")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Efficacy of mRNA and Inactivated Whole Virus Vaccines Against COVID-19 in Patients with Chronic Respiratory Diseases
Authors Kwok WC , Leung SHI, Tam TCC, Ho JCM, Lam DCL, Ip MSM, Ho PL
Received 28 October 2022
Accepted for publication 11 January 2023
Published 19 January 2023 Volume 2023:18 Pages 47—56
DOI https://doi.org/10.2147/COPD.S394101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Wang Chun Kwok,1,* Sze Him Isaac Leung,2,* Terence Chi Chun Tam,1 James Chung Man Ho,1 David Chi-Leung Lam,1 Mary Sau Man Ip,1 Pak Leung Ho3
1Department of Medicine, The University of Hong Kong, Queen Mary Hospital, Hong Kong Special Administrative Region, People’s Republic of China; 2Department of Statistics, The Chinese University of Hong Kong, Hong Kong Special Administrative Region, People’s Republic of China; 3Department of Microbiology and Carol Yu Centre for Infection, The University of Hong Kong, Queen Mary Hospital, Hong Kong Special Administrative Region, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pak Leung Ho, Department of Microbiology, The University of Hong Kong, Queen Mary Hospital, 102 Pokfulam Road, Pok Fu Lam, Hong Kong Special Administrative Region, People’s Republic of China, Tel +852 2255 2584, Fax +852 2855 1241, Email [email protected]
Background: While different COVID-19 vaccines have been developed, there has been lack of data on the efficacy comparison between mRNA and inactivated whole virus vaccine among patients with chronic respiratory diseases, including asthma, chronic obstructive pulmonary disease (COPD), and bronchiectasis.
Methods: This was a retrospective case control study on the efficacy of BNT162b2 (mRNA vaccine) and CoronaVac (inactivated whole virus vaccine) against COVID-19 in patients with chronic respiratory diseases. A total of 327 patients were included, with 109 patients infected with COVID-19 matched with 218 patients without COVID-19. The co-primary outcomes were vaccine effectiveness against symptomatic COVID-19, COVID-19-related hospitalization and COVID-19-related respiratory failure. Vaccine effectiveness was calculated using the formula (1-adjusted odds ratio) x 100.
Results: Patients who received at least 2 doses of CoronaVac had lower risk of being hospitalized for COVID-19 and developing respiratory failure than those who did not have vaccination, with adjusted odds ratio (OR) of 0.189 (95% CI = 0.050– 0.714, p = 0.014) and 0.128 (95% CI = 0.026– 0.638, p = 0.012) respectively. Patients who received at least 2 doses of BNT162b2 had lower risk of being hospitalized for COVID-19 and developing respiratory failure than those who did not have vaccination with adjusted OR of 0.207 (95% CI = 0.043– 0.962, p = 0.050) and 0.093 (95% CI = 0.011– 0.827, p = 0.033) respectively. There was no statistically significant difference in the risks of being hospitalized for COVID-19 and developing respiratory failure between patients who received at least 2 doses of CoronaVac or BNT162b2.
Conclusion: BNT162b2 and CoronaVac vaccines are effective in preventing hospitalization for COVID-19 and respiratory failure complicating COVID-19 among patients with chronic respiratory diseases. Patients with chronic respiratory diseases should be encouraged to have COVID-19 vaccination.
Keywords: COVID-19, COPD, asthma, bronchiectasis, vaccine
Introduction
The development of vaccines to prevent SARS-CoV-2 infection has been one of the major breakthroughs in the management of the COVID-19 pandemic. Various COVID-19 vaccines have been developed using different platforms. The efficacy of COVID-19 vaccines has been demonstrated, in large placebo-controlled trials and observational data, to reduce the risk of symptomatic and severe COVID-19.1–10 In Hong Kong, BNT162b2 and CoronaVac vaccines are available for all Hong Kong residents with vaccine pass being developed to encourage vaccination among the general population. The Hong Kong government implemented a territory-wide COVID-19 Vaccination Programme free of charge for all Hong Kong residents since February 2021. Hong Kong residents can receive the vaccines in community vaccination centers, designated general outpatient clinics of the Hospital Authority, designated clinics of the Department of Health, and designated private clinics. Outreach vaccination service and vaccination by visiting medical officers are also provided for residents in residential care homes and nursing homes. For both BNT162b2 and CoronaVac, completion of vaccination is defined as receiving 2 doses of the vaccine while a booster dose was proposed since late 2021 in light of emergence of COVID-19 variant strains. mRNA vaccines were shown to be more relevant to serious adverse events than viral vector and inactivated vaccines according to systematic review. However, there was no solid evidence to suggest that COVID-19 vaccines directly caused serious adverse events. Regarding vaccine efficacy, it was suggested that two mRNA vaccine doses conferred a lesser risk of SARS-COV-2 infection than vaccination with viral vector and inactivated vaccines, while all COVID-19 vaccines were shown to be able to reduce the risk of severe SARS-CoV-2 infection.11 In a study conducted in Singapore, compared to individuals vaccinated with BNT162b2, recipients of CoronaVac and Sinopharm were 2.37 (95% CI 2.29–2.46) and 1.62 (95% CI 1.43–1.85) times more likely to be infected with COVID-19 respectively, while individuals vaccinated with Moderna were 0.42 (95% CI 0.25–0.70) times less likely to develop severe disease.12
COVID-19 vaccination rates in Hong Kong were low initially, as the number of COVID-19 infected cases and mortality remained low until early 2022. The Delta and Omicron outbreaks in early 2022 led to an exponential increase in COVID-19 infected case numbers with rapid rise in mortality, especially among unvaccinated elderly patients who had underlying co-morbidities.13–15
In Hong Kong, the public health care service is provided by Hospital Authority (HA), which manages 43 hospitals and institutions, and 122 outpatient clinics, managing more than 90% of the patients in Hong Kong. HA is also responsible for coordinating outpatient and inpatient care of COVID-19 patients. The majority of patients with COVID-19 were managed in out-patient setting in designated clinics if they were clinically stable patients with moderate to severe disease and those with multiple medical co-morbidities were admitted to airborne infection isolation room (AIIR) with standard, contact, droplet and airborne precautions. The Hospital Authority Central Committee on Infectious Diseases and Emergency Response (CCIDER) issued updated Interim Recommendation on Clinical Management of Adult Cases with Coronavirus Disease 2019 (COVID- 19) regularly to guide the treatment pathway for COVID-19 cases.16 For patients who have mild symptoms but at risk of disease progression and within 5 days of onset of symptoms, ritonavir-boosted nirmatrelvir (Paxlovid) or molnupiravir (Lagevrio) will be started. Remdesivir (Veklury), dexamethasone and tocilizumab could be given to patients with more severe diseases as well.
While there were also data on mRNA and inactivated COVID-19 vaccines among selected patient subgroups, the results were mainly focusing on immunogenicity or safety.17–23 Patients with chronic respiratory disease, including asthma, chronic obstructive pulmonary disease (COPD) and bronchiectasis were at increased risk of adverse outcomes with COVID-19.24–29 There are literature suggesting asthma being a risk factor for severe COVID-19 with respiratory and systemic complications24 and mortality.30 While in COPD, there were reports on increased risks of hospitalization, ICU admission and mortality.31 Although the degree of disease control of asthma and COPD could also contribute to these observations. COVID-19 in patients with bronchiectasis was reported to have higher rates of supplemental oxygen, extracorporeal membrane oxygenation (ECMO), and higher mortality than those without bronchiectasis.32 There has been a lack of evidence comparing mRNA and inactivated COVID-19 vaccines in these patients. In this study, we aimed to assess the clinical efficacy of two COVID-19 vaccines, BNT162b2 and CoronaVac, among patients with chronic respiratory diseases, including asthma, COPD, and bronchiectasis.
Materials and Methods
Study Design and Data Sources
This was a retrospective case-control study on the efficacy of BNT162b2 and CoronaVac against COVID-19 in patients with chronic respiratory diseases. The study period started on 1 January 2022 and ended on 1st May 2022 for confirmed infection, and ended on 15 May 2022. Adult patients aged ≥18 years who were followed-up in the respiratory clinic in Queen Mary Hospital for asthma, COPD and bronchiectasis were included. Patients’ records were accessed through the electronic patient record (ePR) of the Hong Kong Hospital Authority, which consists of the records of all patients with out-patient clinic attendances and hospital admissions. The information available included patient demographics, clinical notes, investigation results and treatment records. Demographic data (age, gender, smoking status) and clinical data / investigations (comorbidities, spirometry results, date of COVID-19, hospitalization and complications from COVID-19, date and dose of COVID-19 vaccination, type of COVID-19 vaccine) were identified from clinical records. Spirometry was performed with CareFusion Vmax® Encore 22 system. Spirometry data were interpreted with the updated spirometric reference values for adult Chinese in Hong Kong.33 The vaccination records until 1 May 2022 were collected from the Clinical Management System (CMS) of the Hospital Authority. The patients infected with Omicron BA.2 (ie, the fifth wave) of COVID19 outbreak in early 2022 were identified.
The study was approved by the Institutional Review Board of the University of Hong Kong and Hospital Authority Hong Kong West Cluster (UW 22–550).
Outcomes
The primary outcome was the number of hospitalizations for COVID-19. The secondary outcomes included symptomatic COVID-19 and respiratory failure complicating COVID-19. Hospitalization for COVID-19 was defined by an admission to acute medical ward for management of COVID-19 for more than 24 hours. COVID-19 was confirmed by at least two positive PCR tests for SARS-CoV-2. Patients who received at least 2 doses of COVID-19 vaccines more than 14 days prior were considered to be fully vaccinated. Those who received only 1 dose of COVID-19 vaccine or 2 doses but less than 14 days from the last dose were considered to be partially vaccinated. Severe COVID-19 was defined as desaturation with saturation of oxygen below 90% within 14 days of confirmed COVID-19, as per World Health Organization COVID-19 Clinical management Living guidance definition.34 The end date of the study period for severe COVID-19 with respiratory failure was set to 14 days before the date of data retrieval to allow at least 14 days of follow-up time for development of severe illness.
Statistical Analysis
The demographic and clinical data were described in actual frequency, mean ± SD or median ± interquartile range. Baseline demographic and clinical data were compared between the patients with or without COVID-19 with two-sided unpaired t-tests. To identify whether COVID-19 vaccination was associated with protection from hospitalization for COVID-19, symptomatic COVID-19 and development of respiratory failure from COVID-19, univariate logistic regression analyses were performed. Multiple logistic regression modeling was used to account for potential confounders including age, gender, smoking status, residential area, underlying respiratory disease and baseline FEV1, calendar time of COVID-19 (biweekly interval, from 1 Jan 2022 onwards) and number of co-morbidities by a multivariate analysis model. The statistical significance was determined at the level of p=0.05. The odds ratios (OR) and 95% confidence intervals for the outcomes in the vaccinated and unvaccinated groups were calculated by logistic regression. When comparing the two vaccinated groups who had different COVID-19 vaccines, CoronaVac was selected to be the control group. Vaccine effectiveness was calculated as (1 - adjusted odds ratio) x 100 in primary analysis (method 1). All the statistical analyses were done using the 26th version of SPSS statistical package. As for sensitivity analysis, we used multivariate Cox-regression to estimate hazard ratio (HR) of developing the composite end points in vaccinated group and unvaccinated group (method 2). Potential confounders listed in logistic regressions were also controlled in Cox-regression.
Results
A total of 895 patients with asthma, COPD, and bronchiectasis were identified from the clinic cohort. Among these 895 patients in the cohort, 109 patients were infected with COVID-19 and 786 were not. Patients below the age of 18, of non-Chinese ethnicity and those who had previous COVID-19 before inclusion, were excluded. The controls, which were uninfected patients with chronic respiratory diseases were identified within the cohort and case/control were matched at 1 to 2 ratio, as matched by age, gender, smoking status and underlying respiratory diagnosis (Figure 1). If more than 2 suitable control subjects fulfilling the inclusion criteria were identified, the subjects with missing information were removed. A total of 327 patients were included in the analysis (109 COVID-19 infected and 218 not infected) (Figure 1). Among the 327 patients included in the analysis, there were 210 (64.2%) male patients, with mean age of 69.9. There were 153 (46.8%) patients with COPD, 51 (15.6%) with asthma and 123 (37.6%) with bronchiectasis. 130 (39.8%) patients did not receive COVID-19 vaccine, 103 (31.5%) received CoronaVac, and 93 (28.7%) received BNT162b2. The baseline demographics of the patients were listed in Table 1. Figure S1 showed the temporal change in percentages of patients vaccinated with CoronaVac and BNT162b2 from 2/2021 to 5/2022. The median time from receipt of first, second, and third doses for COVID-19 in the two vaccine groups was not significantly different (Table 2).
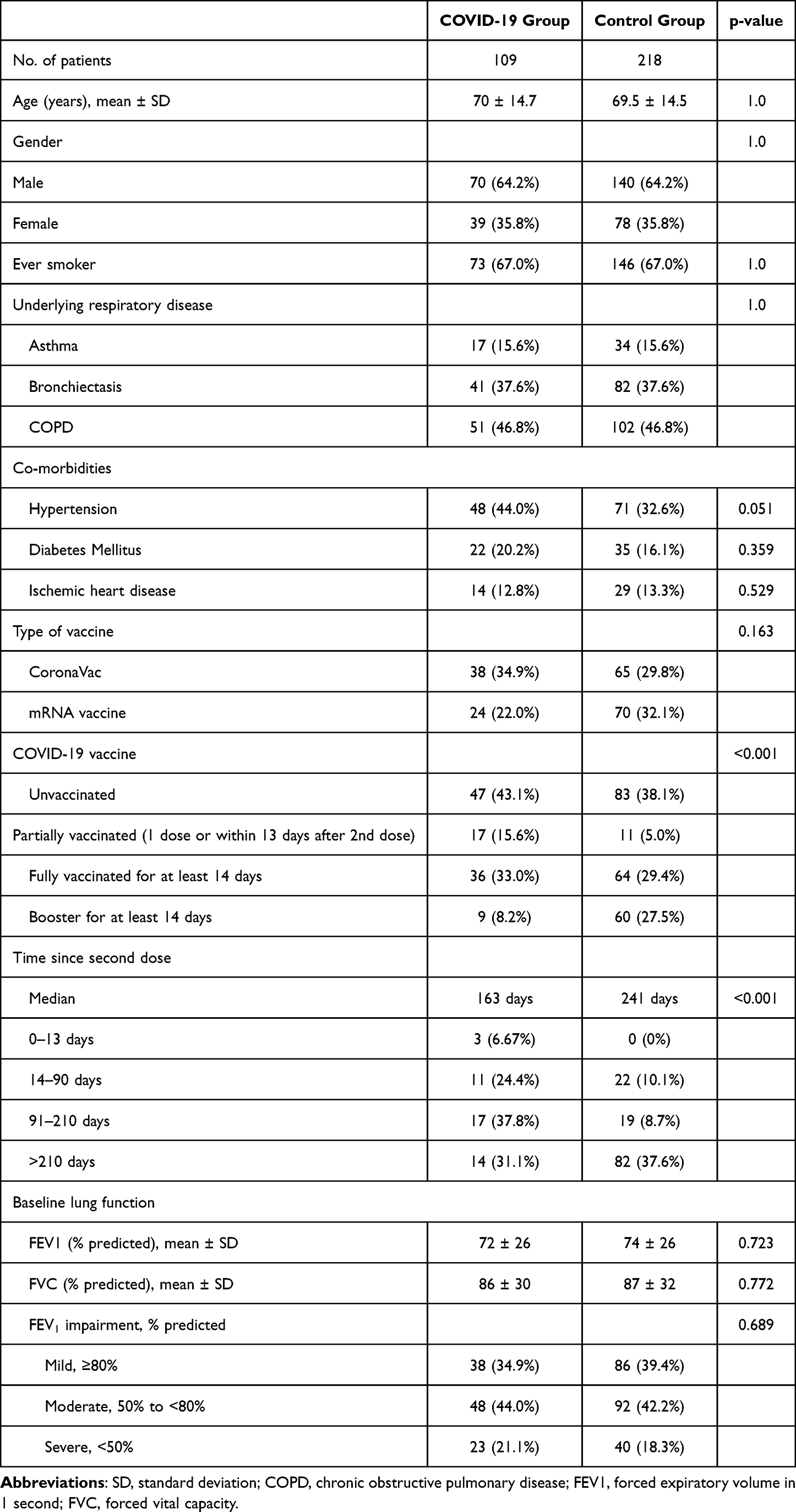 |
Table 1 Baseline Demographic and Clinical Characteristics of Included Patients |
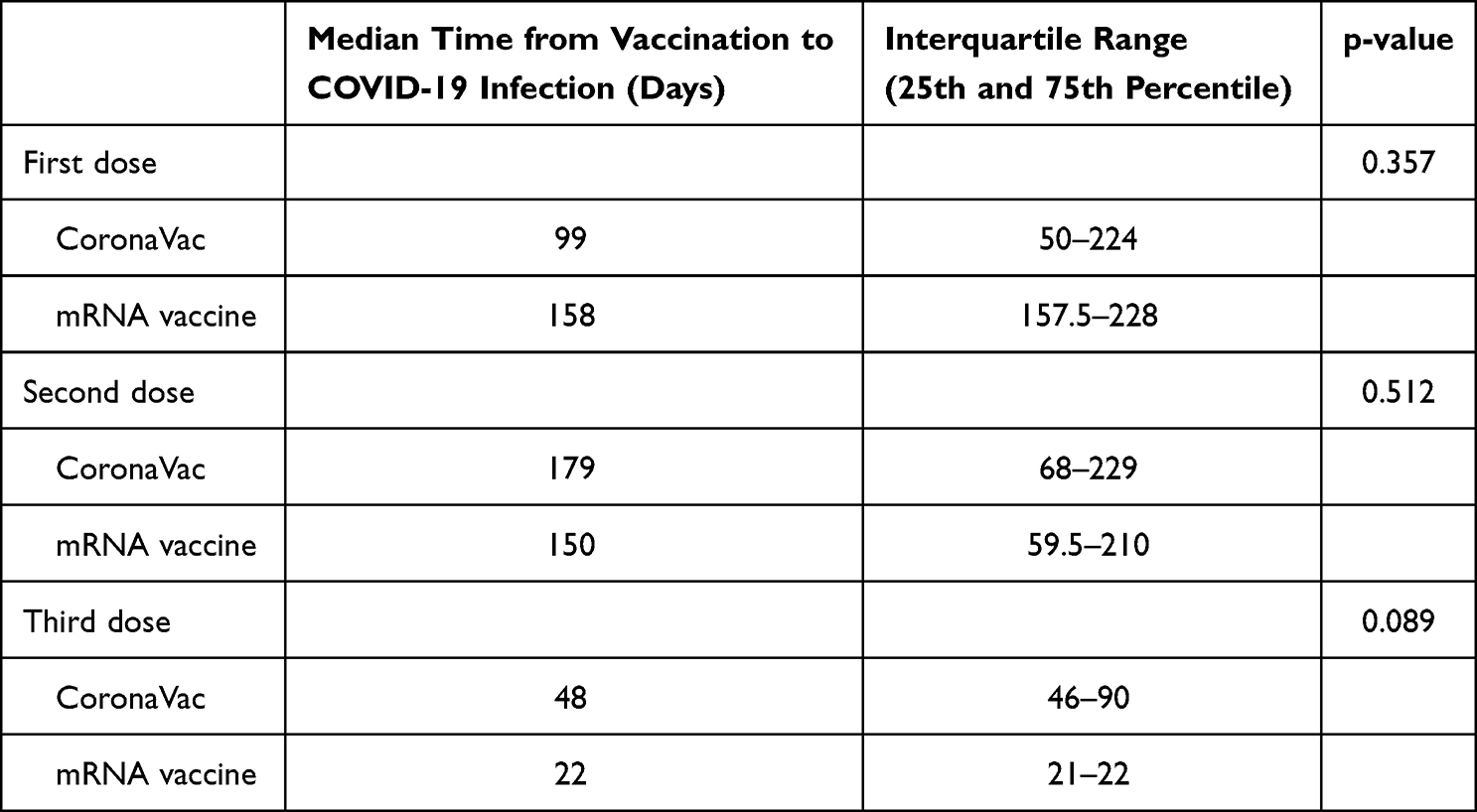 |
Table 2 Time from Vaccination to COVID-19 Infection |
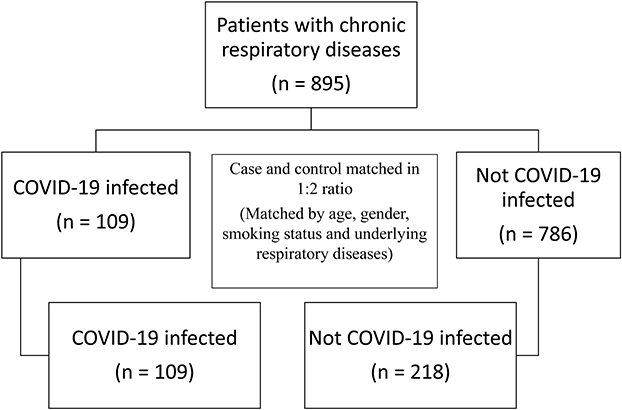 |
Figure 1 Flow diagram for case selection. |
Among the patients infected with COVID-19, 6 received ritonavir-boosted nirmatrelvir, 9 received molnupiravir, 9 received remdesivir, 16 required dexamethasone, 2 required tocilizumab, 5 had add-on interferon Beta-1b.
When comparing subjects who did not have COVID-19 vaccine and those who received at least 2 doses of CoronaVac, there was no difference in the risk of symptomatic COVID-19 at univariate and multivariate analysis. Patients who received at least 2 doses of CoronaVac had lower risk of being hospitalized for COVID-19 and developing respiratory failure than unvaccinated group at univariate and multivariate analysis that were adjusted for confounders including age, gender, smoking status, residential area, underlying respiratory disease and baseline FEV1, calendar time of COVID-19 (biweekly interval, from 1 Jan 2022 onwards) and number of co-morbidities. The results were summarized in Table S1.
The vaccine effectiveness (VE) of at least 2 doses of CoronaVac for preventing symptomatic COVID-19, being hospitalized for COVID-19, and respiratory failure due to COVID-19 was estimated to be 31.7%, 81.1% and 87.2% respectively (Table 3).
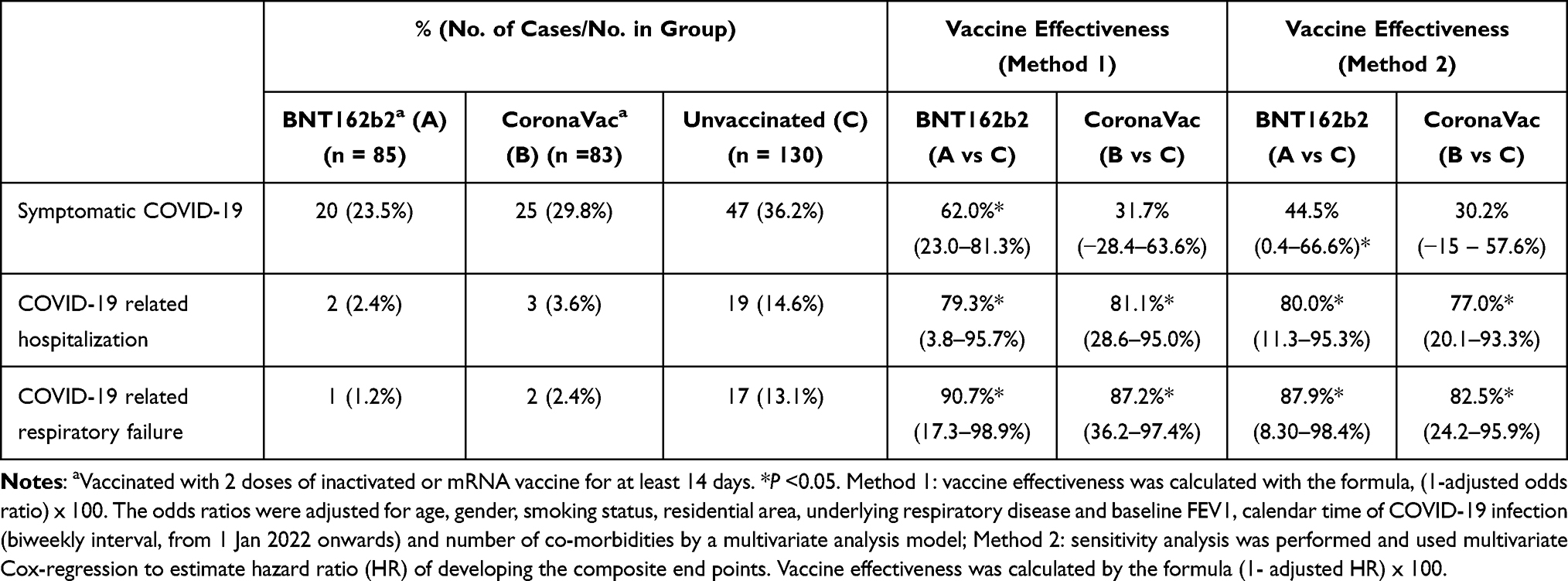 |
Table 3 Comparing Unvaccinated Patients with Those Who Received at Least 2 Doses of Inactivated Whole Virus COVID-19 Vaccine and Those Who Received at Least 2 Doses of mRNA Vaccine |
BNT162b2 reduced the risk of symptomatic COVID-19 with borderline significance at univariate analysis while it was significant at multivariate analysis after adjusting for confounders. Patients in the BNT162b2 group had lower risk of being hospitalized for COVID-19 and developing respiratory failure than the unvaccinated group at univariate and multivariate analysis. The results were summarized in Table S1. The VE for at least 2 doses of BNT162b2 for preventing symptomatic COVID-19, being hospitalized for COVID-19, and respiratory failure due to COVID-19 is estimated to be 62.0%, 79.3% and 90.7% respectively.
The sensitivity analyses using multivariate Cox-regression produced similar results to the primary analysis (Table 3).
Discussion
Our study is the first to provide real world data to suggest that both CoronaVac and mRNA vaccine are effective in preventing hospitalization for COVID-19 and developing respiratory failure upon infection with COVID-19 among patients with chronic respiratory diseases. COVID-19 The findings suggested that both of them can be considered among patients with chronic respiratory diseases, who are at increased risk of developing severe COVID-19.
BNT162b2 is one of the most commonly used COVID-19 vaccines worldwide and is well accepted in many countries. The efficacy of inactivated whole virus vaccines, despite being supported by World Health Organization, has been criticized and until recently some countries did not accept the vaccination record of inactivated whole virus vaccine as the pre-requisite for foreign travelers to enter their country. This could be related to the fact that in some clinical trials involving inactivated whole virus vaccines like CoronaVac, it was reported not to have efficacy as high as mRNA vaccine. Inactivated whole virus vaccines are also not available in most of the Western countries. The criticism on its efficacy and the unavailability made inactivated whole virus vaccine less favored. However, inactivated whole virus vaccines do have the advantages of using a traditional platform in development and manufacture, which is in contrast to mRNA vaccine that is a relatively newer technology and there has not been any long-term safety data on mass vaccination for healthy subjects with mRNA vaccination.
Our data would suggest that inactivated whole virus vaccine, namely CoronaVac, is an efficacious alternative to mRNA vaccine, at least among patients with chronic respiratory diseases, to prevent severe COVID-19 that could lead to hospitalization and respiratory failure. The group of patients included in our study consisted of patients with COPD, asthma and bronchiectasis, in which any respiratory infection can potentially trigger an exacerbation which can lead to respiratory failure or even death. Conducting the study on this group of high risk individuals would be important to assess the efficacy of COVID-19 vaccination, in which the goal of vaccination is to prevent the high risk populations from developing complications and severe infection. Both mRNA and inactivated whole virus vaccines have been well evaluated among healthy subjects regarding efficacy. Among older patients and those with co-morbidities who have increased risk of severe infection, the efficacy of the vaccines is still maintained. A French study suggested that the VE in reducing the risks of COVID-19-related hospitalization ranges from 83% to 97% for patients with different number of co-morbidities. The VE for COVID-19-related hospitalization was at least 90% for those with 1 to 4 comorbidities, while that was 97% for patients without co-morbidities, suggesting that the VE was consistent among patients in different risk groups.35
Another strength of our study is that the efficacy of the vaccines was compared when Hong Kong had the fifth wave of COVID-19 outbreak which was contributed to by the Delta and Omicron variants. The results from our study provide indirect evidence of effectiveness for both mRNA and inactivated whole virus vaccine on the Delta and Omicron variants while the newer variant-specific vaccines are not yet available in the market.
There were local studies on the effectiveness of mRNA and inactivated whole virus vaccine on Omicron BA.2 infection. In a case-control study, both two doses of BNT162b2 and CoronaVac were effective in reducing mortality and severe complications for patients of different age groups, which represented different risk level.36,37
There are a few limitations to our study. First, this study involved only a single center. However, being a tertiary medical center, the respiratory unit receives referrals from all other health care sources. Patients diagnosed with COPD, asthma, and bronchiectasis were managed in a designated respiratory clinic in our center. The patients in this study had comprehensive clinical data available including lung function test results. Second, while the patients were diagnosed with COVID-19 in the fifth wave of outbreak in Hong Kong due to Delta and Omicron variants, there was no further information on the exact variant they were infected with. However, neither BNT162b2 nor CoronaVac were designed for Delta and Omicron variants. The lack of data on the variant strains was not likely a major limitation here as local studies suggested both BNT162b2 and CoronaVac are effective for Omicron variant. The viral load by cycling threshold was not available in all patients in this study, though this is not one of the outcomes in our study. The safety of COVID-19 vaccine was not studied in our study as the overall incidence of major adverse events of COVID-19 vaccines is low. There was a patient who developed Guillain-Barré syndrome after receiving CoronaVac and there were no patients who developed allergic reaction to both vaccines. Nonetheless, the sample size in our study did not give enough statistical power to examine for vaccine safety. A larger population dedicated to assess vaccine safety will be needed to properly examine for vaccine safety, especially after booster dose and among patients who had different vaccines in the initial and booster dose. Our study covered the first 4 months of 2022 with follow up period until 15 May 2022, which was the fifth wave of COVID-19 in Hong Kong, which was the most severe since 2020 with the health care system in Hong Kong being overwhelmed. The COVID-19 situation dampened in subsequent months until the fourth quarter of 2022. The study period should be able to cover the Omicron BA.2 outbreak in Hong Kong while an extended follow-up period could capture the outbreak from other variants.
Conclusion
BNT162b2 and CoronaVac vaccines are effective in preventing hospitalization for COVID-19 and respiratory failure complicating COVID-19 among patients with chronic respiratory diseases. Patients with chronic respiratory diseases should be encouraged to have COVID-19 vaccination.
Abbreviations
AIIR, airborne infection isolation room; CCIDER, Central Committee on Infectious Diseases and Emergency Response; CI, confidence interval; CMS, Clinical Management System; COPD, chronic obstructive pulmonary disease; COVID-19, Coronavirus Disease 2019; ECMO, extracorporeal membrane oxygenation; ePR, electronic patient record; FEV, forced expiratory volume; HA, Hospital Authority; HR, hazard ratio; ICU, Intensive Care Unit; mRNA, messenger RNA; OR, odds ratios; PCR, polymerase chain reaction; SARS‑CoV‑2, severe acute respiratory syndrome coronavirus 2; SD, standard deviation; VE, vaccine effectiveness.
Data Sharing Statement
The data will not be shared as the data are considered property of the Hospital Authority of Hong Kong, which does not allow sharing of data with third party.
Ethics Approval and Informed Consent
The study was approved by the Institutional Review Board (IRB) of the University of Hong Kong and Hospital Authority Hong Kong West Cluster. The requirement for informed consent was waived by the IRB (reference number: UW 22-550). Patient consent was waived in this retrospective study by IRB of the University of Hong Kong and Hospital Authority Hong Kong West Cluster as it is a retrospective study without active patient recruitment while the data were already deidentified. The study was conducted in compliance with the Declaration of Helsinki. Patient data confidentiality was maintained throughout the study.
Consent for Publication
We provided the consent to publish all the relevant materials of the manuscript by International Journal of Chronic Obstructive Pulmonary Disease.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work is supported by internal funding from the Department of Microbiology, University of Hong Kong.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
2. Frenck RW
3. Thompson MG, Stenehjem E, Grannis S, et al. Effectiveness of Covid-19 vaccines in ambulatory and inpatient care settings. N Engl J Med. 2021;385(15):1355–1371. doi:10.1056/NEJMoa2110362
4. Sadoff J, Gray G, Vandebosch A, et al. Safety and efficacy of single-dose Ad26.COV2.S vaccine against Covid-19. N Engl J Med. 2021;384(23):2187–2201. doi:10.1056/NEJMoa2101544
5. Sadoff J, Gray G, Vandebosch A, et al. Final Analysis of Efficacy and Safety of Single-Dose Ad26.COV2.S. N Engl J Med. 2022;386(9):847–860. doi:10.1056/NEJMoa2117608
6. Voysey M, Clemens SAC, Madhi SA, et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet. 2021;397(10269):99–111. doi:10.1016/S0140-6736(20)32661-1
7. Falsey AR, Sobieszczyk ME, Hirsch I, et al. Phase 3 safety and efficacy of AZD1222 (ChAdOx1 nCoV-19) Covid-19 vaccine. N Engl J Med. 2021;385(25):2348–2360. doi:10.1056/NEJMoa2105290
8. Dunkle LM, Kotloff KL, Gay CL, et al. Efficacy and safety of NVX-CoV2373 in adults in the United States and Mexico. N Engl J Med. 2022;386(6):531–543. doi:10.1056/NEJMoa2116185
9. Al Kaabi N, Zhang Y, Xia S, et al. Effect of 2 inactivated SARS-CoV-2 vaccines on symptomatic COVID-19 infection in adults: a randomized clinical trial. JAMA. 2021;326(1):35–45. doi:10.1001/jama.2021.8565
10. Jara A, Undurraga EA, Gonzalez C, et al. Effectiveness of an inactivated SARS-CoV-2 vaccine in Chile. N Engl J Med. 2021;385(10):875–884. doi:10.1056/NEJMoa2107715
11. Fan YJ, Chan KH, Hung IF. Safety and efficacy of COVID-19 vaccines: a systematic review and meta-analysis of different vaccines at phase 3. Vaccines. 2021;9(9):989. doi:10.3390/vaccines9090989
12. Premikha M, Chiew CJ, Wei WE, et al. Comparative effectiveness of mRNA and inactivated whole virus vaccines against COVID-19 infection and severe disease in Singapore. Clin Infect Dis. 2022;75(8):1442–1445. doi:10.1093/cid/ciac288
13. Ma A, Parry J. When Hong Kong’s “dynamic zero” covid-19 strategy met omicron, low vaccination rates sent deaths soaring. BMJ. 2022;377:o980. doi:10.1136/bmj.o980
14. Siu JY, Cao Y, Shum DHK. Perceptions of and hesitancy toward COVID-19 vaccination in older Chinese adults in Hong Kong: a qualitative study. BMC Geriatr. 2022;22(1):288. doi:10.1186/s12877-022-03000-y
15. Chan SM, Chung GK, Chan YH, et al. Resilience and coping strategies of older adults in Hong Kong during COVID-19 pandemic: a mixed methods study. BMC Geriatr. 2022;22(1):299. doi:10.1186/s12877-022-03009-3
16. HA Central Committee on Infectious Diseases and Emergency Response (CCIDER). Interim Recommendation on Clinical Management of Adult Cases with Coronavirus Disease 2019 (COVID-19). CCIDER; 2022.
17. So H, Li T, Chan V, Tam LS, Chan PK. Immunogenicity and safety of inactivated and mRNA COVID-19 vaccines in patients with systemic lupus erythematosus. Ther Adv Musculoskelet Dis. 2022;14:1759720X221089586. doi:10.1177/1759720X221089586
18. Szebeni GJ, Gemes N, Honfi D, et al. Humoral and cellular immunogenicity and safety of five different SARS-CoV-2 vaccines in patients with autoimmune rheumatic and musculoskeletal diseases in remission or with low disease activity and in healthy controls: a single center study. Front Immunol. 2022;13:846248. doi:10.3389/fimmu.2022.846248
19. Ciampi E, Uribe-San-Martin R, Soler B, et al. Safety and humoral response rate of inactivated and mRNA vaccines against SARS-CoV-2 in patients with multiple sclerosis. Mult Scler Relat Disord. 2022;59:103690. doi:10.1016/j.msard.2022.103690
20. Ozakbas S, Baba C, Dogan Y, Cevik S, Ozcelik S, Kaya E. Comparison of SARS-CoV-2 antibody response after two doses of mRNA and inactivated vaccines in multiple sclerosis patients treated with disease-modifying therapies. Mult Scler Relat Disord. 2022;58:103486. doi:10.1016/j.msard.2022.103486
21. Zee JST, Lai KTW, Ho MKS, et al. Serological response to mRNA and inactivated COVID-19 vaccine in healthcare workers in Hong Kong: decline in antibodies 12 weeks after two doses. Hong Kong Med J. 2021;27(5):380–383. doi:10.12809/hkmj219744
22. Sakuraba A, Luna A, Micic D. Serologic response to Coronavirus Disease 2019 (COVID-19) vaccination in patients with immune-mediated inflammatory diseases: a systematic review and meta-analysis. Gastroenterology. 2022;162(1):88–108 e109. doi:10.1053/j.gastro.2021.09.055
23. Li X, Gao L, Tong X, et al. Autoimmune conditions following mRNA (BNT162b2) and inactivated (CoronaVac) COVID-19 vaccination: a descriptive cohort study among 1.1 million vaccinated people in Hong Kong. J Autoimmun. 2022;130:102830. doi:10.1016/j.jaut.2022.102830
24. Kwok WC, Tam AR, Ho JCM, et al. Asthma, from mild to severe, is an independent prognostic factor for mild to severe coronavirus disease 2019 (COVID-19). Clin Respir J. 2022;16(4):293–300. doi:10.1111/crj.13480
25. Rainer L, Bachner F, Eglau K, Ostermann H, Siebert U, Zuba M. Comorbidities and COVID-19 hospitalization, ICU admission and hospital mortality in Austria: a retrospective cohort study. Wien Klin Wochenschr. 2022;134(23–24):856–867. doi:10.1007/s00508-022-02036-9
26. Graziani D, Soriano JB, Del Rio-Bermudez C, et al. Characteristics and prognosis of COVID-19 in patients with COPD. J Clin Med. 2020;9(10):3259. doi:10.3390/jcm9103259
27. Gomez Antunez M, Muino Miguez A, Bendala Estrada AD, et al. Clinical characteristics and prognosis of COPD patients hospitalized with SARS-CoV-2. Int J Chron Obstruct Pulmon Dis. 2021;15:3433–3445. doi:10.2147/COPD.S276692
28. Choi YJ, Park J-Y, Lee HS, et al. Effect of asthma and asthma medication on the prognosis of patients with COVID-19. Eur Respir J. 2021;57(3):2002226. doi:10.1183/13993003.02226-2020
29. Mahdavinia M, Foster KJ, Jauregui E, et al. Asthma prolongs intubation in COVID-19. J Allergy Clin Immunol Pract. 2020;8(7):2388–2391. doi:10.1016/j.jaip.2020.05.006
30. Williamson EJ, Walker AJ, Bhaskaran K, et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584(7821):430–436. doi:10.1038/s41586-020-2521-4
31. Halpin DMG, Rabe AP, Loke WJ, et al. Epidemiology, healthcare resource utilization, and mortality of asthma and COPD in COVID-19: a systematic literature review and meta-analyses. J Asthma Allergy. 2022;15:811–825. doi:10.2147/JAA.S360985
32. Choi H, Lee H, Lee SK, et al. Impact of bronchiectasis on susceptibility to and severity of COVID-19: a nationwide cohort study. Ther Adv Respir Dis. 2021;15:1753466621995043. doi:10.1177/1753466621995043
33. Ip MS, Ko FW, Lau AC, et al. Updated spirometric reference values for adult Chinese in Hong Kong and implications on clinical utilization. Chest. 2006;129(2):384–392. doi:10.1378/chest.129.2.384
34. World Health Organization. COVID-19 Clinical Management Living Guidance. Vol. 3. World Health Organization; 2021:116.
35. Semenzato L, Botton J, Baricault B, et al. Vaccine effectiveness against severe COVID-19 outcomes within the French overseas territories: a cohort study of 2-doses vaccinated individuals matched to unvaccinated ones followed up until September 2021 and based on the national health data system. PLoS One. 2022;17(9):e0274309. doi:10.1371/journal.pone.0274309
36. Yan VKC, Wan EYF, Ye X, et al. Effectiveness of BNT162b2 and CoronaVac vaccinations against mortality and severe complications after SARS-CoV-2 omicron BA.2 infection: a case-control study. Emerg Microbes Infect. 2022;11(1):2304–2314. doi:10.1080/22221751.2022.2114854
37. McMenamin ME, Nealon J, Lin Y, et al. Vaccine effectiveness of one, two, and three doses of BNT162b2 and CoronaVac against COVID-19 in Hong Kong: a population-based observational study. Lancet Infect Dis. 2022;22(10):1435–1443. doi:10.1016/S1473-3099(22)00345-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.