Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Clinical Outcomes and Treatment-Related Complications in Triple-Negative Breast Cancer: A Review of 24 Case Reports from 2020 to 2025
Authors Febriyanti RM ![]() , Hakim MLN
, Hakim MLN ![]() , Rofiidatul I, Islami MS, Utami PS, Qurrotuaini SP
, Rofiidatul I, Islami MS, Utami PS, Qurrotuaini SP ![]() , Halimah E
, Halimah E ![]() , Mohd Hashim N
, Mohd Hashim N ![]() , Diantini A
, Diantini A ![]()
Received 25 April 2026
Accepted for publication 19 June 2026
Published 30 June 2026 Volume 2026:22 619823
DOI https://doi.org/10.2147/TCRM.S619823
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandeep Ajoy Saha
Raden Maya Febriyanti,1 Muhammad Lukman Nur Hakim,2 Itsna Rofiidatul,2 Maura Syafa Islami,2 Putri Sagita Utami,2 Salwa Putri Qurrotuaini,2 Eli Halimah,3 Najihah Mohd Hashim,4 Ajeng Diantini3
1Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Master of Pharmacy Study Program, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 4Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Universiti Malaya, Kuala Lumpur, Malaysia
Correspondence: Raden Maya Febriyanti, Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Ir. Soekarno KM 21, Sumedang, West Java, 45363, Indonesia, Email [email protected]; Ajeng Diantini, Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Ir. Soekarno KM 21, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Abstract: Triple-negative breast cancer (TNBC) is clinically heterogeneous, and selected patients experience rare complications, unusual responses, or biomarker-discordant treatment trajectories that are not fully represented in aggregate trial evidence. This review aims to synthesize published case-report evidence on clinical outcomes and treatment-related complications in TNBC, with an emphasis on host vulnerability, tumor biology, biomarker-guided treatment, and therapy-associated toxicity. A descriptive review of PubMed-indexed case reports was performed for records published from January 1, 2020, to December 31, 2025. Two reviewers independently screened records, extracted data, and appraised the reporting quality using the CARE domains. Results were synthesized narratively without meta-analysis. Seventy-one records were screened, and 24 case reports were included. All patients were female, with a median age of 45 years (range 28– 87 years). The cases consisted of 11 with metastatic or advanced disease, 10 with early or localized disease, 1 with a local recurrence, and 2 with unclear disease settings. Actionable or resistance-informative biomarker signals were described in 12 cases, and biomarker-matched therapy was reported in 11. Immunotherapy was used in 9 cases. Serious or clinically significant complications were reported in 10 cases, including two fatal treatment-related events. Favorable outcomes were reported in 17 cases, but these selected reports cannot be used to estimate response rates, survival, or the incidence of toxicity. TNBC case reports provide clinically instructive, hypothesis-generating evidence on rare toxicities, biomarker-guided treatment decisions, and individualized risk assessment.
Keywords: triple-negative breast cancer, case reports, treatment-related complications, immune checkpoint inhibitors, immune-related adverse events
Introduction
Triple-negative breast cancer (TNBC) is an aggressive breast cancer subtype defined by the absence of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 (HER2) expression.1–4 Because TNBC lacks the endocrine and HER2-directed therapeutic targets used in other breast cancer subtypes, systemic treatment has historically relied on cytotoxic chemotherapy.5,6 Despite therapeutic advances, TNBC remains clinically challenging because of its early relapse pattern, high metastatic potential, frequent visceral dissemination, and poorer prognosis in advanced disease.4,7,8
TNBC accounts for approximately 10–20% of breast cancer cases worldwide, although reported prevalence varies across populations and regions.9–11 Higher proportions have been reported in cohorts from India, Latin America, East Africa, and Barbados, suggesting that genetic ancestry, reproductive factors, health-care access, socioeconomic determinants, and regional diagnostic patterns may influence the observed disease burden.12–15 At the genomic level, TNBC is frequently associated with alterations in DNA damage response pathways and tumor suppressor genes, particularly BRCA1/2 and TP53, which contribute to genomic instability, therapeutic vulnerability, and the evolution of resistance.16–18
Beyond its receptor-negative definition, TNBC is biologically heterogeneous rather than a single uniform disease entity. Molecular classifications include luminal androgen receptor, immunomodulatory, basal-like immunosuppressed, and mesenchymal subtypes, each with distinct pathway dependencies, immune phenotypes, and treatment sensitivities.19,20 TNBC also encompasses rare histological variants, including metaplastic breast carcinoma, adenoid cystic carcinoma, apocrine carcinoma, secretory carcinoma, neuroendocrine carcinoma, and rare lobular phenotypes, whose biological behavior may not be fully predicted by receptor status alone.21,22 Among these, metaplastic breast carcinoma is clinically important because it is commonly triple-negative, morphologically heterogeneous, and frequently less responsive to conventional cytotoxic chemotherapy than non-metaplastic TNBC.23–25 Molecular studies have shown that metaplastic breast carcinoma is enriched for alterations involving PI3K/AKT signaling, epithelial–mesenchymal transition, stemness-associated programs, and Wnt/β-catenin pathway dysregulation, all of which may contribute to intrinsic chemoresistance and aggressive clinical behavior.23,26 This molecular and histological diversity helps explain why standardized treatment approaches may produce markedly different outcomes among patients with the same triple-negative receptor profile.21
The treatment paradigm for TNBC has therefore shifted from reliance on cytotoxic chemotherapy alone to multimodal, biomarker-guided strategies. Anthracyclines, taxanes, and platinum-based regimens remain important components of neoadjuvant, adjuvant, and metastatic treatment. However, early resistance and relapse continue to limit durable disease control in a subset of patients.27–31 More recent therapeutic approaches include poly(ADP-ribose) polymerase inhibitors for selected patients with BRCA1/2 alterations and immune checkpoint inhibitors for selected clinical and biomarker-defined settings.32–34 Although these approaches have expanded therapeutic options, treatment response remains heterogeneous, and intensified regimens may introduce clinically significant toxicity requiring individualized risk assessment.
Large clinical trials are essential for defining population-level efficacy and common safety profiles. Still, they may not fully capture rare, high-severity complications, unusual metastatic presentations, complex comorbidity-related risks, diagnostic mimics of progression, or exceptional responses to biomarker-guided therapy.35–38 Published case reports provide complementary evidence by documenting granular clinical trajectories that are often under-represented in aggregate trial data. In TNBC, such case-level evidence is particularly relevant when reports describe rare immune-related adverse events, severe treatment-limiting complications, or outcomes shaped by uncommon genetic and clinical vulnerabilities. Examples include atezolizumab-associated posterior reversible encephalopathy syndrome and fatal therapy-related myelodysplastic syndrome in a patient with Bloom syndrome.39,40
Accordingly, this review focuses on published case reports of TNBC therapy rather than estimating population-level treatment efficacy or adverse event incidence. The objective was to synthesize case-level evidence on clinical outcomes and treatment-related complications in TNBC, with emphasis on three clinically relevant domains: patient-specific vulnerabilities, tumor histology and molecular biomarkers, and therapy-associated toxicities. By analyzing 24 published case reports from 2020 to 2025, this review aims to clarify how individualized interactions among host factors, tumor heterogeneity, biomarker-guided treatment selection, and complication management may shape TNBC outcomes. The intended contribution is to identify clinically instructive patterns and hypothesis-generating signals that may support individualized risk assessment, toxicity surveillance, and multidisciplinary treatment planning.
Materials and Methods
Study Design
A PRISMA-informed descriptive review of PubMed-indexed case reports was conducted to synthesize published case-level evidence on clinical outcomes and treatment-related complications in TNBC.41 The review was designed as a descriptive case-report synthesis rather than a comparative effectiveness review or meta-analysis. This approach was selected because eligible reports described heterogeneous individual patients, disease stages, therapeutic regimens, biomarker profiles, follow-up durations, and adverse-event reporting formats. No pooled estimate of treatment efficacy, toxicity incidence, or comparative treatment effect was planned. Frequencies and percentages were used only to summarize patterns within the included published case reports. The protocol was not prospectively registered.
Search Strategy and Data Sources
A formal literature search was performed in PubMed because this database provides structured biomedical indexing through Medical Subject Headings (MeSH), publication-type filters, and broad coverage of peer-reviewed clinical case reports. The final search was documented on January 31, 2026, with publication-date limits from January 1, 2020, to December 31, 2025. The PubMed search strategy was: Triple Negative Breast Neoplasms/therapy [MeSH] AND “Case Reports”[Publication Type].
The MeSH term “Triple Negative Breast Neoplasms/therapy” was selected to retrieve records indexed for therapeutic management of TNBC. At the same time, the “Case Reports” [Publication Type] restriction limited the search to individual clinical reports. Additional eligibility restrictions were applied during screening rather than as database search terms. These included English-language publication, full-text availability, confirmed TNBC phenotype, and extractable information on treatment, outcome, and treatment-related toxicity or complications. The search was intentionally focused on clinically detailed case reports rather than all TNBC therapeutic publications. No restrictions were applied by country, patient age, disease stage, metastatic status, treatment setting, or therapeutic modality. Grey literature, conference abstracts, preprints, and non-indexed reports were not included. Reference lists of eligible reports and relevant review articles were screened for additional case reports. No additional eligible records were added.
Study Selection and Screening Process
All records identified through PubMed were screened using a standardized PRISMA 2020-informed workflow.41 After duplicate removal, titles and abstracts were screened independently by two reviewers (AD and RMF). Records judged potentially eligible by either reviewer were retrieved for full-text assessment. Full-text eligibility assessment was also performed independently by the same two reviewers. Disagreements regarding study inclusion or exclusion, or data interpretability, were resolved through discussion and, when needed, arbitration by a third reviewer (EH).
The database search identified 71 records. No duplicates were identified, and all 71 records underwent title and abstract screening. Forty-seven records were excluded during screening because they were review articles, cross-sectional or observational studies, focused on cancer types other than breast cancer or non-TNBC breast cancer, lacked extractable patient-level data, or described cancer treatment without relevant chemotherapy or systemic anticancer therapy. Twenty-four reports were retrieved and assessed for full-text eligibility. All 24 reports met the final eligibility criteria and were included in the descriptive synthesis (Figure 1).
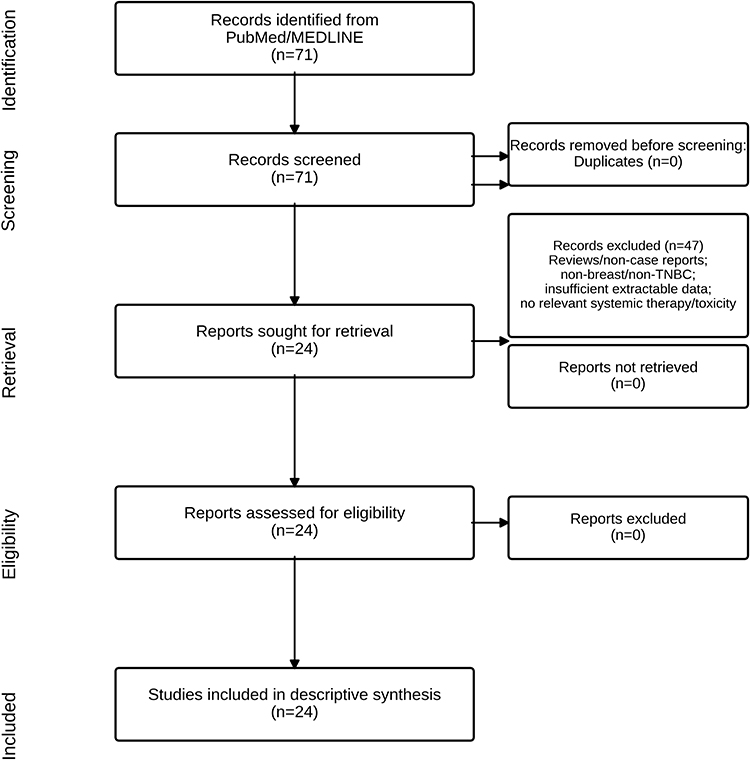 |
Figure 1 PRISMA 2020 flow diagram of study identification, screening, eligibility assessment, and final inclusion of 24 TNBC case reports. |
Eligibility Criteria
Studies were eligible for inclusion if they met all of the following criteria: peer-reviewed case report, English-language publication, publication date between 2020 and 2025, full-text availability, individual patient-level data, primary diagnosis of breast cancer with a triple-negative phenotype, and confirmation of TNBC by immunohistochemistry, defined by absence of estrogen receptor, progesterone receptor, and HER2 expression or HER2 amplification according to the criteria reported in the source article. Eligible reports were also required to describe at least one therapeutic intervention and provide extractable information on clinical outcome, treatment response, disease progression, survival status, treatment-related toxicity, or clinically relevant complications. Reports that included synchronous malignancies or complex comorbidities were retained only when TNBC-specific treatment, outcome, and complication data could be separately extracted.
Data Extraction and Operational Definitions
Data extraction was performed independently by two reviewers (AD and RMF) using a standardized extraction form. Extracted variables included author and year of publication, patient age and sex, disease stage, TNM classification when reported, metastatic sites, histological subtype, baseline receptor status, Ki-67 index, PD-L1 status, BRCA1/2 status, next-generation sequencing results, tumor mutational burden, homologous recombination deficiency markers, circulating tumor DNA or disseminated tumor cell findings, and other clinically relevant biomarkers. Host-related variables included comorbidities, viral carriage, hereditary cancer syndromes, pregnancy status, baseline organ dysfunction, and other patient-specific vulnerabilities that could influence treatment selection or toxicity risk.
Therapeutic data included treatment setting, treatment sequence, surgery, radiotherapy, chemotherapy, immunotherapy, targeted therapy, endocrine or androgen-directed therapy, where relevant, drug names, doses, number of cycles, duration, dose modifications, discontinuation, and subsequent treatment lines, when reported. Clinical outcome variables included complete response, partial response, stable disease, progressive disease, pathological complete response, near-pCR or major pathological response, no evidence of disease, disease-free status, recurrence, survival status, death, and duration of follow-up. Response categories were coded according to the definitions used by the original case-report authors. Treatment-related complications were extracted as reported by the original authors. They included hematologic toxicity, immune-related adverse events, hepatic toxicity, neurologic complications, infectious complications, treatment intolerance, therapy-related secondary malignancy, severe organ dysfunction, treatment discontinuation, hospitalization, and fatal adverse events. Missing or unreported variables were coded as “not reported” and were not imputed.
For descriptive synthesis, disease setting was categorized as early/localized, locally advanced, recurrent, metastatic/advanced, or unclear based on the source report. Outcomes were grouped descriptively as favorable, death/failure, or ongoing/unclear. Favorable outcomes included complete response, pathological complete response, near-pCR or major pathological response, no evidence of disease, disease-free follow-up, or documented partial response/stable disease with clinically meaningful disease control. Death/failure included death attributed to disease progression or treatment-related toxicity, clear progressive disease, hyperprogressive disease, or absence of oncologic benefit. Ongoing/unclear outcomes were assigned when follow-up was insufficient to classify the final clinical trajectory.
Quality Appraisal and Bias Evaluation
The reporting quality of the included case reports was appraised using the CARE guideline framework.42 The appraisal focused on whether each report clearly described the case-report title and keywords, abstract or case uniqueness, patient information, diagnostic assessment, therapeutic intervention, follow-up and outcomes, adverse events, strengths or limitations, and take-away lessons.
Two reviewers independently assessed each report using a standardized CARE compliance matrix (MLNH and IR). Each domain was classified as “Yes” when the relevant information was adequately reported, “Partial” when the information was present but incomplete, and “NR” when the domain was not reported or could not be clearly identified. Disagreements were resolved through discussion, and a third reviewer adjudicated any remaining discrepancies. The CARE compliance matrix is provided as Supplementary Table S1.
Because case reports are inherently susceptible to selective publication, incomplete follow-up, non-standardized outcome assessment, and limited causal attribution, the appraisal was interpreted qualitatively. Attention was given to whether treatment-related complications were explicitly described, whether adverse events were graded or clinically contextualized, and whether the authors acknowledged case-specific limitations. Reports lacking formal toxicity grading or explicit limitations were retained when they provided sufficient patient-level clinical, diagnostic, therapeutic, and outcome data for descriptive synthesis. The appraisal was used to contextualize the strength and interpretability of case-level evidence, not to generate pooled estimates of treatment efficacy or toxicity incidence.
Data Synthesis
A descriptive narrative synthesis was performed due to substantial heterogeneity in patient characteristics, TNBC subtype, disease stage, biomarker profiles, treatment regimens, adverse event reporting, and follow-up duration. Extracted data were summarized in tables to compare baseline clinical characteristics, tumor biology, treatment sequence, response assessment, toxicity profile, and key biomarkers across the included cases. Counts and percentages were calculated only to characterize the 24 included reports. These values should not be interpreted as population-level incidence, prevalence, comparative efficacy, or real-world toxicity risk. The synthesis focused on clinically instructive patterns involving host vulnerability, tumor heterogeneity, biomarker-guided treatment selection, therapeutic response, and treatment-related complications.
Results
A total of 24 case reports met the eligibility criteria and were included in the final descriptive synthesis (Table 1). All reported patients were female, with a median age of 45 years (mean 49.3 years; range, 28–87 years). In terms of disease setting, 11 cases (45.8%) were classified as metastatic or advanced disease, 10 cases (41.7%) as early or localized disease, one case (4.2%) as local recurrence, and two cases (8.3%) as unclear disease setting. These counts describe the composition of the included published case reports only and should not be interpreted as population-level frequencies of TNBC presentation.
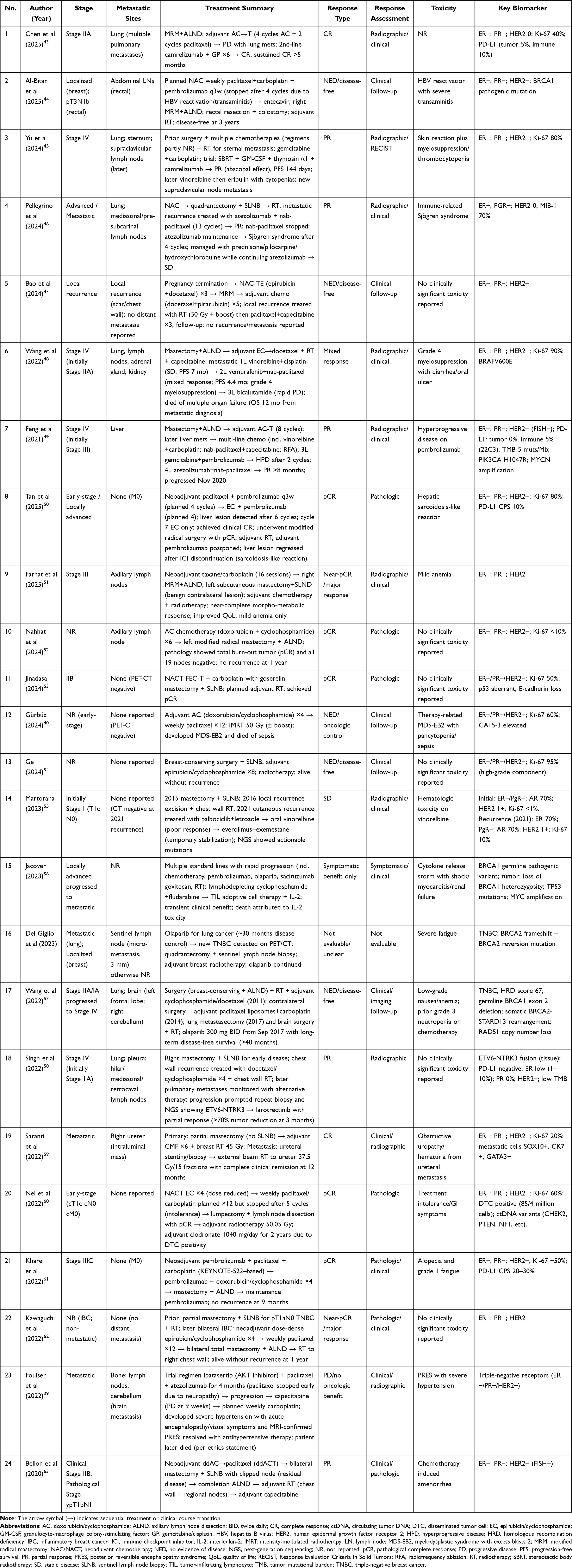 |
Table 1 Summary of Patient Demographics, Clinical Characteristics, Tumor Histology, and Key Baseline Biomarkers of the 24 Included Case Reports |
The biomarker and genomic landscape were heterogeneous across the included reports. Among recurrently described findings, BRCA1/2 alterations and PD-L1 status were each reported in five cases (20.8%), followed by PIK3CA alterations and circulating tumor DNA/disseminated tumor cell-related findings in two cases each (8.3%). BRAF alteration and NTRK fusion were each reported in one case (4.2%). Overall, 12 cases (50.0%) contained an actionable or resistance-informative biomarker signal, and biomarker-matched therapy was reported in 11 cases (45.8%). Among these 11 cases, the source reports described objective response or at least transient disease stabilization in nine cases. This observation indicates that molecular or immune biomarker information frequently informed treatment selection in the published cases. However, because these were selected case reports without control groups or standardized follow-up, these findings cannot establish predictive accuracy, treatment efficacy, or comparative benefit.
Treatment approaches were multimodal and commonly combined systemic chemotherapy with surgery, radiotherapy, immunotherapy, targeted therapy, or biomarker-guided treatment adaptation. Immunotherapy was reported in nine of 24 cases (37.5%). Pembrolizumab was the most frequently reported immune checkpoint inhibitor, appearing in five cases, followed by atezolizumab in three cases and camrelizumab in two cases. Tumor-infiltrating lymphocyte therapy and interleukin-2 were reported once in a highly refractory setting (Figure 2). These frequencies represent treatment exposures among the included published cases and do not indicate real-world utilization rates or comparative effectiveness.
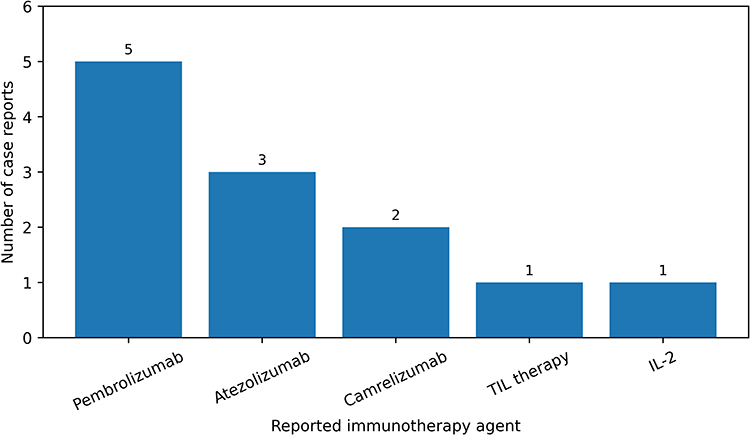 |
Figure 2 Reported immunotherapy agents across the included TNBC case reports. Counts represent exposure frequencies within the reviewed case. |
Clinical outcomes varied across the included reports. Within this selected case-report dataset, 17 cases (70.8%) were categorized as favorable outcomes, four cases (16.7%) as death/failure, and three cases (12.5%) as ongoing or unclear outcomes (Figure 3). Favorable outcomes included complete response, pathological complete response, near-complete or major pathological response, no evidence of disease, disease-free follow-up, partial response, or stable disease with clinically meaningful disease control, as defined by the original case-report authors. Complete or near-complete disease eradication, including complete response, pathological complete response, no evidence of disease/disease-free status, or near-pCR/major response, was described in 14 cases (58.3%).
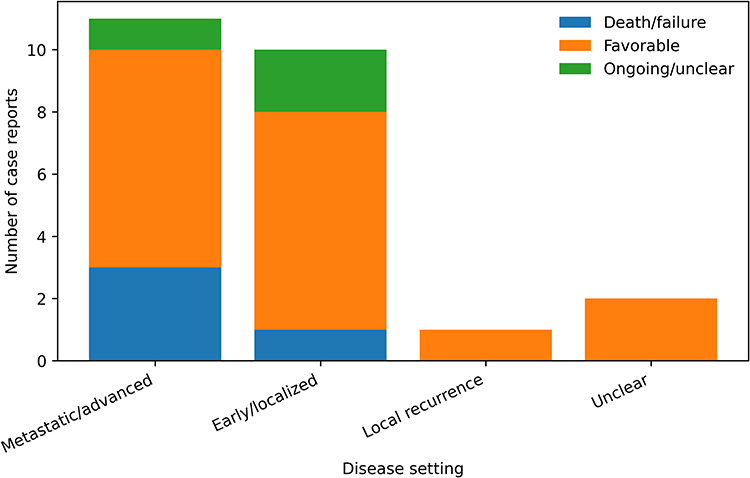 |
Figure 3 Outcome categories by disease setting among the included TNBC case reports. |
Treatment-related toxicity and clinically significant complications were central findings in the included reports. Serious toxicity or clinically significant complications were documented in 10 cases (41.7%), including two fatal treatment-related events (8.3%). Reported complications included hepatitis B virus reactivation with severe transaminitis, immune-related Sjogren syndrome, hepatic sarcoidosis-like reaction mimicking metastatic disease, posterior reversible encephalopathy syndrome, hyperprogressive disease after immune checkpoint inhibition, grade 4 myelosuppression, treatment intolerance, therapy-related myelodysplastic syndrome, and fatal inflammatory toxicity after adoptive cell therapy with interleukin-2. Because adverse-event grading and follow-up duration were inconsistently reported, these counts should not be interpreted as toxicity incidence. Instead, they identify clinically instructive patterns of complications that may inform individualized toxicity surveillance and multidisciplinary risk assessment.
Table 2 integrates these descriptive findings by summarizing the case-level factors that appeared to shape reported clinical outcomes and treatment-related complications across the included reports. The most clinically instructive patterns were not attributable to a single therapeutic modality, but reflected the interaction between patient-specific vulnerability, tumor histology, molecular biomarkers, treatment selection, and toxicity recognition. Patient-specific factors included germline DNA repair alterations, rare inherited vulnerabilities, viral carriage, and pregnancy-associated TNBC. Tumor-level factors included rare histological subtypes, actionable or resistance-informative molecular alterations, receptor conversion, and biomarker-defined therapeutic opportunities. Treatment-related patterns included both favorable responses and clinically significant complications after immune checkpoint inhibitor-containing regimens, severe toxicity after intensive or experimental therapy, and diagnostic uncertainty caused by immune-related mimics of disease progression. Disease-monitoring findings, including ctDNA and DTC discordance with pathological response, further emphasized that case-level TNBC outcomes may require interpretation beyond conventional response categories. These observations remain descriptive and hypothesis-generating, but they support the clinical relevance of individualized risk assessment, repeat pathological or molecular evaluation in selected cases, and multidisciplinary toxicity surveillance.
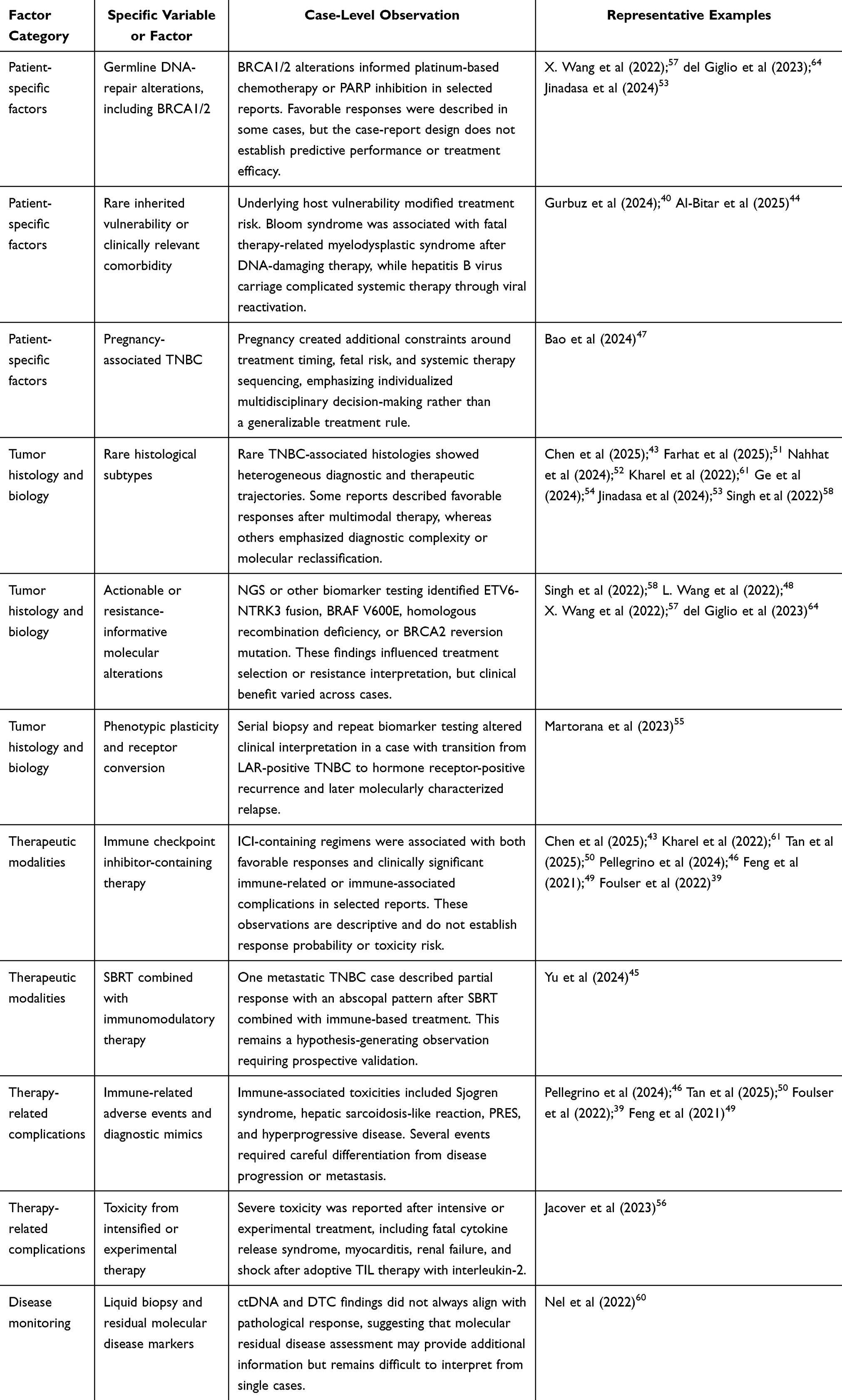 |
Table 2 Case-Level Factors Associated with Reported Clinical Outcomes and Treatment-Related Complications in TNBC Case Reports |
The CARE compliance assessment indicated generally adequate reporting quality across the 24 included case reports. Most reports described patient presentation, diagnostic work-up, therapeutic intervention, follow-up, and clinical outcome with sufficient clarity for descriptive synthesis. The strongest reporting domains were diagnostic assessment, treatment sequence, and case-specific clinical lessons. The least consistently reported domains were formal adverse-event grading, explicit discussion of limitations, and patient perspective (Figure 4). Reports focused on immune-related toxicity, experimental therapy, molecular resistance, or liquid-biopsy interpretation generally provided stronger discussion of clinical uncertainty and case-specific limitations.
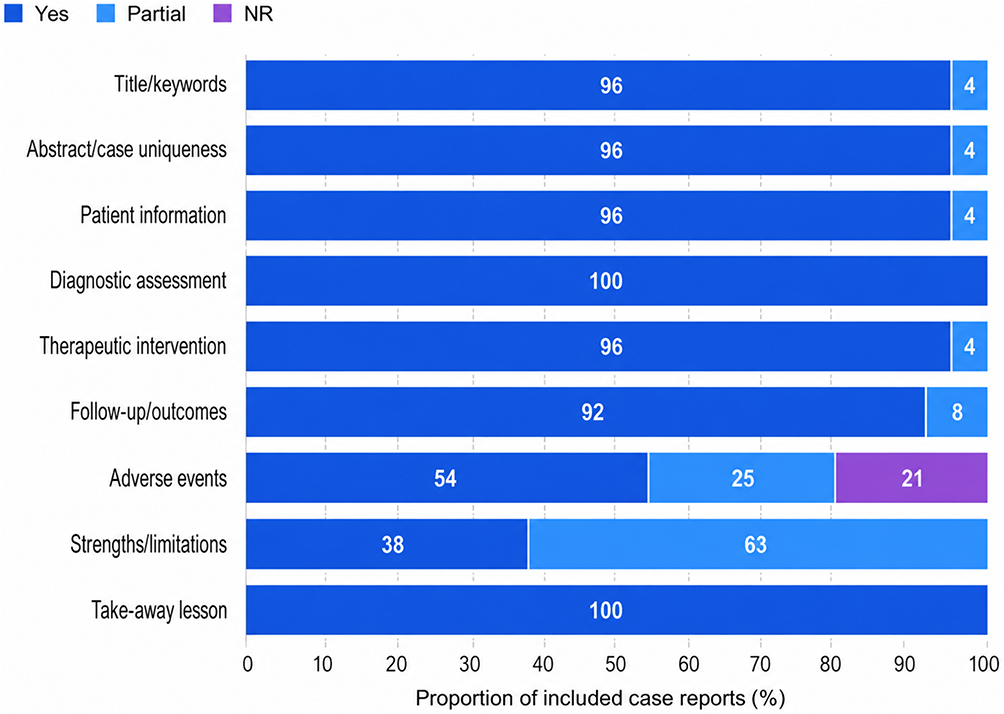 |
Figure 4 Reporting completeness of the included triple-negative breast cancer case reports based on CARE appraisal. |
Discussion
The 24 TNBC case reports in this review underscore the clinical heterogeneity observed in treatment outcomes and complications. This review does not highlight the superiority of any single therapeutic strategy, but rather the significant influence of host vulnerability, tumor biology, treatment selection, and toxicity management on individual patient outcomes. These observations are consistent with the broader characterization of TNBC as an aggressive and biologically diverse subtype, marked by limited receptor-directed options, early relapse, and variable responses to systemic therapy.4,7,8
The reported cases encompassed a broad clinical spectrum, ranging from early-stage or localized disease to locally advanced, inflammatory, recurrent, and metastatic TNBC. Several cases described advanced disease with involvement of the lung, liver, brain, mediastinal lymph nodes, bone, or rare metastatic sites such as the ureter.39,45,46,49,59 Other reports emphasized complex host contexts, including pregnancy-associated TNBC, synchronous rectal adenocarcinoma, hepatitis B virus carriage, hereditary cancer susceptibility, and rare DNA-repair syndromes.40,44,47,53 These findings indicate that TNBC management should not rely solely on receptor status or treatment regimen. Rather, patient-specific vulnerabilities and the broader disease context are central to determining which therapies are both feasible and safe.38
Contemporary TNBC therapy increasingly incorporates platinum chemotherapy, immune checkpoint inhibitors, PARP inhibitors, antibody-drug conjugates, and targeted approaches in selected clinical contexts.32–34 Trial-level evidence remains the primary basis for treatment standards, response expectations, and safety profiles.65,66 In contrast, the present review provides complementary case-level evidence. It captures rare or instructive clinical scenarios that are difficult to characterize in randomized trials, including severe toxicities, diagnostic mimics of disease progression, unusual metastatic patterns, rare histologies, and exceptional or discordant biomarker-associated responses.67–70
Several cases illustrate how baseline host factors influence therapeutic risk. Gurbuz et al (2024) reported that Bloom syndrome heightened vulnerability to DNA-damaging chemotherapy and radiotherapy, resulting in fatal therapy-related myelodysplastic syndrome and sepsis. While this case does not establish causality for all patients with DNA-repair disorders, it underscores the importance of identifying rare inherited vulnerabilities before initiating highly genotoxic treatments.40 Similarly, Al-Bitar et al (2025) described TNBC management complicated by hepatitis B virus reactivation and synchronous rectal adenocarcinoma, demonstrating how viral carriage and concurrent malignancies can impact the safety and sequencing of systemic therapy.44 Additionally, pregnancy-associated TNBC underscores the necessity for individualized treatment timing and multidisciplinary decision-making.47 Building on earlier findings, TNBC management must account for patient-specific vulnerabilities and broader disease context rather than receptor status alone; host profiling should indeed extend beyond basic demographic factors. Real-world data on pembrolizumab illustrate that immune-related adverse events occur across heterogeneous patient backgrounds, emphasizing the need for comprehensive baseline assessment rather than relying on age or performance status alone.38
The reviewed cases confirm that TNBC comprises a heterogeneous group with distinct clinical and biological subtypes. While many patients presented with high-grade invasive ductal carcinoma, some exhibited rare or diagnostically challenging tumor types, such as metaplastic breast carcinoma, inflammatory breast cancer, acinic cell carcinoma, pleomorphic lobular carcinoma, and secretory breast carcinoma.43,51–54,58,61 Given this diversity, thorough pathology review becomes essential whenever clinical presentation, morphologic features, biomarker patterns, or treatment responses deviate from expected TNBC behavior, as demonstrated by studies reporting diagnostic mimics, receptor conversion, misclassification, and discordant bilateral tumor responses.71–74
Molecular profiling influenced both interpretation and treatment selection in several cases. Next-generation sequencing or other biomarker testing identified actionable or resistance-informative alterations, including ETV6-NTRK3 fusion, BRAF V600E mutation, homologous recombination deficiency, BRCA1/2 alterations, and BRCA2 reversion mutation.48,57,58,64 In certain cases, these findings guided targeted therapy or clarified mechanisms of resistance; however, clinical benefit varied among cases. Molecular actionability should not be presumed to guarantee a durable response. Martorana et al (2023) further demonstrated phenotypic plasticity, with receptor conversion under selective pressure, supporting repeat biopsy and reassessment of receptor and molecular status when disease biology appears to change.55
Immune checkpoint inhibitor-containing regimens were reported in several included cases, with outcomes ranging from complete or partial response to immune-related toxicity, hyperprogressive disease, and diagnostic uncertainty.43,46,49,50,61 These cases are clinically instructive because immune checkpoint inhibitors can produce both antitumor activity and immune-mediated complications. However, this dataset cannot determine whether immune checkpoint inhibitors were independently responsible for response or toxicity because most cases involved multimodal treatment, chemotherapy combinations, radiotherapy, surgery, or sequential systemic therapy. Recent evidence in early-stage TNBC treated with pembrolizumab suggests an association between irAE development and pathological complete response, raising the possibility that selected toxicities may reflect immune activation related to treatment response.75 In the present review, irAEs were observed in selected cases with variable outcomes, and the dataset was not designed to test whether irAEs predict response. Therefore, irAEs should primarily be managed as clinically important toxicities, while their possible association with response should be considered hypothesis-generating and evaluated prospectively.
Treatment-related complications were clinically significant across the reviewed cases. Serious events included hepatitis B virus reactivation, immune-related Sjogren syndrome, hepatic sarcoidosis-like reaction, posterior reversible encephalopathy syndrome, hyperprogressive disease, grade 4 myelosuppression, treatment intolerance, fatal therapy-related myelodysplastic syndrome, and fatal toxicity following adoptive TIL therapy with interleukin-2.39,44,46,56 These findings support several practical considerations for multidisciplinary TNBC care. First, host vulnerabilities should be assessed before treatment intensification. This is particularly relevant because DNA repair alterations and homologous recombination deficiency may influence both therapeutic vulnerability and toxicity risk. At the same time, immune checkpoint inhibitors may cause multisystem adverse events requiring coordinated recognition and management.76–78 Second, biomarker and molecular testing may clarify treatment options in selected patients, particularly those with rare histology, refractory disease, discordant clinical behavior, or suspected actionable alterations involving PD-L1, BRCA1/2, HRD, TILs, TMB, or targetable gene fusions.78–81 Third, serial biopsy or repeat molecular profiling should be considered when disease phenotype changes, when receptor status appears discordant, or when progression is inconsistent with expected tumor biology, because TNBC is characterized by genomic, transcriptomic, immune-microenvironmental, and treatment-driven heterogeneity.32,82–84 However, given the limited number of reported cases and the absence of denominator populations, these considerations should not be interpreted as a validated clinical algorithm. Rather, they represent case-derived signals that support individualized risk assessment, early multidisciplinary consultation, and prospective evaluation of toxicity surveillance strategies in TNBC.
Limitations
This review has several limitations. First, it was based on published case reports, which are intrinsically subject to publication bias, including exceptional responses, rare histologies, severe toxicities, unusual diagnostic dilemmas, or unexpected clinical trajectories compared with routine cases. Second, the reports were heterogeneous in disease stage, histology, biomarker testing, treatment regimen, follow-up duration, and documentation of adverse events. This heterogeneity precluded meta-analysis or comparative effectiveness assessment. Third, adverse-event grading was reported inconsistently, limiting cross-case comparisons of toxicity severity. Fourth, treatment attribution was often uncertain because many patients received multimodal or sequential therapy, including surgery, radiotherapy, chemotherapy, immunotherapy, targeted therapy, and supportive interventions. Finally, the search strategy was limited to PubMed-indexed sources, potentially excluding relevant reports from other databases.
Conclusions
Published case reports on TNBC from 2020 to 2025 provide clinically instructive evidence on rare toxicities, unusual presentations, biomarker-guided treatment decisions, and individualized treatment risk. The reviewed cases support the importance of host-factor assessment, pathological and molecular reassessment in selected scenarios, careful evaluation of immune-related diagnostic mimics, and multidisciplinary toxicity management. However, these findings should be interpreted as descriptive and hypothesis-generating. They do not replace randomized or prospective evidence and cannot establish treatment efficacy, toxicity incidence, or causal risk. Future prospective studies should integrate standardized biomarker assessment, adverse-event grading, molecular residual disease monitoring, and longer follow-up to clarify which case-level signals are clinically generalizable.
Abbreviations
AC, doxorubicin/cyclophosphamide; AciCC, acinic cell carcinoma; ALND, axillary lymph node dissection; BLIS, basal-like immunosuppressed; BRCA1/2, breast cancer gene 1/2; CMF, cyclophosphamide/methotrexate/fluorouracil; CR, complete response; CT, computed tomography; ctDNA, circulating tumor DNA; CTCAE, Common Terminology Criteria for Adverse Events; DTC, disseminated tumor cell; EC, epirubicin/cyclophosphamide; ER, estrogen receptor; FISH, fluorescence in situ hybridization; GM-CSF, granulocyte-macrophage colony-stimulating factor; HBV, hepatitis B virus; HER2, human epidermal growth factor receptor 2; HPD, hyperprogressive disease; HRD, homologous recombination deficiency; IBC, inflammatory breast cancer; ICI, immune checkpoint inhibitor; IHC, immunohistochemistry; IL-2, interleukin-2; irAE, immune-related adverse event; LAR, luminal androgen receptor; MDS-EB2, myelodysplastic syndrome with excess blasts 2; MpBC, metaplastic breast carcinoma; MRM, modified radical mastectomy; NAC/NACT, neoadjuvant chemotherapy; NED, no evidence of disease; NGS, next-generation sequencing; NR, not reported; PARP, poly(ADP-ribose) polymerase; pCR, pathological complete response; PD, progressive disease; PD-L1, programmed death-ligand 1; PFS, progression-free survival; PR, partial response; PRES, posterior reversible encephalopathy syndrome; RECIST, Response Evaluation Criteria in Solid Tumors; RT, radiotherapy; SBRT, stereotactic body radiotherapy; SD, stable disease; SLNB, sentinel lymph node biopsy; TIL, tumor-infiltrating lymphocyte; TMB, tumor mutational burden; TNBC, triple-negative breast cancer.
Data Sharing Statement
All data analyzed in this review were extracted from the published case reports cited in the reference list. The extracted descriptive dataset is summarized in Table 1 and Supplementary Table S1.
Funding
This study is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025) awarded to AD (Contract No. 5663/UN6.3.1/PT.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Biswal B, Pandey P, Kumar S, Patel A. Breast cancer: drug delivery system landscape. Drug Delivery Landscape Cancer Res. 2025. doi:10.1016/B978-0-443-29168-5.00005-2
2. Xia C, Shen S, Pang J, et al. Expression of neuroendocrine markers predicts increased survival in triple-negative breast cancer patients. Front Endocrinol. 2023;14:1205631. doi:10.3389/fendo.2023.1205631
3. Zhao S, Yan C, Lv H, Xu J, Shao Z. Deep learning framework for comprehensive molecular and prognostic stratifications of triple-negative breast cancer. Fundam Res. 2024;4(3):678–20. doi:10.1016/j.fmre.2022.06.008
4. Agelidis A, Ter-Zakarian A, Jaloudi M. Triple-negative breast cancer on the rise: breakthroughs and beyond. Breast Cancer. 2025;17:523–529. doi:10.2147/BCTT.S516125
5. Pessoa ADS, Iano FG, Sanches MLR, Ximenes VF, de Oliveira RC. Methyl divanillate enhances doxorubicin efficacy in TNBC cell lines through redox imbalance and apoptotic reprogramming. Biochem Biophys Res Commun. 2026;810:153532. doi:10.1016/j.bbrc.2026.153532
6. Ahmed B, Aga QAK, Cheung K, Kaidar-Person O, Agrawal A. Treatment strategies for triple-negative primary breast cancer in older women: a systematic review. JNCI Cancer Spectr. 2025;9(3):pkaf049. doi:10.1093/jncics/pkaf049
7. Das A, Lather V. Signaling pathways and inhibitors in triple negative breast cancer: current progress. Anticancer Agents Med Chem. 2026;26(7):659–677. doi:10.2174/0118715206402646251115102627
8. Koczka KW, Nixon NA. The role of immunotherapy in metastatic triple negative breast cancer: a narrative review of the current clinical trials. Precis Cancer Med. 2021;4(March):1. doi:10.21037/pcm-20-58
9. Dimitrova M, Milushewa P, Petrova E, Mihaylova D, Tzvetanova N, Petrova G. Triple negative breast cancer in Bulgaria: epidemiological data and treatment patterns based on real-world evidence and patient registries. Biotechnol Biotechnol Equip. 2021;35(1):551–559. doi:10.1080/13102818.2021.1903338
10. Khanna R, Meena RN, Bansal A, et al. Triple negative breast cancer: experience from a North Indian tertiary care center. Indian J Surg. 2018;80(5):474–478. doi:10.1007/s12262-017-1638-7
11. Pajewska M, Partyka O, Czerw A, et al. Advanced and metastatic triple negative breast cancer—potential new treatment. Cancers. 2025;17(7):1183. doi:10.3390/cancers17071183
12. Hercules SM, Hercules JC, Ansari A, et al. High triple-negative breast cancer prevalence and aggressive prognostic factors in Barbadian women with breast cancer. Cancer. 2020;126(10):2217–2224. doi:10.1002/cncr.32771
13. Rugengamanzi E, Dharsee N, Lugina EL, et al. Comparison of clinicopathological features and survival in triple-negative and non-triple-negative breast cancer patients in Tanzania. Oncologist. 2025;30(11). doi:10.1093/oncolo/oyaf345
14. Thakur KK, Bordoloi D, Kunnumakkara AB. Alarming burden of triple-negative breast cancer in India. Clin Breast Cancer. 2018;18(3):e393–9. doi:10.1016/j.clbc.2017.07.013
15. Tiscoski KA, Giacomazzi J, Rocha MS, Gössling G, Werutsky G. Real-world data on triple-negative breast cancer in Latin America and the Caribbean. Ecancermedicalscience. 2023;17:1635. doi:10.3332/ecancer.2023.1635
16. Jeong HM, Kim RN, Kwon MJ, et al. Targeted exome sequencing of Korean triple-negative breast cancer reveals homozygous deletions associated with poor prognosis of adjuvant chemotherapy-treated patients. Oncotarget. 2017;8(37):61538–61550. doi:10.18632/oncotarget.18618
17. Kaleem M, Thool M, Dumore NG, et al. Management of triple-negative breast cancer by natural compounds through different mechanistic pathways. Front Genet. 2024;15:1440430. doi:10.3389/fgene.2024.1440430
18. Weisman PS, CKY N, Brogi E, et al. Genetic alterations of triple-negative breast cancer by targeted next-generation sequencing and correlation with tumor morphology. Mod Pathol. 2016;29(5):476–488. doi:10.1038/modpathol.2016.39
19. Mousmi A, Kumar CA. Correspondence: triple negative breast cancer - a brief insight into pathophysiology. Cancer Control. 2024;31:10732748241263642. doi:10.1177/10732748241263642
20. Vtorushin SV, Krakhmal NV, Zavyalova MV. Triple-negative breast cancer. Modern molecular genetic concepts and their clinical significance. Arkh Patol. 2021;83(2):46–51. doi:10.17116/patol20218302146
21. Thomas A, Reis-Filho JS, Geyer CE, Wen HY. Rare subtypes of triple-negative breast cancer: current understanding and future directions. NPJ Breast Cancer. 2023;9(1). doi:10.1038/s41523-023-00554-x
22. Vohra P, Chen YY, Krings G. Less Common Triple-Negative Breast Cancers. A Comprehensive Guide to Core Needle Biopsies of the Breast.
23. Reddy TP, Rosato RR, Li X, Piwnica-Worms H, Chang JCN, Chang JC. A comprehensive overview of metaplastic breast cancer: clinical features and molecular aberrations. Breast Cancer Res. 2020;22(1). doi:10.1186/s13058-020-01353-z
24. Corso G, Criscitiello C, Nicosia LA, Veronesi P, Fusco N. Metaplastic breast cancer: an all-round multidisciplinary consensus. Eur J Cancer Prev. 2023;32(4):348–363. doi:10.1097/CEJ.0000000000000794
25. Barrientos-Toro EN, Ding Q, Raso MG. Translational aspects in metaplastic breast carcinoma. Cancers. 2024;16(7):1433. doi:10.3390/cancers16071433
26. González-Martínez S, Pérez-Míes B, Carretero-Barrio I, Cortés J, Palacios JL. Molecular features of metaplastic breast carcinoma: an infrequent subtype of triple-negative breast carcinoma. Cancers. 2020;12(7):1832. doi:10.3390/cancers12071832
27. Aldrich JD, Canning M, Bhave MA. Monitoring of triple negative breast cancer after neoadjuvant chemotherapy. Clin Breast Cancer. 2023;23(8):832–834. doi:10.1016/j.clbc.2023.08.001
28. Błaszczak E, Miziak P, Odrzywolski A, Gumbarewicz E, Stepulak A, Stepulak A. Triple-negative breast cancer progression and drug resistance in the context of epithelial–mesenchymal transition. Cancers. 2025;17(2):228. doi:10.3390/cancers17020228
29. de Francesco EM, Cirillo F, Vella V, Maggiolini M, Lappano R, Lappano R. Triple-negative breast cancer drug resistance, durable efficacy, and cure: how advanced biological insights and emerging drug modalities could transform progress. Expert Opin Ther Targets. 2022;26(6):513–535. doi:10.1080/14728222.2022.2094762
30. Tang AH, Hoefer RA, Guye ML, Bear HD. Persistent EGFR/K-RAS/SIAH pathway activation drives chemo-resistance and early tumor relapse in triple-negative breast cancer. Cancer Drug Resistance. 2022;5(3):691–702. doi:10.20517/cdr.2022.31
31. Ma T, Hao X, Chen H, Cai S, Zhang J. Predictive markers of rapid disease progression and chemotherapy resistance in triple-negative breast cancer patients following postoperative adjuvant therapy. Sci Rep. 2025;15:386. doi:10.1038/s41598-024-84785-3
32. Xiong N, Wu H, Yu Z. Advancements and challenges in triple-negative breast cancer: a comprehensive review of therapeutic and diagnostic strategies. Front Oncol. 2024;14:1405491. doi:10.3389/fonc.2024.1405491
33. Previtali A, Guardamagna I, Calandra S, et al. Emerging protein targets in triple-negative breast cancer: beyond conventional therapy. Cancers. 2026;18(4):618. doi:10.3390/cancers18040618
34. Vyas A, Dwivedi S, Koka SS, Darwhekar GN. Triple-negative breast cancer: molecular subtypes, therapeutic challenges, and emerging strategies—a systematic review. Premier J Sci. 2025;13. doi:10.70389/PJS.100101
35. Gong C, Zhao Y, Wang L, Hu X, Wang B. A Phase II randomized trial of gemcitabine plus cisplatin (GP) versus gemcitabine plus carboplatin (GC) as the first-line treatment of patients with metastatic triple-negative breast cancer. ESMO Open. 2026;11(4):106889. doi:10.1016/j.esmoop.2026.106889
36. Gao X, Zhu Y, Wang P, Shen M, Zhang K. Addition of immune checkpoint inhibitors to chemotherapy versus chemotherapy alone in patients with triple-negative breast cancer: a systematic review and meta-analysis. Cancer Med. 2023;12(24):21873–21884. doi:10.1002/cam4.6760
37. Ríos-Hoyo A, Dai J, Noel T, Park TS, Pusztai L, Pusztai L. Immune-related adverse events are associated with better event-free survival in a phase I/II clinical trial of durvalumab concomitant with neoadjuvant chemotherapy in early-stage triple-negative breast cancer. ESMO Open. 2025;10(4):104494. doi:10.1016/j.esmoop.2025.104494
38. Jayan A, Sukumar JS, Fangman BD, Khan SS, Bárcenas CH. Real-world immune-related adverse events in patients with early triple -negative breast cancer who received pembrolizumab. JCO Oncol Pract. 2025;21(9):1265–1273. doi:10.1200/OP.24.00371
39. Foulser PFG, Senthivel N, Downey K, Hart PE, McGrath SE. Posterior reversible encephalopathy syndrome associated with use of Atezolizumab for the treatment of relapsed triple-negative breast cancer. Cancer Treat Res Commun. 2022;31. PubMed PMID: 35305364. doi:10.1016/j.ctarc.2022.100548
40. Gürbüz AF, Eryılmaz MK, Yıldız O, Kılınç F, Araz M, Artaç M. Rare case of myelodysplastic syndrome with excess blasts 2 developing after adjuvant chemoradiotherapy for triple-negative breast cancer in a patient with Bloom syndrome. Strahlentherapie und Onkologie. 2024;200(11):986–990. PubMed PMID: 38995367. doi:10.1007/s00066-024-02257-z
41. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372. doi:10.1136/bmj.n71
42. Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. BMJ Case Rep. 2013;2013:bcr2013201554. PubMed PMID: 24155002. doi:10.1136/bcr-2013-201554
43. Chen J, Liu J, Li Y, et al. Complete response in a patient with metastatic metaplastic breast cancer treated with immune checkpoint inhibitor and chemotherapy: a case report and a review of the literature. J Cancer Res Ther. 2025;21(4):955–959. PubMed PMID: 40905880. doi:10.4103/jcrt.jcrt_285_25
44. Al-Bitar A, Tellawi I, Kamil H, Al-Masalma D, Jeji K, Al-Mahasna S. Synchronous triple-negative breast cancer, rectal adenocarcinoma, and chemotherapy-induced hepatitis B virus reactivation: a case report and review of the literature. J Med Case Reports. 2025;19(1). PubMed PMID: 40753237. doi:10.1186/s13256-025-05423-8
45. Yu J, Wang Q, Wang L, Zong D, He X. PD-1 inhibitor combined with SBRT, GM-CSF, and thymosin alpha-1 in metastatic breast cancer: a case report and literature review. Medicine. 2024;103(34):e39271. PubMed PMID: 39183403. doi:10.1097/MD.0000000000039271
46. Pellegrino C, D’Antonio C, Ierinò D, et al. Sjögren syndrome induced by anti-PDL-1 treatment for TNBC: case report and review of literature. Front Immunol. 2024;15:1417444. PubMed PMID: 39434886. doi:10.3389/fimmu.2024.1417444
47. Bao W, Ma X, Xue Y, Zou X, Guo Y. Pregnancy-associated triple-negative breast cancer: a case report and literature review. Medicine. 2024;103(41):e40059. PubMed PMID: 39465823. doi:10.1097/MD.0000000000040059
48. Wang L, Lu Q, Jiang K, Hong R, Wang S, Xu F. BRAF V600E mutation in triple-negative breast cancer: a case report and literature review. Oncol Res Treat. 2022;45(1–2):54–61. PubMed PMID: 34818649. doi:10.1159/000520453
49. Feng D, Guan Y, Liu M, et al. Excellent response to atezolizumab after clinically defined hyperprogression upon previous treatment with pembrolizumab in metastatic triple-negative breast cancer: a case report and review of the literature. Front Immunol. 2021;12:608292. PubMed PMID: 34135884. doi:10.3389/fimmu.2021.608292
50. Tan Y, Wang Y, Liu X, et al. Case report: hepatic sarcoidosis-like reaction from neoadjuvant pembrolizumab in early-stage triple-negative breast cancer. Front Immunol. 2025;16:1589191. PubMed PMID: 40607429. doi:10.3389/fimmu.2025.1589191
51. Farhat H, Moghnieh R, Tlaiss Y, Bachaalany N, Aoun M, Hage E. Successful regression of metaplastic triple-negative breast cancer with neoadjuvant chemotherapy and surgical intervention: a case report. Medicine. 2025;104(16):e42167. PubMed PMID: 40258768. doi:10.1097/MD.0000000000042167
52. Nahhat F, Doyya M, Zabad K, Ksiri H. Metaplastic breast cancer with a unique presentation and complete response to chemotherapy: a case report. BMC Womens Health. 2024;24(1). PubMed PMID: 38734591. doi:10.1186/s12905-024-03134-8
53. Jinadasa M, Humphreys A, Massey EJ, et al. Triple-negative pleomorphic lobular carcinoma in a BRCA1 mutation carrier: a case of complete pathological response. Am J Case Rep. 2024;25:e943882. PubMed PMID: 39127886. doi:10.12659/AJCR.943882
54. Ge Y, Wei X, Liu JN, Sun PL, Gao H. Elucidating the nature of acinic cell carcinoma of the breast with high-grade morphology: evidence from case report. Diagn Pathol. 2024;19(1). PubMed PMID: 39049123. doi:10.1186/s13000-024-01521-1
55. Martorana F, Di Grazia G, Rosano GN, et al. More than meets the eye: a case of breast cancer switching from being luminal-androgen-receptor-positive to being hormone-receptor-positive. Medicina. 2023;59(10):1875. PubMed PMID: 37893593. doi:10.3390/medicina59101875
56. Jacover A, Zarbiv Y, Tal KH, et al. Tumor-infiltrating lymphocyte transfusion in a patient with treatment-refractory triple-negative breast cancer. Cancer Rep. 2023;6(12):e1894. PubMed PMID: 37750497. doi:10.1002/cnr2.1894
57. Wang X, Hu N, Cui L, et al. Durable disease-free survival in a patient with metastatic triple-negative breast cancer treated with olaparib monotherapy. Curr Cancer Drug Targets. 2022;22(6):530–536. PubMed PMID: 35156571. doi:10.2174/1568009622666220214092207
58. Singh N, Singh R, Decker B, Robins D, Vidal G. Metastatic triple negative breast cancer with NTRK gene fusion on tissue but not on ctDNA molecular profile. BMJ Case Rep. 2022;15(10):e251656. PubMed PMID: 36223973. doi:10.1136/bcr-2022-251656
59. Saranti G, Zolota V, Kalogeropoulou C, et al. Diagnostic and therapeutic challenges in a patient with ureteral metastases from a triple negative breast cancer. Current Oncol. 2022;29(7):4791–4798. PubMed PMID: 35877240. doi:10.3390/curroncol29070380
60. Nel I, Herzog H, Aktas B. Combined analysis of disseminated tumor cells (DTCs) and circulating tumor DNA (ctDNA) in a patient suffering from triple negative breast cancer revealed elevated risk. Front Biosci. 2022;27(7):208. PubMed PMID: 35866394. doi:10.31083/j.fbl2707208
61. Kharel Z, Nemer OP, Xi W, et al. Inflammatory breast cancer with excellent response to pembrolizumab-chemotherapy combination: a case report. Breast Dis. 2022;41(1):255–260. PubMed PMID: 35599460. doi:10.3233/BD-210041
62. Kawaguchi Y, Kuba S, Morita M, et al. Bilateral inflammatory breast cancer that developed two years after treatment for triple-negative breast cancer. Internal Med. 2022;61(15):2387–2391. PubMed PMID: 35022341. doi:10.2169/internalmedicine.7786-21
63. Bellon JR, Burstein HJ, Frank ES, Mittendorf EA, King TA. Multidisciplinary considerations in the treatment of triple-negative breast cancer. CA Cancer J Clin. 2020;70(6):432–442. PubMed PMID: 32986241. doi:10.3322/caac.21643
64. Del Giglio A, Da Costa Aguiar Alves B, Murad AM, Fonseca FLA. Metastatic lung adenocarcinoma with BRCA2 mutation and longstanding disease control on olaparib, developing triple-negative breast adenocarcinoma with additional BRCA2 reversion mutation: a case report. J Med Case Rep. 2023;17(1). PubMed PMID: 37743480. doi:10.1186/s13256-023-04139-x
65. Wang H, Zhang N, Sun Q, Kang W, Shan M. Comparison of the efficacy of taxanes with carboplatin and anthracyclines with taxanes in neoadjuvant chemotherapy for stage II–III triple-negative breast cancer: a retrospective analysis. J Cancer Res Clin Oncol. 2024;150:291. doi:10.1007/s00432-024-05738-x
66. Xu J, Gao Y, Liu Y, Chang JCN, Li X. Comprehensive clinicopathologic evaluations of 149 metaplastic carcinomas of the breast treated with neoadjuvant and adjuvant chemotherapy. Mod Pathol. 2026;39(5):100989. doi:10.1016/j.modpat.2026.100989
67. Brahmer JR, Lacchetti C, Schneider BJ, Wolchok JD, Thompson JA. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: american society of clinical oncology clinical practice guideline. J Clin Oncol. 2018;36(17):1714–1768. doi:10.1200/JCO.2017.77.6385
68. Rong J, Jafri FI, Ngo SB, Thomas AS, Wang Y. Rare irAEs associated with immune checkpoint inhibitor therapy. Expert Opin Drug Saf. 2026;1–15. doi:10.1080/14740338.2026.2629998
69. Schneider BJ, Naidoo J, Santomasso BD, Funchain PF, Bollin KB. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073–4126. doi:10.1200/JCO.21.01440
70. Brahmer JR, Abu-Sbeih H, Ascierto PA, Turner MM, Ernstoff MS. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer. 2021;9(6):e002435. doi:10.1136/jitc-2021-002435
71. Sun H, Cui Y, Wang H, Liu H, Wang T. Comparison of methods for the detection of outliers and associated biomarkers in mislabeled omics data. BMC Bioinf. 2020;21(1). doi:10.1186/s12859-020-03653-9
72. Fulford LG, d’Adamo AP, Reis-Filho JS, Lakhani SR, Hanby AM. Specific morphological features predictive of the basal phenotype in grade 3 invasive ductal carcinoma of the breast. Histopathology. 2006;49(1):22–34. doi:10.1111/j.1365-2559.2006.02453.x
73. Reis-Filho JS, Milanezi F, Steele D, Lakhani SR, Schmitt FC. Metaplastic breast carcinomas are basal-like tumors. Histopathology. 2006;49(1):10–21. doi:10.1111/j.1365-2559.2006.02467.x
74. Won SG, Park YM, Hyun KT, Baek J, Jin LY. Bilateral triple negative invasive ductal breast carcinoma in a BRCA1 mutation carrier with discrepant pathologic response to neoadjuvant chemotherapy. J Korean Soc Radiol. 2020;81:428. doi:10.3348/jksr.2020.81.2.428
75. Güren AK, Demircan NC, Gümüşay Ö, et al. Immune-related adverse events as predictors of pathological complete response in early-stage triple-negative breast cancer treated with pembrolizumab. Immunotherapy. 2026;18(4):317–326. doi:10.1080/1750743X.2026.2662201
76. Mkrtchyan GV, Veviorskiy A, Izumchenko EG, Zhavoronkov AA, Scheibye-Knudsen M. High-confidence cancer patient stratification through multiomics investigation of DNA repair disorders. Cell Death Dis. 2022;13(11). doi:10.1038/s41419-022-05437-w
77. Otahalova B, Volkova Z, Soukupová J, Macůrek L, Kleibl Z. Importance of germline and somatic alterations in human MRE11, RAD50, and NBN genes coding for MRN complex. Int J Mol Sci. 2023;24(6):5612. doi:10.3390/ijms24065612
78. Porta FM, Sajjadi E, Venetis K, Fusco N, Ivanova MD. Immune biomarkers in triple-negative breast cancer: improving the predictivity of current testing methods. J Pers Med. 2023;13(7):1176. doi:10.3390/jpm13071176
79. Sukumar JS, Gast KC, Quiroga DM, Lustberg MB, Williams NO. Triple-negative breast cancer: promising prognostic biomarkers currently in development. Expert Rev Anticancer Ther. 2021;21(2):135–148. doi:10.1080/14737140.2021.1840984
80. Castellano G, Giugliano F, Curigliano G, Marra A. Clinical utility of genomic signatures for the management of early and metastatic triple-negative breast cancer. Curr Opin Oncol. 2023;35(6):479–490. doi:10.1097/CCO.0000000000000989
81. Wang X, Collet L, Rediti M, Sotiriou C, Buisseret L. Predictive biomarkers for response to immunotherapy in triple negative breast cancer: promises and challenges. J Clin Med. 2023;12:953. doi:10.3390/jcm12030953
82. So J, Ohm JE, Lipkowitz S, Yang L. Triple negative breast cancer (TNBC): non-genetic tumor heterogeneity and immune microenvironment: emerging treatment options. Pharmacol Ther. 2022;237:108253. doi:10.1016/j.pharmthera.2022.108253
83. Varzaru VB, Vlad T, Popescu R, Moatar AE, Cobec IM, Cobec IM. Triple-negative breast cancer: molecular particularities still a challenge. Diagnostics. 2024;14(17):1875. doi:10.3390/diagnostics14171875
84. Corea-Dilbert FE, Afzal MZ. The role of genomics and transcriptomics in characterizing and predicting patient response to treatment in triple negative breast cancer (TN BC). Onco. 2025;5(2):18. doi:10.3390/onco5020018
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Mechanisms of Resistance to Immunotherapy in Hepatocellular Carcinoma
Manfredi GF, Celsa C, John C, Jones C, Acuti N, Scheiner B, Fulgenzi CAM, Korolewicz J, Pinter M, Gennari A, Mauri FA, Pirisi M, Minisini R, Vincenzi F, Burlone M, Rigamonti C, Donadon M, Cabibbo G, D'Alessio A, Pinato DJ
Journal of Hepatocellular Carcinoma 2023, 10:1955-1971
Published Date: 3 November 2023
Immune Indicator Changes in Hepatocellular Carcinoma Undergoing TACE Plus ICIs and Anti-VEGF Antibodies/TKIs: A Prognostic Biomarker Analysis
Xu XY, Wang Z, Liu CY, Wu HD, Hu ZX, Lin YY, Zhang S, Shen J, Zhong BY, Zhu XL
Journal of Hepatocellular Carcinoma 2024, 11:2019-2032
Published Date: 22 October 2024
Advances in the Use of Immune Checkpoint Inhibitors for Colorectal Cancer Treatment
Li J, Fu T, Wen Z, Liang J, Qiu Y, Li K, Yang J, Tong Y, Cai H
OncoTargets and Therapy 2025, 18:1159-1168
Published Date: 15 October 2025
Engineering Extracellular Vesicles for Tumor Targeted Therapy: Source Optimization, Modification, and Clinical Application
Sui J, Qin H, Zhang Z, Lv X, Lin X, Liu Z, Zhao X, Liu X, Zhang H
International Journal of Nanomedicine 2026, 21:592579
Published Date: 9 April 2026
Precision Thyroid Oncology: A Review of Multi-Omics Biomarkers and Spatiotemporal Technologies
Huang L, Deng X, Xi Z, Huan X, Mao J, Li X
International Journal of General Medicine 2026, 19:602509
Published Date: 18 May 2026