Back to Journals » Journal of Pain Research » Volume 19
Buccal Acupuncture for Early Postoperative Catheter-Related Bladder Discomfort Following Ureteroscopic Lithotripsy: A Randomized, Sham-Controlled Trial
Authors Wu H ![]() , Wang D
, Wang D ![]() , Chen C, Shi Y
, Chen C, Shi Y ![]() , Zhang F, Zhou Z
, Zhang F, Zhou Z ![]() , Shi M
, Shi M ![]() , Mo S, Li H, Zhang X
, Mo S, Li H, Zhang X ![]()
Received 14 April 2026
Accepted for publication 5 June 2026
Published 9 June 2026 Volume 2026:19 616996
DOI https://doi.org/10.2147/JPR.S616996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Huizhen Wu,1,2,* Dong Wang,1,* Chaojin Chen,3 Yi Shi,1 Fangyi Zhang,1 Zhihu Zhou,2 Min Shi,2 Shan Mo,1 Hong Li,1 Xu Zhang2
1Department of Anesthesiology, No. 924 Hospital of PLA Joint Logistic Support Force, Guilin, Guangxi, People’s Republic of China; 2Department of Anesthesiology, The Second Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, People’s Republic of China; 3Department of Anesthesiology, The Third Affiliated Hospital of Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Li, Department of Anesthesiology, No. 924 Hospital of PLA Joint Logistic Support Force, Guilin, Guangxi, People’s Republic of China, Email [email protected] Xu Zhang, Department of Anesthesiology, The Second Affiliated Hospital of Guilin Medical University, Guilin, Guangxi, People’s Republic of China, Email [email protected]
Purpose: To evaluate whether buccal acupuncture (BA), a minimally invasive facial acupuncture technique, reduces early postoperative catheter-related bladder discomfort (CRBD) after ureteroscopic lithotripsy (URSL).
Patients and Methods: In this single-center, participant- and assessor-blinded, sham-controlled randomized trial, 118 patients undergoing URSL were randomized 1:1 to the BA group (n = 59) or sham group (n = 59). Baseline CRBD was assessed at extubation, followed by a 30-min PACU intervention. The BA group received needle insertion through guide tubes at bilateral Lower Jiao, Lumbar, and Sacral points; the sham group received identical guide-tube contact without needle penetration. The primary endpoint was moderate-to-severe CRBD (score ≥ 2) at 1 h after extubation. Secondary endpoints included CRBD at 2, 6, and 24 h, visual analog scale (VAS) pain, rescue medication use, Quality of Recovery-15 (QoR-15) and Richards-Campbell Sleep Questionnaire (RCSQ) scores on POD 1 and 2, adverse events, and participant blinding.
Results: Moderate-to-severe CRBD at 1 h occurred less frequently in the BA group than in the sham group (13.6% vs. 40.7%; RR 0.33, 95% CI 0.16– 0.68; P = 0.002; NNT = 4, 95% CI 3– 9). This difference persisted at 2 h (6.8% vs. 25.4%; P = 0.012; NNT = 6, 95% CI 4– 18), but not at 6 or 24 h. Fewer BA-group patients required rescue medication. VAS pain and RCSQ scores were comparable between groups. QoR-15 scores on POD 1 were higher in the BA group, although the difference did not reach the minimal clinically important difference. Minor insertion-site bleeding was the only BA-related adverse event, and participant blinding remained acceptable.
Conclusion: BA reduced early postoperative moderate-to-severe CRBD and rescue medication use after URSL. BA may be a safe, non-pharmacological adjunct for acute postoperative CRBD management.
Keywords: Buccal acupuncture, Catheter-related bladder discomfort, ureteroscopic lithotripsy, randomized controlled trial, Sham acupuncture, postoperative recovery
Introduction
Catheter-related bladder discomfort (CRBD) is a common and distressing complication following urological surgery. Among surgical patients requiring postoperative urinary catheterization, the reported incidence of CRBD ranges from 47% to 90%.1,2 In patients undergoing ureteroscopic lithotripsy (URSL), this incidence reaches up to 60%.3 This high incidence may be related to direct trigonal stimulation by the catheter and surgical trauma to the bladder and ureteral mucosa. The indwelling catheter balloon continuously compresses and irritates the sensitive bladder trigone and neck. This mechanical trauma disrupts the urothelium, releasing inflammatory mediators, including prostaglandins, substance P, and histamine. These mediators sensitize peripheral C and A-δ afferent nerve fibers, initiating a parasympathetic reflex. This reflex rapidly overactivates muscarinic receptors (primarily the M2 and M3 subtypes), which forces the detrusor muscle into spasmodic contractions. Patients experience these involuntary spasms as severe suprapubic burning and urinary urgency.4–6 If uncontrolled during emergence from general anesthesia, CRBD precipitates adverse clinical events. In the post-anesthesia care unit (PACU), uncontrolled CRBD acts as a primary trigger for emergence agitation, hypertensive crises, tachycardia, and postoperative delirium. Consequently, CRBD is not merely a transient discomfort, but a clinical risk factor that compromises perioperative safety.
Current management of CRBD relies heavily on pharmacological strategies, such as antimuscarinics, opioids, and adjunctive analgesics. Although these pharmacological treatments can alleviate CRBD, they may also cause adverse effects such as xerostomia, blurred vision, sedation, and hemodynamic instability.7,8 In the PACU, these side effects are particularly problematic, as excessive sedation can obscure consciousness assessments and delay discharge readiness. Consequently, there is a clear clinical need for fast-acting, non-pharmacological interventions. Several acupuncture-related non-pharmacological interventions have been investigated for CRBD management. Transcutaneous electrical acupoint stimulation (TEAS),9 wrist-ankle acupuncture,10 and acupoint injection11 have been reported to reduce the incidence or severity of CRBD, or to relieve CRBD symptoms in postoperative patients. However, these modalities generally require stimulation or injection at somatic acupoints on the lower abdomen, sacral region, or limbs, which can be challenging to implement in the restricted PACU environment without disrupting patient positioning, surgical dressings, urinary catheters, or standard monitoring.
An ideal early postoperative intervention must be minimally invasive, easy to administer, and feasible without disrupting the surgical site, urinary catheter, or patient positioning. Buccal acupuncture (BA) may be a promising alternative. It is quick, minimally invasive, and requires no patient movement. As an emerging micro-needling technique, BA is based on biological holography and Traditional Chinese Medicine (TCM) Da San Jiao theory, in which facial points are mapped to specific body regions.12 In this framework, the buccal Lower Jiao point corresponds to the bladder, whereas the Lumbar and Sacral points are considered to correspond to the lumbosacral region and sacral nerves involved in pelvic organ regulation.
Beyond this traditional theoretical framework, a plausible neurophysiological rationale may also support the use of buccal stimulation for CRBD. The buccal and facial regions are richly innervated by branches of the trigeminal nerve, particularly the maxillary and mandibular divisions. Craniofacial acupuncture stimulation may activate trigeminal sensory afferents and influence central nervous system function through peripheral nerve stimulation pathways.13,14 Recent electrophysiological evidence also suggests that cheek acupuncture can induce immediate changes in brain oscillations and functional connectivity related to pain processing.15 More broadly, acupuncture analgesia may involve activation of peripheral afferent fibers, including myelinated Aδ fibers and unmyelinated C fibers, engagement of descending inhibitory pathways, and somato-autonomic reflex modulation.16 Importantly, lower urinary tract function is regulated by a brain–spinal–peripheral neural network, including the periaqueductal gray, pontine micturition center, and sacral spinal cord, which integrates bladder afferent signals and coordinates detrusor activity.17,18 Therefore, we hypothesized that BA may engage central pain-modulatory and autonomic regulatory pathways through trigeminal sensory afferent activation, may secondarily influence bladder reflex activity and thereby attenuate catheter-induced visceral discomfort. Nevertheless, this proposed trigeminal–central modulation–sacral parasympathetic pathway remains hypothetical, and the present trial was designed to evaluate the clinical efficacy and safety of BA rather than to directly test this neurophysiological mechanism. Furthermore, BA uses fine filiform needles inserted through guide tubes and generally does not require strong needling sensation, which may make it suitable for early postoperative application in the PACU.
Previous studies have successfully utilized BA to manage general perioperative pain and discomfort, highlighting its safety and lack of pharmacological side effects.19–21 To address this knowledge gap, we designed a prospective randomized trial to determine whether BA effectively reduces the incidence of moderate-to-severe CRBD during the early postoperative period in patients undergoing URSL.
Materials and Methods
This study was designed as a randomized, participant- and assessor-blinded, sham-controlled clinical trial. It was approved by the Ethics Committee of the No. 924 Hospital of PLA Joint Logistic Support Force (Approval: Gui Medicine [2024] No. 77) and was registered with the International Traditional Medicine Clinical Trial Registry (Clinical trial number: ITMCTR2024000302; principal investigator: Dong Wang; date of registration: August 26, 2024). The study was conducted in accordance with the Declaration of Helsinki and reported in compliance with the Consolidated Standards of Reporting Trials (CONSORT) and the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA).
Study Population
We screened adult patients scheduled for URSL at the No. 924 Hospital of PLA Joint Logistic Support Force, a tertiary Grade A hospital in Guilin, China, between January and March 2025. During preoperative screening, a designated investigator explained the study purpose, procedures, potential benefits, and possible risks to potentially eligible patients, answered their questions, and obtained written informed consent before enrollment and randomization. Only patients who voluntarily agreed to participate and provided written informed consent were enrolled. The interventions were performed in the Department of Anesthesiology and the PACU. Inclusion criteria were age ≥18 years, American Society of Anesthesiologists (ASA) physical status I–III, and planned postoperative indwelling urinary catheterization. Exclusion criteria included preoperative neurogenic bladder; severe hepatic or renal dysfunction; allergy to routine anesthetics; concurrent participation in another clinical trial; skin lesions, scars, or parotitis at the intended buccal intervention sites; and cognitive or neuropsychiatric conditions precluding reliable symptom reporting. The study protocol prespecified criteria for discontinuing the intervention, including the development of emergence delirium, inability to communicate after PACU recovery, or unplanned intensive care unit (ICU) admission. However, in accordance with the intention-to-treat (ITT) principle, all randomized patients were to be strictly retained in the final analysis regardless of whether they completed the assigned intervention.
Randomization, Concealment, and Blinding
A designated clinical investigator screened and enrolled the participants. Eligible participants were randomly assigned (1:1) to the BA or sham group using a computer-generated random sequence with permuted blocks of sizes 4 and 6. An independent investigator, who was uninvolved in patient enrollment, intervention delivery, or outcome assessment, generated and maintained this sequence. Allocation was concealed using sequentially numbered, opaque, sealed envelopes. This same investigator prepared pre-numbered, visually identical intervention kits containing sterile guide-tube needle assemblies for both groups. In the BA group, the needle handle was released and the needle was inserted through the guide tube; in the sham group, the same guide-tube needle assembly was used, but the needle handle remained locked and was not released or advanced. Following enrollment, an independent researcher assigned the interventions by opening the sealed opaque envelopes. General anesthesia was administered by an anesthesiologist blinded to group allocation. To maintain participant blinding, both interventions used visually similar guide-tube needle assemblies and the same buccal acupoint sequence. Preoperatively, participants were informed that BA typically causes minimal needling sensation and that the most noticeable procedural sensation would be the transient pressure of the guide tube during point localization. During the procedure, participants in both groups were instructed to rest in a supine position with their eyes closed. At the conclusion of the 30-min study period, the acupuncturist gently compressed the corresponding points in both groups with a cotton swab to standardize the end-of-procedure tactile experience.
The intervention was delivered by a licensed acupuncturist with over five years of clinical experience in buccal acupuncture, who had undergone specialized professional training and held a certified qualification in the technique. Due to the nature of the procedure, the acupuncturist could not be blinded. However, all outcomes were evaluated by an independent, blinded assessor. Finally, participant blinding success was evaluated upon transfer from the PACU to the ward by asking participants to guess their group assignment.
Anesthesia and Monitoring
Routine monitoring was initiated upon operating room arrival. General anesthesia was induced with intravenous midazolam (0.03 mg·kg−1), etomidate (0.3 mg·kg−1), sufentanil (0.4 μg·kg−1), and cisatracurium (0.2 mg·kg−1). Maintenance was achieved with propofol (5 mg·kg−1·h−1), remifentanil (0.2 μg·kg−1·min−1), and dexmedetomidine (0.3 μg·kg−1·h−1), keeping the Bispectral Index (BIS) between 40 and 60 and hemodynamics within clinically acceptable ranges. Approximately 10 min before surgery completion, intravenous sufentanil (0.1 μg·kg−1) was administered for postoperative analgesia alongside tropisetron (5 mg) for antiemetic prophylaxis. At the end of surgery, a Double-J ureteral stent and a urinary catheter were placed, with the balloon inflated using 10 mL of distilled water. Patients were transferred to the PACU and extubated upon meeting standard criteria.
Buccal Acupuncture and Sham Procedures
Following a standardized protocol,12 three bilateral buccal acupoints were selected on each side: Lower Jiao, Lumbar, and Sacral (Figure 1A and B), totaling six intervention sites per participant. The Lower Jiao point is located at the anterior margin of the mandibular angle, the Sacral point 0.5 cun anterior and superior to the mandibular angle, and the Lumbar point at the midpoint between the Dorsal and Sacral points. The Dorsal point, serving as a reference landmark, is located in the depression along the lower border of the root of the zygomatic arch (corresponding to the temporomandibular joint).
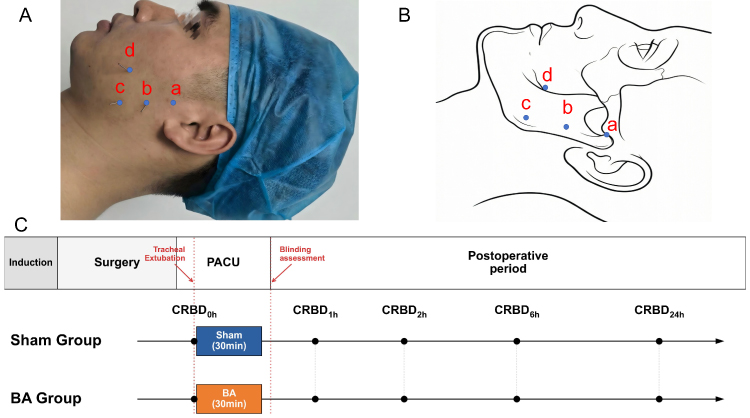 |
Figure 1 Buccal acupuncture points and study timeline. Abbreviations: CRBD, catheter-related bladder discomfort; PACU, post-anesthesia care unit. Notes: (A) shows the locations of facial landmarks and buccal acupuncture points in a participant. (B) shows the corresponding schematic diagram. a, Dorsal point; b, Lumbar point; c, Sacral point; d, Lower Jiao point. The Dorsal point served only as a reference landmark. (C) summarizes the postoperative study timeline: extubation, baseline CRBD assessment at 0 h, a 30-min study period in the PACU, transfer to the ward with participant blinding assessment, and subsequent follow-up assessments. Written informed consent was obtained from the individual shown in Panel A for publication of this image. |
In the BA group, each acupoint was localized and then needled sequentially, one site at a time, with a sterile filiform needle (0.16 mm [diameter] × 15 mm [length], Maanshan Bond Medical Instruments Co., Ltd., Maanshan, China) inserted vertically through a guide tube to a depth of approximately 6–10 mm, corresponding to 0.3–0.5 cun according to the finger-cun measurement method. After all six acupoints had been treated, the needles were retained for 30 min without manual manipulation or intentional elicitation of de qi. In accordance with the standard practice of BA, strong needling sensation is not required, which differs from some forms of conventional manual body acupuncture. At the end of the 30-min retention period, the needles were removed and the treated points were gently compressed with a cotton swab.
In the sham group, after the same six acupoints had been identified, an identical guide-tube needle assembly was used to simulate the needling procedure performed in the BA group. The assembly consisted of a sterile filiform needle preloaded in a guide tube, with the needle handle initially fixed at the top of the tube. During the sham procedure, the guide tube was applied to each acupoint with the same pressure and in the same sequence as in the BA group, but the needle handle was not released or advanced. Thus, only the guide tube contacted the skin, and the needle tip remained inside the guide tube and did not protrude beyond the tube or penetrate the skin. This non-penetrating sham procedure was designed to reproduce the main contextual and procedural components of BA, including buccal acupoint identification, guide-tube contact, procedural sequence, supine positioning, and the same 30-min treatment context, while avoiding skin penetration and active needling stimulation. Its design and reporting were guided by the SHARE recommendations for sham acupuncture reporting and by methodological literature on non-penetrating sham controls and the influence of control interventions in acupuncture trials.22–24
In both groups, localized acupoint contact/pressure was applied in the same sequence and within the same procedural context. In the sham group, this non-penetrating pressure/contact was intended to reproduce the initial contact and procedural context of the BA intervention. Although the sham procedure could not fully reproduce the exact sensation of needle penetration, the use of very fine BA needles, absence of intentional de qi elicitation, eye closure, identical treatment context, and end-of-procedure cotton-swab compression were intended to support participant blinding. Participants in the sham group remained in the PACU for the same 30-min study period. In this study, one cun was defined as the width of the participant’s middle finger.
Study Protocol
Before surgery, all participants received standardized instructions on how to distinguish CRBD from other postoperative discomfort. CRBD was explained as vague, poorly localized visceral discomfort, such as a burning sensation, urinary urgency, or suprapubic discomfort. Participants were also informed that BA was performed using fine filiform needles and generally caused minimal needling sensation, whereas the most noticeable procedural sensation was the pressure of the guide tube during point localization. After surgery, patients were transferred to the PACU. Baseline CRBD (0 h) was assessed after extubation and before any intervention, after which the allocated intervention or sham procedure was administered during a 30-min study period in the PACU. Patients were then transferred to the general ward, where participant blinding was assessed. Rescue medications were administered according to standardized institutional protocols. For patients with persistent moderate-to-severe CRBD (score ≥ 2) or severe acute discomfort despite the allocated intervention, intravenous sufentanil 0.1 μg·kg−1 was provided in the PACU as judged by the PACU anesthesiologist for immediate symptom relief. Following transfer to the general ward, persistent CRBD symptoms or suspected bladder spasm were evaluated by the urologist and treated with intravenous phloroglucinol 80 mg. Tramadol 1 mg·kg−1 was used only when catheter-related discomfort persisted after antispasmodic therapy in the ward. Rescue medication decisions were based on CRBD-related discomfort/bladder spasm and patient intolerance rather than VAS scores alone, because VAS was used to assess postoperative pain or discomfort unrelated to CRBD-specific symptoms. Rescue medication use within the first 24 postoperative hours was recorded. Whenever clinically feasible, scheduled CRBD assessments were performed before administration of rescue medication at the corresponding time point. If immediate treatment was required for severe distress or catheter intolerance, rescue medication was administered without delaying clinical care. A detailed study timeline is shown in Figure 1C.
Assessments
Patient characteristics and intraoperative variables were recorded. CRBD severity was assessed at 0, 1, 2, 6, and 24 h after extubation, with the 0-h assessment performed after extubation and before intervention. CRBD severity was graded using a four-point scale:25 none (score 0), no symptoms even when questioned; mild (score 1), symptoms reported only on questioning; moderate (score 2), symptoms reported spontaneously without behavioral responses; and severe (score 3), symptoms reported spontaneously with behavioral responses, including attempts to remove the urinary catheter, verbal complaints, or agitation. A CRBD score of ≥2 was defined as moderate-to-severe CRBD. Postoperative pain or discomfort unrelated to CRBD was assessed using a VAS26 at 0, 1, 2, 6, 24, and 48 h after extubation. The number of patients requiring rescue antispasmodic or analgesic medications within the first 24 postoperative hours was recorded. Quality of recovery was evaluated using the 15-item Quality of Recovery questionnaire (QoR-15)27 preoperatively and on postoperative day (POD) 1 and POD 2, and sleep quality was assessed using the Richards-Campbell Sleep Questionnaire (RCSQ)28 at the same time points. BA-related adverse events, such as localized hematoma or infection, were monitored throughout the study period.
Primary and Secondary Endpoints
The primary endpoint was the incidence of moderate-to-severe CRBD at 1 h after extubation. Secondary endpoints included the incidence of moderate-to-severe CRBD at 2, 6, and 24 h after extubation; CRBD severity scores at 1, 2, 6, and 24 h after extubation; VAS scores at 1, 2, 6, 24, and 48 h, with the 0-h value as the after extubation baseline; rescue antispasmodic and analgesic medication use within 24 h; QoR-15 and RCSQ scores on POD 1 and POD 2; intervention-related adverse events; and participant blinding.
Statistical Analysis
Sample size calculation was based on the primary endpoint. Previous data indicated a ~34.2% incidence of moderate-to-severe CRBD at 1 h after extubation in untreated URSL patients.29 Pharmacological interventions typically reduce this rate to 10%–15%.2,30 Consequently, we hypothesized that BA would reduce the incidence to 12% at 1 h. Using PASS 2021 (NCSS, LLC, Kaysville, UT, USA), at least 53 patients per group were required to achieve 80% power at a two-sided alpha level of 0.05. Accounting for an anticipated 10% dropout rate, the target sample size was set at 59 patients per group.
Analyses were performed according to the intention-to-treat (ITT) principle. Continuous variables are presented as mean ± SD or median [IQR], and categorical variables as number (%). Binary outcomes were analyzed using the chi-square or Fisher’s exact test and reported as relative risks (RRs) with 95% confidence intervals (CIs). The number needed to treat (NNT) and its 95% CI were calculated from the absolute risk reduction; the 95% CI for the NNT was obtained by inverting the Wald 95% CI for the absolute risk reduction.
Ordinal outcomes (CRBD scores) and non-normally distributed continuous data (VAS, QoR-15, RCSQ) were compared using the Mann–Whitney U-test, with median differences reported as Hodges–Lehmann (HL) estimates alongside 95% CIs. To account for the repeated-measures structure of CRBD severity scores, we performed a supportive rank-transformed longitudinal GEE analysis for CRBD severity scores measured at 0, 1, 2, 6, and 24 h after extubation. This analysis focused on CRBD severity because it was the key repeated ordinal CRBD outcome directly related to the primary endpoint and postoperative symptom trajectory. CRBD severity scores were rank-transformed across all observations and analyzed using a generalized estimating equation model with participant as the clustering unit, an exchangeable working correlation structure, and robust standard errors. The model included group, time, and time-by-group interaction terms, with time treated as a categorical factor. Group, time, and time-by-group interaction effects were assessed using joint Wald tests. The primary endpoint was evaluated at α = 0.05 without multiplicity adjustment; secondary endpoints were treated as supportive. To assess blinding efficacy, the distribution of participants’ guesses was summarized. Bang’s Blinding Index (BI) with 95% CIs was calculated for each arm, retaining “uncertain” responses in the denominator.31 James’ BI and its 95% CI (estimated via a nonparametric bootstrap procedure with 10,000 resamples) were calculated for the overall trial.32 All analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Participant flow is summarized in Figure 2. Of 150 patients screened, 118 were randomized to the BA group (n = 59) or the sham group (n = 59). All randomized participants completed the study and were included in the ITT analysis, with no missing outcome data. Baseline demographic and clinical characteristics were comparable between groups (Table 1). Perioperative variables, including surgery type, anesthesia time, surgical time, anesthetic consumption, ureteral stent size, catheter size, and urinary catheterization duration, were also similar (Table 2). Postoperative outcomes were then assessed according to the prespecified endpoint hierarchy.Baseline CRBD status (0 h), assessed after extubation and before the intervention, was comparable between groups; moderate-to-severe CRBD was present in 37/59 (62.7%) patients in the BA group and 35/59 (59.3%) in the sham group (RR 1.06, 95% CI 0.79–1.41; P = 0.850). Post-intervention, the incidence of moderate-to-severe CRBD at 1 h (the primary endpoint) was significantly lower in the BA group than in the sham group (8/59 [13.6%] vs. 24/59 [40.7%]; RR 0.33, 95% CI 0.16–0.68; P = 0.002; NNT = 4, 95% CI 3–9) (Table 3). This reduction remained significant at 2 h (4/59 [6.8%] vs. 15/59 [25.4%]; RR 0.27, 95% CI 0.09–0.76; P = 0.012; NNT = 6, 95% CI 4–18), but not at 6 h (3/59 [5.1%] vs. 5/59 [8.5%]; RR 0.60, 95% CI 0.15–2.40; P = 0.717) or 24 h, at which point no patient in either group exhibited moderate-to-severe CRBD.
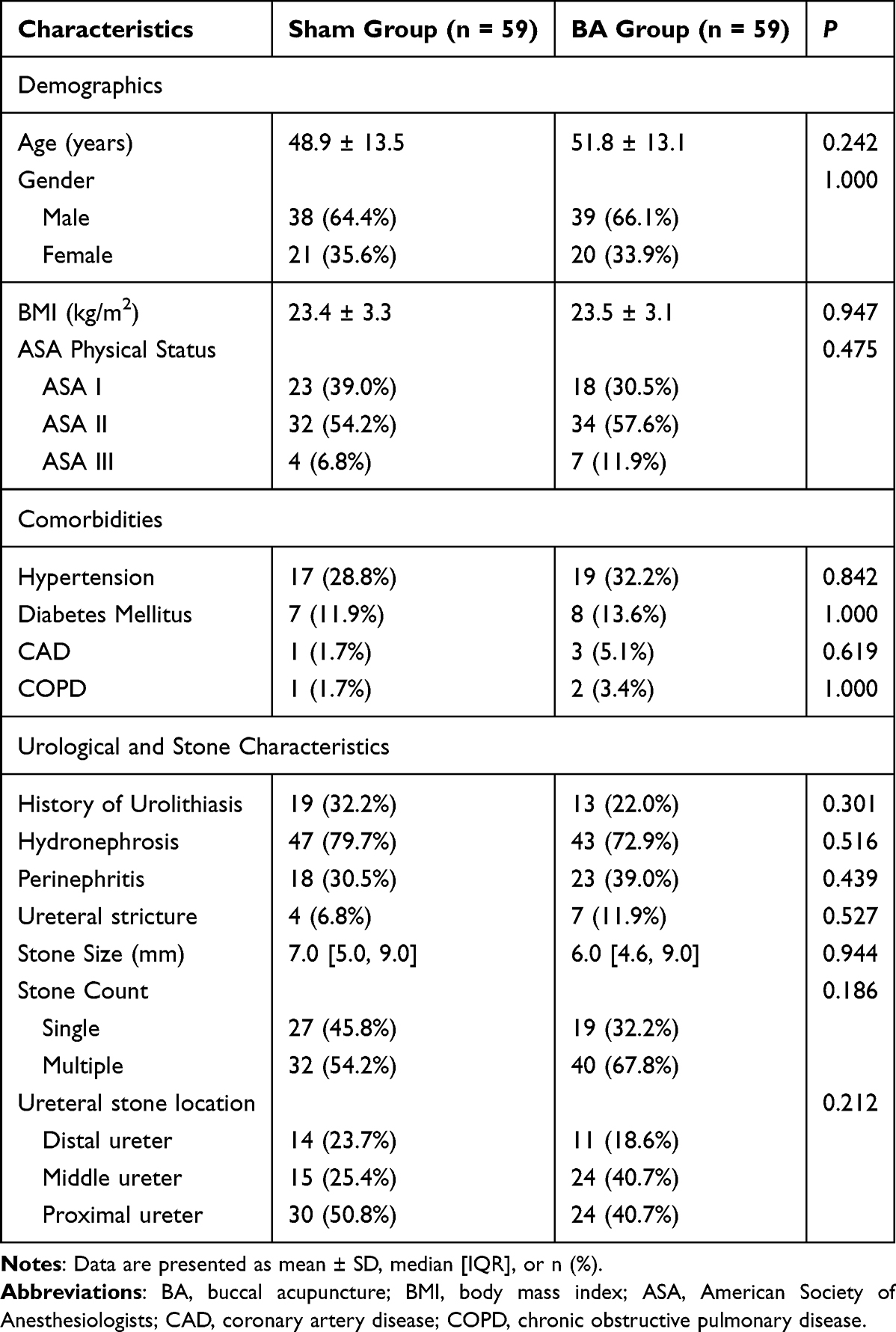 |
Table 1 Baseline Demographic and Clinical Characteristics |
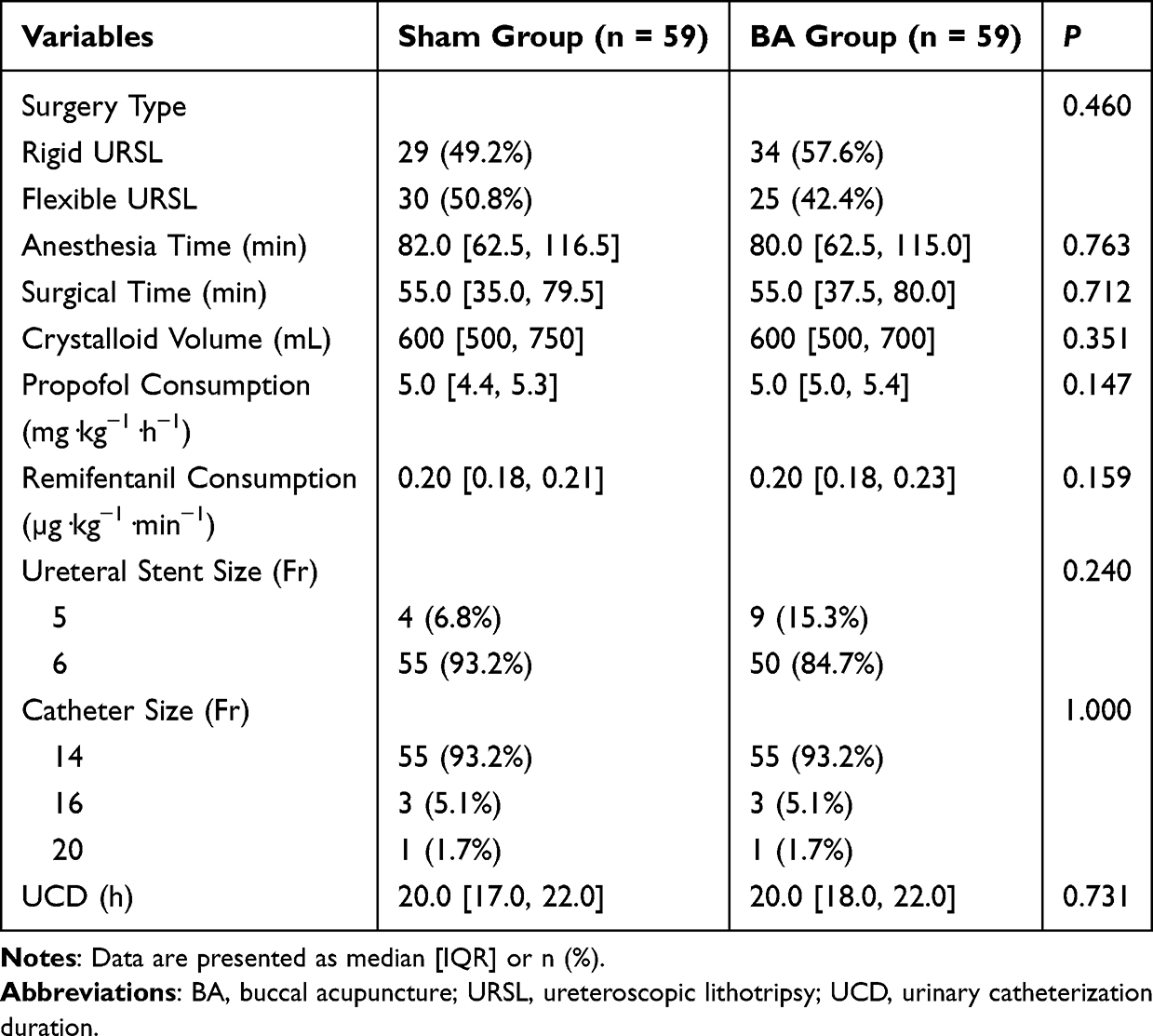 |
Table 2 Perioperative and Catheter-Related Characteristics |
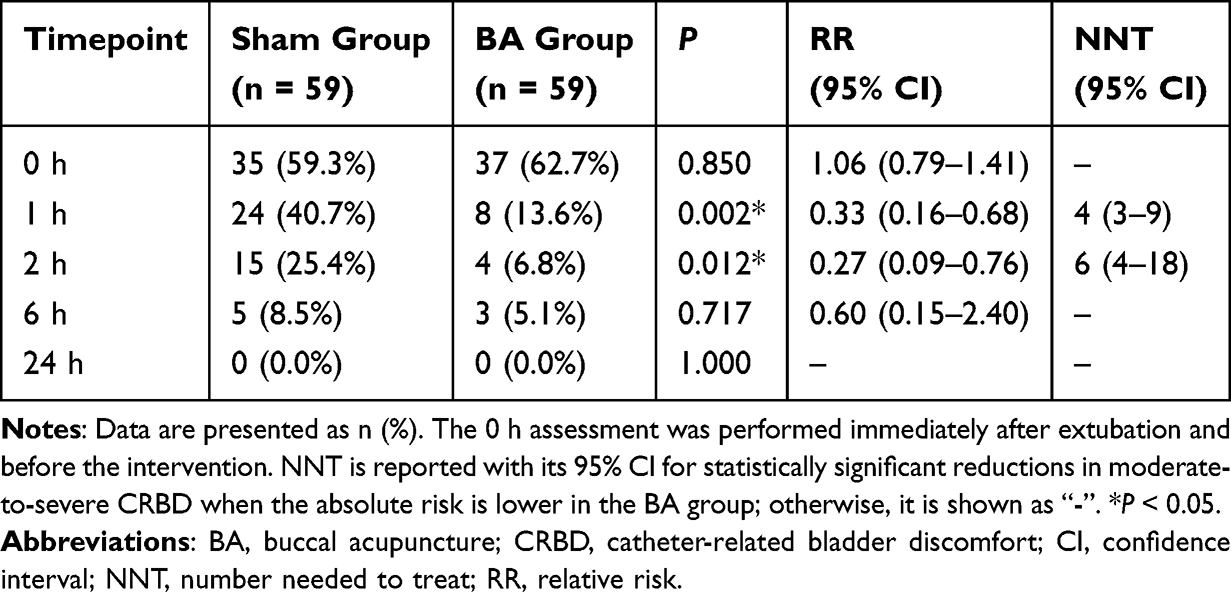 |
Table 3 Incidence of Moderate-to-Severe CRBD |
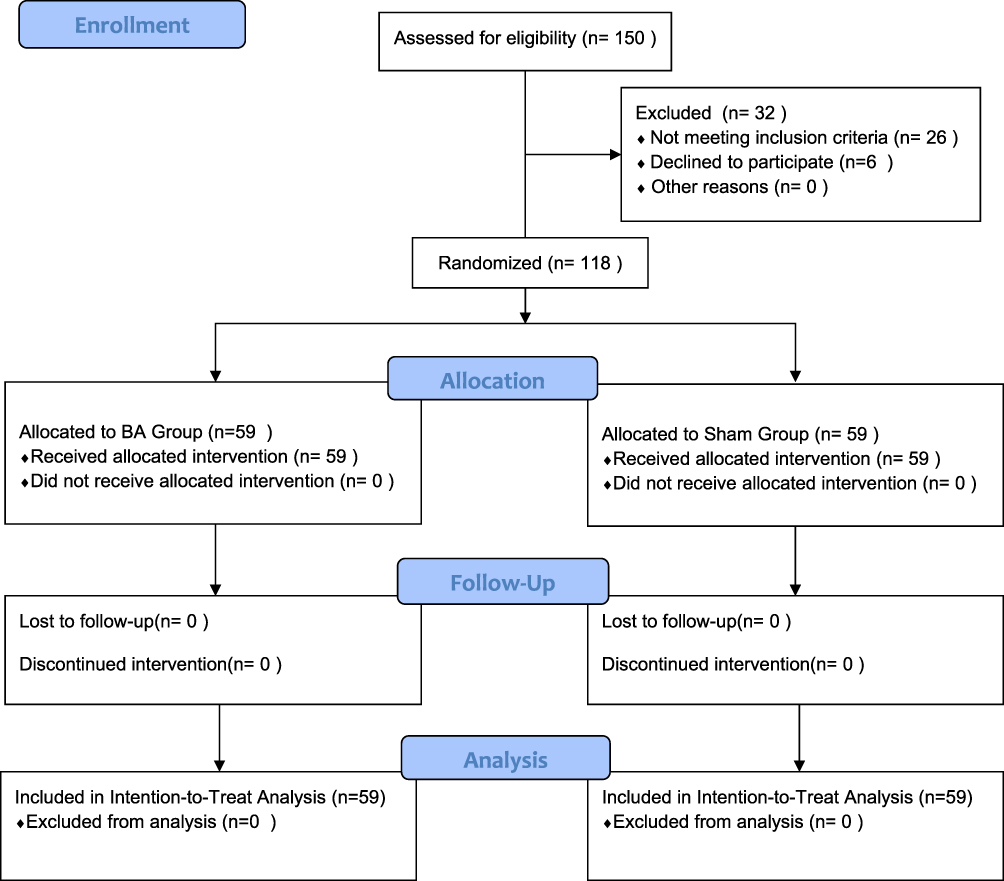 |
Figure 2 CONSORT flow diagram of the study. Abbreviations: BA, buccal acupuncture; ITT, intention-to-treat. |
CRBD severity distribution differed significantly between groups at 1 h (P < 0.001) and 2 h (P = 0.004), but not at 6 h (P = 0.118) or 24 h (P = 0.070) (Figure 3, Supplementary Table 1). This difference at early time points was mainly attributable to a lower proportion of patients with moderate CRBD in the BA group (8/59 [13.6%] vs. 23/59 [39.0%] at 1 h; 4/59 [6.8%] vs. 15/59 [25.4%] at 2 h), coupled with more asymptomatic patients in the BA group at both time points (13/59 [22.0%] vs. 4/59 [6.8%] at 1 h; 16/59 [27.1%] vs. 8/59 [13.6%] at 2 h). Severe CRBD was present at baseline in both groups, but post-intervention it was observed in only one patient in the sham group at 1 h, and was absent thereafter in both groups. By 24 h, most patients were asymptomatic, although mild CRBD persisted in 3 patients (5.1%) in the BA group and 9 patients (15.3%) in the sham group. In the supportive rank-transformed longitudinal GEE analysis of CRBD severity scores, the time-by-group interaction was significant (P < 0.001), indicating that the longitudinal trajectory of CRBD severity differed between the BA and sham groups. The overall time effect was also significant (P < 0.001). The group main effect averaged across all postoperative time points was not significant (P = 0.977), which should be interpreted in the context of the significant time-by-group interaction rather than as absence of time-specific between-group differences. This pattern was consistent with the point-by-point analyses showing that the between-group difference was mainly concentrated during the early postoperative period.
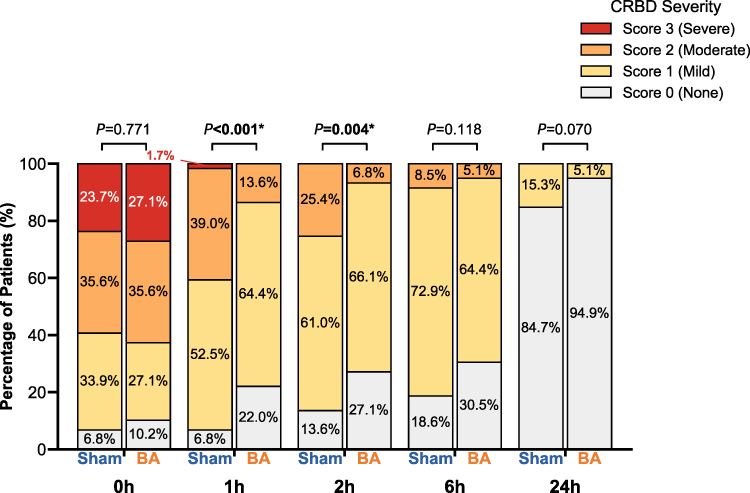 |
Figure 3 CRBD severity distributions at postoperative time points. Abbreviations: BA, buccal acupuncture; CRBD, catheter-related bladder discomfort. Notes: Stacked bar charts show the proportions of patients with CRBD severity scores of 0 (none), 1 (mild), 2 (moderate), and 3 (severe) in the BA and sham groups at 0, 1, 2, 6, and 24 h after extubation. The 0 h assessment was performed immediately after extubation and before the intervention. Bold P values marked with an asterisk (*) indicate statistically significant differences in CRBD severity distribution between the BA and sham groups (P < 0.05). |
Baseline VAS scores (0 h) were comparable between groups (median 3.0 [IQR 2.0, 3.0] in both groups). Postoperatively, no significant differences in VAS scores were observed at 1, 2, 6, 24, or 48 h, although VAS scores were numerically lower in the BA group at 1 h (2.0 [IQR 1.0, 3.0] vs. 2.0 [IQR 2.0, 3.0]; P = 0.093) and 2 h (2.0 [IQR 1.0, 2.5] vs. 2.0 [IQR 1.5, 3.0]; P = 0.084) (Table 4). In contrast, significantly fewer patients in the BA group required rescue medications during the first 24 postoperative hours, including phloroglucinol (17/59 [28.8%] vs. 33/59 [55.9%]; RR 0.52, 95% CI 0.33–0.82; P = 0.005), sufentanil administered in the PACU (12/59 [20.3%] vs. 24/59 [40.7%]; RR 0.50, 95% CI 0.28–0.90; P = 0.028), and tramadol administered in the ward (8/59 [13.6%] vs. 22/59 [37.3%]; RR 0.36, 95% CI 0.18–0.75; P = 0.006).Preoperatively, QoR-15 scores were similar between groups (125.0 [111.5, 132.0] in the BA group vs. 121.0 [105.0, 128.0] in the sham group; HL estimate 2.0, 95% CI −3.0 to 8.0; P = 0.356) (Figure 4, Supplementary Table 2). On POD 1, QoR-15 scores were higher in the BA group than in the sham group (110.0 [100.5, 118.0] vs. 102.0 [100.0, 110.0]; HL 5.0, 95% CI 1.0–9.0; P = 0.004), although this HL estimate did not reach the minimal clinically important difference (MCID) of 8.0. By POD 2, QoR-15 scores were again comparable (135.0 [128.5, 140.0] in the BA group vs. 133.0 [128.0, 135.0] in the sham group; HL 1.0, 95% CI −1.0 to 5.0; P = 0.238). RCSQ scores were also similar between groups preoperatively (76.0 [69.5, 89.0] vs. 78.0 [68.5, 89.0]; HL 0.0, 95% CI −5.0 to 5.0; P = 0.991), on POD 1 (68.0 [65.0, 73.5] vs. 68.0 [65.0, 76.5]; HL 1.0, 95% CI −2.0 to 4.0; P = 0.458), and on POD 2 (83.0 [76.0, 88.0] vs. 83.0 [79.0, 89.5]; HL 1.0, 95% CI −1.0 to 5.0; P = 0.303). Additional postoperative outcomes, including length of hospital stay and hospitalization cost, were comparable between groups. Length of hospital stay was 6.00 [4.50, 7.00] days in the sham group and 6.00 [5.00, 7.00] days in the BA group (P = 0.789), while hospitalization cost was 13,105.46 [9,341.68, 15,556.08] CNY and 10,808.66 [9,028.94, 14,953.45] CNY, respectively (P = 0.262).
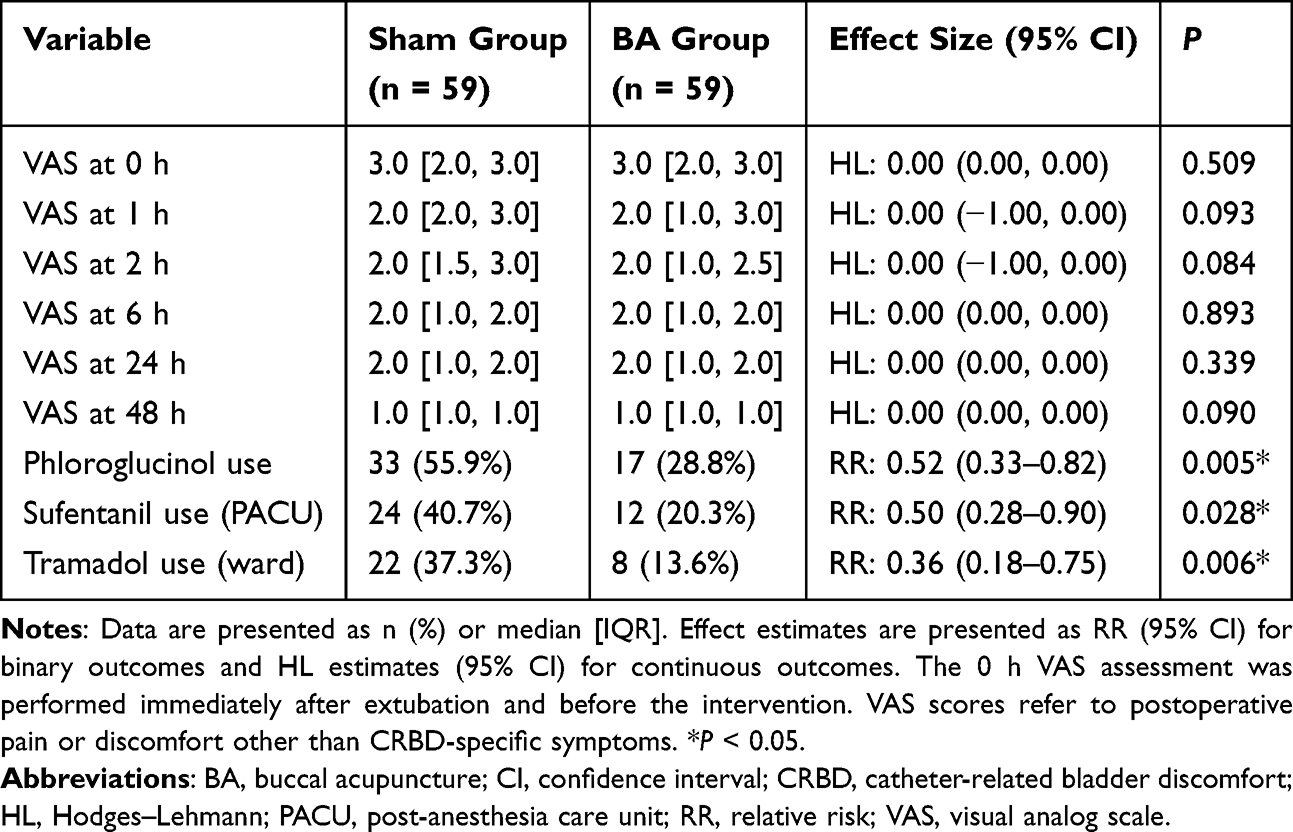 |
Table 4 VAS Scores and Rescue Medication Use |
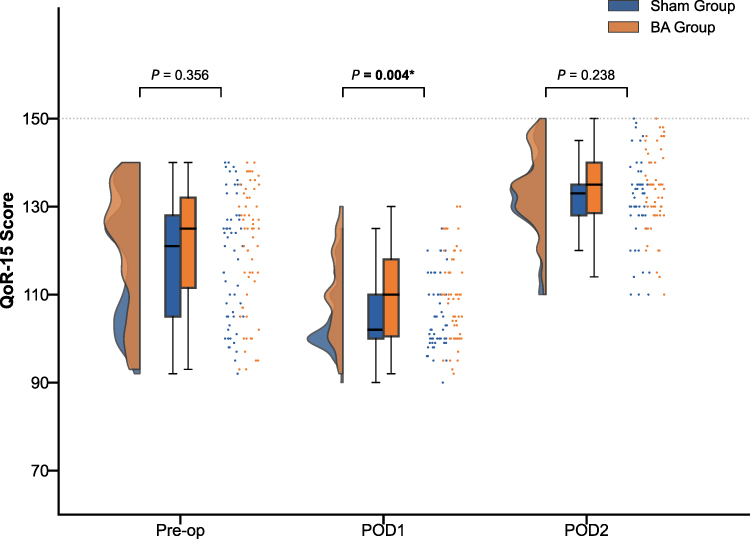 |
Figure 4 Distribution of QoR-15 scores. Abbreviations: BA, buccal acupuncture; Pre-op, preoperative; POD, postoperative day; QoR-15, 15-item Quality of Recovery questionnaire. Notes: Raincloud plots show the distributions of QoR-15 scores in the BA and sham groups preoperatively and on POD 1 and POD 2. Each plot combines a half-violin density plot, a box plot showing the median and IQR, and individual data points. Bold P values marked with an asterisk (*) indicate statistically significant differences in QoR-15 scores between the BA and sham groups (P < 0.05). |
BA-related adverse events were limited to minor bleeding after needle removal at the insertion sites in four patients (6.8%), all of which resolved immediately with local compression. No other BA-related adverse events, including pain at the needle insertion sites, hematoma, or infection, were observed. Treatment guesses were distributed across all three response categories in both groups (Supplementary Table 3). In the BA group, 29 participants (49.2%) guessed “real acupuncture”, 12 (20.3%) guessed “sham acupuncture”, and 18 (30.5%) were uncertain; the corresponding values in the sham group were 32 (54.2%), 11 (18.6%), and 16 (27.1%), respectively. James’ BI was 0.657 (95% CI 0.578–0.737). Bang’s BI was 0.288 (95% CI 0.089–0.488) in the BA group and −0.356 (95% CI −0.554 to −0.158) in the sham group.
Discussion
In this single-center, participant- and assessor-blinded, sham-controlled randomized trial, our results indicate that BA is an effective non-pharmacological adjunct for mitigating early postoperative CRBD following URSL. Consistent with our primary hypothesis, BA significantly reduced the incidence of moderate-to-severe CRBD at 1 hour post-extubation, and this difference remained significant at 2 hours. Concurrently, BA significantly decreased the requirement for rescue medications. While postoperative VAS and RCSQ scores were comparable between groups, and the modest improvement in QoR-15 scores on POD 1 did not reach the MCID, these results point toward the specific utility of BA in the targeted relief of catheter-related symptoms rather than providing generalized analgesia. With adverse events limited to minor insertion-site bleeding and participant blinding adequately maintained, our findings highlight the safety and specific clinical utility of BA.
Most CRBD studies focus on pharmacological treatments. However, adverse effects like sedation and hemodynamic instability often limit their perioperative use.33–35 Although researchers have explored non-pharmacological options like TEAS and wrist-ankle acupuncture,10,11,36 these interventions are typically applied intraoperatively or as preventive measures. In contrast, our study administered BA specifically after tracheal extubation, targeting acute symptoms in the PACU. BA also fundamentally differs from traditional body acupuncture. Grounded in holographic projection theory, BA treats remote urinary symptoms via facial stimulation. This targeted approach may offer potential practical advantages in the PACU environment: requiring no limb exposure or patient movement, BA avoids interfering with surgical sites, catheters, or monitors. Its rapid onset and ease of administration could make BA exceptionally suitable for the early postoperative period, when severe CRBD often peaks. Critically, BA appears to relieve these symptoms without increasing systemic sedation, which might help maintain clear consciousness assessments and avoid unnecessary delays in PACU discharge. The observed benefit was concentrated in the first 1–2 h after extubation, which represents the key clinical window for early CRBD management. During emergence and PACU recovery, severe CRBD may cause substantial distress, catheter intolerance, and agitation, sometimes leading to traumatic catheter manipulation or additional rescue medication. Therefore, reducing CRBD during this acute phase may help improve early postoperative stability and reduce avoidable medication exposure, even though group differences were not observed at later time points.
The early benefits observed in our study may be partly related to the theoretical and neurophysiological basis of BA. BA is a microneedle therapy derived from biological holography, Da San Jiao theory, and mind-body integration.12 In this study, we selected the Lower Jiao, Lumbar, and Sacral points, which are considered to correspond to urinary system function. According to TCM theory, CRBD may be associated with dysregulation of qi movement in the Lower Jiao, which can manifest as urinary urgency and bladder spasm; stimulation of these points is traditionally believed to help regulate qi flow and alleviate bladder-related symptoms.37,38 In addition, BA is performed on the cheeks, where the superficial tissues are richly innervated by afferent fibers of the trigeminal nerve. Buccal stimulation may activate trigeminal sensory afferents and influence central sensory-autonomic regulation. This possibility is supported by recent evidence that cheek acupuncture can induce immediate changes in brain oscillations and functional connectivity, as well as by broader acupuncture literature showing that peripheral afferent activation may engage descending pain-modulatory and somato-autonomic pathways.15,39,40 Studies of overactive bladder and sacral neuromodulation suggest that modulation of bladder afferent signaling, spinal reflex pathways, and supraspinal micturition-control circuits can influence lower urinary tract symptoms.41,42 Acupuncture studies in overactive bladder also suggest potential effects on urinary urgency and micturition-related symptoms.43,44 Given the low VAS scores in this study, the CRBD relief observed with BA may partly involve bladder sensory and reflex modulation rather than general somatic analgesia alone. We hypothesize that buccal stimulation may engage trigeminal sensory-autonomic pathways and secondarily modulate bladder reflex activity, contributing to relief of catheter-induced visceral discomfort. However, the present study was not designed to directly test these mechanisms, and these explanations should therefore be regarded as hypotheses for future investigation.
These proposed mechanisms may also help explain why the observed benefit of BA was concentrated in the early postoperative period. In our study, moderate-to-severe CRBD became less frequent over time in both groups and was no longer observed at 24 h. The absence of separation at later time points should not necessarily be interpreted as loss of the early effect of BA. Instead, it may reflect patients’ gradual adaptation to the indwelling urinary catheter, spontaneous resolution of bladder spasm, and ongoing postoperative recovery, which together would reduce the likelihood of severe CRBD over time. The supportive rank-transformed longitudinal GEE analysis further supported the time-dependent nature of this treatment effect. The significant time-by-group interaction indicated that CRBD severity changed differently over time in the BA and sham groups, with the greatest between-group separation observed during the early post-intervention period. The nonsignificant group main effect likely reflected averaging across early and later postoperative time points and therefore did not negate the early time-specific benefit observed in the point-by-point analyses. Together, these findings support that the benefit of BA was mainly concentrated in early CRBD relief.
We observed that fewer patients in the BA group required rescue antispasmodic or analgesic medications during the first 24 postoperative hours. This reduced reliance on systemic rescue therapies directly correlates with the lower incidence of early moderate-to-severe CRBD in the BA group. By providing effective early relief, BA successfully minimized patients’ exposure to the adverse effects commonly associated with conventional pharmacological management. Interestingly, VAS scores were similar between groups and remained low overall. Because URSL is a minimally invasive procedure with limited somatic surgical trauma, these low VAS scores suggest that postoperative discomfort in this population was driven mainly by catheter-induced bladder irritation rather than surgical pain. This distinction further supports the clinical utility of BA in specifically addressing catheter-related discomfort.
We also observed that QoR-15 scores were higher in the BA group on POD 1. This may be related to the reduction in moderate-to-severe CRBD during the early postoperative period. However, the HL estimate of 5.0 did not reach the MCID of 8.0,45 and the difference was no longer present on POD 2. In addition, RCSQ scores were similar between groups throughout follow-up. These findings suggest that any effect of BA on overall postoperative recovery may be modest and may be more closely related to early relief of CRBD than to broader recovery outcomes.
Like conventional acupuncture, BA appears to have a favorable safety and tolerability profile.46,47 With respect to blinding, the James’ and Bang’s blinding indices suggested that participant blinding was acceptable overall. Specifically, the James’ BI of 0.657 supported reasonable preservation of overall blinding. The Bang’s BI values suggested mild unblinding in the BA group (0.288) and a tendency toward opposite guessing in the sham group (−0.356). Such blinding results are not uncommon in acupuncture trials and do not necessarily negate overall blinding;48–50 however, they do suggest that expectancy-related influences should be considered when interpreting the treatment effect. Taken together, these features suggest that BA may be a feasible adjunctive option for early postoperative CRBD management after URSL.
This study has several limitations. First, this was a single-center study conducted in a tertiary Grade A PLA hospital. Although the standardized perioperative management and relatively homogeneous clinical setting helped improve internal consistency, recruitment from a single institution with a relatively homogeneous patient population may limit the generalizability of our findings. In addition, because surgical trauma, catheterization characteristics, and postoperative recovery pathways may differ across transurethral procedures, these findings should be confirmed in patients undergoing other urological surgeries, such as transurethral bladder tumor or prostate resection. Despite acceptable overall blinding, Bang’s index revealed a mild unblinding tendency in the BA group, likely due to the absence of retained facial placebo needles (eg., Streitberger). While PACU sedation helped mask this, expectancy biases cannot be entirely ruled out. Another limitation is related to rescue-medication use. Because rescue medications were ethically permitted for severe distress or catheter intolerance, rescue treatment may have influenced subsequent symptom assessments, particularly at later time points. However, scheduled CRBD assessments were performed before rescue medication whenever clinically feasible, and immediate treatment was not delayed when clinically required. In addition, BA was administered shortly after emergence from general anesthesia in the PACU; therefore, residual anesthetic and analgesic effects may have influenced sensory afferent transmission, central pain-modulatory pathways, autonomic responses, and patients’ perception of needling sensation. However, because perioperative anesthetic management was standardized between groups, these residual effects would be expected to attenuate sensory or autonomic responses in both groups rather than introduce a systematic between-group bias. Finally, utilizing a single acupuncturist maximizes internal validity but introduces operator dependency, potentially further limiting the generalizability of our findings. Additionally, our single-session design precluded dose-response evaluations, and the underlying physiological mechanisms remain unexplored.
Future multicenter trials involving broader patient populations and objective mechanistic assessments are needed to confirm external validity and elucidate the mechanisms of BA. Given the very low CRBD and VAS scores after 6 h in both groups, later assessments may have been affected by a floor effect related to natural recovery and catheter adaptation, making residual between-group differences difficult to detect. Future trials may therefore benefit from earlier primary endpoints or 0–6 h summary measures, together with more sensitive patient-centered outcomes, such as selected lower urinary tract symptom scales and 5-point Likert ratings of catheter-related inconvenience and patient acceptability of BA. Current BA practice texts commonly describe a single 30–40 min session as one treatment cycle; however, the optimal dosing strategy for postoperative CRBD remains unknown. Further studies should therefore optimize BA protocols for postoperative CRBD, including treatment timing, retention duration, treatment frequency, retreatment indications, and suitable target populations, especially among patients with more severe or persistent symptoms, prolonged catheterization, or other catheter-related complications.
Conclusion
In conclusion, this trial demonstrates that BA significantly reduces the incidence of early postoperative moderate-to-severe CRBD and decreases the requirement for rescue medications following URSL. BA may serve as a safe, non-pharmacological adjunct for the management of acute postoperative CRBD.
Abbreviations
ASA, American Society of Anesthesiologists; BA, Buccal acupuncture; BI, Blinding Index; BIS, Bispectral Index; CI, Confidence interval; CONSORT, Consolidated Standards of Reporting Trials; CRBD, Catheter-related bladder discomfort; HL, Hodges–Lehmann; ICU, Intensive care unit; IQR, Interquartile range; ITT, Intention-to-treat; MCID, Minimal clinically important difference; PACU, Post-anesthesia care unit; POD, Postoperative day; QoR-15, 15-item Quality of Recovery questionnaire; RCSQ, Richards-Campbell Sleep Questionnaire; RR, Relative risk; SD, Standard deviation; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; TCM, Traditional Chinese Medicine; TEAS, transcutaneous electrical acupoint stimulation; URSL, Ureteroscopic lithotripsy; VAS, Visual analog scale.
Data Sharing Statement
Summary data supporting the findings are provided in this article and the online Supplementary Tables. The individual participant-level dataset is not publicly deposited because the ethics approval and participant consent did not permit unrestricted public sharing of patient-level clinical data, and combinations of demographic, perioperative, and urological variables could increase the risk of participant re-identification. Controlled access to de-identified participant-level data underlying the reported results may be arranged through the corresponding author, Dr. Xu Zhang, for researchers with a methodologically sound proposal, subject to institutional approval and completion of a data-use agreement.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki. This study was approved by the ethics committee of the No. 924 Hospital of PLA Joint Logistic Support Force (Approval number: Gui Medicine [2024] No. 77), and was registered with the International Traditional Medicine Clinical Trial Registry (Clinical trial number: ITMCTR2024000302; Official website: http://itmctr.ccebtcm.org.cn/; date of registration: August 26, 2024). Written informed consent was obtained from all participants before their inclusion in the study. In addition, written informed consent was obtained from the individual shown in Panel A of Figure 1 for publication of the image.
Consent for Publication
Written informed consent was obtained from the individual shown in Panel A of Figure 1 for publication of the image. No other identifiable participant information is included in this manuscript.
Acknowledgments
The authors are grateful to all the participants who took part in this study for their time and cooperation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Self-funded Traditional Chinese Medicine Research Project of Guangxi Zhuang Autonomous Region (Grant No. [GXZYC20240397]).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Mitobe Y, Yoshioka T, Baba Y, et al. Predictors of catheter-related bladder discomfort after surgery: a literature review. J Clin Med Res. 2023;15(4):208–16. doi:10.14740/jocmr4873
2. Bai Y, Wang X, Li X, et al. Management of Catheter-related bladder discomfort in patients who underwent elective surgery. J Endourol. 2015;29(6):640–649. doi:10.1089/end.2014.0670
3. Cheon YW, Kim SH, Paek JH, et al. Effects of nefopam on catheter-related bladder discomfort in patients undergoing ureteroscopic litholapaxy. Korean J Anesthesiol. 2018;71(3):201–206. doi:10.4097/kja.d.18.27113
4. Markopoulos T, Katsimperis S, Lazarou L, et al. Catheter-related bladder discomfort: insights into pathophysiology, clinical impact, and management. Cureus. 2025;17(3):e81322. doi:10.7759/cureus.81322
5. Jang EB, Hong SH, Kim KS, et al. Catheter-related bladder discomfort: how can we manage It? Int Neurourol J. 2020;24(4):324–331. doi:10.5213/inj.2040108.054
6. Wang Z, Li H, Wang Y, et al. Esketamine for preventing Catheter-related bladder discomfort after ureteroscopic lithotripsy: a randomized controlled trial. BMC Anesthesiology. 2025;25(1):361. doi:10.1186/s12871-025-03236-2
7. Binhas M, Motamed C, Hawajri N, Yiou R, Marty J. Predictors of catheter-related bladder discomfort in the post-anaesthesia care unit. Ann Fr Anesth Reanim. 2011;30(2):122–125. doi:10.1016/j.annfar.2010.12.009
8. Liang S, Pang Z, Zhou N, et al. Development and validation of a prediction model for catheter-related bladder discomfort: a prospective observational study. Br J Anaesth. 2022;129(6):e147–e149. doi:10.1016/j.bja.2022.08.018
9. Liang D, Jin S, Huang L, et al. The effect of transcutaneous electrical acupoint stimulation on postoperative Catheter-related bladder discomfort in patients undergoing transurethral resection of the prostate. Evid Based Complement Alternat Med. 2021;2021:6691459. doi:10.1155/2021/6691459
10. Hou J, Li Y, Wu Y, et al. Safety and efficacy of wrist-ankle acupuncture in treating catheter-related bladder discomfort after transurethral resection of the prostate: a double-blind randomized clinical trial. Gland Surg. 2022;11(9):1464–1471. doi:10.21037/gs-22-438
11. Guo L, Li P, Li S, Song J, Wang Q, Tian W. Comparison of the effect of acupoint injection and tramadol for the treatment of catheter-related bladder discomfort: a randomized controlled trial. Medicine. 2025;104(37):e44553. doi:10.1097/MD.0000000000044553
12. Wang Y. Cheek Acupuncture Therapy. Beijing: People’s Medical Publishing House; 2017. Chinese.
13. Yang X, Li B, Wu L, Cui Y. Acupuncture treatment of vascular cognitive impairment through peripheral nerve stimulation pathway: a scoping review. Front Aging Neurosci. 2025;17:1515327. doi:10.3389/fnagi.2025.1515327
14. Wang S, Liu K, Wang Y, et al. A proposed neurologic pathway for scalp acupuncture: trigeminal nerve–meninges–cerebrospinal fluid–contacting neurons–brain. Med Acupunct. 2017;29(5):322–326. doi:10.1089/acu.2017.1231
15. Chen X, Tong S, Zhu Y, Xu T, Guo X, Zhong W. Immediate modulations of cheek acupuncture on brain oscillations and connectivity in individuals with chronic pain. IEEE Trans Neural Syst Rehabil Eng. 2025;33:4229–4240. doi:10.1109/TNSRE.2025.3621122
16. Fan Z, Dou B, Wang J, et al. Effects and mechanisms of acupuncture analgesia mediated by afferent nerves in acupoint microenvironments. Front Neurosci. 2024;17:1239839. doi:10.3389/fnins.2023.1239839
17. Fowler CJ, Griffiths D, De Groat WC. The neural control of micturition. Nat Rev Neurosci. 2008;9(6):453–466. doi:10.1038/nrn2401
18. De Groat WC, Griffiths D, Yoshimura N. Neural control of the lower urinary tract. Compr Physiol. 2015;5(1):327–396. doi:10.1002/j.2040-4603.2015.tb00596.x
19. Xu X, Zhao L, Li Y, Zhan L, Zheng L, Wang J. Perioperative pain observation of hip fracture surgery patients with cheek acupuncture. J Pain Res. 2024;17:3719–3727. doi:10.2147/JPR.S491669
20. Y Yi, YE Huijun, Z Huiling, J Lihua. Clinical observation on 90 cases of primary dysmenorrhea treated by buccal acupuncture therapy: a randomized controlled study. J Tradit Chin Med. 2024;44(1):172–181. doi:10.19852/j.cnki.jtcm.20231110.001
21. Zhu Z-X, Chen C, Zheng Y-F, et al. Buccal acupuncture alleviates postoperative pain in patients undergoing radical resection of gastrointestinal cancers: a randomized controlled pilot study. Chin J Integr Med. 2025;31(6):558–565. doi:10.1007/s11655-025-4128-y
22. Ma P, Liu X, Liu Z, et al. The SHARE: Sham acupuncture reporting guidelines and a checklist in clinical trials. J Evid Based Med. 2023;16(4):428–431. doi:10.1111/jebm.12560
23. Lee H, Bang H, Kim Y, et al. Non-penetrating sham needle, is it an adequate sham control in acupuncture research? Complement Ther Med. 2011;19 Suppl 1:S41-S48. doi:10.1016/j.ctim.2010.12.002
24. MacPherson H, Vertosick E, Lewith G, et al. Influence of control group on effect size in trials of acupuncture for chronic pain: a secondary analysis of an individual patient data meta-analysis. PLoS One. 2014;9(4):e93739. doi:10.1371/journal.pone.0093739
25. Agarwal A, Yadav G, Gupta D, Singh PK, Singh U. Evaluation of intra-operative tramadol for prevention of catheter-related bladder discomfort: a prospective, randomized, double-blind study. Br J Anaesth. 2008;101(4):506–510. doi:10.1093/bja/aen217
26. Breivik H, Borchgrevink PC, Allen SM, et al. Assessment of pain. Br J Anaesth. 2008;101(1):17–24. doi:10.1093/bja/aen103
27. Stark PA, Myles PS, Burke JA. Development and psychometric evaluation of a postoperative quality of recovery score: the QoR-15. Anesthesiology. 2013;118(6):1332–1340. doi:10.1097/ALN.0b013e318289b84b
28. Richards KC, O’Sullivan PS, Phillips RL. Measurement of sleep in critically ill patients. J Nurs Measure. 2000;8(2):131–144. doi:10.1891/1061-3749.8.2.131
29. In C-B, Lee S-J, Sung T-Y, Cho C-K, Jee YS. Effects of chlorpheniramine maleate on catheter-related bladder discomfort in patients undergoing ureteroscopic stone removal: a randomized double-blind study. Int J Med Sci. 2021;18(4):1075–1081. doi:10.7150/ijms.53043
30. Ramesh R, Mittal A, Agrawal S. Pharmacological interventions for reducing catheter-related bladder discomfort in patients undergoing elective surgeries under general anaesthesia: a systematic review and meta-analysis. Indian J Anaesth. 2023;67(Suppl 2):S81–S92. doi:10.4103/ija.ija_200_22
31. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials. 2004;25(2):143–156. doi:10.1016/j.cct.2003.10.016
32. James KE, Bloch DA, Lee KK, Kraemer HC, Fuller RK. An index for assessing blindness in a multi-centre clinical trial: disulfiram for alcohol cessation—a va cooperative study. Stat Med. 1996;15(13):1421–1434. doi:10.1002/(SICI)1097-0258(19960715)15:13<1421::AID-SIM266>3.0.CO;2-H
33. Agarwal A, Dhiraaj S, Singhal V, Kapoor R, Tandon M. Comparison of efficacy of oxybutynin and tolterodine for prevention of catheter related bladder discomfort: a prospective, randomized, placebo-controlled, double-blind study. Br J Anaesth. 2006;96(3):377–380. doi:10.1093/bja/ael003
34. Hu B, Li C, Pan M, et al. Strategies for the prevention of catheter-related bladder discomfort: a PRISMA-compliant systematic review and meta-analysis of randomized controlled trials. Medicine. 2016;95(37):e4859. doi:10.1097/MD.0000000000004859
35. Lee S, Kim KT, Kim TB, et al. A multicenter, randomized, single-blind trial evaluating a multi-porous urethral Catheter with continuous local ropivacaine infusion for the reduction of postoperative Catheter-related bladder discomfort. J Clin Med. 2025;14(12):4215. doi:10.3390/jcm14124215
36. Park J-Y, Yu J, Kim C-S, Baek J-W, Mun T, Kim Y-K. Transcutaneous electrical nerve stimulation and catheter-related bladder discomfort following transurethral resection of bladder tumour: a randomised controlled trial. Eur J Anaesthesiol. 2024;41(11):821–830. doi:10.1097/EJA.0000000000002050
37. Wang D, You Y, Zhu Q, et al. Effect of cheek acupuncture on stress urinary incontinence in menopausal women: a randomized clinical trial. QJM. 2025:hcaf287. doi:10.1093/qjmed/hcaf287
38. Wu Y, Li P, Shi J, Li J, Zhang Y, Xiao B. Research trends of acupuncture therapy on stress urinary incontinence from 1992 to 2022: a bibliometric analysis. Heliyon. 2023;9(9):e19732. doi:10.1016/j.heliyon.2023.e19732
39. Chen T, Zhang WW, Chu Y-X, Wang Y-Q. Acupuncture for pain management: molecular mechanisms of action. Am J Chin Med. 2020;48(04):793–811. doi:10.1142/S0192415X20500408
40. Liu S, Wang Z, Su Y, et al. A neuroanatomical basis for electroacupuncture to drive the vagal–adrenal axis. Nature. 2021;598(7882):641–645. doi:10.1038/s41586-021-04001-4
41. Krhut J, Kobbero H, Kanaan R, Fode M, Poulsen M, Zvara P. The mechanism of action of neuromodulation in the treatment of overactive bladder. Nat Rev Urol. 2025;22(7):414–426. doi:10.1038/s41585-024-00967-8
42. Dequirez P-L, De Wachter S, Biardeau X. Sacral neuromodulation for low urinary tract dysfunction: overview and mechanisms of action. Auton Neurosci. 2025;261:103337. doi:10.1016/j.autneu.2025.103337
43. Lee -J-J, Heo J-W, Choi T-Y, Jun JH, Lee MS, Kim J-I. Acupuncture for the treatment of overactive bladder: a systematic review and meta-analysis. Front Neurol. 2023;13:985288. doi:10.3389/fneur.2022.985288
44. Ma J, Ren F, Lu S, et al. Acupuncture therapy of overactive bladder: an umbrella review and meta-analysis. Arab J Urol. 2025;23(1):75–83. doi:10.1080/20905998.2024.2400628
45. Myles PS, Myles DB. An updated minimal clinically important difference for the QoR-15 scale. Anesthesiology. 2021;135(5):934–935. doi:10.1097/ALN.0000000000003977
46. Xu M, Yang C, Nian T, et al. Adverse effects associated with acupuncture therapies: an evidence mapping from 535 systematic reviews. Chin Med. 2023;18(1):38. doi:10.1186/s13020-023-00743-7
47. Nielsen A, Dusek JA, Taylor-Swanson L, Tick H. Acupuncture therapy as an evidence-based nonpharmacologic strategy for comprehensive acute pain care: the academic consortium pain task force white paper update. Pain Med. 2022;23(9):1582–1612. doi:10.1093/pm/pnac056
48. Moroz A, Freed B, Tiedemann L, Bang H, Howell M, Park JJ. Blinding measured: a systematic review of randomized controlled trials of acupuncture. Evid Based Complement Alternat Med. 2013;2013:708251. doi:10.1155/2013/708251
49. Liu T, Jiang L, Li S, et al. The blinding status and characteristics in acupuncture clinical trials: a systematic reviews and meta-analysis. Syst Rev. 2024;13(1):302. doi:10.1186/s13643-024-02692-0
50. Zhao F-Y, Zheng Z, Fu -Q-Q, et al. Acupuncture for comorbid depression and insomnia in perimenopause: a feasibility patient-assessor-blinded, randomized, and sham-controlled clinical trial. Front Public Health. 2023;11:1120567. doi:10.3389/fpubh.2023.1120567
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Dose-Response Analysis of Nalbuphine for Alleviating Catheter-Related Bladder Discomfort After Ureteroscopic Lithotripsy in Men: A Retrospective Study
Tang J, Ni H, Yao M
Drug Design, Development and Therapy 2025, 19:5283-5292
Published Date: 19 June 2025
Effect of Acupuncture for Diminished Ovarian Reserve: A Randomized Sham-Controlled Trial
Wang X, Du P, Yang L, Li J, Hang T, Qi L, Su C, Liu X, Li W, Zhu Y, Lu G, Xu H, Fang Y
International Journal of Women's Health 2026, 18:580821
Published Date: 8 April 2026
Efficacy of Acupuncture for Pain in Parkinson’s Disease: Study Protocol for a Randomized Controlled Trial
Wu Y, Zhang F, Xiao L, Wang Y, Lin S, Wu S, Liu X, Zhuang L
Journal of Pain Research 2026, 19:622950
Published Date: 29 June 2026