Back to Journals » Journal of Pain Research » Volume 15
Effectiveness and Safety of Pharmacopuncture Therapy for Chronic Low Back Pain: A Protocol for a Pragmatic Randomized Controlled Trial
Authors Park KS, Kim S, Seo JY ![]() , Cho H
, Cho H ![]() , Lee JY
, Lee JY ![]() , Lee YJ
, Lee YJ ![]() , Lee J, Kim MJ
, Lee J, Kim MJ ![]() , Choi YE
, Choi YE ![]() , Yang CS
, Yang CS ![]() , Han CH
, Han CH ![]() , Ha IH
, Ha IH ![]()
Received 23 May 2022
Accepted for publication 24 August 2022
Published 1 September 2022 Volume 2022:15 Pages 2629—2639
DOI https://doi.org/10.2147/JPR.S375231
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Kyoung Sun Park,1 Suna Kim,2 Ji Yeon Seo,3 HyunWoo Cho,4 Jee Young Lee,5 Yoon Jae Lee,5 Jinho Lee,1 Min Ji Kim,6 Young Eun Choi,6 Chang Sop Yang,7 Chang-Hyun Han,7,8,* In-Hyuk Ha5,*
1Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea; 2Daejeon Jaseng Hospital of Korean Medicine, Daejeon, Republic of Korea; 3Bucheon Jaseng Hospital of Korean Medicine, Bucheon, Republic of Korea; 4Haeundae Jaseng Hospital of Korean Medicine, Busan, Republic of Korea; 5Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, Seoul, Republic of Korea; 6Clinical Research Coordinating Team, Korea Institute of Oriental Medicine, Daejeon, Republic of Korea; 7KM Science Research Division, Korea Institute of Oriental Medicine, Daejeon, Republic of Korea; 8 Korean Convergence Medicine, University of Science & Technology (UST), Campus of Korea Institute of Oriental Medicine, Daejeon, Republic of Korea
*These authors contributed equally to this work
Correspondence: In-Hyuk Ha, Jaseng Spine and Joint Research Institute, Jaseng Medical Foundation, 2F Vision Tower, 540 Gangnam-daero, Gangnam-gu, Seoul, 06110, Republic of Korea, Tel +82 2 2222 2740, Email [email protected]
Purpose: Chronic low back pain (LBP) is a common musculoskeletal disorder that affects everyday life; moreover, it occasionally causes disability and increases medical expenditure. This pragmatic randomized clinical trial aims to investigate the effects of pharmacopuncture on chronic LBP by comparing the effectiveness of pharmacopuncture and physiotherapy strategies.
Patients and Methods: In this two-armed, parallel, multi-center randomized controlled study, the participants will randomly undergo 10 sessions of pharmacopuncture therapy or physiotherapy over five weeks based on the randomization outcomes. The primary outcome will be the numeric rating scale (NRS) score of LBP. The secondary outcomes will include the NRS score of radiating leg pain, visual analog scale (VAS) score of LBP and radiating leg pain, Oswestry disability index, the Korean version of the Roland–Morris disability questionnaire, patient global impression of change (PGIC), short Form-12 health survey version 2, and 5-level EuroQol-5 dimension (EQ-5D-5L).
Conclusion: This protocol aims to examine the comparative effectiveness of pharmacopuncture, which is a widely used therapy in Korean medicine, with respect to the standard therapy through a pragmatic randomized controlled trial to present useful data to facilitate clinical or policy decision making.
Trial Registration: Clinicaltrials.gov (NCT04833309); Clinical Research Information Service (KCT0006088).
Keywords: low back pain, pharmacopuncture, physical therapy, pragmatic randomized controlled trial, protocol, musculoskeletal disorder, Korean medicine
Introduction
Low back pain (LBP) is the most common musculoskeletal disorder in industrialized society and is among the major absenteeism causes.1 More than 80% of the population experience LBP in their lifetime; further, approximately 10–20%—up to 40% in some reports—of acute LBP cases become chronic.2 Further, chronic LBP has a high recurrence rate, with a one-year and lifetime recurrence rates of 20–44% and 85%, respectively.3 Based on the health claims data published by the Health Insurance Review and Assessment Service (HIRA), LBP is the most frequently claimed condition in Korean medicine outpatient care in 2017, with more than four million patients receiving outpatient care at a Korean medicine clinic or hospital annually. Additionally, LBP was ranked first among the diagnoses that caused hospitalization in a Korean medicine treatment facility for the previous four years, with more than 70,000 patients receiving inpatient care for LBP in 2017.
Pharmacopuncture involves a combination of acupuncture and herbal medicine, with the administration of herbal medicine extracts at acupoints. Combining physical stimulation and chemical effects maximizes and prolongs the effects of accessing the acupoints.4,5 The effects of pharmacopuncture can be immediately observed after treatment because herbal extracts are directly absorbed without the need to pass through the gastrointestinal tract. Additionally, both patients with difficulty swallowing and those who refuse to take herbal medicine may benefit by receiving pharmacopuncture treatment.6 The major benefits of pharmacopuncture in comparison to conventional acupuncture include more rapid effects, additional synergistic effects of acupuncture and herbal extracts, and the ease for controlling dosage.7 In a 2015 survey on Korean medicine doctors (KMDs) in Korean medicine facilities specializing in musculoskeletal disorders, 95.9% of the respondents reported using pharmacopuncture on patients with lumbar intervertebral disc displacement.8
Several studies have investigated the effects of pharmacopuncture on chronic LBP. A randomized controlled trial (RCT) on the efficacy of bee venom pharmacopuncture reported that it was significantly more effective in providing pain relief and functional improvement compared with sham bee venom pharmacopuncture.9,10 However, there have been no RCTs on other pharmacopuncture types; moreover, few studies have compared pharmacopuncture with an active control group. Therefore, there is a need for a well-designed RCT that reflects the clinical settings in Korea and utilizes various pharmacopuncture types. In this context, we planned a pragmatic RCT to investigate the effectiveness of pharmacopuncture on chronic LBP by comparing the effectiveness of pharmacopuncture and physiotherapy strategies.
Materials and Methods
Study Design and Setting
This two-armed, parallel, multi-center RCT will competitively recruit 100 patients in the Jaseng Hospital of Korean Medicine, Daejeon Jaseng Hospital of Korean Medicine, Bucheon Jaseng Hospital of Korean Medicine, and Haeundae Jaseng Hospital of Korean Medicine. The study protocol was approved by the Institutional Review Board (IRB) of Jaseng Hospital of Korean Medicine before participant recruitment (JASENG 2021–02-012, JASENG 2021–02-013, JASENG 2021–02-014, JASENG 2021–02-032). Additionally, the study protocol will be registered with Clinicaltrials.gov (NCT04833309) and Clinical Research Information Service (KCT0006088) and continuously updated.
Participant Timeline
The participants will sign an informed consent form (ICF) on the first visit after receiving explanations regarding the study. Subsequently, the investigators will screen the participants against the inclusion and exclusion criteria. A total of 15 visits will be required; further, the treatment will be given in 10 sessions as two weekly sessions a week for five weeks. There will be follow-up visits on week 6, 13, and 25 from the baseline; additionally, follow-ups will be performed face-to-face or over the phone. The participants will be randomized to the pharmacopuncture or physiotherapy group and will receive the corresponding treatments from week 1. Table 1 presents the time schedule of enrolment, interventions, and assessments for participants.
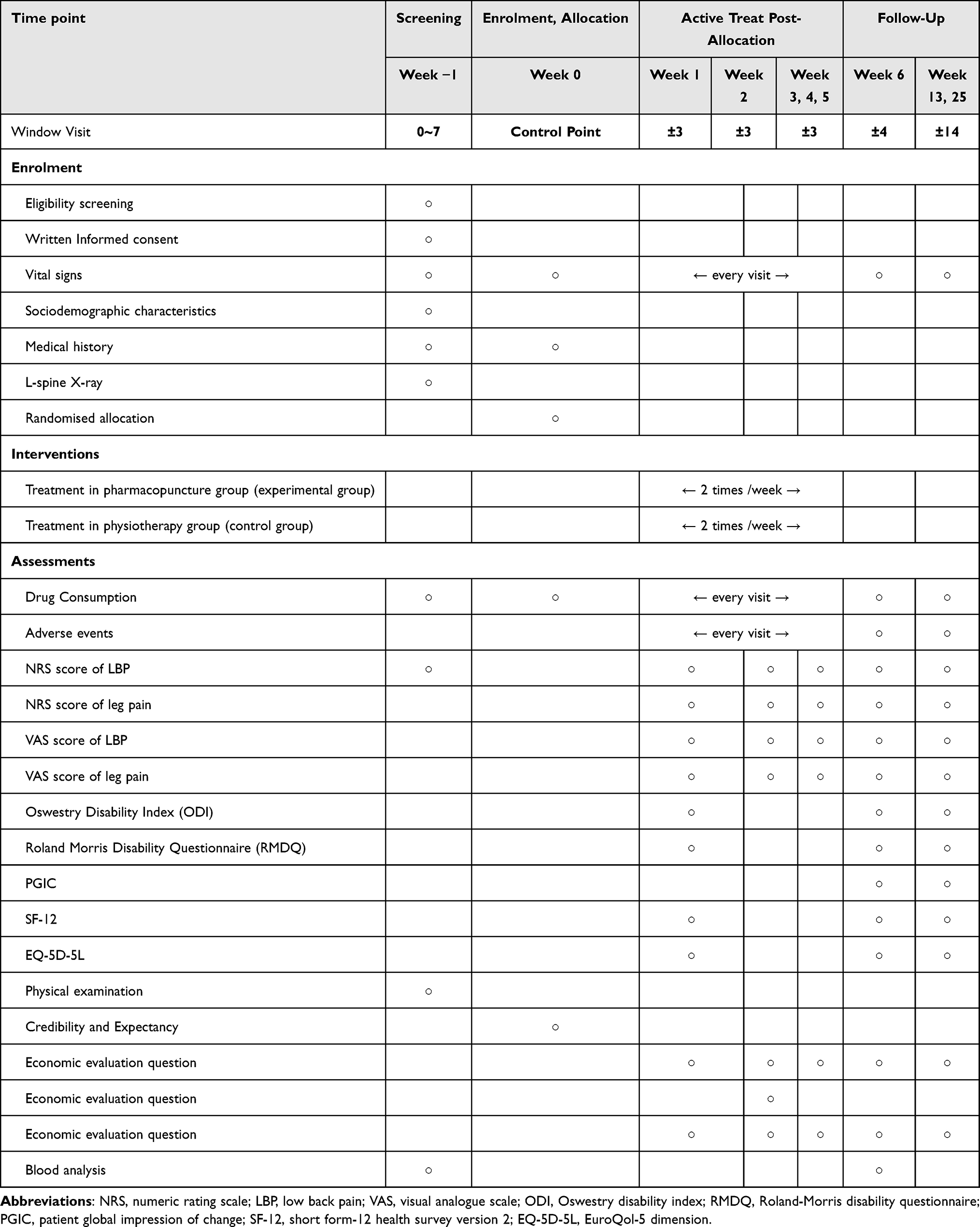 |
Table 1 Time schedule of participants |
Inclusion/Exclusion Criteria
Inclusion Criteria
LBP onset ≥ 6 months
Numeric rating scale (NRS) score of LBP ≥ 5
Age 19–70 years
Signing of the ICF to participate in the clinical trial
Exclusion Criteria
Diagnosis of a serious disease that may cause LBP (eg, spinal metastasis of tumor, acute fracture, spinal dislocation)
Progressive neurological defects or severe neurological symptoms
Pain is caused by soft tissue disease rather than the spine (eg, tumor, fibromyalgia, rheumatic arthritis, gout)
Other chronic diseases that may hinder the interpretation of treatment effects or outcomes (eg, stroke, myocardial infarction, renal disease, diabetic neuropathy, dementia, epilepsy)
Current use of steroids, immunosuppressants, antipsychotic agents, or other drugs that may affect study outcomes
Contraindications for pharmacopuncture, including hemorrhagic diseases, anticoagulant usage, severe diabetes mellitus with risk of infection
Use of drugs that may affect pain, including non-steroidal anti-inflammatory drugs, or pharmacopuncture therapy within the previous week
Pregnant or breastfeeding women, as well as women planning to conceive
Lumbar surgery in the previous three months
Less than one month since participating in another clinical trial or planning to participate in another clinical trial during the study period or follow-up period within 6 months upon enrolment
Declining to sign a consent form to participate
Other disqualifications as determined by the investigators
Interventions
Experimental Group: Pharmacopuncture Therapy
Pharmacopuncture therapy will be given two times a week for five weeks. With reference to a study on the current trend in pharmacopuncture therapy that used electronic medical records from 12 Korean medical hospitals,11 the treatment will be performed following the physician’s clinical judgment. Additionally, all procedure-related matters will be recorded in patients’ charts. Pharmacopuncture procedures will be retrospectively reviewed and recorded in a case report form (CRF) for analysis.
Control Group: Physiotherapy
Based on a study on HIRA data, patients with LBP in Korea are treated using a combination of deep heat therapy, superficial heat therapy, transcutaneous electrical nerve stimulation, and intermittent pelvic traction therapy.12 According to this data, a physician will choose the method, site, and duration of physiotherapy based on their clinical judgment with respect to the patients’ symptoms, radiological findings, and improvement levels. Physiotherapy will be performed twice a week for five weeks; further, all matters regarding the physiotherapy, including the type, duration, and site of physiotherapy, will be recorded in patients’ charts. The treatment method will be retrospectively reviewed and recorded in CRF for comparison.
Criteria for Discontinuation and Withdrawal
A participant may be discontinued from the clinical trial for the following reasons:
Discovery of a previously undetected disease that may affect study outcomes
Request for discontinuation during the study period by the participant or their legal representative or withdrawal of consent by the participant
Confirmation of pregnancy during the study period
Problems regarding the administration of medical and Korean medical procedures for LBP to the participant
Other reasons that warrant discontinuation from the study as determined by the researcher
Concomitant Treatment
Pharmacological therapy and medical care for LBP from another healthcare facility may be permitted during the treatment or follow-up period in case of severe pain. The treatment details and frequency will be recorded in the CRF for analysis.
Outcome
Primary Outcome
NRS score of LBP
The LBP intensity within the previous week will be assessed using the NRS. Patients will be instructed to choose a number from 0–10 that best represents their current discomfort level (0 for no pain, 10 for the worst imaginable pain).
Secondary outcomes
NRS score of radiating leg pain
The intensity of radiating leg pain in the past week will be assessed using the NRS. Patients will be asked to choose a number from 0–10 that best represents their current discomfort level (0 for no pain, 10 for the worst imaginable pain).
Visual analog scale (VAS) score of low back pain and radiating leg pain
The VAS represents the patient’s pain level, where one end of a 100-mm line refers to no pain while the other end indicates the worst imaginable pain. Patients are instructed to indicate their intensity of LBP and radiating leg pain within the previous week by marking a point on the line.
Oswestry disability index (ODI)
The participants’ functional status will be assessed using the ODI, which is a 10-item tool developed to assess LBP-caused disability. Each item is divided into six steps; further, it is rated on a scale from 0–5. A higher score indicates a more severe disability.13 We will use the Korean version of the ODI questionnaire, which has been shown to be reliable and valid.14
Korean version of the Roland–Morris disability questionnaire (RMDQ)
The RMDQ is among the most widely used tools for evaluating the functional state of patients with LBP. It comprises 24 items, with the patient marking the specific activities limited by their LBP. A positive response scores 1 point, and the questionnaire is scored from 0 (minimal disability) to 24 (severe disability).15 We will use the questionnaire of the Korean-adapted version, which has been shown to be reliable and valid.16
Patient Global Impression of Change (PGIC)
The PGIC is a self-reported tool for patients’ improvement levels: 1, very much improved; 2, much improved; 3, minimally improved; 4, no change; 5, minimally worse; 6, much worse; or 7, very much worse. A consistent relationship between the change in NRS and the PGIC was demonstrated regardless of study, disease type, age, sex, study result, or treatment group.17
Short Form-12 Health Survey (SF-12) version 2
The SF-12 is a questionnaire for evaluating health-related quality of life. It comprises 12 items in 8 domains: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health. It usually takes less than five minutes to complete the questionnaire, with a higher score indicating a better health-related quality of life. We will use the Korean version SF-12, which has been shown to be reliable and valid.18
5-level EuroQol-5 dimension (EQ-5D-5L)
The EQ-5D-5L is the most widely used indirect evaluation tool for the health state. The descriptive system comprises five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has 5 levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. The patient is asked to indicate their health state by ticking the box next to the most appropriate statement in each of the five dimensions. This decision results in a 1-digit number that expresses the level selected for that dimension. The digits for the five dimensions can be combined into a 5-digit number that describes the patient’s health state. There are specific weights for the level of each category; moreover, these weights and constant numbers are used to compute the preference score.19 We will use the questionnaire of the Korean-adapted version, which has been shown to be reliable and valid.20
Credibility and Expectancy
Participants’ expectations for the treatment will be assessed using a 9-point Likert scale.
At the enrolment visit, the participants will respond to the question, “How much pain relief do you expect from the pharmacopuncture therapy and physiotherapy? (1 = not at all, 5 = somewhat, and 9 = very much)
Cost Analysis
Cost analysis will be performed using a structured questionnaire for official/unofficial medical costs, non-medical expenses, time costs, and cost of productivity loss. The official medical cost refers to the cost spent utilizing healthcare facility services, while the unofficial medical cost refers to the cost spent on purchasing health supplements and medical equipment. Non-medical expenses refer to the cost incurred while utilizing healthcare, including transportation, patient’s time, and caregiver cost. Cost of productivity loss refers to the cost incurred by lost productivity due to absenteeism and presenteeism due to the disease. The work productivity and activity impairment questionnaire21 will be used to determine productivity loss; additionally, this will be converted to cost for cost-effectiveness analysis.
Drug Consumption
The types and doses of drugs (rescue drugs) taken for LBP during the study period will be surveyed and recorded at each visit. The frequency of other treatment types, including physiotherapy and injections, will be recorded.
Adverse Events
For safety evaluation, hematology tests (white blood cell [WBC], neutrophil, lymphocyte, monocyte, eosinophil, basophil, red blood cell [RBC], hemoglobin [Hgb], hematocrit [Hct], mean corpuscular volume [MCV], mean corpuscular hemoglobin [MCH], mean corpuscular hemoglobin concentration [MCHC], platelet, erythrocyte sedimentation rate [ESR]), clinical chemical tests (T-protein, albumin, T-bilirubin, aminotransferase [ALT], aspartate aminotransferase [AST], r-glutamyl transpeptidase [GTP], blood urea nitrogen [BUN], creatinine), and immunologic tests (C-reactive protein [CRP]) will be performed before and after treatment for both groups to compare the incidence of adverse events.
Adverse events refer to undesirable and unintended signs, symptoms, or diseases that occur after the procedure, including events that may not be caused by the procedure. In this study, data regarding adverse events are collected based on patients’ reports and investigators’ observations. Further, we will analyze the incidence of adverse events, abnormal laboratory parameters, and serious adverse events suspected to be related to the treatment. The causality between the treatment and adverse events will be assessed using a 6-point scale following the World Health Organization-Uppsala Monitoring Centre causality assessment system (1, definitely related; 2. probably related; 3, possibly related; 4, probably not related; 5, definitely not related; and 6, unknown). The severity of all adverse events will be classified into three categories based on the Spilker classification: Mild (1), treatment not required without marked hindrance of normal everyday life (function); Moderate (2); significantly hinders normal everyday life (function) with possible treatment being required and subsequent treatment; Severe (3): serious adverse event requiring advanced treatment and leaving sequelae.
Sample Size Calculation
A pilot study was conducted to compare the effectiveness of pharmacopuncture and physiotherapy in patients with chronic LBP. The between-group difference in the mean reduction of the NRS score for LBP was 1.37 ± 1.94 at the primary endpoint, which is immediately after the 5-week treatment; further, Cohen’s d was calculated as 0.71. The correlation between the baseline and endpoint was 0.53.22 Given a significance of 95% and power of 90%, the sample size was calculated to be 64. Considering a 30% withdrawal rate and the recruitment of participants from four facilities, we aim to recruit 100 patients.
Recruitment
Participants will be recruited using a press release, advertisement posters at the clinical trial facility, and online recruitment sites.
Randomization and Allocation Concealment
A statistician will randomize patients into two groups at the same ratio (50 persons for each) using a randomization table on R studio 1.1.463 (© 2009–2018 RStudio, Inc.). The random sequence will be performed using block randomization; further, the size of each block will be randomly set to 2 or 4. The randomization results will be placed in a sealed opaque envelope and stored in a double-locked cabinet by a third person not involved in the study. The coordinator at each study facility will open the envelope for group allocation. Only participants who provide an ICF will be randomly assigned. The randomization number assigned to each participant will be recorded in the electronic medical record.
Blinding
Since blinding the practitioner administering the treatment and the participants is impossible due to the nature of the intervention, only the outcome assessors will be blinded. Outcome-assessors not involved in the procedure and blinded from the group allocation will perform the assessment before the procedure in an isolated space.
Data Collection and Management
We will use an e-CRF using the Internet-based Clinical Research and Trial management system (iCReaT). The principal investigator will train the outcome assessors and investigators of each facility on the standard operating procedure (SOP) as a reference for the study procedures, including writing a CRF and entering data. A query will be issued for a range check of data values. Data entered into the e-CRF will be cleaned and locked to prevent access by investigators other than the one in charge of data management.
Statistical Methods
We will perform both intention-to-treat (ITT) and per-protocol (PP) analyses, with ITT as the primary analysis. For the PP analysis, we will include participants who complete at least seven treatment sessions over 5 weeks. Missing data will be handled by multiple imputation (MI) for analysis of covariance (ANCOVA) and comparison of area under the curve (AUC), as well as the mixed model for repeated measures for the linear mixed model. For survival analysis, outcomes after the missing time point will be censored. For sensitivity analysis, the last observation carried forward (LOCF) will be used for missing data imputation; further, the normality of distribution will be tested. Nonparametric data will be analyzed using the Wilcoxon-rank sum test.
Sociodemographic characteristics and treatment expectancy of the participants will be assessed according to the group. Continuous variables will be presented as mean (SD) or median (quartile), with between-group differences being analyzed using Student’s t-test or Wilcoxon-rank sum test, depending on their distribution. Categorical variables will be presented as frequency (%) and analyzed with the chi-square test or Fisher’s exact test.
The study endpoints are the differences in the extent of changes in continuous outcomes (NRS, VAS, NDI, NPQ, EQ-5D-5L, SF-12) at each time point from the baseline. As the primary analysis, we will use a linear mixed model with the covariant factors significantly different from the baseline as covariates and the group as the fixed factor. Next, ANCOVA will be performed on sets processed by MI and LOCF.
To compare the total difference in each outcome within a certain period (treatment period and total study period), the AUC will be calculated for each time point after randomization and compared using Student’s t-test. Further, the proportion of patients whose NRS and VAS scores dropped by > 50% from the baseline values will be compared at each time point. The time from randomization to lumbar recovery, which was defined as > 50% reduction in the pain indices, will be compared using Kaplan–Meier survival analysis. Further, the curves will be compared using the Log rank test. Additionally, hazard ratios will be compared using the Cox proportional hazard model.
The significance level will be set at 0.05 for all analyses. All statistical analyses will be performed using the SAS 9.4 (© SAS Institute, Inc., Cary, NC, USA) or R studio 1.1.463 (© 2009–2018 RStudio, Inc.) software. Statistical significance will be set at p < 0.05.
In case the superiority test fails, a non-inferiority test will be performed. The non-inferiority margin will be set to −1 (NRS), which represents half of the minimal clinically important difference.23,24 Pharmacopuncture will be considered non-inferior to physiotherapy if the lower bound of the 95% confidence interval (CI) of the between-group difference of the NRS score reduction does not exceed the non-inferiority margin.
Data Monitoring
The monitoring staff will supervise the clinical trial process, as well as periodically review and confirm whether the study is performed and recorded according to the protocol, SOP, clinical trial management standards, and applicable regulations. The clinical trial will be monitored by the monitoring staff of each clinical trial facility and the sponsor institution using periodic visits and phone calls. At the monitoring visits, the monitoring staff will check the original participant records and data storage (study files). Further, they will inspect the clinical trial procedure and discuss any problems with the investigators.
In case of unexpected or unacceptable risks to participants or occurrence of serious adverse events related to pharmacopuncture or physiotherapy in ≥ 25% of the participants, the clinical trial may be paused. The A analysis will be only accessed by the statistician and principal investigator; additionally, the final decision to terminate the study will be made by the principal investigator.
Harms
Regarding safety evaluation, we will perform hematology tests (WBC, neutrophil, lymphocyte, monocyte, eosinophil, basophil, RBC, Hgb, Hct, MCV, MCH, MCHC, platelet, ESR), clinical chemical tests (T-protein, albumin, T-bilirubin, ALP, AST, ALT, r-GTP, BUN, creatinine), and immunologic test (CRP) before and after the treatment for both groups to compare the incidence of adverse events. Collected blood samples will be immediately discarded after the analysis; further, matters regarding the disposal will adhere to the SOP of the diagnostic testing team. All adverse events reported during the study period will be illustrated in a figure; furthermore, the incidence of adverse events will be computed. Between-group comparisons of the proportion of patients who developed an adverse event will be performed using the Chi-square test or Fisher’s exact test.
Ethics Approval
This study complies with the Declaration of Helsinki. Before beginning the study, the principal investigator submitted the protocol, CRF, ICF, and patient recruitment advertisement to the IRB of Jaseng Hospital of Korean Medicine and obtained approval (JASENG 2021–02-012, JASENG 2021–02-013, JASENG 2021–02-014, JASENG 2021–02-032). Any amendments to the protocol, CRF, ICF, and patient recruitment advertisement will be made with IRB approval; additionally, changes will be updated on the trial registries. All participating investigators will be trained on the Helsinki Declaration and the Korean Good Clinical Practice Guidelines, protocol, and SOP for protecting the participants. The participants’ personal information will be strictly protected under IRB supervision; moreover, their privacy and confidentiality will be guaranteed.
Informed Consent
Before beginning the clinical trial, the investigators will provide an adequate explanation regarding details of the clinical trial and treatment; further, they will obtain a signed written informed consent from the participants. The participants will receive a copy of the consent form. If personal information must be collected, such as a copy of a passbook for a pay-out of transportation fees, the patients will be informed and asked for consent.
Confidentiality
All personal information will be rigorously managed under supervision by the IRB; further, the participants’ confidentiality will be guaranteed. All data collected from consenting participants will be anonymously processed. In case the data are provided to other facilities for research, the personal information may be replaced by arbitrarily assigned codes.
Ancillary and Post-Trial Care
The participants will receive emergency contact information to contact the principal investigator or clinical research coordinator in case of inquiries or development of medical problems or study-related diseases during the study period. Participants who experience an injury directly caused by the intervention will receive proper medical care as determined by the investigator; additionally, compensations will be processed following the pre-established study-related insurance provisions.
Dissemination
The investigators plan to share the study results with the participants, healthcare professionals, and the public by publishing them or through trial registration. Important changes to the protocol after the publication of this article will be periodically updated on the trial registration websites.
Discussion
A pragmatic trial is a study design based on the notion that an explanatory trial does not provide proper clinical outcomes since it is optimized for determining efficacy. Given that previous studies were performed by highly trained investigators on a relatively small and rigorously selected sample, they might have overestimated the benefits and underestimated the harms.25 Schwartz and Lellouch described the difference between an explanatory and pragmatic trial. An explanatory trial is a study that tests a physiological or clinical hypothesis. On the other hand, a pragmatic trial facilitates clinical or policy decision making by providing evidence for selecting interventions in real-world clinical settings.26,27 A pragmatic trial overcomes the limitations regarding existing clinical trial designs; further, it is significant as a clinical trial for determining the therapeutic effects in actual clinical practice. Specifically, a pragmatic trial is more appropriate for Korean medicine clinical trials since they examine the effects of widely used medical techniques or compare the effectiveness of various treatments rather than developing a novel drug or developing/obtaining approval for new medical technology.
The pragmatic–explanatory continuum indicator summary (PRECIS) is a tool with 10 domains for designing clinical trials on a continuum of explanatory attitude (ideal situation) to more pragmatic attitude (usual care).28 However, weaknesses have been highlighted, including the lack of a rating scale, problems with some domains, requirement for better guidance, and lack of validation. The revised version of the PRECIS (PRECIS-2) has nine domains; namely, eligibility criteria, recruitment, setting, organization, flexibility (delivery), flexibility (adherence), follow-up, primary outcome, and primary analysis, with scores from 1 (very explanatory) to 5 (very pragmatic).29
The eligibility criteria can be given a score of 4 since patients with chronic LBP will be recruited regardless of their radiologic findings, but the age criteria will be limited to 19–70 years. Recruitment can be given a score of 3 since the participants will be recruited via subway advertisements and online recruitment websites. Setting can be given a score of 3 since the participants will be only recruited from four hospital-level healthcare facilities. The organization can be given a score of 5 since radiologic equipment will not be used for LBP diagnosis, and other professionals will not participate in the diagnosis or treatment. Flexibility in delivery is given a score of 5 because the physicians will receive data regarding the frequently used pharmacopuncture therapy and physiotherapy in outpatient care.11,12 Moreover, the physicians will have the autonomy to select and perform the type and site of pharmacopuncture or physiotherapy based on their clinical judgment based on the patients’ symptoms and radiologic testing. This will be retrospectively analyzed using charts. Furthermore, flexibility in adherence can be given a score of 4 since participants with insufficient adherence to treatment will not be excluded; however, only participants who can sufficiently visit the clinical trial facility to receive adequate treatment will be selected during the screening process. Follow-up can be given a score of 2 since follow-up requires more time than general treatment sessions, and an additional investigator will be involved in completing several questionnaires based on the phone or in-person follow-up schedules within a specified post-treatment period. The primary outcome can be given a score of 5 since the primary study outcome is the NRS score for LBP, which is directly associated with patients’ symptoms and is an important outcome. Primary analysis can be given a score of 5 since we will conduct an ITT analysis that includes participants showing non-adherence and adherence below the expected level. Figure S1 shows the PRECIS-2 wheel of this protocol.
This pragmatic RCT seeks to provide data supporting clinical or policy decision making regarding pharmacopuncture, which is a widely used technique in Korean medicine clinical practice, by comparing its effectiveness with that of standard treatment.
Abbreviations
ALT, aminotransferase; ANCOVA, analysis of covariance; AST, aspartate aminotransferase; AUC, area under the curve; BUN, blood urea nitrogen; CI, confidence interval; CRF, case report form; CRP, C-reactive protein; EQ-5D-5L, 5-level EuroQol-5 dimension; ESR, erythrocyte sedimentation rate; GTP, r-glutamyl transpeptidase; Hct, hematocrit; Hgb, hemoglobin; HIRA, Health Insurance Review and Assessment Service; ICF, informed consent form; IRB, Institutional Review Board; ITT, intention-to-treat; KMDs, Korean medicine doctors; LBP, low back pain; NRS, numeric rating scale; LOCF, last observation carried forward; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; MI, multiple imputation; ODI, Oswestry disability index; PGIC, patient global impression of change; PP, per-protocol; PRECIS, pragmatic–explanatory continuum indicator summary; RBC, red blood cell; RCT, randomized controlled trial; RMDQ, Roland–Morris disability questionnaire; SOP, standard operating procedure; VAS, visual analog scale; WBC, white blood cell.
Data Sharing Statement
Availability of data and materials: The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Trial Committee Organization and Contributions
Figure S2 shows the details regarding the trial committee (trial steering committee and trial management committee) organization and roles.
Protocol Version
The study protocol version is 1.2 (2021.06.04). Important amendments to the protocol and other changes made after the publication of this article will be periodically updated on the trial registration websites.
Trial Status
The recruitment for this study is ongoing. We anticipate that it would be take 2 years to complete this trial.
Institutional Review Board Statement
This study is approved by the IRB of Jaseng Hospital of Korean Medicine (JASENG 2021-02-012, JASENG 2021-02-013, JASENG 2021-02-014, and JASENG 2021-02-032).
Informed Consent Statement
Informed consent will be obtained from all subjects involved in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the Korea institute of oriental medicine (KIOM), republic of Korea (grant number KSN2022210).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Prevention. Prevalence of disabilities and associated health conditions among adults–United States, 1999. Morbidity Mortality Weekly Rep. 2001;50(7):120–125.
2. Dugan S. The role of exercise in the prevention and management of acute low back pain. Clin Occupational Environ Med. 2006;5(3):615–632. doi:10.1016/j.coem.2006.03.003
3. Krismer M, van Tulder M. Low back pain (non-specific). Best Practice. 2007;21(1):77–91. doi:10.1016/j.berh.2006.08.004
4. Strudwick MW, Hinks RC, Choy SB. Point injection as an alternative acupuncture technique–an exploratory study of responses in healthy subjects. Acupuncture Med. 2007;25(4):166–174. doi:10.1136/aim.25.4.166
5. Luna SP, Angeli AL, Ferreira CL, Lettry V, Scognamillo-Szabo M. Comparison of pharmacopuncture, aquapuncture and acepromazine for sedation of horses. Evidence Based Complement Alter Med. 2008;5(3):267–272. doi:10.1093/ecam/nel096
6. Kwon K. Pharmacopuncturology: Principles and Clinical Applications. Elsevier Korea LLC; 2012.
7. Acupuncture K. The acupuncture and moxibustion medicine. Seoul. 2012;193:549.
8. Shin YS, Shin J-S, Lee J, et al. A survey among Korea Medicine doctors (KMDs) in Korea on patterns of integrative Korean Medicine practice for lumbar intervertebral disc displacement: preliminary research for clinical practice guidelines. BMC Complement Altern Med. 2015;15(1):432. doi:10.1186/s12906-015-0956-1
9. Shin B-C, Kong JC, Park T-Y, Yang C-Y, Kang K-W, Choi S. Bee venom acupuncture for chronic low back pain: a randomised, sham-controlled, triple-blind clinical trial. Eur J Integrative Med. 2012;4(3):e271–e280.
10. Seo B-K, Han K, Kwon O, Jo D-J, Lee J-HJT. Efficacy of bee venom acupuncture for chronic low back pain: a randomized, double-blinded, sham-controlled trial. Toxins. 2017;9(11):361.
11. Lee YJ, Shin J-S, Lee J, et al. Usage report of pharmacopuncture in musculoskeletal patients visiting Korean medicine hospitals and clinics in Korea. BMC Complement Altern Med. 2016;16(1):292. doi:10.1186/s12906-016-1288-5
12. Ahn Y-J, Shin J-S, Lee J, et al. Evaluation of use and cost of medical care of common lumbar disorders in Korea: cross-sectional study of Korean Health Insurance Review and Assessment Service National Patient Sample data. BMJ open. 2016;6(9):e012432. doi:10.1136/bmjopen-2016-012432
13. Fairbank J, Couper J, Davies JB, O’Brien JP. The Oswestry low back pain disability questionnaire. Physiotherapy. 1980;66(8):271–273.
14. Kim D-Y, Lee S-H, Lee H-Y, et al. Validation of the Korean version of the Oswestry disability index. Spine. 2005;30(5):E123–E127. doi:10.1097/01.brs.0000157172.00635.3a
15. Roland M, Morris R. A study of the natural history of back pain: part 1: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;1:548.
16. Lee JS, Lee DH, Suh KT, Kim JI, Lim JM, Goh TS. Validation of the Korean version of the Roland–Morris disability questionnaire. Eur Spine J. 2011;20(12):2115–2119. doi:10.1007/s00586-011-1788-4
17. Farrar JT, Young JJP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158. doi:10.1016/S0304-3959(01)00349-9
18. Kim S-H, Jo M-W, Ahn J, Ock M, Shin S, Park J. Assessment of psychometric properties of the Korean SF-12 v2 in the general population. BMC Public Health. 2014;14(1):1086. doi:10.1186/1471-2458-14-1086
19. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Quality Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
20. Kim S-H, Ahn J, Ock M, et al. The EQ-5D-5L valuation study in Korea. Quality Life Res. 2016;25(7):1845–1852. doi:10.1007/s11136-015-1205-2
21. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
22. Borm GF, Fransen J, Lemmens WA. A simple sample size formula for analysis of covariance in randomized clinical trials. J Clin Epidemiol. 2007;60(12):1234–1238. doi:10.1016/j.jclinepi.2007.02.006
23. Ostelo RW, Deyo RA, Stratford P, et al. Interpreting change scores for pain and functional status in low back pain: towards international consensus regarding minimal important change. Spine. 2008;33(1):90–94. doi:10.1097/BRS.0b013e31815e3a10
24. Lauridsen HH, Hartvigsen J, Manniche C, Korsholm L, Grunnet-Nilsson N. Responsiveness and minimal clinically important difference for pain and disability instruments in low back pain patients. BMC. 2006;7(1):1–16.
25. Ford I, Norrie J. Pragmatic trials. N Eng J Med. 2016;375(5):454–463. doi:10.1056/NEJMra1510059
26. Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J Chronic Dis. 1967;20(8):637–648. doi:10.1016/0021-9681(67)90041-0
27. Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical trials. J Clin Epidemiol. 2009;62(5):499–505. doi:10.1016/j.jclinepi.2009.01.012
28. Thorpe KE, Zwarenstein M, Oxman AD, et al. A pragmatic–explanatory continuum indicator summary (PRECIS): a tool to help trial designers. J Clin Epidemiol. 2009;62(5):464–475. doi:10.1016/j.jclinepi.2008.12.011
29. Loudon K, Treweek S, Sullivan F, Donnan P, Thorpe KE, Zwarenstein M. The PRECIS-2 tool: designing trials that are fit for purpose. BMJ. 2015;350:h2147. doi:10.1136/bmj.h2147
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review and Meta-Analysis Protocol on How Best to Use Non-Pharmacologic Therapies to Manage Chronic Low Back Pain and Associated Depression
Guo Y, Ma Q, Zhou X, Yang J, He K, Shen L, Zhao C, Chen Z, Tan CIC, Chen J
Journal of Pain Research 2022, 15:3509-3521
Published Date: 4 November 2022
Changes in Pain Catastrophizing and Related Outcomes Following a Single-Session Empowered Relief Intervention Delivered by Physical Therapists in Workers with Low Back Pain: A Pilot Study
Carrière JS, Coutu MF, Darnall BD, Léonard G, Royer MP, Li MY, Bordeleau M, Durand MJ
Journal of Pain Research 2025, 18:4845-4857
Published Date: 17 September 2025