Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Neurocognitive Characteristics of Subjective Cognitive Decline and Its Association with Objective Cognition, Negative Emotion, and Sleep Quality in Chinese Elderly
Authors Wu Y ![]() , Mao Z, Cui F, Fan J, Yuan Z, Tang L
, Mao Z, Cui F, Fan J, Yuan Z, Tang L
Received 16 July 2023
Accepted for publication 18 October 2023
Published 25 October 2023 Volume 2023:19 Pages 2261—2270
DOI https://doi.org/10.2147/NDT.S430929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Yue Wu,1,* Zhiqun Mao,2,* Fengwei Cui,2 Jie Fan,1 Zhouling Yuan,3 Li Tang2
1Department of Geriatric Psychiatry, The Affiliated Mental Health Center of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Department of Psychiatry, The Affiliated Mental Health Center of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 3Department of Psychiatry, Huishan No. 2 People’s Hospital, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Li Tang, Department of Psychiatry, The Affiliated Mental Health Center of Jiangnan University, 156 Qianrong Road, Wuxi, 214151, People’s Republic of China, Tel +86 510 83219318, Fax +86 510 830 12201, Email [email protected]
Background and Purpose: Subjective cognitive decline (SCD) is recognized as a preclinical indicator of Alzheimer’s disease (AD), and this stage provides a valuable time window for ultra-early intervention in AD. The aim of this study was to investigate the neurocognitive characteristics of SCD and its correlation with objective cognition, negative emotion and sleep quality in Chinese elderly.
Methods: A total of 1200 volunteers aged 60 and older underwent Brief Elderly Cognitive Screening Inventory, Quick Cognitive Screening Scale for the Elderly, Generalized Anxiety Disorder-7, Patient Health Questionnaire-9, Pittsburgh Sleep Quality Index and Core Neuropsychological Test. According to the examination results, the participants were divided into healthy control (HC) and SCD groups. The neurocognitive function of SCD and its relationship with objective cognition, negative emotion and sleep quality were analyzed.
Results: Compared with the HC group, the SCD group had similar global cognitive function but slightly impaired neurocognitive function. After adjusting for confounding factors such as age, sex, marriage, education and chronic disease, neurocognitive function (Picture-Symbol Matching: OR=0.167, 95% CI: 0.105– 0.266; Word Stem Completion: OR =0.260, 95% CI: 0.131– 0.514; Trail Making Test: OR=0.315, 95% CI: 0.178– 0.560; Picture Recall: OR =0.278, 95% CI: 0.122– 0.636), negative emotion (sub-depressive symptoms: OR=2.287, 95% CI: 1.483– 3.527; sub-anxiety symptoms: OR=1.663, 95% CI: 1.079– 2.563), and poor sleep quality (OR=2.138, 95% CI: 1.571– 2.909) were significantly correlated with the occurrence of SCD.
Conclusion: The study illustrates that SCD is closely related to objective cognition, negative emotion and sleep quality. Clinical evaluation and follow-up of SCD should fully account for these factors.
Keywords: subjective cognitive decline, cognitive function, negative emotions, sleep quality, Alzheimer′s disease
Introduction
Alzheimer′s disease (AD) is a major chronic disease threatening the health and life of the elderly. It is estimated that 50 million people are living with AD in the world at present, and the number will reach 100–130 million between 2040 and 2050, which will cause a great burden on the global society and family economy.1 As there is no effective treatment for the dementia phase of AD, emphasis on prevention, early detection and intervention remains the core principles of the disease’s management. In 2014, the conceptual diagnostic framework of subjective cognitive decline (SCD) was proposed, which push the research on the ultra-early diagnosis and intervention of AD to a new level. SCD refers to individual’s sense of self continuous decline in memory or other cognitive abilities compared to their previous normal state, but neurocognitive tests are within the normal range or extremely mild impairment, and do not meet the diagnostic criteria for mild cognitive impairment (MCI). MCI is defined as mild impairment in more than one domain of objective cognition, but the ability of daily living remains intact. SCD is prevalent in the elderly and may be the earliest warning sign of MCI or AD, which is closer to the normal and early pathological boundary of cognitive aging than MCI. Long-term observational studies have found that SCD occurs on average about 10 years before the diagnosis of dementia, and screening and intervention in the target population during this valuable time window is promising to delay or even reverse the AD process.2 Recent epidemiological data have indicated that the prevalence of SCD in the elderly is as high as 25% to 56%, and the annual conversion rate of dementia is 2.3 to 11.0%, while that of the elderly without SCD is 1.0 to 2.14%.3–5Although the risk of converting SCD to AD is more than double that of older adults without SCD, not all people with SCD will show progressive cognitive decline and progress to dementia. In recent 30 years, the prevalence and incidence of dementia in Europe and the United States have been declining through aggressive control of risk factors affecting SCD conversion.6 China has a large elderly population and is expected to have more than 40 million AD patients by 2050, which will be a serious challenge for Chinese social development.7 Learning from the concept of active prevention and treatment in European and American countries and exploring the characteristic clinical manifestations of SCD population are of great practical significance for early diagnosis and treatment of AD. Due to the high heterogeneity and low specificity of SCD, current reports on whether SCD can reflect objective cognition and its potential relationship with other diseases are inconsistent.8,9 Therefore, the research on SCD still needs to be further explored. Based on a sample of elderly in Chinese communities, this study explored the neurocognitive characteristics of SCD and examined its correlation with objective cognitive impairment, negative emotions and sleep quality, aiming to improve the awareness and assessment ability of primary doctors on SCD, so as to provide personalized medical advice and management strategies for elderly with SCD.
Materials and Methods
Subjects
A cross-sectional study was conducted in Wuxi, Jiangsu Province, China from February 2022 to August 2022. By means of stratified cluster random sampling, 6 neighborhood committees were selected as the investigation points. Using the health records of the elderly in community health service as clues, 1500 volunteers aged 60 years and older were planned to be recruited. Inclusion criteria: (1) age 60–85 years, primary school education or above, regardless of whether or not marriage; (2) having basic verbal expression and writing ability and independently complete neuropsychological tests; (3) local permanent residents, voluntarily accept the survey and signed the informed consent. Exclusion criteria: (1) any serious untreated systemic disease or unstable state of physical disease; (2) severe mental illness, severe anxiety and depression, obvious cognitive impairment; (3) head trauma, epilepsy and other neurological diseases. After initial screening, 1302 volunteers met the inclusion criteria. Structured, face-to-face clinical interviews, scale assessments, and laboratory tests were conducted for each volunteer at a community health center. This study was conducted in accordance with the declaration of Helsinki and approved by the Ethics Committee of Wuxi Mental Health Center (N0: WXMH-CIRB2021LLky001).
Procedure
Screening for Subjective Cognitive Decline
The Brief Elderly Cognitive Screening Inventory (BECSI) was used to evaluate SCD symptoms.10 It contains 14 items that assess four functional areas: subjective memory function, temporal orientation, work efficiency and mental pathological, with each item’s score may be 0, 0.5, 1 or 2. Total score of BECSI distributes from 0 to 28, with higher score representing worse SCD symptoms. The criteria for no SCD was BECSI <10, mild SCD was BECSI: 10–14, obvious SCD was BECSI≥15. BECSI has excellent reliability and validity in the previous application in Chinese old people, with the retest correlation of 0.998, α coefficient of 0.908, partial half-reliability of 0.918, correlation of 0.885 with mini-mental state examination (MMSE),11 and correlation of 0.920 with Chinese Cognitive Ability Scale (CCAS).12
Global Cognitive Evaluation
The Quick Cognitive Screening Scale for the Elderly (QCSS‐E) was used to assess global cognitive function of volunteers.13 It contains 51 items, which measure 12 cognitive domains: immediate memory, naming of objects, visuospatial ability, verbal fluency, digit span, abstract ability, auditory imitation, visual imitation, command, delayed memory, simple calculation, temporal and spatial orientation. QCSS-E showed good reliability and validity among Chinese older adults, and the test-retest reliability and Cronbach′s α coefficient were 0.972 and 0.814 for QCSS-E total score, and the correlation with MMSE is 0.886. Total score of QCSS-E ≥75 represented normal cognitive; 65–74 represented mild cognitive impairment; and < 65 represented obvious cognitive impairment. The total scores of immediate memory, digit span and delayed memory (Quick Cognitive Screening Scale for the Elderly-Memory, QCSS-E-M) indicated objective memory function, and the demarcation criteria for normal memory was QCSS-E-M ≥ 17, 13–16 for mild impairment and < 13 for obvious impairment.
Neurocognitive Assessment
Eight sub-tests, including Digit Span, Picture-Symbol Matching, Verbal Analogy, Numeral Operation, Word Stem Completion, Quick Coding, Picture Recall and Trail-Making Test, were extracted from the CCAS, Multi-dimensional Memory Assessment Scale14 and Halstead-Reitan neuropsychological battery15 to form the Core Neuropsychological Test (CNT). The original score of each sub-test was transformed into the standard score. The criteria for normal or SCD: each sub-test scores >7 or only one sub-test scores distributed 5–7; mild to moderate cognitive impairment: 2 or more sub-tests scores distributed 5–7.
Sleep Quality and Negative Emotion Assessment
Sleep quality was assessed by the Pittsburgh Sleep Quality Index (PSQI),16 which consists of 19 items with a total score of 21 and more than 7 points as poor sleep quality. Symptoms of anxiety and depression were measured by Generalized Anxiety Disorder-7 (GAD-7),17 and Patient Health Questionnaire-9 (PHQ-9),18 respectively, with a total score of 21 and 27. Higher scores indicated a higher level of anxiety or depression. Subclinical emotional problems: total score of GAD-7 or PHQ-9 distributed 5–9; obvious emotional problems: total score of GAD-7 or PHQ-9≥ 10.
Clinical Interview and Diagnostic Grouping
(1) socio-demographic data collection: name, gender, age, marriage, education, tobacco and alcohol preferences, physical condition, body mass index, family history, etc.; (2) medical history collection and examination: information related to memory and cognitive decline, psychiatric examination and physical examination, necessary auxiliary examination such as blood routine, blood glucose, blood lipid, electrocardiogram, brain computed tomography etc.; (3) cognitive assessment: all scales such as BECSI, PSQI, PHQ-9, GAD-7 and CNT were completed in community primary care clinics. Based on the interview and examination results, the participants were divided into the SCD group and the healthy control (HC) group by the clinicians. The criteria for SCD were formulated according to the concepts of the International Working Group in 2014:19 (1) a self-experienced persistent decline in cognitive capacity which was unrelated to an acute event, BECSI≥10; (2) global cognitive and objective memory function were normal, QCSS-E≥75 and QCSS-E-M≥17, each sub-test scores of CNT>7 or only one sub-test scores of CNT distributed 5–7; (3) having specific worries associated with the cognitive decline, but did not reach the level of severe anxiety and depression disorders, with GAD-7 and PHQ-9 both < 9; (4) exclusion of serious physical and mental diseases. HC criteria: (1) having no complaints of subjective cognitive decline, BECSI <10; (2) QCSS-E and QCSS-E-M normal or high score, each sub-test scores of CNT>7 or only one sub-test scores of CNT distributed 5–7; (3) exclusion of serious physical and mental diseases.
Statistical Analysis
Statistical analysis was conducted using SPSS24.0 software (IBM Corporation, Armonk, NY, USA). All normally distribution continuous variables was described by mean ± standard deviation, and skew distribution continuous variables were expressed by median and interquartile distance. Counting data were expressed in terms of frequency and percentage of ingredients. Pearson Chi-square test was used for finding differences between groups for categorical variables, and independent sample t-test or non-parametric test was used for continuous variables. Hierarchical regression model was used to investigate the effects of objective cognition, negative emotion and sleep quality on the occurrence of SCD. The level of significance was set at P< 0.05.
Results
Sample Characteristics
Among 1302 volunteers, 1110 valid samples were obtained according to SCD and HC criteria, and their main characteristics were shown in Table 1. They ranged in age from 60 to 85 years, with mean age 72.13 years (SD 6.38 years). There were 567 males and 533 females, including 622 elderly with healthy cognition (HC group) and 478 elderly patients with SCD (SCD group). All participants completed clinical interview, cognitive assessment and laboratory examination. There were no statistically significant differences among groups in marriage, smoking, drinking, body mass index (BMI), QCSS-E and QCSS-E-M, while there were statistically significant differences among groups in gender, age, education, hypertension or diabetes, BECSI, PSQI, PHQ-9 and GAD-7.
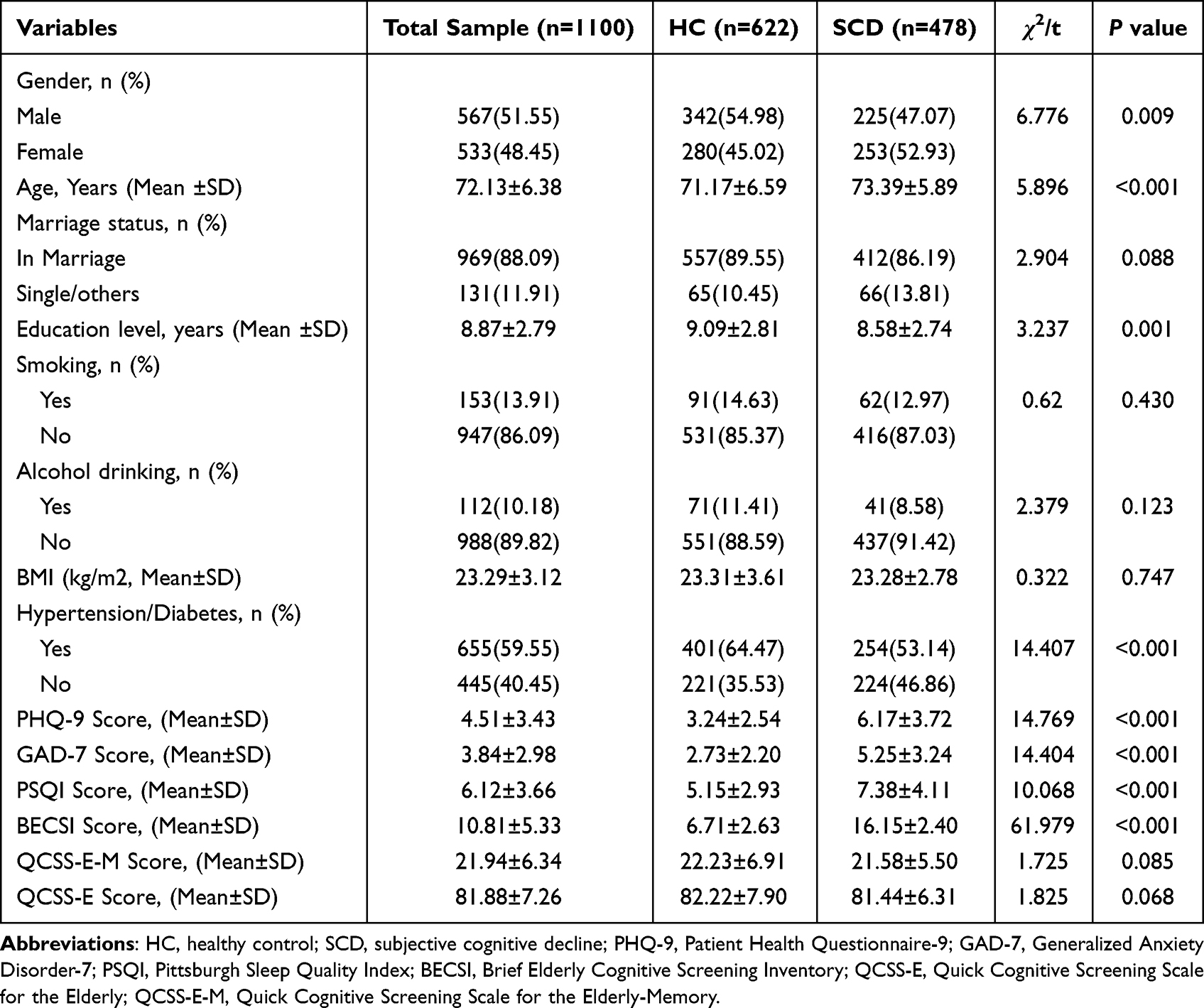 |
Table 1 Comparison of Demographic Characteristics and Clinical Data Between the Two Groups |
Comparison of Neurocognitive Function Between the Two Groups
All Participants scores on the Digit Span, Verbal Analogy and Numeral Operation of the CNT were all more than 7 points. A total of 292 participants scores on the Picture-Symbol Matching, Word Stem Completion, Quick Coding, Picture Recall, Trail-Making Test of the CNT were ranged from 5 to 7 points, including 98 cases in the HC group and 194 cases in the SCD group, with statistically significant differences (χ2=12.262, P<0.001), as shown in Table 2. Comparison of sub-test scores between the two groups showed that the scores of Picture-Symbol Matching, Word Stem Completion and Trail-Making Test in the SCD group were lower than those in the NC group, and the differences were statistically significant, while the differences of Digit Span, Verbal Analogy, Numeral Operation, Quick Coding and Picture Recall were not statistically significant, as shown in Figure 1.
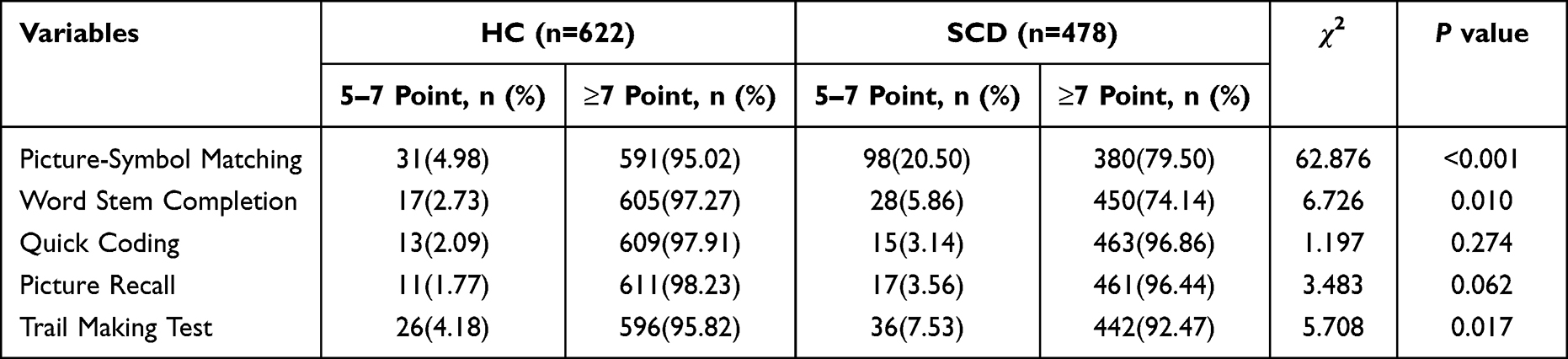 |
Table 2 The Distribution Characteristics of CNT Scores in Each Sub-Test of Two Groups |
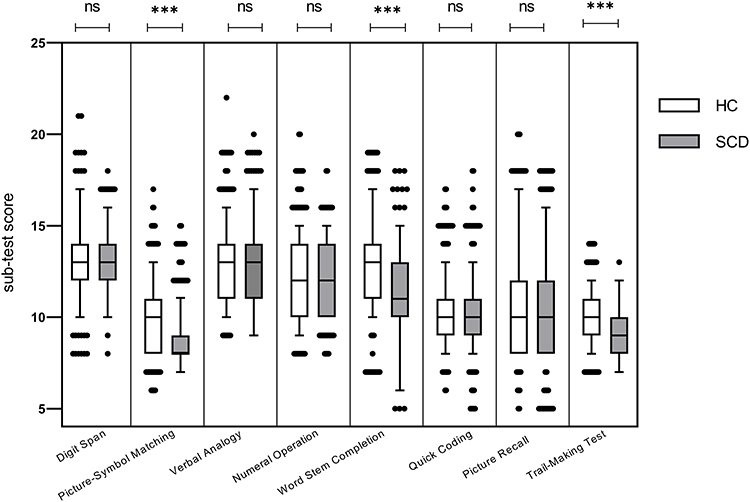 |
Figure 1 Comparison of CNT test scores between the two groups ns P>0.05; ***P<0.001. |
Correlation Between SCD and Objective Cognition, Negative Emotion and Sleep Quality
With SCD as the dependent variable (yes=1, no=0) and gender, age, education level, marriage, hypertension or diabetes, negative emotion, sleep quality, Picture-Symbol Matching, Word Stem Completion, Trail Making Test, Picture Recall and Quick Coding were taken as independent variables for binary Logistic regression model analysis (stratified). The goodness-of-fit measurement results showed that the explanation degree of model 1 to Model 4 gradually increased, and the increasing trend of Cox & Snell R2 showed that negative emotion had the greatest impact on SCD, followed by objective cognition, and sleep quality also had a certain impact on SCD. In addition, advanced age, high blood pressure or diabetes were significantly associated with SCD, as shown in Table 3.
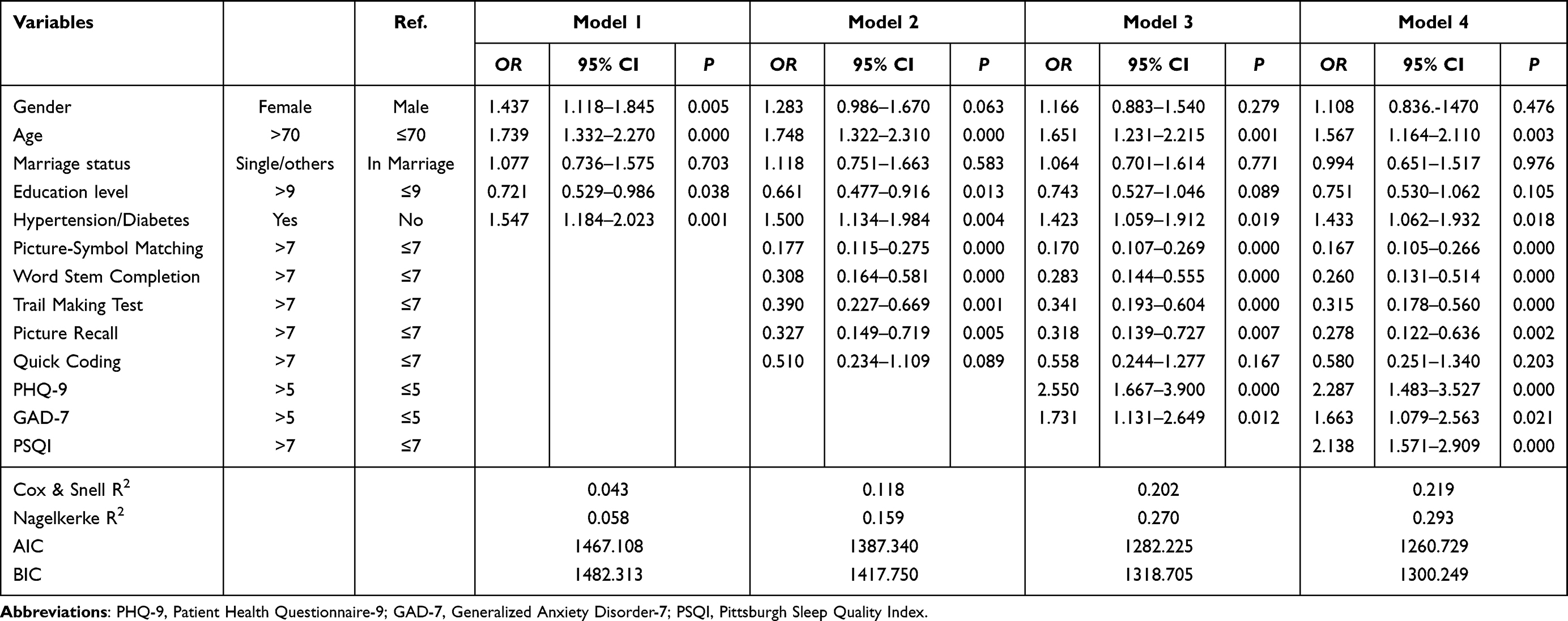 |
Table 3 Logistic Regression Model of Factors Influencing SCD Among Community Older Adults |
Discussion
The association between SCD and objective cognition is complex, which is easily affected by negative emotions, sleep disorders and other chronic diseases. Accurate identification of this relationship might be of great significance for rational choice of treatment and prognosis assessment in individual with SCD. At present, there are relatively few studies about the characteristics and correlates of SCD in Chinese community elderly, and clinicians have insufficient understanding of the conceptual framework of SCD. We surveyed 1110 volunteers aged 60 and older who lived in the community, and found that the prevalence rate of SCD among the elderly in the Chinese community was 43.06%, which was at a high level. In the SCD group, the proportion of women, low years of education, old age, hypertension or diabetes, subclinical anxiety and depression and sleep problems was higher than that in the healthy control. These results objectively reflect that SCD has similar demographic characteristics to AD, which is an important clue for the early community screening of AD. Studies have confirmed that excessive alcohol consumption and smoking in later life are lifestyle risks for dementia.20 However, our results showed similar rates of smoking and drinking between the two groups, which may be related to the fact that we did not stratified smoking and drinking by frequency and duration. Similarly, a community survey of a large elderly population by Park et al21 also showed no difference in smoking and alcohol drinking rates between SMC patients and normal elderly. In the present study, we found that advanced age, hypertension, and diabetes were independent risk factors for SCD, while gender, marriage, and education were not strongly associated with SCD after controlling for confounding factors. These are similar and different from previous literature reports. Previous studies have reported that female, old age, low education, hypertension and diabetes may be risk factors for SCD.22–24 Cosentino et al24 believed that SCD may reflect a wider range of physical health conditions, independent of education, and that other experiences in middle and old age have more influence on cognitive changes in the elderly than normal education.
Most studies consider SCD to have slight cognitive impairment, with the most common areas of cognitive impairment being episodic memory, language, or executive function. However, due to the compensatory effect of cognitive reserve, it is difficult to detect at the individual level and needs to be captured by sensitive and complex neuropsychological tests above the population level.25,26 The results of this study showed that objective memory and global cognition of patients with SCD were in the normal range, but the passing rate of low scores in complex neurocognitive tests such as Picture-Symbol Matching, Word Stem Completion and Trail-Making Test was significantly higher than that of normal elderly people, reflecting that SCD patients had slight impairment in learning ability, information processing and executive function. Research has found that a certain cognitive function is performed jointly by multiple brain structures, and each cognitive subcomponent may have many related connections in the brain neural network, such as the nodes of executive function are in the lateral prefrontal cortex and parietal cortex, the nodes of learning ability in the hippocampal entorhinal region, and the information processing nodes involving the temporal lobe, parietal lobe, prefrontal lobe and limbic system.27 A growing body of neuroimaging studies have found that patients with SCD present with hippocampal and entorhinal cortex atrophy and reduced frontoparietal and parahippocampal gray matter density, with a severity between MCI and healthy individuals.28,29 These results suggest that SCD may be a risk factor of objective cognitive impairment and can predict early diagnosis of AD.
Multivariate logistic regression analysis showed that negative emotion, objective cognition and sleep disturbance were significantly correlated with the occurrence of SCD, and the influence of negative emotion on SCD was slightly higher than that of objective cognitive function on SCD. According to the conceptual framework of SCD research, after excluding severe anxiety and depression, we found that sub-anxiety and depression remained risk factor for SCD (OR=1.663, 95% CI: 1.079–2.563; OR=2.287, 95% CI: 1.483–3.527).
Negative emotion is a common psychological problem in the elderly. A systematic review of SCD and affective symptoms has shown that, at any cross-section, SCD is associated with affective symptoms in older adults, and affective symptoms may be concomitant with SCD or may occur concurrently with SCD due to common underlying causes.30,31 Self-health management intervention could alleviate or eliminate negative emotions in patients with SCD and improve executive function.32
We found that, even after controlling for confounding factors such as socio-demographic factors, negative emotions, and sleep quality, SCD were strongly associated with several objective cognitive subdomains, including Picture-Symbol Matching (OR=0.167, 95% CI: 0.105–0.266), Word Stem Completion (OR=0.260, 95% CI: 0.131–0.514), Trail-Making Test (OR=0.315, 95% CI: 0.178–0.560) and Picture Recall (OR=0.278, 95% CI: 0.122–0.636). These subtests reflect associative learning ability, information processing speed, executive function and delayed memory, respectively. Multiple studies have found that the gray matter density of temporal and frontoparietal lobes in patients with SCD decreases, showing the same atrophy trend as in AD.33,34 As the compensatory effect of cognitive reserve at this stage is sufficient to counterbalance the pathological damage caused by AD, the explicit objective cognitive function test and subjective cognitive perception of patients with SCD are inconsistent. This study also found that among the four cognitive dimensions, executive function has the most significant influence on SCD. Some researchers suggested that,35,36 compared with memory complaints, the executive function changes of SCD seem to be more specific to show the precursor symptoms of AD, and the mechanism may be related to the early pathophysiological changes of the frontal lobe of the brain prior to the atrophy of the hippocampus. Although some studies have shown that the risk of cognitive decline is higher in SCD patients from memory clinics than SCD-community,37,38 in view of the low rate of active consultation with SCD in China, it is very necessary to carry out community-based screening and standardized management of SCD in the elderly population.
Changes in sleep-wake rhythms increase the risk of cognitive impairment in older adults. During sleep, the glymphatic system clears Aβ twice as fast as when awake. Fragmentation or deprivation sleep can interfere with the clearance of toxic substances in the cerebrospinal fluid, resulting in the accumulation of Aβ, which impairs cognitive function.39 Tsapanou et al40,41 pointed out that at any objective cognitive level, sleep disorders are accompanied by subjective cognitive disorders. This study further confirmed the association between sleep disturbances and SCD occurrence (OR=2.138, 95% CI: 1.571–2.909), which was consistent with the results of Stocker et al.42 Sleep is a modifiable factor, so while focusing on subjective complaints, clinicians should not ignore potential sleep problems in patients.
Conclusion
The results of this study suggest that community SCD patients have slight neurocognitive impairment, and the incidence of subjective cognitive decline is significantly related to objective cognitive function, negative emotions, and sleep disorders. This study is a cross-sectional comparative study and has some limitations. First, information about sleep quality was from participant self-reported, rather than obtaining from objective methods such as polysomnography. Secondly, our study found that SCD was associated with objective cognition, negative emotions and sleep quality, but it could not explain the causal relationship between them. At the same time, there may be other potential factors affecting their relationship, such as AD risk genes and personality traits. Despite the above limitations, this study can indeed provide clinical guidance for primary medical staff to correctly identify SCD and timely adopt targeted intervention measures. In future studies, we will follow up two groups of elderly volunteers to further explore the value of SCD in predicting AD progression.
Acknowledgments
The authors thank the participating volunteers. This study was supported by Scientific and technological achievements of Wuxi Municipal Health Commission and appropriate technology extension projects (T202023).
Author Contributions
All authors made a significant contributions to the work reported, whether that in study design, execution, data acquisition and analysis, or in all of these areas; participated in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to take responsibility for all aspects of the work.
Disclosure
The authors declare no conflicts of interest.
References
1. Thakral S, Yadav A, Singh V, et al. Alzheimer’s disease: molecular aspects and treatment opportunities using herbal drugs. Ageing Res Rev. 2023;88:101960. doi:10.1016/j.arr.2023.101960
2. Verlinden VJA, van der Geest JN, de Bruijn R, Hofman A, Koudstaal PJ, Ikram MA. Trajectories of decline in cognition and daily functioning in preclinical dementia. Alzheimers Dement. 2016;12(2):144–153. doi:10.1016/j.jalz.2015.08.001
3. Fernandez-Blazquez MA, Avila-Villanueva M, Maestu F, Medina M. Specific features of subjective cognitive decline predict faster conversion to mild cognitive impairment. J Alzheimers Dis. 2016;52(1):271–281. doi:10.3233/JAD-150956
4. Luck T, Luppa M, Matschinger H, Jessen F, Angermeyer MC, Riedel-Heller SG. Incident subjective memory complaints and the risk of subsequent dementia. Acta Psychiatr Scand. 2015;131(4):290–296. doi:10.1111/acps.12328
5. Mitchell AJ, Beaumont H, Ferguson D, Yadegarfar M, Stubbs B. Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: meta-analysis. Acta Psychiatr Scand. 2014;130(6):439–451. doi:10.1111/acps.12336
6. de Bruijn RF, Bos MJ, Portegies ML, et al. The potential for prevention of dementia across two decades: the prospective, population-based Rotterdam Study. BMC Med. 2015;13(1):132. doi:10.1186/s12916-015-0377-5
7. Liu XW, Zhao XF, Cheng ZH. The concept change, prevalence and advance in diagnosis and treatment of Alzheimer′s disease. Chin Mental Health J. 2021;29(6):1251–1265. doi:10.16128/j.cnki.1005-3611.2021.06.026
8. Zlatar ZZ, Muniz MC, Espinoza SG, et al. Subjective cognitive decline, objective cognition, and depression in older Hispanics screened for memory impairment. J Alzheimers Dis. 2018;63(3):949–956. doi:10.3233/JAD-170865
9. Zlatar ZZ, Muniz M, Galasko D, Salmon DP. Subjective cognitive decline correlates with depression symptoms and not with concurrent objective cognition in a clinic-based sample of older adults. J Gerontol B Psychol Sci Soc Sci. 2018;73(7):1198–1202. doi:10.1093/geronb/gbw207
10. Wu Y, Xu WW, Cheng ZH, Wu B, Tang L, Zhou XQ. Brief elderly cognitive screening inventory: development, reliability and validity. Chin J Geront. 2016;36(5):1211–1213.
11. Folstein MF, Robins LN, Helzer JE. The mini-mental state examination. Arch Gen Psychiatry. 1983;40(7):812. doi:10.1001/archpsyc.1983.01790060110016
12. Cheng ZH, Sun JR, Yang BX, Jiang XJ, Zhou XQ, Li L. Reliability and validity of Chinese Cognitive Ability Scale. Chin Mental Health J. 2007;21(2):103–106.
13. Wu Y, Jiang Y, Tang L, Gu J, Liu XW, Cheng ZH. Performance analysis of Quick Cognitive Screening Scale in screening early Alzheimer disease from community population. Chin Mental Health J. 2020;34(2):106–111.
14. Cheng ZH, Li HH, Zheng H. Reliability and validity of Multiple Memory Assessment Scale. Chin Mental Health J. 2002;16(4):237–241.
15. Zhao QH, Guo QH, Li F, Zhou Y, Wang B, Hong Z. The shape trail test: application of a new variant of the Trail Making Test. PLoS One. 2013;8(2):e57333. doi:10.1371/journal.pone.0057333
16. Mollayeva T, Thurairajah P, Burton K, Mollayeva S, Shapiro CM, Colantonio A. The Pittsburgh Sleep Quality Index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. 2016;25:52–73. doi:10.1016/j.smrv.2015.01.009
17. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
18. Manea L, Gilbody S, McMillan D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen Hosp Psychiatry. 2015;37(1):67–75. doi:10.1016/j.genhosppsych.2014.09.009
19. Jessen F, Amariglio RE, Buckley RF, et al. The characterisation of subjective cognitive decline. Lancet Neurol. 2020;19(3):271–278. doi:10.1016/S1474-4422(19)30368-0
20. Livingston G, Huntley J, Sommerlad A, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet. 2020;396(10248):413–446. doi:10.1016/S0140-6736(20)30367-6
21. Park MH, Min JY, Min HY, Lee HJ, Lee DH, Song MS. Subjective memory complaints and clinical characteristics in elderly Koreans: a questionnaire survey. Int J Nurs Stud. 2007;44(8):1400–1405. doi:10.1016/j.ijnurstu.2006.06.001
22. Lin LH, Wang SB, Xu WQ, et al. Subjective cognitive decline symptoms and its association with socio-demographic characteristics and common chronic diseases in the southern Chinese older adults. BMC Public Health. 2022;22(1):127. doi:10.1186/s12889-022-12522-4
23. Giacomucci G, Mazzeo S, Padiglioni S, et al. Gender differences in cognitive reserve: implication for subjective cognitive decline in women. Neurol Sci. 2022;43(4):2499–2508. doi:10.1007/s10072-021-05644-x
24. Cosentino S, Devanand D, Gurland B. A link between subjective perceptions of memory and physical function: implications for subjective cognitive decline. J Alzheimers Dis. 2018;61(4):1387–1398. doi:10.3233/JAD-170495
25. Fonseca JA, Ducksbury R, Rodda J, et al. Factors that predict cognitive decline in patients with subjective cognitive impairment. Int Psychogeriatr. 2015;27(10):1671–1677. doi:10.1017/S1041610215000356
26. Kielb S, Rogalski E, Weintraub S, Rademaker A. Objective features of subjective cognitive decline in a United States national database. Alzheimers Dement. 2017;13(12):1337–1344. doi:10.1016/j.jalz.2017.04.008
27. Banich MT, Compton RJ. Cognitive Neuroscience.
28. Hong YJ, Yoon B, Shim YS, Ahn KJ, Yang DW, Lee JH. Gray and white matter degenerations in subjective memory impairment: comparisons with normal controls and mild cognitive impairment. J Korean Med Sci Dement. 2015;30(11):1652–1658. doi:10.3346/jkms.2015.30.11.1652
29. Meibrerth D, Scheef L, Wolfsgruber S, et al. Cortical thinning in individuals with subjective memory impairment. J Alzheimers Dis. 2015;45(1):139–146. doi:10.3233/JAD-142322
30. Sabatini S, Woods RT, Ukoumunne OC, Ballard C, Collins R, Clare L. Associations of subjective cognitive and memory decline with depression, anxiety, and two-year change in objectively-assessed global cognition and memory. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2022;29(5):840–866. doi:10.1080/13825585.2021.1923634
31. Kuhn E, Moulinet I, Perrotin A, et al. Cross-sectional and longitudinal characterization of SCD patients recruited from the community versus from a memory clinic: subjective cognitive decline, psychoaffective factors, cognitive performances, and atrophy progression over time. Alzheimers Res Ther. 2019;11(1):61. doi:10.1186/s13195-019-0514-z
32. Whitfield T, Demnitz-King H, Schlosser M, et al. Effects of a mindfulness-based versus a health self-management intervention on objective cognitive performance in older adults with subjective cognitive decline (SCD): a secondary analysis of the SCD-Well randomized controlled trial. Alzheimers Res Ther. 2022;14(1):125. doi:10.1186/s13195-022-01057-w
33. Sun Y, Yang FC, Lin CP, Han Y. Biochemical and neuroimaging studies in subjective cognitive decline: progress and perspectives. CNS Neurosci Ther. 2015;21(10):768–775. doi:10.1111/cns.12395
34. Perrotin A, de Flores R, Lamberton F, et al. Hippocampal subfield volumetry and 3D surface mapping in subjective cognitive decline. J Alzheimers Dis. 2015;48(Suppl 1):S141–S150. doi:10.3233/JAD-150087
35. Valech N, Tort-Merino A, Coll-Padros N, et al. Executive and language subjective cognitive decline complaints discriminate preclinical Alzheimer’s disease from normal aging. J Alzheimers Dis. 2018;61(2):689–703. doi:10.3233/JAD-170627
36. Harrington MG, Chiang J, Pogoda JM, et al. Executive function changes before memory in preclinical Alzheimer’s pathology: a prospective, cross-sectional, case control study. PLoS One. 2013;8(11):e79378. doi:10.1371/journal.pone.0079378
37. Slot RER, Sikkes SAM, Berkhof J, et al. Subjective cognitive decline and rates of incident Alzheimer’s disease and non-Alzheimer’s disease dementia. Alzheimers Dement. 2019;15(3):465–476. doi:10.1016/j.jalz.2018.10.003
38. Snitz BE, Wang T, Cloonan YK, et al. Risk of progression from subjective cognitive decline to mild cognitive impairment: the role of study setting. Alzheimers Dement. 2018;14(6):734–742. doi:10.1016/j.jalz.2017.12.003
39. Ettore E, Bakardjian H, Sole M, et al. Relationships between objectives sleep parameters and brain amyloid load in subjects at risk for Alzheimer’s disease: the INSIGHT-preAD Study. Sleep. 2019;42(9):zsz137. doi:10.1093/sleep/zsz137
40. Tsapanou A, Gu Y, O’Shea DM, et al. Dataset on the associations between sleep quality/duration and cognitive performance in cognitively healthy older adults. Data Brief. 2017;14:720–723. doi:10.1016/j.dib.2017.08.028
41. Tsapanou A, Vlachos GS, Cosentino S, et al. Sleep and subjective cognitive decline in cognitively healthy elderly: results from two cohorts. J Sleep Res. 2019;28(5):e12759. doi:10.1111/jsr.12759
42. Stocker RPJ, Khan H, Henry L, Germain A. Effects of sleep loss on subjective complaints and objective neurocognitive performance as measured by the immediate post-concussion assessment and cognitive testing. Arch Clin Neuropsychol. 2017;32(3):349–368. doi:10.1093/arclin/acx003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Impact of Anesthetic Management Under Bispectral Index Monitoring on the Early Recovery Quality of Elderly Patients Undergoing Laparoscopic Surgery: A Blinded Randomized Controlled Trial
Shi M, Long Y, Zhou Z, Huang L, Wu D, Zhang X
Clinical Interventions in Aging 2025, 20:597-612
Published Date: 14 May 2025
Central Sensitization Severity in Chronic Low Back Pain: Associations with Sleep, Distress, Cortisol, and Visuospatial Working Memory
Sahebalam M, Hatef B, Pirzad Jahromi G
Journal of Pain Research 2026, 19:583843
Published Date: 13 February 2026
Association Between Sleep Quality and Cognitive Function in Patients with Hypertension in Rural Areas of Shanxi Province, China: The Chain Mediating Role of Anxiety and Depression
Li S, Liang R, Liu J, Sun W, Wang J, Li S, Zhao S, Niu Q, Yu H, Zhang H, Qin X, Bai R, Li Y
Psychology Research and Behavior Management 2026, 19:593258
Published Date: 7 April 2026
A Perioperative Care Strategy for Prevention of Postoperative Delirium in Elderly Patients with Gastrointestinal Tumors: A Clinical Observational Study
Xie C, Yang X
Journal of Multidisciplinary Healthcare 2026, 19:581689
Published Date: 8 April 2026
Associations of Sleep Quality with Cognitive Function in Chinese Older Adults: The Roles of Self-Efficacy and Depressive Symptoms
Wang L, Wang Y, Huo J, Luo Y, Ding Y, Wang Z
Clinical Interventions in Aging 2026, 21:594997
Published Date: 20 May 2026