearman analysis. Mediating effect analysis was performed using “mediation” package. Data was analyzed using SPSS 26.0 (Version 26.0) and R (Version 4.5.0). Figures were generated by R (Version 4.5.0) and Graphpad (Version 9.0). P < 0.05 was considered statistically significant.
, while non-normally distributed data were expressed as the M (Q1, Q3). t-tests were used to compare normally distributed quantitative data, and rank sum tests were applied to compare non-normally distributed quantitative data. Chi-Square test was used to compare categorical data. Quantitative variables with missing rate less than 20% was imputed by the multiple imputation, while quantitative variables with missing rate more than 20% or categorical data with missing rate were excluded. The number and proportion of missing values for each variable were shown in supplementary Table 2. Multicolinear diagnostic analysis was applied to evaluate the colinearity among indexes. Subgroup analysis was performed by “jstable” package. Firth Logistic and Cox regression analysis were utilized when complete or quasi-complete separation was observed in certain subgroups using “logistf” and “coxphf” package. Correlation between non-normally distributed data was evaluated by Spearman analysis. Mediating effect analysis was performed using “mediation” package. Data was analyzed using SPSS 26.0 (Version 26.0) and R (Version 4.5.0). Figures were generated by R (Version 4.5.0) and Graphpad (Version 9.0). P < 0.05 was considered statistically significant.
Results
General Condition of Included HCC Patients
This study retrospectively included 239 HCC constituting of 220 males and 19 females. The flow diagram of patient selection was shown in Figure 1. The age of included patients was 54.0 (49.0, 60.0) years. One hundred and four cases received preoperative treatment, and the treatment regimen included both systemic treatment (targeted and immune therapy) and local treatment (transarterial chemoembolization and radiofrequency ablation). All included patients received piggyback orthotopic LT (OLT) and were diagnosed as HCC in postoperative pathological examination. The operation time in included patients was 520.00 (457.00, 612.50) min, and the anhepatic phase was 75.00 (55.00, 120.00) min. The rest baseline data of included patients was summarized in Table 1.
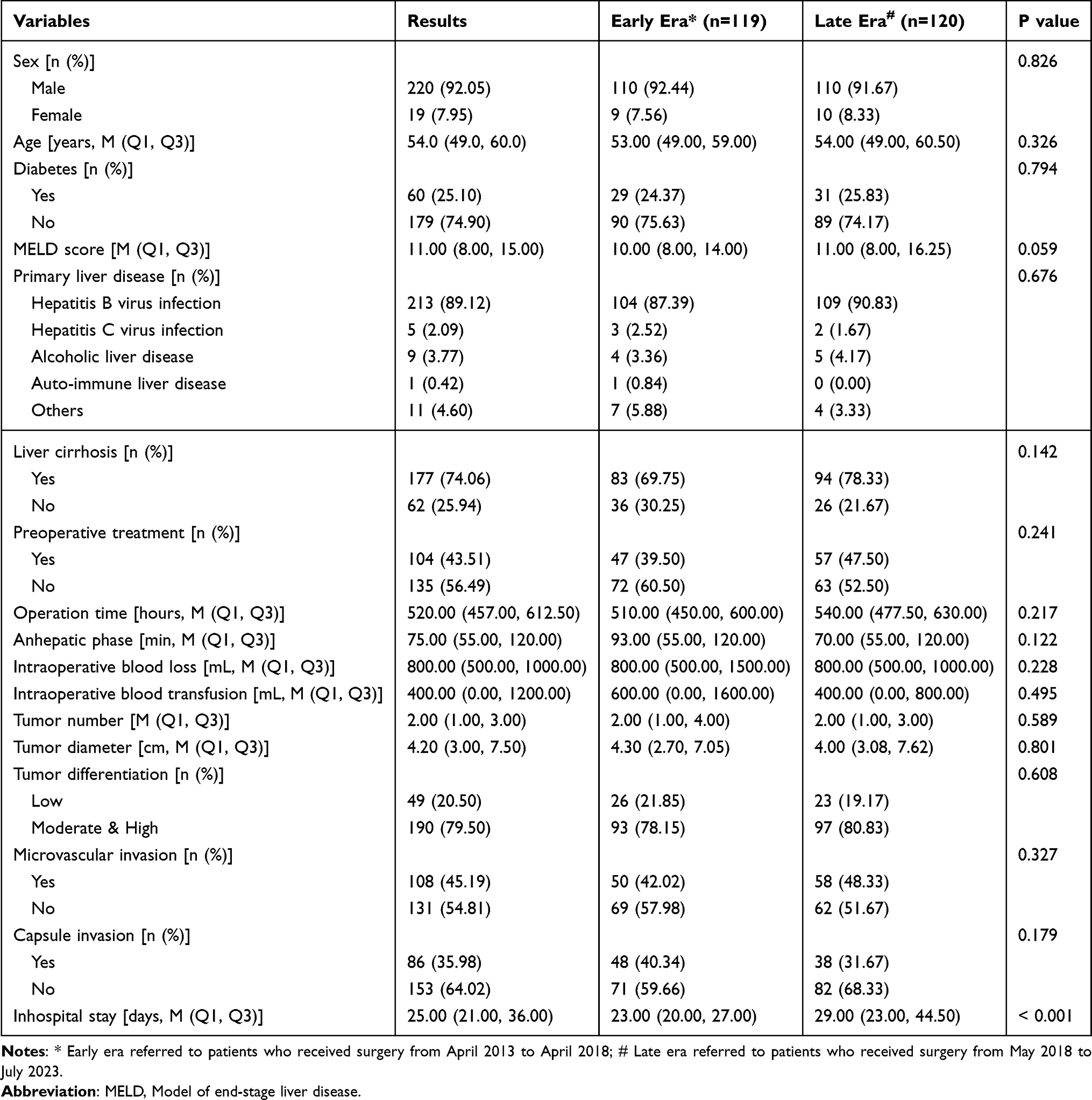 |
Table 1 General Condition of Included Patients |
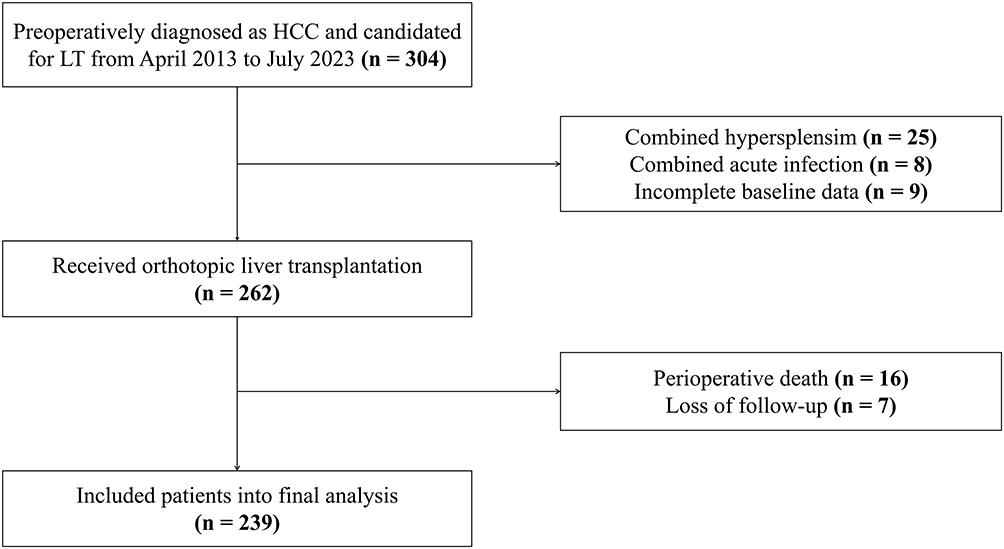 |
Figure 1 Flow diagram of patients selection. |
The follow-up of study ended in December 2025, and the follow-up period of included patients was 68.00 (62.09, 73.91) months. Thirty-nine (16.3%) patients suffered from early tumor recurrence, defined as post-transplantation recurrence within postoperative 12-months. Both the medium OS time and DFS time were not reached in our cohort. The OS rate and DFS rate at postoperative 1-year, 3-year and 5-year were 91.2%, 72.4%, 64.5% and 83.7%, 69.1%, 62.7%, respectively.
Given that this study enrolled patients over a 10-year period, we categorized patients into early era group (underwent OLT from April 2013 to April 2018, n=119) and late era group (underwent OLT from May 2018 to July 2023, n=120). Patients in late era group had prolonged hospital stay, but all other baseline characteristics were comparable (Table 1). The OS and DFS time did not differ significantly between the early and late era groups (Figure S1).
Inflammatory Indexes Can Identify Patients with Poor Long-Term Prognosis
We first categorized patients according to their 5-year DFS and OS to evaluate the effect of preoperative inflammatory indexes on post-transplantation prognosis. As shown in Table 2, patients who suffered post-transplantation death within postoperative 5-year had significantly higher NLR, PLR, systemic immune-inflammatory index (SII), systemic inflammation response index (SIRI), aggregate index of systemic inflammation (AISI), neutrophil-monocyte-to-lymphocyte ratio (NMLR) and neutrophil-to-albumin ratio (NAR) compared to other patients. Further ROC analysis of these indexes showed statistically significant prognostic value for both post-transplantation OS and DFS, especially SII, AISI, PLR and SIRI (Figure 2A and B). The AUC of SII, AISI, PLR and SIRI in predicting post-operative OS were 0.650 (95% CI: 0.579–0.722), 0.638 (95% CI: 0.566–0.711), 0.616 (95% CI: 0.541–0.691) and 0.621 (95% CI: 0.548–0.695), and the AUC in predicting post-operative DFS were 0.673 (95% CI: 0.603–0.743), 0.661 (95% CI: 0.590–0.732), 0.627 (95% CI: 0.553–0.700) and 0.640 (95% CI: 0.568–0.712), respectively. Collinearity analysis of these indexes with their components confirmed no statistically significant co-linear correlation, indicating that their predictive value relied on the combination of multiple indices rather than on any individual index (Figure S2).
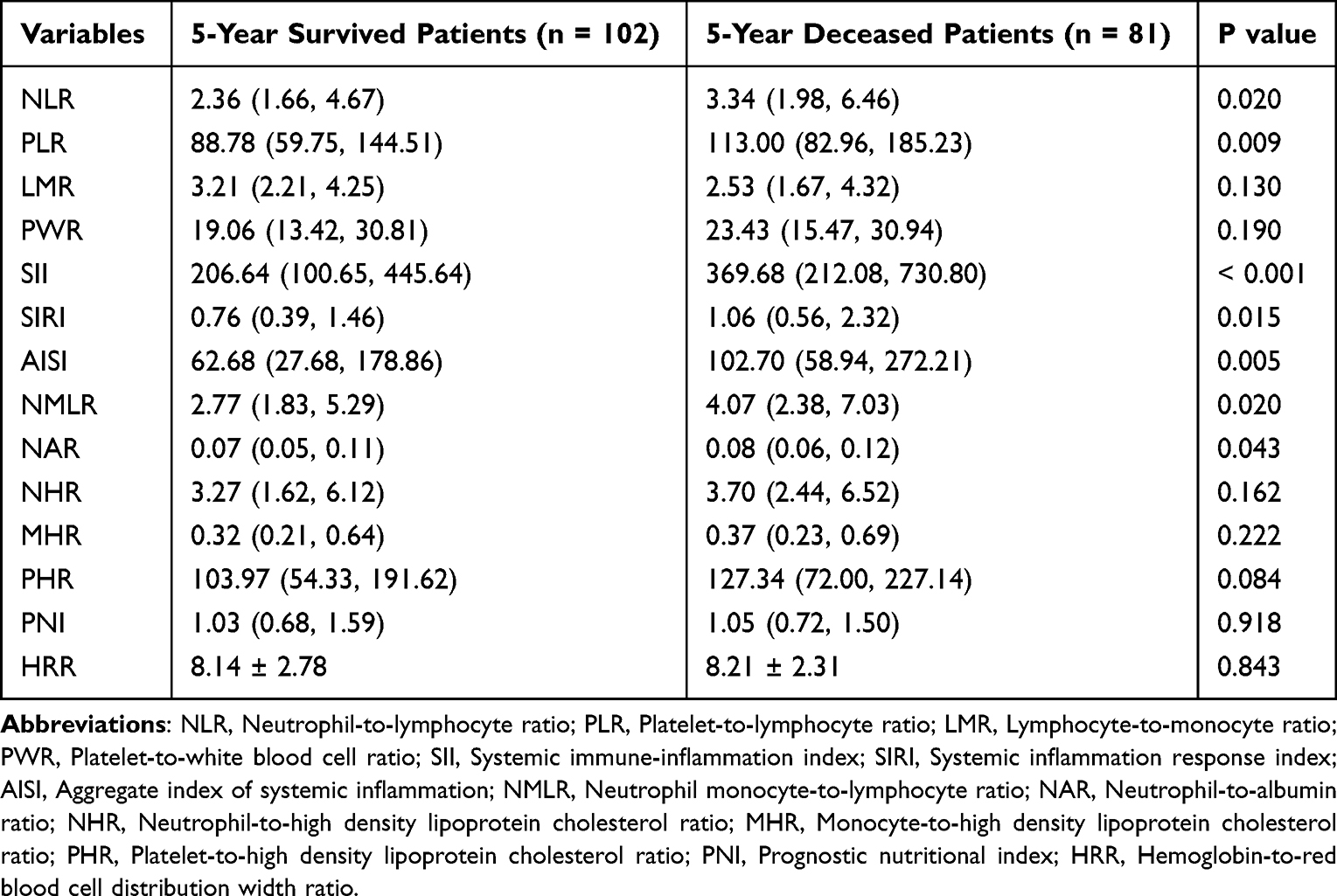 |
Table 2 Comparison of Preoperative Blood Derived Inflammatory Indexes Between 5-Year Survived and Deceased Patients |
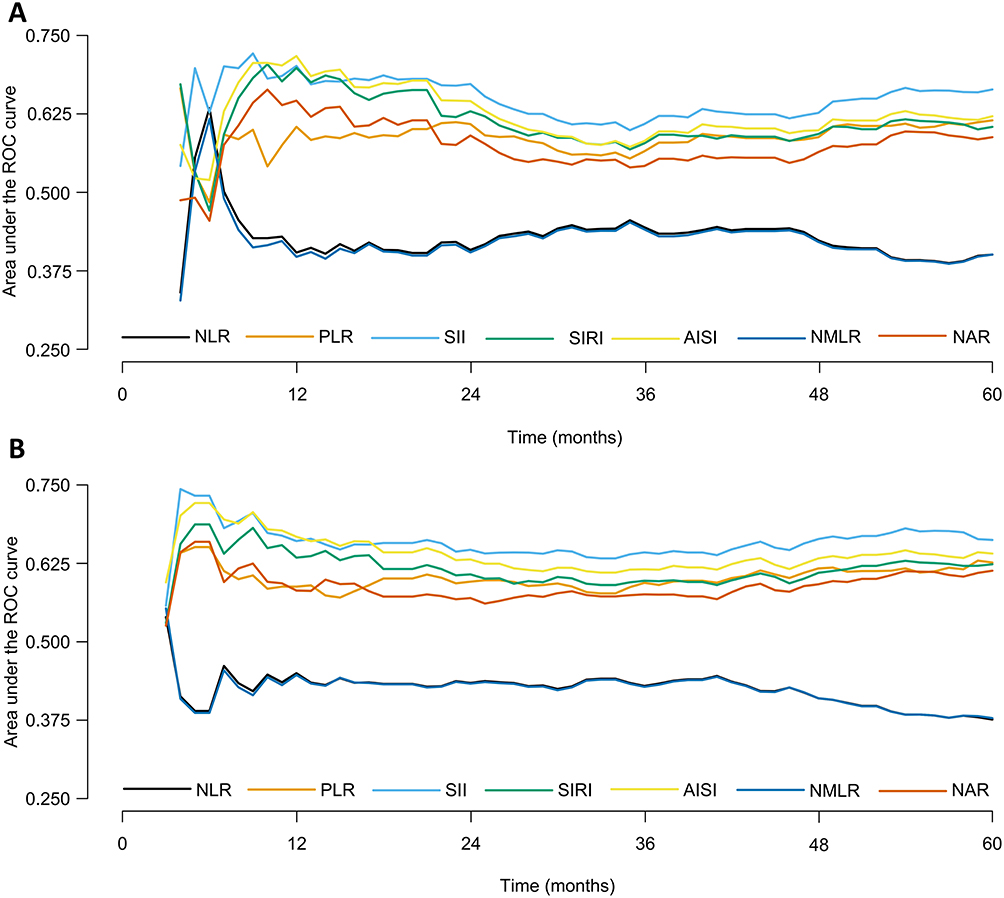 |
Figure 2 Variation of area under the ROC curve of inflammatory indexes and postoperative prognosis: (A) Area under the ROC curve of inflammatory indexes in predicting overall survival; (B) Area under the ROC curve of inflammatory indexes in predicting disease-free survival. Abbreviation: ROC, Receiver operating characteristic curve; NLR, Neutrophil-to-lymphocyte ratio; PLR, Platelet-to-lymphocyte ratio; LMR, Lymphocyte-to-monocyte ratio; PWR, Platelet-to-white blood cell ratio; SII, Systemic immune-inflammation index; SIRI, Systemic inflammation response index; AISI, Aggregate index of systemic inflammation; NMLR, Neutrophil monocyte-to-lymphocyte ratio; NAR, Neutrophil-to-albumin ratio |
We further compared these inflammatory biomarkers in patients who developed post-operative early recurrence with other patients, and the result showed that LMR, SII, SIRI, AISI and MHR were significantly different (Table 3, P < 0.05). ROC analysis indicated that the AUC of LMR, SII, SIRI, AISI and monocyte-to-high density lipoprotein cholesterol (MHR) in predicting postoperative early recurrence were 0.607 (95% CI: 0.500–0.714), 0.615 (95% CI: 0.536–0.693), 0.614 (95% CI: 0.533–0.695), 0.635 (95% CI: 0.558–0.712) and 0.564 (95% CI: 0.484–0.644), respectively. These exploratory results suggested that several preoperative inflammatory indexes may be associated with early recurrence and long‑term prognosis.
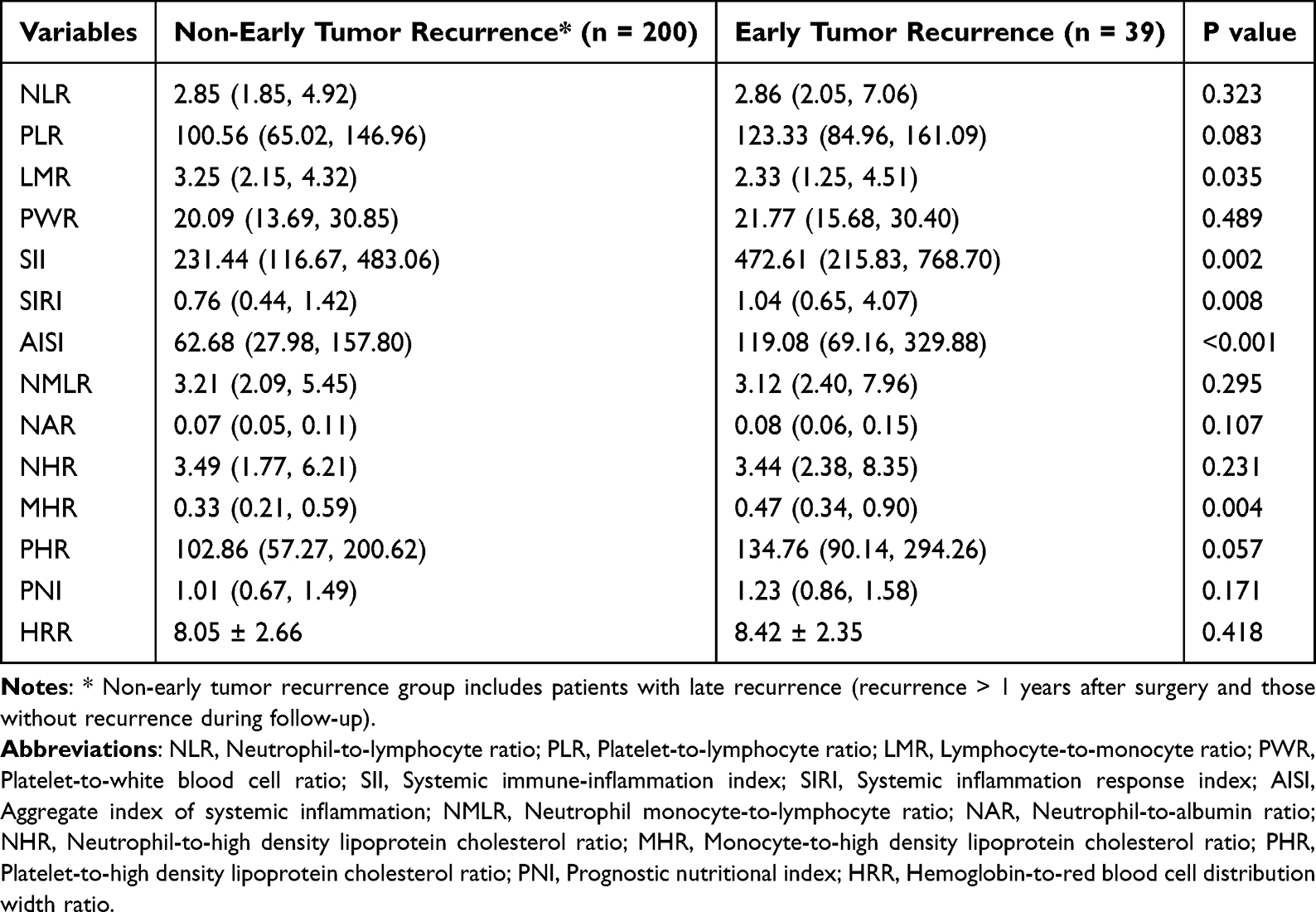 |
Table 3 Comparison of Preoperative Blood Derived Inflammatory Indexes Between Patients with Early Tumor Recurrence and Those Without Early Tumor Recurrence |
LMR Was Associated with Early Tumor Recurrence
Since inflammatory biomarkers differed significantly between patients with and without early tumor recurrence, we further evaluated the predictive value of these differential indexes for early tumor recurrence. According to LASSO regression, primary liver disease, tumor differentiation, MVI, capsule invasion, tumor number, tumor diameter, ALB, AFP and LMR were identified as potential risk factor for early recurrence (Figure 3A and B). After including these factors into multivariate Logistic regression model, only preoperative MVI (RR: 2.675, 95% CI: 1.177–6.081, P=0.019), AFP (per 100 ng/mL increase, RR: 1.015, 95% CI: 1.005–1.024, P=0.002) and LMR (RR: 0.806, 95% CI: 0.675–0.962, P=0.017) were independently correlated with occurrence of early tumor recurrence (Figure 3C). A sensitive analysis excluding patients who received preoperative treatment confirmed that LMR remained significantly associated with early recurrence in this subgroup (Figure S3). Further ROC analysis showed that the optimal cutoff value of LMR for early tumor recurrence was 2.03. Sixty-three (26.4%) patients were categorized into low LMR group including 19 cases that developed early recurrence, while 176 (73.6%) patients were categorized into a high LMR group including 20 cases that developed early recurrence. The distribution of LMR visualized by histogram showed that in Figure S4A. The risk of early recurrence in patients with LMR ≥2.03 was 70% lesser compared to LMR < 2.03 (RR: 0.297, 95% CI: 0.146–0.605, P=0.001). Bootstrap internal validation of LMR cutoff value showed a median of 2.06 and a stability proportion of 47.4%, which may be attributed to the limited number of early recurrence events (n=39). Optimism-corrected OR of LMR categorized by proposed cutoff value was 0.276 (bootstrap 95% CI: 0.148–0.613), and cross‑validated AUC was 0.655, supporting the robustness of the association despite some instability of the exact cutoff. Thus, LMR may be associated with early postoperative HCC recurrence after LT.
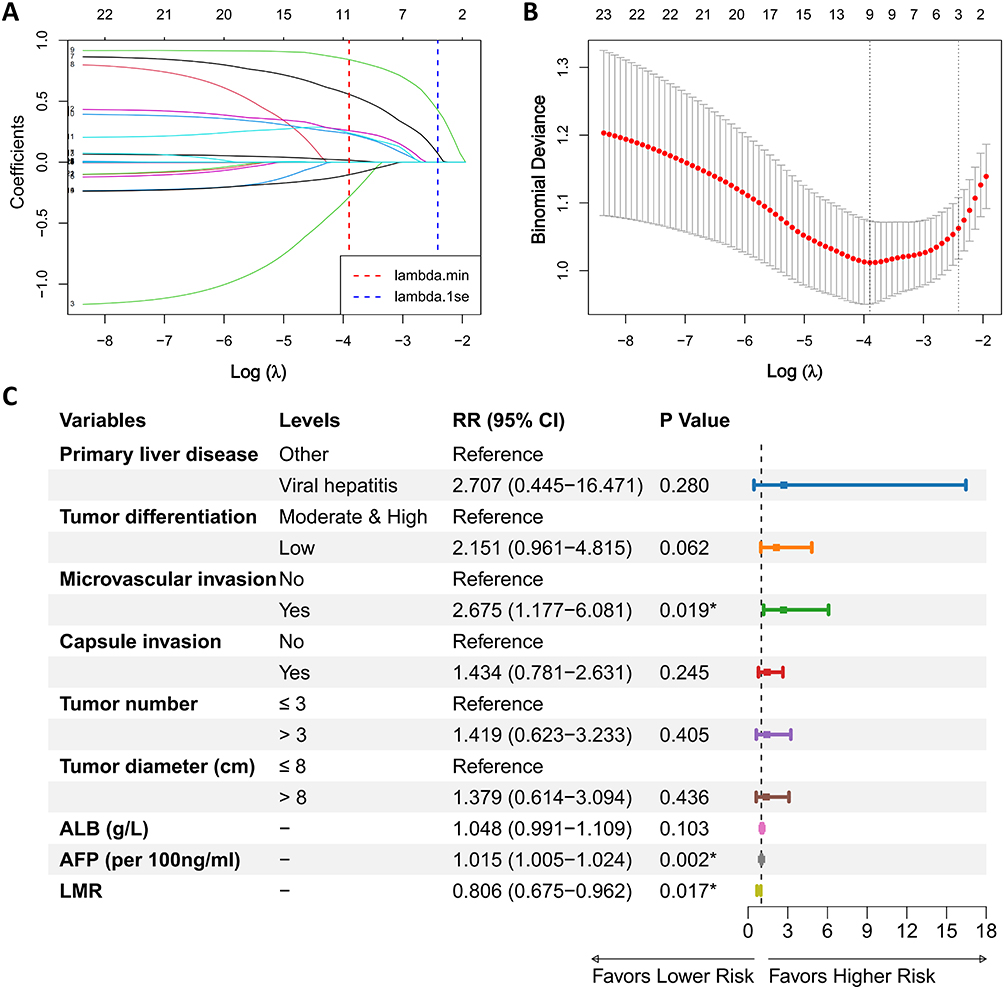 |
Figure 3 Identification of risk factors for post-transplantation early tumor recurrence: (A) Coefficient path plot of LASSO regression; (B) Cross-validation curve of LASSO regression; (C) Result of multivariate logistic regression for postoperative early tumor recurrence. * P < 0.05). Abbreviations: OR, Odds ratio; CI, Confidence interval; ALB, Albumin; AFP, Alpha fetoprotein; LMR, Lymphocyte-to-monocyte ratio. |
SII Served as an Independent Risk Factor for Postoperative Prognosis
Since SII, AISI, PLR and SIRI had significant better prognosis value according to ROC analysis, we further performed maximally selected rank statistics method to determine the optimal cutoff. The optimal cutoff value of SII, AISI, PLR and SIRI were 155.19, 66.42, 73.4 and 1.41, respectively (Figure 4A–D). Other continuous data was also converted to categorical data according to the cutoff value determined by maximally selected rank statistics method (Figure S5). After categorized patients based on these cutoff values, patients with elevated inflammatory indexes had significantly worse OS (Figure 4E–H) and DFS (Figure 4I–L). Univariate analysis confirmed that tumor differentiation, tumor number, tumor diameter, MVI, capsule invasion, neutrophil, platelet, TB, AFP, PLR, SII, SIRI and AISI as potential risk factors for postoperative OS, while primary liver diseases, tumor differentiation, tumor number, tumor diameter, MVI, capsule invasion, neutrophil, platelet, AFP, PLR, SII, SIRI and AISI were potential risk factors for postoperative DFS (Table 4). Further multivariate analysis confirmed MVI (HR: 2.376, 95% CI: 1.294–4.362, P=0.005), capsule invasion (HR: 1.638, 95% CI: 1.005–2.669, P=0.048), tumor diameter >8cm (HR: 1.666, 95% CI: 1.016–2.730, P=0.043), AFP > 156.8 ng/mL (HR: 2.051, 95% CI: 1.280–3.287, P=0.003) and SII >155.19 (HR: 2.604, 95% CI: 1.012–6.698, P=0.047) as independent risk factors for post-transplantation DFS (Figure 5A), and MVI (HR: 2.564, 95% CI: 1.371–4.797, P=0.003), capsule invasion (HR: 1.884, 95% CI: 1.145–3.102, P=0.013), TB > 14.6 umol/L (HR: 2.532, 95% CI: 1.166–5.498, P=0.019), AFP > 156.8 ng/mL (HR: 2.332, 95% CI: 1.421–3.826, P=0.001) and SII >155.19 (HR: 3.472, 95% CI: 1.322–9.119, P=0.012) as independent risk factors for post-transplantation OS (Figure 5B). Further sensitivity analysis excluding patients who received preoperative treatment revealed that preoperative SII > 155.19 remained the independent risk factor for both postoperative DFS (HR: 2.880, 95% CI: 1.125–7.377, P=0.027) and OS (HR: 4.078, 95% CI: 1.581–10.522, P=0.004) as shown in Supplementary Table 3 and Figure S6. The distribution of SII visualized by histogram showed that in Figure S4B. Bootstrap internal validation showed that the median bootstrap cutoff of SII was also 155.19, and 72.6% of bootstrap cutoffs fell within ±10% of the original. Optimism correction HR of SII categorized by the proposed cutoff value in univariate Cox model was 3.277 (bootstrap 95% CI: 2.072–7.735), and the ten‑fold cross‑validation yielded a mean C‑index of 0.616 (95% CI: 0.579–0.653), supporting the robustness of proposed cutoff value of SII. These results indicated that SII served as an effective prognostic biomarker for postoperative long-term prognosis.
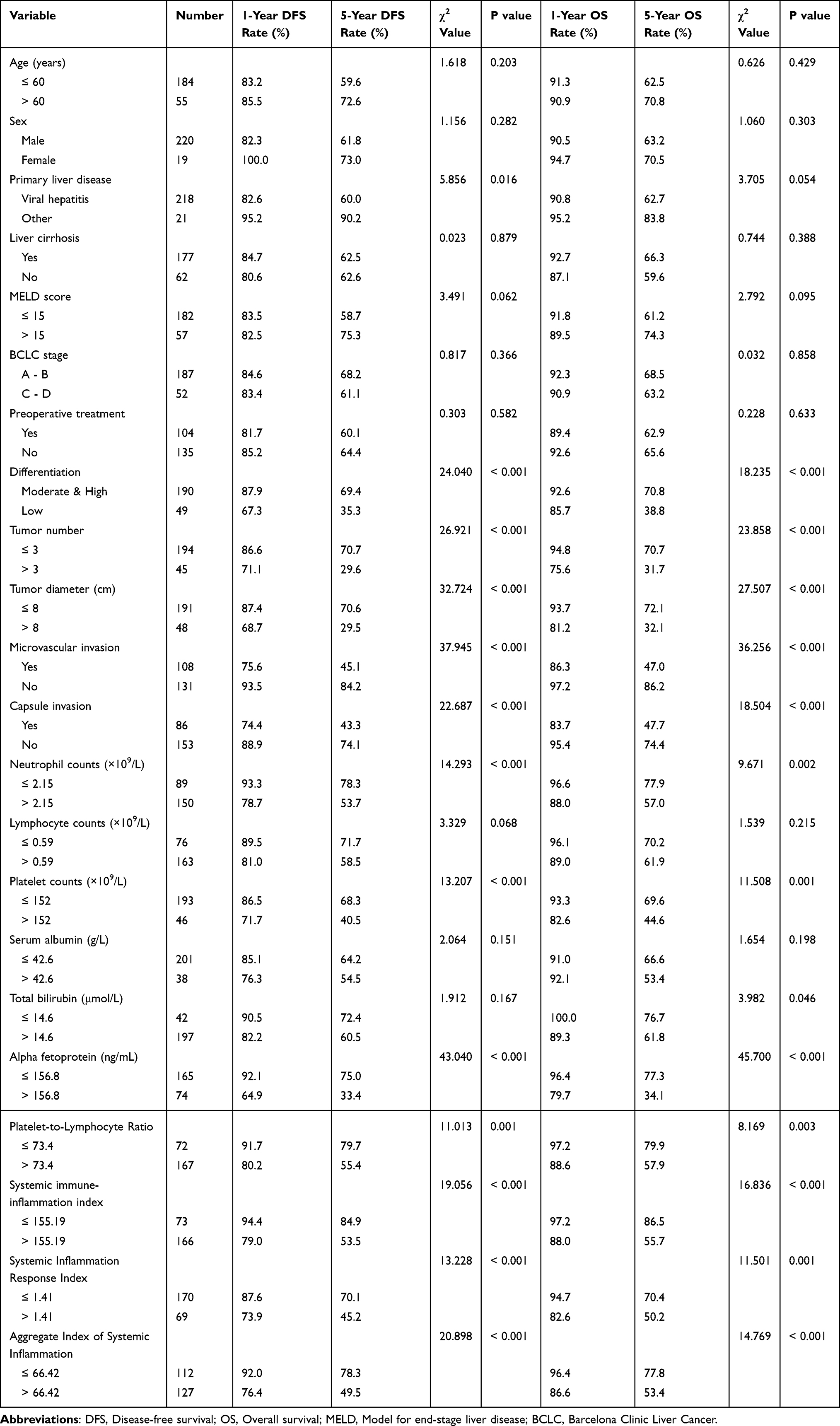 |
Table 4 Univariate Analysis for Postoperative Disease-Free and Overall Survival |
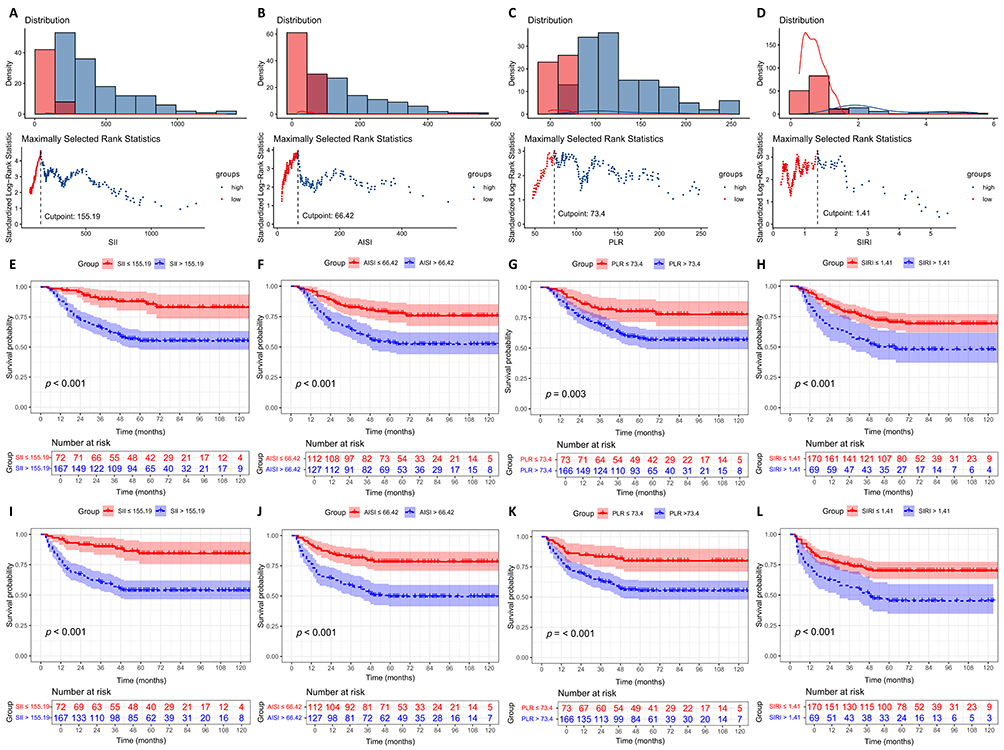 |
Figure 4 Impact of preoperative inflammatory indexes on postoperative prognosis: (A-D) determination of cutoff value of SII (A), AISI (B), PLR (C) and SIRI (D); (E–H) comparison of overall survival in patients with different SII (E), AISI (F), PLR (G) and SIRI (H) level; (I–L) comparison of curve of disease-free survival in patients with different SII (I), AISI (J), PLR (K) and SIRI (L) level. Abbreviations: SII, systemic immune-inflammation index; AISI, aggregate index of systemic inflammation; PLR, platelet-to-lymphocyte ratio; SIRI, Systemic inflammation response index. |
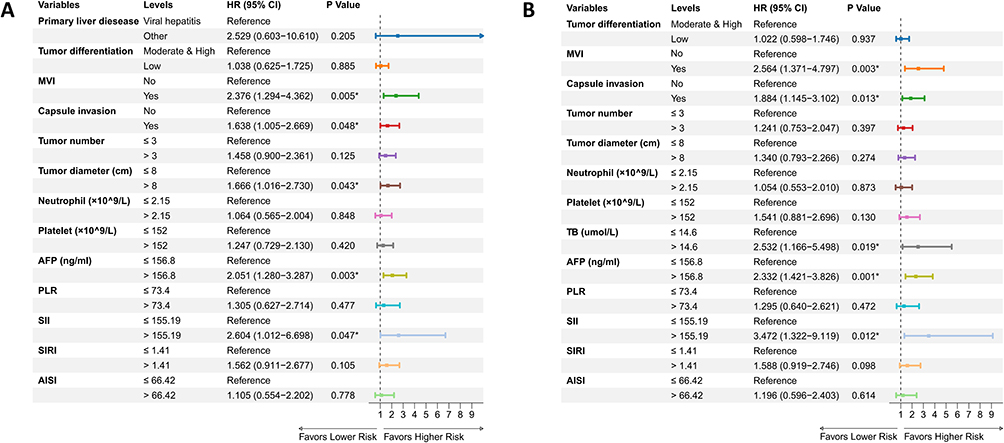 |
Figure 5 Result of multivariate analysis of independent risk factors for post-transplantation prognosis: (A) Independent risk factor for disease-free survival; (B) Independent risk factor for overall survival. * P < 0.05). Abbreviations: HR, Hazard ratio; CI, Confidence interval; MVI, Microvascular invasion; AFP, Alpha fetoprotein; TB, Total bilirubin; SII, systemic immune-inflammation index; AISI, aggregate index of systemic inflammation; PLR, platelet-to-lymphocyte ratio; SIRI, Systemic inflammation response index. |
Predictive Value of Inflammatory Indexes for Early Tumor Recurrence and Long-Term Prognosis in Different Subgroups
To further evaluate the predictive value of previously identified inflammatory indexes, we categorized patients into different subgroups according to their age, primary liver disease, liver cirrhosis, BCLC stage, preoperative treatment, Milan criteria, Hangzhou criteria and UCSF criteria and performed subgroup analysis. As shown in Figure 6A, patients with LMR ≥2.03 had significantly lower risk of early tumor recurrence in age ≤60, viral hepatitis, with and without liver cirrhosis, early BCLC stage, receiving preoperative treatment, beyond Milan, Hangzhou and UCSF criteria subgroups. Since the number of early tumor recurrence in age >60, other primary liver disease, BCLC stage C-D subgroups was less than 10, we used Firth regression to evaluate the predictive value of LMR in these subgroups (Supplementary Table 4). The odds ratio of LMR to early recurrence in age >60, other primary liver disease, BCLC stage C-D subgroups were 0.50 (95% CI: 0.11–2.42, P=0.366), 0.06 (95% CI: 0.00–1.51, P=0.088), 0.04 (95% CI: 0.00–0.37, P=0.001), respectively.
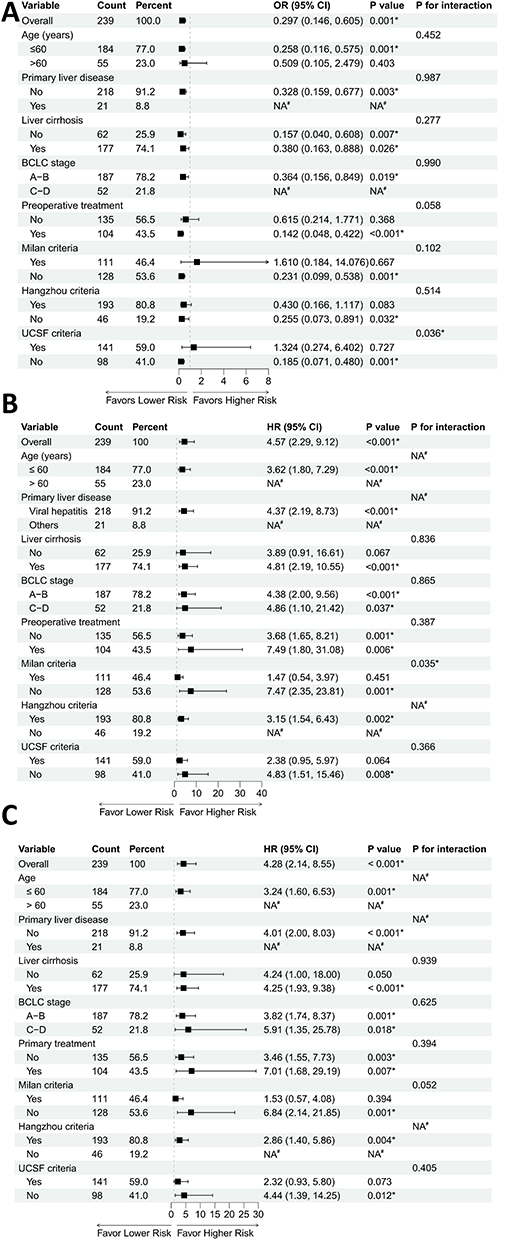 |
Figure 6 Subgroup analysis result of predictive value of LMR and SII for postoperative early recurrence and prognosis: (A) Subgroup analysis of predictive value of LMR for post-transplantation early recurrence; (B) Subgroup analysis of predictive value of SII for post-transplantation disease-free survival; (C) Subgroup analysis of predictive value of SII for post-transplantation overall survival. * P < 0.05; #: Not estimable due to zero events in one of the comparison groups. Abbreviations: BCLC, Barcelona clinic liver cancer; UCSF, University of California, San Francisco; RR, Risk ratio; HR, Hazard ratio; CI, Confidence interval; NA, Not applicable. |
Meanwhile, SII ≥155.19 was either significantly or borderline significantly correlated with worse DFS and OS in nearly all subgroups except for patients within Milan criteria, supporting the robustness of this index (Figure 6B and C). Since zero events was observed in age >60, other primary liver disease, beyond Hangzhou criteria subgroups, we used Firth regression to evaluate the predictive value of SII in these subgroups. The hazard ratio of SII to DFS in age >60, other primary liver disease, beyond Hangzhou criteria subgroups were 15.71 (95% CI: 2.12–2006.43, P=0.002), 3.00 (95% CI: 0.24–413.38, P=0.429), 13.04 (95% CI: 1.83–1654.09, P=0.004), respectively. The hazard ratio of SII to OS in age > 60, other primary liver disease, beyond Hangzhou criteria subgroups were 17.14 (95% CI: 2.32–2187.13, P=0.001), 4.09 (95% CI: 0.40–550.51, P=0.272), 12.59 (95% CI: 1.77–1596.90, P=0.005), respectively.
Prediction Model Including Inflammatory Indexes Could Better Predict Post-Transplantation Prognosis
To further improve the predictive accuracy of postoperative prognosis in HCC patients after LT, we tried to establish machine-learning prediction model using preoperative general data and laboratory examination result in the entire cohort. Continuous data was categorized into different group according to the cutoff value determined in previous section. The apparent and bootstrap-corrected C-index of RSF prediction model was the highest among all models, reaching the 0.814 and 0.754, respectively (Figure 7A). Its apparent and bootstrap-corrected AUC when predicting postoperative 12, 18, 24, 30, 36, 42, 48, 54 and 60 months were 0.913, 0.892, 0.872, 0.847, 0.835, 0.848, 0.835, 0.858, 0.854 and 0.872, 0.843, 0.812, 0.779, 0.767, 0.781, 0.765, 0.793, 0.788 (Figure 7B). The survival probability predicted by RSF model was similar to the actual survival probability in both apparent and bootstrap-corrected calibration curve, indicating the good calibration of this model (Figure 7C), while the DCA confirmed that RSF model provided significant net benefits compared to other models (Figure 7D). Therefore, we considered that RSF model was the best prediction model and visualized the variable importance using SHAP. The result showed that AFP and SII were the most important variables in established RSF model, consistent with the identified independent risk factors for post-transplantation long-term prognosis (Figure 7E).
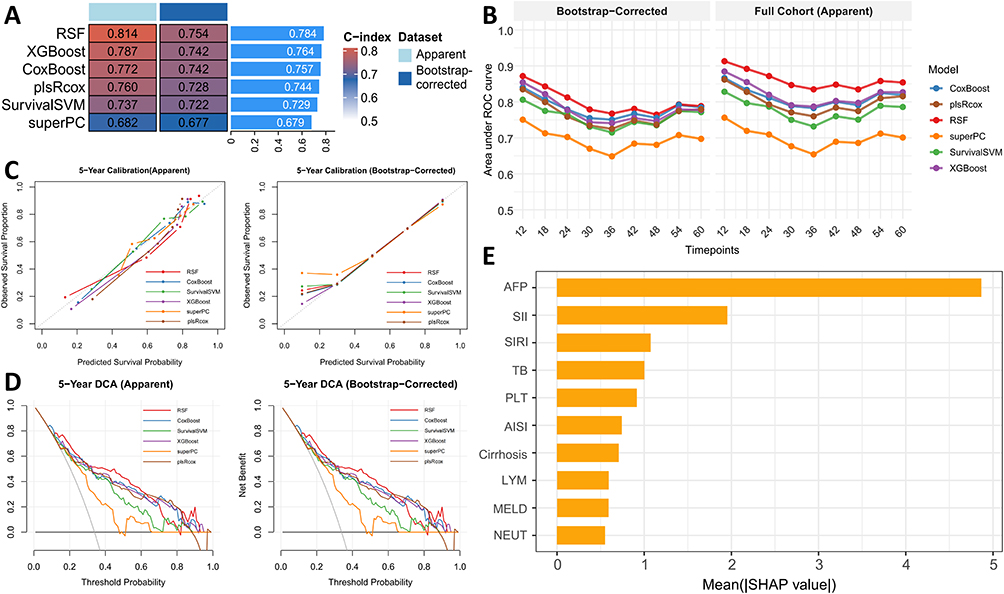 |
Figure 7 Machine-learning prediction model for post-transplantation prognosis incorporating preoperative factors: (A) Apparent and bootstrap-corrected concordance index for established prediction models; (B) Apparent and bootstrap-corrected area under receiver characteristic curve of established prediction models at different timepoints; (C) Apparent and bootstrap-corrected calibration curve of established prediction models in predicting post-transplantation 5-year survival; (D) Apparent and bootstrap-corrected decision curve analysis of established prediction models in predicting post-transplantation 5-year survival; (E) Variable importance the optimal random survival forest model visualized by Shapley additive explanation. Abbreviations: XGBoost, eXtreme gradient boosting; RSF, Random survival forest; plsRcox:Partial least squares regression for Cox models; SurvivalSVM:Survival support vector machine; SuperPC:Supervised principal components; AFP, Alpha fetoprotein; SII, systemic immune-inflammation index; MELD, Model for end-stage liver disease; SIRI, Systemic inflammation response index; TB, Total bilirubin; PLT, Platelet; NEUT, Neutrophil. |
Tumor Burden and Liver Function as Mediators Between Inflammatory Indexes and Post-Transplantation Prognosis
To better elucidate the underlying reason for the predictive ability of LMR and SII, we first compared the LMR and SII value in patients with different liver function and tumor burden. As shown in Figure 8A and B, LMR was significantly higher in patients with early tumor stage and less tumor number, while SII was significantly elevated in patients with late T stage and MVI. LMR was also confirmed to have a negative correlation with MELD score (r=−0.370) and albumin-bilirubin index (r=−0.353), which was not observed in SII (Figure 8C–F). Further mediating analysis showed that MELD score had suppression effect on the correlation between LMR and early recurrence (Figure 8G), while T stage (Figure 8H) and tumor number (Figure 8I) exerted mediating effect on the correlation between LMR and early recurrence. T stage had a significantly mediating effect on the correlation between SII and postoperative DFS (Figure 8J) and OS (Figure 8K). Albumin-bilirubin index (ALBI) had borderline significant mediating effect on correlation between LMR and early recurrence, while the mediating effect of other indexes was not significant (Figure S7). These results indicated that the liver function and tumor burden may partly explain the predictive value of LMR and SII for postoperative early recurrence and prognosis.
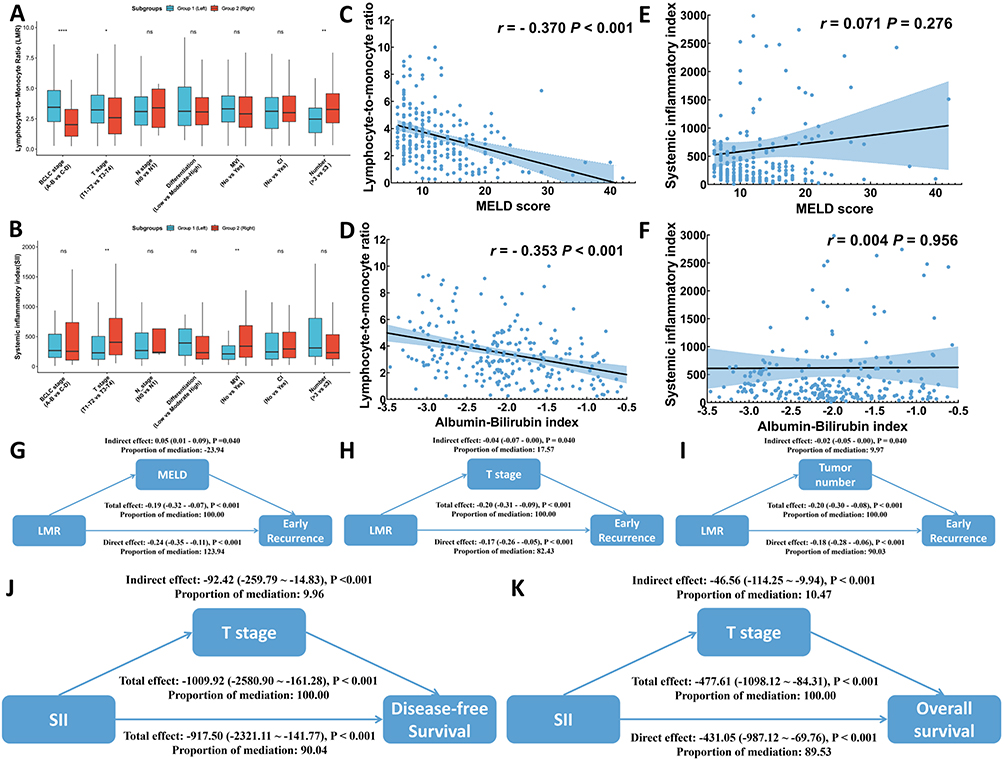 |
Figure 8 Impact of liver function and tumor burden on inflammatory index and post-transplantation prognosis: (A and B) Comparison of lymphocyte-to-monocyte ratio (A) and systemic immune-inflammation index (B) between different subgroups with different tumor burden; (C and D) Correlation between lymphocyte-to-monocyte ratio and liver function including model for end-stage liver disease score (C) and albumin-bilirubin index (D); (E and F) Correlation between systemic immune-inflammation index and liver function including model for end-stage liver disease score (E) and albumin-bilirubin index (F); (G and I) Mediating effect of model for end-stage liver disease score (G), T stage (H) and tumor number (I) between lymphocyte-to-monocyte ratio and early recurrence; (J and K) Mediating effect of T stage between systemic immune-inflammation and post-transplantation disease-free survival (J) and overall survival (K). ns P > 0.05; * P < 0.05; ** P < 0.01; **** P < 0.0001). Abbreviations: BCLC, Barcelona clinic liver cancer; MVI, Microvascular invasion; CI, Capsule invasion; MELD, Model for end-stage liver disease; LMR, Lymphocyte-to-monocyte ratio; SII, Systemic immune-inflammation index. |
Discussion
Current retrospective study of 239 HCC patients undergoing LT systematically evaluated the prognostic value of preoperative inflammatory indexes. We found that the low LMR was associated with early tumor recurrence, while the elevated SII served as an independent risk factor for long-term prognosis after LT. Furthermore, we also established a RSF machine-learning model incorporating SII, AFP and other preoperative clinical variables which demonstrated the highest predictive accuracy and clinical benefit compared to other models. These findings are of certain clinical valuable as they provide a non-invasive, accessible stratification tool to identify high-risk patients and tailor personalized post-transplantation surveillance and management strategies.
Since not all HCC patients receiving LT have satisfying outcomes, clinicians have kept working on identifying the risk factors for poor post-transplantation prognosis so as to enable better stratification of suitable recipients. Since blood-derived inflammatory indexes had special advantages over other indexes due to its easy accessibility and cost-effectiveness, researchers have focused on exploring their prognostic value for post-transplantation prognosis in HCC and reported markers including NLR, derived NLR, PLR as effective markers to predict post-LT survival, demonstrating the clinical utility of these indexes.18–20 But their predictive value was less compared in researches, limiting their clinical application. In our research, we identified LMR as an effective index for predicting early recurrence and SII served as an independent risk factor for long-term prognosis, offering a theoretical basis for the clinical selection of inflammatory markers. For LMR, Mano et al found that LMR > 2.75 was significantly correlated with nearly 30% improved 5-year survival compared to the control group in a living donor LT cohort.9 Ismael et al further extended the prognostic value of LMR to all HCC patients and proposed a cutoff value of 3.45.18 In line with previous studies, our results showed that elevated LMR was a protective factor against early recurrence, further broadened the clinical value of LMR to the prediction of early recurrence. In terms of SII, it was also an effective predictive marker for HCC prognosis but less evaluated in HCC patients after LT.21 Fu et al observed a significant survival benefits in SII <226 HCC patients within Hangzhou criteria, while Zhang et al reported the prognostic value of SII for DFS in all HCC patients after LT, which were consistent with our findings in current research.22,23 Moreover, our research also demonstrated that SII had significant predictive value for both OS and DFS in HCC patients beyond Hangzhou criteria, extending the utility of SII in clinical practice. However, although all researches have verified that low LMR and high SII are correlated with poor post-LT prognosis, the specific cutoff value varies in predicting different clinical outcomes. Clinicians should apply cutoff values flexibly to fulfill different clinical demands.
As for the reason for the predictive value of inflammatory index for postoperative outcome, we attributed it to their ability to reflect both tumor burden and local tumor micro-environment. Current researchers believed that the systemic inflammation response is driven by tumor through various pathway, therefore inflammatory index can reflect tumor burden directly.24 According to researches, elevated NLR was significantly correlated with aggressive pathological features including larger tumor stage, high histological grade and vascular invasion.25 Besides, it was also reported that increasing circulating platelet count also reflected larger tumor size in HCC patients.26 Therefore, increased SII, which constituted of both NLR and platelet, may also reflect a more aggressive disease status. Our findings aligned with this hypothesis, demonstrating that elevated SII was significantly associated with advanced T stage and the presence of MVI. Our mediating analysis further confirmed that T stage significantly mediates the correlation between SII and post-transplantation OS and DFS, supporting that the predictive value of SII may be correlated with advanced tumor stage. Besides, previous research also reported the potential correlation between systemic inflammatory indexes and local tumor micro-environment. For instance, Mano et al reported that HCC patients with lower LMR had decreased CD3+/CD68+ cell ratio.9 Ha et al found that HCC patients with NLR ≥2.5 had significantly decreased local T cell infiltration.27 These results further demonstrated that abnormal systemic inflammatory indexes may also reflect a suppressive and pro-tumor micro-environment, which may also explain their predictive value for post-LT outcomes.
According to previous researches, liver dysfunction was correlated with higher level of inflammatory indexes in LT patients and could impact both short-term and long-term prognosis.28–30 Therefore, we hypothesized that poor liver function in different LMR and SII groups may partly explain their predictive value and further evaluated their correlation with both MELD and ALBI which were reported as effective biomarker for liver function.31 A interesting finding of our study is the paradoxical relationship where better preoperative liver function may correlate with a higher tendency for early postoperative recurrence, as evidenced by the suppression effect of the MELD score and ALBI score on the correlation between LMR and early recurrence. In previous researches, HCC patients with poor preoperative liver function suffered tumor recurrence earlier than others, inconsistent with our finding.32 We thought that this phenomenon can potentially be explained by both tumor biology and organ allocation dynamics. According to Sasaki et al, residual tumor and micro-metastasis were the main reason for tumor recurrence in HCC patients without liver cirrhosis.33 Biologically, liver with less fibrosis provides a highly vascularized and nutrient-rich environment that may paradoxically support rapid tumor proliferation and the establishment of micro-metastasis before LT. Clinically, patients with better liver function tended to have longer times on waiting list unless prioritized by HCC exception points. This prolonged waiting period also provides a time window for HCC to disseminate prior to transplantation, thereby increasing the risk of early post-transplant recurrence. As for the reason for the inconsistency between our research and Blüthner’s research, they evaluated the predictive effect of liver function in HCC patients after liver resection instead of LT. In these patients, poor liver function was usually a sign of liver cirrhosis which was known as the important risk factor for the occurrence and recurrence of HCC, significantly increasing the risk of de novo recurrence. However, LT removes the entire liver and eliminates the primary source of de novo recurrence, thereby attenuating the impact of preoperative liver function on post-transplant tumor recurrence.
Moreover, we also identified AFP and a series of pathological indexes including MVI, capsule invasion, tumor diameter as independent risk factor for early recurrence and long-term prognosis. These findings were similar to previous researches, further demonstrating their prognostic value in HCC.34–37
Current study is also subject to several limitations. First, as a study conducted at a single center and included patients in a 10-year period, selection and chronological biases were unavoidable. Second, as a single-center retrospective study, the lack of external validation limits the generalizability of our proposed prediction model, representing an important limitation of this study. Future multi-center prospective research is necessary to further validate the clinical utility and promotional value of our proposed model. Third, the cutoff values of SII and LMR were determined using data-driven methods, which may lead to overfitting and significant variability across different cohorts. Independent, multicenter external validation is necessary to fully verify the clinical implication of these proposed cutoff value. Fourth, since the detailed preoperative treatment data was incomplete, we failed to adjust for potential confounding effects of caused by heterogeneity in preoperative therapies. Fifth, although the mediating effect of tumor burden and liver function was statistically significant, their proportion of mediation was rather limited, indicating that there may be other potential factors contributing to the predictive value of inflammatory indexes. Further researches are necessary to fully elucidate these issues. Finally, whether systemic inflammatory indexes could reflect and influence the characteristic of local micro-environment remained unknown since the resected tumor tissue of our cohort was not available currently. The exact molecular cross-talk between peripheral inflammatory cells and the hepatic tumor micro-environment was also unexplored in current study. Future prospective investigations are warranted to verify this hypothesis and elucidate these underlying molecular mechanisms.
Conclusion
Inflammatory indexes were significantly different among patients with different post-transplantation prognosis in HCC patients. Among these indexes, LMR ≥ 2.03 was associated with early HCC recurrence while SII ≥ 155.19 was correlated with poor post-transplantation DFS and OS. Their predictive value for postoperative outcomes may be partly mediated or suppressed by tumor burden and liver function. A machine-learning model incorporating inflammatory indexes with preoperative variables showed promising predictive performance in our cohort. These indexes and proposed prediction model may serve as potential complementary tools to conventional prognostic markers and criteria and aid early risk stratification and clinical decision making in the future after being further validated in prospective and multi-center studies.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
The acquisition of clinical data complied with the Declaration of Helsinki and was approved by the Ethics Committee of Beijing Chao-Yang Hospital (No.2020-D.-303). Participant informed consent was exempted due to the retrospective study design, and the study design was approved by the appropriate ethics review board.
Author Contributions
Han-xuan Wang: Conceptualization, Methodology, Formal analysis, Visualization, Writing-original draft; Xiao-yong Ye: Methodology, Investigation, Data curation, Formal analysis, Writing-original draft; Tao Jiang: Investigation, Resource, Writing-review&editing; Shao-cheng Lyu: Investigation, Resource, Writing-review&editing; Qiang He: Investigation, Resource, Writing-review&editing; Zhi-li Ji: Resource, Supervision, Writing-review&editing; Ren Lang: Conceptualization, Resource, Supervision, Project administration, Writing-review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
The authors declare that no funding was received for this study.
Disclosure
The authors have nothing to disclose.
References
1. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Nation Cancer Center. 2024;4:47–20. doi:10.1016/j.jncc.2024.01.006
2. Zhang C, Cheng Y, Zhang S, Fan J, Gao Q. Changing epidemiology of hepatocellular carcinoma in Asia. Liver in. 2022;42:2029–2041. doi:10.1111/liv.15251
3. Kim B, Kahn J, Terrault NA. Liver transplantation as therapy for hepatocellular carcinoma. Liver in. 2020;40(Suppl 1):116–121. doi:10.1111/liv.14346
4. Qu Z, Ling Q, Gwiasda J, et al. Hangzhou criteria are more accurate than Milan criteria in predicting long-term survival after liver transplantation for HCC in Germany. Langenbecks Arch Surg. 2018;403:643–654. doi:10.1007/s00423-018-1696-8
5. De’Angelis N, Landi F, Carra MC, Azoulay D. Managements of recurrent hepatocellular carcinoma after liver transplantation: a systematic review. World J Gastroenterol. 2015;21:11185–11198. doi:10.3748/wjg.v21.i39.11185
6. Parraga X, Abdulrazzak E, Chumdermpadetsuk RR, et al. Hepatocellular carcinoma recurrence after liver transplantation: current insights and future directions. J Clin Med. 2025;14:7009. doi:10.3390/jcm14197009
7. Aguilar-Cazares D, Chavez-Dominguez R, Marroquin-Muci OM, et al. The systemic-level repercussions of cancer-associated inflammation mediators produced in the tumor microenvironment. Front Endocrinol. 2022;13:929572 doi:10.3389/fendo.2022.929572.
8. Haruki K, Taniai T, Yanagaki M, et al. Sustained systemic inflammatory response predicts survival in patients with hepatocellular carcinoma after hepatic resection. Ann Surg Oncol. 2023;30:604–613. doi:10.1245/s10434-022-12464-6
9. Mano Y, Yoshizumi T, Yugawa K, et al. Lymphocyte-to-monocyte ratio is a predictor of survival after liver transplantation for hepatocellular carcinoma. Liver Transplantation. 2018;24:1603–1611. doi:10.1002/lt.25204
10. Peng J, Chen H, Chen Z, Tan J, Wu F, Li X. Prognostic value of neutrophil-to-lymphocyte ratio in patients with hepatocellular carcinoma receiving curative therapies: a systematic review and meta-analysis. Bmc Cancer. 2025;25:571. doi:10.1186/s12885-025-13972-w
11. Xia W, Ke Q, Wang Y, et al. Predictive value of pre-transplant platelet to lymphocyte ratio for hepatocellular carcinoma recurrence after liver transplantation. World J Surg Oncol. 2015;13:60. doi:10.1186/s12957-015-0472-2
12. Benchimol EI, Smeeth L, Guttmann A. RECORD WC: the reporting of studies conducted using observational routinely-collected health data (RECORD) statement. Plos Med. 2015;12:e1001885. doi:10.1371/journal.pmed.1001885
13. Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. doi:10.1053/jhep.2001.22172
14. Ijtsma AJC, van der Hilst CS, de Boer MT, et al. The clinical relevance of the anhepatic phase during liver transplantation. Liver Transplantation. 2009;15:1050–1055. doi:10.1002/lt.21791
15. Zheng Z, Guan R, Jianxi W, et al. Microvascular invasion in hepatocellular carcinoma: a review of its definition, clinical significance, and comprehensive management. J Oncol. 2022;2022:9567041. doi:10.1155/2022/9567041
16. Iguchi T, Aishima S, Taketomi A, et al. Extracapsular penetration is a new prognostic factor in human hepatocellular carcinoma. Am J Surg Pathol. 2008;32:1675–1682. doi:10.1097/PAS.0b013e31817a8ed5
17. Sapisochin G, Bruix J. Liver transplantation for hepatocellular carcinoma: outcomes and novel surgical approaches. Nat Rev Gastroenterol Hepatol. 2017;14:203–217 doi:10.1038/nrgastro.2016.193.
18. Ismael MN, Forde J, Milla E, Khan W, Cabrera R. Utility of inflammatory markers in predicting hepatocellular carcinoma survival after liver transplantation. Biomed Res Int. 2019;2019:7284040. doi:10.1155/2019/7284040
19. Xiao G, Liu C, Liu D, Yang J, Yan L. Neutrophil-lymphocyte ratio predicts the prognosis of patients with hepatocellular carcinoma after liver transplantation. World J Gastroenterol. 2013;19:8398–8407. doi:10.3748/wjg.v19.i45.8398
20. Cui S, Cao S, Chen Q, He Q, Lang R. Preoperative systemic inflammatory response index predicts the prognosis of patients with hepatocellular carcinoma after liver transplantation. Front Immunol. 2023;14:1118053. doi:10.3389/fimmu.2023.1118053
21. Hu B, Yang X, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20:6212–6222. doi:10.1158/1078-0432.CCR-14-0442
22. Fu H, Zheng J, Cai J, et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients after liver transplantation for hepatocellular carcinoma within hangzhou criteria. Cellular Physiol Biochem. 2018;47:293–301. doi:10.1159/000489807
23. Zhang W, Bi Y, Yang K, et al. A new model based on gamma-glutamyl transpeptidase to lymphocyte ratio and systemic immune-inflammation index can effectively predict the recurrence of hepatocellular carcinoma after liver transplantation. Front Oncol. 2023;13:1178123. doi:10.3389/fonc.2023.1178123
24. Sanghera C, Teh JJ, Pinato DJ. The systemic inflammatory response as a source of biomarkers and therapeutic targets in hepatocellular carcinoma. Liver in. 2019;39:2008–2023. doi:10.1111/liv.14220
25. Hung H, Lee J, Cheng C, et al. Impact of neutrophil to lymphocyte ratio on survival for hepatocellular carcinoma after curative resection. J Hepato-Bil-Pan Sci. 2017;24:559–569 doi:10.1002/jhbp.498.
26. Carr BI, Lin C, Lu S. Platelet-related phenotypic patterns in hepatocellular carcinoma patients. Semin Oncol. 2014;41:415–421. doi:10.1053/j.seminoncol.2014.04.001
27. Ha SY, Choi S, Park S, et al. Prognostic effect of preoperative neutrophil-lymphocyte ratio is related with tumor necrosis and tumor-infiltrating lymphocytes in hepatocellular carcinoma. Virchows Archiv. 2020;477:807–816. doi:10.1007/s00428-020-02841-5
28. Klein KB, Stafinski TD, Menon D. Predicting survival after liver transplantation based on pre-transplant MELD score: a systematic review of the literature. PLoS One. 2013;8:e80661. doi:10.1371/journal.pone.0080661
29. Kwon H, Moon Y, Jung K, et al. Neutrophil-to-lymphocyte ratio is a predictor of early graft dysfunction following living donor liver transplantation. Liver in. 2019;39:1545–1556. doi:10.1111/liv.14103
30. Morales-Arráez D, Ventura-Cots M, Altamirano J, et al. The MELD score is superior to the maddrey discriminant function score to predict short-term mortality in alcohol-associated hepatitis: a global study. Am J Gastroenterol. 2022;117:301–310. doi:10.14309/ajg.0000000000001596
31. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J clin Oncol. 2015;33:550–558. doi:10.1200/JCO.2014.57.9151
32. Blüthner E, Bednarsch J, Malinowski M, et al. Dynamic liver function is an independent predictor of recurrence-free survival after curative liver resection for HCC - A retrospective cohort study. Int J Surg. 2019;71:56–65. doi:10.1016/j.ijsu.2019.08.033
33. Sasaki K, Shindoh J, Margonis GA, et al. Effect of background liver cirrhosis on outcomes of hepatectomy for hepatocellular carcinoma. JAMA Surg. 2017;152:e165059. doi:10.1001/jamasurg.2016.5059
34. Zhang Z, Jiang C, Qiang Z, et al. Role of microvascular invasion in early recurrence of hepatocellular carcinoma after liver resection: a literature review. Asian J Surg. 2024;47:2138–2143. doi:10.1016/j.asjsur.2024.02.115
35. Wang H, Wu M, Cong W. Microvascular invasion predicts a poor prognosis of solitary hepatocellular carcinoma up to 2cm based on propensity score matching analysis. Hepatol Res. 2019;49:344–354. doi:10.1111/hepr.13241
36. Xu L, Li L, Wang P, et al. Novel prognostic nomograms for hepatocellular carcinoma patients with microvascular invasion: experience from a single center. Gut Liver. 2019;13:669–682. doi:10.5009/gnl18489
37. He L, Ji W, Jin H, et al. Development of a nomogram for predicting liver transplantation prognosis in hepatocellular carcinoma. World J Gastroenterol. 2024;30:2763–2776. doi:10.3748/wjg.v30.i21.2763
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Decaprenyl Diphosphate Synthase Subunit 1 (PDSS1): A Potential Prognostic Biomarker and Immunotherapy-Target for Hepatocellular Carcinoma
Yang Y, Li J, Tang M, Nie B, Huang W
Cancer Management and Research 2022, 14:1627-1639
Published Date: 3 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Low MARCO Expression is Associated with Poor Survival in Patients with Hepatocellular Carcinoma Following Liver Transplantation
Zhang Q, Wei Y, Li Y, Jiao X
Cancer Management and Research 2022, 14:1935-1944
Published Date: 11 June 2022
The Fibrinogen-to-Albumin Ratio (FAR) Predicts Prognosis in Hepatocellular Carcinoma Patients After Liver Transplantation: Development and Validation of a Novel Nomogram
Ye XY, Leng AX, He Q, Ji Z, Ma J
Journal of Hepatocellular Carcinoma 2026, 13:588619
Published Date: 8 April 2026
Prognostic Impact of the Systemic Immune-Inflammation Index in Unresectable Hepatocellular Carcinoma Undergoing Second-Line Combination Therapy: A Multicenter Study
Chen X, Li X, Jiang Y, Xie Q, Zhang P, Zhou X, Wei C, Xie P, Cao L
Cancer Management and Research 2026, 18:613658
Published Date: 3 June 2026