Back to Journals » Journal of Inflammation Research » Volume 18
Clinical Features, Treatment Effectiveness and Long-Term Outcomes in Children with Moderate-to-Severe Generalized Pustular Psoriasis: A Retrospective Cohort Study
Authors Cao Z ![]() , Peng B, Li Z, Li R, Fan R, Mi B
, Peng B, Li Z, Li R, Fan R, Mi B ![]() , Li B, Song X, Shi J
, Li B, Song X, Shi J ![]() , Geng S
, Geng S
Received 19 June 2025
Accepted for publication 18 September 2025
Published 4 October 2025 Volume 2025:18 Pages 13787—13798
DOI https://doi.org/10.2147/JIR.S548192
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Anish R. Maskey
Zhiqiang Cao,1,* Bin Peng,1,* Zonghao Li,2 Ruiqi Li,1 Ruitao Fan,1 Baibing Mi,2 Bingjie Li,1 Xiangjin Song,1 Jing Shi,1 Songmei Geng1
1Department of Dermatology, Northwest Hospital, The Second Hospital Affiliated of Xi’an Jiaotong University, Xi’an, Shaanxi, 710004, People’s Republic of China; 2Department of Epidemiology and Biostatistics, School of Public Health, Xi’an Jiaotong University Health Science Center, Xi’an, Shaanxi, 710061, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Songmei Geng, Department of Dermatology, Northwest Hospital, The Second Hospital Affiliated of Xi’an Jiaotong University, Xi’an, Shaanxi, 710004, People’s Republic of China, Tel +86 13060423612, Email [email protected]
Background: Generalized pustular psoriasis (GPP) is a rare inflammatory skin disorder, frequently accompanied by systemic inflammatory manifestations. Pediatric GPP presents unique clinical features and requires tailored treatment approaches. However, real-world data on pediatric moderate-to-severe GPP remain limited.
Objective: To describe the clinical profiles of pediatric moderate-to-severe GPP, evaluate the effectiveness of various treatments, and their impact on disease recurrence.
Methods: This retrospective observational study enrolled pediatric moderate-to-severe GPP inpatients in our department from March 2017 to February 2024. Clinical characteristics, treatment regimens, and recurrence were collected and analyzed using electronic medical records and follow-up data.
Results: 61 pediatric patients were included, with a male-to-female ratio of 1.54: 1, an average age of 10.6± 3.2 years. Concomitant symptoms were present in 93.4% of patients, including pruritus, fever, and skin pain. Common comorbidities included hypoproteinemia, anemia, and hyperlipidemia. Over 80% of patients exhibited elevated inflammatory markers, including IL-6, TNF-α. GPP with psoriasis vulgaris (PV) and without PV had similar clinical presentations. Regarding treatment outcomes, compared with traditional drugs, biologics significantly reduced both hospitalization time (6.0 days vs 8.0 days, P=0.002) and pustule clearance time (3.0 days vs 7.0 days, P=0.013), with a lower incidence of adverse events. Post-discharge follow-up data on annual flare indicated the biologics group was associated with fewer annual flares (0 vs 0.3 per person-year, P=0.052) and lower recurrence rate (21.1% vs 60.0%, P=0.034), compared with the traditional drugs group. Furthermore, serum proteomic analysis revealed significantly elevated IL-17 level and activation of the IL-17 signaling pathway in pediatric GPP compared with healthy controls, elucidating the mechanism underlying the high effectiveness of biologic-targeted therapies.
Conclusion: For moderate-to-severe pediatric GPP, biologics exhibit faster effectiveness and better safety than traditional systemic drugs. Specifically, biologics can significantly reduce hospitalization time and pustule clearance time, and decrease disease recurrence.
Keywords: children, clinical profile, generalized pustular psoriasis, moderate-to-severe, recurrence, treatment
Introduction
Psoriasis is a chronic, immune-mediated cutaneous disorder that affects approximately 3% of the global population.1 It is broadly categorized into pustular and non-pustular types. Among the non-pustular variants, psoriasis vulgaris (PV) is the most prevalent, accounting for up to 90% of all psoriasis cases, typically characterized by well-defined, scaly plaques. In contrast, pustular psoriasis (PP) is far less common, representing only about 1%–2% of all psoriasis cases. Clinically, it is distinguished by the presence of superficial, sterile pustules that are rich in neutrophils. From a pathogenetic perspective, PV exhibits a prominent adaptive immune response, whereas PP is dominated by innate immune responses.2,3
Generalized pustular psoriasis (GPP), as a type of PP, is a rare, chronic inflammatory dermatosis characterized by recurrent eruptions of nonacral neutrophilic pustules.4 In addition to cutaneous findings, patients may present with systemic manifestations, including fever, malaise, laboratory abnormalities, and even multiorgan involvement. Without prompt diagnosis and treatment, GPP can be life-threatening.5 Recent studies using electronic databases have revealed significant variations in the prevalence rate of GPP across different countries, with the prevalence in China documented at 14 cases per million population.6 Its rarity and the absence of a standardized therapeutic framework have limited large-scale clinical investigations, hindering our understanding of disease presentations and the management of evidence-based treatments.7
Managing GPP in pediatric patients poses unique challenges.8 While conventional systemic therapies, such as methotrexate, retinoids, and cyclosporine, remain mainstays of treatment. Some studies have introduced biologic agents targeting key cytokines, including TNF-α, IL-17, and IL-23, which play critical roles in GPP pathophysiology.9 Furthermore, recent advances indicate that a selective humanized antibody against the IL-36 receptor (IL36R), spesolimab, effectively controls acute flare of GPP.10 However, data supporting the effectiveness of systemic therapies, particularly biologics, in pediatric inpatients remains sparse. This study reports a series of pediatric moderate-to-severe GPP cases from our institution, evaluating clinical responses to both traditional drugs and biological agents and assessing their potential to achieve sustained disease remission. Meanwhile, we conducted a comprehensive comparison between biologic agents and traditional drugs for pediatric GPP, elucidating differences in their clinical efficacy—encompassing both the management of acute flares and the maintenance of long-term remission—as well as in their adverse events, thereby supplementing real-world research data focused on pediatric GPP.
Materials and Methods
Study Design and Patients
This single-center, retrospective cohort study included pediatric patients (<18 years) diagnosed with GPP and hospitalized in our department from March 2017 to February 2024 (Figure S1). Each diagnosis was confirmed by at least two experienced dermatologists. Following Asia-Pacific consensus guidelines,6 GPP was defined by characteristic clinical presentation, histopathology, and medical history. Flare definition and severity level classification were in accordance with the Asia-Pacific consensus.6 Patients with psoriasis vulgaris (PV) either preceding GPP diagnosis by more than 6 months or occurring after GPP remission were classified as GPP with PV, otherwise, they were classified as GPP without PV.11 Patients were excluded if pustules were confined to existing psoriasis plaques or if GPP was not the primary diagnosis during the index hospitalization. This study was approved by the Ethics Committee of our hospital (2024–121) and conducted in accordance with the Declaration of Helsinki.
Data Collected and Follow-Up
We reviewed electronic medical records for demographic characteristics, personal and family history, clinical features, diagnosis, laboratory findings, treatment, and outcomes. Follow-up data, such as flare times, obtained through electronic records and telephone interviews using structured questionnaires, were collected until June 2024. To reduce bias in telephone follow-up, we adopted a standardized process based on the guidelines of clinical research telephone-based follow-up (T/CRHA 067–2024).
Criteria for Severity and Effectiveness Assessment
Primary effectiveness endpoints included the General Psoriasis Physician Assessment of Generalized Pustular Psoriasis (GPPGA) and pustular subscore.12 The scores were assessed by two experienced dermatologists, and it would be decided by a senior doctor if their results were inconsistent. Treatment effectiveness was defined as patients achieving GPPGA 0/1. Adverse drug reactions were recorded. Patients who self-discharged (n=3) or lacked pustule lesions at admission (n=3) were excluded from these analyses.
Treatments
Patients were categorized into two groups for treatment comparison: one group included patients receiving biologics alone (n=14, including secukinumab, adalimumab, and ustekinumab), and another included those receiving traditional agents (n=37, such as cyclosporine, retinoids, methotrexate, or glucocorticoids). Treatment effectiveness was evaluated based on GPPGA scores, pustule clearance time, hospitalization time (total duration of treatment), effective rate, pustule clearance rate, and recurrence. Four children who did not respond to first-line traditional therapies were switched to a combination of biologics with traditional drugs (n=4). These patients were excluded from the comparative analysis of treatment effectiveness.
Olink Proteomic
The protein levels in sera were determined by Olink Proteomic (target 96 Inflammation panel) from 5 pediatric GPP inpatients and 4 age- and sex-matched healthy children as control (registration number: ChiCTR2400083906). Informed consent of 9 children was signed by their guardians. The differentially expressed proteins were analysed via the Rstatix R package.
Statistical Analyses
Descriptive data are presented as follows: for continuous variables obeying a normal distribution, the mean±standard deviation (SD) is used; for skewed continuous data, the median (interquartile range, IQR) is adopted; and for categorical variables, frequency (percentage) is reported. Pearson chi-square (χ2) or Fisher’s exact test was used for categorical comparisons. For comparisons between two groups, continuous variables were assessed using independent sample t-test for normal distribution data or the Mann–Whitney U-test for skewed data. Kaplan-Meier survival analysis was applied to compare recurrence rates across treatment groups. Statistically, significance was defined as P≤0.05 (2-sided). All analyses were performed using SPSS Statistics version 26.0 (IBM) and GraphPad Prism software version 10.1.
Results
General Demographic and Clinical Characteristics of Pediatric GPP
Sixty-one pediatric inpatients with GPP were included (Table 1). All patients had moderate-to-severe GPP (GPPGA≥2). The cohort included 36 males and 25 females (male-to-female ratio,1.54: 1). The mean age was 10.6±3.2 years, with disease onset ranging from 3 to 17 years (mean, 8.8±3.7 years). Among identified triggers of initial onset, 14.8% were associated with upper respiratory tract infections, while 70.5% had no defined trigger. Upper respiratory tract infection (n=9) was also a key recurrent inducement. A family history of psoriasis was documented in 19.7% of patients. 93.4% of patients experienced different symptoms. Pruritus occurred in 48 patients, fever in 39, and skin pain in 19 (Table S1). Seasonal distribution showed the highest incidence in spring (33.7%), while approximately equal rates (22.1%) were observed in the other seasons.
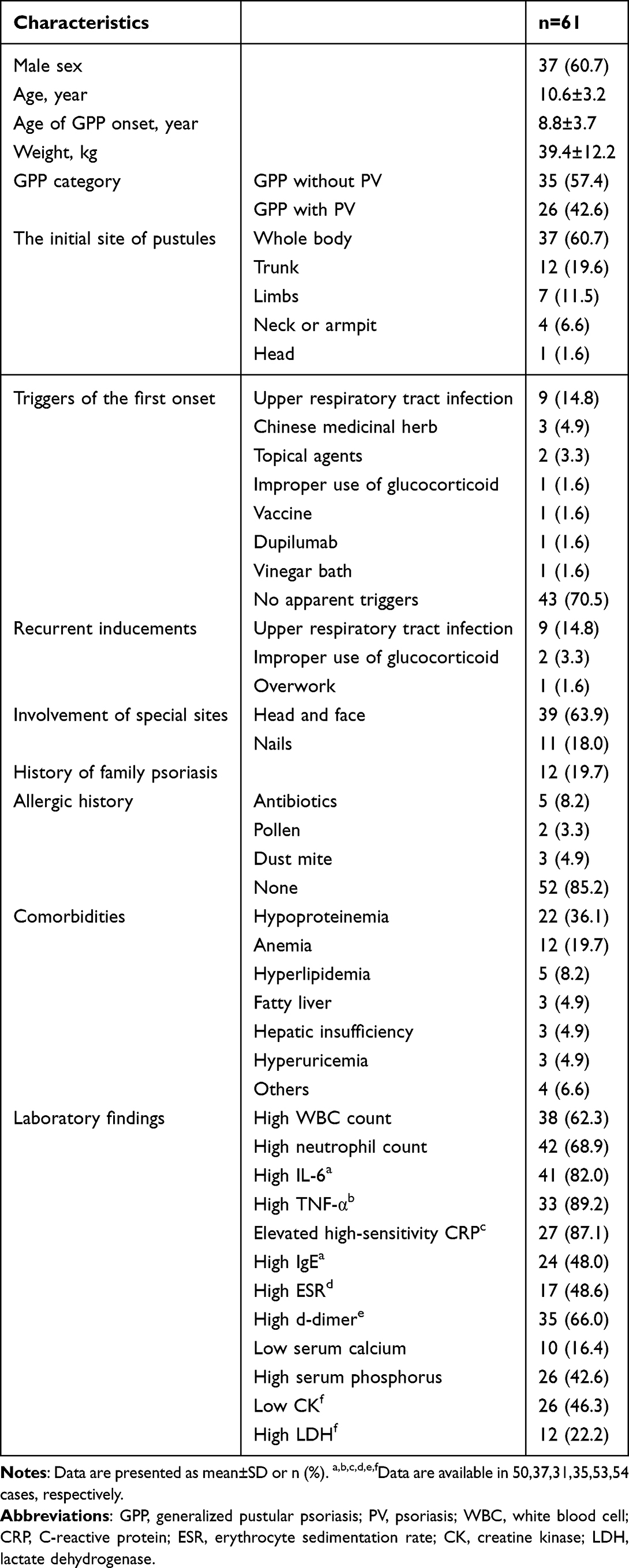 |
Table 1 Clinical Characteristics of All Patients |
Common comorbidities included hypoproteinemia (36.1%), anemia (19.7%), hyperlipidemia (8.2%), fatty liver (4.9%), and hyperuricemia (4.9%). Other uncommon types, including pyemia, atopic dermatitis, IgA nephropathy, and glomerulonephritis, had one case, respectively. Laboratory data showed elevated white blood cell (WBC) counts in 62.3%, increased neutrophil counts in 68.9%, and elevated inflammatory markers (IL-6, TNF-α, high-sensitivity CRP) in more than 80% of patients. Elevated IgE, ESR, and D-dimer were observed in 48.0%, 48.6%, and 66.0% of patients, respectively. Additional abnormalities included high serum phosphorus (42.6%) and low creatine kinase (46.3%).
To elucidate the relationship between GPP and PV, we compared the characteristics of GPP patients with and without PV (Table S1). Compared with GPP with PV, GPP without PV group seemed to have a lower family history of psoriasis and a higher proportion of concomitant symptoms (including skin pain and arthralgia), but there was no statistical difference. No significant differences were found in other aspects, including GPPGA scores at baseline, treatment outcomes (P>0.05).
Clinical Effectiveness and Safety of Different treatments in All Patients
At discharge, the biologics group (n=14) achieved a 100% effectiveness rate, including application of secukinumab (9 cases), adalimumab (4 cases), and ustekinumab (1 case), with secukinumab achieving the highest pustule clearance rate (77.8%). The traditional drugs group yielded a 97.3% effectiveness rate, and 84.6% of patients achieved pustule clearance. Adverse events occurred in 8 patients, mainly labial mucosal dryness with acitretin (7 cases) and glucocorticoid-related obesity (1 case). No adverse events were reported with biologics.
Comparisons between the biologics and traditional drug groups showed no significant difference in baseline or post-treatment GPPGA and pustule subscores. However, hospitalization time (6.0 days vs 8.0 days, P=0.002) and pustule clearance time (3.0 days vs 7.0 days, P=0.013) were significantly shorter in the biologics group (Table 2, Figure S2A and B). The overall effectiveness rate did not differ significantly between the two groups during hospitalization (100% vs 97.3%, P>0.999).
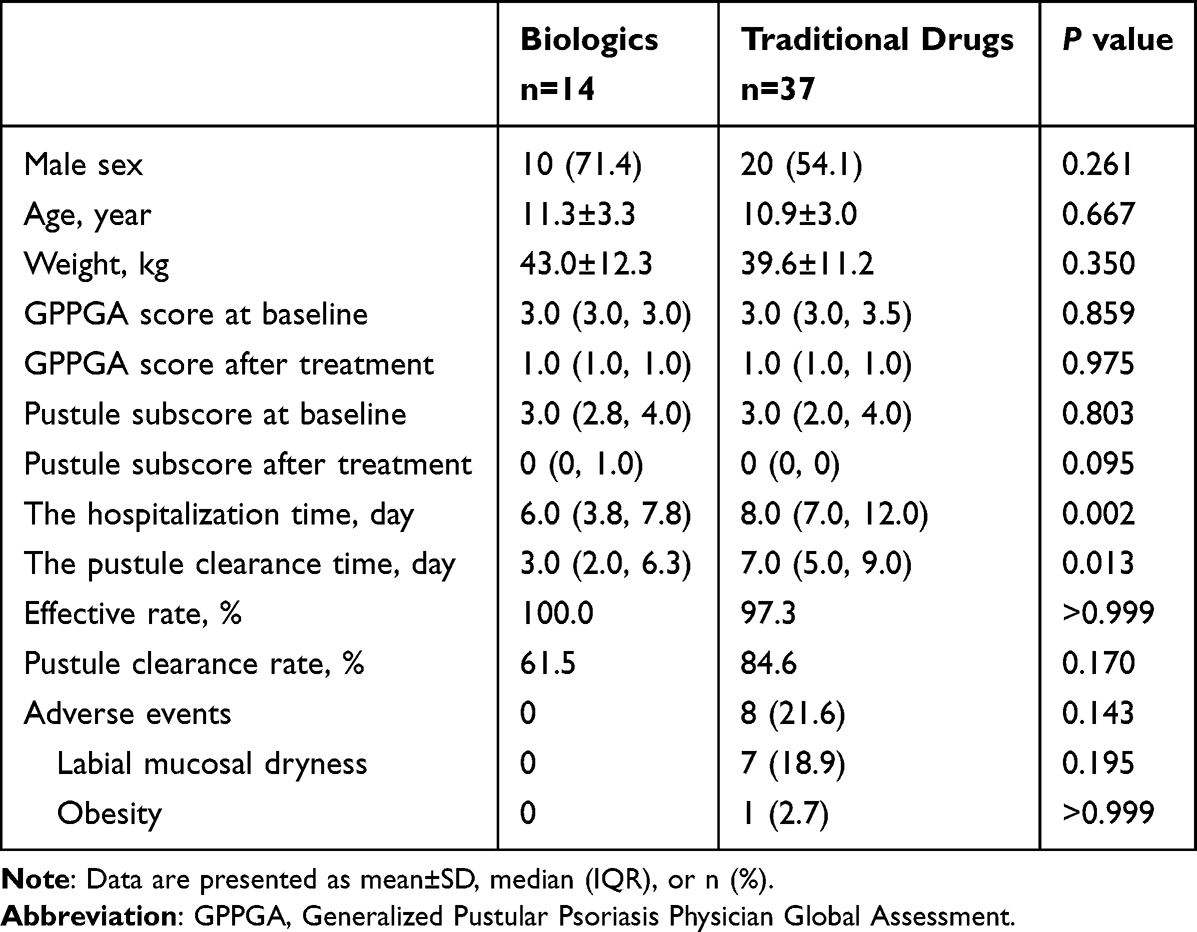 |
Table 2 Comparison of Clinical Effectiveness of GPP with Treatments of Biologics Alone and Traditional Drugs |
Combination therapy, reserved for patients who did not significantly respond to initial traditional drugs within a few days, ultimately improved through biologics application. This group included secukinumab with glucocorticoids (2 cases), secukinumab with acitretin (1 case), and adalimumab with acitretin (1 case). All cases achieved GPPGA 0/1 at discharge.
GPP Recurrence During Follow-Up After Discharge
To assess recurrence, patients were divided into two groups based on post-discharge treatment, those continuing traditional drugs and those receiving or initiating biologics alone (biologics group). 34 patients had complete follow-up data on the flare situation (Table 3). In the traditional drugs group, the annual flare frequency decreased from 1.088 to 0.223 flares/year, and per-patient flares declined from 1.0 to 0.3 flares per person-year. In the biologics group, annual flares declined from 1.576 to 0.147 flares/year, and from 1.0 to 0 flares per person-year. Compared with traditional therapies, the biologic therapy at post-discharge was associated with fewer annual flares (0 vs 0.3 per person-year, P=0.052) and lower recurrence rate (21.1% vs 60.0%, P=0.034).
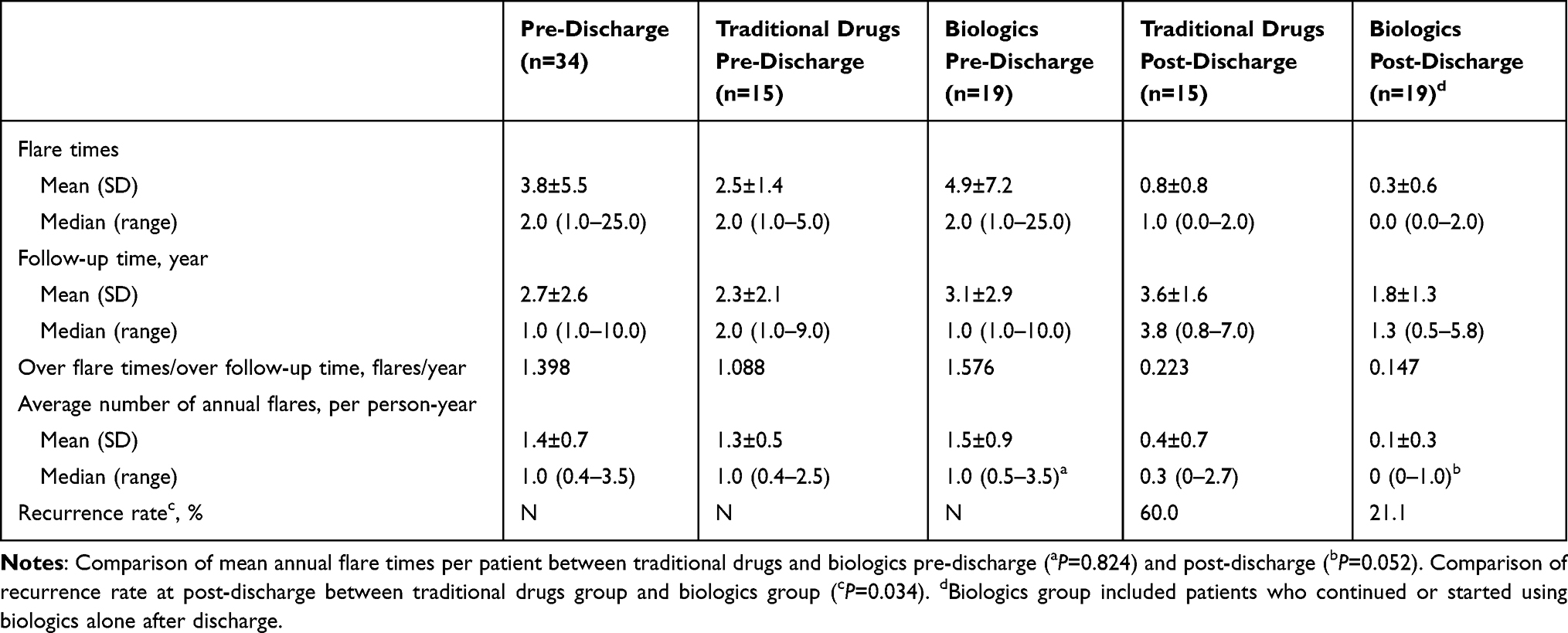 |
Table 3 The Status of GPP Flares During Follow-Up Pre- and Post-Discharge |
Kaplan-Meier analysis (Figure 1) showed a higher and earlier recurrence rate in the traditional drugs group compared with the biologics group (P=0.042; RR, 3.112; 95% CI, 1.034–9.362). The median time to 50% recurrence in the traditional drugs group was 12 months; in the biologics group, the recurrence rate remained notably lower. Post-discharge GPPGA and pustule subscores (Figure 2A and B) showed that traditional drugs initially maintained improvement but eventually demonstrated rising scores after 8 weeks, while biologic therapy provided more sustained disease control until after week 24. Overall, the average GPPGA and pustule scores remained at a low level throughout a 96-week follow-up period.
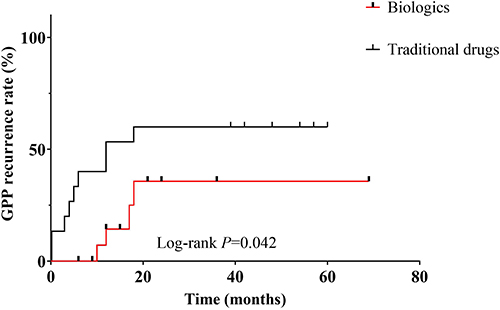 |
Figure 1 Kaplan-Meier survival analysis of the time to GPP recurrence after discharge between biologics and traditional drugs. |
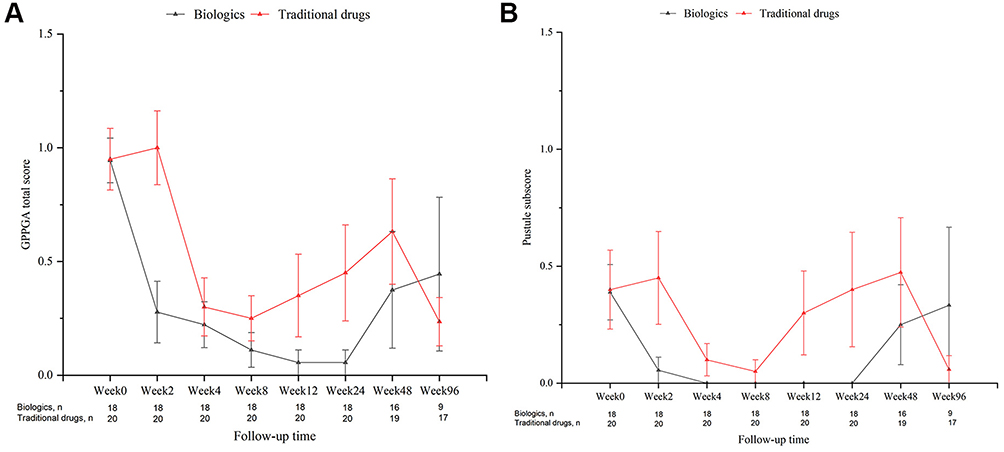 |
Figure 2 GPP remission and recurrence were performed based on changes in the GPPGA scores from weeks 0 (discharge) to weeks 2, 4, 8, 12, 24, 48, 96. Changes in the mean GPPGA total score (A) and pustule subscore (B) for pediatric patients with GPP of 96-week follow-up after discharge. All data presented in this study are the mean±SEM of all participants. Biologics group, n=18, 16, 9 at week 24, 48, 96, respectively. Traditional drugs group, n=20, 19, 17 at week 24, 48, 96, respectively. Abbreviations: GPPPGA, Generalized Pustular Psoriasis Physician Global Assessment; SEM, Standard Error of the Mean. |
Inflammation Biomarker Differences Between Pediatric GPP and Healthy Children
For providing the evidence in application of targeting treatment (biologics), Olink Proteomic in sera from 5 pediatric GPP and 4 healthy children showed 9 different proinflammatory protein expression, with 6 upregulation and 3 downregulation (Figure 3A). IL-17A, IL-17C, and IL-6 significantly increased in GPP group compared with the healthy control group (Figure 3B–D). GO enrichment analysis revealed signaling receptor activator activity, receptor ligand activity, and cytokine activity (Figure 3E). KEGG showed IL-17 signaling pathway and cytokine-cytokine interaction (Figure 3F).
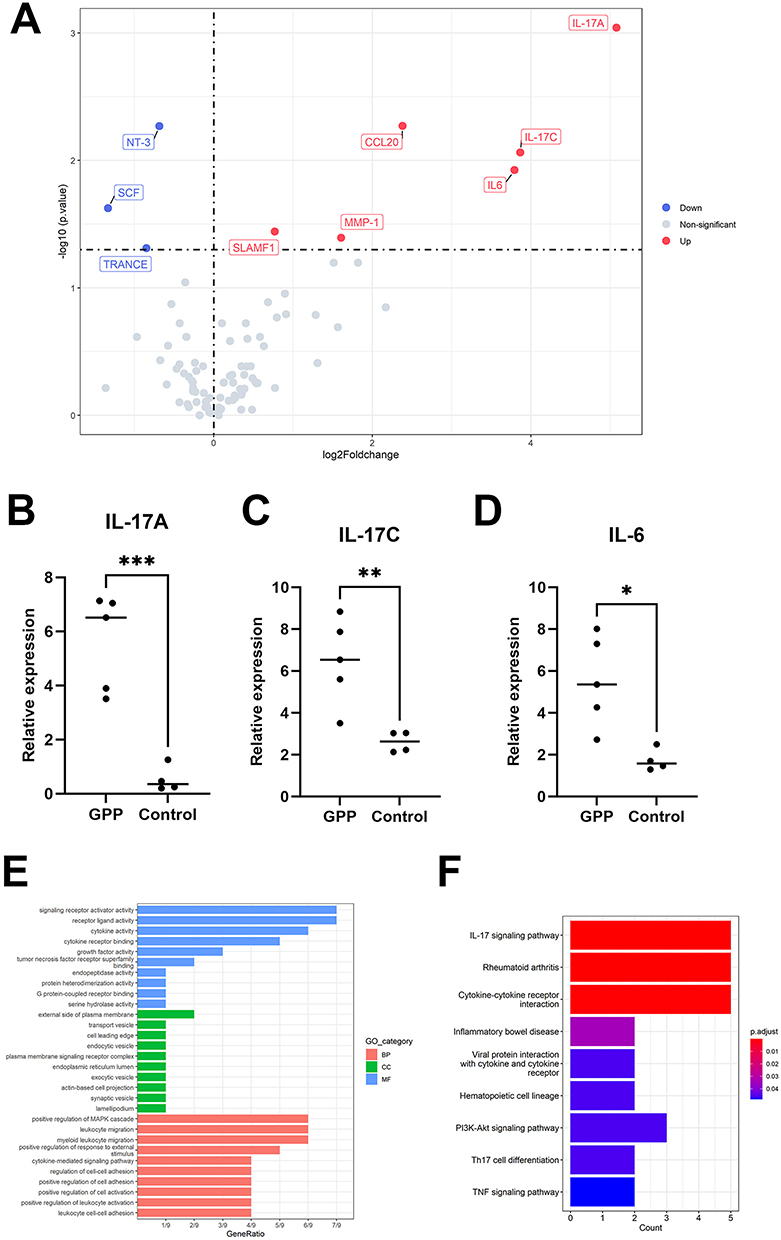 |
Figure 3 Olink Proteomic results between GPP inpatients and healthy controls. The different proinflammatory protein expression (A), relative expression of IL17A, IL-17C, IL-6 protein (B–D). The results of GO (E) and KEGG (F) enrichment analysis. *P<0.05, **P<0.01, ***P<0.001. |
Discussion
Due to its rarity, pediatric GPP remains insufficiently understood in terms of clinical characteristics and treatment options. This study retrospectively analyzed the clinical characteristics, laboratory findings, treatment responses, and long-term outcomes of 61 children with moderate-to-severe GPP, aiming to enhance understanding and improve clinical management of GPP in children.
Compared with previous studies, our pediatric cohort showed similarities in clinical characteristics alongside some novel observations. In our cohort, the male-to-female ratio was 1.54:1, with a mean age of 10.6±3.2 years and an onset age of 8.8±3.7 years. However, findings on certain clinical features varied across studies, possibly due to differences in sample inclusion.13–15 Triggers for initial onset and recurrent factors included upper respiratory tract infections, improper glucocorticoid use, vaccination, and overexertion, consistent with previous reports.13,16 19.7% of patients had a family history of psoriasis, which aligns with the findings of Xu et al (16.7%)11 but is lower than reported in other studies.13,15
GPP is frequently associated with systemic symptoms, including fever, chills, malaise, arthritis, nail changes, abnormal liver function, and laboratory abnormalities.7 In our study, nearly all inpatients presented with various symptoms, with pruritus and fever being the most common, underscoring the importance of managing pediatric moderate-to-severe GPP. Comorbidities, primarily hypoproteinemia, anemia, and hyperlipidemia, may result from increased metabolic demand and inflammatory response, as reflected in elevated inflammation-related laboratory markers (neutrophil counts, IL-6, TNF-α). Nearly half of the patients had elevated IgE, which was consistent with Wang et al’s report,16 confirming that IgE was a general indicator of the severity of systemic inflammation in GPP and PV.17 The increase in D-dimer and muscle enzyme abnormalities may be related to immune dysregulation associated with inflammation, attracting little attention. Multiple symptoms, comorbidities, and elevated indicators showed the status of systemic inflammation in GPP patients. Our findings indicate that there was no significant difference in clinical presentations between the GPP with PV and without PV, though GPP without PV had a lower proportion of family history of psoriasis, and a higher proportion of skin pain and arthralgia.
Traditional systemic therapies, including retinoids, glucocorticoids, and immunosuppressants, are commonly used in pediatric GPP, though they provide short-term effects and may cause organ-specific toxicities.18,19 Acitretin has shown effectiveness in treating GPP, especially in severe or drug-resistant cases. A retrospective study of acitretin monotherapy in children with pustular psoriasis showed that skin lesions began to resolve 5–7 days after treatment initiation, with complete clearance within 4–6 weeks.20 Mild adverse effects, such as dry skin, dry mouth, cheilitis, and pruritus, were observed in 80% (12/15) of patients; however, these side effects were generally transient. GPP recurred following acitretin discontinuation, although retreatment was still effective.20 Additionally, a study reported satisfactory clinical responses in 22 pediatric GPP patients treated with traditional therapies (16 on acitretin, 4 on acitretin combined with low-dose corticosteroids, and 2 on cyclosporine), with no severe complications or fatalities.16
However, with advancing understanding of the pathogenesis of GPP, treatment approaches are evolving. Biologic targeting key pathways is emerging as a new option for managing GPP,9,21 with some case studies confirming their high effectiveness and tolerability in pediatric cases. An Asia-Pacific consensus shows IL-17 inhibitors and TNF-α inhibitors are recommended for the management of pediatric GPP patients. In recent years, secukinumab, an IL-17 inhibitor, has been used in pediatric GPP.22,23 A systematic review reported that all 46 pediatric patients achieved a GPPASI90 after 12 weeks of secukinumab treatment, with approximately 96% attaining GPPASI100.24 Nine patients in our cohort received secukinumab treatment, achieving a 100% effectiveness rate during hospitalization. Adalimumab also showed a rapid response in pediatric GPP,25 consistent with our results. Hospitalization and pustule clearance time were significantly shorter in biologic group than traditional drug group, proving faster response outcomes. In refractory cases where conventional therapies proved ineffective, combining biologics with traditional drugs can rapidly improve skin lesions and reduce systemic inflammation.26 For example, infliximab has been reported to provide immediate and sustained symptom relief in a child who failed methotrexate monotherapy.27 Two cases treated with secukinumab in combination with oral methotrexate or corticosteroids achieved rapid remission of fever and significant skin lesion improvement.28,29 Consistent with these reports, all four of our refractory GPP patients who received combined therapies demonstrated favorable outcomes. The most common adverse events associated with biologics include nasopharyngitis, upper respiratory tract infections, headache, and hypertension, all of which are generally mild and resolve within a short period.30,31 During follow-up, adverse events were observed only in the traditional drugs group, primarily associated with acitretin, such as dry skin and cheilitis. In contrast, no adverse events were reported in the biologics group, highlighting their safety in pediatric GPP management.
Further, we compared the effectiveness of biologics alone and traditional drugs in the treatment of pediatric GPP. At baseline, there were no significant differences between the two groups in terms of disease severity. While the effective rates and scores at discharge were similar between the two groups, the biologics group demonstrated significantly shorter hospitalization time and pustule clearance time compared with the traditional drugs group. Recurrence is a critical feature of GPP,32 and its management reflects the long-term effectiveness of treatment. Our analysis revealed that the average annual flare frequency per patient significantly decreased after discharge in both the biologics and traditional drugs groups compared with their pre-treatment levels, indicating effective control of recurrence. This finding suggests that pediatric GPP is relatively less stubborn, with a higher potential for long-term remission,25 and highlights the importance of standardized, systemic treatment in maintaining disease stability over time. However, the biologics group exhibited a lower average annual flare frequency and recurrence rate during post-discharge follow-up compared with the traditional drugs group, which was confirmed by survival analysis. Maintenance of response and prevention of flares is the key treatment goal in GPP patients.6 Over the 96-week follow-up period, GPP remained resolved in both groups, although differences became apparent in the eighth week after discharge. In the traditional drugs group, scores began to rebound at this time, suggesting a loss of therapy responses and the onset of relapses in some patients. In contrast, the biologics group showed continued improvement, with almost all patients achieving pustule clearance by the fourth week, maintaining remission until the 24th week, and only a few experiencing recurrence thereafter. Overall, biologics demonstrated superior long-term effectiveness and recurrence control throughout the long-term follow-up period.
Moreover, Olink proteomic analysis of serum samples showed IL-17A and IL-17C were the most significantly upregulated cytokines in GPP compared with healthy children. These findings indicate that biologics, primarily secukinumab, demonstrate faster responses compared with traditional drugs, effectively improving skin symptoms and controlling systemic inflammation while maintaining good tolerability. These results align with current research.22,23 In addition, we explored the impact of different treatments on GPP recurrence and further confirmed that biologics can effectively mitigate clinical relapse. In cases where non-biological therapies are ineffective or a rapid response is required, biologics may offer a compelling treatment option for pediatric GPP. Their advantages include convenient dosing schedules, minimal laboratory monitoring requirements, and targeted therapeutic effects that potentially reduce the risk of end-organ toxicity. In summary, our study conducted a comprehensive comparison between biologic agents and traditional drugs for pediatric GPP, elucidating differences in their clinical efficacy—encompassing both acute flare management and long-term remission maintenance—as well as in their adverse events. Notably, such detailed comparative findings were lacking in prior research focused on pediatric GPP.
Particularly, at present, spesolimab is advocated as the first-line treatment and received expanded approval in China for acute flare of adult GPP and reducing the occurrence of GPP flares in adults and adolescents, as it is the only biologic with robust evidence of its effectiveness and safety.6 However, the clinical application of these advanced therapies, particularly spesolimab, faces significant real-world barriers that extend beyond efficacy. The foremost challenge is the profound economic burden and limited insurance coverage, especially in resource-limited regions like Northwest China we are located, which creates stark disparities in access. Furthermore, diagnostic delays due to the disease’s rarity and regulatory hurdles associated with off-label use in younger children often postpone critical time-sensitive intervention. The infrastructure required for facility-based intravenous administration is also an obstacle. Addressing these challenges necessitates a multi-stakeholder effort involving policymakers, insurers, and healthcare systems to develop innovative access schemes and clinical pathways that ensure equitable delivery of care.
Beyond our findings, several actionable research gaps merit prioritization. First, establishing international prospective registries is imperative to pool longitudinal data on biologics’ long-term safety and efficacy in children, overcoming current sample size limitations. Second, future studies must identify predictive biomarkers of treatment response to guide personalized therapy, moving beyond a one-size-fits-all approach. Third, while logistically complex, head-to-head comparative trials between different biologics and conventional therapies are essential to establish a definitive standard of care. Finally, research should explore the pharmacogenomic drivers of pediatric GPP, which may differ from adults, to uncover novel therapeutic targets. This structured roadmap is crucial to translating current evidence into tangible clinical advancements for this vulnerable population.
Limitations
This study was a single-center retrospective investigation, which inherently lacks the generalizability of multi-center data and the robustness of a prospective design. Second, the patients enrolled were those with moderate-to-severe pediatric GPP, so our findings cannot be extrapolated to the entire pediatric GPP population. Furthermore, due to the limited clinical application of spesolimab in pediatric GPP across China, our current research is constrained by the absence of relevant data on this specific population.
Conclusion
This study reports the clinical characteristics, treatment outcomes, and follow-up data on flares of 61 pediatric inpatients with moderate-to-severe GPP. Most patients present concomitant symptoms, including pruritus, fever, and skin pain. Over 80% of the patients exhibited elevated levels of inflammatory markers (including IL-6 and TNF-α), which reflects systemic involvement in the disease process. Compared with traditional drug therapy for pediatric GPP, biologics offer faster symptom relief in terms of reducing hospitalization time and pustule clearance time and show greater advantages in safety. For patients with a high frequency of flares or a tendency toward recurrence, biologics appear to be a more suitable option for controlling recurrence and maintaining disease remission compared with traditional medications. Our study compared the effectiveness and long-term remission between biologic agents and traditional drugs, and our findings based on real-world data contribute to a better understanding of the clinical features of pediatric GPP and provide insights into optimizing future treatment strategies. Future research should include larger, multi-center studies to validate these findings and further elucidate optimal treatment approaches for pediatric GPP.
Abbreviations
GPP, generalized pustular psoriasis; PV, psoriasis vulgaris; PP, pustular psoriasis; GPPGA, General Psoriasis Physician Assessment of Generalized Pustular Psoriasis; SD, standard deviation; IQR, interquartile range; WBC, white blood cell; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; CK, creatine kinase; LDH, lactate dehydrogenase.
Ethical Approval
This study was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital of Xi’an Jiaotong University (2024-121) on 30 July 2024. Due to the anonymity of patient data, the requirement for informed consent was waived in this study.
Funding
This work was sponsored by grants from Bethune Charitable Foundation [grant number J202301E036], and this work was also sponsored by grants from the Key Research and Development Program of Shaanxi [grant number 2020GXLH-Y-022].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Young KZ, Sarkar MK, Gudjonsson JE. Pathophysiology of generalized pustular psoriasis. Exp Dermatol. 2023;32(8):1194–1203. doi:10.1111/exd.14768
2. Rivera-Díaz R, Daudén E, Carrascosa JM, Cueva P, Puig L. Generalized pustular psoriasis: a review on clinical characteristics, diagnosis, and treatment. Dermatol Ther. 2023;13(3):673–688. doi:10.1007/s13555-022-00881-0
3. Liang Y, Sarkar MK, Tsoi LC, Gudjonsson JE. Psoriasis: a mixed autoimmune and autoinflammatory disease. Curr Opin Immunol. 2017;49:1–8. doi:10.1016/j.coi.2017.07.007
4. Navarini AA, Burden AD, Capon F, et al. European consensus statement on phenotypes of pustular psoriasis. J Eur Acad Dermatol Venereol. 2017;31(11):1792–1799. doi:10.1111/jdv.14386
5. Boehner A, Navarini AA, Eyerich K. Generalized pustular psoriasis - a model disease for specific targeted immunotherapy, systematic review. Exp Dermatol. 2018;27(10):1067–1077. doi:10.1111/exd.13699
6. Choon SE, Foley PA, Asawanonda P, et al. Asia-Pacific consensus recommendations on the management of generalized pustular psoriasis. J Dermatol. 2024;51(12):1579–1595. doi:10.1111/1346-8138.17471
7. Puig L, Choon SE, Gottlieb AB, et al. Generalized pustular psoriasis: a global Delphi consensus on clinical course, diagnosis, treatment goals and disease management. J Eur Acad Dermatol Venereol. 2023;37(4):737–752. doi:10.1111/jdv.18851
8. Fialová J, Vojáčková N, Vaňousová D, Hercogová J. Juvenile generalized pustular psoriasis treated with etanercept. Dermatol Ther. 2014;27(2):105–108. doi:10.1111/dth.12065
9. Chen Y, Xiang X, Wang Z, Miao C, Xu Z. The update of treatment strategies in pediatrics with generalized pustular psoriasis in China. Pediatr Investig. 2023;7(3):191–198. doi:10.1002/ped4.12395
10. Bernardo D, Thaçi D, Torres T. Spesolimab for the treatment of generalized pustular psoriasis. Drugs. 2024;84(1):45–58. doi:10.1007/s40265-023-01988-0
11. Xu Z, Liu Y, Qu H, et al. Clinical characteristics and heterogeneity of generalized pustular psoriasis: a comparative study in a large retrospective cohort. Exp Dermatol. 2024;33(1):e14891. doi:10.1111/exd.14891
12. Burden AD, Bachelez H, Choon SE, et al. The Generalized Pustular Psoriasis Physician Global Assessment (GPPGA) score: online assessment and validation study of a specific measure of GPP disease activity. Br J Dermatol. 2023;189(1):138–140. doi:10.1093/bjd/ljad071
13. Lau BW, Lim DZ, Capon F, Barker JN, Choon SE. Juvenile generalized pustular psoriasis is a chronic recalcitrant disease: an analysis of 27 patients seen in a tertiary hospital in Johor, Malaysia. Int J Dermatol. 2017;56(4):392–399. doi:10.1111/ijd.13489
14. Popadic S, Nikolic M. Pustular psoriasis in childhood and adolescence: a 20-year single-center experience. Pediatr Dermatol. 2014;31(5):575–579. doi:10.1111/pde.12296
15. Zelickson BD, Muller SA. Generalized pustular psoriasis in childhood. Report of thirteen cases. J Am Acad Dermatol. 1991;24(2 Pt 1):186–194. doi:10.1016/0190-9622(91)70025-W
16. Wang Q, Liu W, Zhang L. Clinical features of von Zumbusch type of generalized pustular psoriasis in children: a retrospective study of 26 patients in southwestern China. An Bras Dermatol. 2017;92(3):319–322. doi:10.1590/abd1806-4841.20175536
17. Ding Y, Yi X, Yu N. Serum IgE levels are increased in patients with generalized pustular psoriasis. Clin Exp Dermatol. 2013;38(5):549–552. doi:10.1111/ced.12086
18. Posso‐De Los Rios CJ, Pope E, Lara-Corrales I. A systematic review of systemic medications for pustular psoriasis in pediatrics. Pediatr Dermatol. 2014;31(4):430–439. doi:10.1111/pde.12351
19. Zheng J, Chen W, Gao Y, et al. Clinical analysis of generalized pustular psoriasis in Chinese patients: a retrospective study of 110 patients. J Dermatol. 2021;48(9):1336–1342. doi:10.1111/1346-8138.15958
20. Chen P, Li C, Xue R, et al. Efficacy and safety of Acitretin monotherapy in children with pustular psoriasis: results from 15 cases and a literature review. J DermatolTreat. 2018;29(4):353–363. doi:10.1080/09546634.2017.1395798
21. Sachdeva M, Rankin BD, Mufti A, et al. Management of pediatric generalized pustular psoriasis using biologics: an evidence-based review. J Am Acad Dermatol. 2022;87(2):484–486. doi:10.1016/j.jaad.2021.10.028
22. Ruan SF, Zhang LL, Liu Z, et al. Real-world data on the clinical use of secukinumab in pediatric generalized pustular psoriasis: a 48-week retrospective study. J Am Acad Dermatol. 2023;88(1):243–246. doi:10.1016/j.jaad.2022.04.064
23. Miao C, Chen Y, Wang Z, Xiang X, Liu Y, Xu Z. Real-world data on the use of secukinumab and Acitretin in pediatric generalized pustular psoriasis. J Dermatol. 2023;50(2):258–261. doi:10.1111/1346-8138.16551
24. Wei K, Li P, He X, et al. Clinical efficacy and safety of secukinumab in the treatment of generalized pustular psoriasis in the pediatric population: a systematic review of the literature. Front Med. 2024;11:1377381. doi:10.3389/fmed.2024.1377381
25. Arasiewicz H, Lesiak A, Dec M, Lesniak-Jakubiec L. Successful treatment of a child’s generalized pustular psoriasis with Adalimumab in combination with low-dose Acitretin. Postepy Dermatol Alergol. 2023;40(3):464–466. doi:10.5114/ada.2023.128984
26. Tang MM, Spanou Z, Tang H, Schibler F, Pelivani N, Yawalkar N. Rapid downregulation of innate immune cells, interleukin-12 and interleukin-23 in generalized pustular psoriasis with infliximab in combination with Acitretin. Dermatology. 2012;225(4):338–343. doi:10.1159/000346243
27. Skrabl-Baumgartner A, Weger W, Salmhofer W, Jahnel J. Childhood generalized pustular psoriasis: longtime remission with combined infliximab and methotrexate treatment. Pediatr Dermatol. 2015;32(1):e13–4. doi:10.1111/pde.12457
28. Köstner K, Prelog M, Almanzar G, Fesq H, Haas JP, Hügle B. Successful use of secukinumab in a 4-year-old patient with deficiency of interleukin-36 antagonist. Rheumatology. 2018;57(5):936–938. doi:10.1093/rheumatology/kex510
29. Cordoro KM, Ucmak D, Hitraya-Low M, Rosenblum MD, Liao W. Response to Interleukin (IL)-17 inhibition in an adolescent with severe manifestations of il-36 receptor antagonist deficiency (DITRA). JAMA Dermatol. 2017;153(1):106–108. doi:10.1001/jamadermatol.2016.3490
30. Bodemer C, Kaszuba A, Kingo K, et al. Secukinumab demonstrates high efficacy and a favourable safety profile in paediatric patients with severe chronic plaque psoriasis: 52-week results from a Phase 3 double-blind randomized, controlled trial. J Eur Acad Dermatol Venereol. 2021;35(4):938–947. doi:10.1111/jdv.17002
31. Hsieh CY, Tsai TF. Clinical advances in biological therapy for generalized pustular psoriasis: a review. Expert Opin Biol Ther. 2024;24(1–2):37–50. doi:10.1080/14712598.2024.2309301
32. Choon SE, Lebwohl MG, Turki H, et al. Clinical characteristics and outcomes of generalized pustular psoriasis flares. Dermatology. 2023;239(3):345–354. doi:10.1159/000529274
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Recurrent Hepatocellular Carcinoma: Patterns, Detection, Staging and Treatment
Papaconstantinou D, Tsilimigras DI, Pawlik TM
Journal of Hepatocellular Carcinoma 2022, 9:947-957
Published Date: 3 September 2022
Updated Perspectives on the Diagnosis and Management of Onychomycosis
Falotico JM, Lipner SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1933-1957
Published Date: 15 September 2022
Community-Acquired Stenotrophomonas Maltophilia Infection in a Child: A Case Report and Literature Review
Jiang Z, Ren Y, Zhang C, Yin Y, Li C
Infection and Drug Resistance 2022, 15:5469-5474
Published Date: 19 September 2022
Treatment of Erythrodermic Psoriasis in Children with Secukinumab: A Case Report
Lu X, Wang W
Clinical, Cosmetic and Investigational Dermatology 2023, 16:1977-1981
Published Date: 29 July 2023
Recurrence of Histiocytic Necrotizing Lymphadenitis in Children: A 10-year Multicenter Retrospective Study
Xie YP, Xu YW, Li Y, Zhang H, Xu SS, Lu MN, Chen YP, Tian JM, Huang XF, Liu ZF, Gao ZG, Huang LS
Journal of Inflammation Research 2025, 18:4307-4318
Published Date: 24 March 2025