Back to Journals » Journal of Pain Research » Volume 15
“Self-Healing”: A Novel and Integrated Multimodal Concept for the Management of Musculoskeletal Pain
Authors Mobasheri A ![]()
Received 16 August 2022
Accepted for publication 10 October 2022
Published 1 November 2022 Volume 2022:15 Pages 3479—3482
DOI https://doi.org/10.2147/JPR.S386508
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Ali Mobasheri1– 4
1Research Unit of Medical Imaging, Physics and Technology, Faculty of Medicine, University of Oulu, Oulu, FI-90014, Finland; 2Department of Regenerative Medicine, State Research Institute Centre for Innovative Medicine, Vilnius, LT-08406, Lithuania; 3Department of Joint Surgery, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, 510080, People’s Republic of China; 4World Health Organization Collaborating Center for Public Health Aspects of Musculo-Skeletal Health and Ageing, Division of Public Health, Epidemiology and Health Economics, University of Liège, Liege, 4000, Belgium
Correspondence: Ali Mobasheri, Research Unit of Medical Imaging, Physics and Technology, Faculty of Medicine, University of Oulu, Oulu, FI-90014, Finland, Email [email protected]
Background and Objective: Musculoskeletal (MSK) conditions, particularly low back pain and osteoarthritis, are a leading cause of disability worldwide. The number of people with MSK conditions is set to increase over the coming decades highlighting the need for better tools for both patients and medical practitioners. A recent paper by McSwan, Gudin and co-authors introduces the concept of the innate ability of the body to “self-heal” through five body networks, whilst being optimized by integrative multi-modal medicine and natural remedies ranging from the physical to psychological, that are starting to be incorporated into clinical management and treatment guidelines.
Conclusion: “Self-Healing” is a new concept for MSK pain management and reinforces the potential for integrating multi-modal medicine into current care through open dialogue between patients and healthcare providers.
Keywords: musculoskeletal pain, pain management, low back pain, osteoarthritis, self-healing
Commentary
According to the World Health Organization (WHO) more than 1.7 billion people suffer from musculoskeletal (MSK) conditions.1,2 MSK conditions are the leading contributor to disability worldwide, with low back pain (LBP) and osteoarthritis (OA) being the leading causes of physical disability globally, with a prevalence of 700 million and 500 million people, respectively.3,4 Ageing, demographic change and the ever increasing global population mean that the number of people with MSK conditions is rapidly increasing and the disability associated with MSK disorders is projected to continue to rise in the next decades. This highlights the need to prioritise MSK disorders and increase the core competency of medical practitioners to develop better tools to help and reassure their patients, with increasing numbers of cases.5–8
MSK conditions are typically characterized by pain, which is frequently chronic and persistent, with limitations in mobility, dexterity and overall level of functioning, reducing quality of life and the ability to work.1 Traditionally, the treatment of MSK pain and its clinical management has focused on the use of conventional pharmaceuticals to relieve symptoms. However, many of the currently available pain medications have significant side-effects and adverse impacts on the cardiovascular, renal and gastrointestinal systems.9–12 The opioid epidemic has also highlighted the unmet medical need for pain management; highlighting opportunities for developing, testing and implementing multimodal pain management solutions.13–15
A recent review paper by McSwan, Gudin and co-authors has introduced the “Self-Healing” concept for MSK pain management.16 In this paper, the authors discuss the role of multidisciplinary, multi-modal and integrative approaches in MSK pain management.16 They emphasize the increased use of alternative and complementary treatments by patients and the need for integration of natural remedies in clinical management and treatment guidelines. Aside from highlighting the role of alternative and complementary treatments they propose the novel and plausible concept that the human body has an innate capacity to “self-heal” and that this ability can be optimized by the use of integrative medical strategies (Figure 1). The factors that trigger acute or recurring MSK pain are diverse and can range from physical to psychological stresses, which apply to many age groups, including adolescents.17 The mechanisms used by the body to respond to these pain triggers and “self-heal” are thought to work through five body networks. The nervous system can promote restoration and healing of the body through the relaxation response. Psychology and decreasing mental stress can help reduce muscle activity and thus pain. Modulation of the immune system through acute inflammation can play a critical role in the regeneration of muscle. An increase in microcirculation may promote healing and reduce pain. Muscular relaxation/contraction increases the supply of oxygen and nutrients and relaxes the muscle. These restorative processes are potentially be enhanced through the application of multimodal and integrative approaches, thus promoting the idea of “self-healing” despite the unfamiliar processes and complexities.18,19
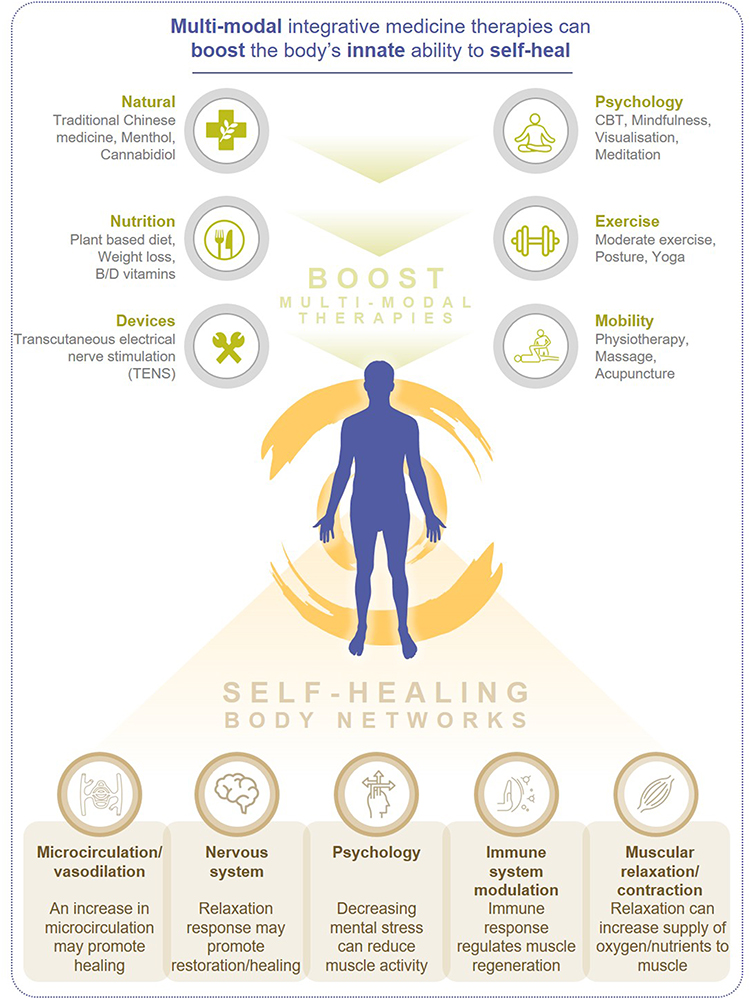 |
Figure 1 Self-healing and multi-modal integrative medicine. |
“Self-Healing” is a new way of thinking for MSK pain management and reinforces the potential for integrating multi-modal medicine through new research, and implementation of multimodal approaches through open dialogue between patients and healthcare providers.20 The effectiveness of pain management solutions should be specific based on diagnosis, but can encompass modification of lifestyle including through nutrition, assessment of dietary intake, posture, physical activity and exercise,21 cognitive behavioral therapy and mind/body techniques,22 many of which are starting to appear in treatment guidelines.
Unfortunately, the pandemic has set us back in every previously established initiative to improve MSK health, highlighting the need for pragmatic approaches to pain management in the post-COVID-19 era.23 Outlining the key priorities for establishing the concept of “Self-Healing” in a primary healthcare context is clearly beyond the scope of this editorial and the efforts of a single author. Further work by academia, industry, health authorities and regulatory agencies is needed to establish the concept of “Self-Healing” as a priority area in pain management.
In summary, “Self-Healing” aims to harness the innate ability of the body and mind to promote mechanisms to restore physiological setpoints and restore balance to the MSK system, reducing pain and disability in a natural and holistic manner.24 The body has an innate ability to “self-heal” but this ability is compromised in older individuals, especially those with chronic co-morbidities. However, including “Self-Healing” in integrative medicine has the capacity to optimize the body’s endogenous repair processes and restore homeostasis.
Acknowledgments
Minor editing and formatting for journal requirements was undertaken by Ella Palmer, PhD, CMPP of inScience Communications, Springer Healthcare Ltd, UK, and was funded by Sanofi.
Author Contributions
AM contributed exclusively to the preparation of this commentary.
Funding
No specific funding was sought or secured in relation to this editorial.
Disclosure
AM is President of the Osteoarthritis Research Society International (OARSI). He has no conflict of interest regarding the publication of this editorial.
References
1. March L, Smith EU, Hoy DG., et al. Burden of disability due to musculoskeletal (MSK) disorders. Best Pract Res Clin Rheumatol. 2014;28(3):353–366. doi:10.1016/j.berh.2014.08.002
2. Guillemin F, Carruthers E, Li LC. Determinants of MSK health and disability--social determinants of inequities in MSK health. Best Pract Res Clin Rheumatol. 2014;28(3):411–433. doi:10.1016/j.berh.2014.08.001
3. Hoy DG, Smith E, Cross M, et al. The global burden of musculoskeletal conditions for 2010: an overview of methods. Ann Rheum Dis. 2014;73(6):982–989. doi:10.1136/annrheumdis-2013-204344
4. George SZ, Fritz JM, Silfies SP, et al. Interventions for the management of acute and chronic low back pain: revision 2021. J Orthop Sports Phys Ther. 2021;51(11):Cpg1–cpg60. doi:10.2519/jospt.2021.0304
5. Locke R, Wilkinson E, Collier R, Harden B. Musculoskeletal (MSK) practitioners in primary care: an evaluation of a MSK core capabilities framework and review process. Educ Prim Care. 2020;31(1):32–35. doi:10.1080/14739879.2019.1687016
6. Cheung L, Soundy A. The impact of reassurance on musculoskeletal (MSK) pain: a qualitative review. Behav Sci. 2021;11(11):150. doi:10.3390/bs11110150
7. Cummings DL, Smith M, Merrigan B, Leggit J. MSK30: a validated tool to assess clinical musculoskeletal knowledge. BMJ Open SEM. 2019;5(1):e000495. doi:10.1136/bmjsem-2018-000495
8. Scott DIC, McCray DG, Lancaster PG, Foster PNE, Hill DJC. Validation of the Musculoskeletal Health Questionnaire (MSK-HQ) in primary care patients with musculoskeletal pain. Semin Arthritis Rheum. 2020;50(5):813–820. doi:10.1016/j.semarthrit.2020.06.022
9. Harirforoosh S, Asghar W, Jamali F. Adverse effects of nonsteroidal antiinflammatory drugs: an update of gastrointestinal, cardiovascular and renal complications. Int J Pharm Pharm Sci. 2013;16(5):821–847. doi:10.18433/J3VW2F
10. Kean WF, Rainsford KD, Kean IR. Management of chronic musculoskeletal pain in the elderly: opinions on oral medication use. Inflammopharmacology. 2008;16(2):53–75. doi:10.1007/s10787-008-1623-7
11. Labianca R, Sarzi-Puttini P, Zuccaro SM, Cherubino P, Vellucci R, Fornasari D. Adverse effects associated with non-opioid and opioid treatment in patients with chronic pain. Clin Drug Investig. 2012;32(1):53–63. doi:10.2165/11630080-000000000-00000
12. McCrae JC, Morrison EE, MacIntyre IM, Dear JW, Webb DJ. Long-term adverse effects of paracetamol - a review. Br J Clin Pharmacol. 2018;84(10):2218–2230. doi:10.1111/bcp.13656
13. Wardhan R, Chelly J. Recent advances in acute pain management: understanding the mechanisms of acute pain, the prescription of opioids, and the role of multimodal pain therapy. F1000Research. 2017;6:2065. doi:10.12688/f1000research.12286.1
14. Delle JM, Gazley C. Advocating for multimodal pain management and reducing the need for opioids in the acute and chronic pain setting. Nurs Clin North Am. 2021;56(3):357–367. doi:10.1016/j.cnur.2021.04.003
15. Kelly MA. Addressing the opioid epidemic with multimodal pain management. Am J Orthop. 2016;45(7):S6–S8.
16. McSwan J, Gudin J, Song XJ, et al. Self-healing: a concept for musculoskeletal body pain management - scientific evidence and mode of action. J Pain Res. 2021;14:2943–2958. doi:10.2147/JPR.S321037
17. Kamper SJ, Henschke N, Hestbaek L, Dunn KM, Williams CM. Musculoskeletal pain in children and adolescents. Braz J Phys Ther. 2016;20(3):275–284. doi:10.1590/bjpt-rbf.2014.0149
18. Lee C, Crawford C, Swann S. Multimodal, integrative therapies for the self-management of chronic pain symptoms. Pain Med. 2014;15 Suppl 1:S76–S85. doi:10.1111/pme.12408
19. Crawford C, Lee C, Freilich D. Effectiveness of active self-care complementary and integrative medicine therapies: options for the management of chronic pain symptoms. Pain Med. 2014;15 Suppl 1:S86–S95. doi:10.1111/pme.12407
20. Wanless B, Berry A, Noblet T. Self-management of musculoskeletal (MSK) conditions: what is most useful to patients? Protocol for a mixed methods systematic review. Musculoskeletal Care. 2021;20:271–278.
21. Geneen LJ, Moore RA, Clarke C, Martin D, Colvin LA, Smith BH. Physical activity and exercise for chronic pain in adults: an overview of Cochrane Reviews. Cochrane Database Syst Rev. 2017;4(4):Cd011279. doi:10.1002/14651858.CD011279.pub3
22. Lee C, Crawford C, Hickey A. Mind-body therapies for the self-management of chronic pain symptoms. Pain Med. 2014;15 Suppl 1:S21–S39. doi:10.1111/pme.12383
23. Widyadharma IPE, Sari N, Pradnyaswari KE, et al. Pain as clinical manifestations of COVID-19 infection and its management in the pandemic era: a literature review. Egypt J Neurol Psychiatry Neurosurg. 2020;56(1):121. doi:10.1186/s41983-020-00258-0
24. Kaufman JA. Nature, mind, and medicine: a model for mind-body healing. Explore. 2018;14(4):268–276. doi:10.1016/j.explore.2018.01.001
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024
Hospital-Treated Infections and 15-year Incidence of Musculoskeletal Disorders: A Large Population-Based Cohort Study
Gao Y, McGagh D, Ding L, Hong S, Ouyang Z, Wei J, Zeng C, Lei G, Xie J
Clinical Epidemiology 2025, 17:251-264
Published Date: 11 March 2025
Changes in Pain Catastrophizing and Related Outcomes Following a Single-Session Empowered Relief Intervention Delivered by Physical Therapists in Workers with Low Back Pain: A Pilot Study
Carrière JS, Coutu MF, Darnall BD, Léonard G, Royer MP, Li MY, Bordeleau M, Durand MJ
Journal of Pain Research 2025, 18:4845-4857
Published Date: 17 September 2025