Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Bridging Clinical Trials to Real-World Clinical Practice: TCHP Neoadjuvant Therapy Outcomes in HER2-Positive Breast Cancer
Authors Sharaf B ![]() , Seif A, Bani Hani H, Alhasan M, Khader R, Al-Yag'oub M, Ghanem A
, Seif A, Bani Hani H, Alhasan M, Khader R, Al-Yag'oub M, Ghanem A ![]() , Bani Ata J, Ajlouni B, Jawarneh Q
, Bani Ata J, Ajlouni B, Jawarneh Q ![]() , Jaffal A
, Jaffal A ![]() , Tamimi F
, Tamimi F ![]() , Jehad S, Al-Abdallat H
, Jehad S, Al-Abdallat H ![]() , Mahafdah O, Abdel-razeq H
, Mahafdah O, Abdel-razeq H ![]()
Received 26 August 2025
Accepted for publication 14 March 2026
Published 9 April 2026 Volume 2026:18 559555
DOI https://doi.org/10.2147/BCTT.S559555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Harikrishna Nakshatri
Baha Sharaf,1 Alaa Seif,2 Hira Bani Hani,1 Maha Alhasan,1 Rnad Khader,1 Maram Al-Yag’oub,1 Ameed Ghanem,1 Jinan Bani Ata,1 Batool Ajlouni,1 Qutaiba Jawarneh,1 Adel Jaffal,1 Faris Tamimi,1 Sharif Jehad,3 Haneen Al-Abdallat,4 Osama Mahafdah,1 Hikmat Abdel-razeq1,4
1Internal Medicine Department, King Hussein Cancer Center, Amman, Jordan; 2Surgical Department, King Hussein Cancer Center, Amman, Jordan; 3School of Medicine, Yarmouk University, Irbid, Jordan; 4School of Medicine, The University of Jordan, Amman, Jordan
Correspondence: Hikmat Abdel-razeq, Department of Internal Medicine, King Hussein Cancer Center, 202 Queen Rania Al Abdullah Street P.O. Box: 1269, Amman, 11941, Jordan, Tel +962-6 5300460, Ext: 1000, Email [email protected]
Purpose: Trastuzumab-based neoadjuvant therapy (NAT) is standard for HER2-positive breast cancer (HER2+ BC). The TCHP regimen (docetaxel, carboplatin, trastuzumab, pertuzumab) demonstrated efficacy in clinical trials; however, real-world evidence remains limited. This study evaluates the effectiveness and safety of TCHP in routine clinical practice at King Hussein Cancer Center (KHCC).
Patients and Methods: This retrospective study included 161 patients with HER2+ BC who received at least one cycle of TCHP between January 2022 and October 2024. The primary endpoint was pathological complete response (pCR; ypT0/is, ypN0). Secondary endpoints included safety, emergency room (ER) visits, and hospitalization rates. Logistic regression was used to identify predictors of pCR, reporting odds ratios (OR) and 95% confidence intervals (CI).
Results: The cohort included 160 females and one male, with a median age of 51 years (24– 80). Most patients were ER/PR-positive (73.9%), and 26.1% were ER/PR-negative. Tumors were predominantly high-grade (grade 3 in 106 patients), with nodal involvement in 95 patients. Surgical resection was performed in 143 patients. pCR was achieved in 45.5% of patients. HER2 IHC 3+ expression (adjusted OR 11.76; 95% CI 3.69– 54.00; p< 0.001) and ER/PR-negative status (adjusted OR 2.59; 95% CI 1.09– 6.50; p=0.035) were independent predictors of pCR, while tumor stage and nodal status, were not. No cardiac toxicity or ejection fraction decline was observed. Anti-HER2 therapy was discontinued in six patients, and 11 did not complete six cycles. Chemotherapy dose reductions occurred in 38 patients, mainly due to hematologic toxicity. A median of three ER visits per patient was recorded, with hospitalization required in 42 patients, primarily for neutropenic fever and diarrhea.
Conclusion: In this real‑world cohort, TCHP achieved a moderate pCR rate (45.5%), lower than clinical trial reports, with HER2 IHC 3+ and ER/PR‑negative status predicting response, but substantial toxicity—including frequent emergency visits and hospitalization, highlighting the need for improved patient selection, strengthened supportive care, and consideration of de‑escalation strategies to maintain efficacy while reducing morbidity.
Keywords: TCHP, HER2-positive breast cancer, neoadjuvant therapy, pCR, real-world evidence
Introduction
HER2-positive breast cancer (HER2+ BC) constitutes 15–20% of all breast cancer cases,1 and is known for its aggressive tumor biology and poor prognosis without targeted therapy.2 The development of trastuzumab, a monoclonal antibody targeting HER2, has completely revolutionized the treatment for HER2+ BC patients, with dramatic improvement treatment outcomes.3 Further progress was achieved with the addition of pertuzumab to trastuzumab and cytotoxic chemotherapy, demonstrating improved overall survival in patients with HER2-positive metastatic BC.4,5 This combination has been validated in numerous clinical trials, consistently showing efficacy across various treatment settings for HER2+ BC.6–8
In the neoadjuvant setting, integrating trastuzumab into cytotoxic chemotherapy regimens has been shown to enhance both pCR rates and event-free survival (EFS).9,10 Furthermore, incorporation of pertuzumab to trastuzumab-based regimens has further improved therapeutic efficacy, in metastatic, adjuvant and neoadjuvant setting.11 In the neoadjuvant setting the combination of pertuzumab, trastuzumab, and cytotoxic chemotherapy has been associated with higher pCR rates and improved survival outcomes.4,7–9 Consequently, current treatment guidelines for early or locally advanced HER2+ BC recommend trastuzumab, with or without pertuzumab, combined with chemotherapy as the standard therapeutic approach.6,12
Among these regimens, the TCHP regimen comprising docetaxel, carboplatin, trastuzumab, and pertuzumab has become a standard neoadjuvant therapy (NAT) for HER2+ BC. Clinical trials such as TRYPHAENA and KRISTINE have demonstrated promising pCR rates and manageable safety profiles with TCHP.9,13 The TRYPHAENA clinical trial, a notable Phase II study, evaluated the use of pertuzumab and trastuzumab in combination with either anthracycline- or carboplatin-based neoadjuvant chemotherapy (NAC) for HER2-positive breast cancer. The trial was primarily designed to assess cardiac safety and was not statistically powered to allow direct comparisons between the three treatment arms, all of which demonstrated relatively high pathological complete response (pCR) rates compared to historical data. Notably, despite differences in regimen intensity, the 5-year follow-up revealed no significant differences in symptomatic heart failure or declines in left ventricular ejection fraction (LVEF) between the anthracycline and non-anthracycline arms.14 In the short term, the TCHP (carboplatin-based) regimen showed numerically better cardiac safety outcomes.
However, the trial included a highly selected patient population,15 which may limit the applicability of its findings to real-world clinical settings. Moreover, considerable side effects were reported, particularly in the TCHP arm: approximately 30% of patients experienced severe adverse events (SAEs), around 70% developed diarrhea, and nearly 50% had grade 3/4 neutropenia. In addition, a substantial proportion of patients had not completed the planned 5-year follow-up, which constrains the interpretation of long-term outcomes.14
This study aims to evaluate the real-world efficacy and safety of TCHP neoadjuvant therapy in HER2+ BC patients treated at King Hussein Cancer Center (KHCC) in Jordan. By analyzing pCR rates, predictors of response, and treatment-related adverse events, this research provides valuable insights into the practical application of TCHP in a real-world clinical setting.
Materials and Methods
Study Design and Population
This retrospective study included 161 HER2+ BC patients who received at least one cycle of TCHP neoadjuvant therapy at KHCC between January 2022 and October 2024 (Figure 1). Patients were eligible if they had histologically confirmed HER2+ early breast cancer and were scheduled to receive TCHP as neoadjuvant treatment. Exclusion criteria included metastatic disease, bilateral breast cancer, previous diagnosis with breast cancer, and patients with missing or insufficient data on anti-HER2 therapy regimens, dosages, or treatment durations or patients receiving regimen other than TCHP. This study was approved by the Institutional Review Board at King Hussein Cancer Center (approval number: 22 KHCC 184) and conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective nature of the study and lack of patients’ identifiers, consent to participate was waived by the IRB.
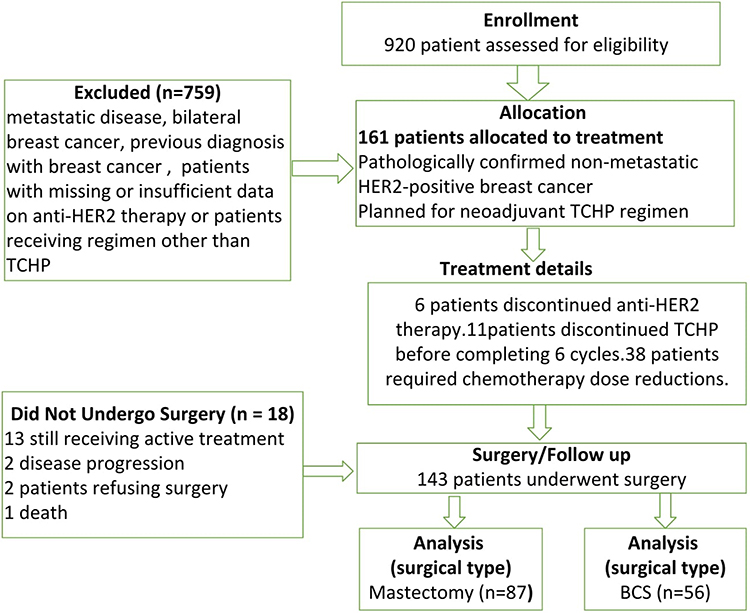 |
Figure 1 CONSORT Flow Diagram of Patient Selection and Treatment Outcomes. |
Treatment Regimen
The TCHP regimen consisted of docetaxel (75 mg/m2), carboplatin (AUC 6), trastuzumab (8 mg/kg loading dose, followed by 6 mg/kg), and pertuzumab (840 mg loading dose, followed by 420 mg), administered every 3 weeks for up to 6 cycles. Dose adjustments, treatment interruptions and discontinuation were carried out according to toxicity profiles and clinical judgment at the time.
Endpoints
The primary endpoint was pCR, defined as the absence of invasive or in-situ tumor cells in the breast and axillary lymph nodes (ypT0/Tis ypN0) upon surgical resection. Secondary endpoints were surgical outcome, safety parameters including emergency visits, discontinuation rate and hospitalization rates.
Data Collection and Analysis
We extracted data concerning patient demographics, clinical characteristics, and treatment outcome from electronic medical records. This included details such as age at diagnosis, HR status (including estrogen and progesterone receptors), HER2 status by IHC, genetic testing and lymph node involvement at diagnosis. The primary outcome was pathological complete response (pCR), defined as the absence of invasive or in situ carcinoma in both breast and axillary lymph nodes (ypT0/Tis ypN0) following neoadjuvant therapy. Follow-up time was calculated descriptively from the date of initiation of neoadjuvant TCHP to the date of the last documented clinical encounter available in the medical record. Because the primary endpoint of this study was pCR rather than a time-to-event outcome, follow-up was reported to describe duration of observation rather than for formal survival analysis, Descriptive statistics were used to summarize baseline patient characteristics. Continuous variables were reported as medians with ranges. Categorical variables were summarized as frequencies and percentages. Logistic regression analysis was used to identify predictors of pCR, with odds ratios (OR), 95% confidence intervals (CI) reported, and statistical significance was determined at a p-value threshold of <0.05.
Predictors were prespecified based on clinical relevance and prior literature and included HER2 status by IHC (2+/FISH positive vs 3+), ER/PR status (positive vs negative), axillary status (biopsy negative, biopsy positive, no biopsy), and clinical T stage (T1–2, T3–4, Tx). All prespecified variables were entered simultaneously into the multivariable logistic regression model (forced entry). Logistic regression analyses were restricted to patients who underwent surgery and had evaluable pCR (n=143). Results are reported as odds ratios with 95% confidence intervals and two-sided p values, with p<0.05 considered statistically significant.
Multicollinearity among predictors in the multivariable logistic regression model was assessed using variance inflation factors and tolerance statistics.
Results
Patient Characteristics
The study cohort included 160 females and 1 male, with a median age of 51 years (range: 24–80). No formal a prior sample size calculation was performed because this was a retrospective cohort including all consecutive eligible patients treated during the study period, The median duration of follow-up, calculated from initiation of neoadjuvant TCHP to the last documented clinical encounter, was 12.6 months (range, 1.0 to 35.3); Hormone receptor status was negative in 26.1% of patients and positive in 73.9%. Tumor histology included no special type (NST) in 116 patients 72%, invasive ductal carcinoma (IDC) in 37 patients 23%, and invasive lobular carcinoma (ILC) in 8 patients 5.0%. Clinical T-stage distribution: T1 (12 patients 7.5%), T2 (93 patients 57.8%), T3 (43 patients 26.7%), and T4 (10 patients 6.2%). Nodal involvement was present in 95 patients (59%). Tumor grade distribution was grade 1 (1 patient), grade 2 (54 patients), and grade 3 (106 patients) Table 1.
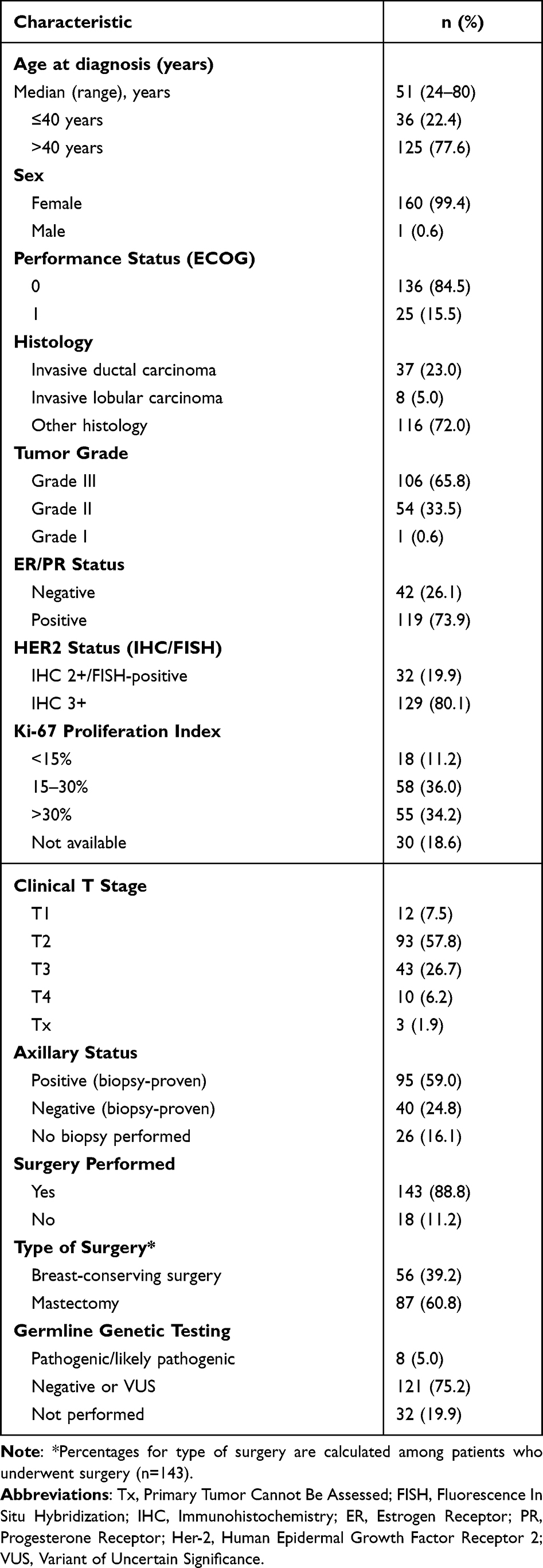 |
Table 1 Overall Cohort Characteristics (n=161) |
Baseline characteristics according to pCR status are also are shown in Table 2 In unadjusted comparisons, HER2 IHC status, hormone receptor status, and tumor grade differed significantly between patients with and without pCR, whereas ECOG performance status, clinical T stage, axillary status, and Ki-67 did not.
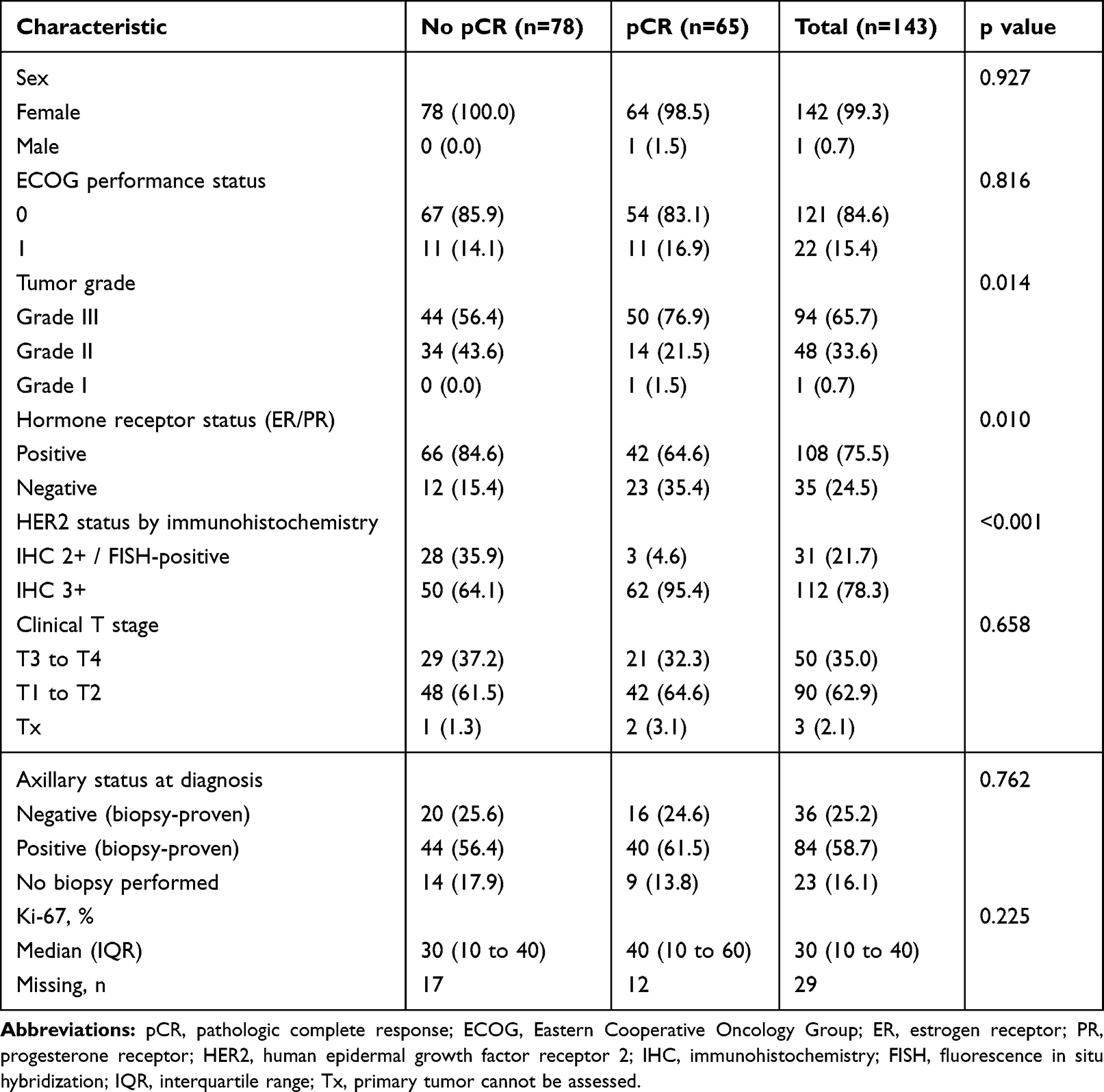 |
Table 2 Characteristics According to pCR Status (N = 143) |
Treatment Outcomes
The pCR rate in this cohort was 45.5% (65/143 patients). To evaluate predictors of pCR, univariate and multivariate logistic regression analyses were performed, with pCR (ypT0/Tis ypN0) as the outcome variable.
In univariate analysis, HER2 IHC 3+ status was strongly associated with higher odds of achieving pCR compared with HER2 IHC 2+/FISH positive tumors (OR 11.57; 95% CI 3.82–50.38; p<0.001). ER/PR negative status was also associated with higher odds of pCR relative to ER/PR positive tumors (OR 3.01; 95% CI 1.38–6.87; p=0.007). Axillary status and clinical T stage were not significantly associated with pCR in univariate analysis.
In the multivariate model adjusting for HER2 status, ER/PR status, axillary status, and clinical T stage, HER2 IHC 3+ remained an independent predictor of pCR (adjusted OR 11.76; 95% CI 3.69–54.00; p<0.001). ER/PR negative status also remained independently associated with higher odds of pCR (adjusted OR 2.59; 95% CI 1.09–6.50; p=0.035). No statistically significant independent associations were observed for axillary status (positive vs negative: adjusted OR 0.97; 95% CI 0.40–2.39; p=0.955; no biopsy vs negative: adjusted OR 0.40; 95% CI 0.11–1.33; p=0.141) or clinical T stage (T1–2 vs T3–4: adjusted OR 1.67; 95% CI 0.76–3.75; p=0.203; Tx vs T3–4: adjusted OR 6.71; 95% CI 0.41–216.56; p=0.208) (Figure 2, Table 3).
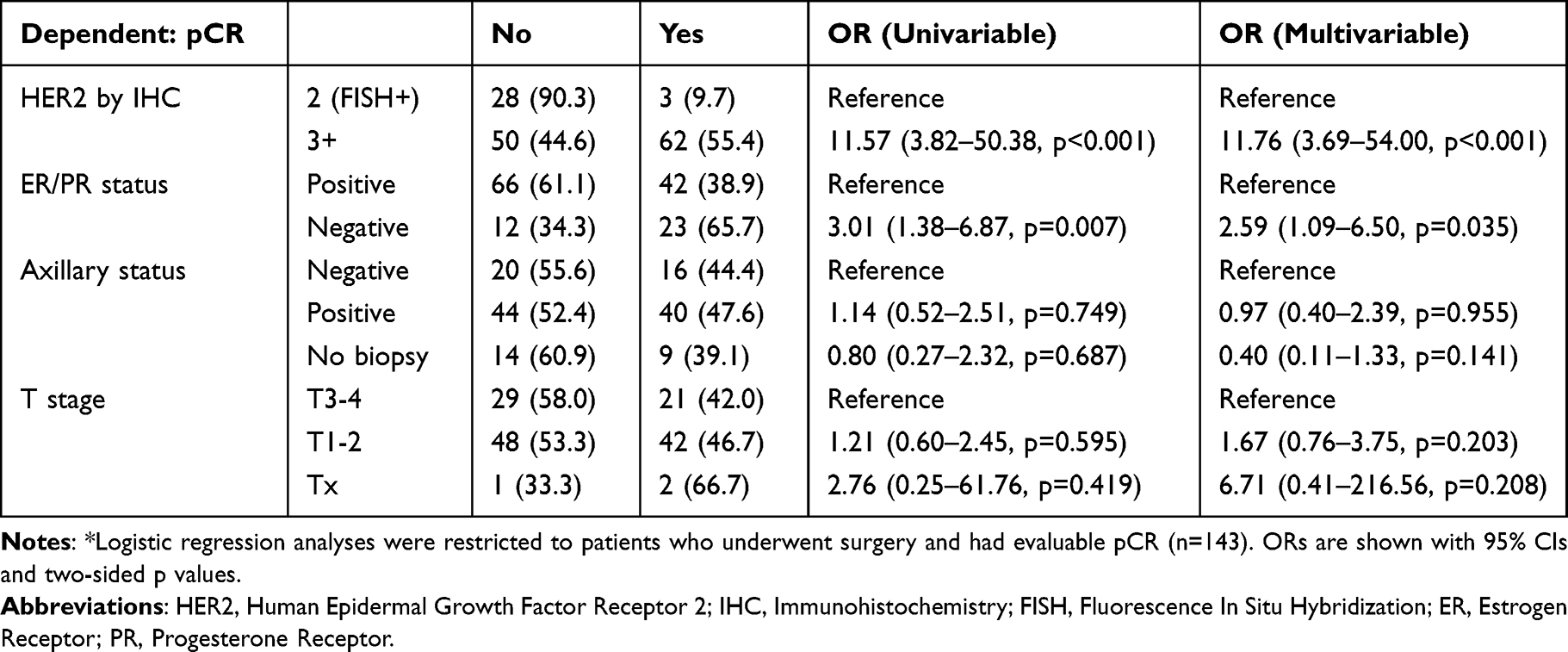 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Predictors of Pathologic Complete Response (pCR)* |
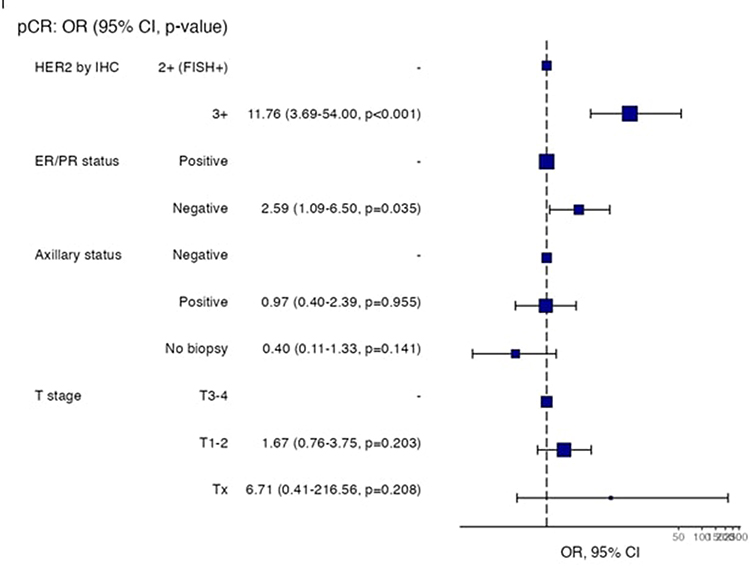 |
Figure 2 Forest plot of the multivariable logistic regression model for predictors of pathologic complete response (pCR) among patients with evaluable pCR (n=143). Squares represent adjusted odds ratios and horizontal lines represent 95% confidence intervals. Reference categories were HER2 IHC 2+/FISH positive, ER/PR positive, axillary biopsy negative, and clinical T stage T3–4. |
Multicollinearity diagnostics did not indicate problematic collinearity among predictors, with variance inflation factors ranging from 1.02 to 1.04 and tolerance values ranging from 0.96 to 0.98.
Safety Profile
No significant cardiac toxicity or decline in left ventricular ejection fraction (LVEF) was observed. All patients underwent baseline echocardiographic evaluation, followed by serial assessments every 9 weeks or earlier if cardiac symptoms developed. Anti-HER2 therapy was discontinued in 6 patients, and 11 patients stopped TCHP before completing 6 cycles mostly due to diarrhea. Chemotherapy dose reductions were required in 38 patients, primarily due to hematologic toxicity. Emergency visits occurred at a median of 3 per patient (range: 0–17); 58 patients had ≥4 visits, and 42 patients (26%) required hospitalization. The primary causes of hospital admissions were diarrhea-related issues, which accounted for 71.4% of cases. Neutropenic fever was the second most common reason, responsible for 33.3% of admissions. Infections, excluding neutropenic fever, contributed to 11.9% of the admissions, while electrolyte abnormalities not directly linked to diarrhea were also seen in 11.9% of cases. Other causes accounted for 16.7% of hospital admissions (Figure 3).
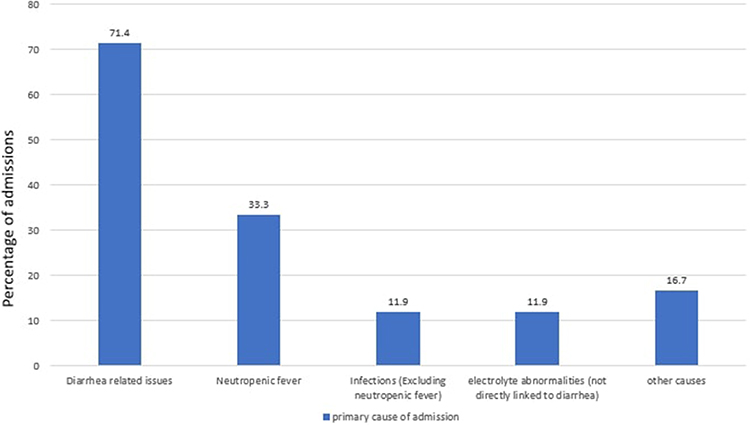 |
Figure 3 Causes of hospital admission. |
Surgical Outcomes
Of the 161 patients, 143 underwent surgical intervention, with 56 undergoing breast conservative surgery (BCS) and 87 undergoing mastectomies. The remaining 18 patients, 13 patients of them still receiving neoadjuvant therapy or waiting surgery at time of analysis, two patients refused surgery, two patients experienced disease progression and 1 patient died.
Out of 143 patients underwent surgical intervention, 86 had biopsy-proven axillary involvement. Among these 86 patients:
- Complete axillary disease resolution was observed in 47 patients (54.7%). Data were not reported for 11 patients.
- Of the 47 patients with axillary resolution, 16 underwent axillary dissection.
- 15 patients (17.4%) demonstrated residual disease in the primary breast tumor despite complete axillary resolution.
- 4 patients (4.7%) had complete resolution of the primary tumor but residual axillary disease.
- 32 patients (37.2%) achieved complete pathologic response in both the breast and axilla.
Patients with HER2/neu-positive breast cancer should be offered the opportunity for sentinel lymph node biopsy (SLNBx) following neoadjuvant therapy, irrespective of their initial nodal status or radiologic response.
Discussion
We found a pCR rate of 45.5% in our real-world cohort. This is lower than the rates seen in RCTs like TRAIN-2 (68%), TRYPHAENA (66.2%) and KRISTINE (55.7%). These differences may be largely likely reflecting differences in patient populations, adherence to treatment, and supportive care practices.
However, the TRYPHAENA trial, being a Phase II study, was not powered for direct comparisons between treatment arms. Therefore, these findings are descriptive and not statistically significant. Along with the three arms demonstrated pCR rates exceeding 55%, reflecting a highly selected patient population. However, there is large range in pCR rate between several retrospective real-world studies, such as Canino et al (45.6%),16 Zhukova et al (58%),17 and Howell et al (63.7%).18
A key factor likely contributing to the lower pCR rate in our cohort is the higher proportion of ER/PR-positive tumors, which comprised 73.9% of patients—substantially more than in TRYPHAENA arm C (51.9%) and TRAIN-2 (42%), as shown in Table 4. This difference in tumor biology may partly explain the observed gap in treatment response. In our multivariate analysis, ER/PR-negative status was independently associated with higher odds of achieving pCR (OR 2.59; 95% CI: 1.09–6.50; p = 0.035), consistent with previously published data.2,6,10
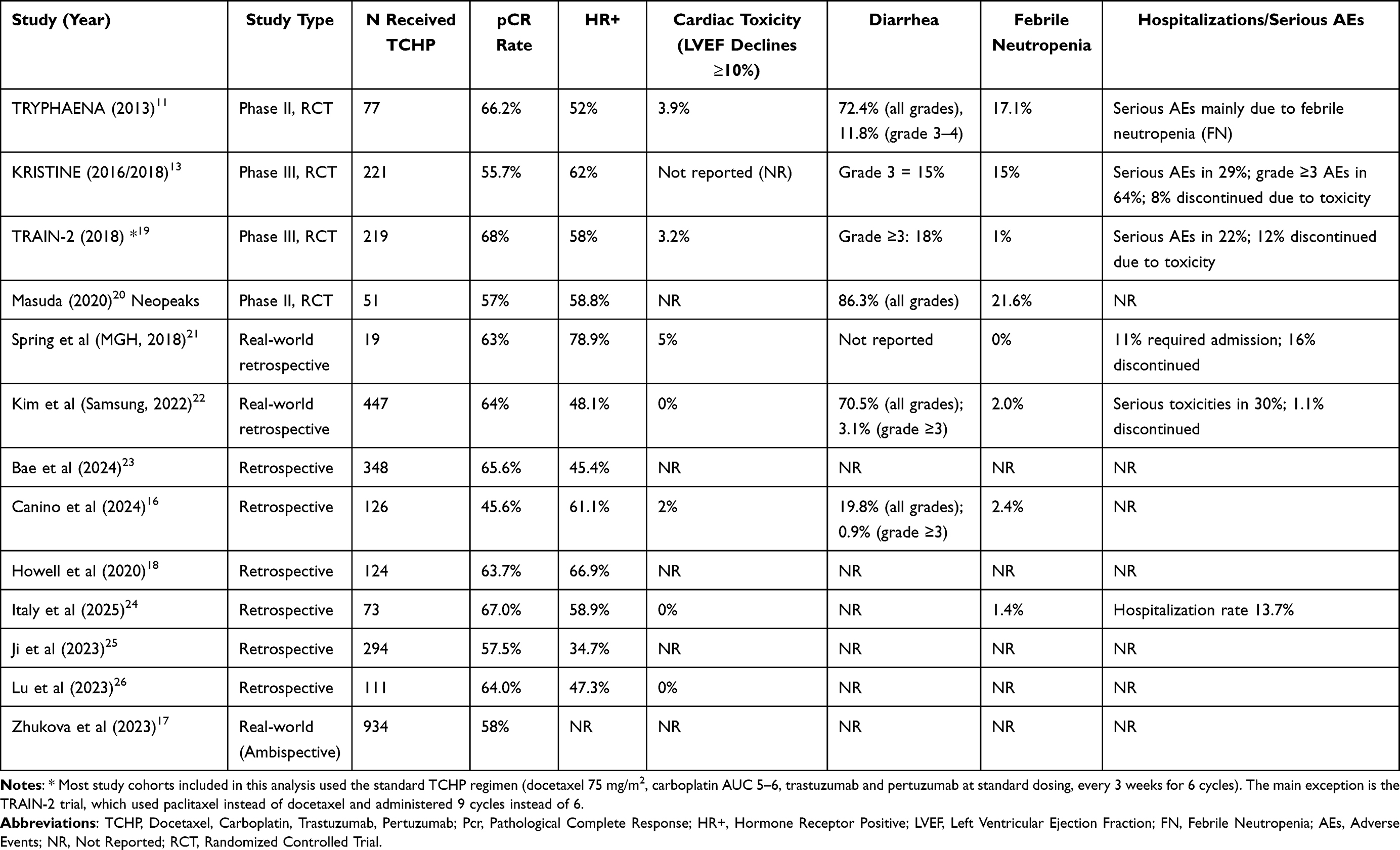 |
Table 4 TCHP Regimen in Neoadjuvant HER2+ in Breast Cancer: Clinical Trials and Real-World Outcomes |
Similarly, HER2 IHC 3+ tumors demonstrated significantly better response compared to HER2 IHC 2+/FISH+ tumors, with pCR rates of 55.4% and 9.7%, respectively. HER2 IHC 3+ status was also a strong independent predictor of pCR (OR 11.76; 95% CI: 3.69–54.00; p < 0.001). Overall, ER/PR-negative tumors had a pCR rate of 65.7%, compared to 38.9% in hormone receptor–positive tumors.
These findings are consistent with outcomes reported in TRYPHAENA and TRAIN-2, both of which included more favorable tumor profiles in highly selected populations. Of note, 21.7% of patients in our study had HER2 IHC 2+/FISH+ tumors, compared to only 2.6% in TRYPHAENA further contributing to the differences in pCR outcomes.
Moreover, the differences in study design should be considered. RCTs typically enroll highly selected patients with 63.6% of patient with stage T3N1 and lower and 49.4% T2n1 and lower in TRYPHAENA trial, similarly 68% of the patient in TRAIN −2 trail was stage2 also close monitoring and uniform treatment adherence, factors that likely contribute to their higher reported pCR rates. In contrast, real-world studies, including ours, reflect a broader and more heterogeneous patient population with variable comorbidities, treatment interruptions, and adherence issues.27 Our cohort included patients with incomplete TCHP cycles (11 patients discontinued early), dose reductions (38 patients), and hospitalizations (42 patients), which may have attenuated treatment intensity and efficacy. These limitations are inherent to routine clinical practice and underscore the difference between efficacy in controlled trials and effectiveness in real-world settings.
In this real-world study evaluating the impact of neoadjuvant TCHP (docetaxel, carboplatin, trastuzumab, and pertuzumab) in patients with HER2-positive early breast cancer, surgical outcomes demonstrate the significant clinical value of this regimen in enabling both oncologic control and surgical de-escalation.
Of the 161 patients included, 143 (88.8%) proceeded to surgery following neoadjuvant therapy. Breast-conserving surgery (BCS) was achieved in 56 patients (39.2%), while 87 patients (60.8%) underwent mastectomy. The relatively high mastectomy rate, despite a potent systemic regimen, may reflect a range of factors including tumor size, multifocality, genetic predisposition (eg, BRCA mutation), and patient or physician preference. Nonetheless, the substantial proportion of patients eligible for BCS highlights the ability of TCHP to induce meaningful tumor down-staging in routine clinical practice.
Eighteen patients (11.2%) had not undergone surgery at the time of data cutoff—thirteen were still completing neoadjuvant therapy or awaiting surgery, two declined surgical management, one died and two experienced disease progression, indicating the importance of close multidisciplinary coordination to optimize treatment completion and timing of surgery.
Axillary response to neoadjuvant TCHP was particularly noteworthy. Of the 143 surgical patients, 95 (59.0%) had biopsy-proven axillary node involvement prior to treatment. Following neoadjuvant therapy, complete nodal resolution was achieved in 47 patients (54.7%). Interestingly, 16 of these patients still underwent axillary lymph node dissection (ALND), possibly due to lack of standardized protocols for axillary restaging or limited use of targeted axillary dissection techniques. Among the remaining patients, 15 (17.4%) had residual disease in the breast despite axillary clearance, and four patients (4.7%) demonstrated persistent nodal disease despite pCR in the breast. A total of 32 patients (37.2%) achieved complete pathologic response in both breast and axilla, reflecting a robust tumoricidal effect and consistent with previously reported pCR rates in landmark clinical trials.
These results underscore the growing consensus that patients with HER2-positive breast cancer regardless of initial nodal burden should be considered for sentinel lymph node biopsy (SLNBx) following neoadjuvant therapy, especially in the setting of radiologic or clinical response.28–30 De-escalation of axillary surgery in responders is supported by multiple guidelines and clinical trials,31,32 and may significantly reduce long-term complications such as lymphedema and shoulder dysfunction, improving patients’ postoperative quality of life.33
From an oncologic standpoint, pathologic complete response (pCR) is a validated surrogate marker for improved disease-free and overall survival in HER2-positive breast cancer,34 While long-term follow-up is needed, the high rate of total pCR (tpCR) observed in our cohort suggests a favorable prognosis and aligns with outcomes from pivotal trials such as TRAIN-2,19 TRYPHAENA,11 and NEOSPHERE.8 Importantly, patients who achieve pCR following neoadjuvant TCHP (docetaxel, carboplatin, trastuzumab, and pertuzumab) are known to have lower recurrence rates, particularly in hormone receptor-negative subtypes.35
Cosmetic outcomes are also an important consideration in early breast cancer management. Achieving breast-conserving surgery (BCS) not only confers equivalent survival compared to mastectomy,36,37 but also improves body image, psychosocial well-being, and patient satisfaction.38,39 The potential to shift more patients toward BCS following neoadjuvant TCHP thus carries both oncologic and quality-of-life implications.
In summary, the surgical outcomes in this study provide real-world validation of the efficacy of neoadjuvant TCHP in HER2-positive early breast cancer. The regimen facilitates both breast and axillary down-staging, supports less invasive surgical strategies, and contributes to favorable pathologic and potentially long-term oncologic outcomes. Future directions should include longitudinal follow-up to assess survival and recurrence, as well as prospective strategies to standardize surgical decision-making post-neoadjuvant therapy in routine practice.
Safety Profile and Hospitalization Rates
The safety profile of TCHP in our study was similar to the data of clinical trial and also retrospective trial Kim et al,22 other retrospective series24,26 The mean baseline LVEF was 60.2% ± 2.3, and the mean lowest LVEF during therapy was 59.5% ± 2.3, corresponding to a mean change of −0.73% ± 1.71. Importantly, none of the patients experienced an absolute decline of ≥10%, or LVEF <50% at any time during treatment or follow-up.
And this is reassuring in the view of known cardiotoxicity risk associated with HER2 targeted therapies. Nonetheless, the substantial rates of emergency visits (median 3/ patient) and hospitalizations (42 patients (26.1%) underscore the difficulties encountered in the management of treatment-associated toxicities in actual practice. Real-world studies, just like the study by spring et al et al (2018),21 who found a hospitalization rate of 11%, and another real-world data by Itay et al,24 who found a hospitalization rate of 14%, which is consistent with our findings.
Regarding treatment tolerability, anti-HER2 therapy was discontinued in 3.7% (n=6) of our patients, while 6.8% (n=11) discontinued the TCHP regimen prior to completing the planned six cycles. These discontinuation rates are comparable to landmark trials; for instance, the TRYPHAENA trial reported discontinuation rates of 7.9% for anti-HER2 therapy and 9.2% for chemotherapy, while the TRAIN-2 trial noted a 6.2% discontinuation rate due to adverse events.
With the goal of minimizing treatment-related toxicity and improving tolerability without compromising oncologic outcomes, strategies for chemotherapy de-escalation are increasingly supported by recent Phase III evidence.
The HELEN-006 trial40 demonstrated that a carboplatin-free regimen utilizing weekly nab-paclitaxel with dual HER2-blockade achieved a significantly higher pCR rate compared to standard TCHP (66.3% vs. 57.6%; p=0.011), while significantly reducing gastrointestinal toxicities. In our clinical environment, where 71.4% of hospitalizations were directly attributed to diarrhea and related complications, this approach would be most beneficial for patients with limited physiological reserve or those at high risk for the severe dehydration observed in our cohort, and may significantly reduce hospital admissions. Furthermore, the neoCARHP trial41 recently confirmed that omitting carboplatin from the TCHP backbone resulted in non-inferior pCR rates (64.1% vs. 65.9%) but with a markedly improved safety profile, including lower rates of Grade 3–4 myelosuppression, these findings suggest a clear path for treatment optimization. Specifically, patients in our cohort who are elderly, have significant baseline comorbidities, or exhibit early signs of hematologic toxicity would likely benefit from a carboplatin-free approach to avoid the treatment-related morbidity that necessitated inpatient care in our practice.
Furthermore, for patients with triple-positive or early-stage disease, the PHERGAIN-2 trial42 (PMID: 41079649) showed that PET-CT-guided, chemotherapy-free strategies can safely identify exceptional responders. This strategy identifies a low-risk subgroup—specifically those with small, highly hormone-sensitive tumors with significant reduction in hospitalization and complication by entirely by avoiding systemic chemotherapy, Given the high rate of hospitalizations (26.1%) and dose reductions in our TCHP cohort, these findings suggest that omitting carboplatin in favor of a more tolerable taxane-based dual blockade or utilizing biomarker-guided de-escalation could maintain efficacy while significantly mitigating the treatment-related morbidity encountered in routine clinical practice.
This issue is particularly relevant in Jordan, where breast cancer presents at a younger age—median 48–51 years43 versus 62–63 years in Western populations44 and is more frequently high grade, limiting tolerance to intensive HER2-directed regimens such as TCHP. Common regional comorbidities, including obesity and type 2 diabetes,45 may further intensify carboplatin-related mucosal injury and taxane-associated fatigue, contributing to the higher rates of gastrointestinal-related admissions in our cohort. These challenges are compounded by widespread tobacco exposure, with more than 60% of households reporting at least one regular smoker,46 which is known to worsen chemotherapy tolerance. Together, these factors help explain the real-world toxicity observed and support consideration of tailored de-escalation strategies.
Study Limitations
Despite the significant real-world evidence provided by this study, several limitations must be acknowledged. First, its retrospective, single-center design may limit the generalizability of the findings to broader populations or different healthcare settings. Second, the sample size, particularly for the subset of 18 patients who did not undergo surgery, is relatively small, which may affect the statistical power of the analysis regarding reasons for surgical exclusion such as disease progression or patient refusal. Furthermore, because the data was derived from routine clinical practice rather than a controlled trial environment, there is an inherent risk of under-reporting subjective toxicities, and the criteria for chemotherapy dose reductions or ER visits may vary based on individual physician discretion. Finally, while pCR was used as a primary efficacy endpoint, this study does not yet provide robust long-term data. We explored overall survival and recurrence-free outcomes in this cohort; however, the number of survival events during the available follow-up was very small, and any Kaplan–Meier estimates would be statistically unstable with wide confidence intervals and limited interpretability.
An additional limitation relates to the size of the regression dataset relative to the number of modeled parameters. The multivariable logistic regression was restricted to 143 patients with evaluable pCR, including 65 pCR events. Although the model was intentionally limited to a small number of prespecified clinically relevant predictors, the available event count still permits the possibility of limited statistical power and some degree of overfitting, particularly for categories with small cell counts such as Tx. This may have reduced estimate precision, as reflected by the wide confidence intervals for some covariates, and the adjusted model should therefore be interpreted cautiously.
Conclusion
In routine practice, neoadjuvant TCHP produced a moderate pCR rate (45.5%) yet imposed a substantial toxicity burden, including 26.1% hospitalizations and frequent dose reductions, revealing a clear efficacy–tolerability gap in the real‑world setting. While HER2 IHC 3+ and HR‑negative disease remained strong predictors of response, their key value in this context is improving patient selection, helping identify those most likely to benefit from full‑intensity TCHP. These findings highlight the importance of combining better upfront selection with strengthened supportive care and consideration of de‑escalation approaches—such as carboplatin omission or biomarker‑guided tailoring—to preserve oncologic efficacy while reducing treatment‑related morbidity in everyday clinical practice.
Institutional Review Board Statement
The study was approved by the IRB at King Hussein Cancer Center. Approval number: 22 KHCC 184. The study was conducted in accordance with the principles of the Declaration of Helsinki. Given the retrospective nature of the study and lack of patients’ identifiers, consent to participate was waived by the IRB.
Data Sharing Statement
Data related to this manuscript will be made available on reasonable requests to the corresponding author.
Funding
This project received no funding. However, publications fees will be provided by King Hussein Cancer Center.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Owens MA, Horten BC, Da Silva MM. HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556 breast cancer tissues. Clin Breast Cancer. 2004;5(1):63–14. doi:10.3816/cbc.2004.n.011
2. Slamon DJ, Clark GM, Wong SG, Levin WJ, Ullrich A, McGuire WL. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science. 1987;235(4785):177–182. doi:10.1126/science.3798106
3. Slamon DJ, Leyland-Jones B, Shak S, et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N Engl J Med. 2001;344(11):783–792. doi:10.1056/NEJM200103153441101
4. Swain SM, Baselga J, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel in HER2-positive metastatic breast cancer. N Engl J Med. 2015;372(8):724–734. doi:10.1056/NEJMoa1413513
5. Baselga J, Cortés J, Kim SB, et al. Pertuzumab plus trastuzumab plus docetaxel for metastatic breast cancer. N Engl J Med. 2012;366(2):109–119. doi:10.1056/NEJMoa1113216
6. von Minckwitz G, Procter M, de Azambuja E, et al. Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer [published correction appears in N Engl J Med. New Engl J Med. 2017;377(2):122–131. doi:10.1056/NEJMoa1703643
7. Piccart M, Procter M, Fumagalli D, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer in the APHINITY trial: 6 years’ follow-up. J Clin Oncol. 2021;39(13):1448–1457. doi:10.1200/JCO.20.01204
8. Gianni L, Pienkowski T, Im YH, et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre open-label Phase 2 trial. Lancet Oncol. 2012;13(1):25–32. doi:10.1016/S1470-2045(11)70336-9
9. Buzdar AU, Ibrahim NK, Francis D, et al. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol. 2005;23(16):3676–3685. doi:10.1200/JCO.2005.07.032
10. Gianni L, Eiermann W, Semiglazov V, et al. Neoadjuvant chemotherapy with trastuzumab followed by adjuvant trastuzumab versus neoadjuvant chemotherapy alone, in patients with HER2-positive locally advanced breast cancer (the NOAH trial): a randomised controlled superiority trial with a parallel HER2-negative cohort. Lancet. 2010;375(9712):377–384. doi:10.1016/S0140-6736(09)61964-4
11. Schneeweiss A, Chia S, Hickish T, et al. Pertuzumab plus trastuzumab in combination with standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer: a randomized phase II cardiac safety study (TRYPHAENA). Ann Oncol. 2013;24(9):2278–2284. doi:10.1093/annonc/mdt182
12. Gradishar WJ, Moran MS, Abraham J, et al. NCCN Guidelines® Insights: breast Cancer, Version 4.2023. J Natl Compr Canc Netw. 2023;21(6):594–608. doi:10.6004/jnccn.2023.0031
13. Hurvitz SA, Martin M, Jung KH, et al. Neoadjuvant trastuzumab emtansine and pertuzumab in human epidermal growth factor receptor 2-positive breast cancer: three-year outcomes from the Phase III KRISTINE study. J Clin Oncol. 2019;37(25):2206–2216. doi:10.1200/JCO.19.00882
14. Schneeweiss A, Chia S, Hickish T, et al. Long-term efficacy analysis of the randomised, phase II TRYPHAENA cardiac safety study: evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early breast cancer. Eur J Cancer. 2018;89:27–35. doi:10.1016/j.ejca.2017.10.021
15. Kim ES, Bernstein D, Hilsenbeck SG, et al. Modernizing eligibility criteria for molecularly driven trials. J Clin Oncol. 2015;33(25):2815–2820. doi:10.1200/JCO.2015.62.1854
16. Canino F, Barbolini M, De Giorgi U, et al. Safety and efficacy analysis of neoadjuvant pertuzumab, trastuzumab and standard chemotherapy for HER2-positive early breast cancer: real-world data from NeoPowER study. BMC Cancer. 2024;24(1):735. doi:10.1186/s12885-024-12506-0
17. Zhukova L, Sorokina I, Danilova A, et al. INSIGHT-HER2BC: real-world evidence of TCHP regimen to describe the best patient profile and open up questions—The interim results. J Clin Oncol. 2023;41(16_suppl):e12607. doi:10.1200/JCO.2023.41.16_suppl
18. Howell SJ, Coe F, Wang X, Horsley L, Ekholm M. Carboplatin dose capping affects pCR rate in HER2-positive breast cancer patients treated with neoadjuvant Docetaxel, Carboplatin, Trastuzumab, Pertuzumab (TCHP). Breast Cancer Res Treat. 2020;184(2):481–489. doi:10.1007/s10549-020-05868-z
19. van Ramshorst MS, van der Voort A, van Werkhoven E, et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive breast cancer (TRAIN-2): a multicentre, open-label, randomised, Phase 3 trial. Lancet Oncol. 2018;19(12):1630–1640. doi:10.1016/S1470-2045(18)30570-9
20. Masuda N, Ohtani S, Takano T, et al. A randomized, 3-arm, neoadjuvant, phase 2 study comparing docetaxel + carboplatin + trastuzumab + pertuzumab (TCbHP), TCbHP followed by trastuzumab emtansine and pertuzumab (T-DM1+P), and T-DM1+P in HER2-positive primary breast cancer. Breast Cancer Res Treat. 2020;180(1):135–146. doi:10.1007/s10549-020-05524-6
21. Spring L, Niemierko A, Haddad S, et al. Effectiveness and tolerability of neoadjuvant pertuzumab-containing regimens for HER2-positive localized breast cancer. Breast Cancer Res Treat. 2018;172(3):733–740. doi:10.1007/s10549-018-4959-8
22. Kim JY, Nam SJ, Lee JE, et al. Real-world evidence of neoadjuvant docetaxel/carboplatin/trastuzumab/pertuzumab (TCHP) in patients with HER2-positive early or locally advanced breast cancer: a single-institutional clinical experience. Cancer Res Treat. 2022;54(4):1091–1098. doi:10.4143/crt.2021.901
23. Bae SJ, Kim JH, Lee MJ, et al. Predictive markers of treatment response to neoadjuvant systemic therapy with dual HER2-blockade. Cancers. 2024;16(4):842. doi:10.21203/rs.3.rs-3801073/v1
24. Itay A, Globus O, Levanon K, et al. A retrospective, single-center study comparing neoadjuvant ACTHP vs DCbHP in HER2-positive early breast cancer patients. Cancers. 2025;17(2):250. doi:10.3390/cancers17020250
25. Ji JH, Bae SJ, Kim S, et al. Anaemia and pathologic complete response rate according to carboplatin dose in HER2-positive breast cancer treated with neoadjuvant TCHP. Cancer Med. 2023;12(2):1409–1417. doi:10.1002/cam4.5022
26. Lu H, Yan H, Liao S, et al. Efficacy, cardiotoxicity and factors affecting pathologic complete response of neoadjuvant chemotherapy with anthracycline-containing versus anthracycline-free regimens plus dual HER2 blockade for HER2-positive early-stage breast cancer: a retrospective study. Transl Cancer Res. 2023;12(6):1490–1502. doi:10.21037/tcr-22-2547
27. Sharaf B, Tamimi F, Al-Abdallat H, et al. Dual anti-HER2 therapy vs trastuzumab alone with neoadjuvant anthracycline and taxane in HER2-positive early-stage breast cancer: real-world insights. Biolog Targets Ther. 2025;19:59–71. doi:10.2147/BTT.S468650
28. Boughey JC, Suman VJ, Mittendorf EA, et al. Sentinel lymph node surgery after neoadjuvant chemotherapy in patients with node-positive breast cancer: the ACOSOG Z1071 (Alliance) clinical trial. JAMA. 2013;310(14):1455–1461. doi:10.1001/jama.2013.278932
29. Kuehn T, Bauerfeind I, Fehm T, et al. Sentinel-lymph-node biopsy in patients with breast cancer before and after neoadjuvant chemotherapy (SENTINA): a prospective, multicentre cohort study. Lancet Oncol. 2013;14(7):609–618. doi:10.1016/S1470-2045(13)70166-9
30. Simons JM, van Nijnatten TJA, van der Pol CC, Luiten EJT, Koppert LB, Smidt ML. Diagnostic accuracy of different surgical procedures for axillary staging after neoadjuvant systemic therapy in node-positive breast cancer: a systematic review and meta-analysis. Ann Surg. 2019;269(3):432–442. doi:10.1097/SLA.0000000000003075
31. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology: breast Cancer. Version 4.2024. Updated November 20, 2024. Available from: https://www.nccn.org.
32. van der Noordaa MEM, van Duijnhoven FH, Voogd AC, et al. Toward omitting axillary surgery in clinically node-positive breast cancer after neoadjuvant systemic therapy. Ann Surg Oncol. 2021;28(10):5732–5740.
33. Lucci A, McCall LM, Beitsch PD, et al. Surgical complications associated with sentinel lymph node dissection (SLND) plus axillary lymph node dissection compared with SLND alone in the American College of Surgeons Oncology Group Trial Z0011. J Clin Oncol. 2007;25(24):3657–3663. doi:10.1200/JCO.2006.07.4062
34. Cortazar P, Zhang L, Untch M, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. 2014;384(9938):164–172. doi:10.1016/S0140-6736(13)62422-8
35. Bianchini G, Veer LJ, Desmedt C, et al. Dual HER2 blockade in HER2-positive breast cancer: comparative effectiveness and biomarkers. Lancet Oncol. 2016;17(6):738–754. doi:10.1016/S1470-2045(16)00150-9
36. Fisher B, Anderson S, Bryant J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. N Engl J Med. 2002;347(16):1233–1241. doi:10.1056/NEJMoa022152
37. van Dongen JA, Voogd AC, Fentiman IS, et al. Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. J Natl Cancer Inst. 2000;92(14):1143–1150. doi:10.1093/jnci/92.14.1143
38. Al-Ghazal SK, Fallowfield L, Blamey RW. Comparison of psychological aspects and patient satisfaction following breast conserving surgery, simple mastectomy and breast reconstruction. Eur J Cancer. 2000;36(15):1938–1943. doi:10.1016/S0959-8049(00)00197-0
39. King TA, Sakr R, Patil S, et al. Prospective study of surgical decision-making processes in women with breast cancer. J Clin Oncol. 2012;30(12):1484–1490. doi:10.1200/JCO.2011.36.7771
40. Chen XC, Jiao DC, Qiao JH, et al. De-escalated neoadjuvant weekly nab-paclitaxel with trastuzumab and pertuzumab versus docetaxel, carboplatin, trastuzumab, and pertuzumab in patients with HER2-positive early breast cancer (HELEN-006): a multicentre, randomised, phase 3 trial. Lancet Oncol. 2025;26(1):27–36. doi:10.1016/S1470-2045(24)00581-3
41. Gao HF, Li W, Wu Z, et al. De-escalated neoadjuvant taxane plus trastuzumab and pertuzumab with or without carboplatin in HER2-positive early breast cancer (neoCARHP): a multicentre, open-label, randomised, phase 3 trial. J Clin Oncol. 2025;43(17_suppl):LBA500. doi:10.1200/JCO.2025.43.17_suppl.LBA500
42. Pérez-García JM, Gebhart G, Ruiz Borrego M, et al. Chemotherapy de-escalation using an $^{18}$F-FDG-PET-based pathological response-adapted strategy in patients with HER2-positive early breast cancer (PHERGain): a multicentre, randomised, open-label, non-comparative, phase 2 trial. Lancet Oncol. 2021;22(6):858–871. doi:10.1016/S1470-2045(21)00122-4
43. Mousa RH, Melhem JM, Hammad EA. Epidemiology of women diagnosed with breast cancer in Jordan: a 5‑year survival analysis and patients’ characteristics from 2 public hospitals. Saudi Med J. 2021;42(7):776–783. doi:10.15537/smj.2021.42.7.20210112
44. Komen SG. Breast Cancer Risk Factors: age. Median age of breast cancer diagnosis in U.S. women: 63 years.
45. Al-Taani GM, El-Osta A, Alnahar SA. Prevalence and socioeconomic factors of diabetes: a population-based cross-sectional analysis from Jordan. J Glob Health. 2025;15:04095. doi:10.7189/jogh.15.04095
46. Awidi M. Choking growth one puff at a time: how tobacco is strangling Jordan’s economy. Tob Control. 2025:tc–2025–059525. Documents extraordinarily high smoking rates in Jordan. doi:10.1136/tc-2025-059525
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Optimal Choice of Neoadjuvant Chemotherapy for HER2-Negative Breast Cancer: Clinical Insights
Lucas MW, Kelly CM
Cancer Management and Research 2022, 14:2493-2506
Published Date: 17 August 2022
Innovative Surgical Approaches That Improve Individual Outcomes in Advanced Breast Cancer
Luțenco V, Rebegea L, Beznea A, Tocu G, Moraru M, Mihailov OM, Ciuntu BM, Luțenco V, Stanculea FC, Mihailov R
International Journal of Women's Health 2024, 16:555-560
Published Date: 30 March 2024
Predicting Human Epidermal Growth Factor Receptor 2 Expression in Breast Cancer Based on Radiomics of MRI Habitat and US
Lin Z, Huang F, Wei L, Liao X, Gao Y
Breast Cancer: Targets and Therapy 2025, 17:711-725
Published Date: 15 August 2025
Development and Validation of a Radiomics-Based Nomogram for Predicting HER-2 Status in Breast Cancer: A Retrospective Study with Small Validation Cohort
Qiu Q, Chen C, Chen J, Liao C, Tang L
Breast Cancer: Targets and Therapy 2025, 17:1119-1132
Published Date: 2 December 2025