Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Chronic Obstructive Pulmonary Disease is Not Associated with In-Hospital Mortality in COVID-19: An Observational Cohort Analysis
Authors Toppen W ![]() , Yan P
, Yan P ![]() , Markovic D, Shover CM
, Markovic D, Shover CM ![]() , Buhr RG
, Buhr RG ![]() , Fulcher JA, Tashkin DP, Barjaktarevic I
, Fulcher JA, Tashkin DP, Barjaktarevic I ![]()
Received 19 August 2022
Accepted for publication 24 November 2022
Published 19 December 2022 Volume 2022:17 Pages 3111—3121
DOI https://doi.org/10.2147/COPD.S386463
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
William Toppen,1,* Peter Yan,2,* Daniela Markovic,3 Carolyn M Shover,4,5 Russell G Buhr,4,6 Jennifer A Fulcher,6,7 Donald P Tashkin,4 Igor Barjaktarevic4
1Section of Hospital Medicine, David Geffen School of Medicine, University of California, Los Angeles, CA, USA; 2David Geffen School of Medicine, University of California, Los Angeles, CA, USA; 3Department of Medicine Statistics Core, David Geffen School of Medicine, University of California, Los Angeles, CA, USA; 4Division of Pulmonary, Critical Care and Sleep Medicine, David Geffen School of Medicine, University of California, Los Angeles, CA, USA; 5Offsite Care, Santa Rosa, CA, USA; 6Department of Medicine, Greater Los Angeles Veterans Affairs Health Care System, Los Angeles, CA, USA; 7Division of Infectious Diseases, David Geffen School of Medicine, University of California, Los Angeles, CA, USA
*These authors contributed equally to this work
Correspondence: Igor Barjaktarevic, 10833 Le Conte Avenue, 43118 CHS, Los Angeles, CA, 90095, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is associated with worsened outcomes in COVID-19 (coronavirus disease 2019). However, data remain fraught with heterogeneity and bias from comorbid conditions. Additionally, data on the impact of COPD-specific factors, such as pre-hospital medications and pulmonologist involvement, remain sparse.
Objective: We report a single-center analysis of COPD patients hospitalized with COVID-19 compared to those without COPD. Primary outcomes include ICU admission, mechanical ventilation, and in-hospital mortality.
Methods: We evaluated all patients ≥ 40 years admitted with PCR-confirmed COVID-19 between February 2020 and February 2021. COPD was defined by documented ICD-10 diagnosis of COPD, confirmed smoking history, and active bronchodilator use. We compared outcomes between COPD patients and the remainder of the COVID-19 cohort. Multivariable analyses were adjusted for age, sex, smoking status, and comorbid conditions.
Results: Of 1537 hospitalized COVID-19 patients, 122 (7.9%) carried a diagnosis of COPD. The COPD cohort was older (74 ± 13 vs 66 ± 15 years, P < 0.001) and more often former smokers (P < 0.001). Comorbid conditions including diabetes, cardiovascular disease, and kidney disease were more prevalent in the COPD group (P < 0.001). After adjusting for comorbid conditions, the COPD cohort had higher severity scores and trended towards fewer hospital-free days. Among patients with COPD, pre-hospital use of aspirin was associated with decreased ICU admissions (aHR 0.56, P = 0.049) and mechanical ventilation (aHR 0.25, P = 0.008), while LAMAs (long-acting muscarinic antagonists) were associated with decreased in-hospital mortality (aHR 0.34, P = 0.047). Involvement of pulmonology in pre-hospital management of COPD was not found to significantly affect outcomes.
Conclusion: When corrected for comorbid illnesses, COPD was associated with more severe disease but not with increased ICU admission, mechanical ventilation, or in-hospital mortality rates. Among COPD patients, prehospital treatment with aspirin and COPD-directed therapies were associated with improved outcomes.
Keywords: COVID-19, COPD, survival, critical illness, ARDS
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has infected over 90 million Americans, resulting in over one million deaths in the United States since the beginning of 2020.1 Although mortality rates for COVID-19 have been trending down in the United States concordant with increased vaccination rates, new treatment options, and improved clinical understanding of COVID-19,2–4 at the time of writing, intensive care units (ICUs) worldwide remain congested with patients with severe COVID-19.5,6
Researchers have identified a multitude of risk factors associated with severe COVID-19. Congestive heart failure, diabetes, and chronic pulmonary conditions are strongly correlated with increased in-hospital mortality in COVID-19 patients,7–9 while behavioral risk factors such as previous tobacco use and substance use disorder are linked to worse clinical trajectory.10,11 It stands to reason, then, that chronic obstructive pulmonary disease (COPD), a chronic pulmonary condition most often caused by longstanding tobacco use, would result in worsened outcomes for hospitalized COVID-19 patients.
Consistent with these findings, published literature suggests a greater risk of adverse outcomes in COVID-19 in patients with concomitant COPD diagnosis.12–16 However, the majority of these retrospective studies lack individual patient-level data and details on pre-hospital and hospital management.17 Besides, the need to better understand the association between COPD staging and COVID-19 outcomes, it remains unclear whether adequate outpatient management of COPD prior to the onset of COVID-19 has an impact on clinical outcomes in patients with COPD hospitalized for COVID-related complications. We hypothesized that variations in COPD treatment regimens and objective markers of COPD severity would be associated with differences in outcomes. To this aim, we conducted a retrospective analysis of ever-smokers with formal COPD diagnosis treated with inhaled therapies who were hospitalized with acute COVID-19, focusing on specific endpoints of ICU admission, need for mechanical ventilation, and in-hospital mortality.
Methods
Cohort Specification
We compiled a retrospective cohort analysis of 1537 patients admitted for COVID-19 infection to both UCLA Ronald Reagan and UCLA Santa Monica Medical Centers between February 2020 and February 2021. Eligible patients were at least 40 years old with a positive COVID-19 PCR requiring hospitalization at any level of care (non-monitored, monitored, intermediate, or intensive care unit). COPD cohort was defined as having all three of the following: documented International Classification of Diseases (ICD)-10 diagnosis of COPD (ICD-10 code J44.9), self-reported tobacco smoking history, and self-reported outpatient bronchodilator use. Comorbid conditions were reported by a similar methodology using ICD-10 codes (Supplemental Table 1). All data was prospectively maintained within our institutional registry database and individual chart review of electronic medical record (EMR) was done to complete missing or incomplete data to the extent possible. Outside institution records were reviewed when available via Care Everywhere™ (Epic Systems, Verona, WI) and included if they were more recent than those available in our EMR or relevant to our patient’s medical records (eg, non-established UCLA patients with no prior records at our institution). Each COPD diagnosis was independently reviewed prior to analysis to ensure the above inclusion criteria for COPD categorization were met. Patients were excluded from the COPD group for misdiagnosis of COPD (eg, asthma) or history of lung transplantation.
Outcome Measures
Primary outcomes were ICU admission, need for mechanical ventilation, and in-hospital mortality. Secondary outcomes included supplemental oxygen requirement, length of hospitalization, and NIH (National Institutes of Health) severity scores (defined below).
Supplemental oxygen use was defined by any supplementation of oxygen above ambient atmosphere. Mechanical ventilation was defined by invasive ventilation requiring endotracheal intubation, whereas non-invasive mechanical ventilation was defined by the use of high-flow nasal-cannula systems or positive airway pressure (PAP) ventilation with bi-level or continuous PAP. Ordinal scores from the NIH Severity Scale18 were defined with scores corresponding to the level of COVID severity as referenced in Supplemental Table 2.
Covariate Specification
Available data on COPD treatment was collected for patients within the COPD cohort. We tabulated the prescription of long-acting muscarinic antagonists (LAMA), long-acting beta agonists (LABA), and inhaled corticosteroids (ICS) prior to hospital admission. We additionally collected data on the pre-admission prescription of daily aspirin (ASA) and oral beta-blockers, as these two groups of medications have been associated with improving outcomes in COPD.19,20 Most recent pulmonary function testing (PFT), collected if available, included forced expiratory volume in the first second (FEV1), forced vital capacity (FVC), total lung capacity (TLC), and diffusing lung capacity for carbon monoxide (DLCO). We also reviewed charts for evidence of prior COPD exacerbations that necessitated a prescription of a limited course of oral corticosteroids with or without antibiotics in our COPD cohort. Lastly, we recorded whether patients were being managed by a pulmonologist for their COPD rather than a general practitioner. Prospective data were exported to a REDCap (Vanderbilt University, Nashville, TN) database daily, with “admission” values considered to be those collected at intake (or within 24 hours of hospital admission if intake values were not available).
COVID-19 specific interventions and management were conducted by individual treatment teams without input from study personnel and in accordance with best practice guidelines available at the time of admission and treatment. This study was approved by the University of California, Los Angeles institutional review board (IRB 20–200473), which provided a waiver of consent for all admitted patients with a COVID diagnosis to prevent confounding. Collected patient records were de-identified to protect patient confidentiality and kept in an encrypted institution-provided cloud-based database.
Statistical Analysis
Preliminary comparisons of baseline characteristics between COPD and non-COPD groups were carried out using Welch’s t-test for continuous variables, chi-square test for categorical variables and Mood’s median test for non-normally distributed laboratory test values. Time dependent outcomes were compared by COPD status using the Gray’s test. NIH severity score and length of stay were compared between groups using the Wilcoxon rank sum test. Hospital-free days, as defined by the length of time a patient is alive and not in the hospital within a study window of 28 days, was compared using linear regression models.
The Fine and Gray competing risk regression model was used to evaluate time-dependent outcomes by COPD status before and after adjusting for covariates and results were summarized as unadjusted and adjusted hazard ratios (HR). The following pre-specified covariates were adjusted for in the models: age, sex, tobacco smoking status, history of chronic kidney disease, congestive heart failure, and diabetes. Competing risk models for ICU admission and mechanical ventilation accounted for competing events including in-hospital death and hospital discharge. Competing risk model for in-hospital death was adjusted for hospital discharge as a competing event; meanwhile, the competing model for hospital discharge was adjusted for in-hospital death. Patients who were transferred to another hospital were treated as censored observations. The nominal logistic model was used to evaluate the relationship between COPD status and NIH severity score before and after adjusting for the same covariates as above. We used the nominal logistic model rather than the ordinal logistic model after verifying that assumptions of the ordinal model were not met and the nominal model was, therefore, more appropriate in this data. Results were reported as unadjusted and adjusted odds ratios (OR) using the lowest NIH category as the reference group for computing the odds ratios.
Subset analyses were performed among patients with COPD to assess the relationship between pre-hospitalization COPD treatment variables and specific clinical outcomes. Time dependent outcomes were analyzed using the Fine and Gray competing risk model similarly as above. The NIH severity score, an ordinal outcome, was analyzed using the ordinal logistic model after verifying the proportional odds assumption. For this model, values of the dependent variable were cumulated over lower ordered categories and results were reported as cumulative odds ratios (OR). All models were adjusted for the same covariates as above using the propensity score method. Correlations between pulmonary function tests versus NIH severity score and LOS were assessed using Spearman correlation. The relationship between pulmonary function tests and time-dependent outcomes was performed using similar methods as above. P-value <0.05 were considered statistically significant.
Results
Baseline Demographics and Inflammation in COPD vs Non-COPD Patients
Of the 1537 hospitalized COVID-19 patients in our dataset, 122 (7.9%) had a concomitant diagnosis of COPD as defined by our inclusion criteria (Table 1). COPD patients were significantly older (74 ± 13 vs 6 ± 15 years, P < 0.001) and more likely to be active smokers (10% vs 4%, P = 0.002) or former tobacco users (90.2% vs 24.3%, P < 0.001) compared to their non-COPD counterparts. Comorbidities including diabetes, cardiovascular diseases, and chronic kidney disease were more prevalent in COPD patients, while differences in liver disease were not statistically significant. No appreciable differences in BMI (body mass index) or sex were noted between the groups, and both groups also had similar inflammatory profiles at hospital admission.
 |
Table 1 Baseline Demographics, Comorbidities and Outcomes in COPD vs Non-COPD Patients |
COPD Status and Clinical Outcomes
Preliminary unadjusted analysis demonstrated statistically higher rates of in-hospital mortality among COPD patients (Table 1). ICU admission and mechanical ventilation rates were also increased among patients with COPD but did not reach statistical significance. COPD patients had greater utilization rates for oxygen therapy during hospitalization (95.9% vs 86.1%, P = 0.002). These findings are reflected by increased composite NIH severity scores in COPD patients compared to non-COPD patients (P = 0.009). Secondary metrics for COVID severity including length of hospitalization were also notably higher in patients with COPD (13 vs 10 days, P = 0.009). Both groups were just as likely to receive COVID-specific treatments such as remdesivir, dexamethasone, and other systemic steroids.
After adjusting for covariates including age, sex, smoking status, and comorbidities associated with poor clinical outcomes in COVID-19 (chronic kidney disease, congestive heart failure, and diabetes),7,8,21 patients with COPD maintained higher NIH severity scores and had fewer hospital-free days (Table 2). Despite reaching statistical significance, the effective differences between the two groups were notably smaller after adjusting for covariates.
 |
Table 2 Assessment of COPD Impact on COVID Severity |
Primary outcomes (ICU admission, mechanical ventilation, and in-hospital mortality) were also examined after accounting for competing risks including hospital transfers and discharge (Table 3). Patients with COPD were more likely to experience in-hospital mortality (HR 1.67 [1.09, 2.55], P = 0.018) while hazards for ICU admission and mechanical ventilation were comparable to patients without COPD. However, there was no statistical difference in all three outcomes after adjusting for covariates on top of competing risk analysis. The proportion of censored patients in competing risk analysis fluctuated between 12.93% and 29.51% with in-hospital death having the most censored patients in both patient groups (Supplemental Table 3).
 |
Table 3 Primary Outcomes and Medication Effect Among Patients with COPD |
Pre-Hospitalization COPD Management and COVID-19 Outcomes
The effects of pre-admission COPD management, including both prescribed medications and health system interventions, on COVID outcomes were evaluated among COPD patients in Table 3. Chart review showed that neither management by a pulmonologist nor previous history of COPD exacerbation was associated with any difference in primary outcomes during the index hospitalization (Supplemental Table 4). However, patients prescribed aspirin (ASA) prior to hospitalization had lower hazards of ICU admission (aHR 0.56, P = 0.049) and mechanical ventilation (aHR 0.25, P = 0.008) after propensity score matching (Table 3). Long-acting beta agonists (LABAs) were also associated with decreased hazards of mechanical ventilation (aHR 0.38, P = 0.050) and lower NIH severity scores (aOR 0.45, P = 0.040), while use of long-acting muscarinic antagonists (LAMAs) was correlated with less need for mechanical ventilation and lower in-hospital mortality (aHR 0.18, P = 0.024 and aHR 0.34, P = 0.047, respectively). Only ASA was associated with shorter hospitalizations (11 ± 1 vs 15 ± 2 days, P = 0.040). Inhaled corticosteroid use did not confer any effects on primary or secondary outcomes.
Pre-Hospitalization PFTs as a Predictor of Outcomes in COPD Patients with COVID-19
Pulmonary function tests (PFTs) were available in a subset of our COPD cohort (n = 44; 36.1% of COPD patients). Median time since last known PFT prior to index hospitalization was 1108 days with an inter-quartile range of 1281 days (minimum: 175 days, maximum: 4661 days). In univariable analyses, most recent PFTs obtained prior to hospital admission demonstrated no clear association with COVID outcomes (Figure 1; Supplemental Table 5). No correlation was appreciated between PFT values and NIH severity scores or hospitalization duration.
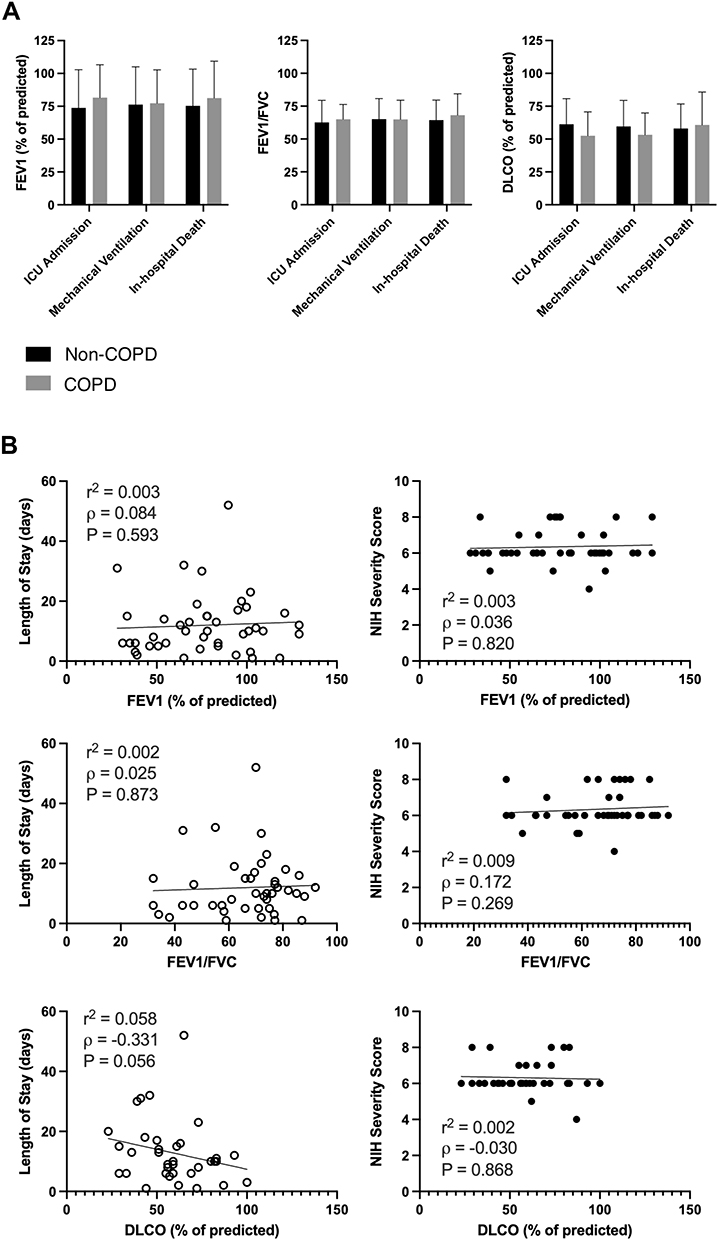 |
Figure 1 Pulmonary Function Test values and outcomes among COPD group. Outcome measurements for COPD patients with pulmonary function test (PFT) values (FEV1, FEV/FVC, DLCO). (A) PFTs among COPD patients stratified by outcome status. (B) Spearman correlations between PFTs and length of stay and NIH severity scores. |
Discussion
In our study of hospitalized patients with COVID-19, while associated with higher severity scores and fewer hospital-free days, after adjustments for comorbid conditions, COPD was not associated with drastically worsened outcomes. Additionally, we attempted to identify signals within the COPD cohort predictive of improved outcomes and found that outpatient use of ASA, LAMA, and LABA prior to hospitalization was associated with better outcomes within the COPD cohort. Analyzing a small subset of those with available data, neither PFT values nor prior management by a pulmonologist correlated with specific COVID outcomes. Our study, therefore, adds an additional and more balanced view to the predominantly held position of COPD being an absolute risk factor for poor outcomes in the setting of COVID-19.
SARS-CoV-2 virus has a clear predilection for pulmonary involvement, leading to COVID-19 pneumonia. Given the resulting inflammation and disruption of gas exchange characteristics of the disease, it stands to reason that patients with pulmonary pathology at baseline are at increased risk for more severe disease and worsened clinical course. Furthermore, because the natural progression of COPD involves chronic inflammation and damage to small airways as well as impaired gas exchange from ventilation/perfusion mismatch, one might expect patients with advanced COPD to fare worse with COVID than those with milder disease due to lack of pulmonary reserve. Multiple studies identified COPD as a significant risk factor for more severe disease and even death.17,22 However, most previous studies do not correct for comorbidities that can worsen COVID outcomes when assessing for associations between COPD and COVID disease severity.7,8,21 One of the earliest studies to address COPD as a risk factor for severe COVID, Guan et al, reported that COPD patients had higher 30-day risks of invasive ventilation, admission to intensive care unit, or death if hospitalized for COVID-19.23 While an early landmark publication in the study of COVID-19, it did not correct for the possible confounding of coexisting illnesses that often accompany COPD diagnoses. Given the large patient population included, especially for so early in the pandemic, this often-cited study frequently comprises a large percentage of subsequent COVID meta-analyses.24,25 As a result, it is possible that the markedly worse outcomes seen in COPD patients in earlier studies may have been over-attributed to COPD itself due to under-recognition of the contribution of associated conditions. Indeed, a long-term national study in South Korea by Jeong et al undertaken concurrently with ours also found COPD to be an independent risk factor for contracting COVID while not increasing risk for disease severity or death, strengthening our findings and highlighting the impact of population-level disease on COVID-related outcomes research.26 Moreover, our cohort reflects a relatively long period of more experienced COVID-19 management, thus the impact of initial gaps in adequate management and global confusion over effective therapeutics earlier in the pandemic is less evident in comparison to earlier studies.27 All patients were managed in a large academic center with tightly coordinated management in accordance with the latest evidence-based approach at the time.
Another plausible explanation for the reduced effects of COPD on COVID outcomes in our study may lie in the prevalence of active tobacco smoking within our dataset. Active smoking has been found to upregulate the ACE2 (angiotensin-converting enzyme 2) receptors used for viral entry into the cell. Additional studies have shown increased viral replication in patients who actively smoked, more so than former smokers.12 Our study population had a relatively small percentage of active tobacco users (<10%) within the COPD cohort, thus further diluting the negative effects of having a concurrent COPD diagnosis and active smoking in COVID patients.
Exciting new research also may further implicate genomic differences in COVID-19 susceptibility throughout different populations. Recent literature suggests polymorphisms of both the ACE and ACE2 genes likely play a significant role in disease severity and mortality.28,29 Indeed, individual alleles in the ACE gene have even been associated with different risks of severe disease. The II allele, which produces the least amount of ACE in tissue and plasma, is associated with the most severe COVID disease courses, whereas the DD allele, producing the most ACE in tissue and plasma, is the allele most associated with asymptomatic disease.30 Fließer et al further added to this understanding by demonstrating between decreased soluble ACE levels in COPD, which may inform on the increased severity of disease seen in COPD patients, though, as our results suggest, perhaps not to the level previously believed.31 While our study design did not allow genomic evaluation, future research may consider correlation of disease severity and genomic analyses.
Further analysis within the cohort of COPD patients yielded several other interesting findings. While COPD severity defined by FEV1% predicted did not appear to influence clinical outcomes, possibly due to the low number of participants with PFTs available, it is interesting to note that we also could not identify any association between the outcomes and specialized pulmonology-based care prior to the admission; having an outpatient pulmonologist was not associated with better outcome, despite having a pulmonologist has previously been shown to affect the optimization of COPD management,32 though biases inherent to database studies may call this finding into question. On the other hand, after propensity score matching to account for confounders, ASA, LAMA, and LABA medications were each associated with significant improvements in length of stay, ICU admission, mechanical ventilation, and even death. This finding is not altogether surprising as the use of these medications could be associated with several biases based on patient compliance with prescribed medication and better outpatient management in comparison to those without inhalers. On the other hand, limited evidence suggests a true positive effect of the inhaled LAMA/LABA since these medications have been found to decrease viral replication in cultured tracheal and nasopharyngeal tissue.33 Interestingly, the latter study also showed decreased viral replication with ICS, although no significant association of ICS therapy with the outcomes was found in our patient population. Lastly, our finding of decreased ICU admission, mechanical ventilation, and length of stay associated with pre-hospital aspirin supports the findings in a recent publication suggesting that early aspirin administration may be associated with improved COVID outcomes.19 Given the inflammatory and prothrombotic nature of COVID with inflammatory disruption of gas exchange as well as thrombotic disease such as pulmonary embolism, it is not surprising that a medication with both anti-inflammatory and antithrombotic properties such as aspirin could be associated with improved outcomes.
Our study has limitations which are important to be emphasized. As a retrospective analysis of a relatively small number of individuals with COPD from a single center, our study is prone to inherent biases and unmeasured confounding that could influence our overall findings. Complete medical and medication history collection has been based on standardized care and may be prone to certain inaccuracies, especially considering the rapidly evolving landscape of COVID-19 management approaches over the period studied. Only a third of the identified cohort had documented PFTs in our database prior to the hospitalization. Missing PFT values are likely a function worse outpatient management due to healthcare disparities and are, therefore, likely not random and cannot be rectified with imputation. COPD diagnosis was also based on ICD-10 coding with its inherent flaws of underreporting COPD diagnoses.34 As a result, a documented history of ever tobacco smoking and use of bronchodilators were added as inclusion criteria to reduce the effect of ICD-10 coding inaccuracies. It is also possible that some individuals with COPD might have been clustered in the “non-COPD” cohort. To account for this, data was prospectively maintained as completely as possible over the study period and only augmented as necessary from the EMR. Additionally, independent investigators reviewed the diagnoses of all patients within the COPD cohort to ensure accuracy. While treatment and management were guided by standard practice at the time, these practices were changing at times daily. The rise of SARS-CoV-2 variants also presents new variables as our study interval likely only captured the Alpha variant. Major variants including Delta and Omicron were not assessed in our study pool as the two variants were not endemic in the United States until March 2021 and December 2021, respectively.35 As a result, COVID-19 specific treatments varied across time and are not able to be standardized across study groups, adding a possible confounding element for which we are unable to account.
Nevertheless, several strengths should be emphasized. This report is based on data from a large and well-characterized database from a large quaternary academic center from the early phase of the COVID-19 pandemic. Medical and supportive management were mandated to follow current CDC guidelines, and our centers did not have any major shortages or system limitations that could impact outcomes. In addition to comparing the outcomes of COPD patients to those without this disease, this study evaluated the association between COPD characteristics (including PFTs, past COPD exacerbations, medications, and provider history) and COVID-19 outcomes. As opposed to multiple other studies identifying COPD based on ICD codes, a method which carries risk of significant inaccuracy,36 we applied additional criteria which included smoking history and use of inhaler therapies, thus maximizing the specificity and allowing for the study to better understand the disease course in those who are more likely to be clinically diagnosed and managed for COPD.
Conclusion
Patients with COPD hospitalized for acute COVID-19 at a major medical center had higher NIH severity scores and longer hospital stays in comparison to those without COPD after adjusting for age and comorbidities. However, there was no difference in mortality or rates of ICU admission and mechanical ventilation. While there was no association between pulmonary function and major outcomes, long-acting muscarinic agonists and aspirin were associated with lower rates of mechanical ventilation. Our findings highlight the complex relationship between SARS-CoV2 infection, underlying patient characteristics and COPD. With continuing waves of new variants and viral mutations, the better understanding we have of COVID-19 and its complex interaction with human diseases, the better we can prepare ourselves to care for our patients and loved ones.
Disclaimers
Drs. Buhr and Fulcher are employed by the Veterans Health Administration. The views in this manuscript do not necessarily represent those of the Department of Veterans Affairs or US Government.
Ethics Approvals
This study was reviewed and approved by the UCLA Institutional Review Board (20-200473) on June 12, 2020.
Funding
This study was not directly supported by any funding source. Dr. Barjaktarevic is supported by NIH/NCATS grant UL1TR001881. Dr. Buhr is additionally supported by NIH/NCATS grant KL2TR001882 and NIH/NHLBI award L30HL134025. Dr. Fulcher is additionally supported by NIH/NIAID grant K08AI124979.
Disclosure
Dr Russell G Buhr reports grants from NIH/NCATS, during the conduct of the study; grants from NIH/NHLBI, personal fees from Viatris/Theravance Biopharma, personal fees from Dynamed/American College of Physicians, outside the submitted work; and Dr. Buhr is employed by the Department of Veterans Affairs. The content of this manuscript does not necessarily represent the views or positions of the US Federal Government. Dr Igor Barjaktarevic reports grants, personal fees from Theravance and Viatris, grants from Amgen, personal fees from Astra Zeneca, personal fees from Verona, personal fees from Inhibrx, personal fees from Grifols, personal fees from GSK, personal fees from Aerogen, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. World Health Organization. WHO coronavirus (COVID-19) dashboard; 2022. Available from: https://covid19.who.int.
2. Horwitz LI, Jones SA, Cerfolio RJ, et al. Trends in COVID-19 risk-adjusted mortality rates. J Hosp Med. 2021;16(2):90–92. doi:10.12788/jhm.3552
3. Xu S, Huang R, Sy LS, et al. COVID-19 vaccination and non–COVID-19 mortality risk — seven integrated health care organizations, United States, December 14, 2020–July 31, 2021. MMWR Morb Mortal Wkly Rep. 2021;70(43):1520–1524. doi:10.15585/mmwr.mm7043e2
4. Elsawah HK, Elsokary MA, Abdallah MS, ElShafie AH. Efficacy and safety of remdesivir in hospitalized Covid-19 patients: systematic review and meta-analysis including network meta-analysis. Rev Med Virol. 2021;31(4):e2187. doi:10.1002/rmv.2187
5. Hospital utilization; 2022. Available from: https://protect-public.hhs.gov/pages/hospital-utilization.
6. French G, Hulse M, Nguyen D, et al. Impact of hospital strain on excess deaths during the COVID-19 pandemic — United States, July 2020–July 2021. MMWR Morb Mortal Wkly Rep. 2021;70(46):1613–1616. doi:10.15585/mmwr.mm7046a5
7. Loffi M, Piccolo R, Regazzoni V, et al. Coronary artery disease in patients hospitalised with Coronavirus disease 2019 (COVID-19) infection. Open Heart. 2020;7(2):e001428. doi:10.1136/openhrt-2020-001428
8. Singh AK, Singh R. Hyperglycemia without diabetes and new-onset diabetes are both associated with poorer outcomes in COVID-19. Diabetes Res Clin Pract. 2020;167:108382. doi:10.1016/j.diabres.2020.108382
9. Aveyard P, Gao M, Lindson N, et al. Association between pre-existing respiratory disease and its treatment, and severe COVID-19: a population cohort study. Lancet Respir Med. 2021;9(8):909–923. doi:10.1016/S2213-2600(21)00095-3
10. Wang QQ, Kaelber DC, Xu R, Volkow ND. COVID-19 risk and outcomes in patients with substance use disorders: analyses from electronic health records in the United States. Mol Psychiatry. 2021;26(1):30–39. doi:10.1038/s41380-020-00880-7
11. Reddy RK, Charles WN, Sklavounos A, Dutt A, Seed PT, Khajuria A. The effect of smoking on COVID‐19 severity: a systematic review and meta‐analysis. J Med Virol. 2020. doi:10.1002/jmv.26389
12. Leung JM, Yang CX, Tam A, et al. ACE-2 expression in the small airway epithelia of smokers and COPD patients: implications for COVID-19. Eur Respir J. 2020;55(5):2000688. doi:10.1183/13993003.00688-2020
13. Acevedo N, Escamilla-Gil JM, Espinoza H, et al. Chronic obstructive pulmonary disease patients have increased levels of plasma inflammatory mediators reported upregulated in severe COVID-19. Front Immunol. 2021;12:678661. doi:10.3389/fimmu.2021.678661
14. Singh D, Mathioudakis AG, Higham A. Chronic obstructive pulmonary disease and COVID-19: interrelationships. Curr Opin Pulm Med. 2022;28(2):76–83. doi:10.1097/MCP.0000000000000834
15. Leung JM, Niikura M, Yang CWT, Sin DD. COVID-19 and COPD. Eur Respir J. 2020;56(2):2002108. doi:10.1183/13993003.02108-2020
16. Pardhan S, Wood S, Vaughan M, Trott M. The risk of COVID-19 related hospitalsation, intensive care unit admission and mortality in people with underlying asthma or COPD: a systematic review and meta-analysis. Front Med. 2021;8:668808. doi:10.3389/fmed.2021.668808
17. Gerayeli FV, Milne S, Cheung C, et al. COPD and the risk of poor outcomes in COVID-19: a systematic review and meta-analysis. EClinicalMedicine. 2021;33:100789. doi:10.1016/j.eclinm.2021.100789
18. Beigel JH, Tomashek KM, Dodd LE, et al. Remdesivir for the treatment of covid-19 — final report. N Engl J Med. 2020;383(19):1813–1826. doi:10.1056/NEJMoa2007764
19. Chow JH, Khanna AK, Kethireddy S, et al. Aspirin use is associated with decreased mechanical ventilation, intensive care unit admission, and in-hospital mortality in hospitalized patients with coronavirus disease 2019. Anesth Analg. 2021;132(4):930–941. doi:10.1213/ANE.0000000000005292
20. Clemente-Moragón A, Martínez-Milla J, Oliver E, et al. Metoprolol in critically ill patients with COVID-19. J Am Coll Cardiol. 2021;78(10):1001–1011. doi:10.1016/j.jacc.2021.07.003
21. Pakhchanian H, Raiker R, Mukherjee A, Khan A, Singh S, Chatterjee A. Outcomes of COVID-19 in CKD patients: a multicenter electronic medical record cohort study. CJASN. 2021;16(5):785–786. doi:10.2215/CJN.13820820
22. Higham A, Mathioudakis A, Vestbo J, Singh D. COVID-19 and COPD: a narrative review of the basic science and clinical outcomes. Eur Respir Rev. 2020;29(158):200199. doi:10.1183/16000617.0199-2020
23. Jie GW, Hua LW, Shi Y, et al. Chronic respiratory diseases and the outcomes of COVID-19: a nationwide retrospective cohort study of 39,420 Cases. J Allergy Clin Immunol Pract. 2021;9(7):2645–2655.e14. doi:10.1016/j.jaip.2021.02.041
24. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, severity and mortality associated with COPD and smoking in patients with COVID-19: a rapid systematic review and meta-analysis. PLoS One. 2020;15(5):e0233147. doi:10.1371/journal.pone.0233147
25. Fang X, Li S, Yu H, et al. Epidemiological, comorbidity factors with severity and prognosis of COVID-19: a systematic review and meta-analysis. Aging. 2020;12(13):12493–12503. doi:10.18632/aging.103579
26. Jeong JS, Kim JS, You YS, Yeom SW, Lee YC. COPD is a risk factor for COVID-19, but does not confer increased severity of the disease. Respir Med. 2021;189:106640. doi:10.1016/j.rmed.2021.106640
27. Chaplin S. COVID‐19: a brief history and treatments in development. Prescriber. 2020;31(5):23–28. doi:10.1002/psb.1843
28. Sieńko J, Kotowski M, Bogacz A, et al. COVID-19: the influence of ACE genotype and ACE-I and ARBs on the course of SARS-CoV-2 infection in elderly patients. Clin Interv Aging. 2020;15:1231–1240. doi:10.2147/CIA.S261516
29. Möhlendick B, Schönfelder K, Breuckmann K, et al. ACE2 polymorphism and susceptibility for SARS-CoV-2 infection and severity of COVID-19. Pharmacogenet Genomics. 2021;31(8):165–171. doi:10.1097/FPC.0000000000000436
30. Gintoni I, Adamopoulou M, Yapijakis C. The impact of ACE and ACE2 gene polymorphisms in pulmonary diseases including COVID-19. In Vivo. 2022;36(1):13–29. doi:10.21873/invivo.12672
31. Fließer E, Birnhuber A, Marsh LM, et al. Dysbalance of ACE2 levels – a possible cause for severe COVID‐19 outcome in COPD. J Pathol Clin Res. 2021;7(5):446–458. doi:10.1002/cjp2.224
32. Keller TL, Wright J, Donovan LM, et al. Association of patient and primary care provider factors with outpatient COPD care quality. Chronic Obstr Pulm Dis. 2022;9(1):55–67. doi:10.15326/jcopdf.2021.0232
33. Yamaya M, Nishimura H, Deng X, et al. Inhibitory effects of glycopyrronium, formoterol, and budesonide on coronavirus HCoV-229E replication and cytokine production by primary cultures of human nasal and tracheal epithelial cells. Respir Investig. 2020;58(3):155–168. doi:10.1016/j.resinv.2019.12.005
34. Gothe H, Rajsic S, Vukicevic D, et al. Algorithms to identify COPD in health systems with and without access to ICD coding: a systematic review. BMC Health Serv Res. 2019;19:737. doi:10.1186/s12913-019-4574-3
35. Aleem A, Akbar Samad AB, Slenker AK Emerging variants of SARS-CoV-2 and novel therapeutics against coronavirus (COVID-19). StatPearls: StatPearls Publishing; 2021. Available from: http://www.ncbi.nlm.nih.gov/books/NBK570580/.
36. O’Malley KJ, Cook KF, Price MD, Wildes KR, Hurdle JF, Ashton CM. Measuring diagnoses: ICD code accuracy. Health Serv Res. 2005;40(5 Pt 2):1620–1639. doi:10.1111/j.1475-6773.2005.00444.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy of mRNA and Inactivated Whole Virus Vaccines Against COVID-19 in Patients with Chronic Respiratory Diseases
Kwok WC, Leung SHI, Tam TCC, Ho JCM, Lam DCL, Ip MSM, Ho PL
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:47-56
Published Date: 19 January 2023
Hospital Admission Rates in Patients with COPD Throughout the COVID-19 Pandemic
Andreen N, Westin J, Vanfleteren LE
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1763-1772
Published Date: 17 August 2023
RETRO-POPE: A Retrospective, Multicenter, Real-World Study of All-Cause Mortality in COPD
Koblizek V, Milenkovic B, Svoboda M, Kocianova J, Holub S, Zindr V, Ilic M, Jankovic J, Cupurdija V, Jarkovsky J, Popov B, Valipour A
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2661-2672
Published Date: 17 November 2023
Real-World Effectiveness Study of Nirmatrelvir-Ritonavir or Molnupiravir in Hospitalized Unvaccinated Patients with Chronic Respiratory Diseases and Moderate COVID-19 at Presentation
Kwok WC, Tam TCC, Ho JCM, Lam DCL, Ip MSM, Ho PL
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:77-86
Published Date: 9 January 2024
The Impact of the COVID-19 Pandemic on Incidence and Short-Term Survival for Common Solid Tumours in the United Kingdom: A Cohort Analysis
Barclay NL, Burkard T, Burn E, Delmestri A, Miquel Dominguez A, Golozar A, Guarner-Argente C, Avilés-Jurado FX, Man WY, Roselló Serrano À, Rosen AW, Tan EH, Tietzova I, Prieto Alhambra D, Newby D
Clinical Epidemiology 2024, 16:417-429
Published Date: 11 June 2024