Back to Journals » Journal of Pain Research » Volume 19
Central Sensitization Severity in Chronic Low Back Pain: Associations with Sleep, Distress, Cortisol, and Visuospatial Working Memory
Authors Sahebalam M ![]() , Hatef B, Pirzad Jahromi G
, Hatef B, Pirzad Jahromi G
Received 4 December 2025
Accepted for publication 5 February 2026
Published 13 February 2026 Volume 2026:19 583843
DOI https://doi.org/10.2147/JPR.S583843
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Mohamad Sahebalam, Boshra Hatef, Gila Pirzad Jahromi
Neuroscience Research Center, Baqiyatallah University of Medical Sciences, Tehran, 14359-15381, Iran
Correspondence: Boshra Hatef, Neuroscience Research Center, Baqiyatallah University of Medical Sciences, Sheikh Bahaei Street, Tehran, 14359-15381, Iran, Email [email protected]
Background: Central sensitization (CS) is increasingly recognized as a key mechanism underlying chronic low back pain (CLBP), and has been linked to disturbed sleep, psychological distress, altered hypothalamic–pituitary–adrenal (HPA) axis function, low-grade inflammation, and cognitive dysfunction. However, few studies have simultaneously examined these domains in patients with different levels of CS compared with pain-free individuals.
Methods: In this cross-sectional study, adults with CLBP were classified into severe and mild CS groups using the Central Sensitization Inventory and were compared with healthy controls. Sleep quality, psychological distress, and pain-related cognition were assessed using the Pittsburgh Sleep Quality Index, Depression Anxiety Stress Scales-21, and pain measures. Morning salivary cortisol, interleukin-6 (IL-6), and fasting blood glucose were obtained as biological markers, and cognitive performance was evaluated using the Corsi Block-Tapping and Tower of London tasks. Group differences were analyzed using one-way ANOVA with Tukey post-hoc tests.
Results: Forty-two participants (patients with CLBP and pain-free controls) completed the study. Compared with both mild CS patients and controls, the severe CS group showed markedly poorer sleep quality and higher levels of psychological distress. Morning cortisol concentrations were significantly elevated only in the severe CS group, whereas no statistically significant differences were detected for fasting glucose or IL-6 between groups. On the Corsi Block-Tapping task, healthy controls outperformed both CS groups, indicating reduced visuospatial working memory in patients, whereas no significant group differences were observed on the Tower of London planning task.
Conclusion: Severe central sensitization in CLBP is associated with poor sleep, increased emotional distress, elevated morning cortisol, and deficits in visuospatial working memory, even in the absence of clear differences in IL-6 or fasting glucose. These findings support a biopsychosocial profile characterized by both neuroendocrine and cognitive alterations in patients with high levels of CS and highlight potential targets for multimodal assessment and intervention.
Plain Language Summary: Chronic low back pain is very common and often does not respond well to usual treatments. One important reason may be “central sensitization”, which means that the brain and spinal cord become overly sensitive and keep amplifying pain signals. People with chronic pain and central sensitization often also have poor sleep, emotional distress, and problems with thinking skills, but these relationships are not fully understood.
In this study, we examined adults with non-specific chronic low back pain who attended orthopedic clinics. We divided them into two groups based on their score on the Central Sensitization Inventory: a high central sensitization group and a low central sensitization group. We measured sleep quality, symptoms of depression, anxiety, and stress, morning levels of the stress hormone cortisol, inflammatory and metabolic markers (interleukin-6 and fasting blood glucose), and performance on tests of visuospatial working memory and planning.
People with high central sensitization reported worse sleep and higher emotional distress. They also showed higher morning cortisol levels and slightly poorer visuospatial working memory. In contrast, interleukin-6 and fasting blood glucose did not clearly differ between the groups. These findings suggest that poor sleep, psychological distress, stress-system changes, and subtle cognitive problems are important features of chronic low back pain with central sensitization, and they should be considered in assessment and treatment.
Keywords: central sensitization, chronic low back pain, cognitive function, cortisol, interleukin-6, psychological distress, sleep quality
Introduction
Chronic low back pain (CLBP) is a leading cause of disability worldwide and is increasingly understood as a condition in which nociceptive input interacts with central nervous system processes rather than reflecting peripheral pathology alone.1–3 Non-specific chronic low back pain refers to persistent low back pain in the absence of an identifiable structural, inflammatory, or neurological pathology, and represents the majority of cases encountered in clinical practice.
Focusing on non-specific CLBP is clinically relevant, as this category accounts for most patients seen in routine care and poses particular challenges for mechanism-based assessment and management. Central sensitization (CS) has emerged as a key mechanism underlying chronic pain, characterized by heightened responsiveness of nociceptive pathways and amplified pain perception in response to both noxious and non-noxious stimuli.1,2 This phenomenon can help explain why many patients with CLBP report disproportionate pain, widespread symptoms, and poor response to treatments targeting only peripheral structures.2,3
Beyond persistent pain, CS is closely linked to dysregulation of stress-related systems, particularly the hypothalamic–pituitary–adrenal (HPA) axis.4–7 Chronic stress and sustained pain can alter cortisol secretion patterns, which in turn influence immune responses, mood, and pain sensitivity.4–7 Morning cortisol is commonly used as an index of basal hypothalamic–pituitary–adrenal (HPA) axis activity and provides clinically relevant information about stress-system regulation, although it cannot capture full diurnal variation.
Neuroinflammatory processes and glial activation have also been implicated in the maintenance of central pain states, with cytokines such as interleukin-6 (IL-6) contributing to ongoing sensitization in conditions like fibromyalgia and chronic widespread pain.6,7 However, findings regarding specific hormonal and inflammatory markers in chronic pain populations remain heterogeneous, and it is unclear how such alterations relate to different levels of CS in patients with CLBP.4–7 Interleukin-6 (IL-6) was selected as a widely studied pro-inflammatory cytokine implicated in chronic pain conditions, while fasting blood glucose was included as a pragmatic metabolic marker reflecting interactions between stress, inflammation, and metabolic regulation.
Together, these markers allow a focused, clinically feasible assessment of neuroendocrine and inflammatory correlates of central sensitization.
Sleep disturbance and psychological distress are highly prevalent in chronic pain and show a bidirectional relationship with pain intensity and disability.8–11 Poor sleep has been associated with heightened pain sensitivity, increased emotional reactivity, and greater risk of pain chronification, whereas pain itself disrupts sleep continuity and quality, creating a vicious cycle.8–10 Cognitive-behavioral and multidisciplinary approaches that target both sleep and pain have been shown to improve clinical outcomes, underscoring the importance of addressing these domains concurrently.12,13 Yet, few studies have examined sleep and emotional distress specifically in relation to CS severity within CLBP populations.
Cognitive changes represent another important, but often underrecognized, aspect of chronic pain. Evidence indicates that patients with persistent pain can exhibit deficits in attention, working memory, and executive functioning, possibly reflecting overlapping neural circuits for pain, emotion, and cognition.14,15 Experimental and neuroimaging work has documented structural and functional brain alterations in chronic pain that may contribute to cognitive inefficiencies and altered pain modulation.3,14,15 Nevertheless, the extent to which cognitive performance differs between CLBP patients with severe versus mild CS, and how this relates to neuroendocrine and psychological factors, is not well understood.
Although alterations in sleep, stress-related biology, and cognition have been reported in chronic pain more broadly, evidence specific to non-specific CLBP remains limited and heterogeneous, particularly in studies that stratify patients by central sensitization severity.
Despite growing recognition that chronic pain is best explained within a biopsychosocial framework, integrating biological, psychological, and social determinants,16,17 relatively few studies have simultaneously assessed sleep quality, psychological distress, neuroendocrine and inflammatory markers, and cognitive functioning in patients stratified by CS severity. In the present study, central sensitization is operationalized using the Central Sensitization Inventory (CSI), representing a symptom-based stratification of probable CS rather than a diagnosis based on quantitative sensory testing or detailed sensory profiling. The present study aimed to address this gap by comparing individuals with CLBP and severe CS, CLBP with mild CS, and pain-free controls. Specifically, we hypothesized that (1) patients with severe CS would show poorer sleep quality, greater depression, anxiety, and stress, elevated cortisol, and more pronounced cognitive deficits than both mild CS patients and controls; and (2) mild CS patients would display intermediate alterations, consistent with a graded expression of CS within the biopsychosocial model of chronic pain.1–3,16,17
From a clinical perspective, stratifying patients by central sensitization severity may help identify individuals who are more likely to benefit from integrated interventions targeting sleep disturbance and psychological distress. In addition, examining cognitive performance may have practical implications for rehabilitation, as working memory and planning abilities can influence treatment adherence, learning, and engagement with self-management strategies.
Methods
Study Design and Participants
This cross-sectional study was conducted between July 2024 and April 2025 at the outpatient orthopedic clinics of Iran University of Medical Sciences, Tehran, Iran and was approved by the Institutional Review Board (IR.BMSU.BAQ.REC.1404.027). All procedures adhered to the Declaration of Helsinki, and all participants provided written informed consent prior to participation.
Adults aged 18–65 years with non-specific CLBP of at least 3 months’ duration were recruited from outpatient services and the community. Exclusion criteria included specific spinal pathology (eg, fracture, tumor, infection), previous spinal surgery, diagnosed neurological or severe psychiatric disorders, systemic inflammatory or endocrine disease, current pregnancy, use of systemic corticosteroids or immunosuppressive medication, and inability to complete the questionnaires or cognitive tasks. Additional exclusion criteria included acute infection within the preceding two weeks, current smoking or nicotine use on the day of testing, shift work, and use of medications known to affect cortisol secretion, immune function, or cognitive performance. Pain-free healthy controls were matched to the patient groups for age and sex and had no history of chronic musculoskeletal pain or major neurological or psychiatric conditions.
A total of 42 participants were enrolled and allocated to three groups: patients with CLBP and severe CS, patients with CLBP and mild CS, and healthy controls. Patients with CLBP were classified into mild and severe central sensitization (CS) groups based on the Central Sensitization Inventory (CSI), using a cut-off score of 35. Participants with CSI scores ≥35 were classified as having severe CS, whereas those scoring <35 were classified as having mild CS. This cut-off has been previously used to identify clinically meaningful levels of CS-related symptomatology in chronic pain populations.18–20
We acknowledge that CSI-based classification may overlap with psychological distress and symptom burden; therefore, CS severity in the present study should be interpreted as a dimensional, symptom-based stratification rather than a mechanistic diagnosis.
Healthy controls scored below the clinical threshold for CS and reported no current low back pain. The sample size was determined based on feasibility and the available pool of eligible participants.
Clinical and Questionnaire Measures
All assessments were performed in a quiet, temperature-controlled room by a trained examiner following a standardized protocol. Demographic and clinical data included age, sex, body mass index (BMI), low back pain duration, and current pain intensity. Pain intensity over the past week was assessed using a 10-cm visual analog scale (VAS), anchored from “no pain” to “worst imaginable pain.”
Central sensitization symptoms were evaluated using the CSI, a 25-item self-report questionnaire that measures somatic and emotional symptoms associated with CS and has demonstrated good reliability and validity in chronic pain populations.18,19 We administered the validated Persian version of the CSI, which has shown good psychometric properties in patients with chronic pain.21
Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI), a widely used measure that yields a global score reflecting subjective sleep disturbances over the past month.22 The validated Persian version of the PSQI, which has demonstrated acceptable reliability and validity in Iranian samples, was used in the present study.23
Psychological distress was measured using the Depression Anxiety Stress Scales-21 (DASS-21), which provides separate subscale scores for depression, anxiety, and stress; higher scores indicate greater symptom severity.24 We used the validated Persian version of the DASS-21, which has shown good psychometric characteristics among Iranian health professionals.25
All assessments were conducted by a trained examiner who was blinded to participants’ group allocation (severe CS, mild CS, or control).
Biological Markers
Biological markers included morning salivary cortisol, IL-6, and fasting blood glucose (FBG). The sampling window was anchored to clock time (07:00–09:00 a.m.) rather than time since awakening; however, participants’ self-reported wake time was recorded on the day of testing to minimize between-subject variability. Participants were instructed to abstain from caffeine, alcohol and vigorous physical activity for at least 24 hours prior to sampling, and compliance was confirmed verbally on the day of assessment. Oral hygiene (mouth rinsing with water) was performed immediately before saliva collection. Because cortisol is highly sensitive to circadian timing and acute state factors, a single morning sample provides a snapshot of basal HPA-axis activity but cannot capture diurnal dynamics.
To minimize acute state-related influences on cortisol, participants were required to have had adequate sleep the night before sampling and to report no unusual psychological stress. If a participant reported poor sleep quality or excessive stress on the day of testing, biological sampling was postponed and rescheduled. Saliva samples for cortisol and IL-6 analysis were collected in sterile commercial saliva collection tubes with swabs, and were immediately stored on ice and subsequently frozen at –20°C until analysis. Blood samples were obtained by venipuncture FBG determination.
Cortisol and IL-6 concentrations were measured using commercially available enzyme-linked immunosorbent assay (ELISA) kits according to the manufacturers’ instructions. All samples were run in duplicate, and intra- and inter-assay coefficients of variation below 10% were accepted as valid. No samples fell below the detection limit, and no statistical outliers were excluded from analyses. Fasting blood glucose was analyzed using standard automated laboratory procedures at the hospital’s central laboratory.
Cognitive Assessment
Cognitive testing was conducted in a quiet, temperature-controlled room with standardized instructions. Participants completed brief practice trials before each task to ensure task comprehension. The order of cognitive tasks was fixed across participants; given the brief duration of the tasks, fatigue effects were considered minimal but cannot be fully excluded. Cognitive performance was evaluated using two standardized neuropsychological tests focusing on visuospatial working memory and executive planning. The Corsi Block-Tapping task was used to assess visuospatial working memory.26 Participants were required to reproduce sequences of block taps in the same order as demonstrated by the examiner, with sequence length increasing progressively. The primary outcome was the total number of correctly reproduced sequences across all trials.
Executive functioning and planning were measured using the Tower of London (TOL) task.27 In this task, participants were presented with an initial and a target configuration of colored balls on pegs and were instructed to reach the target configuration in as few moves as possible, following standard rules. After a practice phase, participants completed a series of problems of increasing difficulty. The main outcome measure was the total number of moves required to solve the problems, with higher values reflecting less efficient planning. Both cognitive tests were administered in a fixed order by a trained examiner, and standardized instructions were used for all participants.
Statistical Analysis
Data were analyzed using SPSS (version 26.0). Continuous variables are presented as mean ± standard deviation (SD) and categorical variables as frequencies and percentages. Group differences in demographic and clinical variables (age, BMI, sex) were examined using one-way analysis of variance (ANOVA) and chi-square tests, as appropriate. Separate one-way ANOVAs were conducted to compare the three groups (severe CS, mild CS, healthy controls) on sleep quality (PSQI), psychological distress (DASS-21 subscales), biological markers (morning salivary cortisol, IL-6, FBG), and cognitive performance (Corsi Block-Tapping and TOL outcomes). When a significant main effect of group was detected, Tukey’s honestly significant difference (HSD) test was applied for post-hoc pairwise comparisons. Statistical significance was set at p<0.05 (two-tailed).
Results
Demographic and Clinical Characteristics
A total of 42 participants were included in the analyses, comprising patients with CLBP and severe CS, patients with CLBP and mild CS, and pain-free controls. Given the exploratory nature of the study, sleep quality (PSQI), psychological distress (DASS-21), morning cortisol, and visuospatial working memory (Corsi task) were considered primary outcomes. Other variables were treated as secondary/exploratory outcomes. Assumptions of normality were inspected visually and using Shapiro–Wilk tests. When distributions deviated from normality, results were interpreted with caution. The three groups were comparable in age, BMI, and sex distribution (Table 1). As expected, both CLBP groups reported substantially higher pain intensity than controls, and CSI scores were highest in the severe CS group, intermediate in the mild CS group, and lowest in controls, consistent with the intended group classification.
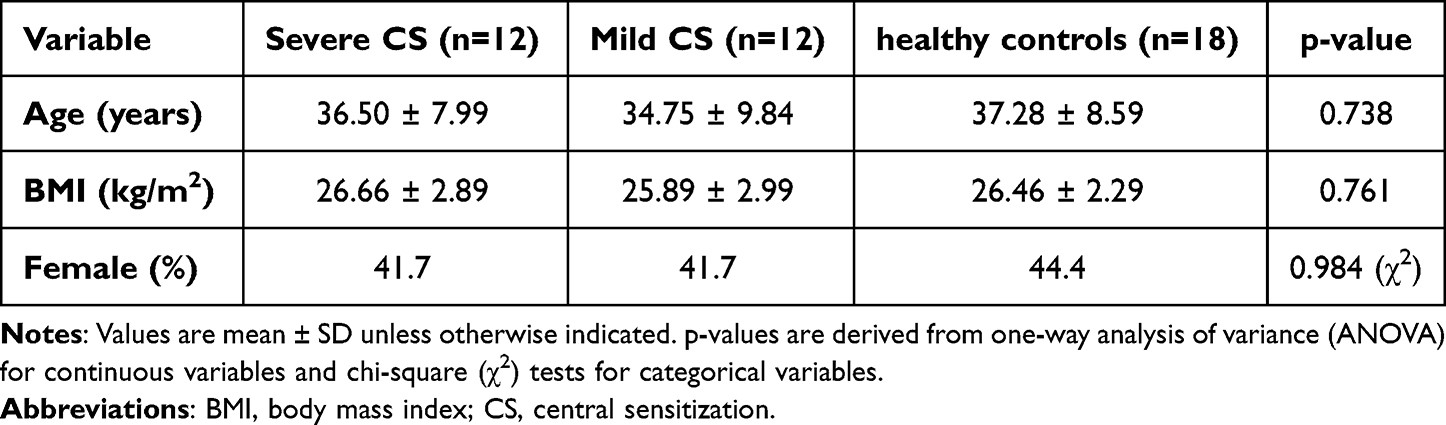 |
Table 1 Demographic and Clinical Characteristics of Participants |
Sleep Quality
There was a clear group effect for sleep quality (Table 2, Figure 1). Patients with severe CS reported the poorest sleep, whereas controls reported the best sleep, with the mild CS group showing intermediate levels. Post-hoc comparisons indicated that sleep quality in the severe CS group was significantly worse than in both the mild CS and control groups, while no statistically significant difference emerged between mild CS patients and controls.
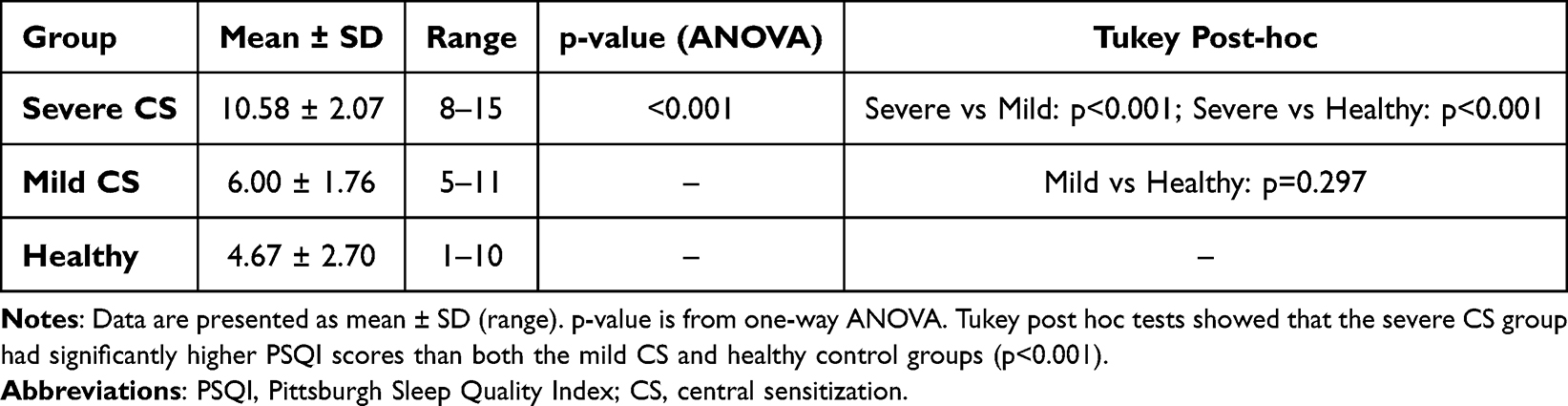 |
Table 2 Sleep Quality (PSQI) Across Groups |
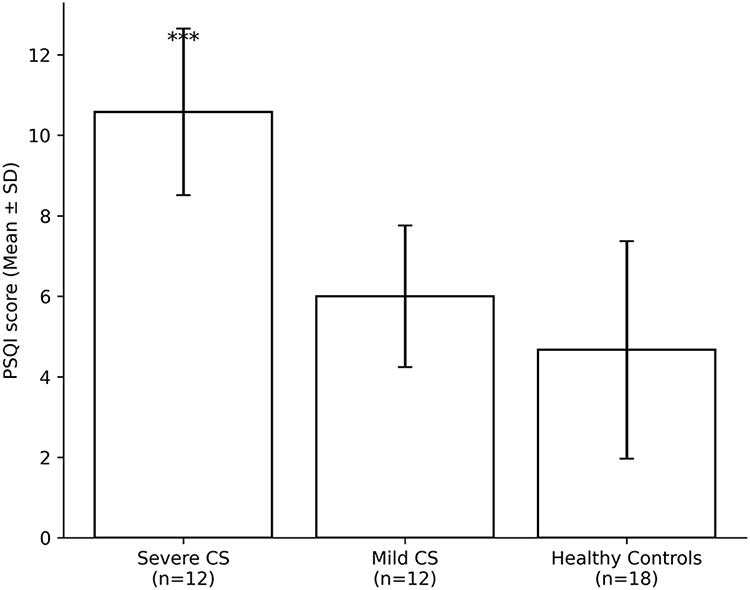 |
Figure 1 Sleep quality assessed by the Pittsburgh Sleep Quality Index (PSQI) across study groups. Data are presented as mean ± SD. Sample sizes are indicated below each group. ***p < 0.001 compared with Mild CS and Healthy Controls (one-way ANOVA with Tukey post-hoc test). |
Psychological Distress
Group differences were also observed for psychological distress (Table 3, Figure 2). Overall, patients with severe CS showed higher levels of depressive symptoms, anxiety, and stress compared with controls. Anxiety and stress were most pronounced in the severe CS group, with the mild CS group generally showing intermediate values between severe CS and controls. For depression, severe CS patients differed significantly from controls, whereas scores in the mild CS group did not consistently differ from either of the other two groups.
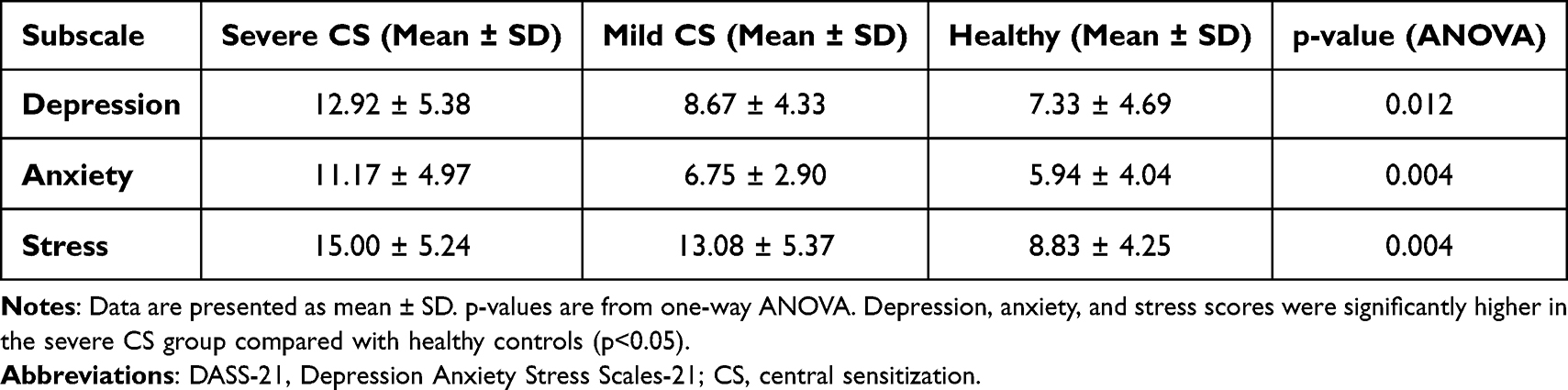 |
Table 3 Psychological Distress (DASS-21) Across Groups |
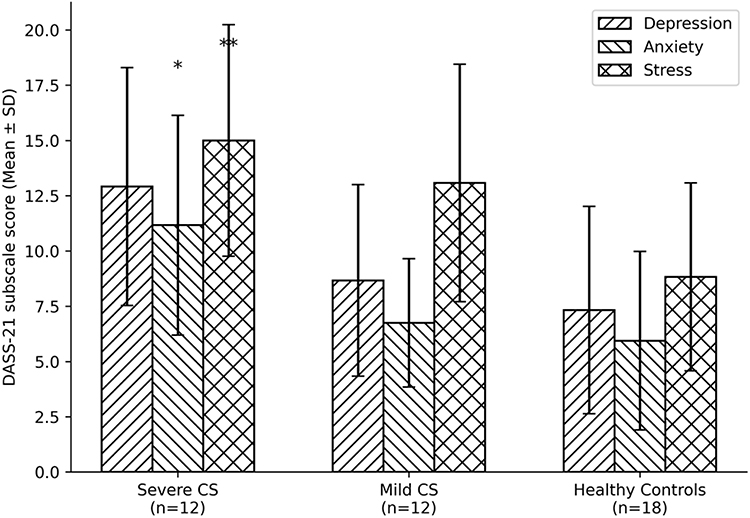 |
Figure 2 Depression, anxiety, and stress scores (DASS-21) across study groups. Data are presented as mean ± SD. Sample sizes are shown below each group. *p < 0.05, **p < 0.01 for main group effects (one-way ANOVA). |
Biological Markers
Regarding biological markers, a significant group effect was found for morning cortisol (Table 4, Figure 3). Patients with severe CS exhibited higher cortisol levels than both mild CS patients and controls, whereas cortisol values did not differ meaningfully between the mild CS and control groups. In contrast, no significant group differences were detected for FBG or IL-6, indicating that these metabolic and inflammatory markers were broadly comparable across all three groups.
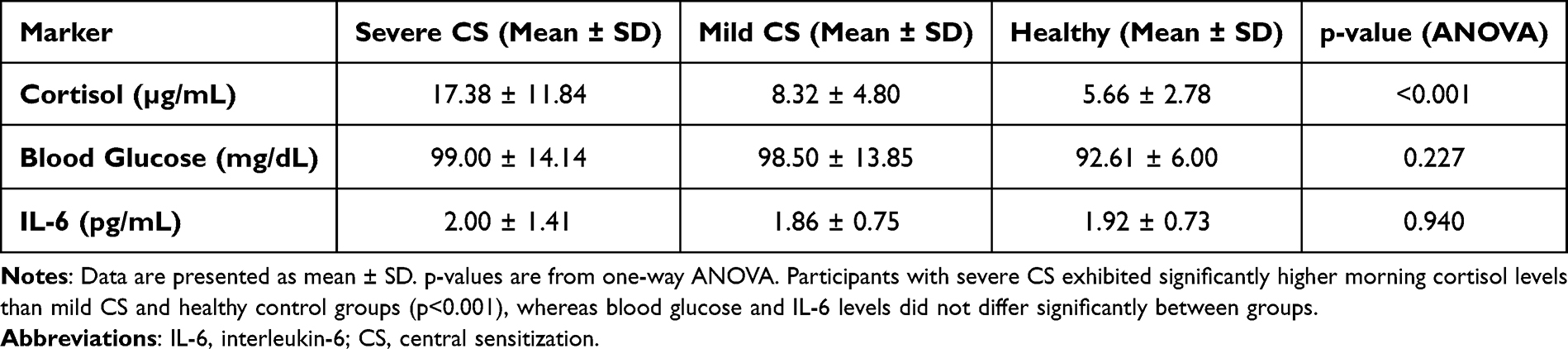 |
Table 4 Biological Markers Across Groups |
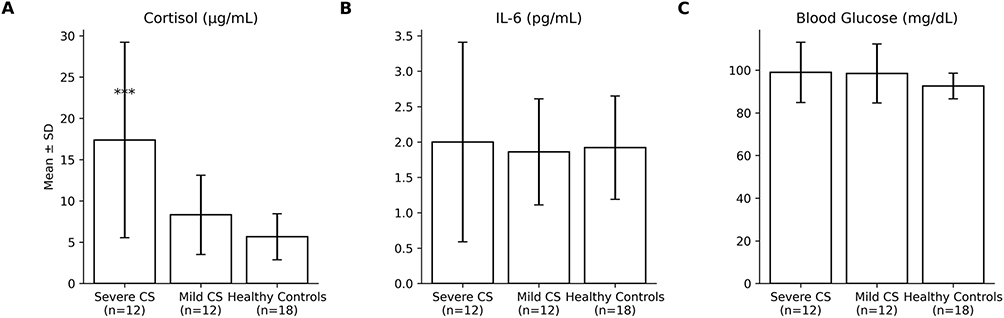 |
Figure 3 Biological markers across groups. (A) Morning salivary cortisol (µg/mL), (B) interleukin-6 (IL-6; pg/mL), and (C) fasting blood glucose (mg/dL) in participants with severe central sensitization (CS), mild CS, and healthy controls. Bars represent mean ± standard deviation (SD). Sample sizes are indicated below each group. ***p < 0.001 for severe CS compared with both mild CS and healthy controls. No statistically significant between-group differences were detected for IL-6 or fasting blood glucose. |
Cognitive Performance
Group differences emerged for visuospatial working memory but not for executive planning (Table 5, Figure 4). On the Corsi Block-Tapping task, healthy controls performed better than both CS groups, while severe and mild CS patients showed similar levels of performance. In contrast, no significant differences between groups were observed on the TOL task, suggesting that overall planning efficiency was relatively preserved despite the presence of chronic pain and elevated CS in the patient groups.
 |
Table 5 Cognitive Performance Outcomes Across Groups |
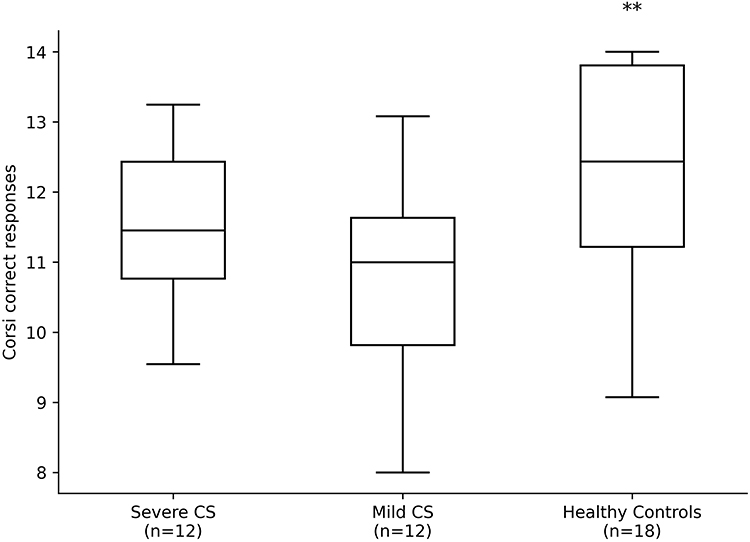 |
Figure 4 Visuospatial working memory performance assessed by the Corsi Block-Tapping task. Boxes represent median and interquartile range, with whiskers indicating the data range. Sample sizes are shown below each group. **p < 0.01 for group effect (one-way ANOVA). |
Discussion
This cross-sectional study investigated the inter-relationships among clinical pain, CS-related symptoms, sleep quality, psychological distress, and cognitive performance in adults with chronic low back pain (CLBP) compared with pain-free controls. Overall, participants with CLBP and probable CS, as indicated by elevated CSI scores, reported higher pain intensity, poorer sleep quality, greater emotional distress, and subtle deficits in working memory when compared with pain-free controls. These findings support contemporary conceptualizations of CS as a multidimensional phenomenon involving sensory, affective, and cognitive domains rather than a purely nociceptive process.1–3,14,16
Sleep Quality and Pain–Sensitization Interactions
Consistent with prior experimental and clinical work, we observed that poorer subjective sleep quality was closely associated with higher pain intensity and greater CS-related symptom burden.8–11 Chronic pain and sleep disturbance are known to interact bidirectionally: sleep loss amplifies pain sensitivity and reduces endogenous pain inhibition, whereas persistent pain disrupts sleep continuity and architecture.8–10 In patients with chronic musculoskeletal pain, alterations in sleep continuity and reduced slow-wave and REM sleep have been linked to lower pain thresholds, enhanced temporal summation, and impaired conditioned pain modulation.8,10 These mechanisms are compatible with the present observation that CLBP participants with higher CSI scores also demonstrated worse PSQI scores compared with controls.
The pattern of results is in line with data from other chronic pain cohorts—including studies in chronic musculoskeletal and orofacial pain—showing that poor sleep quality is common and often correlates with higher pain intensity and more complex pharmacotherapy.8–11 In our sample, sleep disturbance remained a robust correlate of pain and CS-related symptoms, suggesting that sleep should be considered a core treatment target in CS-phenotyped CLBP rather than a secondary complaint.8–13
Psychological Distress and Central Sensitization
Participants with CLBP and probable CS also reported higher levels of depression, anxiety, and stress compared with controls. This is consistent with the growing literature indicating that altered pain processing in CS rarely occurs in isolation but is embedded within a broader affective and cognitive vulnerability profile.2,3,14–17 Mood disturbances can amplify pain perception, promote pain catastrophizing, and interfere with descending inhibitory control, thereby contributing to sustained pain and disability.2,3,16,17 From a clinical standpoint, these findings support the use of biopsychosocial assessment frameworks and CS screening tools, such as the CSI, to identify patients in whom emotional distress and CS-related symptom clusters are likely to maintain pain.1–3,16–19 Such patients are less likely to respond to strictly biomedical or structurally oriented interventions and may benefit more from multimodal care combining pain neuroscience education, graded activity or exercise, cognitive–behavioral strategies, and targeted sleep interventions.2,3,8,12,13,16–19
Cortisol, IL-6 and Stress-System Markers
We also explored markers of stress-system activity by assessing morning salivary cortisol and IL-6. Group differences in cortisol were modest, and IL-6 levels did not differ significantly between CLBP participants and controls. The observed elevation in morning cortisol should be interpreted cautiously, as single time-point measurements are sensitive to wake time and acute stress and do not capture diurnal HPA-axis dynamics. Therefore, cortisol findings should be viewed as suggestive of altered HPA-axis activity rather than definitive evidence of neuroendocrine dysregulation. These findings are broadly in line with systematic reviews in fibromyalgia and other diffuse chronic pain syndromes suggesting that, although some pro-inflammatory cytokines (eg, IL-6, IL-8, TNF-α) may be elevated on average, effect sizes are small and findings are heterogeneous, likely reflecting methodological differences, medication effects, and the clinical heterogeneity of chronic pain populations.6,7 Our results suggest that single-time-point measurements of IL-6 may be insufficiently sensitive to detect subtle immune dysregulation in relatively young adults with CLBP in this sample. Null findings for IL-6 do not contradict the biopsychosocial model of central sensitization but likely reflect the variability of inflammatory markers and the limitations of single-time-point, cross-sectional assessments.
Rather than interpreting the absence of significant IL-6 differences as evidence against neuroimmune involvement, it may be more appropriate to view it as a limitation of cross-sectional sampling and the focus on one cytokine.4–7 Longitudinal designs with repeated sampling, broader panels of inflammatory markers, and integration with quantitative sensory testing may be better suited to delineate the contribution of neuroinflammatory processes to CS in CLBP.2,4–7
Cognitive Performance in CLBP with Probable Central Sensitization
Consistent with our hypotheses, CLBP participants with higher CSI scores demonstrated subtle but meaningful reductions in working memory span on the Corsi task relative to controls, while planning performance on the TOL did not differ significantly between groups. Importantly, this pattern suggests a targeted difference in visuospatial working memory rather than a generalized cognitive impairment, as executive planning performance was preserved across groups. These findings align with meta-analyses showing that individuals with chronic pain exhibit small-to-moderate impairments in working memory and executive functions compared with pain-free controls.14,15 Working memory and executive abilities are essential for goal-directed behavior, adherence to self-management strategies, and flexible coping with fluctuating symptoms.14,15 Chronic pain may interfere with these processes through several mechanisms, including persistent pain-related attentional capture, sleep disturbance, emotional distress, and potential CS-related alterations in brain networks subserving executive control.3,8–10,14,15 These findings should be interpreted in light of potential confounders known to influence cognitive performance, including sleep quality, depressive symptoms, medication use, and pain intensity, which were not formally controlled for in the present analyses.
Neuroimaging studies in centralized pain conditions, such as fibromyalgia, have reported altered functional connectivity within default mode, salience, and executive networks, which may provide a neural substrate for both increased pain sensitivity and cognitive inefficiency.3,14 Although the magnitude of cognitive differences in our sample was modest, even small decrements in working memory could influence the ability of individuals with CLBP to perform complex tasks in daily life or work settings.These results underscore the importance of considering cognitive functioning when designing rehabilitation programs for CS-phenotyped CLBP, for example by simplifying educational materials, using more structured behavioral plans, and integrating cognitive strategy training where appropriate.14–17
Integration Within a Biopsychosocial and Precision-Medicine Framework
Taken together, the present findings support the view that CLBP with probable CS is characterized by a constellation of sensory, affective, sleep-related, and cognitive alterations rather than by spinal pathology alone.1–3,16,17 Within such a framework, CS is not a unitary diagnosis but a clinically useful construct that helps identify patients in whom altered central pain processing, emotional dysregulation, and sleep disturbance jointly contribute to pain chronicity and treatment resistance.1–3,16–19 Our results are consistent with proposals that CS-phenotyping, for example using the CSI combined with clinical examination, could guide more individualized treatment selection.2,18,19 Patients with high CSI scores, prominent sleep disturbance, and psychological distress may derive particular benefit from multidisciplinary programs that integrate pain neuroscience education, graded activity or exercise therapy, cognitive–behavioral or acceptance-based interventions, and structured sleep optimization.2,3,8,12,13,16–19
Emerging evidence further suggests that adequately addressing sleep disturbance may enhance analgesic outcomes and reduce the need for high-risk pharmacotherapies such as long-term opioids or sedative–hypnotics.8–10,12,13 Incorporating CS-informed assessment and management into routine care could therefore support a more precise and efficient allocation of limited clinical resources across different healthcare settings.2,16–19
Strengths and Limitations
This study has several strengths, including the recruitment of a relatively homogeneous sample of adults with and without CLBP, the concurrent assessment of CS-related symptoms, sleep, mood, endocrine and immune markers, and the inclusion of objective cognitive tests tapping both working memory and planning. The use of validated instruments such as the CSI, PSQI, and DASS-21, as well as their psychometrically supported Persian versions, enhances the interpretability and comparability of our findings with prior literature.18–25
However, several limitations should be acknowledged. First, the cross-sectional design precludes causal inferences about the directionality of associations among pain, CS-related symptoms, sleep, and cognitive performance. Longitudinal and interventional studies are needed to determine whether improving sleep and mood can reduce CS-related symptom burden and enhance cognitive functioning in CLBP.3,9–11 Accordingly, the present findings should be viewed as exploratory and hypothesis-supporting rather than definitive.
Second, sleep was assessed using a self-report questionnaire rather than polysomnography or actigraphy. Although the PSQI is widely used and well validated, objective sleep measures would allow more detailed characterization of sleep architecture and its relationship to pain and cognitive outcomes.8–11,22 Third, only morning cortisol and a single pro-inflammatory cytokine (IL-6) were measured. More comprehensive and repeated biomarker assessments may be required to detect subtle HPA-axis or immune alterations in relatively young and physically active individuals.4–7
Finally, the sample size was modest, and the study may have been underpowered to detect small effect sizes, particularly for biomarker and cognitive outcomes. Replication in larger and more diverse CLBP populations, including cohorts from different clinical and community settings and with a broader age range and higher proportion of women, will be important to confirm the generalizability of these findings.4–7,14–17
Clinical Implications and Future Directions
Despite these limitations, the present study adds to a growing body of evidence indicating that CLBP with probable CS should be conceptualized and managed within a biopsychosocial, precision-medicine framework.1–3,16–19 Clinicians caring for individuals with CLBP are encouraged to systematically assess CS-related symptoms (eg, via CSI), sleep quality, and emotional distress, and to recognize that cognitive load and planning demands may influence patients’ capacity to engage with complex rehabilitation programs.14–19,21,23 Future research should examine whether tailored interventions that simultaneously target sleep, mood, and pain-related education yield greater improvements in pain, function, and readiness than standard unimodal approaches in CS-phenotyped CLBP.2,3,8,12,13,16–19 In addition, integrating quantitative sensory testing, neuroimaging, and multimodal biomarker panels may help refine CS-phenotypes and identify subgroups most likely to benefit from specific non-pharmacological and pharmacological treatments.2–7
Conclusions
Severe central sensitization in individuals with non-specific chronic low back pain is associated with poor sleep quality, increased emotional distress, dysregulated morning cortisol, and subtle deficits in visuospatial working memory, even in the absence of clear differences in IL-6 or fasting glucose. These findings support a biopsychosocial profile characterized by neuroendocrine and cognitive alterations in patients with high levels of CS and highlight sleep, mood, and cognitive functioning as key targets for multimodal assessment and intervention. Longitudinal and interventional studies are needed to determine whether treatments that simultaneously address these domains can reduce CS-related symptom burden and improve pain and function in this population.
Abbreviations
CLBP, chronic low back pain; CS, central sensitization; HPA, hypothalamic–pituitary–adrenal; IL-6, interleukin-6; FBG, fasting blood glucose; CSI, Central Sensitization Inventory; PSQI, Pittsburgh Sleep Quality Index; DASS-21, Depression Anxiety Stress Scales-21; BMI, body mass index; VAS, visual analog scale; TOL, Tower of London; SD, standard deviation; ANOVA, analysis of variance; REM, rapid eye movement.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional and ethical restrictions but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This cross-sectional study was approved by the Research Ethics Committee of Baqiyatallah Hospital, Baqiyatallah University of Medical Sciences, Tehran, Iran (approval ID: IR.BMSU.BAQ.REC.1404.027). The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). All participants provided written informed consent prior to enrollment. Patient recruitment and data collection were performed at the outpatient orthopedic clinics of Iran University of Medical Sciences, Tehran, Iran, under a formal memorandum of understanding (MoU) between Baqiyatallah University of Medical Sciences and Iran University of Medical Sciences, which granted permission for the study activities at the site. This collaboration was facilitated because the principal investigator is a PhD student at Iran University of Medical Sciences, and patients were more accessible there.
Consent for Publication
Consent for publication is not applicable. The manuscript does not contain any individual person’s identifiable data in any form.
Acknowledgments
The authors would like to thank the participants for their time and commitment to this study and the staff of the outpatient orthopedic clinics at Iran University of Medical Sciences for their support during recruitment and data collection.
The authors used the generative AI tool ChatGPT (model: GPT-5.1 Thinking, OpenAI) to assist with language editing and refining the plain language summary. All content generated by the tool was carefully reviewed, edited, and approved by the authors, who take full responsibility for the integrity and accuracy of the final manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3):S2–13. doi:10.1016/j.pain.2010.09.030
2. Nijs J, George SZ, Clauw DJ, et al. Central sensitisation in chronic pain conditions: latest discoveries and their potential for precision medicine. Lancet Rheumatol. 2021;3(5):e742–e753. doi:10.1016/S2665-9913(21)00032-1
3. Clauw DJ. Fibromyalgia: a clinical review. JAMA. 2014;311(15):1547–1555. doi:10.1001/jama.2014.3266
4. Sanabria-Mazo JP, Colomer-Carbonell A, Carmona-Cervelló M. Immune-inflammatory and hypothalamic-pituitary-adrenal axis biomarkers in individuals with non-specific low back pain: a systematic review. Front Immunol. 2022;13:945513. doi:10.3389/fimmu.2022.945513
5. Kumbhare D, Hassan S, Diep D, et al. Potential role of blood biomarkers in patients with fibromyalgia: a systematic review with meta-analysis. Pain. 2022;163(7):1232–1253. doi:10.1097/j.pain.0000000000002510
6. Uçeyler N, Häuser W, Sommer C. Systematic review with meta-analysis: cytokines in fibromyalgia syndrome. BMC Musculoskelet Disord. 2011;12(1):245. doi:10.1186/1471-2474-12-245
7. O’Mahony LF, Srivastava A, Mehta P, Ciurtin C. Is fibromyalgia associated with a unique cytokine profile? A systematic review and meta-analysis. Rheumatology. 2021;60(6):2602–2614. doi:10.1093/rheumatology/keab146
8. Nijs J, Mairesse O, Neu D, et al. Sleep disturbances in chronic pain: neurobiology, assessment, and treatment in physical therapist practice. Phys Ther. 2018;98(5):325–335. doi:10.1093/ptj/pzy020
9. Li MT, Robinson CL, Ruan QZ, Surapaneni S, Southerland W. The influence of sleep disturbance on chronic pain. Curr Pain Headache Rep. 2022;26(10):795–804. doi:10.1007/s11916-022-01074-2
10. Haack M, Simpson N, Sethna N, Kaur S, Mullington J. Sleep deficiency and chronic pain: potential underlying mechanisms and clinical implications. Neuropsychopharmacology. 2020;45(1):205–216. doi:10.1038/s41386-019-0439-z
11. Liang M, Zheng Y, Zhu L, et al. A narrative review of the reciprocal relationship between sleep deprivation and chronic pain. J Pain Res. 2023;16:1579–1595.
12. Afolalu EF, Ramlee F, Tang NKY. Effects of sleep changes on pain-related health outcomes in the general population: a systematic review of longitudinal studies with meta-analysis. Sleep Med Rev. 2017;38:107–116.
13. Morin CM, Vallières A, Guay B, et al. Cognitive behavioral therapy, singly and combined with medication, for persistent insomnia: a randomized controlled trial. JAMA. 2009;301(19):2005–2015. doi:10.1001/jama.2009.682
14. Berryman C, Stanton TR, Bowering JK, Tabor A, McFarlane A, Moseley LG. Evidence for working memory deficits in chronic pain: a systematic review and meta-analysis. Pain. 2013;154(8):1181–1196. doi:10.1016/j.pain.2013.03.002
15. Berryman C, Stanton TR, Bowering KJ, et al. Do people with chronic pain have impaired executive function? A meta-analytical review. Clin Psychol Rev. 2014;34(7):563–579. doi:10.1016/j.cpr.2014.08.003
16. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
17. Gupta A, Silman AJ, Ray D, et al. The role of psychosocial factors in predicting the onset of chronic widespread pain: results from a prospective population-based study. Rheumatology. 2006;46(4):666–671. doi:10.1093/rheumatology/kel363
18. Neblett R, Cohen H, Choi Y, et al. The Central Sensitization Inventory (CSI): establishing clinically significant values for identifying central sensitivity syndromes in an outpatient chronic pain sample. J Pain. 2013;14(5):438–445. doi:10.1016/j.jpain.2012.11.012
19. Mayer TG, Neblett R, Cohen H, et al. The development and psychometric validation of the central sensitization inventory. Pain Pract. 2012;12(4):276–285. doi:10.1111/j.1533-2500.2011.00493.x
20. Zheng X, Lamoth CJC, Timmerman H, et al. Establishing central sensitization inventory cut-off values in chronic low back pain patients by unsupervised machine learning. Comput Biol Med. 2024;178:108739. doi:10.1016/j.compbiomed.2024.108739
21. Noorollahzadeh K, Kahrizi S, Gholami Fesharaki M, Heidarian M, Neblett R, Behzadipour S. Cross-cultural adaptation and psychometric validation of the Persian version of the central sensitization inventory. Musculoskelet Sci Pract. 2021;51:102269.
22. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Farrahi Moghaddam J, Nakhaee N, Sheibani V, Garrusi B, Amirkafi A. Reliability and validity of the Persian version of the Pittsburgh sleep quality index (PSQI-P). Sleep and Breathing. 2012;16(1):79–82. doi:10.1007/s11325-010-0478-5
24. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales.
25. Kakemam E, Navvabi E, Albelbeisi AH, Saeedikia F, Rouhi A, Majidi S. Psychometric properties of the Persian version of depression anxiety stress scale-21 items (DASS-21). BMC Health Services Res. 2022;22(1):111.
26. Berch DB, Krikorian R, Huha EM. The corsi block-tapping task: methodological and theoretical considerations. Brain Cogn. 1998;38(3):317–338. doi:10.1006/brcg.1998.1039
27. Shallice T. Specific impairments of planning. Philos Trans R Soc Lond B Biol Sci. 1982;298(1089):199–209.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Prospective Biopsychosocial Repeated Measures Study of Stress and Dropout from Substance Addiction Treatment
Bøhle K, Otterholt E, Bjørkly SK
Substance Abuse and Rehabilitation 2023, 14:61-75
Published Date: 13 July 2023
Neurocognitive Characteristics of Subjective Cognitive Decline and Its Association with Objective Cognition, Negative Emotion, and Sleep Quality in Chinese Elderly
Wu Y, Mao Z, Cui F, Fan J, Yuan Z, Tang L
Neuropsychiatric Disease and Treatment 2023, 19:2261-2270
Published Date: 25 October 2023
The Sequelae and Moderators of Influence of Dandruff on Mental Health Among Mainland Chinese Adults
Chan CS, Smith T, He Z, Garter C
Clinical, Cosmetic and Investigational Dermatology 2024, 17:1333-1346
Published Date: 11 June 2024
The Impact of Anesthetic Management Under Bispectral Index Monitoring on the Early Recovery Quality of Elderly Patients Undergoing Laparoscopic Surgery: A Blinded Randomized Controlled Trial
Shi M, Long Y, Zhou Z, Huang L, Wu D, Zhang X
Clinical Interventions in Aging 2025, 20:597-612
Published Date: 14 May 2025
Association Between Sleep Quality and Cognitive Function in Patients with Hypertension in Rural Areas of Shanxi Province, China: The Chain Mediating Role of Anxiety and Depression
Li S, Liang R, Liu J, Sun W, Wang J, Li S, Zhao S, Niu Q, Yu H, Zhang H, Qin X, Bai R, Li Y
Psychology Research and Behavior Management 2026, 19:593258
Published Date: 7 April 2026