Back to Journals » Clinical Interventions in Aging » Volume 17
Breast Cancer in Geriatric Patients: Current Landscape and Future Prospects
Authors Abdel-Razeq H ![]() , Abu Rous F
, Abu Rous F ![]() , Abuhijla F
, Abuhijla F ![]() , Abdel-Razeq N, Edaily S
, Abdel-Razeq N, Edaily S ![]()
Received 28 June 2022
Accepted for publication 14 September 2022
Published 28 September 2022 Volume 2022:17 Pages 1445—1460
DOI https://doi.org/10.2147/CIA.S365497
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Hikmat Abdel-Razeq,1,2 Fawzi Abu Rous,3 Fawzi Abuhijla,4 Nayef Abdel-Razeq,3 Sarah Edaily1
1Department of Internal Medicine, King Hussein Cancer Center, Amman, Jordan; 2School of Medicine, The University of Jordan, Amman, Jordan; 3Henry Ford Health System, Detroit, MI, USA; 4Department of Radiation Oncology, King Hussein Cancer Center, Amman, Jordan
Correspondence: Hikmat Abdel-Razeq, Department of Internal Medicine, King Hussein Cancer Center, 202 Queen Rania Al Abdullah Street, Amman, 11941, Jordan, Tel +962-6 5300460, Ext: 1000, Email [email protected]
Abstract: Breast cancer is the most common cancer diagnosed among women worldwide and more than half are diagnosed above the age of 60 years. Life expectancy is increasing and the number of breast cancer cases diagnosed among older women are expected to increase. Undertreatment, mostly due to unjustifiable fears of advanced-age and associated comorbidities, is commonly practiced in this group of patients who are under-represented in clinical trials and their management is not properly addressed in clinical practice guidelines. With modern surgery and anesthesia, breast surgeries are considered safe and is usually associated with very low complication rates, regardless of extent of surgery. However, oncoplastic surgery and management of the axilla can be tailored based on patients’- and disease-related factors. Most of chemotherapeutic agents, along with targeted therapy and anti-Human epidermal growth factor receptor-2 (HER2) drugs can be safely given for older patients, however, dose adjustment and close monitoring of potential adverse events might be needed. The recently introduced cyclin-D kinase (CDK) 4/6-inhibitors in combination with aromatase inhibitors (AI) or fulvestrant, which changed the landscape of breast cancer therapy, are both safe and effective in older patients and had substituted more aggressive and potentially toxic interventions. Despite its proven efficacy, adjusting or even omitting adjuvant radiation therapy, at least in low-risk older patients, is safe and frequently practiced. In this paper, we review existing data related to breast cancer management among older patients across the continuum; from resection of the primary tumor through adjuvant chemotherapy, radiation and endocrine therapy up to the management of recurrent and advanced-stage disease.
Keywords: breast cancer, age, elderly patients, geriatric
Introduction
Breast cancer is the most common cancer diagnosed among women worldwide.1 The median age at diagnosis in the United States (US) is 63 and the incidence increases with age.2 Over a third of patients diagnosed with invasive breast cancer, and almost half of breast cancer-related mortalities in Western societies are reported among those over 70 years of age.3 Life expectancy is increasing and the number and percentage of breast cancer diagnosed among older patients are expected to increase. Data on the management of breast cancer among elderly patients is scarce;4,5 many such patients have comorbidities and are not included in clinical trials.6 Delaying or omitting chemotherapy,7 radiotherapy8,9 and even surgical resection of the tumor are commonly practiced in this age group. Such undertreatment may negatively impact on treatment outcomes and prognosis.10 Proper geriatric assessment is extremely important to hopefully avoid unnecessary undertreatment or expose patients to intolerable toxicities. However, such assessment is not routinely practiced; lack of skills, expertise and proper training along with lack of time in busy service, are major contributing factors.
In this paper, we review existing data related to breast cancer management among older patients. It is hoped that such review should highlight the importance of geriatric oncology, and direct oncologists to proper assessment of aging, in an evidence-based decision-making process.
Surgery
Surgical resection with proper surgical margins remains the cornerstone of breast cancer therapy. With modern surgery and anesthesia, breast surgeries are considered safe and is usually associated with very low complication rates regardless of extent of surgery; breast-conserving (BCS) or mastectomy.11,12 Omitting surgical resection in such patients, can have a negative impact on treatment outcomes regardless of age, tumor stage, hormone receptor and human epidermal growth factor receptor-2 (HER2) status.13,14 In a prospective multicenter study in UK that included women aged 70 or older with primary operable invasive breast cancer (T1-4N0-2M0), researchers found that age, frailty and comorbidities affected decision for mastectomy and axillary dissection. In such older patients, breast cancer surgery was shown to be safe with low to moderate adverse events (19.3%) and no 30-day mortality. However, surgery had negative impact on quality of life and functional independence.15
Surgical Options for Primary Disease
Type and extent of primary surgery for breast cancer are usually based on multiple factors related to comorbidities, functional status, and tumor stage. However, patient’s age remains an independent factor for health care professionals in selecting the surgery type.16 Morgan et al, showed a higher tendency for mastectomy for older age group,16 which was also shown in large retrospective study in which patients aged 70 or older were less likely to have BCS, most likely to avoid adjuvant radiation to minimize additive toxicity for such patients.17
Surgical Management of the Axilla
Early studies on surgical management of breast cancer in older patients revealed that those with early-stage breast cancer with clinically negative nodes can be safely treated with surgery to primary disease without axillary lymph node dissection (ALND).18,19 Mandelblatt et al, assessed the sequelae of ALND in early-stage breast cancer for patients ≥ 67 years and reported consistent adverse effect on quality of life including higher rates for lymphedema, arm pain and shoulder movement limitation.20 Furthermore, a randomized trial addressed the role of ALND in patients 60 years or older with clinically negative axillary lymph nodes and positive hormonal receptor, showed better quality of life without ALND.21 The use of sentinel lymph node biopsy (SLNB) grants a less intensified form for axillary surgical management.22 Although SLNB may still be omitted to avoid overtreatment for low-risk group in elderly patients, it may still be useful to better guide oncologists on aggressiveness of adjuvant therapy for medically fit older patients.23,24 However, these findings should not be generalized for all elderly patients as the omission of axillary staging might result in higher risk of regional recurrence, however, with no impact on overall survival (OS) or breast cancer-specific survival (BCSS).25 A predictive nomogram for survival benefit of SLNB for elderly patients was suggested to better classify patients into risk groups, were SLNB can be selected based on risk stratification.26
There are multiple ongoing trials addressing axillary management on older patients based on clinical stage, response to chemotherapy and findings on SLNB. The SENOMAC27 (NCT02240472) and SERC28 (NCT01717131) trials are randomizing patients to ALND or no ALND following a finding of positive SLNB for patients with clinically node-negative, cT1-3 (SENOMAC), or cT1-2 (SERC). The POSNOC29 study (NCT02401685) assesses the role of axillary management via ALND or axillary radiation therapy compared to no further management for patients who have 1 or 2 lymph nodes macro-metastases on SLNB. The MA39trial (NCT03488693) randomizes patients with pT1-2N1, who underwent mastectomy or BCS to regional nodal irradiation (RNI) or no RNI.30 For patients with clinically positive nodes pre neoadjuvant chemotherapy (NACT), the Alliance A011202 (NCT01901094) randomize patients with cT1-3N1 with positive SLNB into ALND followed by RNI compared to RNI without ALND, while the NSABP B-51/RTOG 1304 trial (NCT01872975), randomizes cT1-3N1 patients with negative SLNB to RNI compared to no RNI.31
Despite the fact that most of these trials were not strict for elderly groups, the results of these trials would aid decision making for different scenarios based on tumor response and SLNB findings, especially for older groups in whom any possible de-escalated therapy would make a difference in their quality of life, without compromising the oncological outcomes.
Oncoplastic Surgery
A comprehensive review for reconstructive surgeries for older women with breast cancer showed equivalent outcomes to younger age groups, yet these patients are less likely to be offered these reconstructive techniques, due to lack of care standards, concerns related to operative risks, preconceptions to body image and lack of engagement in decision making with patients.32 In one study, physical and psychosocial well-being scores were significantly higher in older women compared to younger age group for both conventional surgical techniques and oncoplastic surgeries.33
Adjuvant Therapy
Adjuvant Chemotherapy
Older patients can derive survival benefit from adjuvant chemotherapy; however, they are at a higher risk of developing adverse events such as acute kidney injury, electrolyte imbalance, cardiac and hematological toxicities.34 Those with high-risk, HER2-positive or triple negative disease, will derive greater benefit from adjuvant chemotherapy compared to HER2-negative and hormone sensitive breast cancer.35 In a study that included 592 breast cancer patients older than 70 years with comorbidities and lymph node positive disease, patients who received adjuvant chemotherapy had better survival compared to those who did not (Hazard Ratio 0.67, 95% CI 0.48–0.98).36 In a SEER database study of 5000 patients 65 years and older with non-metastatic hormone receptor-negative breast cancer, adjuvant chemotherapy resulted in 15% reduction in mortality that was mainly seen in patients with larger tumors and positive lymph nodes.37 On the other hand, a Medicare study showed that patients older than 65 years have a higher risk of short-term mortality and hospitalization after receiving chemotherapy compared to younger patients.38 Another analysis of SEER database showed that 2.9% of patients older than 65 years with early breast cancer died after one year of receiving chemotherapy.39
HER2-Negative Breast Cancer
The standard chemotherapeutic regimens that can be offered for patients older than 65 years with HER2-negative breast cancer are docetaxel and cyclophosphamide (TC), anthracycline based regimens such as doxorubicin and cyclophosphamide followed by paclitaxel (AC-T), or the older regimen cyclophosphamide, methotrexate, and fluorouracil (CMF). The choice of regimen depends on clinical status (fit versus non-fit), disease risk (high versus low risk), cardiac function and other comorbidities. In the CALGB-49907 trial, 633 patients 65 years or older with stage I–IIIB were randomized to receive CMF or AC versus single agent capecitabine. At 10-years, relapse-free survival (RFS) was worse with capecitabine compared to CMF or AC (50% vs 56%), as were OS rates (26% vs 62%). Toxicities, however, were less common in the capecitabine arm.40 In the ICE Phase III trial, patients older than 65 were randomized to receive adjuvant ibandronate with or without capecitabine. Results showed no OS or disease-free survival (DFS) benefit of adding capecitabine to ibandronate.41 Single agent docetaxel was compared to CMF in a cohort of 601 older patients in the ELDA randomized trial and was found to be not superior, while causing worse quality of life (QOL) and multiple side effects such as hair loss, fatigue, diarrhea, rash, and neuropathy.42
For medically fit older patients with normal cardiac function and high-risk disease (node positive, larger tumors, and triple-negative tumors >1cm) anthracycline-based regimens (AC-T) have been shown to result in better outcomes compared to CMF.43 However, the benefit of treatment should be weighed against the risk of major toxicities such as hematological and cardiac toxicities. In the CALGB 40101 trial, 3800 patients with lower-risk disease were randomized to four or six cycles of paclitaxel administered weekly or bi-weekly versus AC, noninferiority was not demonstrated and patients who received paclitaxel had worse OS (Hazard Ratio 1.27). Grade 3 or higher hematological toxicities were more common in the AC arm, whereas neuropathy was more common in the paclitaxel arm. Two patients receiving AC had cardiac deaths and 7 patients developed myelodysplastic syndrome (MDS) and acute myelogenous leukemia (AML).44 In a large SEER database study evaluating the risk of cardiac toxicity after anthracycline-based regimens, the rates of developing congestive heart failure (CHF) in patients aged 66–70 years who received anthracyclines were 19% and 38% at 5 and 10 years, respectively; whereas the 5- and 10-year rates were 18% and 33% in those who received non-anthracycline-based regimens.45
In older patients with lower risk disease (lymph node negative, hormone receptor-positive, triple- negative tumors <1cm) or those with comorbidities precluding the use of anthracycline-based regimen, TC can be an appropriate regimen. In the US Oncology Research Trial 9735, patients were randomized to receive adjuvant AC or TC for four cycles. At 7-years of follow up, patients in the TC arm had better DFS (81% vs 75%, P=0.033, Hazard Ratio 0.74) and OS (87% vs 82%, P=0.32, Hazard Ratio 0.69) compared to the AC arm. The survival benefit was consistent in older (≥65 years) and younger patients; however, older patients developed more febrile neutropenia with TC necessitating Granulocyte Colony-Stimulating Factor (G-CSF) prophylaxis.46 In a joint analysis of the ABC trials, TC was compared to an anthracycline-based regimen in more than 4000 patients; 30% of whom were ≥60 years old. In terms of invasive DFS, TC was inferior to anthracycline-based regimens; however, anthracycline-based regimens did not significantly improve outcomes in patients with hormone receptor-positive or triple-negative, lymph node negative disease.47 Clinical frailty and QOL declined in the first three months after receiving TC but recovered fully at one year.48 Table 1 summarizes important clinical trials addressing the use of adjuvant chemotherapy in patients with HER2-negative disease.
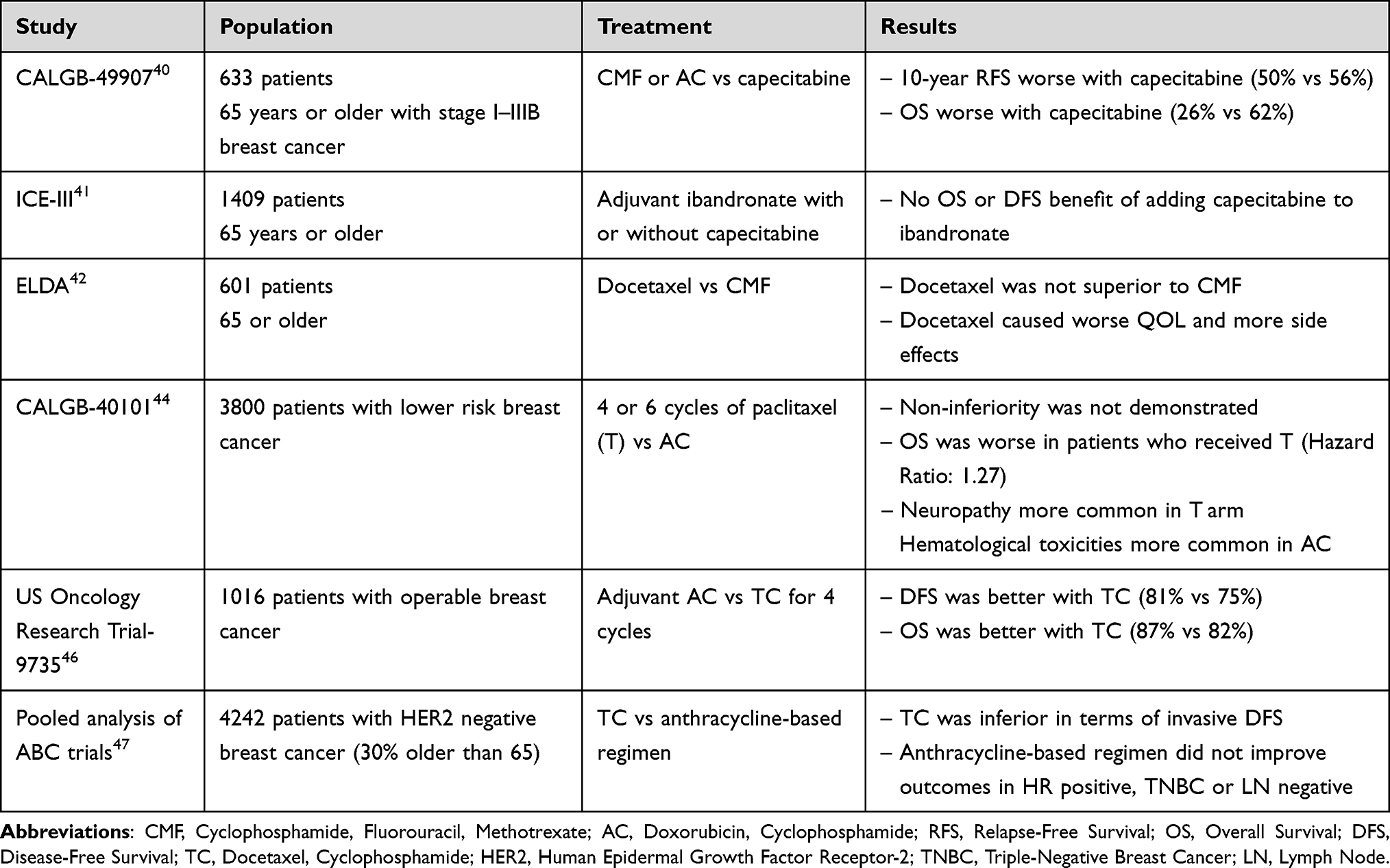 |
Table 1 Chemotherapy Clinical Trials for Patients with HER2-Negative Breast Cancer |
HER2-Positive Breast Cancer
In a systematic review of the randomized trials evaluating the use of adjuvant trastuzumab in addition to chemotherapy in patients older than 60 years, the addition of trastuzumab resulted in a 47% relative risk reduction compared to chemotherapy alone (Hazard Ratio 0.53, 95% CI 0.36–0.77) and 5% of patients receiving trastuzumab had cardiac events.49 In a Phase II randomized trial from Japan, 275 older patients (median age 73.5 years) were randomized to receive chemotherapy plus trastuzumab or trastuzumab alone. Single agent trastuzumab failed to show noninferiority but was well tolerated and resulted in fewer side effects compared to the combination.50
For higher-risk fit patients, a combination of trastuzumab plus anthracycline-taxane can be used. However, cardiac toxicity is a major issue when trastuzumab is used along with an anthracycline, moreover anthracycline-taxane-trastuzumab combinations were mainly studied in younger fit populations with poor representation of patients >60 years.51 Another option is taxane-anti-HER2 combinations such as docetaxel, carboplatin and trastuzumab (TCH) regimen but patients older than 70 years were excluded from the BCIRG 001 trial, besides hematological toxicity is a concern in older patients receiving carboplatin with docetaxel.52 Two studies showed positive results with the combinations of paclitaxel plus trastuzumab, and TC plus trastuzumab; placing them among the options for older patients.53,54 In terms of duration, one year of adjuvant trastuzumab should be administered in older patients similar to the recommendation for younger patients.55
The rate of CHF in patients ≥66 years treated with trastuzumab is 29% compared to 19% in patients treated without trastuzumab.56 Although echocardiogram is recommended every 3 months in patients receiving trastuzumab, older patients are less likely to undergo cardiac monitoring.57
In the Aphinity trial, pertuzumab was added to trastuzumab and resulted in a minor decrease in invasive DFS and higher rates of diarrhea which might be detrimental in older patients.58 The same case is with neratinib that showed DFS benefit following adjuvant trastuzumab in the ExteNET trial but caused significant diarrhea necessitating the use of prophylactic antidiarrheal medications which carries the risk of dehydration and constipation in older patients.59
In the KATHRINE trial, adjuvant trastuzumab emtansine (T-DM1) reduced the risk of recurrence compared to trastuzumab in patients with residual disease after receiving trastuzumab-based neoadjuvant treatment. However, T-DM1 caused significant toxicities such as neuropathy and pneumonitis which can be serious in older patients. Additionally, less than 10% of the study population were ≥65 years old.60 Table 2 summarizes important clinical trials addressing the use of adjuvant chemotherapy and anti-HER2 therapy in patients with HER2-positive patients.
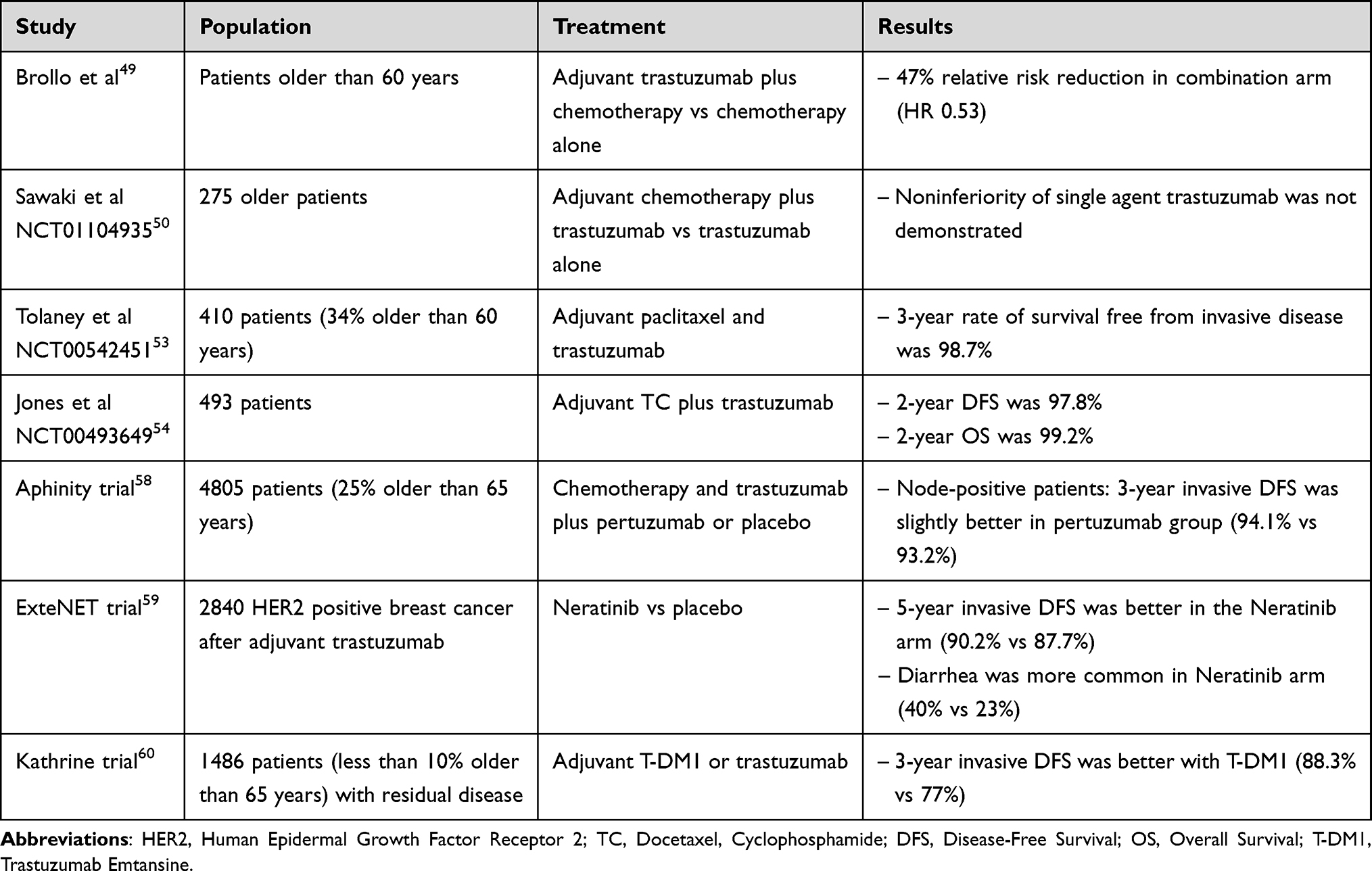 |
Table 2 Chemotherapy Clinical Trials for Patients with HER2-Positive Breast Cancer |
Adjuvant Radiotherapy
Adjuvant radiation has been proven to decrease locoregional relapse in breast cancer. For elderly patients, radiation therapy can be recommended based on risk stratification; as it might be safely omitted for low-risk group.61 Older patients carry higher risk of radiation-related toxicities due to accumulative effect related to heart and respiratory comorbidities. However, recent advances in radiation therapy and utilization of modern organ sparing techniques, resulted in better understanding of underlying factors that may enhance toxicities.62,63
Hypofractionated Radiation Therapy
Moderate hypofractionation radiation therapy over 3 weeks has been shown to be equivalent to conventional 5 weeks treatment with similar or better cosmetic outcomes, leading to better tolerance of the treatment course with less hospital visits.64–66 Another study, the FAST-forward, evaluated ultra-hypofractionated radiation therapy over one week time, as 26Gy in 5 fractions, compared to moderate hypofractionation, as 40Gy in 15 fractions. At five years follow up, ultra-hypofractionation technique was shown to be as safe, and as effective. In their report, more than 50% of patients were above the age of 60 and 15% were above 70 years in each arm, providing another de-escalated form of radiation delivery for elderly group.67
Partial Breast Irradiation
The efficacy of partial breast irradiation (PBI) for early-stage breast cancer was addressed in the UK IMPORT LOW trial and reported non-inferiority in local relapse for PBI, with equivalent or fewer late normal-tissue adverse events.68 The RAPID trial compared whole breast irradiation (40Gy over 15 fractions or 50Gy over 25 fractions) to accelerated partial breast irradiation (APBI) with 38.5Gy over 10 fractions (twice daily). Local control was similar, but higher acute toxicity was observed in whole breast radiation group, while APBI arm carried higher late toxicity. The mean age in the studied groups was 61 years (ranged 54–68).69 The APBI-IMRT-Florence trial randomized patients with early-stage breast cancer to APBI, using intensity modulated radiation therapy (IMRT) as 30Gy over 5 fractions, or conventional 50Gy over 25 fractions. The APBI arm had significantly less acute toxicity, late toxicity and better cosmetic outcomes. Patients 60 or above represented more than 50% in both arms, and 70 or more of age were 22% in each arm.70 Another study used interstitial brachytherapy APBI to avoid whole breast irradiation for early-stage breast cancer in women 66 year of age or older resulted in high mastectomy-free survival and reasonable local control.71
Omission of Radiotherapy
Despite the long-term local control benefit of adjuvant radiation therapy for early-stage breast cancer,72 that was also reflected in older patients’ age group in a meta-analysis by Matuschek et al, the idea of omitting radiation therapy remains tempting to avoid radiation related morbidities and decrease patient hospital visits for elderly low-risk hormone receptor-positive patients.73 The CALGB 9343 trial randomized patients 70-year-old or more, clinically staged T1N0, ER-positive to receive tamoxifen plus radiation therapy or tamoxifen alone following lumpectomy. Long term results have shown small locoregional recurrence difference in favor of radiation arm but it was not reflected into significant difference in time to mastectomy, time to distant metastases, BCSS or OS.74 The PRIME II trial compared adjuvant radiation omission to adjuvant whole breast radiotherapy (WBRT) for patients 65 or older with primary tumor <3cm, node negative and hormone receptor- positive disease, found better local control for WBRT arm, with comparable quality of life in both arms.75
Adjuvant Radiation in Neoadjuvant Chemotherapy Settings
The role of adjuvant radiation therapy following adjuvant chemotherapy for locally-advanced breast cancer is well known. However, in the era of neoadjuvant chemotherapy, the role of adjuvant radiation therapy based on chemotherapy response is not well established. A recent meta-analysis showed reduced risk of locoregional recurrence following adjuvant locoregional radiation therapy for clinically lymph node involvement with complete response following neoadjuvant chemotherapy with no statistical difference on DFS or OS.76 Mandish et al, reported in their ASTRO 2020 abstract, that adjuvant radiation omission for patients above 70-year-old of age following BCS with complete response does not impact OS.77 Some unanswered questions for clinical scenarios based on chemotherapy response for initially clinically-positive nodal disease are being addressed in ongoing trials discussed in surgery section.
These findings can be translated with caution to omit radiation for elderly patients who undergo mastectomy or BSC with complete response in elderly group based on other factors for risk assessment.
Radiation Therapy in Precision Medicine Era
The past decade witnessed the evolution of several tools for radiation therapy patient selection in adjuvant settings, tailoring treatment based on genomic biomarkers to obtain higher benefit and minimize potential toxicity. A 7-gene signature tools was developed from the Danish 82b and 82c trials to identify low-risk group for which postmastectomy radiation therapy had no benefit.78 Another study used a 41-gene classifier to identify patients who are unlikely to respond to adjuvant radiation therapy requiring treatment intensification.79 A 10-gene radiation sensitivity index (RSI) and genomically adjusted radiation dose (GARD) were generated by research group from Moffit cancer center offering a predictive biomarker designed for breast cancer radiation therapy.80–82 To assess the potential benefit of adjuvant radiation for Ductal carcinoma in situ (DCIS), the Oncotype-Dx score83 and DecisionRT84 were developed as selection tools to mark patients who benefit of adjuvant radiation therapy post BCS.
The results of the current ongoing trials will add another layer of information to guide clinical decisions in personalized fashion. The IDEA85 (NCT02400190) is a single arm Phase 2 trial evaluates radiation therapy omission for Oncotype-Dx score ≤18, while LUMINA86 (NCT01791829) studies the omission of radiation following BCS in low-risk luminal-A subtype. The PRECISION trial87 (NCT02653755) assesses radiation therapy omission safety for PAM50 low-risk patients following BCS. For low-risk (Oncotype-Dx ≤18, ER-positive, HER2-negative), node positive disease, the TAILOR RT30 (NCT03488693) addresses the impact of avoidance of regional nodal irradiation.
Adjuvant Endocrine Therapy
In elderly women with early-stage breast cancer, endocrine therapy can be offered as the only treatment modality (primary endocrine therapy) and can also be offered in the neoadjuvant setting replacing the more toxic chemotherapy, or in the usual adjuvant setting following surgical resection alone or surgery and chemotherapy.
A retrospective cohort of 504 patients; all were older than 65 years, with T1-2N0, hormone receptor-positive breast cancer treated with BCS were analyzed.88 Around two thirds of the patients (n=311) were treated with adjuvant radiotherapy and endocrine therapy, while 193 patients were treated with radiotherapy alone. Non-adherence to endocrine therapy predicted for higher risk of distant metastasis (Hazard Ratio, 5.03; 95% CI, 1.98–12.66) and worse DFS (Hazard Ratio, 4.24; 95% CI, 1.9–10.3). On the other hand, 83.8% of the patients who developed distant metastasis had tumors more than 1 cm in size which points that radiotherapy alone can be an appropriate option for women with tumors ≤ 1 cm especially if significant side effects from endocrine therapy are expected.
Another study from Korea Breast Cancer Registry investigated 53,582 patients who had curative surgery for breast cancer between 2005 and 2010. The primary end point was OS difference between elderly group (older than 75 years) and younger group (less than 75 years). Elderly patients had higher stages, but were less likely to receive adjuvant treatment. The use of adjuvant endocrine therapy in elderly patients was associated with better OS (adjusted OR 0.417; 95% CI, 0.240–0.726; p= 0.002).89
In a review of 483 women aged 70 years or older treated with BCS for stage I–III hormone receptor- positive breast cancer, and after adjustment for confounding factors, a significant advantage in OS (Hazard Ratio 0.44; 95% CI 0.25–0.77; p= 0.004) and DFS (Hazard Ratio 0.42; 95% CI 0.28–0.64; p < 0.01) were gained from adjuvant endocrine therapy.90 However, another study on 224 patients aged 65 years or older with low risk, hormone receptor-positive, early-stage (T1N0M0) disease showed no significant difference in 10-year contralateral breast relapse or in OS between patients who did and did not receive adjuvant tamoxifen.91
Given the conflicting results, and failure to come up with a model predictive of response, tolerance and adherence to endocrine therapy,92 the decision to offer adjuvant endocrine therapy for older woman should be individualized after careful assessment of the cancer recurrence risk and the possible side effects of treatment, and with consideration of the patient’s preference.
Neoadjuvant Endocrine Therapy
Neoadjuvant endocrine therapy can be a suitable option for elderly patients with inoperable hormone receptor-positive breast cancer. A multicenter study randomized 337 postmenopausal women with hormone receptor-positive breast cancer to letrozole or tamoxifen for 4 months, the overall response rate was significantly higher in the letrozole group.93 Another trial compared letrozole or anastrozole to tamoxifen, concluded that letrozole and anastrozole showed similar efficacy, and both had a better clinical response compared to tamoxifen.94 Exemestane was also tested in the neoadjuvant setting in a phase II trial. Postmenopausal patients (n=42) with locally advanced hormone receptor-positive breast cancer were given exemestane for 16 weeks and the overall clinical response was 73.3%.95
Compared to tamoxifen, researchers found that aromatase inhibitors (AI) when used as first line treatment in the neoadjuvant setting, are associated with higher objective response rates and increased rate of BCS with all three available AI demonstrating equivalent benefit. It’s also advisable to extend the duration of neoadjuvant treatment beyond 3 or 4 months, for at least 6 months, or even until maximal clinical response.96 Evidence on using other endocrine agents like CDK 4/6 inhibitors and everolimus in the neoadjuvant setting is still immature.97
Primary Endocrine Treatment (PET)
Clinicians tend to offer definitive endocrine therapy rather than surgery for elderly women with newly diagnosed nonmetastatic estrogen receptor-positive breast cancer.98 A systematic review of 7 randomized controlled trials in older women compared primary endocrine therapy (Tamoxifen) with surgery alone or surgery followed by adjuvant tamoxifen. Surgery alone compared to primary endocrine therapy showed no significant OS benefit but a significant PFS difference. (Hazard Ratio 0.55, 95% CI 0.39–0.77, p=0.0006). When surgery followed by adjuvant tamoxifen was compared to primary endocrine therapy, a significant difference in PFS (Hazard Ratio 0.65, 95% CI 0.53–0.81, p=0.0001), but not OS, was observed. However, one of the studies included showed a higher psychosocial morbidity at 3 months post-surgery which resolved by 2 years.99
A more recently published review showed almost similar results, but with a non-statistically significant trend for improved OS with surgery followed by adjuvant endocrine therapy.100 Another review by Johnston et al evaluated randomized trials comparing surgery with primary endocrine therapy in elderly women with operable, non-metastatic breast cancer showed no significant difference in survival, although most trials were small.101
Another study from UK showed that most of the interviewed healthcare professionals thought that primary endocrine treatment is not suitable for patients below 80 years unless they had significant comorbidities, and patient preference was the most important factor when discussing treatment options.102
A cohort of 5150 female Medicare beneficiaries with new prescription of tamoxifen or AI between 2007 and 2010 was analyzed for adherence and persistence. Adherence was defined as having the ET on 80% or more of the days covered while persistence was defined as continuation of ET for at least one year period or until death, whichever came first. With a mean age of 76.4 years, non-adherence was observed in 41% and non-persistence in 49%, with exemestane having the least adherence and persistence, followed by letrozole and then anastrozole. Patients on tamoxifen had best compliance.103 Physicians should therefore carefully assess compliance of their patients on the prescribed endocrine therapy and if poor compliance is an issue other alternative local treatments should be discussed like surgery and/or radiotherapy.104
In another study that utilized the SEER database from 2001 to 2015, a total of 552 elderly women with stage I–III ER-positive breast cancer were evaluated; 82% being 80 years or older. All patients were treated with primary endocrine therapy, the authors concluded that adherence to endocrine therapy was not associated with statistically significant reduction in risk of death from breast cancer, but this can be explained by the fact that patients who were adherent to treatment were more likely to have larger tumors which means a significant bias in this conclusion.105
Metastatic Disease
The goal of treatment for any patient, regardless of the age, with metastatic breast cancer is palliative; control the cancer while maintaining the patient’s performance status and QOL. Older patients with metastatic breast cancer generally have worse survival rates compared to younger ones.106
Chemotherapy
Chemotherapy may be offered in the first line for older patients with metastatic breast cancer when the disease is rapidly progressing and threatening organ function.107 In older patients, especially those who are unfit, it is recommended to use single agent as opposed to combination chemotherapy.108 The choice of agent should be based on the side effect profile, the patient’s comorbidities, and preference status.104
Capecitabine is an oral chemotherapy that is effective in older patients and usually better tolerated if started at a lower dose (1000 mg/m2 twice daily). In a trial involving 73 patients ≥65 years with treatment-naïve metastatic breast cancer, capecitabine showed an overall response rate (ORR) of 37% with grade 3–4 adverse events (AEs) occurring in <10% of the patients.109
Vinorelbine is an active medication when used as a single agent in older patients with metastatic disease, neutropenia could be a dose-limiting AE. One trial evaluated vinorelbine in a first line setting in 56 patients ≥60 years and showed a response rate of 38% with 2 complete responses, 45 (80%) patients had at least one episode of grade 3–4 neutropenia.110 Erbulin, antimicrotubule agent, was shown to be effective in heavily pretreated patients. In a trial involving 93 patients ≥70 years, erbulin showed a PFS of 4.1 months, however, 25% of the patients needed dose reduction due to AEs.111
Taxanes are highly effective agents for metastatic breast cancer in the first line setting and pretreated patients. In a phase II randomized trial evaluating weekly paclitaxel vs weekly docetaxel in older unfit patients, weekly paclitaxel showed a better response rate (72% vs 54%) that was more pronounced in patients ≥70 years (67% vs 44%). Time to progression was longer with weekly paclitaxel as well (21 vs 13 weeks). Weekly paclitaxel caused more anemia, whereas- weekly docetaxel caused more edema and fatigue.112
Anthracyclines are effective in treating metastatic breast cancer. However, the risk of cardiac toxicity is higher in older patients which necessitates close monitoring with echocardiogram. Pegylated liposomal doxorubicin carries a lower risk of cardiac toxicity when compared to conventional doxorubicin, and hence it is the preferred anthracycline in older patients with metastatic disease.113 Two studies evaluated liposomal doxorubicin in older patients ≥65 who were treatment naïve or medically unfit. Overall response rate was 30% and AEs included anorexia, fatigue, hematological toxicities, and stomatitis.114,115
In older patients with HER2-positive metastatic breast cancer, anti-HER2 therapy should be used in combination with endocrine therapy or chemotherapy. The RegistHER study included 209 patients ≥65 years with HER2-positive metastatic breast cancer, 50% of which had hormone receptor-positive disease. Patients who received trastuzumab had better PFS compared to those who did not (11.7 vs 4.6 months, respectively). Patients ≥75 years had the highest rate of cardiac events compared to patients aged 65–74 years (25.4% versus 6.7%). However, only 3.2% (compared to <2.0% in younger patients) had CHF.116 In the EORTC 75111–10,114 phase II trial, 80 patients ≥60 years with HER2-positive metastatic breast cancer were randomized to receive trastuzumab and pertuzumab with or without oral cyclophosphamide. At median follow up of 20.7 months, patients who received trastuzumab, pertuzumab and cyclophosphamide had better PFS compared to those who received trastuzumab and pertuzumab alone (12.7 vs 5.6 months, respectively). Upon disease progression, patients were allowed to start T-DM1 which was given for 22 patients and had a PFS of 5 months. More than 50% of the patients receiving pertuzumab had diarrhea which can be serious in older adults.117 Table 3 summarizes clinical trials addressing the systemic therapy for patients with metastatic disease.
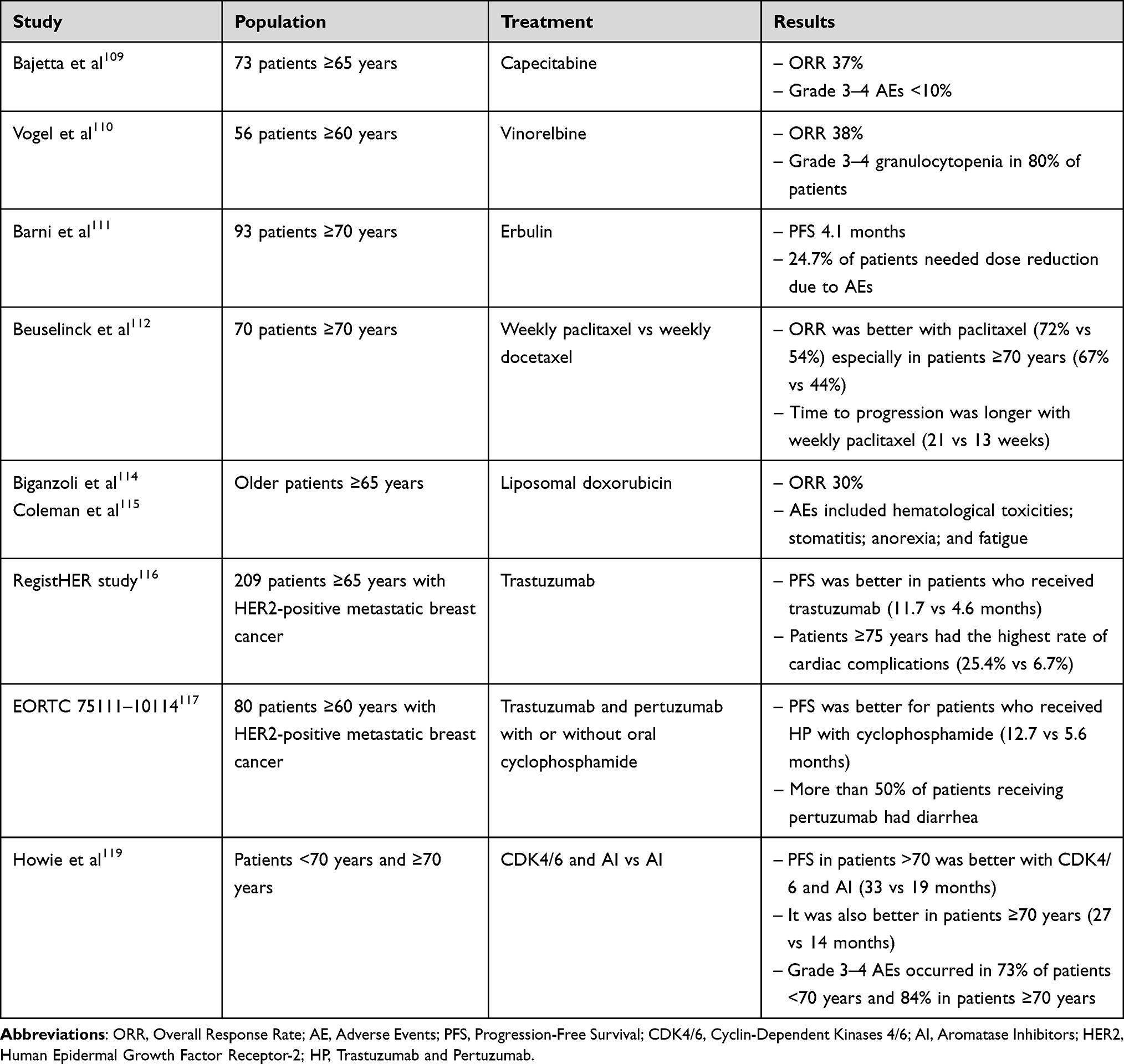 |
Table 3 Clinical Trials for Metastatic Disease |
Endocrine Therapy for Metastatic Disease
Recent studies had established CDK4/6 inhibitors, with AI or fulvestrant, as the treatment of choice for patients with hormone receptor-positive, HER2-negative metastatic breast cancer. All three CDK4/6 inhibitors; palbociclib, ribociclib and abemaciclib, are effective and tolerable treatment in older adults.118 An FDA pooled analysis from three randomized controlled trials (n=1827) of different CDK4/6 inhibitors combined with AI for the first line treatment of postmenopausal women with hormone receptor-positive metastatic breast cancer was conducted to evaluate the effect of age on treatment outcomes and toxicities. Patients aged 75 years or older (n=198) treated with a CDK4/6 inhibitor and an AI had a median PFS of 31.1 months (95% CI, 20.2 months to not reached) compared with 3.7 months (95% CI, 10.9–24.9) for patients treated with an AI alone. The incidence of grade 3–4 adverse events was 88.8% in patients aged 75 years or older compared with 73.4% in younger patients. The most common AE in patients ≥70 years were fatigue, acute kidney injury and neutropenia.119
Another pooled analysis of the randomized PALOMA trials, evaluated the outcomes in patients aged 65 or older when treated with palbociclib and endocrine therapy, including letrozole or fulvestrant. In patients treated with palbociclib and letrozole (n=218), the median PFS was improved for patients aged 65–74 years (Hazard Ratio, 0.66; 95% CI, 0.45–0.97; p= 0.016) and in older group (≥75 years) (Hazard Ratio, 0.31; 95% CI, 0.16–0.61; p<0.001). Additionally, treatment with palbociclib and fulvestrant (n=86) showed a significant benefit in patients aged 65–74 years (Hazard Ratio, 0.27; 95% CI, 0.16–0.48; p<0.001), while only few patients aged 75 years or older were given this combination resulting in a nonsignificant difference. Myelosuppression was more common in patients aged 75 or older but grade 3 or higher myelosuppression was similar among all age groups, and quality of life was maintained in this elderly population.120
A review of the trials comparing endocrine therapy alone versus combinations with targeted agents showed that efficacy was similar in different age-stratified subgroups, with a reduced risk of disease progression when endocrine therapy was combined with everolimus, palbociclib, or ribociclib, but this benefit was on the expense of worse tolerability. Discontinuation rates were not different in elderly patients treated with CDK4/6 inhibitors, but a higher rate of discontinuation was noted in patients aged 70 years or older when receiving everolimus and exemestane.118
Another study focused on elderly patients treated with everolimus-exemestane from the EVA study. Among the 404 patients included in the trial, 154 (38.1%) were 65 years or older. Median duration of treatment was 28.5 weeks in patients aged 65–69 years, and 24.4 weeks in older (≥70 years). Grade 3–4 toxicities were seen in 55 (35.7%) patients, and were mainly stomatitis (10.9%), rash (5.8%) and non-infectious pneumonitis (3.6%). Weight loss and anemia were observed specifically in patients aged 70 years or older.121
Safety and efficacy data in elderly patients were reported after an 18 months median follow up of the phase III randomized trial (BOLERO-2), where patients with advanced hormone receptor positive breast cancer were randomized to receive everolimus-exemestane combination versus exemestane and placebo after treatment with a nonsteroidal AI. Combination treatment resulted in improved PFS regardless of age [hazard ratio, 0.59 (≥ 65 years) and 0.45 (≥ 70 years)]. Adverse events included stomatitis, rash, pneumonitis, infections and hyperglycemia occurred in similar incidences in younger and older patients, but on-treatment deaths were higher in the elderly group, so this treatment combination can be considered in older patients but needs careful monitoring and management of adverse events with appropriate treatment interruptions and dose reductions.122
A descriptive study evaluated medical reports of 51 older patients aged 65 years or older treated with alpilisib outside clinical trials. Median age was 71 years and median time on drug was 2.6 months; 15 (29.4%) patients stopped alpilisib for adverse events, which included hyperglycemia, diarrhea, rash, fatigue and mucositis with 5 patients needed hospitalization for hyperglycemia.123
Conclusions
Management of breast cancer in geriatric age group is a challenging task, yet it is extremely important to be mastered by the caring team. In an era of population ageing, clinical decisions should be optimized based on several factors rather than patients’ age alone. These factors are related to patients’ comorbidities, performance status, life expectancy and tumor pathological and molecular characteristics. Proper geriatric assessment, a process that is not practiced by many, is extremely important to hopefully avoid unnecessary undertreatment or expose patients to intolerable toxicities. The introduction of “geriatric oncology” as a specialty with proper focused training for oncologists across all field of oncology, will hopefully improve the care of such very vulnerable group of patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Siegel RL, Miller KD, Fuchs HE, Jemal A. Cancer statistics, 2022. CA Cancer J Clin. 2022;72(1):7–33. doi:10.3322/CAAC.21708
2. Cancer statistics review, 1975–2018 - SEER statistics; 2022. Available from: https://seer.cancer.gov/archive/csr/1975_2018/.
3. DeSantis CE, Ma J, Gaudet MM, et al. Breast cancer statistics, 2019. CA Cancer J Clin. 2019;69(6):438–451. doi:10.3322/CAAC.21583
4. Shachar SS, Hurria A, Muss HB. Breast cancer in women older than 80 years. J Oncol Pract. 2016;12(2):123–132. doi:10.1200/JOP.2015.010207
5. Markopoulos C, van de Water W, van de Velde CJ. Breast cancer in the elderly: reducing the losses. Future Oncol. 2013;9(9):1253–1256. doi:10.2217/FON.13.120
6. Hutchins LF, Unger JM, Crowley JJ, Coltman CA, Albain KS. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N Engl J Med. 1999;341(27):2061–2067. doi:10.1056/NEJM199912303412706
7. Smith-Graziani D, Lei X, Giordano SH, Zhao H, Karuturi M, Chavez-MacGregor M. Delayed initiation of adjuvant chemotherapy in older women with breast cancer. Cancer Med. 2020;9(19):6961–6971. doi:10.1002/CAM4.3363
8. Abu-Gheida I, Hammoudeh L, Abdel-Razeq H. Controversies of radiation therapy omission in elderly women with early stage invasive breast cancer. Transl Cancer Res. 2020;9(Suppl 1):S126. doi:10.21037/TCR.2019.06.47
9. Huang XZ, Chen Y, Chen WJ, et al. Effect of radiotherapy after breast-conserving surgery in older patients with early breast cancer and breast ductal carcinoma in situ: a meta-analysis. Oncotarget. 2017;8(17):28215. doi:10.18632/ONCOTARGET.15998
10. Bouchardy C, Rapiti E, Fioretta G, et al. Undertreatment strongly decreases prognosis of breast cancer in elderly women. J Clin Oncol. 2003;21(19):3580–3587. doi:10.1200/JCO.2003.02.046
11. Wildiers H, Kunkler I, Biganzoli L, et al. Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology. Lancet Oncol. 2007;8(12):1101–1115. doi:10.1016/S1470-2045(07)70378-9
12. Parks R, Cheung KL. Challenges in geriatric Oncology-A surgeon’s perspective. Curr Oncol. 2022;29(2):659–674. doi:10.3390/CURRONCOL29020058
13. Ward SE, Richards PD, Morgan JL, et al. Omission of surgery in older women with early breast cancer has an adverse impact on breast cancer-specific survival. Br J Surg. 2018;105(11):1454–1463. doi:10.1002/BJS.10885
14. Yin M, Verschraegen C, Vincent VH, Patel SM, George T, Truica CI. Impact of lack of surgery on outcomes in elderly women with nonmetastatic breast cancer-A surveillance, epidemiology, and end results 18 population based study. Medicine. 2020;99(3):e18745. doi:10.1097/MD.0000000000018745
15. Morgan JL, George J, Holmes G, et al. Breast cancer surgery in older women: outcomes of the Bridging Age Gap in Breast Cancer study. Br J Surg. 2020;107(11):1468–1479. doi:10.1002/BJS.11617
16. Morgan JL, Walters SJ, Collins K, et al. What influences healthcare professionals’ treatment preferences for older women with operable breast cancer? An application of the discrete choice experiment. Eur J Surg Oncol. 2017;43(7):1282–1287. doi:10.1016/J.EJSO.2017.01.012
17. Peters E, Anzeneder T, Jackisch C, et al. The treatment of primary breast cancer in older women with adjuvant therapy: a retrospective analysis of data from over 3000 patients from the PATH biobank, with two-year follow-up. Deutsches Ärzteblatt International. 2015;112(35–36):577. doi:10.3238/ARZTEBL.2015.0577
18. Martelli G, Miceli R, Costa A, et al. Elderly breast cancer patients treated by conservative surgery alone plus adjuvant tamoxifen: fifteen-year results of a prospective study. Cancer. 2008;112(3):481–488. doi:10.1002/CNCR.23213
19. Soyder A, Özbaş S, Koçak S. Locoregional recurrence and survival rates after breast-conserving surgery and hormonal therapy in 70-year-old or older patients with Stage I or IIA breast carcinoma. Breast Care. 2013;8(2):134. doi:10.1159/000350776
20. Mandelblatt JS, Edge SB, Meropol NJ, et al. Sequelae of axillary lymph node dissection in older women with stage 1 and 2 breast carcinoma. Cancer. 2002;95(12):2445–2454. doi:10.1002/CNCR.10983
21. Rudenstam CM, Zahrieh D, Forbes JF, et al. Randomized trial comparing axillary clearance versus no axillary clearance in older patients with breast cancer: first results of International Breast Cancer Study Group Trial 10–93. J Clin Oncol. 2006;24(3):337–344. doi:10.1200/JCO.2005.01.5784
22. Wang Z, Wu LC, Chen JQ. Sentinel lymph node biopsy compared with axillary lymph node dissection in early breast cancer: a meta-analysis. Breast Cancer Res Treat. 2011;129(3):675–689. doi:10.1007/S10549-011-1665-1
23. Christian N, Heelan Gladden A, Friedman C, et al. Increasing omission of radiation therapy and sentinel node biopsy in elderly patients with early stage, hormone-positive breast cancer. Breast J. 2020;26(2):133–138. doi:10.1111/TBJ.13483
24. Sun J, Mathias BJ, Sun W, et al. Is it wise to omit sentinel node biopsy in elderly patients with breast cancer? Ann Surg Oncol. 2021;28(1):320–329. doi:10.1245/S10434-020-08759-1
25. Liang S, Hallet J, Simpson JS, Tricco AC, Scheer AS. Omission of axillary staging in elderly patients with early stage breast cancer impacts regional control but not survival: a systematic review and meta-analysis. J Geriatr Oncol. 2017;8(2):140–147. doi:10.1016/J.JGO.2016.12.003
26. Xu L, Wen N, Qiu J, et al. Predicting survival benefit of sparing sentinel lymph node biopsy in low-risk elderly patients with early breast cancer: a population-based analysis. Front Oncol. 2020;10:1718. doi:10.3389/FONC.2020.01718/BIBTEX
27. Sentinel node biopsy in breast cancer: omission of axillary clearance after macrometastases. A Randomized Trial. - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02240472.
28. Axillary node dissection versus no dissection in breast cancer with positive sentinel lymph node - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT01717131.
29. POSNOC - A trial looking at axillary treatment in early breast cancer - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02401685.
30. Regional radiotherapy in biomarker low-risk node positive and T3N0 breast cancer - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT03488693.
31. Standard or comprehensive radiation therapy in treating patients with early-stage breast cancer previously treated with chemotherapy and surgery - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT01872975.
32. James R, McCulley SJ, Macmillan RD. Oncoplastic and reconstructive breast surgery in the elderly. Br J Surg. 2015;102(5):480–488. doi:10.1002/BJS.9733
33. Ritter M, Ling BM, Oberhauser I, et al. The impact of age on patient-reported outcomes after oncoplastic versus conventional breast cancer surgery. Breast Cancer Res Treat. 2021;187(2):437–446. doi:10.1007/S10549-021-06126-6
34. Lichtman SM, Cirrincione CT, Hurria A, et al. Effect of pretreatment renal function on treatment and clinical outcomes in the adjuvant treatment of older women with breast cancer: alliance A171201, an ancillary study of CALGB/CTSU 49907. J Clin Oncol. 2016;34(7):699–705. doi:10.1200/JCO.2015.62.6341
35. Giordano SH, Duan Z, Kuo YF, Hortobagyi GN, Goodwin JS. Use and outcomes of adjuvant chemotherapy in older women with breast cancer. J Clin Oncol. 2006;24(18):2750–2756. doi:10.1200/JCO.2005.02.3028
36. Tamirisa N, Lin H, Shen Y, et al. Association of chemotherapy with survival in elderly patients with multiple comorbidities and estrogen receptor-positive, node-positive breast cancer. JAMA Oncol. 2020;6(10):1548–1554. doi:10.1001/JAMAONCOL.2020.2388
37. Elkin EB, Hurria A, Mitra N, Schrag D, Panageas KS. Adjuvant chemotherapy and survival in older women with hormone receptor-negative breast cancer: assessing outcome in a population-based, observational cohort. J Clin Oncol. 2006;24(18):2757–2764. doi:10.1200/JCO.2005.03.6053
38. Barcenas CH, Niu J, Zhang N, et al. Risk of hospitalization according to chemotherapy regimen in early-stage breast cancer. J Clin Oncol. 2014;32(19):2010–2017. doi:10.1200/JCO.2013.49.3676
39. Rosenstock AS, Lei X, Tripathy D, Hortobagyi GN, Giordano SH, Chavez-MacGregor M. Short-term mortality in older patients treated with adjuvant chemotherapy for early-stage breast cancer. Breast Cancer Res Treat. 2016;157(2):339–350. doi:10.1007/S10549-016-3815-Y
40. Muss HB, Polley MYC, Berry DA, et al. Randomized trial of standard adjuvant chemotherapy regimens versus capecitabine in older women with early breast cancer: 10-year update of the CALGB 49907 trial. J Clin Oncol. 2019;37(26):2338–2348. doi:10.1200/JCO.19.00647
41. Gralow JR, Barlow WE, Paterson AHG, et al. Phase III randomized trial of bisphosphonates as adjuvant therapy in breast cancer: S0307. J Natl Cancer Inst. 2020;112(7):698–707. doi:10.1093/JNCI/DJZ215
42. Perrone F, Nuzzo F, Di Rella F, et al. Weekly docetaxel versus CMF as adjuvant chemotherapy for older women with early breast cancer: final results of the randomized phase III ELDA trial. Ann Oncol. 2015;26(4):675–682. doi:10.1093/ANNONC/MDU564
43. Albain K, Anderson S, Arriagada R, et al. Comparisons between different polychemotherapy regimens for early breast cancer: meta-analyses of long-term outcome among 100,000 women in 123 randomised trials. Lancet. 2012;379(9814):432–444. doi:10.1016/S0140-6736(11)61625-5
44. Shulman LN, Berry DA, Cirrincione CT, et al. Comparison of doxorubicin and cyclophosphamide versus single-agent paclitaxel as adjuvant therapy for breast cancer in women with 0 to 3 positive axillary nodes: CALGB 40101 (Alliance). J Clin Oncol. 2014;32(22):2311–2317. doi:10.1200/JCO.2013.53.7142
45. Pinder MC, Duan Z, Goodwin JS, Hortobagyi GN, Giordano SH. Congestive heart failure in older women treated with adjuvant anthracycline chemotherapy for breast cancer. J Clin Oncol. 2007;25(25):3808–3815. doi:10.1200/JCO.2006.10.4976
46. Jones S, Holmes FA, O’Shaughnessy J, et al. Docetaxel with Cyclophosphamide is associated with an overall survival benefit compared with doxorubicin and Cyclophosphamide: 7-year follow-up of US oncology research trial 9735. J Clin Oncol. 2009;27(8):1177–1183. doi:10.1200/JCO.2008.18.4028
47. Blum JL, Flynn PJ, Yothers G, et al. Anthracyclines in Early Breast Cancer: the ABC Trials-USOR 06-090, NSABP B-46-I/USOR 07132, and NSABP B-49 (NRG Oncology). J Clin Oncol. 2017;35(23):2647–2655. doi:10.1200/JCO.2016.71.4147
48. Brouwers B, Hatse S, Dal Lago L, et al. The impact of adjuvant chemotherapy in older breast cancer patients on clinical and biological aging parameters. Oncotarget. 2016;7(21):29977. doi:10.18632/ONCOTARGET.8796
49. Brollo J, Curigliano G, Disalvatore D, et al. Adjuvant trastuzumab in elderly with HER-2 positive breast cancer: a systematic review of randomized controlled trials. Cancer Treat Rev. 2013;39(1):44–50. doi:10.1016/J.CTRV.2012.03.009
50. Sawaki M, Taira N, Uemura Y, et al. Randomized controlled trial of trastuzumab with or without chemotherapy for HER2-positive early breast cancer in older patients. J Clin Oncol. 2020;38(32):3743–3752. doi:10.1200/JCO.20.00184
51. Shenoy C, Klem I, Crowley AL, et al. Cardiovascular complications of breast cancer therapy in older adults. Oncologist. 2011;16(8):1138–1143. doi:10.1634/THEONCOLOGIST.2010-0348
52. Mackey JR, Martin M, Pienkowski T, et al. Adjuvant docetaxel, doxorubicin, and cyclophosphamide in node-positive breast cancer: 10-year follow-up of the Phase 3 randomised BCIRG 001 trial. Lancet Oncol. 2013;14(1):72–80. doi:10.1016/S1470-2045(12)70525-9
53. Tolaney SM, Barry WT, Dang CT, et al. Adjuvant paclitaxel and trastuzumab for node-negative, HER2-positive breast cancer. New Engl J Med. 2015;372(2):134–141. doi:10.1056/NEJMOA1406281
54. Jones SE, Collea R, Paul D, et al. Adjuvant docetaxel and cyclophosphamide plus trastuzumab in patients with HER2-amplified early stage breast cancer: a single-group, open-label, phase 2 study. Lancet Oncol. 2013;14(11):1121–1128. doi:10.1016/S1470-2045(13)70384-X
55. Vaz-Luis I, Keating NL, Lin NU, Lii H, Winer EP, Freedman RA. Duration and toxicity of adjuvant trastuzumab in older patients with early-stage breast cancer: a population-based study. J Clin Oncol. 2014;32(9):927–934. doi:10.1200/JCO.2013.51.1261
56. Chavez-MacGregor M, Zhang N, Buchholz TA, et al. Trastuzumab-related cardiotoxicity among older patients with breast cancer. J Clin Oncol. 2013;31(33):4222–4228. doi:10.1200/JCO.2013.48.7884
57. Chavez-MacGregor M, Niu J, Zhang N, et al. Cardiac monitoring during adjuvant trastuzumab-based chemotherapy among older patients with breast cancer. J Clin Oncol. 2015;33(19):2176–2183. doi:10.1200/JCO.2014.58.9465
58. von Minckwitz G, Procter M, de Azambuja E, et al. Adjuvant pertuzumab and trastuzumab in early HER2-positive breast cancer. New Engl J Med. 2017;377(2):122–131. doi:10.1056/NEJMOA1703643/SUPPL_FILE/NEJMOA1703643_DISCLOSURES.PDF
59. Chan A, Delaloge S, Holmes FA, et al. Neratinib after trastuzumab-based adjuvant therapy in patients with HER2-positive breast cancer (ExteNET): a multicentre, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2016;17(3):367–377. doi:10.1016/S1470-2045(15)00551-3
60. von Minckwitz G, Huang CS, Mano MS, et al. Trastuzumab emtansine for residual invasive HER2-positive breast cancer. New Engl J Med. 2019;380(7):617–628. doi:10.1056/NEJMOA1814017/SUPPL_FILE/NEJMOA1814017_DATA-SHARING.PDF
61. Stueber TN, Diessner J, Bartmann C, et al. Effect of adjuvant radiotherapy in elderly patients with breast cancer. PLoS One. 2020;15(5):e0229518. doi:10.1371/JOURNAL.PONE.0229518
62. Zureick AH, Grzywacz VP, Almahariq MF, et al. Dose to the left anterior descending artery correlates with cardiac events after irradiation for breast cancer. Int J Radiat Oncol Biol Phys. 2022;114(1):130–139. doi:10.1016/J.IJROBP.2022.04.019
63. Duma MN, Baumann R, Budach W, et al. Heart-sparing radiotherapy techniques in breast cancer patients: a recommendation of the breast cancer expert panel of the German society of radiation oncology (DEGRO). Strahlentherapie und Onkologie. 2019;195(10):861–871. doi:10.1007/S00066-019-01495-W
64. Offersen B, Alsner J, Nielsen HM, et al. Hypofractionated versus standard fractionated radiotherapy in patients with early breast cancer or ductal carcinoma in situ in a randomized Phase III Trial: the DBCG HYPO Trial. J Clin Oncol. 2020;38(31):3615–3636. doi:10.1200/JCO.20.01363
65. Whelan TJ, Pignol JP, Levine MN, et al. Long-term results of hypofractionated radiation therapy for breast cancer. N Engl J Med. 2010;362(6):513–520. doi:10.1056/NEJMOA0906260
66. Agrawal RK, Aird EGA, Barrett JM, et al. The UK Standardisation of Breast Radiotherapy (START) Trial B of radiotherapy hypofractionation for treatment of early breast cancer: a randomised trial. Lancet. 2008;371(9618):1098–1107. doi:10.1016/S0140-6736(08)60348-7
67. Murray Brunt A, Haviland JS, Wheatley DA, et al. Hypofractionated breast radiotherapy for 1 week versus 3 weeks (FAST-Forward): 5-year efficacy and late normal tissue effects results from a multicentre, non-inferiority, randomised, phase 3 trial. Lancet. 2020;395(10237):1613–1626. doi:10.1016/S0140-6736(20)30932-6
68. Coles CE, Griffin CL, Kirby AM, et al. Partial-breast radiotherapy after breast conservation surgery for patients with early breast cancer (UK IMPORT LOW trial): 5-year results from a multicentre, randomised, controlled, phase 3, non-inferiority trial. Lancet. 2017;390(10099):1048–1060. doi:10.1016/S0140-6736(17)31145-5/ATTACHMENT/77605C63-0D13-49A4-979C-B2C6CFF18200/MMC1.PDF
69. Whelan TJ, Julian JA, Berrang TS, et al. External beam accelerated partial breast irradiation versus whole breast irradiation after breast conserving surgery in women with ductal carcinoma in situ and node-negative breast cancer (RAPID): a randomised controlled trial. Lancet. 2019;394(10215):2165–2172. doi:10.1016/S0140-6736(19)32515-2
70. Meattini I, Marrazzo L, Saieva C, et al. Accelerated partial-breast irradiation compared with whole-breast irradiation for early breast cancer: long-term results of the randomized Phase III APBI-IMRT-Florence Trial. J Clin Oncol. 2020;38(35):4175–4183. doi:10.1200/JCO.20.00650
71. Sumodhee S, Levy J, Chamorey E, et al. Accelerated partial breast irradiation for elderly women with early breast cancer: a compromise between whole breast irradiation and omission of radiotherapy. Brachytherapy. 2017;16(5):929–934. doi:10.1016/J.BRACHY.2017.06.006
72. Darby S, McGale P, Correa C, et al. Effect of radiotherapy after breast-conserving surgery on 10-year recurrence and 15-year breast cancer death: meta-analysis of individual patient data for 10,801 women in 17 randomised trials. Lancet. 2011;378(9804):1707–1716. doi:10.1016/S0140-6736(11)61629-2
73. Matuschek C, Bölke E, Haussmann J, et al. The benefit of adjuvant radiotherapy after breast conserving surgery in older patients with low risk breast cancer- a meta-analysis of randomized trials. Radiat Oncol. 2017;12(1). doi:10.1186/S13014-017-0796-X
74. Hughes KS, Schnaper LA, Bellon JR, et al. Lumpectomy plus tamoxifen with or without irradiation in women age 70 years or older with early breast cancer: long-term follow-up of CALGB 9343. J Clin Oncol. 2013;31(19):2382–2387. doi:10.1200/JCO.2012.45.2615
75. Kunkler IH, Williams LJ, Jack WJL, Cameron DA, Dixon JM. Breast-conserving surgery with or without irradiation in women aged 65 years or older with early breast cancer (PRIME II): a randomised controlled trial. Lancet Oncol. 2015;16(3):266–273. doi:10.1016/S1470-2045(14)71221-5
76. Nikyar N, Tegnelius E, Valachis A. Adjuvant locoregional radiation therapy in breast cancer patients with pathologic complete response after neoadjuvant chemotherapy: a systematic review and meta-analysis. Clin Transl Radiat Oncol. 2022;33:45–52. doi:10.1016/J.CTRO.2021.12.010
77. Mandish SF, Gaskins JT, Yusuf MB, Amer YM, Eldredge-Hindy H. The effect of omission of adjuvant radiotherapy after neoadjuvant chemotherapy and breast conserving surgery with a pathologic complete response. Acta Oncol. 2020;59(10):1210–1217. doi:10.1080/0284186X.2020.1797161
78. Tramm T, Mohammed H, Myhre S, et al. Development and validation of a gene profile predicting benefit of postmastectomy radiotherapy in patients with high-risk breast cancer: a study of gene expression in the DBCG82bc cohort. Clin Cancer Res. 2014;20(20):5272–5280. doi:10.1158/1078-0432.CCR-14-0458
79. Speers C, Chang SL, Pesch A, et al. A signature that may be predictive of early versus late recurrence after radiation treatment for breast cancer that may inform the biology of early, aggressive recurrences. Int J Radiat Oncol Biol Phys. 2020;108(3):686–696. doi:10.1016/J.IJROBP.2020.05.015
80. Torres-Roca JF, Fulp WJ, Caudell JJ, et al. Integration of a radiosensitivity molecular signature into the assessment of local recurrence risk in breast cancer. Int J Radiat Oncol Biol Phys. 2015;93(3):631–638. doi:10.1016/J.IJROBP.2015.06.021
81. Eschrich SA, Fulp WJ, Pawitan Y, et al. Validation of a radiosensitivity molecular signature in breast cancer. Clin Cancer Res. 2012;18(18):5134–5143. doi:10.1158/1078-0432.CCR-12-0891
82. Ahmed KA, Liveringhouse CL, Mills MN, et al. Utilizing the genomically adjusted radiation dose (GARD) to personalize adjuvant radiotherapy in triple negative breast cancer management. EBioMedicine. 2019;47:163–169. doi:10.1016/J.EBIOM.2019.08.019
83. Rakovitch E, Nofech-Mozes S, Hanna W, et al. Multigene expression assay and benefit of radiotherapy after breast conservation in ductal carcinoma in situ. J Natl Cancer Inst. 2017;109:4. doi:10.1093/JNCI/DJW256
84. Bremer T, Whitworth PW, Patel R, et al. A biological signature for breast ductal carcinoma in situ to predict radiotherapy benefit and assess recurrence risk. Clin Cancer Res. 2018;24(23):5895–5901. doi:10.1158/1078-0432.CCR-18-0842
85. The IDEA Study (Individualized Decisions for Endocrine Therapy Alone) - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02400190.
86. A prospective cohort study evaluating risk of local recurrence following breast conserving surgery and endocrine therapy in low risk luminal a breast cancer - Full Text View - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT01791829.
87. The PRECISION Trial (Profiling Early Breast Cancer for Radiotherapy Omission): a Phase II study of breast-conserving surgery without adjuvant radiotherapy for favorable-risk breast cancer - Full Text View - ClinicalTrials.gov. Available from: https://www.clinicaltrials.gov/ct2/show/NCT02653755.
88. Murphy CT, Li T, Wang LS, et al. Comparison of adjuvant radiation therapy alone versus radiation therapy and endocrine therapy in elderly women with early-stage, hormone receptor-positive breast cancer treated with breast-conserving surgery. Clin Breast Cancer. 2015;15(5):381–389. doi:10.1016/J.CLBC.2015.02.005
89. Jeon YW, You SH, Lee JE, et al. Optimal treatment of breast cancer in women older than 75 years: a Korea Breast Cancer Registry analysis. Breast Cancer Res Treat. 2019;178(3):693. doi:10.1007/S10549-019-05426-2
90. Crystal JS, Rand J, Johnson J, et al. Adjuvant endocrine therapy is associated with improved overall survival in elderly hormone receptor-positive breast cancer patients. Breast Cancer Res Treat. 2020;184(1):63–74. doi:10.1007/S10549-020-05823-Y
91. Khan AJ, Parikh RR, Neboori HJ, Goyal S, Haffty BG, Moran MS. The relative benefits of tamoxifen in older women with T1 early-stage breast cancer treated with breast-conserving surgery and radiation therapy. Breast J. 2013;19(5):490–495. doi:10.1111/TBJ.12150
92. Meneveau MO, Keim-Malpass J, Camacho TF, Anderson RT, Showalter SL. Predicting adjuvant endocrine therapy initiation and adherence among older women with early-stage breast cancer. Breast Cancer Res Treat. 2020;184(3):805–816. doi:10.1007/S10549-020-05908-8
93. Eiermann W, Paepke S, Appfelstaedt J, et al. Preoperative treatment of postmenopausal breast cancer patients with letrozole: a randomized double-blind multicenter study. Ann Oncol. 2001;12(11):1527–1532. doi:10.1023/A:
94. Miller WR, Dixon JM, Cameron DA, Anderson TJ. Biological and clinical effects of aromatase inhibitors in neoadjuvant therapy. J Steroid Biochem Mol Biol. 2001;79(1–5):103–107. doi:10.1016/S0960-0760(01)00149-2
95. Exemestane as neoadjuvant hormonotherapy for locally advanced breast cancer: results of a phase II trial - PubMed. Available from: https://pubmed.ncbi.nlm.nih.gov/17695434/.
96. Madigan LI, Dinh P, Graham JD. Neoadjuvant endocrine therapy in locally advanced estrogen or progesterone receptor-positive breast cancer: determining the optimal endocrine agent and treatment duration in postmenopausal women-a literature review and proposed guidelines. Breast Cancer Res. 2020;22(1). doi:10.1186/S13058-020-01314-6
97. Barchiesi G, Mazzotta M, Krasniqi E, et al. Neoadjuvant endocrine therapy in breast cancer: current knowledge and future perspectives. Int J Mol Sci. 2020;21(10):3528. doi:10.3390/IJMS21103528
98. Kantor O, Pesce C, Liederbach E, Wang CH, Winchester DJ, Yao K. Surgery and hormone therapy trends in octogenarians with invasive breast cancer. Am J Surg. 2016;211(3):541–545. doi:10.1016/J.AMJSURG.2015.11.005
99. Hind D, Wyld L, Reed MW. Surgery, with or without tamoxifen, vs tamoxifen alone for older women with operable breast cancer: cochrane review. Br J Cancer. 2007;96(7):1025. doi:10.1038/SJ.BJC.6603600
100. Pepping RMC, Portielje JEA, van de Water W, de Glas NA. Primary endocrine therapy in older women with breast cancer. Curr Geriatr Rep. 2017;6(4):239–246. doi:10.1007/S13670-017-0223-Z
101. Johnston SJ, Cheung KL. The role of primary endocrine therapy in older women with operable breast cancer. Future Oncol. 2015;11(10):1555–1565. doi:10.2217/FON.15.13
102. Morgan JL, Collins K, Robinson TG, et al. Healthcare professionals’ preferences for surgery or primary endocrine therapy to treat older women with operable breast cancer. Eur J Surg Oncol. 2015;41(9):1234–1242. doi:10.1016/J.EJSO.2015.05.022
103. Cheung WY, Lai ECC, Ruan JY, Chang JT, Setoguchi S. Comparative adherence to oral hormonal agents in older women with breast cancer. Breast Cancer Res Treat. 2015;152(2):419–427. doi:10.1007/S10549-015-3455-7
104. Marinopoulos S, Dimitrakakis C, Kalampalikis A, Zagouri F, Andrikopoulou A, Rodolakis A. Adjuvant treatment of elderly breast cancer patients: offer the best chances of cure. Breast Care. 2022;17(1):71–80. doi:10.1159/000513708
105. Yuan C, Xie Z, Bian J, Huo J, Daily K. Outcomes of primary endocrine therapy in elderly women with stage I-III breast cancer: a SEER database analysis. Breast Cancer Res Treat. 2020;180(3):819–827. doi:10.1007/S10549-020-05591-9
106. Poorvu PD, Vaz-Luis I, Freedman RA, et al. Variation in guideline-concordant care for elderly patients with metastatic breast cancer in the United States. Breast Cancer Res Treat. 2018;168(3):727–737. doi:10.1007/S10549-018-4659-4
107. Aapro M, Monfardini S, Jirillo A, Basso U. Management of primary and advanced breast cancer in older unfit patients (medical treatment). Cancer Treat Rev. 2009;35(6):503–508. doi:10.1016/J.CTRV.2009.04.002
108. Carrick S, Parker S, Thornton CE, Ghersi D, Simes J, Wilcken N. Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev. 2009;2009(2). doi:10.1002/14651858.CD003372.PUB3
109. Bajetta E, Procopio G, Celio L, et al. Safety and efficacy of two different doses of capecitabine in the treatment of advanced breast cancer in older women. J Clin Oncol. 2005;23(10):2155–2161. doi:10.1200/JCO.2005.02.167
110. Vogel CL, O’Rourke M, Winer E, et al. Vinorelbine as first-line chemotherapy for advanced breast cancer in women 60 years of age or older. Ann Oncol. 1999;10(4):397–402. doi:10.1023/A:1008364222793
111. Barni S, Livraghi L, Gravina A, et al. Feasibility of Eribulin Mesylate in older patients with locally advanced or metastatic breast cancer: a post-hoc analysis of the ESEMPiO study. J Geriatr Oncol. 2019;10(6):990–993. doi:10.1016/J.JGO.2019.05.003
112. Beuselinck B, Wildiers H, Wynendaele W, Dirix L, Kains JP, Paridaens R. Weekly paclitaxel versus weekly docetaxel in elderly or frail patients with metastatic breast carcinoma: a randomized phase-II study of the Belgian Society of Medical Oncology. Crit Rev Oncol Hematol. 2010;75(1):70–77. doi:10.1016/J.CRITREVONC.2009.07.001
113. O’Brien MER, Wigler N, Inbar M, et al. Reduced cardiotoxicity and comparable efficacy in a phase III trial of pegylated liposomal doxorubicin HCl (CAELYX/Doxil) versus conventional doxorubicin for first-line treatment of metastatic breast cancer. Ann Oncol. 2004;15(3):440–449. doi:10.1093/ANNONC/MDH097
114. Biganzoli L, Coleman R, Minisini A, et al. A joined analysis of two European Organization for the Research and Treatment of Cancer (EORTC) studies to evaluate the role of pegylated liposomal doxorubicin (Caelyx) in the treatment of elderly patients with metastatic breast cancer. Crit Rev Oncol Hematol. 2007;61(1):84–89. doi:10.1016/J.CRITREVONC.2006.07.008
115. Coleman RE, Biganzoli L, Canney P, et al. A randomised phase II study of two different schedules of pegylated liposomal doxorubicin in metastatic breast cancer (EORTC-10993). Eur J Cancer. 2006;42(7):882–887. doi:10.1016/J.EJCA.2005.12.011
116. Kaufman PA, Brufsky AM, Mayer M, et al. Treatment patterns and clinical outcomes in elderly patients with HER2-positive metastatic breast cancer from the registHER observational study. Breast Cancer Res Treat. 2012;135(3):875. doi:10.1007/S10549-012-2209-Z
117. Wildiers H, Tryfonidis K, Dal Lago L, et al. Pertuzumab and trastuzumab with or without metronomic chemotherapy for older patients with HER2-positive metastatic breast cancer (EORTC 75111-10114): an open-label, randomised, phase 2 trial from the Elderly Task Force/Breast Cancer Group. Lancet Oncol. 2018;19(3):323–336. doi:10.1016/S1470-2045(18)30083-4
118. Freedman RA, Tolaney SM. Efficacy and safety in older patient subsets in studies of endocrine monotherapy versus combination therapy in patients with HR+/HER2- advanced breast cancer: a review. Breast Cancer Res Treat. 2018;167(3):607–614. doi:10.1007/S10549-017-4560-6
119. Howie LJ, Singh H, Bloomquist E, et al. Outcomes of older women with hormone receptor-positive, human epidermal growth factor receptor-negative metastatic breast cancer treated with a CDK4/6 inhibitor and an aromatase inhibitor: an FDA pooled analysis. J Clin Oncol. 2019;37(36):3475–3483. doi:10.1200/JCO.18.02217
120. Rugo HS, Turner NC, Finn RS, et al. Palbociclib plus endocrine therapy in older women with HR+/HER2- advanced breast cancer: a pooled analysis of randomised PALOMA clinical studies. Eur J Cancer. 2018;101:123–133. doi:10.1016/J.EJCA.2018.05.017
121. Cazzaniga M, Verusio C, Ciccarese M, et al. Everolimus (EVE) and exemestane (EXE) in patients with advanced breast cancer aged ≥ 65 years: new lessons for clinical practice from the EVA study. Oncotarget. 2018;9(61):31877. doi:10.18632/ONCOTARGET.25874
122. Pritchard KI, Burris HA, Ito Y, et al. Safety and efficacy of everolimus with exemestane vs. exemestane alone in elderly patients with HER2-negative, hormone receptor-positive breast cancer in BOLERO-2. Clin Breast Cancer. 2013;13(6):421–432.e8. doi:10.1016/J.CLBC.2013.08.011
123. Almodallal Y, Le-Rademacher JG, Cook KD, et al. Observations with alpelisib in older patients (≥ 65 year of age) with breast cancer in a non-clinical trial setting. Breast Cancer Res Treat. 2021;188(1):15–20. doi:10.1007/S10549-021-06277-6
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Updated Perspectives on the Diagnosis and Management of Onychomycosis
Falotico JM, Lipner SR
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1933-1957
Published Date: 15 September 2022
Breast Cancer Management in the Era of Covid-19; Key Issues, Contemporary Strategies, and Future Implications
Prodhan ASU, Islam DZ, Khandker SS, Jamiruddin MR, Abdullah A, Godman B, Opanga S, Kumar S, Sharma P, Adnan N, Pisana A, Haque M
Breast Cancer: Targets and Therapy 2023, 15:51-89
Published Date: 27 January 2023
Insight into Dysmenorrhea Research from 1992 to 2022: A Bibliometric Analysis
Dong Y, Li MJ, Hong YZ, Li WJ
Journal of Pain Research 2023, 16:3591-3611
Published Date: 27 October 2023
Regulating Lipid Metabolism in Gout: A New Perspective with Therapeutic Potential
Zhang X, Liu J
International Journal of General Medicine 2024, 17:5203-5217
Published Date: 12 November 2024
Mechanisms and Management of Albumin-Paclitaxel-Induced Peripheral Neuropathy in Breast Cancer
Xu X, Han Q, Qiu S, Gao S, Ren C, Li X
Breast Cancer: Targets and Therapy 2025, 17:693-709
Published Date: 13 August 2025