Back to Journals » Journal of Pain Research » Volume 18
Changes in Pain Catastrophizing and Related Outcomes Following a Single-Session Empowered Relief Intervention Delivered by Physical Therapists in Workers with Low Back Pain: A Pilot Study
Authors Carrière JS, Coutu MF, Darnall BD ![]() , Léonard G
, Léonard G ![]() , Royer MP, Li MY, Bordeleau M, Durand MJ
, Royer MP, Li MY, Bordeleau M, Durand MJ
Received 15 April 2025
Accepted for publication 21 July 2025
Published 17 September 2025 Volume 2025:18 Pages 4845—4857
DOI https://doi.org/10.2147/JPR.S527830
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Überall
Junie S Carrière,1– 4 Marie-France Coutu,1– 4 Beth D Darnall,5 Guillaume Léonard,3,4,6 Marie-Pier Royer,1,3,4 Mei Yue Li,4 Martine Bordeleau,3,4,6 Marie-José Durand1– 4
1Centre d’Action en Prévention et Réadaptation de l’Incapacité au Travail (CAPRIT), Longueuil, Quebec, Canada; 2Centre de recherche Charles-Le Moyne, Longueuil, Quebec, Canada; 3École de réadaptation, Sherbrooke, Quebec, Canada; 4Faculté de médecine et des sciences de la santé, Université de Sherbrooke, Sherbrooke, Canada; 5Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine, Palo Alto, CA, USA; 6Centre de recherche sur le vieillissement (CdRV), CIUSSS de l’Estrie – CHUS, Sherbrooke, Quebec, Canada
Correspondence: Junie S Carrière, Email [email protected]
Purpose: Low back pain is among the most prevalent pain conditions. Cognitive behavioral therapy reduces the negative effects of low back pain, but access to treatment is limited. Empowered Relief is a 2-hour single-session pain management skills intervention that has demonstrated efficacy at improving pain outcomes in individuals with chronic low back pain. The objectives were 1) to assess the acceptability of Empowered Relief delivered by physical therapists in a sample of French-Canadian workers with low back pain; and 2) to explore changes in pain catastrophizing and other pain-related outcomes following Empowered Relief and physical therapy.
Methods: The study was an uncontrolled prospective pilot trial of Empowered Relief and physical therapy for low back pain. Participants were 63 French-Canadian individuals undergoing physical therapy for subacute and chronic low back pain (< 1 year duration). Participants completed baseline measures of demographic and measure of pain catastrophizing, pain intensity, symptoms of anxiety and depression, physical function and pain interference before taking part in a single-session 2-hour Empowered Relief virtual course. Participants then completed a post-class acceptability questionnaire and a 4-week follow-up questionnaire assessing the same measures as baseline.
Results: A 2-hour single-session of Empowered Relief demonstrated high acceptability among participants. Pain catastrophizing scores reduced by an average of 28 points, with 90% achieving clinically significant change. Participation in Empowered Relief and physical therapy was associated with reductions in pain intensity, and clinically meaningful improvements in symptoms of anxiety and depression, physical function and pain interference at 4-weeks follow-up. Effect sizes were moderate to large, and the largest changes were found in individuals with subacute low back pain.
Conclusion: Empowered Relief, when delivered by physical therapists, may offer a rapid, scalable intervention to complement physical therapy and improve early outcomes in workers with low back pain. The results provide evidence to support a future randomized controlled trial evaluating the effect of Empowered Relief delivered by physical therapists for low back pain.
Plain Language Summary: Low back pain is one of the most common types of pain, and while therapy can help, many people have trouble accessing treatment. Empowered Relief is a one-time, two-hour class that teaches pain management skills and has been shown to help people with chronic low back pain. This study looked at whether the class was well-received by French-Canadian workers with low back pain and whether there were changes in pain and well-being after Empowered Relief combined with physical therapy. We worked with 63 French-Canadian adults receiving physical therapy for low back pain that had lasted less than a year. They answered questions about their pain levels, physical abilities, and mental health before and after taking the class. They also completed a follow-up survey four weeks later. Participants found the Empowered Relief class highly acceptable. After four weeks, they tended to report less pain, improved mood, and better physical function. The biggest improvements were seen in people with subacute (between 1-3 months) back pain. Empowered Relief is a quick and easy way to teach pain management skills early in recovery. These results suggest that it could be a useful tool to complement physical therapy and help people with back pain feel better faster.
Keywords: empowered relief, physical therapy, pain management, low back pain, psychological
Introduction
Low back pain affects approximately 25% of the global population.1,2 Persistent low back pain significantly impacts both physical and mental health and is a leading contributor to long-term disability and rising healthcare expenditures.3 In Quebec, low back pain accounts for over 54% of all musculoskeletal injuries reported to the provincial compensation system and costs over 509 million dollars annually in disability-related costs.4 The Global Burden of Diseases, Injuries, and Risk Factors Study states that low back pain is the leading cause of disability in most countries.5
Physical therapists play an essential role in the management of low back pain and related disability. Research on patterns of care following musculoskeletal injury suggests that 75% of workers who have submitted a time-loss claim for a musculoskeletal injury are treated by a physical therapist within the first 6 weeks post-injury.6,7 The proportion of injured workers who are treated by a physical therapist approaches 90% once the period of work-disability exceeds 6 weeks. Despite their early involvement in rehabilitation, physical therapists often feel ill-equipped to address the psychological aspects of pain, which they recognize are important but often beyond their expertise.8
Cognitive behavioral therapy is an established evidence-based treatment for low back pain in which participants acquire pain management skills.9 Access to cognitive behavioral therapy for pain is often limited by multiple barriers, such as high costs, travel demands, lengthy wait times, limited availability in rural regions, and the time-intensive format of most interventions, which typically require over 16 hours of psychologist involvement.10 These barriers leave many people untreated and perpetuate health disparities.
Empowered Relief is an evidenced-based single-session, 2-hour course designed to rapidly equip individuals with pain self-management skills. Empowered Relief is rooted in cognitive behavioral theory and incorporates pain education, self-regulatory skills and mindfulness principles.11 Empowered Relief targets pain catastrophizing, defined as persistent negative cognitive and emotional responses to actual or anticipated pain,12 that is known to worsen pain and contribute to pain chronicity.13 A three-arm randomized controlled trial (N = 263) evaluated the effectiveness of a single session of Empowered Relief compared to a one-time health education session and a 16-hour psychologist-led cognitive behavioral therapy program in adults with chronic low back pain. Findings showed that Empowered Relief outperformed a single-session health education intervention and was non-inferior to 16 hours of cognitive behavioral therapy at the 3-month follow-up in reducing pain catastrophizing, intensity, interference, bothersomeness, as well as symptoms of depression, anxiety, fatigue, and sleep disturbance.14 A 6-month follow-up indicated further improvements in catastrophizing, bothersomeness, and anxiety.15
To date, published research on Empowered Relief has exclusively been psychologist-delivered and conducted in individuals with chronic pain in the United States.16,17 However, results hold promise for administering Empowered Relief as a brief, low cost, low burden complementary treatment offered by a variety of trained clinicians and as early as possible in the pain treatment process to help curb pain chronicity.18,19 This study was the first to implement Empowered Relief delivered by physical therapists (rather than psychologists) outside of the United States to individuals with pain lasting less than one year. Participants consisted of French-Canadian workers in physical therapy for occupational low back pain lasting between 4 weeks and 12 months. This study had two goals: 1) to assess the acceptability of Empowered Relief delivered by physical therapists to French-Canadian workers with low back pain; and 2) to explore changes in pain catastrophizing and other pain-related outcomes following Empowered Relief in combination with physical therapy. We hypothesized high mean participant ratings (>80%) based on previous research.11,18 We hypothesized there would be a significant decrease in pain catastrophizing following Empowered Relief and physical therapy at 4-week follow-up. We also hypothesized that scores on measures of pain intensity, physical function, pain interference and symptoms of anxiety and depression would improve by 4-week follow-up.
Materials and Methods
Study Design and Participants
The study was an uncontrolled prospective pilot trial of Empowered Relief and physical therapy for low back pain. Data were gathered at three distinct time points: prior to treatment (baseline), one week after the intervention, and four weeks post-intervention. Participants were recruited from private physical therapy clinics across Quebec, where they were receiving care for work-related low back injuries. Physical therapists participating in the study handed out brochures that outlined the study’s procedures and invited individuals to authorize follow-up contact from the research team. Potential participants who provided written authorization were contacted by the research coordinator via telephone to undergo screening for eligibility based on inclusion and exclusion criteria. An a priori power analysis was conducted using G*Power version 3.1.9.720 to estimate the sample size needed to test the study’s hypotheses. Results showed that a sample size of 52 participants would be required to detect a moderate effect size with 80% power at a significance level of α =0.05. Inclusion criteria included: (1) non-specific work-related low back pain, (2) injury sustained 1–12 months prior, (3) participation in a physiotherapy program (4) currently absent from regular job, (5) French fluency, (6) ability to attend an online class and complete web-based surveys. Exclusion criteria included: (1) severe spinal pathology or any medical contraindications, (2) Previous participation in Empowered Relief. Eligible individuals provided freely given, informed consent with research staff over the phone, after which they provided an electronic signature to the consent form emailed to them.
One week prior to the intervention, participants completed a baseline survey which included information relating to their demographic, physical and psychological characteristics (see section 2.2). The psychological questionnaires included in the study are known correlates of pain and disability.21–23 Participants then took part in the treatment intervention (Empowered Relief; described below), delivered as an individual or group class using “Zoom” (Zoom Video Communications, California, United States) or “Teams” (Microsoft, Washington, United States). Within a week following the intervention, participants completed a post-class questionnaire assessing the acceptability class and its virtual format. At 4-week follow-up, participants completed a set of measures of physical and psychological characteristics identical to those at baseline. The structure and content of the physical therapy programs from which participants were recruited aligned with clinical guidelines for musculoskeletal injury rehabilitation and adhered with the reimbursement policies of the provincial compensation system.24 A 40$ compensation was offered at each data collection point. The study protocol was approved by the Comité d’éthique de la recherche en éducation et sciences sociales (project #2022-3392). This study complies with the Declaration of Helsinki.
Treatment Intervention
Empowered Relief is a single-session, 2-hour pain class that includes pain neuroscience education, mindfulness principles, and cognitive behavioral therapy skills (identifying distressing thoughts and emotions, cognitive reframing, a relaxation response exercise, and a self-soothing action plan).11 At the end of the course, participants receive a 20-minute relaxation audio file with binaural tones. In this study, the intervention was delivered by a licensed physical therapist and certified instructor (MPR) of Empowered Relief via Zoom or Teams using an electronic slide deck to patients in a single session lasting 120 minutes. There were two ways to receive Empowered Relief, individually or in group-format. The decision on which format participants received was largely determined by the availability of both the participants and the instructor. This study utilized the French-Canadian version of Empowered Relief © Stanford University.
Measures
Demographics and Job Characteristics
Questionnaires assessed age, sex at birth (male, female), gender (on a sliding scale between 0= male and 100 = female), relationship status, ethnicity and education. Additional questions assessed history of musculoskeletal injury and workplace characteristics such as employment industry.
Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCS) consists of 13-items to assess patterns of negative cognition and emotion in the context of actual or anticipated pain.12 The PCS directs participants to consider how they tend to think and feel in the broad context of pain. A sample item from the PCS: “I become afraid that the pain will get worse”. Participants rate their endorsement of frequency for each item using a 0–4 Likert scale (0= not at all; 4= all the time). The PCS is comprised of 3 subscales: magnification, rumination, and feelings of helplessness. All items are summed to create a total score. The psychometric sufficiency of the PCS has been demonstrated.12,25 A cut-off score of 30 or higher indicates clinically relevant levels of catastrophizing that are with a higher risk of developing chronic pain and poorer outcomes in pain management.12
National Institutes of Health PROMIS Measures
The National Institutes of Health PROMIS short-form measures have been applied in pain research,26–30 and selected domains were identified by the Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials31,32 as core outcomes. Participants were asked to reference the previous 7 days to rate items for pain intensity (version 1a), physical function (version 8b), pain interference (version 8a), depression (version 8a), anxiety (version 8a). Higher scores on PROMIS measures indicate greater symptom severity, except for physical function, wherein higher scores reflect better function. The web-based PROMIS assessment center33 software34 was used to calculate the short-form T scores using Item Response Theory scoring algorithms that apply the Bayesian expected A posteriori method.35
Post-Class Acceptability Questionnaire
Immediately after the class, participants received an online questionnaire to assess their perceptions about the class, including acceptability, satisfaction, perceived usefulness of information, comprehensiveness, ease of understanding, likelihood to use the skills learned, likelihood of recommending the class, satisfaction with the instructor and the virtual format. All items use a 6-point scale, where 1 is the lowest rating and 6 is the highest possible rating. This survey has been used in prior work.10,11,16
Statistical Analysis
Continuous and categorical baseline variables were summarized using mean (SD) and count (proportions), respectively. Means, SDs, and percentage ratings were calculated for the 5-item anonymous post-class acceptability questionnaire. Individuals with pain lasting between 4-weeks and 3 months were considered to have subacute pain, and those with pain lasting between 3 months and 1 year were considered to have chronic pain.36 Normality of distribution was assessed using the Shapiro-Wilk test. Independent t-tests were used to compare men and women on normally distributed variables, and Mann-Whitney U tests were used for variables that did not meet normality assumptions.
Paired t-tests were conducted to compare pain catastrophizing scores at baseline and at the 4-week follow-up for the total sample. Cohen’s d was used to assess treatment effect sizes. Treatment response for each participant was calculated using the percentage change in pain catastrophizing from baseline to 4-week follow-up ((Baseline score – Follow-up score)/Baseline score)×100). Given the limited sample size, baseline Pain Catastrophizing Scale scores were summarized descriptively for individuals with subacute and chronic pain. Mann-Whitney U tests were conducted to explore group differences in PCS scores at baseline and at follow-up. The clinical significance of changes in pain catastrophizing scores at follow-up was classified according to IMMPACT guidelines: a 15% change is clinically insignificant, 15%-30% is minimally clinically important, 30%-50% is moderately clinically important, and a 50% change is substantially clinically important.31 For PROMIS measures, the minimal important change typically ranges from 2 to 6 T-score points.37 The minimally important difference for PROMIS measures were: 1.5 for pain intensity,38 4 for pain interference,39 4 for physical function,40 3 for depression,41 and 3 for anxiety.42
Results
Patient Characteristics
A total of 89 individuals met initial eligibility criteria and were screened by the research team, resulting in the enrollment of 77 participants in the study. Of the patients who were scheduled for Empowered Relief from January 2023 through March 2024, 63 attended the class (82% engagement rate). All class participants completed the post-class acceptability survey. A total of 58 participants completed the 4-week follow-up questionnaire. See Figure 1 for Flowchart.
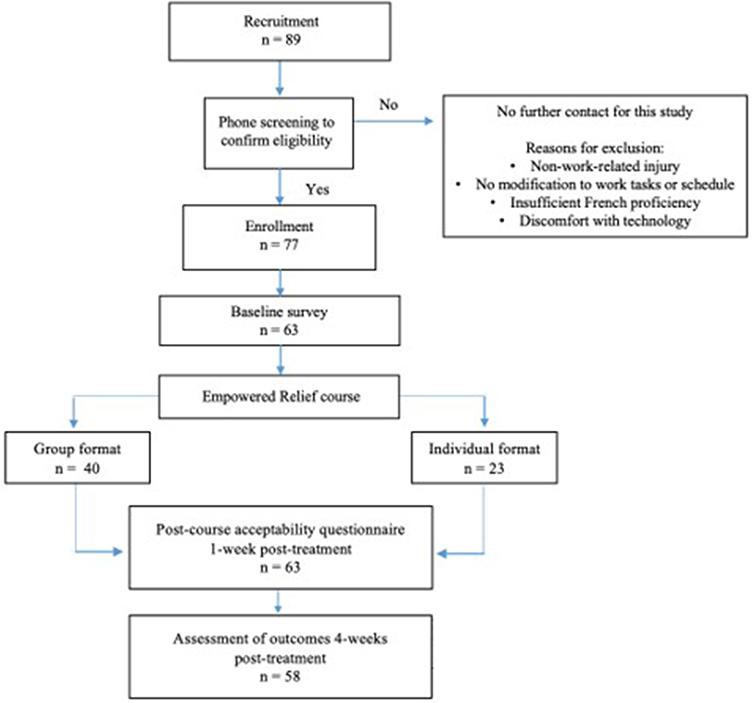 |
Figure 1 Study flowchart. |
The participant mean age was 45.7 (SD = 10.60) with 58.7% women and 81% white. At baseline, 42 participants reported subacute pain (pain lasting less than 3 months), and 21 reported chronic pain (pain lasting between 3 months and 1 year). Participants lost to follow-up were female, reported chronic pain, and were slightly older (Mean = 56.2, SD = 12.7, range = 41–75 years). Shapiro-Wilk tests indicated that catastrophizing, depression, pain interference and pain intensity variables deviated from normality (p <0.05). A Mann-Whitney U test revealed a significant difference in pain intensity scores between men and women, U = 334.5, p =0.038, with women having higher pain intensity scores (Median = 6, M = 5.78, SD = 1.87) than men (Median = 5, Mean = 4.65, SD = 2.28). No significant differences between men and women were found for baseline measures of pain catastrophizing, pain interference, physical function, anxiety and depression. About two-thirds (60%) of the sample took part in the group-format Empowered Relief. Table 1 describes the baseline characteristics of the study participants.
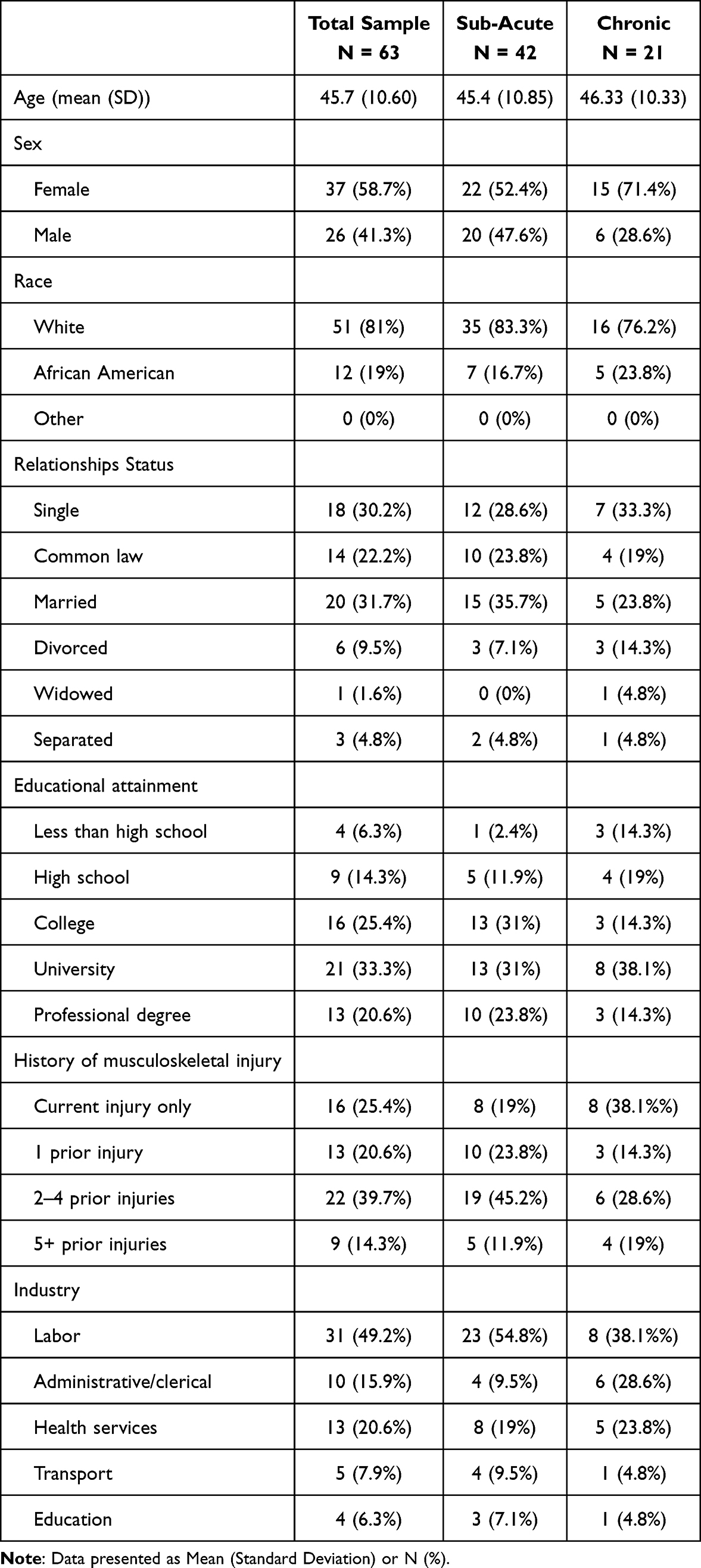 |
Table 1 Baseline Demographic Characteristics |
Acceptability
Acceptability measures indicated that average scores surpassed the 80% threshold (equivalent to 4.8/6) across all items, including perceived acceptability, satisfaction, usefulness, clarity, intended use, and likelihood of recommendation. Satisfaction with the virtual format was also well above the 80% threshold. No differences in the acceptability of the course were found between the individual- and group-format classes or between study completers and participants lost to follow-up. Table 2 displays acceptability scores.
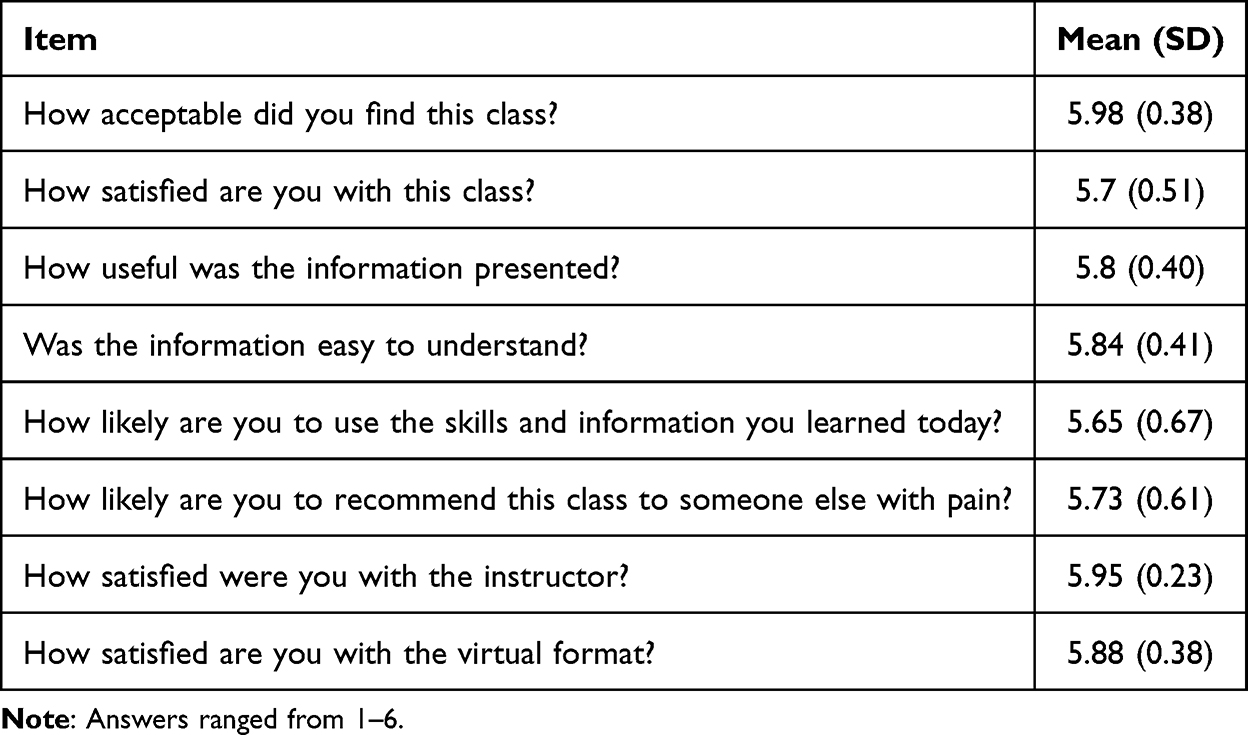 |
Table 2 Post-Class Survey Result (N=58) |
Changes in Pain Catastrophizing
In the total sample, the average pain catastrophizing score went from 43.79 (SD = 8.71) at baseline to 15.6 (SD = 12.85) at 4-week post-intervention. Treatment effect size was large for baseline to 4-weeks post-intervention (Cohen’s d = 2.33). Of the 52 (90%) of participants who scored above the established cut-off score of 30 at baseline, only 8 (14%) participants scored above that threshold at 4-weeks post-intervention. Seven of the 8 participants who scored above the pain catastrophizing cut off score at 4-weeks post-intervention reported chronic pain at baseline. A Mann-Whitney U test revealed there was no significant difference in baseline pain catastrophizing scores between participants with subacute pain (n = 42, Median = 44, Mean = 42.26, SD = 9.53) and chronic pain (n = 21, Median = 46, Mean = 42.95, SD = 10.39), U = 398.00, p =0.53). However, at 4-weeks post-intervention, participants with subacute pain (n = 42, Median = 9, Mean = 12.02, SD = 10.69) had significantly lower pain catastrophizing scores than participants with chronic pain (n = 17, Median = 26, Mean = 24.24, SD = 13.53). Figure 2 illustrates the changes in average pain catastrophizing scores in the subacute and chronic pain groups from baseline to 4-week post-intervention.
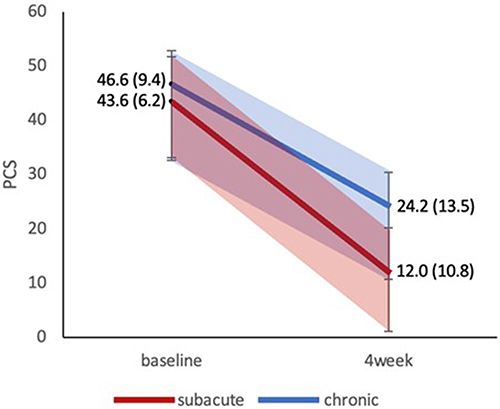 |
Figure 2 Pain catastrophizing score changes from baseline to 4-week post-intervention in workers with subacute and chronic low back pain. Note: Scores are presented as means (standard deviation), PCS = Pain Catastrophizing Scale. |
Table 3 displays the clinical importance of pain catastrophizing changes and the number of participants in each category of clinical importance at 4-weeks post-intervention. Of the 58 participants with follow-up data, 57 achieved clinically significant reductions in pain catastrophizing at follow-up, with 89.7% (N = 52) achieving moderately or substantially important reductions.
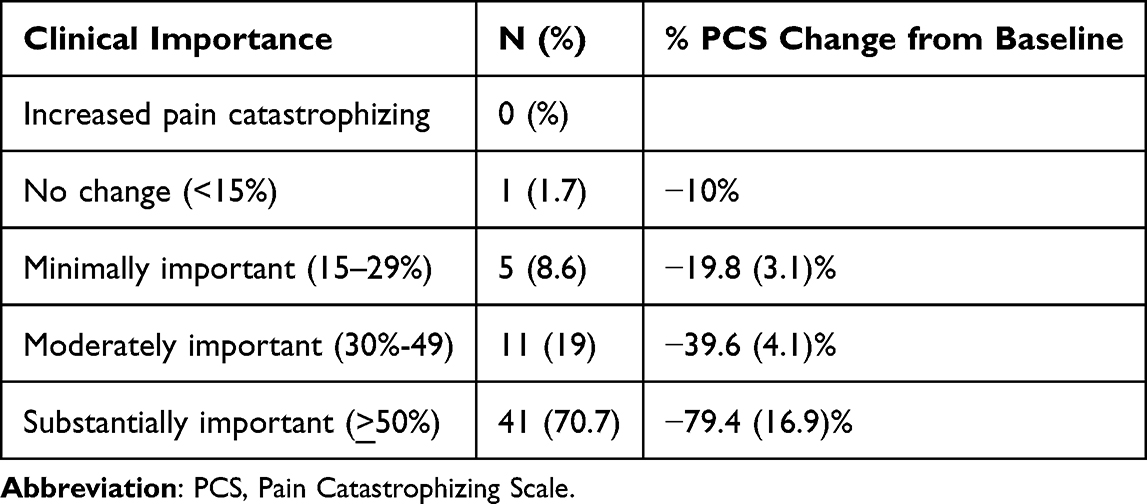 |
Table 3 Clinical Importance of Post-Intervention PCS Changes in Total Sample (N=58) |
Changes in Pain-Related Outcomes
Table 4 displays changes in secondary outcomes, showing clinically meaningful changes in PROMIS measures of pain interference, physical function, anxiety and depression. Although improvements in pain intensity were observed, these changes did not reach the minimally important difference of 1.5.38
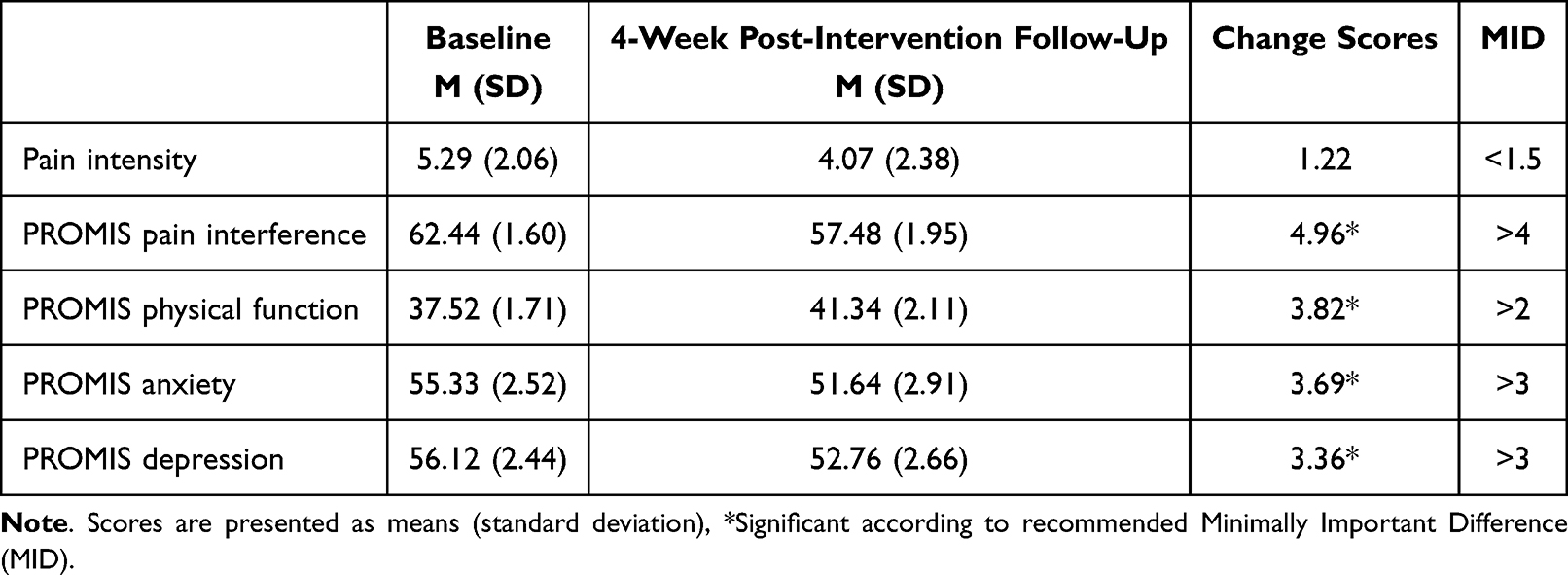 |
Table 4 Change Scores for Secondary Outcomes (N=58) |
Discussion
This study examined the acceptability of Empowered Relief and changes in pain catastrophizing and pain-related outcomes following its delivery by physical therapists to French-Canadian workers with subacute and chronic low back pain (3–12 months). The highly positive results of the post-class acceptability survey indicate that Empowered Relief delivered by physical therapists was well received among French Canadians and that most participants felt the class was useful, understandable and satisfactory. Results suggest that workers who participated in Empowered Relief and physical therapy reported significant changes in pain catastrophizing and physical and mental health outcomes.
On the basis of previous research, the present study sought to examine whether participating in Empowered Relief was associated with clinically significant changes in pain catastrophizing in individuals with occupational low back pain. Analysis of pre- and post-intervention pain catastrophizing measures revealed a large effect size and clinically significant reduction in scores on the Pain Catastrophizing Scale in both participants with subacute and chronic pain at the 4-week follow-up. Furthermore, an examination of individual scores revealed that 44 of the 52 participants who initially scored above the clinical cut-off for pain catastrophizing were subsequently below this threshold following participation in the intervention. These findings are important since previous studies have shown that interventions targeting and reducing pain catastrophizing at an early stage may contribute to improved responses to subsequent pain management approaches.43,44 Future randomized controlled trials could explore whether Empowered Relief enhances long-term recovery outcomes and supports a successful return to work following injury.
Given the nature of this study, it is impossible to determine whether the observed changes in pain catastrophizing are due to Empowered Relief, physical therapy, or a combination of both. It is also possible that the “effect of care” that may come from participating in the study and talking about pain and symptoms, as well as the effect of time may also have impacted results.45 However, prior research examining the effects of physical therapy alone provides useful context.46,47 For example, Sullivan et al, found that individuals with back pain who received physical therapy alone experienced a 24% reduction in catastrophizing. In contrast, those who received physical therapy and 10 weekly 1-hour psychosocial sessions saw a greater than 50% reduction in catastrophizing.46 Similarly, George et al reported only a 20% reduction with four weeks of standard physical therapy.48 In the current study, 71% of participants reported a 50% or greater reduction in catastrophizing after a single 2-hour session of Empowered Relief alongside physical therapy. This may be due to the intervention’s targeted focus on pain education, cognitive reframing and self-regulation strategies. If replicated, the combination of Empowered Relief and physical therapy may be a highly efficient way to reduce catastrophizing in a significantly short timeframe.
Consistent with previous research,14 the findings revealed that participants reported changes across pain-related outcomes, including in pain intensity, physical function, pain interference and symptoms of depression and anxiety. Changes in pain intensity did not meet the non-inferiority margin, yet were considerably larger in this study than in previous research reporting on changes in pain intensity at 4-week follow-up in individuals with chronic low back pain who received Empowered Relief.14 In accordance with previous research, participants also reported clinically meaningful improvements in physical function and pain interference.14 This is especially pertinent to work-related injuries, as improvements in physical function are key metrics used by insurers to determine the approval or denial of rehabilitation services from both clinical and policy standpoints.49 Pain interference, on the other hand, provides insights into how pain affects a person’s ability to function and participate in a wide range of activities.26 Interestingly, the baseline levels of anxiety, depression, physical function and pain interference were already high. Clinically, this is particularly interesting, as studies with moderate baseline levels often have limited clinical relevance. While improvements were observed at 4 weeks post-intervention, it is unknown whether these effects persist beyond that point, as no longer-term follow-up data were collected in this study.
Physical therapists are strategically positioned to intervene early in the pain trajectory given their expertise in musculoskeletal and functional health. Their accessibility and established relationships with patients make them well suited to address not only physical symptoms but also the psychosocial aspects of pain. This is particularly important in contexts where access to pain psychologists is limited. Expanding the role of physical therapists in this way may help close critical gaps in care.50 Additionally, individuals with chronic pain may be hesitant to seek help from mental health professionals, in part due to concerns about being labeled as having psychological issues – particularly in certain populations.51 As trusted members of the healthcare team, physical therapists may offer a more acceptable avenue for patients to receive psychosocial support. This approach could be beneficial for underserved populations with limited access to specialized pain care, such as rural workers or those with financial and logistical barriers to multidisciplinary pain care.
In this context, Empowered Relief emerges as a practical, scalable intervention that can be delivered by physical therapists to enhance early-stage rehabilitation. Developed as a brief, skills-based intervention grounded in cognitive behavioral therapy and pain neuroscience education, Empowered Relief has demonstrated meaningful clinical benefits at 3- and 6-month follow-ups in randomized controlled trials.14,15,18 In the present study, the intervention was successfully delivered online by physical therapists in primary care, offering additional evidence of its flexibility and relevance to real-world settings. Clinicians may understandably question whether a single-session intervention is sufficient for managing complex conditions like low back pain. However, while Empowered Relief is not intended to replace the longer-course cognitive behavioral therapy, our findings suggest it may meaningfully contribute to early care. Finally, while no significant differences emerged between group and individual class formats, format remains a relevant consideration. Group sessions may foster engagement and learning through peer interaction and social modeling of positive coping behaviors, while individual sessions may allow for greater personalization. Future research could further explore whether delivery format influences outcomes, adherence, or patient satisfaction.
Several limitations merit consideration. First, the uncontrolled design limits our ability to attribute observed changes solely to the intervention. However, this approach aligns with the priorities of governing bodies such as the Canadian Institutes of Health Research, which supports the need for pilot studies to establish feasibility and inform future trials55. The sample size further highlights the need for larger, controlled studies to characterize responders and non-responders. Despite this, robust treatment appraisal data (N=63), demonstrate a strong and favorable signal for broad implementation. Other limitations include the sample being predominantly white, educated and in a relationship. The sample may not accurately represent the broader population due to potential selection bias and the large number of workers from labor-related industries. More women than men participated, which contrasts with typical occupational low back pain samples. This prompts consideration into factors such as gender differences in health-seeking behavior and preventative care.52,53 Understanding differences in health-seeking behavior may help in designing more effective outreach and recruitment strategies to ensure a more balanced representation of individuals who experience low back pain. Finally, no data was collected on other concurrent treatments (eg, occupational therapy, chiropractic care, or massage therapy), which could have influenced results.
This study was the first to implement Empowered Relief alongside physical therapy for occupational low back pain, delivered by physical therapists rather than psychologists. The findings highlight the high acceptability of Empowered Relief delivered by physical therapists in a new population and clinical setting, as well as in its virtual format. Results demonstrated that a 2-hour single-session of Empowered Relief in combination with physical therapy was associated with clinically meaningful changes in pain catastrophizing, symptoms of anxiety and depression, physical function and pain interference at 4-weeks post-intervention. The results suggest that Empowered Relief could serve as a brief, low-burden, and complementary intervention within physical therapy for workers with occupational low back pain. Larger, controlled studies are needed to determine the unique contribution of the intervention to patient outcomes and overall clinical efficacy. Future studies could further validate whether incorporating Empowered Relief early in the care trajectory may help prevent the chronicization of pain and disability.
Abbreviations
PCS, Pain Catastrophizing Scale; PROMIS, Patient-Reported Outcomes Measurement Information System; SD, standard deviation; IMMPACT, The Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials.
Data Availability
Data that support the findings of this study are available from the corresponding author, JSC, upon reasonable request.
Ethics Approval
Primary project was approved by the Comité d’éthique de la recherche – Éducation et sciences sociales of the Université de Sherbrooke (#2022-3392).
Acknowledgments
The authors would like to thank Joanie Rollin for her participation as a patient partner. The authors would also like to thank Clinique Physio-Expert, Physio Atlas (Sherbrooke, Magog, Granby, Mont St-Hilaire, Windsor), Clinique PhysioMédic, Physio-Santé (Drummondville), Urgence Physio, Clinique de Physiothérapie Estrie, Clinique Khoury, Ma Clinique Générale, MyoSynergie Amos, Clinique Aviva, Physiothérapie universelle Longueuil, Kinatex Chambly, Impact Réadaptation (Drummondville), Iso Santé, La Boîte Thérapeutique, Mouvement Physio Laval Ste-Rose, Physio Summum (Jean-Talon O)., Clinique Cigonia, and Physiothérapie Solution Active Verdun for their participation in this study.
Funding
This work was supported by the Canadian Institutes of Health Research (JSC;75367), the Fonds de recherche du Québec Santé (Carrière) and Société et Culture (Carrière), as well as the Chaire de recherche en réadaptation au travail Fondation J. Armand Bombardier et Pratt & Whitney Canada. Stanford University receives revenue for continuing medical education on Empowered Relief (ER) instructor certification training provided to clinicians. Dr. Darnall is Chief Science Advisor at AppliedVR, and her consulting role with this company (personal fees) is unrelated to the current research. Dr. Darnall receives royalties for 4 pain treatment books she has authored or coauthored. She is the principal investigator for 2 pain research awards from the Patient-Centered Research Outcomes Research Institute, both of which involve either E.R., C.B.T., or both. Dr. Darnall is principal investigator for 2 NIH grants that are investigating the efficacy of E.R. Dr. Darnall serves on the Board of Directors for the American Academy of Pain Medicine, the Board of Directors for the Institute for Brain Potential, and the Medical Advisory Board for the Facial Pain Association. Dr. Darnall is a scientific member of the NIH Interagency Pain Research Coordinating Committee, a former member of the Centers for Disease Control and Prevention Opioid Workgroup (2020–2021), and a current member of the Pain Advisory Group of the American Psychological Association. None of the funders listed above had any role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Disclosure
Dr Beth Darnall reports Stanford University owns the copyright and trademark to the Empowered Relief and receives fees for CME clinician certification workshops. Dr. Darnall receives no personal monies for Empowered Relief; Dr. Darnall has research awards from the NIH and PCORI to investigate the efficacy and comparative effectiveness of Empowered Relief. The authors declare no other conflicts of interest in this work.
References
1. AC VT, Arora M, Barber RM, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet. 2016;388(10053):1545–1602.
2. Hoy D, Bain C, Williams G, et al. A systematic review of the global prevalence of low back pain. Arthritis Rheum. 2012;64(6):2028–2037. doi:10.1002/art.34347
3. Manchikanti L, Singh V, Falco FJE, Benyamin RM, Hirsch JA. Epidemiology of low back pain in adults. Neuromodulation. 2014;17(Suppl 2):3–10. doi:10.1111/ner.12018
4. AIlaire M, Ricard G Statistiques sur les affections vertébrales 2003-2006. 2007.
5. Chen S, Chen M, Wu X, et al. Global, regional and national burden of low back pain 1990–2019: a systematic analysis of the global burden of disease study 2019. J Orthop Translat. 2022;32:49–58. doi:10.1016/j.jot.2021.07.005
6. Côté P, Cassidy JD, Carroll L. The treatment of neck and low back pain: who seeks care? Who goes where?. Med Care. 2001;39(9):956–967. doi:10.1097/00005650-200109000-00006
7. Côté P, Baldwin ML, Johnson WG. Early patterns of care for occupational back pain. Spine. 2005;30(5):581–587. doi:10.1097/01.brs.0000154613.17511.dd
8. Sanders T, Ong BN, Sowden G, Foster N. Implementing change in physiotherapy: professions, contexts and interventions. J Health Organ Manage. 2014;28(1):96–114. doi:10.1108/JHOM-10-2011-0102
9. Mariano TY, Urman RD, Hutchison CA, Jamison RN, Edwards RR. Cognitive behavioral therapy (CBT) for subacute low back pain: a systematic review. Curr Pain Headache Rep. 2018;22(3):15. doi:10.1007/s11916-018-0669-5
10. Darnall BD, Scheman J, Davin S, et al. Pain psychology: a global needs assessment and national call to action. Pain Med. 2016;17(2):250–263. doi:10.1093/pm/pnv095
11. Darnall BD, Sturgeon JA, Kao M-C, Hah JM, Mackey SC. From catastrophizing to recovery: a pilot study of a single-session treatment for pain catastrophizing. J Pain Res. 2014;7:219–226. doi:10.2147/JPR.S62329
12. Sullivan MJL, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7(4):524–532. doi:10.1037/1040-3590.7.4.524
13. Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother. 2009;9(5):745–758. doi:10.1586/ern.09.34
14. Darnall BD, Roy A, Chen AL, et al. Comparison of a single-session pain management skills intervention with a single-session health education intervention and 8 sessions of cognitive behavioral therapy in adults with chronic low back pain: a randomized clinical trial. JAMA Netw Open. 2021;4(8):e2113401. doi:10.1001/jamanetworkopen.2021.13401
15. Darnall BD, Burns JW, Hong J, et al. Empowered relief, cognitive behavioral therapy, and health education for people with chronic pain: a comparison of outcomes at 6-month follow-up for a randomized controlled trial. Pain Rep. 2024;9(1):e1116. doi:10.1097/PR9.0000000000001116
16. Davin SA, Savage J, Thompson NR, Schuster A, Darnall BD. Transforming standard of care for spine surgery: integration of an online single-session behavioral pain management class for perioperative optimization. Front Pain Res. 2022;3:856252. doi:10.3389/fpain.2022.856252
17. Ziadni MS, Anderson SR, Gonzalez-Castro L, Darnall BD. Comparative efficacy of a single-session “empowered relief” videoconference-delivered group intervention for chronic pain: study protocol for a randomized controlled trial. Trials. 2021;22(1):358. doi:10.1186/s13063-021-05303-8
18. Ziadni MS, Gonzalez-Castro L, Anderson S, Krishnamurthy P, Darnall BD. Efficacy of a single-session “empowered relief” zoom-delivered group intervention for chronic pain: randomized controlled trial conducted during the COVID-19 pandemic. J Med Internet Res. 2021;23(9):e29672. doi:10.2196/29672
19. Darnall BD. Psychological treatment for chronic pain: improving access and integration. Psychol Sci Public Interest. 2021;22(2):45–51. doi:10.1177/15291006211033612
20. Faul F, Erdfelder E, Lang A-G, Buchner A G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39(2):175–191. doi:10.3758/BF03193146
21. Iles RA, Davidson M, Taylor NF. Psychosocial predictors of failure to return to work in non-chronic non-specific low back pain: a systematic review. Occup Environ Med. 2008;65(8):507–517. doi:10.1136/oem.2007.036046
22. Gore M, Sadosky A, Stacey BR, Tai K-S, Leslie D. The burden of chronic low back pain: clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine. 2012;37(11):E668–77. doi:10.1097/BRS.0b013e318241e5de
23. Sullivan MJL, Scott W, Trost Z. Perceived injustice: a risk factor for problematic pain outcomes. Clin J Pain. 2012;28(6):484–488. doi:10.1097/AJP.0b013e3182527d13
24. Koes BW, van Tulder M, Lin C-WC, Macedo LG, McAuley J, Maher C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur Spine J. 2010;19(12):2075–2094. doi:10.1007/s00586-010-1502-y
25. Osman A, Barrios FX, Gutierrez PM, Kopper BA, Merrifield T, Grittmann L. The pain catastrophizing scale: further psychometric evaluation with adult samples. J Behav Med. 2000;23(4):351–365. doi:10.1023/A:1005548801037
26. Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173–182. doi:10.1016/j.pain.2010.04.025
27. Hung M, Hon SD, Franklin JD, et al. Psychometric properties of the PROMIS physical function item bank in patients with spinal disorders. Spine. 2014;39(2):158–163. doi:10.1097/BRS.0000000000000097
28. Pilkonis PA, Choi SW, Reise SP, Stover AM, Riley WT, Cella D. Item banks for measuring emotional distress from the patient-reported outcomes measurement information system (PROMIS®): depression, anxiety, and anger. Assessment. 2011;18(3):263–283. doi:10.1177/1073191111411667
29. Rose M, Bjorner JB, Gandek B, Bruce B, Fries JF, Ware JE Jr. The PROMIS physical function item bank was calibrated to a standardized metric and shown to improve measurement efficiency. J Clin Epidemiol. 2014;67(5):516–526. doi:10.1016/j.jclinepi.2013.10.024
30. Stone AA, Broderick JE, Junghaenel DU, Schneider S, Schwartz JE. PROMIS fatigue, pain intensity, pain interference, pain behavior, physical function, depression, anxiety, and anger scales demonstrate ecological validity. J Clin Epidemiol. 2016;74:194–206. doi:10.1016/j.jclinepi.2015.08.029
31. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1):9–19. doi:10.1016/j.pain.2004.09.012
32. Turk DC, Dworkin RH, Allen RR, et al. Core outcome domains for chronic pain clinical trials: IMMPACT recommendations. Pain. 2003;106(3):337–345. doi:10.1016/j.pain.2003.08.001
33. PROMIS-Assessment. Assessment Center. Available from: https://www.assessmentcenter.net/.
34. Gershon RC, Rothrock N, Hanrahan R, Bass M, Cella D. The use of PROMIS and assessment center to deliver patient-reported outcome measures in clinical research. J Appl Measure. 2010;11(3):304–314.
35. Fischer HF, Rose M. Scoring depression on a common metric: a comparison of EAP estimation, plausible value imputation, and full Bayesian IRT modeling. Multi Behav Res. 2019;54(1):85–99. doi:10.1080/00273171.2018.1491381
36. Banerjee S, Argáez C. CADTH Rapid Response Reports. Multidisciplinary Treatment Programs for Patients with Acute or Subacute Pain: A Review of Clinical Effectiveness, Cost-Effectiveness, and Guidelines. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health Copyright © 2019 Canadian Agency for Drugs and Technologies in Health; 2019.
37. Terwee CB, Peipert JD, Chapman R, et al. Minimal important change (MIC): a conceptual clarification and systematic review of MIC estimates of PROMIS measures. Qual Life Res. 2021;30(10):2729–2754. doi:10.1007/s11136-021-02925-y
38. Kovacs FM, Abraira V, Royuela A, et al. Minimal clinically important change for pain intensity and disability in patients with nonspecific low back pain. Spine. 2007;32(25):2915–2920. doi:10.1097/BRS.0b013e31815b75ae
39. Amtmann D, Kim J, Chung H, Askew RL, Park R, Cook KF. Minimally important differences for patient reported outcomes measurement information system pain interference for individuals with back pain. J Pain Res. 2016;9:251–255. doi:10.2147/JPR.S93391
40. Hays RD, Spritzer KL, Fries JF, Krishnan E. Responsiveness and minimally important difference for the patient-reported outcomes measurement information system (PROMIS) 20-item physical functioning short form in a prospective observational study of rheumatoid arthritis. Ann Rheum Dis. 2015;74(1):104–107. doi:10.1136/annrheumdis-2013-204053
41. Kroenke K, Stump TE, Chen CX, et al. Minimally important differences and severity thresholds are estimated for the PROMIS depression scales from three randomized clinical trials. J Affect Disord. 2020;266:100–108. doi:10.1016/j.jad.2020.01.101
42. Lee AC, Driban JB, Price LL, Harvey WF, Rodday AM, Wang C. Responsiveness and minimally important differences for 4 patient-reported outcomes measurement information system short forms: physical function, pain interference, depression, and anxiety in knee osteoarthritis. J Pain. 2017;18(9):1096–1110. doi:10.1016/j.jpain.2017.05.001
43. Burns JW, Kubilus A, Bruehl S, Harden RN, Lofland K. Do changes in cognitive factors influence outcome following multidisciplinary treatment for chronic pain? A cross-lagged panel analysis. J Consult Clin Psychol. 2003;71(1):81–91. doi:10.1037/0022-006X.71.1.81
44. Campbell CM, McCauley L, Bounds SC, et al. Changes in pain catastrophizing predict later changes in fibromyalgia clinical and experimental pain report: cross-lagged panel analyses of dispositional and situational catastrophizing. Arthritis Res Ther. 2012;14(5):R231. doi:10.1186/ar4073
45. Sean M, Coulombe-Lévêque A, Nadeau W, et al. Counting your chickens before they hatch: improvements in an untreated chronic pain population, beyond regression to the mean and the placebo effect. Pain Rep. 2024;9(3):e1157. doi:10.1097/PR9.0000000000001157
46. Sullivan MJL, Adams H. Psychosocial treatment techniques to augment the impact of physiotherapy interventions for low back pain. Physiother Can. 2010;62(3):180–189. doi:10.3138/physio.62.3.180
47. Sullivan MJ, Adams H, Rhodenizer T, Stanish WD. A psychosocial risk factor–targeted intervention for the prevention of chronic pain and disability following whiplash injury. Phys Ther. 2006;86(1):8–18. doi:10.1093/ptj/86.1.8
48. George SZ, Zeppieri G Jr, Cere AL, et al. A randomized trial of behavioral physical therapy interventions for acute and sub-acute low back pain (NCT00373867). Pain. 2008;140(1):145–157. doi:10.1016/j.pain.2008.07.029
49. Karayannis NV, Sturgeon JA, Chih-Kao M, Cooley C, Mackey SC. Pain interference and physical function demonstrate poor longitudinal association in people living with pain: a PROMIS investigation. Pain. 2017;158(6):1063–1068. doi:10.1097/j.pain.0000000000000881
50. Driscoll MA, Edwards RR, Becker WC, Kaptchuk TJ, Kerns RD. Psychological interventions for the treatment of chronic pain in adults. Psychol Sci Public Interest. 2021;22(2):52–95. doi:10.1177/15291006211008157
51. Perugino F, De Angelis V, Pompili M, Martelletti P. Stigma and chronic pain. Pain Ther. 2022;11(4):1085–1094. doi:10.1007/s40122-022-00418-5
52. Thompson AE, Anisimowicz Y, Miedema B, Hogg W, Wodchis WP, Aubrey-Bassler K. The influence of gender and other patient characteristics on health care-seeking behaviour: a QUALICOPC study. BMC Fam Pract. 2016;17(1):38. doi:10.1186/s12875-016-0440-0
53. Matheson FI, Smith KLW, Fazli GS, Moineddin R, Dunn JR, Glazier RH. Physical health and gender as risk factors for usage of services for mental illness. J Epidemiol Community Health. 2014;68(10):971–978. doi:10.1136/jech-2014-203844
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Pharmacopuncture Therapy for Chronic Low Back Pain: A Protocol for a Pragmatic Randomized Controlled Trial
Park KS, Kim S, Seo JY, Cho H, Lee JY, Lee YJ, Lee J, Kim MJ, Choi YE, Yang CS, Han CH, Ha IH
Journal of Pain Research 2022, 15:2629-2639
Published Date: 1 September 2022
“Self-Healing”: A Novel and Integrated Multimodal Concept for the Management of Musculoskeletal Pain
Mobasheri A
Journal of Pain Research 2022, 15:3479-3482
Published Date: 1 November 2022
Clinical Applications and Potential Mechanism of Cold Acclimation Therapy
Wang Y, Wang Y, Han D, Sun W, Qiao Y, Wang C, Zhang X, Xu J
Journal of Multidisciplinary Healthcare 2025, 18:4113-4120
Published Date: 19 July 2025