Back to Journals » Patient Preference and Adherence » Volume 19
Bridging Knowledge Gaps in Prostate Cancer Screening Among Northern Saudi Males: Implications for Improving Screening Adherence and Early Detection
Authors Sayeed MU, Alanazi MM, Alanazi TM, Alwaladali SM, Alanazi IM, Alashjaee RH, Alanazi AA, Thirunavukkarasu A
Received 25 June 2025
Accepted for publication 1 October 2025
Published 23 October 2025 Volume 2025:19 Pages 3295—3306
DOI https://doi.org/10.2147/PPA.S549612
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Emma Veale
Mohammed Ubaidullah Sayeed,1 Muhannad Mohammed Alanazi,2 Turki Mutad Alanazi,2 Saud Mudhhi Alwaladali,2 Ibrahim Mohammed Alanazi,2 Rayan Harbi Alashjaee,2 Abdullah Ayed Alanazi,2 Ashokkumar Thirunavukkarasu3
1Department of Pathology, College of Medicine, Jouf University, Sakaka, Aljouf, Saudi Arabia; 2College of Medicine, Jouf University, Sakaka, Aljouf, Saudi Arabia; 3Department of Family and Community Medicine, College of Medicine, Jouf University, Sakaka, Aljouf, Saudi Arabia
Correspondence: Mohammed Ubaidullah Sayeed, Department of Pathology, College of Medicine, Jouf University, Sakaka, 72388, Saudi Arabia, Tel +966-506835394, Email [email protected]
Background and Objectives: Prostate cancer (PCa) is the second most commonly diagnosed cancer among men worldwide Insufficient awareness and poor attitudes towards PCa adversely impact early detection efforts among men. The present study aimed to assess the knowledge, attitude, and associated factors towards PCa and its screening among northern Saudi males.
Methods: Using a validated data collection tool, we surveyed 381 males in this cross-sectional study in the Arar and Aljouf regions of Saudi Arabia. We applied Spearman’s test to find the correlation between knowledge and attitude domains. Using the binary logistic regression model, we determined the predictors associated with the knowledge and attitude.
Results: We found that less than half of the males had high levels of knowledge (37.0%) and attitude (47.5%) towards PCa. Knowledge was significantly higher among those working in the private sector (adjusted odds ratio [aOR] = 2.79, 95% confidence interval [CI] = 1.63– 4.22, p = 0.003) and among those with a family history of PCa (aOR = 2.11, 95% CI = 1.75– 2.81, p = 0.017). Significantly lower levels of knowledge are observed in people aged above 55 years (aOR = 0.78, 95% CI = 0.53– 0.91, p = 0.009) and those residing in rural areas (aOR = 0.53, 95% CI = 0.27– 0.81, p = 0.007). Regarding attitude, we found that smokers (aOR = 0.48, 95% CI = 0.27– 0.62, p = 0.001) and those living in rural areas (aOR = 0.59, 95% CI = 0.44– 0.81, p = 0.004) had significantly lower levels.
Conclusion: Suboptimal knowledge and attitudes toward PCa screening highlight the need for targeted public health campaigns, workplace education, and rural outreach programs to improve early detection and reduce the burden of PCa.
Keywords: prostate cancer, screening adherence, knowledge, attitude, Saudi Arabia
Introduction
Prostate cancer (PCa) is the second most commonly diagnosed cancer among men worldwide, accounting for approximately 14.2% of new cancer cases in men, according to the Global Cancer Observatory database of the International Agency for Research on Cancer data.1 The incidence of PCa varies widely by geography, with the highest rates reported in high-income countries such as those in North America and Europe, and the lowest rates observed in many African and Southeast Asian countries.2–4 This variation across the countries could be attributed to differences in the readiness and utilization of healthcare facilities and the existence of knowledge and healthcare coverage policies, such as screening.4 Although the exact etiology of PCa is multifactorial, several risk factors have been established, including increasing age, family history, and specific genetic factors (mutations in BRCA1 and BRCA2), as well as lifestyle factors such as smoking and obesity.3,5,6
Similar to several developed countries, the prevalence of PCa is alarming and ranked the second most common cancer among men in the Kingdom of Saudi Arabia (KSA).7,8 The increasing incidence parallels global trends, highlighting the need for effective early detection strategies. In the KSA, recently Alasker A et al analyzed the PCa patients’ data retrospectively and found that more than 30% of the PCa patients presented with metastasis.9 The evidence documented by Alasker A et al indicates an alarming rate of late diagnosis of PCa in this region. Hence, it is critical to diagnose PCa at an early stage through a screening program, so that the patient’s treatment outcomes and quality of life can be significantly improved. Furthermore, this would decrease the healthcare cost associated with the late diagnosis.10,11
In the KSA, all healthcare services at the Ministry of Health (MOH) facilities are provided free of charge.12,13 Although there is no mandatory screening program in the KSA, the MOH encourages screening for PCa for those who are at higher risk of developing PCa.9
Insufficient awareness and poor attitudes towards PCa adversely impact early detection efforts among men. Previous studies from the Middle East and other regions indicate that a sizable proportion of men had less desirable knowledge of the PCa risk, symptoms, and the importance of early diagnosis.14–16 For example, a study by Maladze A et al in 2023 demonstrated that about two-thirds of their participants who were older than 40 years had inadequate awareness of PCa. Even though their study showed that a majority of the participants had an overall positive attitude, some critical domains of attitude, such as the benefits of treatment, had poor attitudes.17 In 2022, Jarb AF et al evaluated the awareness of Saudi men in Western cities and found that only about 11% of them had good knowledge.16 Another Saudi study that was carried out among the general male population reported that about 55% had good knowledge and attitude.18 Furthermore, there are cultural barriers and misconceptions about PCa screening, which will also limit early health-seeking behaviors among Saudi males. Numerous patients are afraid of receiving a diagnosis, making certain conclusions about the results of the test, and not trusting healthcare organizations.15
These existing knowledge gaps and a lack of sufficient awareness regarding PCa are very much critical in PCa screening program uptake among high-risk populations. Advances in prostate cancer diagnostics, including multiparametric MRI and refined clinical predictors, have improved early detection. However, these benefits can only be realized if men are aware of the need for screening and actively seek evaluation.19 Additionally, ongoing assessment of men’s awareness and attitude toward PCa is essential for policymakers to plan for the appropriate strategies that include targeted interventions. This is essential to improve awareness and reshape attitudes towards PCa screening. However, we did not find adequate studies in this region, especially in northern Saudi Arabia. Therefore, the present study aimed to assess the knowledge and attitudes of northern Saudi males towards PCa and its screening. Additionally, we determined the predictors that are associated with the participants’ knowledge and attitude.
Materials and Methods
Study Design and Setting
We used a cross-sectional study design. The present study was conducted from January 2025 to May 2025 at various public places in two regions of northern Saudi Arabia (Arar and Aljouf). The public places included were public parks, mosques, and malls.
Inclusion and Exclusion Criteria
The present study included all male Saudi participants aged 40 to 65 years who belonged to these two regions. We excluded those who were unwilling, mentally unstable, and already screened or diagnosed PCa patients.
Sample Size Estimation
The present study used an online sample size calculator to estimate the sample size.20 This online calculator follows the same principles as the WHO sample size formula (n = z²pq / e²). Here, the minimum eligible participants (n) were determined with 95% confidence intervals, n =1.96, expected proportion (p) = 54.7% (0.547), q = 0.453 (1-p), and margin of error (e) = 5%. This expected proportion (p) was derived from a study by Shaqran T M et al.18 Hence, we concluded that the minimum number of eligible male participants required was 381.
Recruitment Strategies
The present study employed a convenience sampling method to recruit the eligible participants. In this method, eligible participants were invited from public places according to the data collection time and participant availability. Data collectors approached individuals in locations such as parks, malls, and community centers, briefly explained the study, and invited eligible males to participate on the spot. Participation was voluntary and based on immediate availability.
Ethical Considerations
The study was conducted in accordance with the principles outlined in the Declaration of Helsinki. After obtaining ethical approval and other necessary clearances from the relevant authorities (IRB of Jouf University, approval no. 11/3/46, dated January 29, 2025), the data collection process was initiated. Informed consents were secured from all participants prior to data collection, ensuring that they understood the purpose of the study and their right to withdraw at any time without consequence. Confidentiality was maintained throughout the research process, with data anonymized to protect participants’ identities.
Data Collection Tool
We used a structured Arabic version of the questionnaire that was prepared by the research team after a focus group discussion with the experts from public health, pathology, and urology departments (content validity). During the focus group discussion, we produced and discussed the items based on existing evidence from open-source research studies.16,17,21 The participants had to respond to the data collection tool through a Google form on their personal devices, which was prepared according to the approved LCBE documents. Originally, the questionnaire was developed in English. However, we made standard protocols to get the final Arabic version of the tool.22,23 This tool was tested in the pilot study among 32 eligible males to check face validity and cultural suitability. The pilot study analysis explored acceptable Cronbach’s alpha values of 0.84 for the knowledge section and 0.79 for the attitude section. These values indicate a high level of internal consistency, suggesting that the items within each section reliably measure the intended constructs. The tool consisted of three sections. The first section inquired about background characteristics of the study participants, such as age, region, income, occupation, etc.
Scoring and Categorization of Knowledge and Attitude
The second section consisted of 10 questions related to knowledge. The participants must respond with “yes”, “no”, or “not sure”. The wrong answers and the not-sure answers were marked as 0 points, and the correct responses were marked as 1 point. In the attitude section, the responses will be recorded in a 5-point Likert’s scale format, in which the participants responded from strongly agree to strongly disagree. We scored the attitude section responses on a scale from 1 (strongly disagree) to 5 (strongly agree). The research team gave reverse scoring for the negatively phrased questions. The total scores in knowledge and attitude were computed and categorized according to Bloom’s criteria as low (≤ 60% of the total score), medium (60–79%), and high (≥ 80%). This approach was selected because Bloom’s cutoffs provide a standardized method to convert raw scores into meaningful ordinal categories, allowing for better comparability with previous KAP studies and facilitating logistic regression analysis. Categorizing scores into three distinct levels also helps identify target groups for public health interventions by distinguishing participants with clearly inadequate knowledge or attitudes from those who are partially informed or fully knowledgeable.24,25
Data Analysis
We used the Statistical Package of Social Sciences (SPSS, V.23) for coding, analysis, and report generation. Descriptive statistics summarized demographic characteristics, knowledge levels, and attitudes toward prostate cancer screening. The Spearman correlation (non-parametric) test was applied to find the eligible males’ knowledge and attitude towards PCa and its screening. This test was chosen as PCa knowledge and attitude scores were skewed. We performed binary logistic regression to find the predictors that are associated with the participants’ knowledge and attitude. For regression analysis, we dichotomized each outcome as High = 1 and Low/Medium = 0. The following categories were used as reference groups: age (45–55 years), marital status (currently married), education (university and above), income (≤10,000 SAR), occupation (government sector), residence (city), smoking (non-smoker), and family history of PCa (no). We used the enter method in the logistic regression model. All selected independent variables were entered into the model simultaneously to assess their individual contributions while controlling for the effects of other variables. A p-value less than 0.05 was considered statistically significant.
Results
We approached 431 eligible males during the data collection process to obtain the minimum number of participants for the survey (response rate = 88.4%). Of the 381 participants, 50.7% belonged to the 45- to 55-year age group (mean ± SD = 55.18 ± 9.2). The majority were currently married (82.2%), falling in the income group of 5000 to 10000 SAR (1 USD = 3.75 SAR), working in the private sector (36.2%), living in cities (60.9%), non-smokers (70.1%), and had no family history of PCa (91.1%) (Table 1).
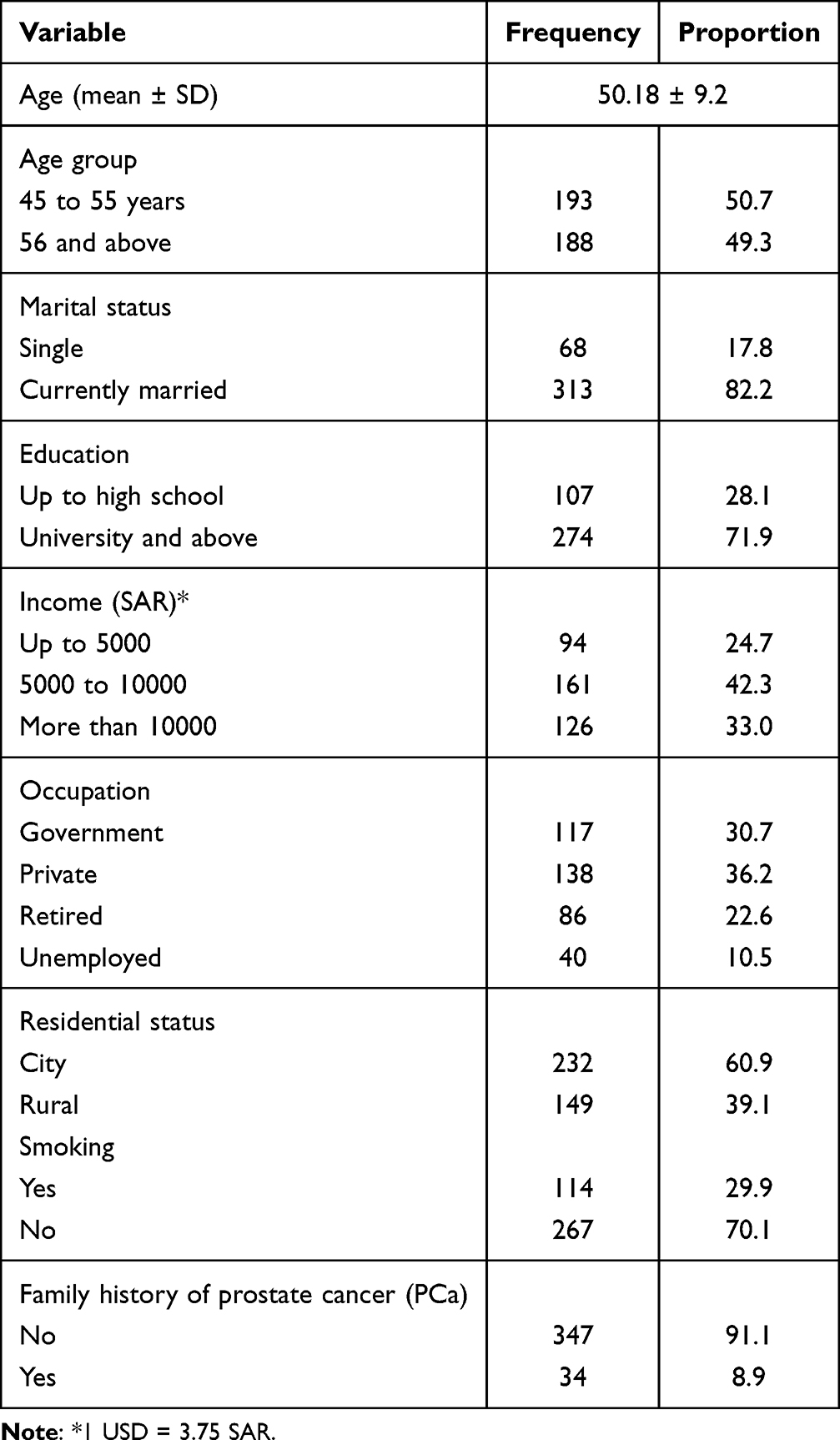 |
Table 1 Background Characteristics of the Patients (N= 381) |
Regarding participants’ knowledge of PCa and its screening, the highest proportion of correct answers was noted in “healthy lifestyle reduces PCa risks (66.7%)”, followed by “high-risk age groups (55.6%)”, and smoking is a risk factor (54.3%). The participants responded with the highest proportion of wrong answers in PCa always causes symptoms in the early stage (68.8%) (Table 2).
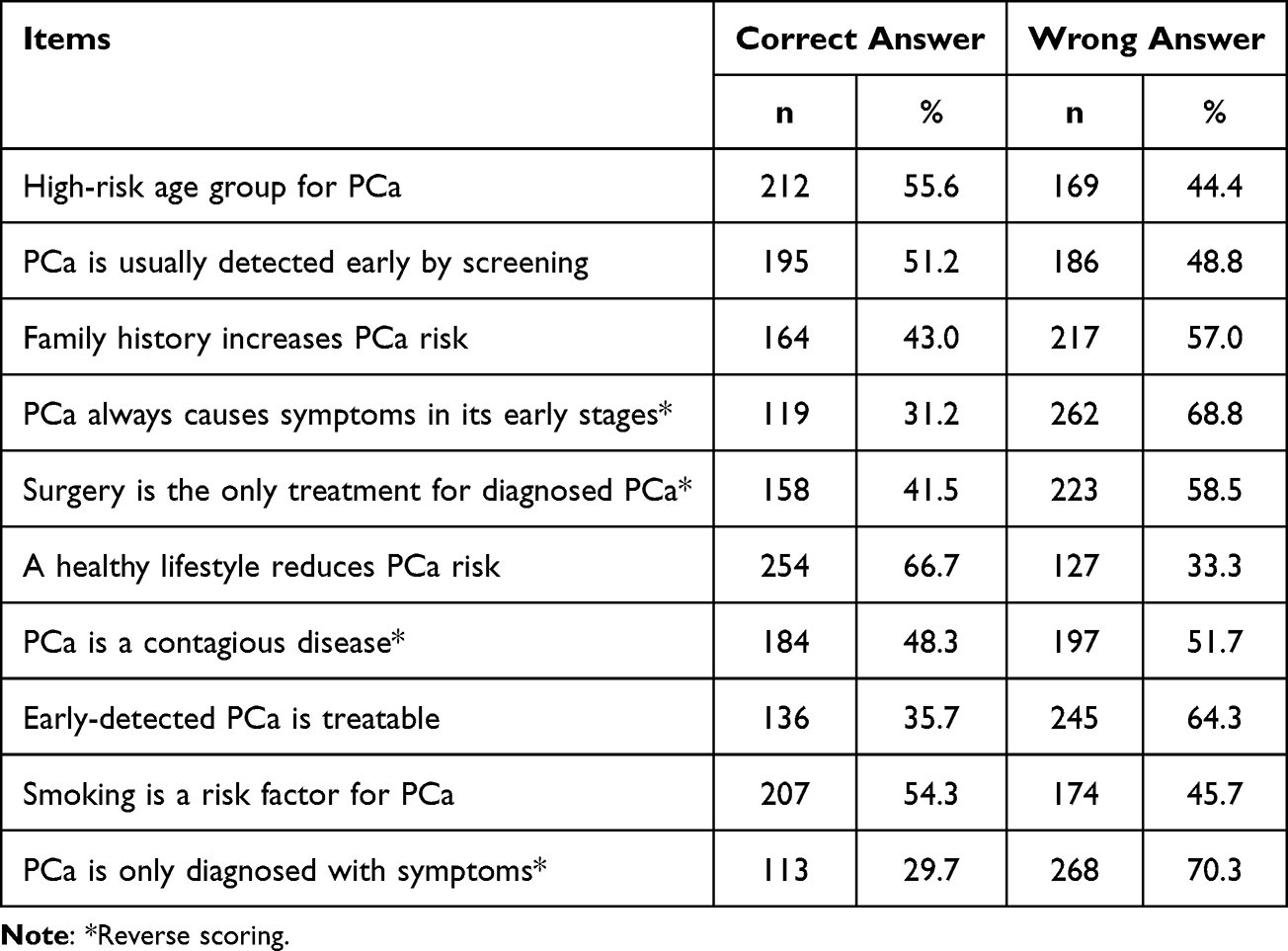 |
Table 2 Participants’ Responses in the Knowledge Category (N= 381) |
Regarding participants’ attitude, the highest promotion of agreement was observed for the statement, “I am confident that I know enough about PCa to make informed decisions about screening (overall = 69.1%, strongly agree = 26.8%, agree = 42.3%)” and “I would be willing to undergo PCa screening if recommended by my doctor (overall = 65.8%, strongly agree = 34.6%, agree = 31.2%)” (Table 3).
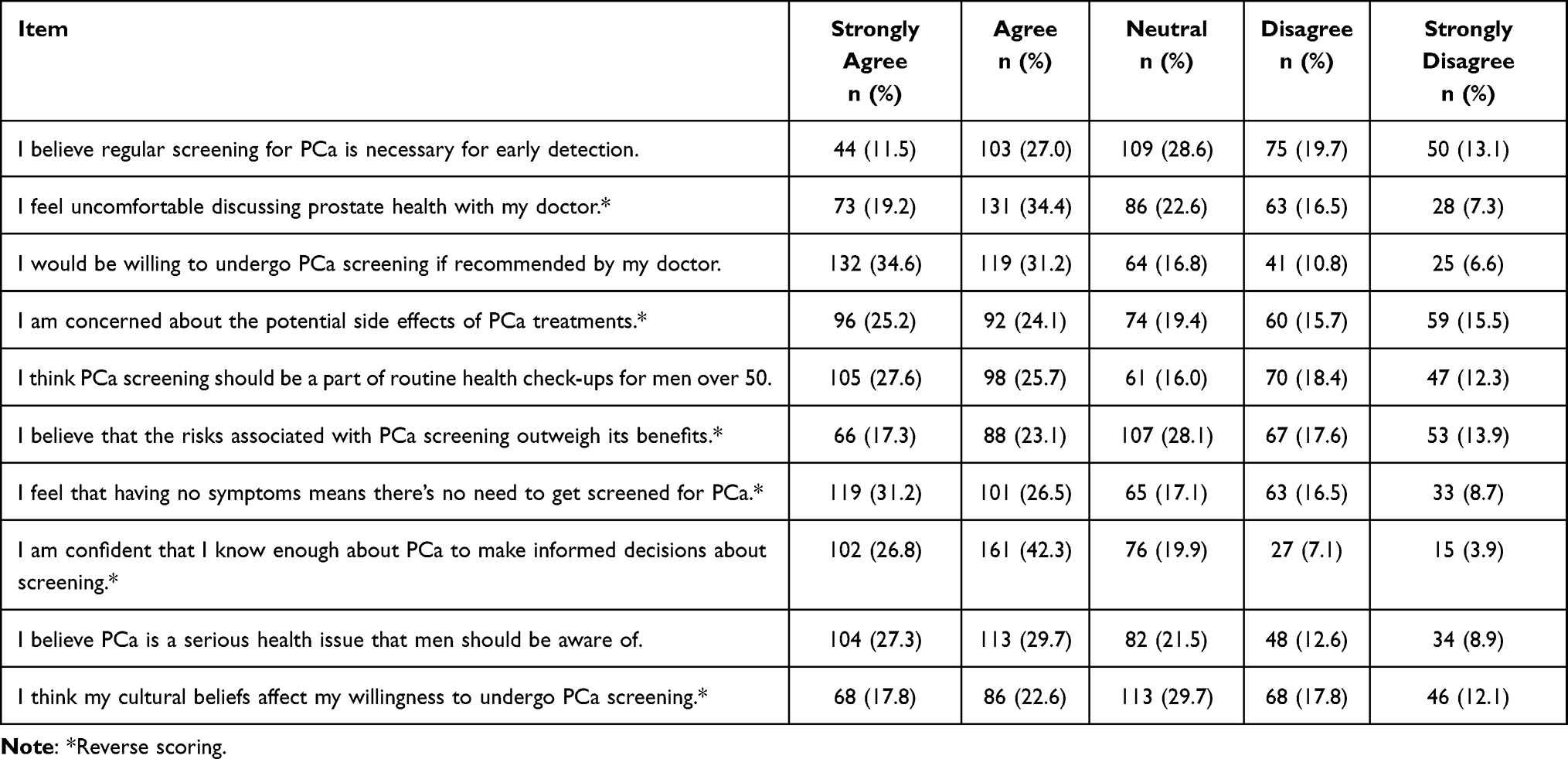 |
Table 3 Participants’ Responses in the Attitude Section (n = 381) |
Of the 381 participants, 23.1% had low, 39.9% had medium, and 37.0% had high levels of knowledge towards PCa. Regarding attitude, 18.4% had low, 34.1% had medium, and 47.5% had high levels of attitude towards PCa and its screening (Figure 1). The Spearman correlation test revealed a positive and significant correlation between knowledge and attitude (rho = 0.609, p = 0.001) (Table 4). Furthermore, a scatter plot showing the positive correlation between knowledge and attitude scores toward prostate cancer screening among participants is presented in Figure 2.
 |
Table 4 Spearman Correlation Analysis Between Knowledge and Attitude |
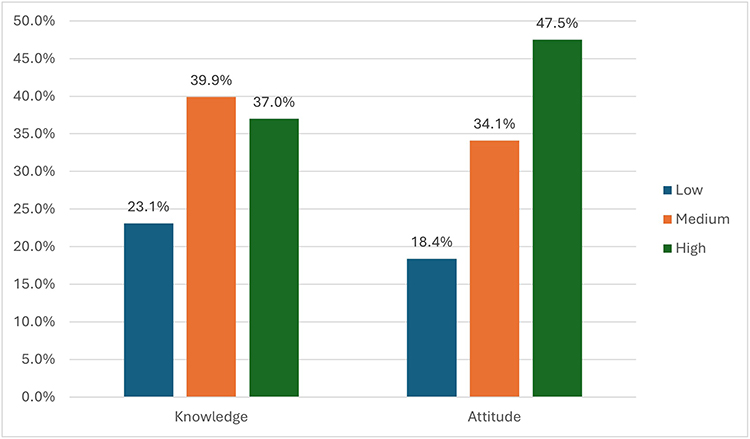 |
Figure 1 Distribution of Knowledge and Attitude Levels toward Prostate Cancer Screening among Participants (n = 381). Low = ≤60%, Medium = 61–79%, High = ≥80% (Bloom’s criteria). |
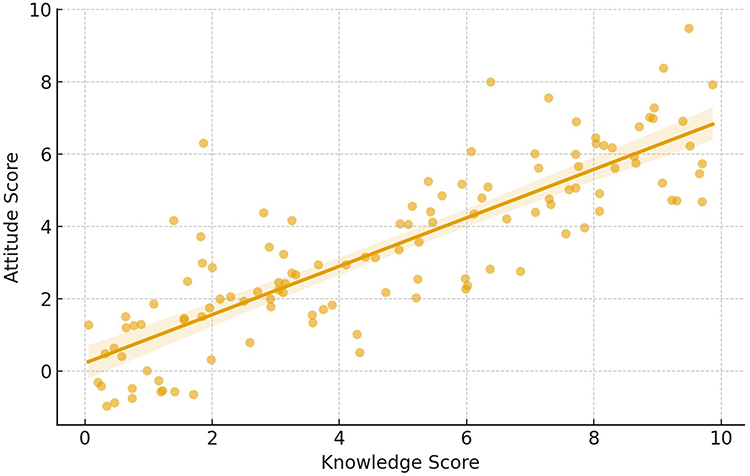 |
Figure 2 Scatter plot showing the positive correlation between knowledge and attitude scores toward prostate cancer screening among participants (n = 381). |
Through the binary logistic regression, after adjusting with the independent variables, we found that knowledge was significantly higher among those working in the private sector (ref: government sector, adjusted odds ratio (aOR) = 2.79, 95% confidence interval (CI) = 1.63–4.22, and p = 0.003) and had a family history of PCa (ref: no family history, aOR = 2.11, 95% CI = 1.75–2.81, and p = 0.017). Significantly lower levels of knowledge are observed in people aged above 55 years (ref: 45 to 55 years, aOR = 0.78, 95% CI = 0.53–0.91, and p = 0.009) and those who live on the rural side (ref: live in the city, aOR = 0.53, 95% CI = 0.27–0.81, and p = 0.007) (Table 5).
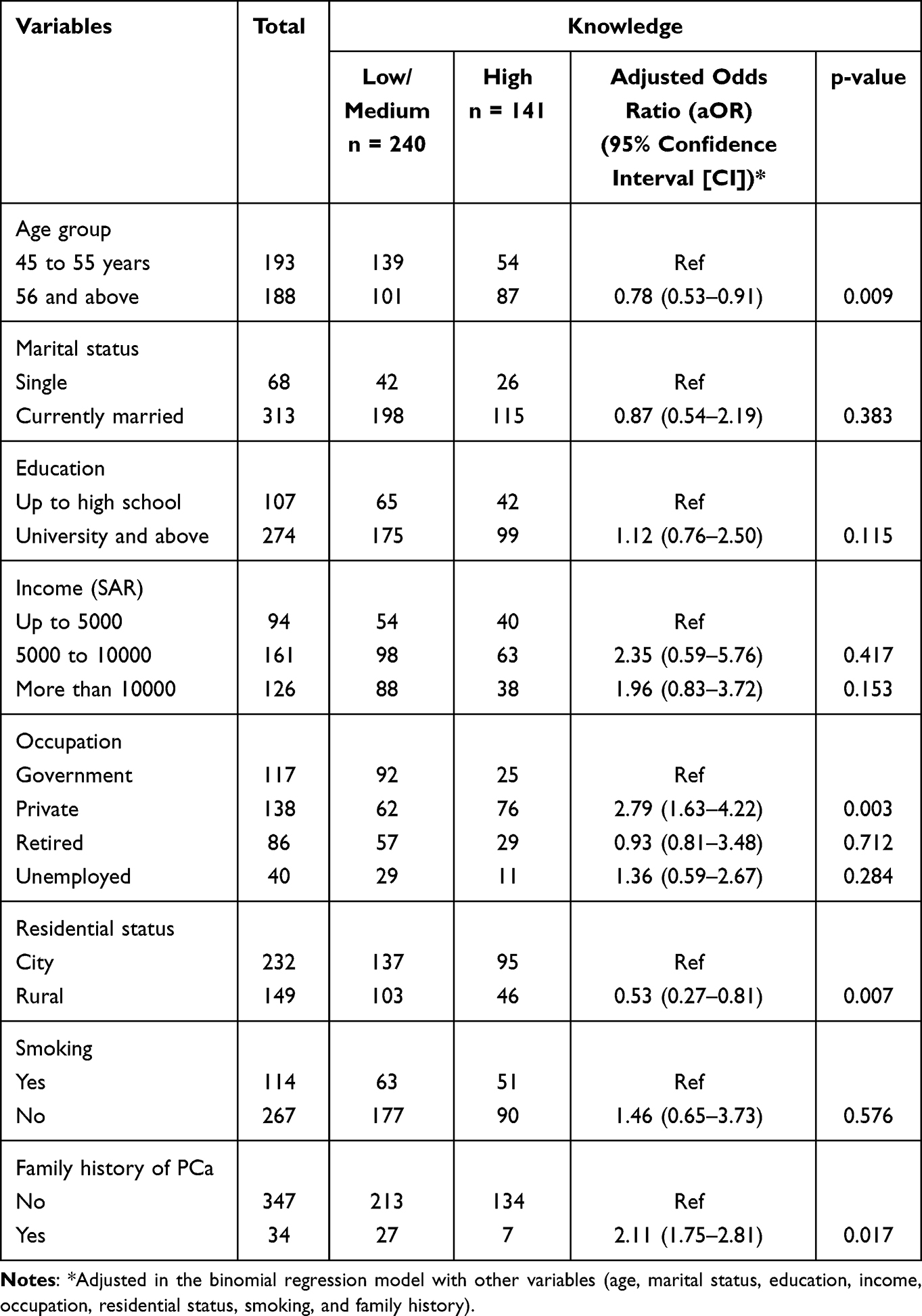 |
Table 5 Binary Logistic Regression Analysis of Knowledge Towards PCa Risk Factors and Screening (n = 381) |
Regarding attitude, we found that smokers (ref: non-smokers, aOR = 0.48, 95% CI = 0.27–0.62, and p = 0.001) and those who live on the rural side (ref: live in the city, aOR = 0.59, 95% CI = 0.44–0.81, and p = 0.004) had significantly lower levels (Table 6).
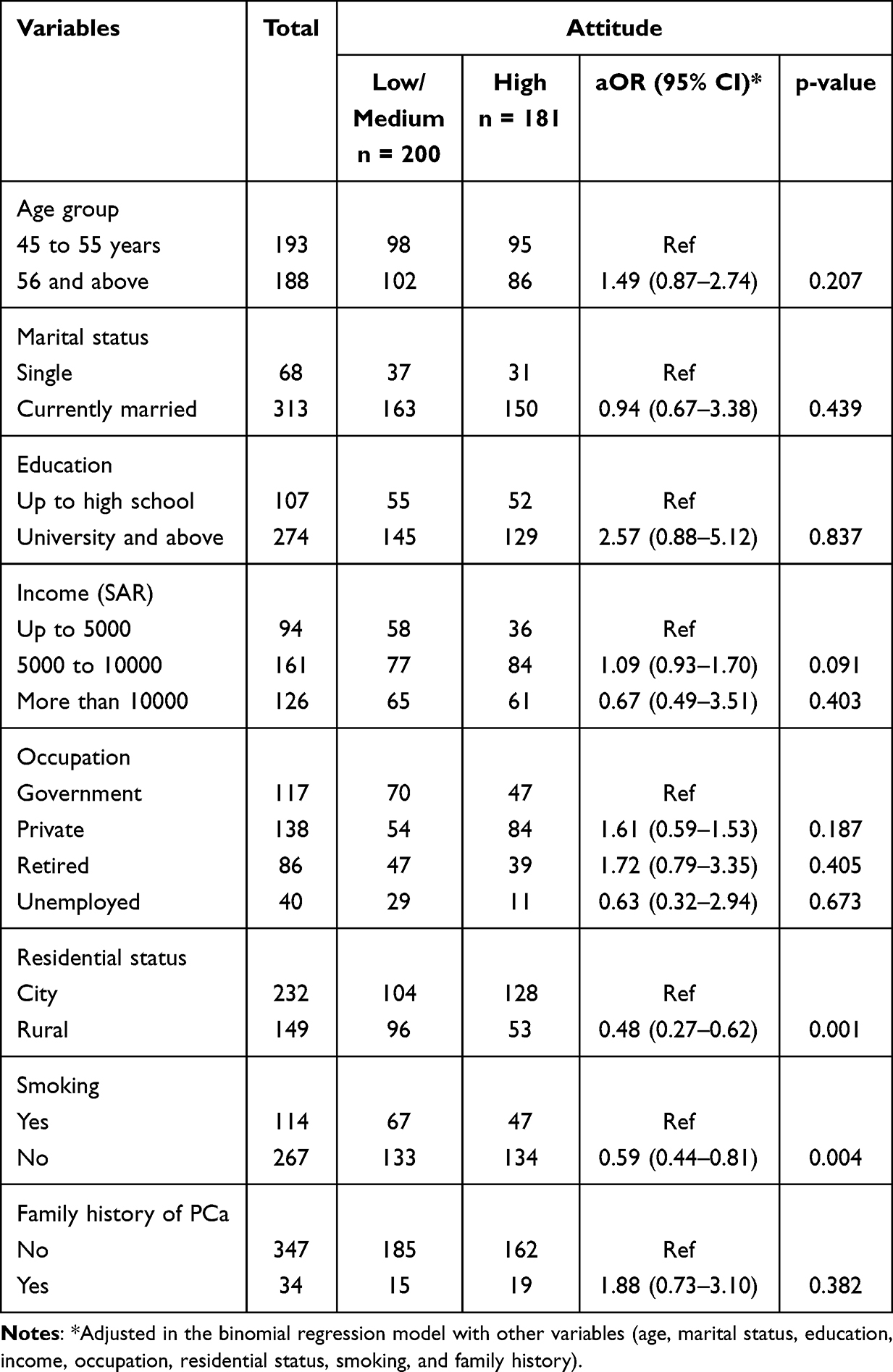 |
Table 6 Binary Logistic Regression Analysis of Attitude Towards PCa Risk Factors and Screening |
Discussion
PCa, being one of the predominant cancer types among Saudi men and among males worldwide, sufficient awareness is a pivotal factor in early detection and reducing mortality rates. The present study assessed the northern Saudi males’ knowledge and attitude towards PCa and its screening.
Knowledge Level Regarding PCa
Despite the advancements in healthcare and information distribution, the present study results indicate that a substantial proportion of eligible northern Saudi males still have low or medium knowledge of PCa and its screening. This finding highlights potential barriers to health education and awareness in this population.
The proportion of adequate and inadequate knowledge varies across the studies from different countries and within KSA.17,21,26,27 A survey by Maladze N et al in South Africa stated that more than 60% of their participants had insufficient awareness of PCa.17 Another study by Morlando M et al conducted in a European country, reported a moderate level of knowledge of PCa among its participants.27 Interestingly, Musalli ZF et al have shown that more than 60% of their participants had adequate knowledge of PCa.26 These variations may reflect differences in sociocultural and demographic profiles, as well as in the data collection tools used. For example, Musalli ZF et al conducted a study in the capital city of KSA.
To address these gaps, tailored regional-specific public health efforts, such as mobile health awareness campaigns and teleservices, are required, especially in rural settings.
Predictors of Knowledge
In this study, the older population demonstrated a lower level of knowledge than younger people. Other factors associated with a higher-level awareness of PCa and its screening methods were work setting and family history. The finding that older participants had significantly lower knowledge is particularly concerning, as advancing age is the primary risk factor for PCa. This gap may be partly explained by lower digital literacy among older adults, limiting their exposure to online health information campaigns, as well as cultural stigma or fatalistic beliefs about cancer that reduce interest in screening.28,29 Similar to the present study, Maladze N et al found a negative association between age and PCa awareness.17 In contrast to the present study, some studies have not fond an association with the age of the participants, and those studies found a significant association with other sociodemographic characteristics, including education and marital status.30,31 Higher awareness among private-sector employees may be attributed to increased exposure to corporate wellness programs, periodic health check-ups, and health campaigns offered as employee benefits. This is supported by evidence that workplace wellness programs in Saudi Arabia improve general health behaviors.32 This group also tends to be younger, more urban, and more educated, which may partly account for their higher knowledge. Differences in health insurance coverage and occupational health initiatives between sectors could further contribute to this disparity. Similarly, those with a family history of prostate-related problems are more likely to be more aware as a result of their own experiences or referred to counseling by their healthcare providers.
Previous studies regarding this variable support our research findings.33,34 It is crucial to note that knowledge of PCa was significantly lower among individuals from rural areas compared to those in urban settings. Similarly, Musalli ZF et al26 and Ariyo DA et al35 found a higher knowledge among their participants from urban settings.
To reach the many rural communities, outreach programs should include mobile health units designed to travel to these sites, such as, community leaders, and local health workers to provide prostate cancer education and screening services. Furthermore, campaigns need to consider the literacy level of their target audience, which means relying on visual aids, storytelling, and other means to convey health education messages.
Attitude Toward PCa Screening
A higher proportion of participants demonstrated a high-level attitude compared to those with high knowledge. Still, a considerable proportion of males had either a low or medium attitude toward PCa and uptake of PCa screening. Similar to the variations in the proportion of different knowledge categories, the attitudes also vary in various settings. Some studies have shown high levels of positive attitude and perceptions, and others have shown inadequate levels of attitude.33,35–37
Predictors of Attitude
We found that attitudes toward PCa and its screening were lower among those in rural areas and smokers. The lower attitudes observed among rural participants may reflect disparities in health literacy and access to primary care services, which are more concentrated in urban areas. These findings add further evidence that health-related attitudes are influenced by sociodemographic and lifestyle factors. Similar barriers may also affect knowledge, as lower attitudes among rural populations may derive from less access to healthcare resources, less exposure to health promotion campaigns, and existing cultural norms that discourage proactive health-seeking behaviors. However, smoking status may be associated with lower attitudes, at least in part, a result of a complicated interplay between behavioral and psychological factors. Smoking is often related to risk-taking behavior and lower priority in the prevention of healthcare.38,39
Prostate cancer awareness should be integrated with overall smoking cessation programs for smokers, according to public health campaigns. Addressing PCa screening and smoking at the same time can foster healthier behaviors while changing attitudes. Integrating PCa awareness into other existing national programs, such as chronic disease clinics and wellness initiatives, could efficiently reach high-risk groups and maximize resources. Strengthening rural outreach, mobile health units, and community-based education is essential to bridging this gap and aligns with the goals of Vision 2030 to reduce health inequities. Collaboration with community leaders, mosques, and local media may enhance trust and participation in screening efforts. Together, these strategies could contribute to earlier detection, improved treatment outcomes, and reduced burden on the healthcare system.
Correlation Between Knowledge and Attitude
Our study demonstrated a strong positive correlation between knowledge and attitude scores, indicating that participants with better knowledge are also more likely to have favorable attitudes toward PCa screening.
This finding underscores the importance of health education campaigns, as improving knowledge may simultaneously improve attitudes and increase willingness to participate in screening programs. Similar associations have been reported in previous KAP studies, supporting the link between awareness and health-seeking behavior.31,40
Even though we conducted this study on a unique population on essential health issues using a standardized and validated questionnaire, Readers of this study should consider the following limitations:
- This epidemiological study was conducted in two regions of KSA. Due to varying sociodemographic profiles in the country, it is difficult to generalize the findings.
- The present study revealed the association between certain variables with knowledge and attitudes. But cannot establish the temporal or causal relationship.
- Due to the nature of the study methods, we could not evaluate the qualitative component of the participants’ knowledge and attitudes towards PCa.
- As this study used convenience sampling at public places, selection bias cannot be excluded, and the findings may not fully represent all northern Saudi males.
Conclusion
This study revealed that a sizable proportion of Northern Saudi males had either low or medium levels of knowledge and attitudes toward PCa and its screening, with a positive correlation between knowledge and attitude. Tailored regional-specific public health efforts, such as mobile health awareness campaigns and teleservices, are required to address these gaps, especially in rural settings. Integrating PCa awareness with broader smoking cessation initiatives can enhance early detection efforts and align with comprehensive cancer control strategies. Moreover, we recommend evaluating the qualitative aspects associated with the participants’ understanding of PCa through a multi-region mixed-method survey. Future initiatives should also focus on involving primary healthcare providers, community pharmacists, and religious/community leaders to improve trust and participation in screening programs. These strategies may help bridge inequities in cancer care and support Saudi Arabia’s Vision 2030 goals for improving population health.
Funding
This work was funded by the Deanship of Graduate Studies and Scientific Research at Jouf University under grant No. (DGSSR-2024-01-01032).
Disclosure
The authors report no conflicts of interest in this work.
References
1. GLOBOCAN–IARC. Statistics at a glance, 2022 Top 5 most frequent cancers. 2023 [cited September 13, 2025]. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/900-world-fact-sheet.pdf?utm_source=chatgpt.com.
2. Giona S. The Epidemiology of Prostate Cancer. In: Bott SRJ, Ng KL, editors. Prostate Cancer. Brisbane (AU): Exon Publications; 2021.
3. Bergengren O, Pekala KR, Matsoukas K, et al. 2022 update on prostate cancer epidemiology and risk factors-a systematic review. Eur Urol. 2023;84(2):191–206. doi:10.1016/j.eururo.2023.04.021
4. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
5. Berenguer CV, Pereira F, Câmara JS, Pereira JAM. Underlying features of prostate cancer-statistics, risk factors, and emerging methods for its diagnosis. Curr Oncol. 2023;30(2):2300–2321. doi:10.3390/curroncol30020178
6. Junejo NN, AlKhateeb SS. BRCA2 gene mutation and prostate cancer risk. Comprehensive review and update. Saudi Med J. 2020;41(1):9–17. doi:10.15537/smj.2020.1.24759
7. Althubiti M, Eldein MMN. Trends in the incidence and mortality of cancer in Saudi Arabia. Saudi Med J. 2018;39(12):1259–1262. doi:10.15537/smj.2018.12.23348
8. Bandar M. Prostate cancer in Saudi Arabia: trends in incidence, morphological and epidemiological characteristics. Int J Res Med Sci. 2020;8(11):3899–3904. doi:10.18203/2320-6012.ijrms20204559
9. Alasker A, Arabi TZ, Alghafees MA, et al. Prostate cancer among Saudis: a registry review. Ann Med Surg Lond. 2024;86(1):56–61. doi:10.1097/MS9.0000000000001448
10. Mujamammi AHA, Sabi EM, Zawawi BA, et al. The relevance of prostate cancer screening among Saudi men attending outpatient clinics of tertiary-care hospitals in Riyadh, Saudi Arabia. Imam J Applied Sci. 2021;6(1):11–16. doi:10.4103/ijas.ijas_10_21
11. Grossman DC, Curry SJ, Owens DK, et al. Screening for prostate cancer: US preventive services task force recommendation statement. JAMA. 2018;319(18):1901–1913. doi:10.1001/jama.2018.3710
12. Gurajala S. Healthcare system in the Kingdom of Saudi Arabia: an expat doctor’s perspective. Cureus. 2023;15(5):e38806. doi:10.7759/cureus.38806
13. Nair KS, Mughal YH, Albejaidi F, Alharbi AH. Healthcare financing in Saudi Arabia: a comprehensive review. Healthcare. 2024;12(24):2544. doi:10.3390/healthcare12242544
14. Sayan M, Eren AA, Tuac Y, et al. Prostate cancer awareness in the middle east: a cross-sectional international study. JCO Glob Oncol. 2024;10:e2400171.
15. Arafa MA, Rabah DM. With increasing trends of prostate cancer in the Saudi Arabia and Arab world: should we start screening programs? World J Clin Oncol. 2017;8(6):447. doi:10.5306/wjco.v8.i6.447
16. Jarb AF, Aljuaid AK, Alghamdi SM, Almathami AA, Altawili A, Alesawi A. Awareness about prostate cancer and its screening in medina, jeddah, and makkah, Saudi Arabia population. Urol Ann. 2022;14(1):27–32. doi:10.4103/ua.ua_113_21
17. Maladze N, Maphula A, Maluleke M, Makhado L. Knowledge and attitudes towards prostate cancer and screening among males in Limpopo province, South Africa. Int J Environ Res Public Health. 2023;20(6):5220. doi:10.3390/ijerph20065220
18. Shaqran TM, Alanazi RM, Haider AM, et al. Knowledge and awareness of screening for prostate cancer risk factors and symptoms among the general population in Tabuk City, Saudi Arabia. Cureus. 2023;15(10):e46472. doi:10.7759/cureus.46472
19. Massanova M, Vere R, Robertson S, et al. Clinical and prostate multiparametric magnetic resonance imaging findings as predictors of general and clinically significant prostate cancer risk: a retrospective single-center study. Curr Urol. 2023;17(3):147–152. doi:10.1097/CU9.0000000000000173
20. Calculator net Sample Size Calculator. 2024 [cited January 15, 2024]. Available from: https://www.calculator.net/sample-size-calculator.html.
21. Makungu ML, Mweya CN. Assessing knowledge, attitude and practice towards prostate cancer screening among males in Southwest Tanzania: a cross-sectional study. Cancer Treat Res Commun. 2023;36:100716. doi:10.1016/j.ctarc.2023.100716
22. Tsang S, Royse CF, Terkawi AS. Guidelines for developing, translating, and validating a questionnaire in perioperative and pain medicine. Saudi J Anaesth. 2017;11(Suppl 1):S80–s9. doi:10.4103/sja.SJA_203_17
23. McIlvenny S, Ahmed MH, Dunn E, Swadi H, Balshie M. The translation into Arabic and revalidation of a fatigue questionnaire. East Mediterr Health J. 1999;5(3):503–514. doi:10.26719/1999.5.3.503
24. Thirunavukkarasu A, Al-Hazmi AH, Dar UF, et al. Knowledge, attitude and practice towards bio-medical waste management among healthcare workers: a northern Saudi study. PeerJ. 2022;10:e13773.
25. Alzahrani MM, Alghamdi AA, Alghamdi SA, Alotaibi RK. Knowledge and attitude of dentists towards obstructive sleep apnea. Int Dental J. 2022;72(3):315–321. doi:10.1016/j.identj.2021.05.004
26. Musalli ZF, Alobaid MM, Aljahani AM, Alqahtani MA, Alshehri SS, Altulaihi BA. Knowledge, attitude, and practice toward prostate cancer and its screening methods among primary care patients in King Abdulaziz Medical City, Riyadh, Saudi Arabia. Cureus. 2021;13(4):e14689. doi:10.7759/cureus.14689
27. Morlando M, Pelullo CP, Di Giuseppe G. Prostate cancer screening: knowledge, attitudes and practices in a sample of men in Italy. A survey. PLoS One. 2017;12(10):e0186332. doi:10.1371/journal.pone.0186332
28. Nutakor J, Zhou L, Larnyo E, Addai-Dansoh S. The impact of digital health literacy on cancer prevention behaviors among older. Innov Aging. 2024;8(Suppl 1).
29. Paillaud E, Galvin A, Doublet S, et al. Health literacy and the use of digital tools in older patients with cancer and their younger counterparts: a multicenter, nationwide study. Patient Educ Couns. 2025;130:108420. doi:10.1016/j.pec.2024.108420
30. Alothman AM, Altamimi AF, Alhenaki AW, Almansour NM, Alhusaini AK, Alateeq F. The knowledge and attitude towards prostate cancer and screening practices among males in Saudi Arabia. J Family Med Primary Care. 2022;11(6):2637–2642. doi:10.4103/jfmpc.jfmpc_1802_21
31. Elyas A, Mahfouz MS, Suwaydi AZA, et al. Prostate cancer knowledge and attitude toward screening practices among men 40 and over in the Jazan Region, Saudi Arabia. J Cancer Epidemiol. 2024;2024(1):2713372. doi:10.1155/2024/2713372
32. Altwaijri Y, Hyder S, Bilal L, et al. Evaluating the impact of a workplace wellness program in Saudi Arabia: an intra-department study. J Occup Environ Med. 2019;61(9):760–766. doi:10.1097/JOM.0000000000001656
33. Gift S, Nancy K, Victor M. Assessment of knowledge, practice and attitude towards prostate cancer screening among male patients aged 40 years and above at Kitwe Teaching Hospital, Zambia. African J Urol. 2020;26(1):70. doi:10.1186/s12301-020-00067-0
34. Baobaid MF, Abdalqader MA, Ghazi HF, Shebl H, Abdalrazak HA. The study of knowledge, attitude and practice of prostate cancer prevention and its Relationship with socio-demographic characteristics among men at ppr lembah subang 1, Selangor, Malaysia. Malaysian J Med Health Sci. 2020;16(7).
35. Ariyo D, Abiodun O, Daramola O, Ikeh I, Babalola N. Assessment of knowledge and perception on prevention of prostate cancer among male staff in achievers University, Owo, Ondo State. Western Nigeria J Medl Sci. 2024;7(1):42–52.
36. Onyeodi I, Akintelure S, Oladipo A, Fashola T. Knowledge, attitude and screening practices of prostate cancer among men in an urban community in Lagos, Nigeria. J Community Med Primary Health Care. 2022;34(3):82–97. doi:10.4314/jcmphc.v34i3.7
37. Alqudah MAY, Al-Samman R, Matalgah O, Abu Farhah R. Early detection of prostate cancer: self-reported knowledge and attitude of physicians in Jordan. Inquiry. 2022;59:469580221095822. doi:10.1177/00469580221095822
38. Celebi C, Calik-Kutukcu E, Saglam M, Bozdemir-Ozel C, Inal-Ince D, Vardar-Yagli N. Health-promoting behaviors, health literacy, and levels of knowledge about smoking-related diseases among smokers and non-smokers: a cross-sectional study. Tuberc Respir Dis. 2021;84(2):140–147. doi:10.4046/trd.2020.0158
39. Li C, Sun J. The impact of current smoking, regular drinking, and physical inactivity on health care-seeking behavior in China. BMC Health Serv Res. 2022;22(1):52. doi:10.1186/s12913-022-07462-z
40. Alenezi AM, Thirunavukkarasu A, Wani FA, et al. Female healthcare workers’ knowledge, attitude towards breast cancer, and perceived barriers towards mammogram screening: a multicenter study in North Saudi Arabia. Curr Oncol. 2022;29(6):4300–4314. doi:10.3390/curroncol29060344
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitude, Perceived Responsibilities, and Associated Factors Regarding Colostomy Care Among Nurses Working in Surgical Units at Amhara Region General and Referral Hospitals, Ethiopia: A Mixed Method Study
Tiruneh TE, Alem G, Taddele M, Tizazu ZM, Minale FK, Alemu KD
Nursing: Research and Reviews 2022, 12:191-206
Published Date: 13 October 2022
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Gebremichael MA, Lema TB
International Journal of Women's Health 2023, 15:1383-1395
Published Date: 4 September 2023
Dermatologists’ Knowledge, Attitude, and Practice Pattern Toward Low-Dose Oral Minoxidil in Hair Loss in Saudi Arabia
Altalhab S
Clinical, Cosmetic and Investigational Dermatology 2024, 17:653-662
Published Date: 15 March 2024
Knowledge, Attitude and Practice Towards Hepatitis B Infection and HBV Vaccine Among the Healthy Population in Makkah, Saudi Arabia
Almalki F, Alraffah YM, Alasiri RA, Dhafar MW, Albogami FM, Alhazmi MN, Alyazidi AM, Alharbi LA, Alotaibi ME
Infection and Drug Resistance 2025, 18:2153-2164
Published Date: 28 April 2025