Back to Journals » Infection and Drug Resistance » Volume 19
Clinical Nomogram for Early Identification of Necrotizing Soft Tissue Infections: Development and Internal Validation in Hospitalized Patients
Authors Xia Y, Wang Y, Tao Z, Lu Z ![]()
Received 26 August 2025
Accepted for publication 30 January 2026
Published 7 February 2026 Volume 2026:19 559267
DOI https://doi.org/10.2147/IDR.S559267
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Yu Xia,1,2 Yiping Wang,1,2 Zhangbin Tao,1,2 Zhongqiu Lu1,2
1Department of Emergency Medicine, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People’s Republic of China; 2Wenzhou Key Laboratory of Emergency and Disaster Medicine, Wenzhou, 325000, People’s Republic of China
Correspondence: Zhongqiu Lu, Department of Emergency Medicine, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, 325000, People’s Republic of China, Email [email protected]
Purpose: To develop and validate a predictive model for necrotizing soft tissue infections (NSTIs) in hospitalized patients with skin and soft tissue infections (SSTIs).
Patients and Methods: In this retrospective single-center study, 131 patients with SSTIs admitted between April 2021 and March 2024 were divided into NSTI (n=72) and non-NSTI (n=59) groups. Demographic information, clinical characteristics, and key severity scores were collected. LASSO regression was used to select variables, and a logistic regression model was then developed. Model performance was evaluated using AUC, sensitivity, specificity, and the Hosmer-Lemeshow test. Internal validation was performed using 1000 bootstrap resamples. Model discrimination, calibration, and clinical utility were assessed through ROC curve, calibration curve, and decision curve analysis (DCA), respectively.
Results: Four independent predictors—age, temperature, depth of infection, and SOFA score—were identified. A nomogram constructed based on these variables exhibited good discriminative performance, with an AUC of 0.832 (95% CI: 0.763– 0.900), a sensitivity of 0.722, and a specificity of 0.797. Internal validation revealed an AUC of 0.832 (95% CI: 0.752– 0.897). The model passed the H-L test (p = 0.322). The calibration curve showed close alignment between predicted and observed outcomes (slope = 0.916), indicating good calibration. DCA demonstrated net clinical benefit across a wide range of threshold probabilities (0.1– 0.9).
Conclusion: The predictive model is simple and practical, with good discriminative and calibration performance. It may serve as a useful decision-support tool for early identification of NSTIs. However, future multicenter prospective studies are still needed for external validation to assess its practical application value.
Keywords: skin and soft tissue infections, necrotizing soft tissue infections, sepsis, prediction model
Introduction
Necrotizing soft tissue infections (NSTIs) are a group of rapidly progressive and life-threatening infections caused by microbial pathogens, primarily affecting the skin, subcutaneous tissue, fascia, and muscle.1 The incidence of NSTIs ranges from 0.86 to 32.64 per 100,000 person-years, which is influenced by factors such as climate and seasonal variations.2 The disease often follows a fulminant clinical course and is frequently complicated by sepsis, septic shock, and multiple organ dysfunction syndrome, with mortality rates reported as high as 23.1%-30%.3,4 Although NSTIs are rare, they are markedly more severe than other types of skin and soft tissue infections (SSTIs), and any delay in diagnosis or treatment can worsen disease severity and outcomes.
Early identification of NSTIs remains a significant clinical challenge. Some patients may have no obvious history of trauma or may initially present with only mild, nonspecific symptoms such as erythema, swelling, localized pain, or fever.5 Notably, the severity of pain is often disproportionate to the apparent skin damage, and typical signs such as bullae, ecchymosis, skin necrosis, or subcutaneous crepitus may not appear until the disease is in an advanced stage.6,7 Timely surgical intervention is critical to reducing mortality and disability in NSTIs. However, it has been reported that over 50% of NSTI cases are initially misdiagnosed as non-necrotizing soft tissue infections, delaying appropriate surgical and antimicrobial therapy and negatively affecting patient outcomes.8,9
Among existing assessment tools, the Laboratory Risk Indicator for Necrotizing Fasciitis (LRINEC) score is currently regarded as one of the most useful screening tools for early detection of NSTIs. It incorporates six laboratory parameters—C-reactive protein, white blood cell count, hemoglobin, sodium, creatinine, and blood glucose—and a score ≥ 6 is considered highly suggestive of NSTIs.10 However, a recent systematic review and meta-analysis involving 23 studies (n = 5982) reported a sensitivity of 68.2% and specificity of 84.8% for LRINEC ≥ 6.11 Additionally, an 18-year retrospective study found that the sensitivity of LRINEC ≥ 6 was only 59% with a positive predictive value of 57%, indicating a substantial risk of missed diagnosis in clinical practice.12 In addition to the LRINEC score, several models such as the modified LRINEC,13 SIARI,14 and NAS15 scores have been proposed. However, these tools have limited accuracy or lack extensive validation.
Recent studies have also explored the use of nomograms and artificial intelligence (AI) to improve the diagnosis of NSTIs. For example, MacLeod et al16 developed a nomogram incorporating age, C-reactive protein, and nonlinear albumin. However, its applicability is limited to people who inject drugs. Another study proposed an AI-based model capable of automatically detecting NSTI-related features on CT imaging.17 This approach relies on high-quality CT datasets and is more suitable for refining diagnostic certainty and assisting surgeons in delineating surgical margins on CT scans, rather than serving as an initial screening tool in the emergency setting. In addition, Wu et al18 identified several promising NSTI biomarkers based on biochemical analysis of infectious fluids. Nonetheless, procedures such as ultrasound-guided aspiration, fluid culture, and biochemical testing limit the model’s clinical feasibility, and it remains unclear whether all NSTI subtypes produce suprafascial fluid. Therefore, a simple, reliable, and bedside-applicable diagnostic tool that integrates severity scoring with key clinical variables through an appropriate algorithm is still needed. To fill this gap, this study aimed to develop and validate a predictive nomogram to facilitate the early diagnosis of NSTIs and guide timely intervention.
Methods
Study Setting and Source of Data
This retrospective study utilized data extracted from the electronic medical record system of the First Affiliated Hospital of Wenzhou Medical University, a provincial tertiary (Level 3A) hospital with 3800 beds in Zhejiang Province, eastern China. Data were collected between March and August 2024. This study was reported in accordance with the TRIPOD guidelines.
Participants
The study populations were hospitalized patients with SSTIs admitted to the Emergency Department of the First Affiliated Hospital of Wenzhou Medical University between April 2021 and March 2024. Inclusion criteria were: (a) age ≥ 18 years; and (b) a diagnosis of SSTIs based on medical history, physical examination, and laboratory findings, etc. (the minimum criterion being a skin lesion with the typical inflammatory tetrad—tenderness, erythema, edema, and warmth).19 Patients with incomplete clinical data were excluded. Ultimately, a total of 131 patients with SSTIs were included in the study. Among them, 72 patients were diagnosed with NSTIs through surgical exploration. The patient enrollment process is shown in Figure 1.
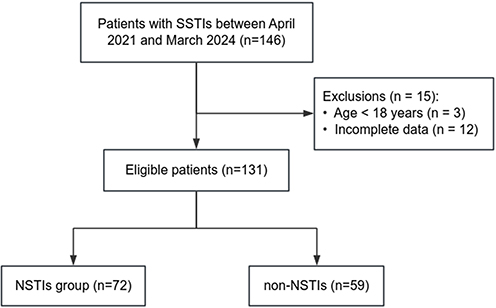 |
Figure 1 Patient enrollment flowchart. |
Outcome and Predictors
The outcome was the diagnosis of NSTIs. The length of hospital stay and mortality of patients were also collected but were not primary outcomes.
Potential predictors of NSTIs were selected based on literature review and clinical plausibility.20–22 These included demographic characteristics (sex, age), lifestyle (drinking, smoking), vital signs (respiratory rate, heart rate, axillary temperature, and mean arterial pressure), preoperative comorbidities (diabetes mellitus, hypertension, heart disease, chronic liver disease, and chronic kidney disease), laboratory values (C-reactive protein, white blood cell, procalcitonin, and creatine kinase), deep of infection (skin or subcutaneous/fascia/muscle), treatment measures (non-invasive ventilation, invasive ventilation, hemodialysis), as well as disease severity (SOFA score, APACHE II score, LRINEC scores, and occurrence of shock).
Vital signs, SOFA, APACHE II, and LRINEC scores were the results measured at the time of admission. Mean arterial pressure is calculated as diastolic blood pressure plus one-third of the difference between systolic and diastolic blood pressures. Laboratory values were the worst results obtained within 24 hours of admission. The depth of infection was determined at admission based on local skin manifestations and finger compression/palpation examination. Skin-limited infection (skin) was characterized by localized erythema and pain with clear margins; on finger compression, skin tension was similar to that of surrounding tissue, without crepitus. Infection involving the subcutaneous tissue (subcutaneous/fascia/muscle) was characterized by localized erythema with purplish discoloration or ecchymosis, severe pain, and the presence of bullae or hemorrhagic blisters; on palpation, increased skin tension, softening of the subcutaneous tissue, and crepitus could be detected.23,24
Entry of outcome variables was blinded. The outcome was collected separately from the other predictors to ensure that researchers did not know information about the other side when collecting the outcome or predictors.
Sample Size
The prediction model developed in this study included 4 predictors. According to the 10 times EPV principle, the sample should have at least 40 NSTI cases and 40 non-NSTI cases. Therefore, the sample size of the study met the statistical requirements.
Statistical Analysis
All statistical analyses were performed using SPSS 28.0 software and R 4.3.3 software.
(1) Univariate analysis: The Kolmogorov–Smirnov test was used to assess the normality of continuous variables. Variables with a normal distribution were expressed as mean ± standard deviation (SD) and compared between groups using independent samples t-tests. Non-normally distributed continuous variables were presented as median with interquartile range (IQR) and compared using the Mann–Whitney U-test. Categorical variables were expressed as numbers and percentages (n, %) and compared using the chi-square test or Fisher’s exact test, as appropriate. Associations between variables and the outcome were quantified using odds ratios (OR) and corresponding 95% confidence intervals (CI).
(2) Model development: A ten-fold cross-validated least absolute shrinkage and selection operator (LASSO) regression was performed using the “glmnet” package in R to determine the optimal penalty parameter lambda (λ). Variables selected by LASSO regression were subsequently entered into a forward stepwise logistic regression model, and statistically significant predictors were retained to construct the risk scoring model, which was then visualized as a nomogram. Logistic regression analyses were conducted using the lrm() function, and the nomogram was constructed using the nomogram() function in the “rms” package.
(3) Model evaluation and validation: The discrimination of model was assessed using the receiver operating characteristic (ROC), with sensitivity, specificity, the area under the curve (AUC), net reclassification improvement (NRI), and integrated discrimination improvement (IDI) calculated. Model calibration was evaluated using the Hosmer-Lemeshow (H-L) goodness-of-fit test and calibration curves. Decision curve analysis (DCA) and decision threshold heatmap were conducted to assess the clinical utility of the model. Internal validation was performed using 1000 bootstrap resamples.25 ROC curve plotting and AUC calculation were performed using the “pROC” and “fbroc” package; calibration curves were generated using the “rms” package; DCA was conducted with the “rmda” package; and decision threshold heatmap was generated using the “ggplot2” package. A sensitivity analysis was performed by adjusting for demographic factors and comorbidities to assess the robustness of the model. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Ethics Consideration
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Review Committee of the First Affiliated Hospital of Wenzhou Medical University (Approval No. KY2024-R194). A waiver for informed consent was allowed by the ethics review committee in view of the retrospective nature of the research and the anonymity of the data.
Results
Characteristics of Patients
The clinical data of 131 patients with SSTIs were retrospectively analyzed, including 83 (63.4%) males and 48 (36.6%) females. The median age was 62.0 years (IQR: 53.0, 74.0). Patients were categorized into NSTI (n=72) and non-NSTI (n=59) groups based on clinical features and surgical exploration findings. Univariate analyses revealed significant differences between NSTI and non-NSTI groups in several variables, including age (OR=0.965, 95% CI: 0.940–0.990), heart rate (OR=1.021, 95% CI: 1.004–1.038), temperature (OR=0.588, 95% CI: 0.386–0.896), chronic liver disease (OR=2.770, 95% CI: 1.204–6.370), depth of infection (OR=5.556, 95% CI: 2.382–12.957), procalcitonin (OR=1.004, 95% CI: 0.993–1.016), hemodialysis (OR=4.929, 95% CI: 1.573–15.448), SOFA (OR=1.208, 95% CI: 1.090–1.340), APACHE II (OR=1.100, 95% CI: 1.035–1.168), LRINEC (OR=1.167, 95% CI: 1.041–1.308), and shock (OR=3.592, 95% CI: 1.684–7.663). Furthermore, the NSTI group had a longer length of stay and a higher mortality rate than the non-NSTI group, although only the difference in length of stay was statistically significant (p = 0.006). Detailed results are shown in Table 1.
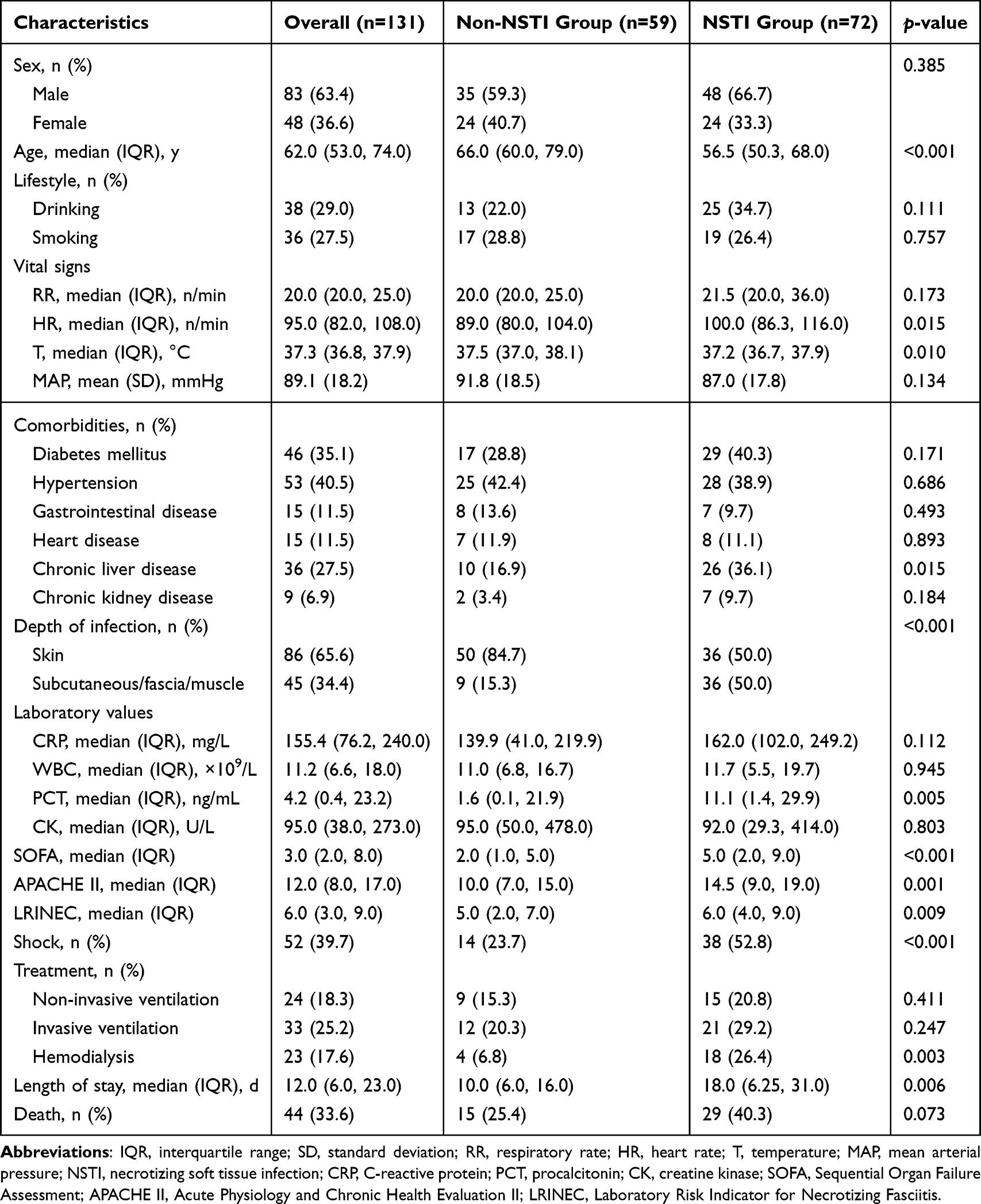 |
Table 1 Baseline Characteristics of Patients |
Selection of Predictors
A cross-validated LASSO regression was performed using the 11 significant factors from Table 1 to identify variables for the prediction model. As shown in Figure 2A, the minimum criteria (λ.min) and the one-standard-error criteria (λ.1se) corresponded to models containing 8 and 3 variables, respectively. Given that the model selected at λ.min demonstrated the best predictive accuracy, we selected the 8 variables it included: depth of infection, temperature, chronic liver disease, LRINEC score, SOFA score, age, APACHE II score, and hemodialysis (Figure 2B).
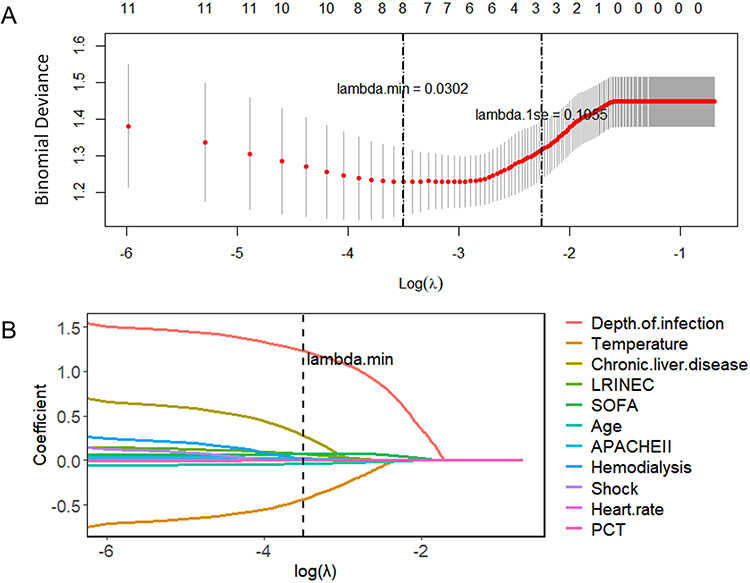 |
Figure 2 Variable selection using the least absolute shrinkage and selection operator (LASSO) regression. (A) The binomial deviance curve obtained from ten-fold cross-validation is plotted against log(λ). The left dotted line indicates the value of λ that minimizes the mean cross-validated binomial deviance (λ.min), corresponding to a model with 8 non-zero coefficients. The right dotted line represents the largest value of λ within one standard error of the minimum (λ.1se), corresponding to a model with 3 non-zero coefficients. (B) LASSO coefficient profiles of the 11 candidate variables. |
Development of Prediction Model
Stepwise forward logistic regression was performed using the 7 variables selected by LASSO regression. Ultimately, four statistically significant independent risk factors were identified and included in the final logistic regression model: depth of infection, age, SOFA score, and temperature (see Table 2). The risk prediction formula based on these four variables is as follows:
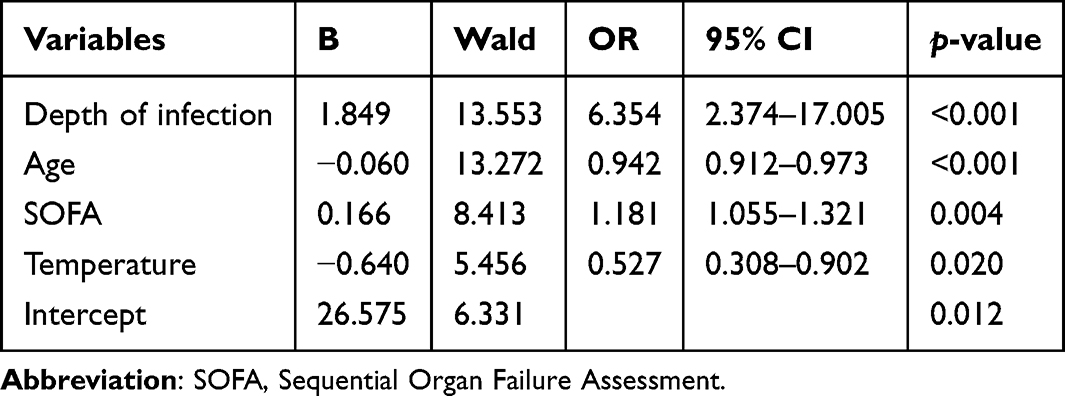 |
Table 2 Results of the Multivariate Logistic Regression |
P = 1/[1 + exp(−26.575–1.849 × Depth of infection + 0.060 × Age - 0.166 × SOFA score + 0.640 × Temperature)].
To facilitate clinical application, a nomogram was constructed based on this model. As depicted in Figure 3, each variable corresponds to a specific number of points according to the patient’s characteristics. The total score is obtained by summing the individual points, which can then be used to estimate the probability of NSTIs in a given patient (An example is provided in the Supplementary Materials Figure S1).
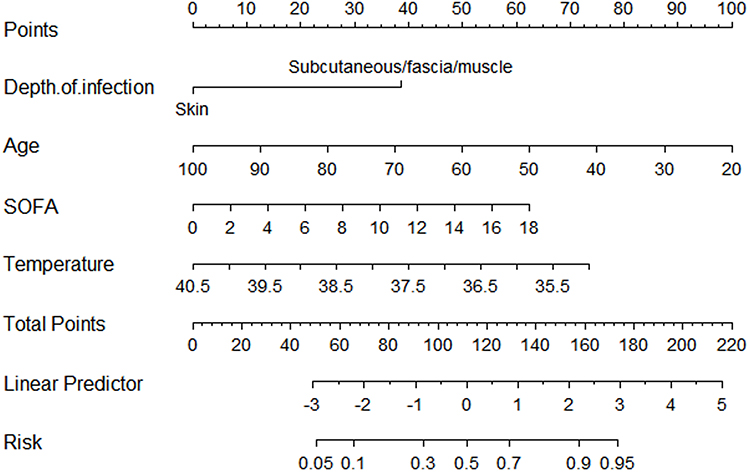 |
Figure 3 Nomogram for predicting the risk of necrotizing soft tissue infections. |
Model Evaluation and Validation
The nomogram model achieved an AUC of 0.832 (95% CI: 0.763–0.900), with a sensitivity of 0.722 (95% CI: 0.613–0.825) and a specificity of 0.797 (95% CI: 0.689–0.891). In contrast, the SOFA score (AUC=0.698, 95% CI: 0.609–0.788), APACHE II score (AUC=0.662, 95% CI: 0.570–0.755), and LRINEC score (AUC=0.632, 95% CI: 0.537–0.727) demonstrated relatively lower performance (Figure 4A). The NRI and IDI analyses demonstrated that the nomogram was significantly improved compared with the three scoring systems (Table 3).
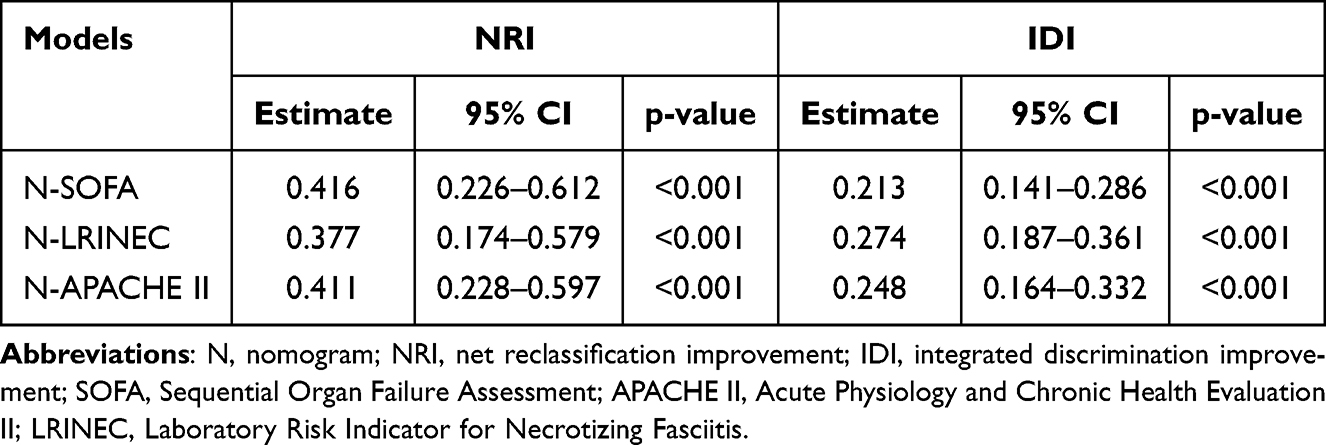 |
Table 3 NRI and IDI of the Nomogram Model Compared with SOFA, LRINEC, and APACHE II Scores |
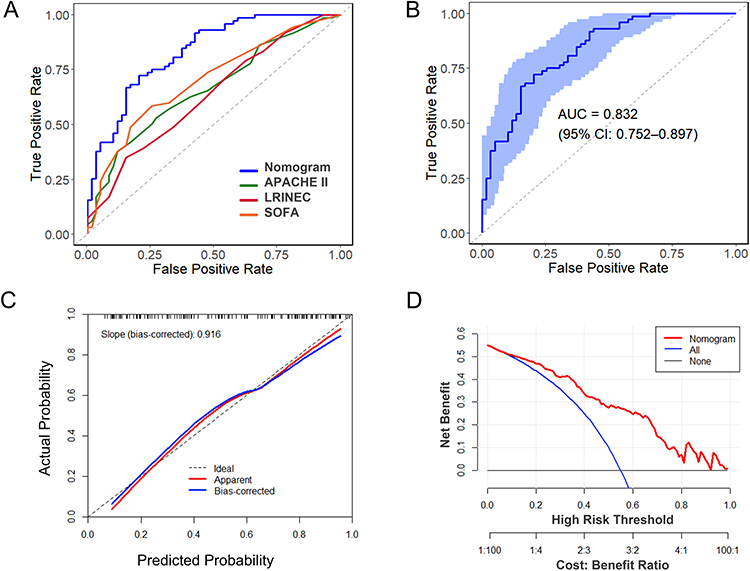 |
Figure 4 Evaluation and internal validation of the nomogram model. (A) Receiver operating characteristic curve of the nomogram, APACHE II, LRINEC, and SOFA scores. (B) Receiver operating characteristic curve of the nomogram using 1000 bootstrap resamples. (C) Calibration curve of the nomogram using 1000 bootstrap resamples. (D) Decision curve analysis of the nomogram. |
Internal validation was performed using 1000 bootstrap resamples. As shown in Figure 4B, the AUC of the nomogram was 0.832 (95% CI: 0.752–0.897), further confirming its strong discriminative ability.
The H-L test yielded a chi-square value of 9.245 with a p-value of 0.322, suggesting an adequate model fit. Calibration was assessed using a calibration curve generated from 1000 bootstrap samples. In Figure 4C, the bias-corrected curve closely aligned with the ideal reference line, with a slope of 0.916, indicating good agreement between predicted and observed outcomes.
DCA was conducted to assess the clinical utility of the nomogram. As illustrated in Figure 4D, within the threshold probability range of 0.1 to 0.9, the nomogram yielded a net benefit consistently greater than either the “treat-all” or “treat-none” strategies, suggesting that decisions based on the nomogram would provide clinical benefit within this range. The decision threshold heatmap (Figure S2) further showed that the model achieved its optimal overall performance within the mid-range of decision thresholds (approximately 0.4–0.6). Surgical intervention may be warranted when a patient’s predicted risk exceeds this range.
Sensitivity Analysis
Sensitivity analyses were performed by sequentially adjusting for demographic factors and comorbidities. As shown in Table S1, the estimated effect sizes across the original and adjusted models exhibited only minor changes. These findings indicated that the model results are robust.
Discussion
In this study, we developed and internally validated a predictive model for NSTIs among patients with SSTIs. The final model incorporated four independent predictors—age, temperature, depth of infection, and SOFA score—and demonstrated strong discrimination and calibration performance. A nomogram was also constructed to facilitate clinical application, and DCA showed meaningful net clinical benefit within a broad range of threshold probabilities.
Among the identified predictors, SOFA score was an independent risk factor for NSTIs, consistent with recent findings that highlight its prognostic value for mortality and ICU outcomes in severe infections, including NSTIs.26,27 However, some studies have suggested that models based on broader clinical characteristics may outperform SOFA or APACHE II scores alone in mortality prediction.28 The SOFA score reflects systemic inflammation and multi-organ dysfunction, which can impair tissue perfusion and immune function, creating a favorable environment for bacterial invasion and tissue necrosis. Early identification of organ dysfunction through the SOFA score may therefore help clinicians intervene earlier and improve outcomes in high-risk patients.
Hypothermia also emerged as a significant predictor of NSTIs in our model. This aligns with previous research showing that hypothermia in septic patients is associated with dysregulated immune responses and increased mortality.29 In the context of severe infections, hypothermia may reflect advanced disease progression, impaired thermoregulation, or systemic inflammatory failure.30 It can also compromise neutrophil function and antimicrobial defense, further promoting pathogen spread and tissue destruction. Therefore, clinicians should regard hypothermia as a potential marker of disease severity and escalate treatment when observed.
Interestingly, our study found that younger age was associated with a higher likelihood of NSTIs, which appears to contrast with the traditional view that older adults are more vulnerable to severe infections.31 Nevertheless, this finding is supported by several studies showing that younger patients may have a stronger immune response that paradoxically results in excessive inflammation and tissue damage.32 Additionally, younger individuals may be more likely to engage in activities that result in traumatic injuries or exposure to pathogens, thereby increasing their risk of severe infections.9 Previous reports have also shown that young adolescents have a higher incidence of NSTIs.33,34 Further research is needed to explore the interplay between immune response dynamics and behavioral factors.
The depth of infection was another strong and clinically intuitive predictor. Deeper infections involving fascia or muscle layers are more prone to necrosis due to reduced perfusion and oxygenation, facilitating anaerobic bacterial growth.9 This highlights the importance of timely surgical evaluation and debridement. Prior studies have demonstrated that early surgical intervention (within 6–12 hours of admission) is associated with significantly lower mortality.35–37 Thus, rapid recognition of deep tissue involvement should prompt aggressive surgical management. Surgeons should avoid limiting debridement to superficial or fascial layers and instead extend exploration based on the full clinical picture, especially given the complexity of deep anatomical planes and the difficulty in early diagnosis.
The NSTIs risk prediction nomogram developed in this study demonstrates significant potential for clinical application. Compared with existing scoring systems or models based on CT imaging and microbiological cultures,17,18 this model requires fewer variables that are easily obtainable, making it suitable for rapid bedside risk assessment. This enables early identification of NSTIs and supports preoperative emergency decision-making. In the future, the model could be further integrated into electronic medical record (EMR) systems to achieve intelligent alerts.
Nevertheless, this study has several limitations. It was a single-center retrospective study, which may be subject to selection bias. Given the rarity of NSTIs, the available data at our center were limited. Although internal validation was performed using the bootstrap method, external validation in multicenter and prospective cohorts is needed to assess the model’s applicability across different healthcare settings. Secondly, the included predictive variables were relatively limited. Future studies may consider incorporating imaging, microbiological, and other biomarker data to develop real-time dynamic prediction models. This would facilitate the early and precise identification of NSTIs, enable refined patient management, and improve clinical outcomes.
Conclusion
We developed and internally validated a clinically applicable nomogram for predicting NSTIs in SSTI patients, incorporating four easily obtainable clinical variables. The model may serve as an adjunct to existing severity scores and has potential for digital integration in triage systems.
Abbreviations
NSTIs, necrotizing soft tissue infections; SSTIs, skin and soft tissue infections; LRINEC, Laboratory Risk Indicator for Necrotizing Fasciitis; SOFA, Sequential Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II; SD, standard deviation; IQR, interquartile range; OR, odds ratio; CI, confidence interval; LASSO, least absolute shrinkage and selection operator; ROC, receiver operating characteristic; AUC, area under the curve; DCA, decision curve analysis.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Review Committee of the First Affiliated Hospital of Wenzhou Medical University (Approval No. KY2024-R194). A waiver for informed consent was allowed by the ethics review committee in view of the retrospective nature of the research and the anonymity of the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Key R&D Program Projects of Zhejiang Province (Grant number: 2021C03072).
Disclosure
The authors declare that they have no competing interests.
References
1. Hua C, Urbina T, Bosc R, et al. Necrotising soft-tissue infections. Lancet Infect Dis. 2023;23(3):e81–11. doi:10.1016/s1473-3099(22)00583-7
2. Allaw F, Wehbe S, Kanj SS. Necrotizing fasciitis: an update on epidemiology, diagnostic methods, and treatment. Curr Opin Infect Dis. 2024;37(2):105–111. doi:10.1097/qco.0000000000000988
3. Sartelli M, Coccolini F, Kluger Y, et al. WSES/GAIS/WSIS/SIS-E/AAST global clinical pathways for patients with skin and soft tissue infections. World J Emerg Surg. 2022;17(1):3. doi:10.1186/s13017-022-00406-2
4. Dhanasekara CS, Marschke B, Morris E, et al. Global patterns of necrotizing soft tissue infections: a systematic review and meta-analysis. Surgery. 2021;170(6):1718–1726. doi:10.1016/j.surg.2021.06.036
5. McDermott J, Kao LS, Keeley JA, et al. Necrotizing soft tissue infections: a review. JAMA Surg. 2024;159(11):1308–1315. doi:10.1001/jamasurg.2024.3365
6. Weaver C. Necrotizing Soft Tissue Infections. Med Clin North Am. 2025;109(3):625–640. doi:10.1016/j.mcna.2024.12.005
7. Branch CMDAEP, Branch CMAEM, Medicine CMDACoRaD, et al. Expert consensus on the emergency diagnosis and treatment of necrotizing soft tissue infections. Chin J Emerg Med. 2023;32(11):1465–1475. doi:10.3760/cma.j.issn.1671-0282.2023.11.007
8. Erickson BA, Miller AC, Warner HL, et al. Understanding the prodromal period of necrotizing soft tissue infections of the genitalia (Fournier’s Gangrene) and the incidence, duration, and risk factors associated with potential missed opportunities for an earlier diagnosis: a population-based longitudinal study. J Urol. 2022;208(6):1259–1267. doi:10.1097/ju.0000000000002920
9. Goh T, Goh LG, Ang CH, et al. Early diagnosis of necrotizing fasciitis. Br J Surg. 2014;101(1):e119–125. doi:10.1002/bjs.9371
10. Wong CH, Khin LW, Heng KS, et al. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32(7):1535–1541. doi:10.1097/01.ccm.0000129486.35458.7d
11. Fernando SM, Tran A, Cheng W, et al. Necrotizing soft tissue infection: diagnostic accuracy of physical examination, imaging, and LRINEC score: a systematic review and meta-analysis. Ann Surg. 2019;269(1):58–65. doi:10.1097/sla.0000000000002774
12. Breidung D, Malsagova AT, Barth AA, et al. Diagnostic and prognostic value of the Laboratory Risk Indicator for Necrotising Fasciitis (LRINEC) based on an 18 years’ experience. J Plast Reconstr Aesthet Surg. 2023;77:228–235. doi:10.1016/j.bjps.2022.11.061
13. Borschitz T, Schlicht S, Siegel E, et al. Improvement of a clinical score for necrotizing fasciitis: ‘pain out of proportion’ and high CRP levels aid the diagnosis. PLoS One. 2015;10(7):e0132775. doi:10.1371/journal.pone.0132775
14. Cribb BI, Wang MTM, Kulasegaran S, et al. The SIARI score: a novel decision support tool outperforms LRINEC score in necrotizing fasciitis. World J Surg. 2019;43(10):2393–2400. doi:10.1007/s00268-019-05061-4
15. Harasawa T, Kawai-Kowase K, Tamura J, et al. Accurate and quick predictor of necrotizing soft tissue infection: usefulness of the LRINEC score and NSTI assessment score. J Infect Chemother. 2020;26(4):331–334. doi:10.1016/j.jiac.2019.10.007
16. MacLeod CS, O’Neill HL, Shaalan R, et al. Predicting necrotising soft tissue infections in people who inject drugs: poor performance of the laboratory risk indicator for necrotising fasciitis score and development of a novel clinical predictive nomogram in a retrospective cohort with internal validation. Int J Surg. 2023;109(6):1561–1572. doi:10.1097/js9.0000000000000367
17. Lin HY, Chiu MC, Kao TL, et al. Automated detection of necrotizing soft tissue infection features by computed tomography. Diagnostics. 2025;15(16). doi:10.3390/diagnostics15162030
18. Wu KH, Wu PH, Wang HS, et al. Biochemical analysis of soft tissue infectious fluids and its diagnostic value in necrotizing soft tissue infections: a 5-year cohort study. Crit Care. 2024;28(1):354. doi:10.1186/s13054-024-05146-0
19. Moffarah AS, Al Mohajer M, Hurwitz BL, et al. Skin and soft tissue infections. Microbiol Spectr. 2016;4(4). doi:10.1128/microbiolspec.DMIH2-0014-2015
20. Anshu DA, Dwivedi DS, Murali DM, et al. Necrotising soft tissue infection in the present era: an analysis of clinicopathological features and predictors of mortality. Surg Pract Sci. 2023;13:100163. doi:10.1016/j.sipas.2023.100163
21. Tiffany LM, Tran QK, Abdel-Wahab M, et al. Outcomes and factors associated with occult septic shock in emergency department patients with soft tissue infection. J Emerg Trauma Shock. 2022;15(3):128–134. doi:10.4103/jets.jets_38_22
22. Suijker J, Pijpe A, Hoogerbrug D, et al. Identification of potentially modifiable factors to improve recognition and outcome of necrotizing soft-tissue infections. Shock. 2024;61(4):585–591. doi:10.1097/shk.0000000000002325
23. Andreasen TJ, Green SD, Childers BJ. Massive infectious soft-tissue injury: diagnosis and management of necrotizing fasciitis and purpura fulminans. Plast Reconstr Surg. 2001;107(4):1025–1035. doi:10.1097/00006534-200104010-00019
24. Zhou L, Li H, Luo G. Consensus on the diagnosis and treatment of adult necrotizing fasciitis (2025 Edition). Burns Trauma. 2025;13:tkaf031. doi:10.1093/burnst/tkaf031
25. Li N, Mahamad S, Parpia S, et al. Development and internal validation of a clinical prediction model for the diagnosis of immune thrombocytopenia. J Thromb Haemost. 2022;20(12):2988–2997. doi:10.1111/jth.15885
26. Qiu X, Lei YP, Zhou RX. SIRS, SOFA, qSOFA, and NEWS in the diagnosis of sepsis and prediction of adverse outcomes: a systematic review and meta-analysis. Expert Rev Anti Infect Ther. 2023;21(8):891–900. doi:10.1080/14787210.2023.2237192
27. Ogica A, Burdelski C, Rohde H, et al. Necrotizing soft tissue infections in intensive care. J Intensive Care Med. 2022;37(3):393–400. doi:10.1177/08850666211010127
28. Zhang LY, Zheng WJ, Li K, et al. Risk model for predicting mortality in patients with necrotizing soft tissue infections in the intensive care unit. Burns. 2024;50(3):578–584. doi:10.1016/j.burns.2023.11.008
29. Kushimoto S, Gando S, Saitoh D, et al. The impact of body temperature abnormalities on the disease severity and outcome in patients with severe sepsis: an analysis from a multicenter, prospective survey of severe sepsis. Crit Care. 2013;17(6):R271. doi:10.1186/cc13106
30. Laupland KB, Zahar JR, Adrie C, et al. Determinants of temperature abnormalities and influence on outcome of critical illness. Crit Care Med. 2012;40(1):145–151. doi:10.1097/CCM.0b013e31822f061d
31. Eguia E, Vivirito V, Cobb AN, et al. Predictors of death in necrotizing skin and soft tissue infection. World J Surg. 2019;43(11):2734–2739. doi:10.1007/s00268-019-05087-8
32. Hua C, Bosc R, Sbidian E, et al. Interventions for necrotizing soft tissue infections in adults. Cochrane Database Syst Rev. 2018;5(5):Cd011680. doi:10.1002/14651858.CD011680.pub2
33. Zundel S, Lemaréchal A, Kaiser P, et al. Diagnosis and treatment of pediatric necrotizing fasciitis: a systematic review of the literature. Eur J Pediatr Surg. 2017;27(2):127–137. doi:10.1055/s-0036-1584531
34. Liu J, Chen J, Wang Y, et al. The clinical characteristics and risk factors for necrotizing soft tissue infection in children. Pediatr Investig. 2024;8(1):21–26. doi:10.1002/ped4.12408
35. Chao WN, Tsai CF, Chang HR, et al. Impact of timing of surgery on outcome of Vibrio vulnificus-related necrotizing fasciitis. Am J Surg. 2013;206(1):32–39. doi:10.1016/j.amjsurg.2012.08.008
36. Hadeed GJ, Smith J, O’Keeffe T, et al. Early surgical intervention and its impact on patients presenting with necrotizing soft tissue infections: a single academic center experience. J Emerg Trauma Shock. 2016;9(1):22–27. doi:10.4103/0974-2700.173868
37. Boyer A, Vargas F, Coste F, et al. Influence of surgical treatment timing on mortality from necrotizing soft tissue infections requiring intensive care management. Intensive Care Med. 2009;35(5):847–853. doi:10.1007/s00134-008-1373-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Predictive Model Based on Inflammatory and Coagulation Indicators for Sepsis-Induced Acute Kidney Injury
Xin Q, Xie T, Chen R, Zhang X, Tong Y, Wang H, Wang S, Liu C, Zhang J
Journal of Inflammation Research 2022, 15:4561-4571
Published Date: 11 August 2022
Comprehensive Sepsis Risk Prediction in Leukemia Using a Random Forest Model and Restricted Cubic Spline Analysis
Kou Y, Tian Y, Ha Y, Wang S, Sun X, Lv S, Luo B, Yang Y, Qin L
Journal of Inflammation Research 2025, 18:1013-1032
Published Date: 22 January 2025
Development and Validation of a Nomogram for Predicting Sepsis-Associated Acute Respiratory Distress Syndrome
Yan C, Cai Y, Cai W, Wang Q, Li W, Geng Q
International Journal of General Medicine 2025, 18:5917-5925
Published Date: 29 September 2025
Influencing Factors of New-Onset Atrial Fibrillation in Sepsis Patients and Construction of a Nomogram Prediction Model: Based on LASSO Regression
Tang J, Ou W, Han B, Wen W
International Journal of General Medicine 2026, 19:565434
Published Date: 22 January 2026
Development and Validation of a 28-Day Mortality Prediction Model for Patients with Sepsis Complicated by Autoimmune Diseases Using Two Machine Learning Methods
Wang Z, Xiao X, Li S, He J, Li Y, Huang F, Wang J
Journal of Inflammation Research 2026, 19:555953
Published Date: 5 February 2026