Back to Journals » Journal of Pain Research » Volume 18
Characteristics of the Pediatric Chronic Pain Service in a Developing Country: A Retrospective Study
Authors Kiatchai T ![]() , Mandee S
, Mandee S ![]() , Panchoowong S, Finley GA
, Panchoowong S, Finley GA ![]()
Received 15 August 2025
Accepted for publication 28 November 2025
Published 22 December 2025 Volume 2025:18 Pages 7005—7014
DOI https://doi.org/10.2147/JPR.S555385
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Helen Koechlin
Taniga Kiatchai,1 Sahatsa Mandee,1 Skaorat Panchoowong,1 G Allen Finley2,3
1Department of Anesthesiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, 10700, Thailand; 2Department of Anesthesia, Pain Management and Perioperative Medicine, Dalhousie University, Halifax, NS, B3K 6R8, Canada; 3Center for Pediatric Pain Research, IWK Health, Halifax, NS, Canada
Correspondence: Sahatsa Mandee, Department of Anesthesiology, Faculty of Medicine, Siriraj Hospital, Mahidol University, 2 Wanglang road, Bangkok Noi, Bangkok, 10700, Thailand, Email [email protected]
Objective: This study aimed to describe the need for multidisciplinary management in a pediatric chronic pain service, characteristics of pediatric patients, types of pain management, and outcomes in a tertiary care university hospital in Thailand.
Methods: This retrospective study included pediatric patients aged between 0 and 17 years old receiving chronic pain services, both inpatient and outpatient, between August 2021 and December 2023. Demographic data, primary medical diagnosis, pain diagnosis, pain characteristics, psychological diagnosis, multidisciplinary management, and patient outcomes were collected. Pain-related diagnoses were then coded into the 11th revision of the International Classification of Diseases (ICD-11) of the World Health Organization.
Results: There were 99 patients included in the study. Mean (SD) age of the patients was 11.5 (4.8) years old. Most patients were male sex (60.6%). The most common pain diagnoses were chronic cancer-related pain (43.4%) and chronic neuropathic pain (21.2%). For multidisciplinary management, 46 (46.5%) patients were sent for psychiatric consultation (95% CI 37.0– 56.2), which turned out to be 36 (36.4%) patients who had mental health disorders (95% CI 27.6– 46.2). Fifty-six (56.6%) patients had rehabilitation (95% CI 46.7– 65.9). Twenty (20.2%) patients required both psychiatric and rehabilitation treatments. Gabapentinoids were used in 68 (68.7%) patients. Strong opioids via oral route were reported in 59 (59.6%) patients. Overall, 54 (54.5%) patients were able to be discharged from the service, while 27 (27.3%) patients died.
Conclusion: A significant proportion of children with chronic pain required psychiatric and rehabilitation management.
Keywords: chronic pain, child, pain management, cancer pain, mental health
Introduction
Chronic pain is a significant problem in children and adolescents. A recent systematic review and meta-analysis in 1 million population reported the overall prevalence of chronic non-cancer pain in children and adolescents was 20.8%, and ranged from 6.9% to 25.7% depending on pain types.1 The pain types with highest prevalence were headache and musculoskeletal pain (25.7%). Other types of pain included abdominal, back, multisite/general, and others. Chronic pain can have major impact on quality of life of patient and family, increased risk of depression and anxiety, school absences, and social problems.2 This specific group of patients need specialized healthcare facilities and a multidisciplinary approach that focuses on evaluating, diagnosing, and treating children and adolescents who experience persistent or recurrent pain.3–5
Common causes of pediatric chronic pain were primary headache disorder, musculoskeletal pain, and abdominal pain.1,2 Pediatric pain clinics typically involve a multidisciplinary team of healthcare professionals, such as pain specialists, pediatrician, psychologists, physical therapists, and occupational therapists, who collaborate to achieve the goal of needs in individual patients.6–11 Youth with chronic pain were more likely to show a mental health disorder than youth without chronic pain.12 Mental health disorders in pediatric patients with chronic pain can range between 21% and 60%.12–14 The majority of psychological diagnoses included depressive, dysthymic, bipolar, anxiety, and panic disorders. Other psychological diagnoses were conversion and somatization disorders, suicidal attempts, and post-traumatic stress disorder.13 Chronic pain in youth even increased risks for first lifetime onset of anxiety, depression, and suicidality.15 Psychological treatment was reported to reduce pain severity and improve quality of life with or without pain medication.16
In Thailand, while chronic pain clinics for adults are well established, those dedicated to pediatric chronic pain are still in an early stage of development. To establish effective management, understanding the characteristics and treatment associated with chronic pediatric pain in the setting of a developing country is very important. The primary objective of this study is to describe the need for multidisciplinary management in pediatric chronic pain services in a tertiary care university hospital in Thailand. The secondary objective is to explore characteristics of pediatric patients, types of pain management and outcomes in a pediatric chronic pain service in the same hospital.
Methods
This retrospective study was conducted at the Department of Anesthesiology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. Ethical approval was provided from Siriraj Institutional Review Board (Si 175/2024). The inclusion criteria were pediatric patients aged between 0 and 17 years old who had chronic pain service consultation, both inpatient and outpatient, between August 2021 and December 2023. To maximize the picture of pediatric chronic pain service, there were no exclusion criteria in this study. Informed consent was waived by the ethics committee due to the nature of the retrospective study. Data confidentiality was in compliance with the Declaration of Helsinki.
Institutional Practice
Siriraj Hospital is a tertiary care referral hospital for adult and pediatric patients. Pain service provided in the hospital is divided into acute and chronic pain service, both managed by anesthesiologists. The Acute Pain Service provides specific care regarding acute postoperative and injury pain within 14 days for patients admitted to the hospital. Patients with repeated acute postoperative or injury pain longer than 14 days are then transferred to the Chronic Pain Service. These patients were still diagnosed with acute pain, but the care was provided by the Pediatric Chronic Pain Service. Pediatric patients with chronic pain or difficult-to-manage pain are consulted to the Pediatric Chronic Pain Services from primary physicians who could be surgeons or pediatricians. Newborns with difficult-to-wean from pain medication were consulted from neonatologists. In older children who were able to self-report their pain, pain scores were asked from numerical rating scale or face-pain scale. Pain scores were measured using Children’s Hospital of Eastern Ontario Pain Scale (CHEOPS) for children under 7 years who cannot self-report pain score, and Neonatal and Infant Pain Scale (NIPS) for infants up to 12 months. Although infants and toddlers cannot describe pain characteristics, pain specialists were consulted in those with difficult-to-manage pain. Neuropathic pain in young children is assessed meticulously by physical examination and behavioral observation. Impact of pain, related medical conditions, and functional assessment for sleep, school, social, and sports were assessed in all children as appropriated with age.
The Chronic Pain Service operates 5 days/week by 8 adult pain physicians who previously provided care to both adult and pediatric patients. Due to the different characteristic of pediatric patients, a Pediatric Chronic Pain Service was formally established in August 2021 to care for both in-patient and out-patient persistent pain. The pediatric pain section receives outpatient appointments once a week. The care is provided by two pediatric pain physicians (anesthesiologists; TK and SM), and three pain nurses. After initial assessment by the pain physician, a multidisciplinary team is available upon consultation. It should be noted that our clinic does not have direct access to physical therapy or psychology services – these are assigned through the corresponding medical specialty department. The decision to consult is initiated by the attending pain physician.
Rehabilitation is provided by one of the two pediatric rehabilitation physicians, who may assign a physical therapist. The availability of physical modalities includes desensitization, hydrotherapy, cryotherapy, graded exercise and functional training, heat and cold modalities, orthosis, aroma massage, and electrical therapy—transcutaneous electrical nerve stimulation (TENS), extracorporeal magnetotransduction therapy (EMTT), and peripheral magnetic stimulation (PMS). Psychiatric consultation is provided by the pediatric psychiatry team, of which one psychiatrist has specialized in pain management. A psychologist may then be involved in the care of the patient. Psychological treatment involves cognitive-behavioral therapy (CBT), school intervention, and family counselling. In our institution, psychoeducational interventions were provided by both physical medicine and psychiatric department. All healthcare providers in the hospital (except pediatric psychiatrists and psychologists from the Department of Pediatrics) provide care to both pediatric and adult patients.
Data Collection
We retrospectively collected data from a database that has been prospectively maintained since the formal initiation of a pediatric chronic pain service in the hospital. Demographic data, primary medical diagnosis, pain diagnosis, pain characteristics (nociceptive or neuropathic), psychological diagnosis, and multidisciplinary management were collected. Data during each hospital admission and each outpatient visit were reviewed. Pain-related diagnoses were then coded into the 11th revision of the International Classification of Diseases (ICD-11) of the World Health Organization (WHO).17 The person responsible for coding was a pediatric pain specialist (TK), using the WHO website: https://icd.who.int/browse11/l-m/en/. Discharge outcome was collected on the 120th day after enrollment of the last patient in December 2023.
Sample Size Calculation
Regarding inpatient characteristics of the child admitted with chronic pain, Coffelt et al13 reported the prevalence of psychiatric morbidity as 44% among 3752 children. In our study, we estimated the prevalence of psychiatric morbidity as 0.40, confidence level 0.95, 2-sided interval, and error 0.10. The calculated sample size was expected to be 93 patients.
Statistical Analysis
Descriptive statistics were used to describe demographic data, pain diagnosis, pain management and outcomes. Non-pharmacological and pharmacological management were reported as frequencies (%) with a 95% confidence interval (CI). The CI was calculated using the Wilson Score method. Subgroup analysis for multidisciplinary consultation and pain management was categorized by pain diagnoses. Psychiatric disorder and rehabilitation were compared between pain diagnosis using Chi-square test. Loss to follow-up was described in outcomes. Cancer status was categorized for subgroup analysis for patient outcomes due to the impact on survival. Subgroup analysis stratified by age was conducted for pain diagnosis. The age group was stratified into 0–6, 7–11, and 12–17 years old. Data were analyzed using IBM SPSS Statistics for Windows (version 29.0.2.0; IBM Corp., Armonk, NY, USA).
Results
During the 29-month study period, there were 99 patients included in the study resulting in a total of 285 encounters (188 outpatient visits, 97 inpatient admissions with 3,159 admission days). No participants were excluded or withdrawn due to incomplete data. Mean (SD) age of the patients was 11.5 (4.8) years old. Most patients were male sex (60.6%). Forty-seven (47.5%) patients had malignancy as co-morbidity. Other demographic data are presented in Table 1.
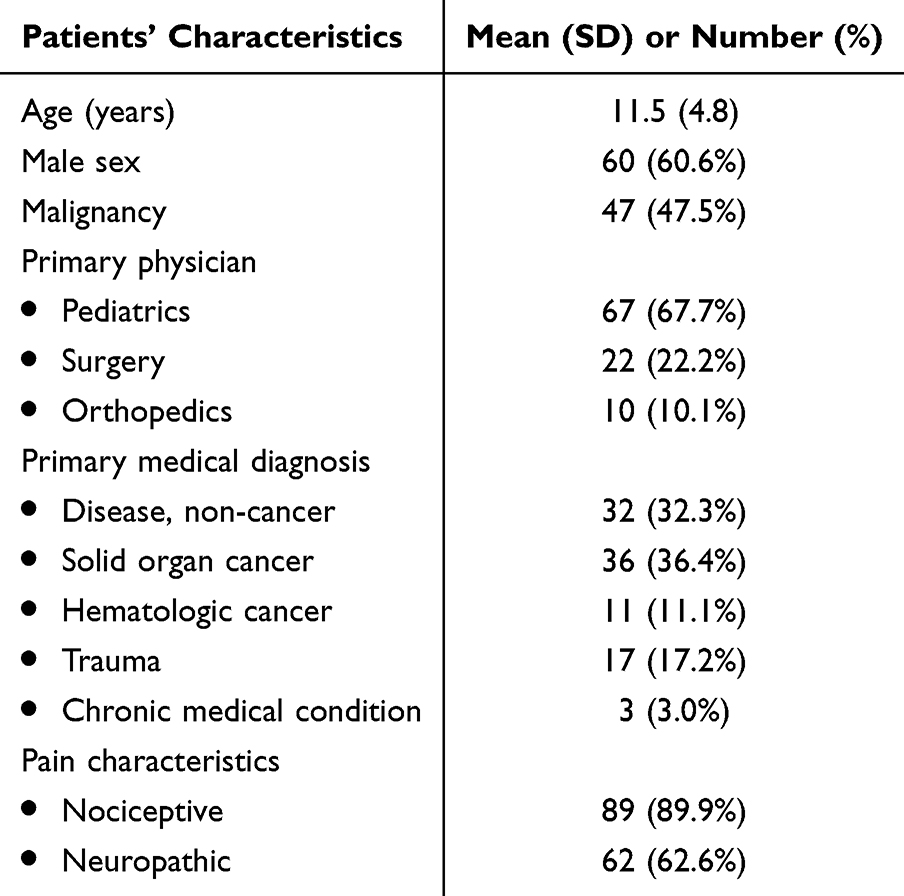 |
Table 1 Demographic Data (N=99) |
There was no patient diagnosed with chronic primary pain during the study period. The most common diagnoses were chronic cancer-related pain (43.4%), chronic neuropathic pain (21.2%), and acute pain (16.2%). Details of pain diagnoses are presented in Table 2.
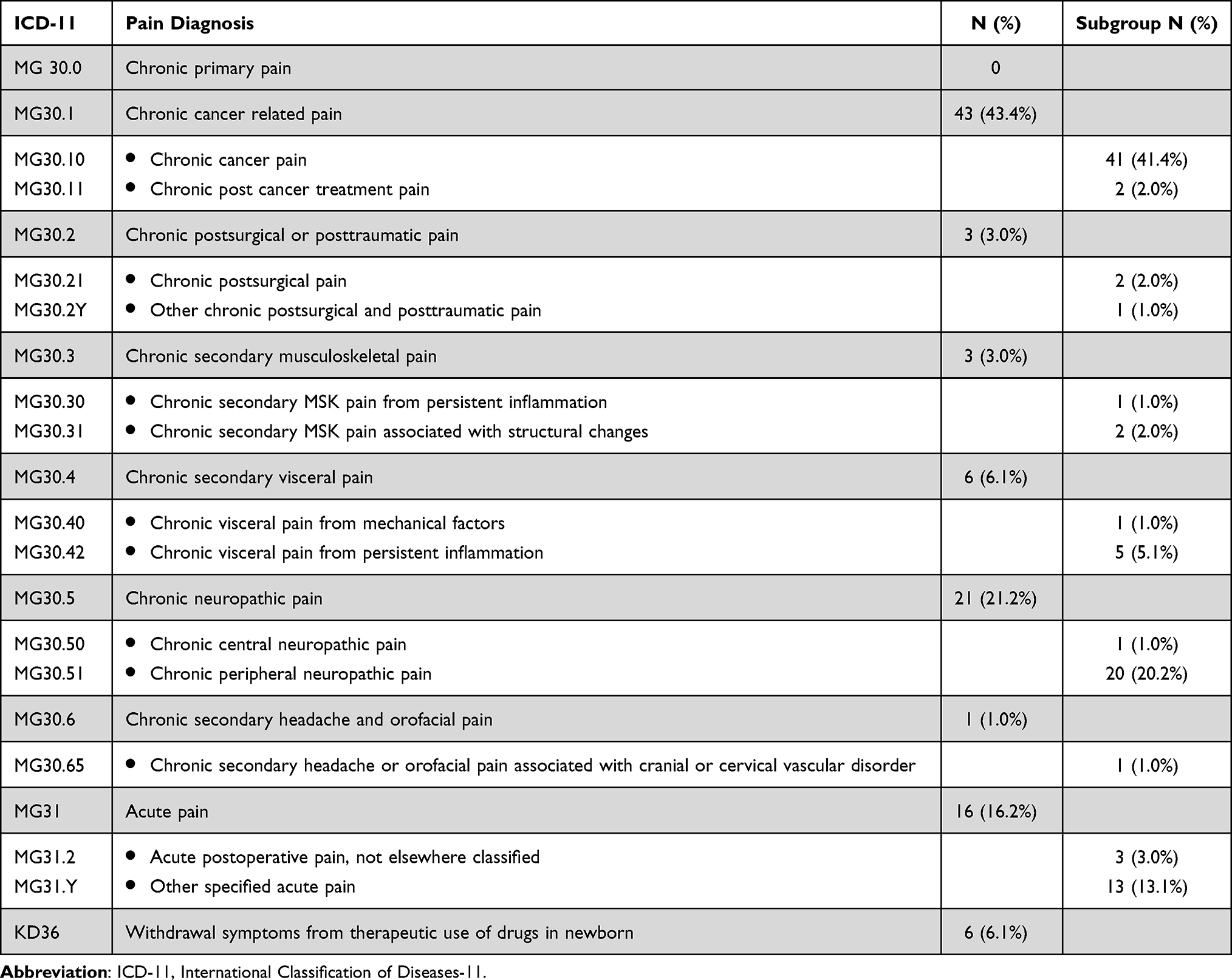 |
Table 2 Pain Diagnosis (N=99) |
Non-pharmacological and pharmacological managements are described in Table 3. Forty-six (46.5%) patients were sent for psychiatric consultation (95% CI 37.0–56.2), which turned out to be 36 (36.4%) patients who had psychiatric disorders (95% CI 27.6–46.2). Ten (10.1%) patients received psychiatric consultation but were diagnosed as having no major psychiatric disorder or a normal reaction. The psychiatric morbidities included adjustment disorder (13 patients, 13.1%), depressive disorder (12 patients, 12.1%), anxiety disorder (4 patients, 4.0%), and others (7 patients, 7.1%). Five patients had multiple psychological diagnoses. Fifty-six (56.6%) patients had rehabilitation (95% CI 46.7–65.9). Twenty (20.2%) patients required both psychiatric and rehabilitation treatments. The most common medications prescribed in this study were gabapentinoids (68.7%). Opioids were prescribed for chronic cancer pain or persistent nociceptive pain. Intravenous patient-controlled analgesia was provided for acute on top of chronic pain. In complicated patients requiring high-dose opioid or uncontrolled mixed nociceptive-neuropathaic pain, opioid rotation and methadone were provided. Among 59 (59.6%) patients who required strong oral opioids, methadone was prescribed in 9 (9.1%) patients. Overall, 54 (54.5%) patients were able to be discharged from the service, while 27 (27.3%) patients died (Table 4). Median (interquartile range) duration of service was 2.3 (0.7, 7.6) months.
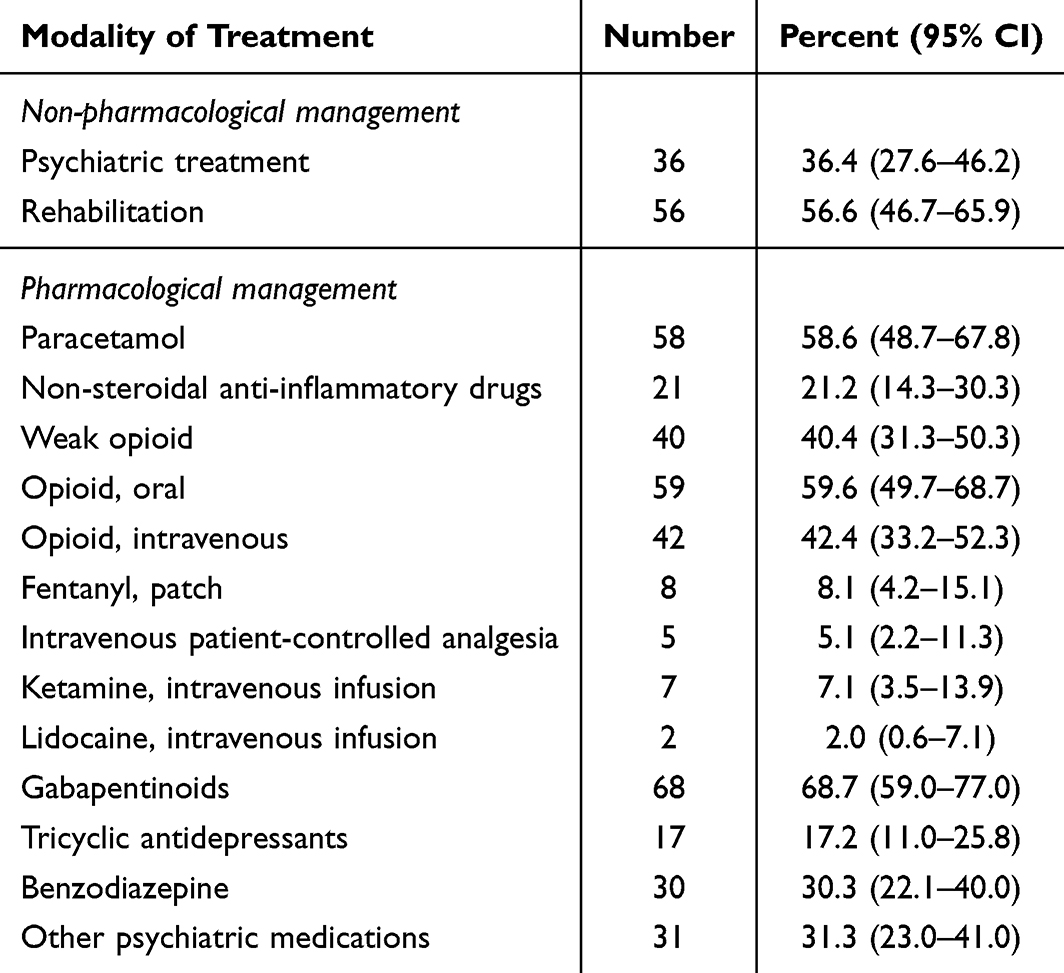 |
Table 3 Non-Pharmacological and Pharmacological Management (N=99). Medications Were Administered via Oral Route if Not Otherwise Specified |
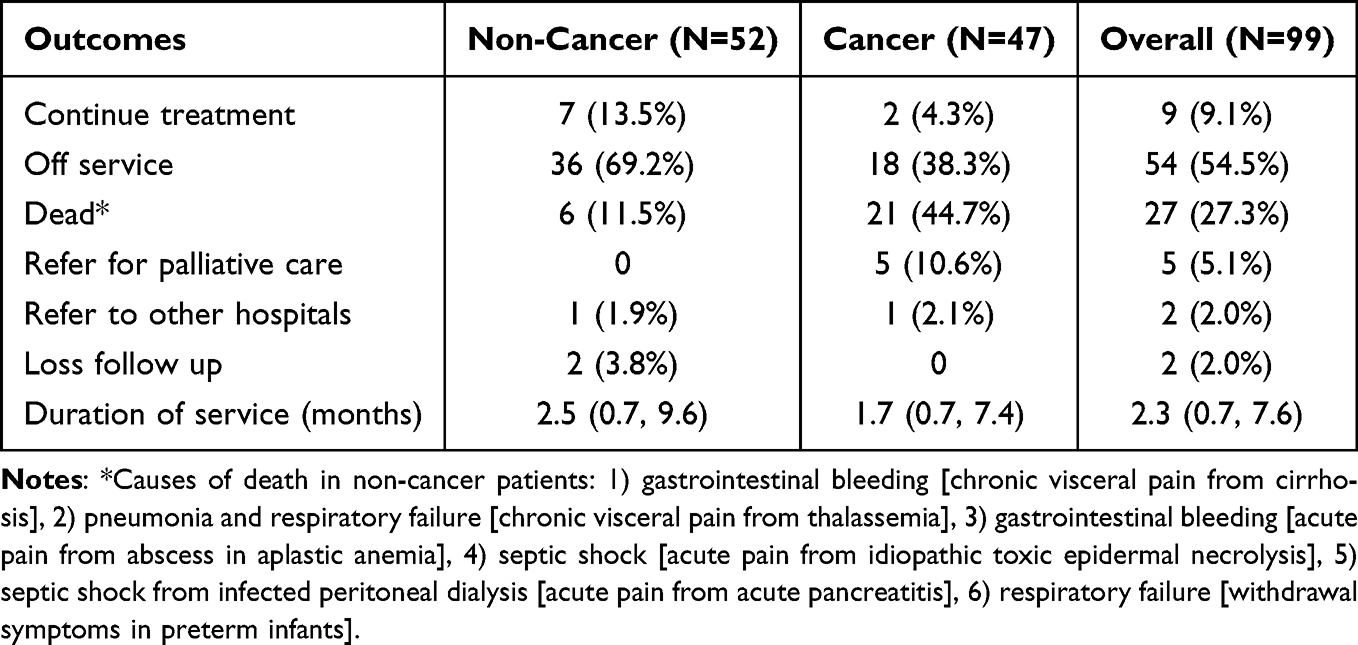 |
Table 4 Outcomes of Patients, Data Presented as Number (%) or Median (Interquartile Ranges) |
Subgroup analysis for psychiatric disorder and rehabilitation treatment was categorized by pain diagnoses and described in Table 5. There was no statistical difference among different pain diagnoses for psychiatric disorders (p = 0.312), while there was statistical difference for rehabilitation consultation (p = 0.001). Types of medication for each pain diagnosis are illustrated in Figure 1. Strong opioids were not utilized in chronic postsurgical pain and chronic secondary musculoskeletal pain. We reported the use of intravenous ketamine or lidocaine infusion in chronic cancer-related pain, chronic secondary visceral pain, chronic neuropathic pain, and acute pain.
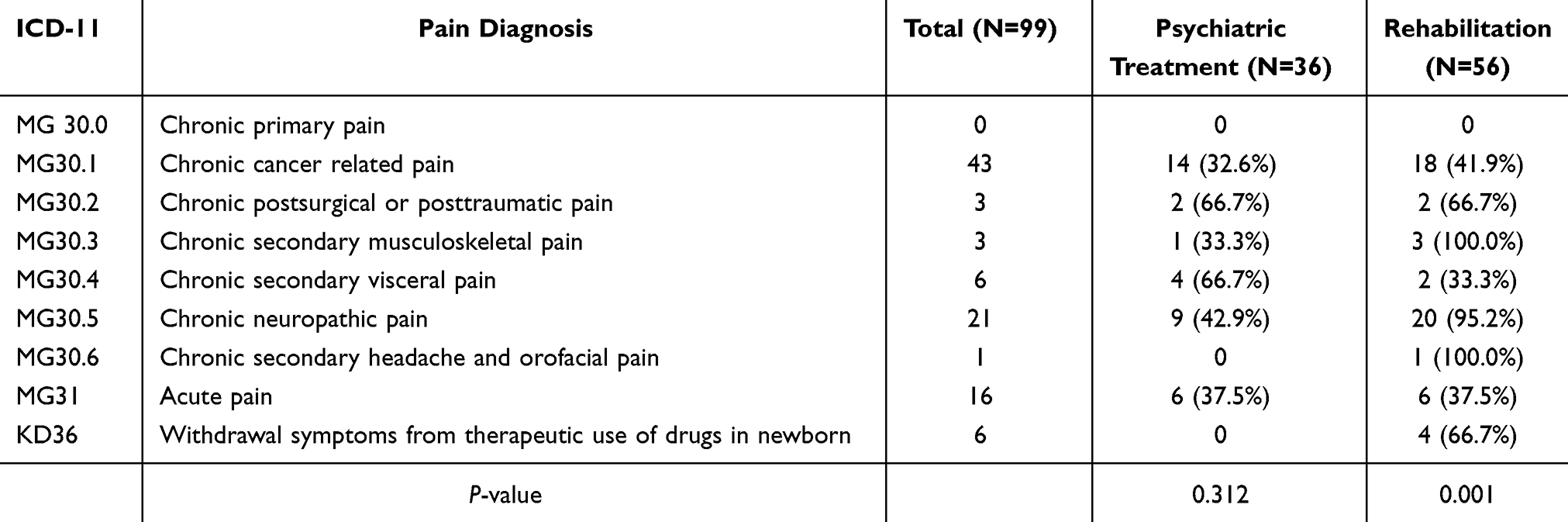 |
Table 5 Multidisciplinary Management Categorized by Pain Diagnosis |
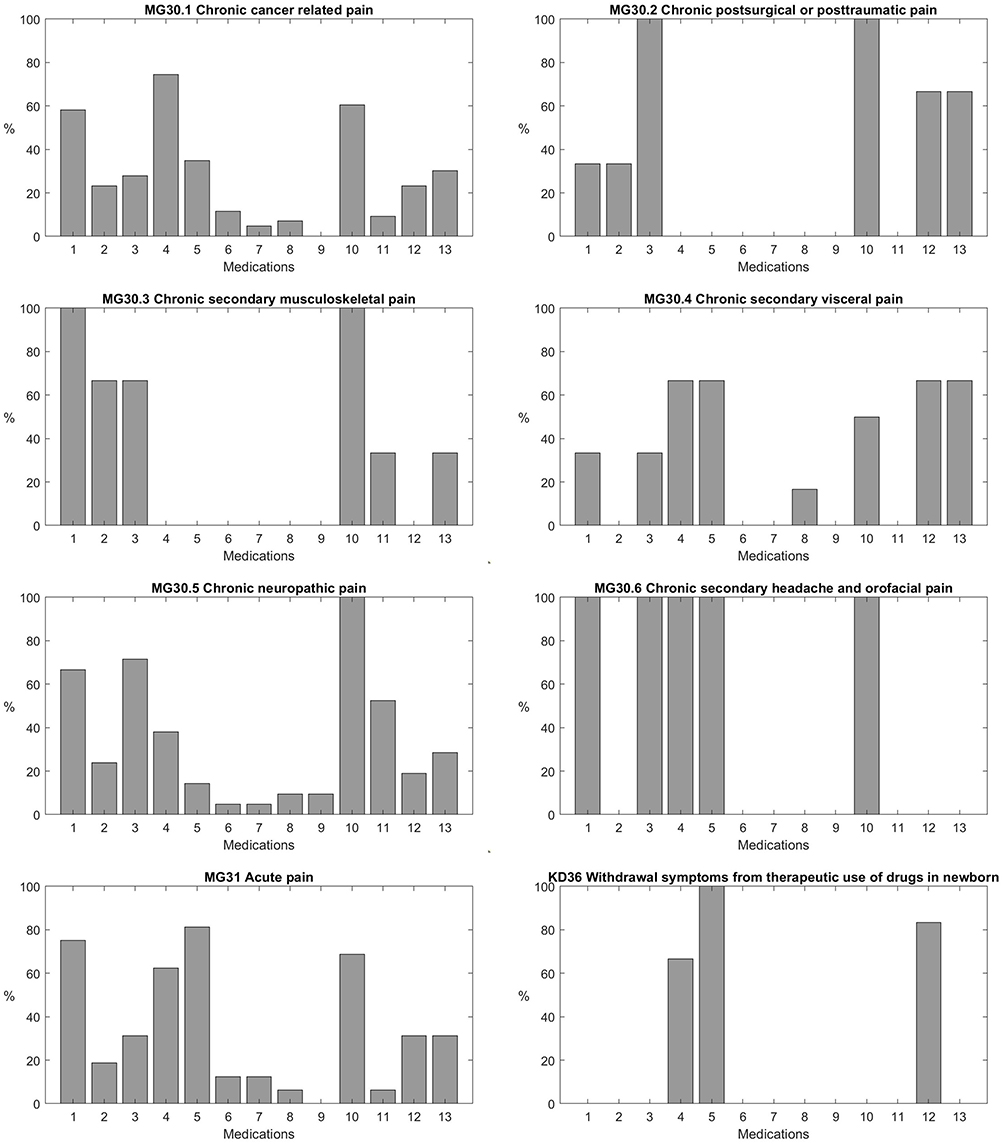 |
Figure 1 Pharmacological management categorized by pain diagnosis. Medications are defined as 1) paracetamol, 2) non-steroidal anti-inflammatory drugs, 3) weak opioid, 4) opioid, oral, 5) opioid, intravenous, 6) fentanyl, patch, 7) intravenous patient-controlled analgesia, 8) ketamine, intravenous infusion, 9) lidocaine, intravenous infusion, 10) gabapentinoids, 11) tricyclic antidepressants, 12) benzodiazepine, 13) other psychiatric medications. |
To illustrate the distribution of age and pain diagnosis, 53 (53.5%) patients were adolescents (Table 6). In very young children age 1–3 years, acute pain was reported in 3 patients (burn 2, toxic epidermal necrolysis 1). In infants <1 year, withdrawal symptoms from therapeutic use of drugs in newborn were reported in 6 patients. The lowest age for patient with chronic cancer pain was 4 years old, while the lowest age for chronic non-cancer pain was 5 years old (chronic peripheral neuropathic pain).
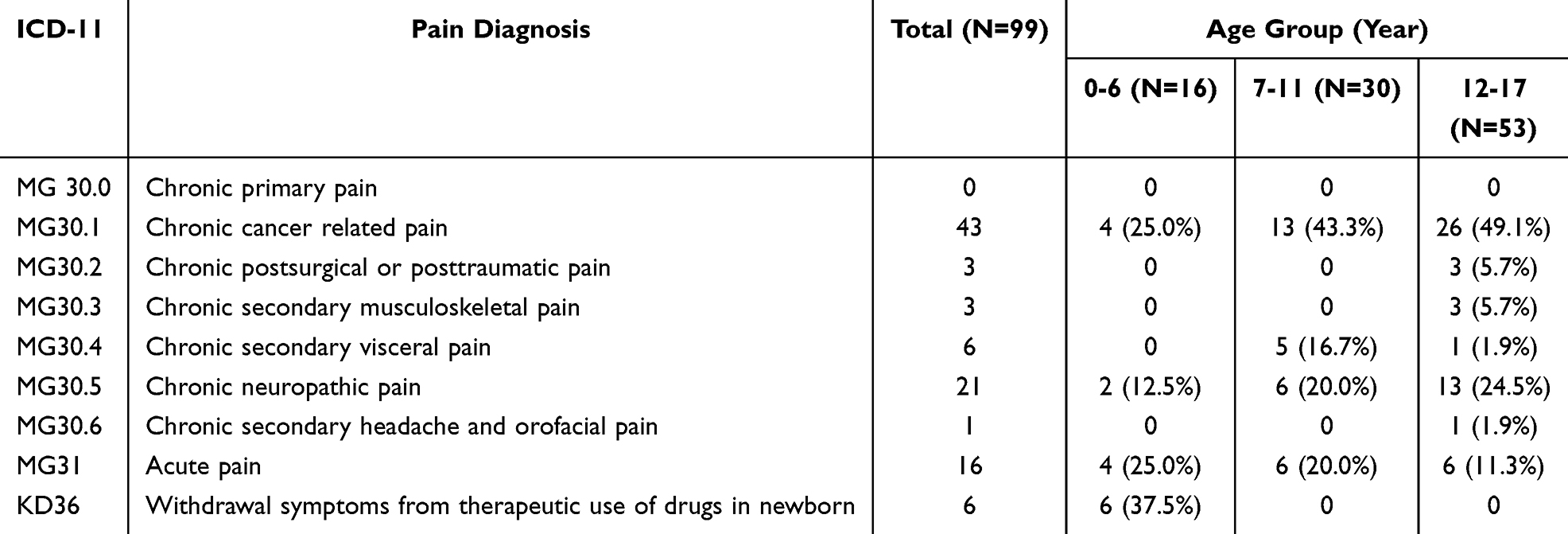 |
Table 6 Pain Diagnosis Stratified by Age Groups |
Discussion
This study describes the characteristics of the Pediatric Chronic Pain Service in a developing country and emphasizes the need for multidisciplinary care in the pediatric chronic pain service. The most common diagnosis was chronic cancer-related pain (43.4%) followed by chronic neuropathic pain (21.2%), corresponding to ICD-11 codes MG30.1 and MG30.5. These characteristics are similar to the report from another major tertiary care service in Thailand that chronic pediatric pain patients consisted of cancer pain (89%) and neuropathic pain (11%).18 The requirement for psychological therapy and rehabilitation was 36.4% and 56.6% of participants, respectively.
However, patients’ characteristics including proportion of pain diagnoses for chronic pediatric pain services in our study differed from what has been reported in the literature. For example, most patients had chronic cancer pain while in developed countries most patients had chronic non-cancer pain.19,20 This could be explained by the fact that procedure-related and cancer pain care are usually provided by acute pain and transitional pain services in North America.21 Since most of the patients had chronic cancer pain, the number of inpatient services in this study were similar to outpatient services. This also highlights the importance of ensuring a clear understanding of the term “chronic pain”. In our setting, patients with pain persisting longer than 2 weeks or requiring special pain care would be accepted on to the Chronic Pain Service, whereas most research focusing on chronic non-cancer pain uses a threshold of 3 months as the defining limit, and usually deals with pain due to nociplastic or neuropathic pain, not ongoing tissue injury. For example, pediatric patients with multiple injuries or extensive burns who are susceptible to chronic post-traumatic pain were also managed initially by the Acute Pain Service and then transferred to the Pediatric Chronic Pain Service. Clinicians, researchers, and administrators must be certain that they are all referring to the same condition when discussing chronic pain or developing new programs.
Among non-pharmacological management, psychological therapy and rehabilitation were provided in 36.4% and 56.6% of participants, respectively. The prevalence of psychiatric comorbidity in this study is similar to 21–60% reported in other studies.12–14 Konijnenberg et al explored children with chronic pain using a clinical and questionnaire model, then categorized into low risk and high risk groups. The model was based on age, social-problem indicators, family structure, parental somatization, and school problems. They reported the different proportions of psychiatric morbidity as 15–27% in the low risk group, and as high as 89–93% in the high risk group.14 Pediatric chronic pain treatment was not based only on pharmacology, but success was achieved by a “3P” multidisciplinary approach (pharmacological, physical/physiological and psychological strategies).3–5 The importance of 3P multidisciplinary approach can be elaborated by an example of a 12-year-old boy diagnosed with enthesitis-related arthritis who experienced chronic musculoskeletal pain since 10 years old. He had severe bilateral hip pain, limiting walking upstairs and school attendance. He received immunosuppressive therapy from pediatric rheumatologists. His pain medications included paracetamol, codeine, gabapentin, tolperisone, and nortriptyline. Psychiatric evaluation revealed that he had undiagnosed autistic spectrum disorder (high function), learning disability (writing) and anxiety disorder. He received psychoeducation to encourage self-esteem, develop social and communication skills, mind-body connections, and appropriate emotional responses. Family counselling and a school conference were arranged. He received strengthening exercises, total contact orthoses for flexible flat feet, and electrical therapy (EMTT). The integrative interdisciplinary approach was proved to be an effective intervention and cost-saving.6 However, the limitation in our institution is that either Child Life support or psychological strategies such as distraction or reframing technique were officially provided only if the patient received psychiatric consultation. This finding emphasizes the importance of a multidisciplinary pain service.
The high proportion of cancer pain and injury-related pain in this study also explained the high proportion of male patients instead of female patients in chronic non-cancer pain. The duration of service was short (2.3 months) due to the high proportion of cancer patients, as the outcome was death in 27.3%. Patients with uncomplicated cancer pain are usually managed by primary physicians, hematologists, oncologists, or the pediatric palliative care service. However, complicated cancer patients are referred to the pediatric pain service. Although patients with chronic non-cancer pain are mostly school age and adolescents, various types of chronic pain were also reported in 3–5 year-old age group.22–24 We did not find chronic pain in children below 4 years of age in our small study.
Interestingly, chronic primary pain was not reported during the study period, this could be explained by the under-recognition of this condition and resulting lack of referrals to the pediatric pain clinic. The Pediatric Pain Service is a lesser known division in the hospital and very little known outside the hospital. As the program is in the early stages of development, a wider advertising campaign to primary care physicians has not taken place. In the setting of a developing county, chronic primary pain is underrecognized in medical practice and so is underreported in the literature.25
This study identified limitations of available medications in our country. Currently, strong intravenous opioids consist of morphine, fentanyl, and pethidine. Fentanyl is only available as the transdermal patch. Strong oral opioids include morphine syrup, morphine tablet (immediate and sustained release), and methadone. Oxycodone and hydromorphone are not available. Due to the concept that children should return to normal activity as much as possible, our goal is that pain should not be the main reason for school absence.2 Even though communications between parents, teachers, and healthcare providers were made, strong opioid administration during school time is still unacceptable in most of the schools in Thailand. With the reasons of limited availability of strong opioid and school acceptance, the use of tramadol and codeine in the pediatric population still exists despite the warning from the Centers for Disease Control and Prevention.26
There are several limitations to this study. First, this is a small, retrospective, single center study in a tertiary care hospital of a developing country. Generalizability may be limited due to the specific setting. Second, characteristics of chronic non-cancer pain among the population are likely to be underreported. Third, we were unable to report the functional outcomes. Although functional outcomes were measured using Pediatric Quality of Life (PedsQL) questionnaire, the tool is not practical to accurately measure the outcome for inpatients. A few patients were restricted to bed due to pain, but most due to other medical instability, monitoring, or parenteral therapy, so it was difficult to assess or encourage movement or physical activity.
Conclusions
The requirement for psychological therapy and rehabilitation was 36.4% and 56.6% of participants in the pediatric chronic pain service in Thailand. Even though cancer-related and neuropathic pain are the predominant causes of pediatric chronic pain in a tertiary-care setting within a developing country and the characteristics of the patients differed from those of developed countries, the requirement for multidisciplinary approaches still remained. In a setting where resources are limited, at-risk patients should be identified for appropriate management.
Abbreviations
CBT, cognitive-behavioral therapy; CHEOPS, Children’s Hospital of Eastern Ontario Pain Scale; CI, confidence interval; EMTT, extracorporeal magnetotransduction therapy; ICD-11, International Classification of Diseases; NIPS, Neonatal and Infant Pain Scale; PedsQL, Pediatric Quality of Life questionnaire; PMS, peripheral magnetic stimulation; SD, standard deviation; TENS, transcutaneous electrical nerve stimulation; WHO, World Health Organization.
Data Sharing Statement
The data generated in this study are available for 2 years upon reasonable request to the corresponding author.
Ethical Approval and Informed Consent
Ethical approval was provided from Siriraj Institutional Review Board (Si 175/2024). Informed consent was waived by the ethics committee due to the nature of the retrospective study. In our institution, Siriraj Institutional Review Board provides ethical approval for the studies in the Faculty of Medicine Siriraj Hospital, Mahidol University. The data confidentiality was in compliance with the Declaration of Helsinki.
Acknowledgments
We thank Miss Arporn Pimtong from the Department of Anesthesiology, Faculty of Medicine Siriraj Hospital for administrative support. We also thank Orawan Supapueng, PhD, from the Department of Research and Development, Faculty of Medicine Siriraj Hospital for statistical advice.
This paper was presented as a poster at the 10th Association of Southeast Asian Pain Societies Congress, held from 2 to 4 May 2025 in Singapore.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chambers CT, Dol J, Tutelman PR, et al. The prevalence of chronic pain in children and adolescents: a systematic review update and meta-analysis. Pain. 2024;165(10):2215–2234. doi:10.1097/j.pain.0000000000003267
2. Friedrichsdorf SJ, Giordano J, Desai Dakoji K, Warmuth A, Daughtry C, Schulz CA. Chronic pain in children and adolescents: diagnosis and treatment of primary pain disorders in head, abdomen, muscles and joints. Children. 2016;3(4):42. doi:10.3390/children3040042
3. Guidelines on the management of chronic pain in children. World Health Organization. Available from: https://www.who.int/publications/i/item/9789240017870.
4. Hechler T, Kanstrup M, Holley AL, et al. Systematic review on intensive interdisciplinary pain treatment of children with chronic pain. Pediatrics. 2015;136(1):115–127. doi:10.1542/peds.2014-3319
5. Rastogi S, McCarthy KF. Complex pain in children and young people; part 2: management. BJA Educ. 2018;18(3):82–88. doi:10.1016/j.bjae.2017.12.001
6. Sommers E, D’Amico S, Goldstein L, Gardiner P. Integrative approaches to pediatric chronic pain in an urban safety-net hospital: cost savings, clinical benefits, and safety. J Integr Complement Med. 2022;28(5):445–453. doi:10.1089/jicm.2021.0296
7. Wren AA, Ross AC, D’Souza G, et al. Multidisciplinary pain management for pediatric patients with acute and chronic pain: a foundational treatment approach when prescribing opioids. Children. 2019;6(2):33. doi:10.3390/children6020033
8. Law E, Fisher E, Eccleston C, Palermo TM. Psychological interventions for parents of children and adolescents with chronic illness. Cochrane Database Syst Rev. 2019;(3). doi:10.1002/14651858.CD009660.pub4
9. Harrison LE, Pate JW, Richardson PA, Ickmans K, Wicksell RK, Simons LE. Best-Evidence for the rehabilitation of chronic pain part 1: pediatric pain. J Clin Med. 2019;8(9):1267. doi:10.3390/jcm8091267
10. Odell S, Logan DE. Pediatric pain management: the multidisciplinary approach. J Pain Res. 2013;6:785–790. doi:10.2147/jpr.S37434
11. Checa-Peñalver A, Lírio-Romero C, Luiz Ferreira EA, et al. Effectiveness of non-pharmacological interventions in the management of pediatric chronic pain: a systematic review. Children. 2024;11(12):1420. doi:10.3390/children11121420
12. Vinall J, Pavlova M, Asmundson GJ, Rasic N, Noel M. Mental health comorbidities in pediatric chronic pain: a narrative review of epidemiology, models, neurobiological mechanisms and treatment. Children. 2016;3(40):40. doi:10.3390/children3040040
13. Coffelt TA, Bauer BD, Carroll AE. Inpatient characteristics of the child admitted with chronic pain. Pediatrics. 2013;132(2):e422–9. doi:10.1542/peds.2012-1739
14. Konijnenberg AY, de Graeff-Meeder ER, van der Hoeven J, et al. Psychiatric morbidity in children with medically unexplained chronic pain: diagnosis from the pediatrician’s perspective. Pediatrics. 2006;117(3):889–897. doi:10.1542/peds.2005-0109
15. Soltani S, Noel M, Bernier E, Kopala-Sibley DC. Pain and insomnia as risk factors for first lifetime onsets of anxiety, depression, and suicidality in adolescence. Pain. 2023;164(8):1810–1819. doi:10.1097/j.pain.0000000000002879
16. Carter BD, Threlkeld BM. Psychosocial perspectives in the treatment of pediatric chronic pain. Pediatr Rheumatol. 2012;10(1):15. doi:10.1186/1546-0096-10-15
17. Rau L-M, Korwisi B, Barke A, Frosch M, Zernikow B, Wager J. 11th revision of the international classification of diseases chronic primary pain diagnoses in children and adolescents: representation of pediatric patients in the new classification system. Pain. 2025;166(2):328–337. doi:10.1097/j.pain.0000000000003386
18. Horatanaruang D, Bunsangjareon P, Krisanaprakornkit W. Pediatric pain service in srinagarind hospital. Srinagarind Med J. 2004;19(3):141–145.
19. Evans S, Taub R, Tsao JC, Meldrum M, Zeltzer LK. Sociodemographic factors in a pediatric chronic pain clinic: the roles of age, sex and minority status in pain and health characteristics. J Pain Manag. 2010;3(3):273–281.
20. Caverius U, Åkerblom S, Lexell J, Fischer MR. Characteristics of children with persistent pain and their parents in a tertiary interdisciplinary pain clinic. Paediatr Neonatal Pain. 2025;7(2):e70005. doi:10.1002/pne2.70005
21. Isaac L, Rosenbloom BN, Tyrrell J, Ruskin DA, Birnie KA. Development and expansion of a pediatric transitional pain service to prevent complex chronic pain. Front Pain Res. 2023;4. doi:10.3389/fpain.2023.1173675
22. Cavestro C, Montrucchio F, Benci P, et al. Headache prevalence and related symptoms, family history, and treatment habits in a representative population of children in Alba, Italy. Pediatr Neurol. 2014;51(3):348–353. doi:10.1016/j.pediatrneurol.2014.05.022
23. Du Y, Knopf H, Zhuang W, Ellert U. Pain perceived in a national community sample of German children and adolescents. Eur J Pain. 2011;15(6):649–657. doi:10.1016/j.ejpain.2010.11.009
24. Khayat A, Algethami G, Baik S, Alhajori M, Banjar D. The effect of using Rome IV criteria on the prevalence of functional abdominal pain disorders and functional constipation among children of the Western Region of Saudi Arabia. Glob Pediatr Health. 2021;8:2333794X211022265. doi:10.1177/2333794X211022265
25. Lo Cascio A, Cascino M, Dabbene M, et al. Epidemiology of pediatric chronic pain: an overview of systematic reviews. Curr Pain Headache Rep. 2025;29(1):71. doi:10.1007/s11916-025-01380-5
26. Maisat W, Yuki K. The perioperative use of codeine and tramadol in pediatric population. Transl Perioper Pain Med. 2025;12(1):694–696. doi:10.31480/2330-4871/198
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Surveying Canadian Pain Physicians’ Attitudes and Beliefs Regarding Medical Cannabis for Chronic Noncancer Pain: A Qualitative Study
Ng JY, Quach H, Phillips MR, Busse JW
Journal of Pain Research 2022, 15:3899-3910
Published Date: 14 December 2022
Radiofrequency Ablation for Chronic Lumbar Zygapophyseal Joint Pain Using a V-Shaped Active Tip Needle: An Observational Retrospective Study
Lo Bianco G, Misseri G, Stogicza AR, Cesare G, Li S, Day M, Kennedy DJ, Schatman ME
Journal of Pain Research 2023, 16:1243-1255
Published Date: 11 April 2023
Interventional Pain Procedures: A Narrative Review Focusing on Safety and Complications. Part 1 Injections for Spinal Pain
Lo Bianco G, Tinnirello A, Papa A, Torrano V, Russo G, Stogicza A, Mercadante S, Cortegiani A, Mazzoleni S, Schatman ME
Journal of Pain Research 2023, 16:1637-1646
Published Date: 18 May 2023
A Randomized, Double-Blind, Placebo-Controlled Trial to Evaluate the Therapeutic Effect of Magnesium-L-Threonate Supplementation for Persistent Pain After Breast Cancer Surgery
Ni Y, Deng F, Yu S, Zhang J, Zhang X, Huang D, Zhou H
Breast Cancer: Targets and Therapy 2023, 15:495-504
Published Date: 25 July 2023
A Review of the Application of Myofascial Release Therapy in the Treatment of Diseases
Lv Y, Yin Y
Journal of Multidisciplinary Healthcare 2024, 17:4507-4517
Published Date: 26 September 2024