Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Biomarker-Defined Iron Deficiency in Heavy Smokers with and without COPD and/or Emphysema
Authors Hardang IM ![]() , Neumann K
, Neumann K ![]() , Gjønnes GT, Strand TE, Ashraf H, Einvik G
, Gjønnes GT, Strand TE, Ashraf H, Einvik G
Received 16 November 2025
Accepted for publication 29 January 2026
Published 1 April 2026 Volume 2026:21 573503
DOI https://doi.org/10.2147/COPD.S573503
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Ingrid Marie Hardang,1,2 Kirill Neumann,2,3 Geir Tormod Gjønnes,3 Trond-Eirik Strand,4,5 Haseem Ashraf,2,6 Gunnar Einvik2,3
1Department of Multidisciplinary Laboratory Medicine and Medical Biochemistry, Akershus University Hospital, Lørenskog, Norway; 2Institute of Clinical Medicine, University of Oslo, Lørenskog, Norway; 3Pulmonary Department, Akershus University Hospital, Lørenskog, Norway; 4Oslo University Hospital, Oslo, Norway; 5Department of Community Medicine, UiT The Arctic University of Norway, Tromsø, Norway; 6Department of Diagnostic Imaging, Akershus University Hospital, Lørenskog, Norway
Correspondence: Gunnar Einvik, Pulmonary Department, Akershus University Hospital, Lørenskog, Norway, Tel +47-41104542, Email [email protected]
Purpose: Assess whether iron deficiency prevalence in heavy smokers is higher in presence of COPD and/or emphysema, how the prevalence of iron deficiency is impacted by the biomarker used to define it, and examine the prevalence of anemia and polycythemia in heavy smokers with or without COPD.
Patients and Methods: A cross-sectional analysis was conducted on 1002 participants from the Norwegian Early Lung Cancer Screening study. All participants underwent chest CT scans, spirometry, and venous blood sampling to analyze iron-related parameters, C-reactive protein (CRP), and hemoglobin. Iron deficiency was defined using transferrin saturation (TSat) < 20%, ferritin < cutoff (CRP-dependent), or a combination of both.
Results: The prevalence of iron deficiency varied from 3% to 30%, being highest when defined by TSat < 20%, and was more prevalent in participants with COPD. Emphysema was not associated with iron deficiency. Decreasing hemoglobin, increasing soluble transferrin receptor (sTfR) and CRP were associated with TSat < 20%. COPD was not independently associated with iron deficiency. Increasing age and sTfR, along with female sex, were associated with ferritin < cutoff. Anemia was more common than polycythemia, with approximately one-third of anemia cases attributable to iron deficiency.
Conclusion: Iron deficiency was more prevalent in heavy smokers with COPD than in those without, but not in individuals with emphysema. TSat < 20% identified significantly more cases of iron deficiency than ferritin < cutoff. Eight percent of participants had anemia, while four percent had polycythemia, with neither condition related to COPD or emphysema.
Keywords: comorbidity, COPD, iron deficiency, smoking
Introduction
Tobacco smoke is the primary factor in developing both emphysema and chronic obstructive pulmonary disease (COPD). Emphysema is a histopathological disorder of alveolar destruction, whereas COPD is defined by physiological airflow limitation and associated symptoms. In practice and in this study, emphysema is most often detected by radiological imaging and can be present without a clinical diagnosis of COPD. 1 Lung damage in COPD may impact the physiological processes involved in iron metabolism via chronic inflammation and hypoxemia. Chronic inflammation can hinder iron absorption from the intestines and its release from storage,2 while hypoxemia stimulates erythropoiesis,3 leading to increased iron consumption. These processes are clinically relevant because iron deficiency and anemia can worsen functional capacity, dyspnea, and quality of life in individuals with COPD.
Although assessment of iron status is not currently included in the evaluation for treatable traits in COPD, studies report a higher prevalence of iron deficiency among individuals with COPD compared to healthy individuals.4,5 Before determining whether iron deficiency would be meaningful as a treatable trait in COPD, an extension of empirical data is needed to clarify the relationship between iron metabolism and COPD.
Most previous studies on this topic have focused on hospital cohorts with severe COPD; therefore, population-based or less selected cohorts are required. While various iron deficiency biomarkers exist, few studies systematically assess these biomarkers in COPD patients. Additionally, the influence of COPD phenotypes on the relationship between COPD and iron metabolism warrants further investigation. The predominant emphysema phenotype is characterized by alveolar destruction, resulting in hyperinflation and reduced gas diffusion, which subsequently leads to hypoxemia. However, we are not aware of research examining the relationship between emphysema and iron deficiency. Consequently, we hypothesize that emphysema may impact iron metabolism differently compared to individuals without emphysema.
A lung cancer screening program represents a relevant population for addressing these knowledge gaps by selecting individuals from the general population with high lifetime tobacco consumption. Accordingly, this study aimed to (1) compare three biomarkers of iron deficiency in individuals with and without COPD; (2) explore the associations between iron deficiency biomarkers and clinical phenotypes of COPD, such as emphysema and inflammation; and (3) delineate the proportion of individuals with either anemia or polycythemia.
Materials and Methods
The Norwegian Early Lung Cancer Screening study (TIDL) is a pilot program for lung cancer screening in Norway, conducted by Akershus University Hospital. In 2022, all approximately 125,000 residents of Akershus county aged 60–79 years were invited to complete a digital survey regarding smoking and other risk factors to estimate future lung cancer risk according to PLCOm2012.6 Among about 13,500 respondents, 2499 individuals with at least 35 pack-years of tobacco consumption or a six-year lung cancer risk of ≥2.6% were randomly assigned to participate in a low-dose computed tomography (LDCT) screening intervention (n=1250) or not (n=1249). The size of the LDCT group was determined by available funding. A total of 1007 participants (80%) in the intervention group completed an LDCT scan of the chest. Spirometry was offered as a voluntary examination on the same day as the LDCT, with 1003 accepting. Furthermore, all participants scheduled for the LDCT were also invited to provide venous blood samples for biobanking, with 1004 consenting. Consequently, a total of 1002 participants completed all examinations (Figure 1).
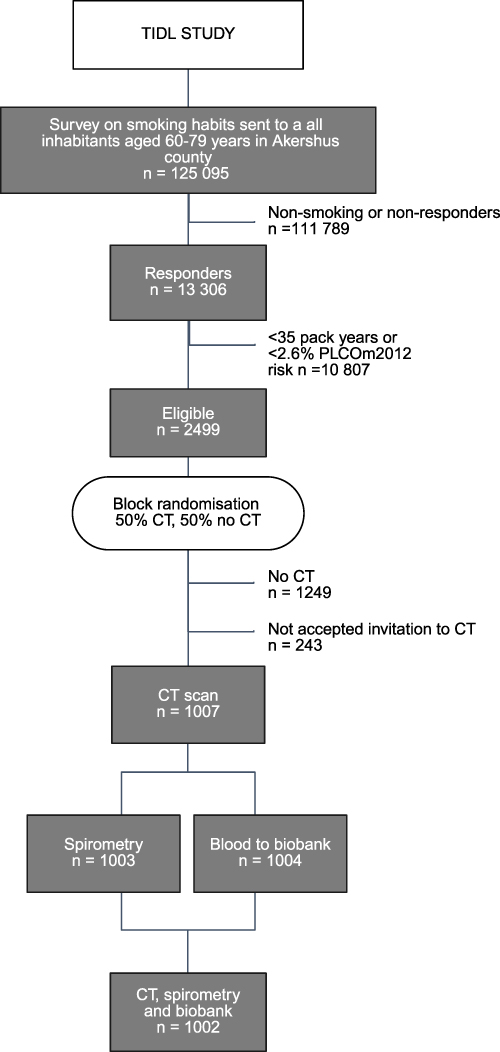 |
Figure 1 Flowchart of the participants. |
Both the lung cancer screening program and the associated biobank study received approval from the regional medical ethics committee (REK nos. 197434 and 401898) and the local data protection officer. All participants provided written informed consent prior to study commencement, and the study complied with the Declaration of Helsinki.
The severity of respiratory symptoms was assessed through interviews. Dyspnea was evaluated using the 5-point modified Medical Research Council (mMRC) scale.7 Chronic cough, defined as coughing daily for at least eight weeks per year, was recorded in the survey and responses were categorized as “yes” or “no”. Current and past tobacco consumption was documented in the survey, and current smoking status was also confirmed at the LDCT visit.
Spirometry was conducted according to the European Respiratory Society and American Thoracic Society guidelines and was performed regardless of the use of prescribed bronchodilators on the same day.8 Participants’ expected performance was determined using GLI-2012 reference values.9 In this study, a diagnosis of COPD was confirmed if the ratio of forced expiratory volume in one second (FEV1)/forced vital capacity (FVC) was below the lower limit of normal and accompanied by airway symptoms.
Venous blood samples were drawn and, if indicated, centrifuged within 90 minutes. The samples were aliquoted into cryotubes and frozen at –80°C within 120 minutes. Subsequent analyses were conducted in batches of several hundred samples. C-reactive protein (CRP), iron, transferrin, and soluble transferrin receptor (sTfR) were analyzed using the cobas pro c503, while ferritin was analyzed on the cobas pro e801. Hemoglobin was measured on the Sysmex XN-10 after a comparative study showed no significant differences in hemoglobin measurement between fresh and frozen-thawed samples (Supplemental Figure 1).
The LDCT was performed without venous contrast. An experienced radiologist (HA) assessed all CT scans for the degree of emphysema, categorizing the findings subjectively as none (score 0), mild (score 1), moderate (score 2), or severe (score 3). In some analyses, these categories were dichotomized, combining moderate and severe emphysema to indicate the presence of potentially clinically significant emphysema. Participants with tumors requiring immediate referral for clinical workup were classified as having lung cancer (n=12).
The three diagnostic criteria for iron deficiency utilized in this study were based on guidance from international experts,10 standard practices in research involving individuals with COPD,11 and conclusions drawn from two previous studies.12,13 The criteria included: transferrin saturation (TSat) <20%; ferritin < cutoff (100 µg/L in presence of inflammation, 30 µg/L in absence of inflammation); and a combination of these two criteria. Presence of inflammation was defined as CRP ≥5 mg/L.
Anemia was defined according to WHO criteria as hemoglobin levels <12 g/dL for women and <13 g/dL for men. Polycythemia was defined as hemoglobin levels above the reference range: >15.3 g/dL for women and >17.0 g/dL for men.
The data are presented as means with standard deviations (SD) for variables with symmetrical distributions, and as medians with the 25th and 75th percentiles for skewed variables. Continuous parameters were compared between groups using the t-test for symmetrically distributed data and the Mann–Whitney U-test for non-symmetrical data. For dichotomized variables, we applied the chi-squared test and Fisher’s exact test. Cuzick’s extension of the Wilcoxon rank-sum test, a non-parametric method for trend analysis, was used to compare dyspnea and emphysema scores between groups. Prevalence of iron deficiency across different biomarker definitions was compared conducted using McNemar’s test. Odds ratios (OR) for various iron deficiency criteria were estimated through bivariate and multivariable logistic regression analyses.
To explore the association between clinical or biochemical aspects of COPD and iron deficiency biomarkers, we considered the following covariates: age, sex, COPD diagnosis, emphysema presence, current smoking status, hemoglobin, sTfR, CRP, BMI (body mass index (kg/m2)), and estimated glomerular filtration rate (eGFR). Covariates with a bivariate p-value <0.05 were included in the multivariable analysis, and no multicollinearity was detected among them. Given the established association between inflammation and iron biomarkers, we predefined interaction terms for CRP×COPD and CRP×emphysema in multivariable analyses.
All p-values are two-sided, with a p-value <0.05 considered statistically significant. Missing data are indicated by footnotes in the tables. Data analysis was performed using Stata version 18.0.
Results
Table 1 presents the characteristics of the study population, categorized by presence or absence of COPD. Approximately 23% of the total population had COPD based on the current definition. While age, sex, and pack-years were similar across groups, the COPD group exhibited lower BMI and FEV1 as a percentage of predicted, higher mMRC scores, and a greater prevalence of cough and current smoking compared to the non-COPD group. The degree of emphysema was significantly greater (p<0.001) in participants with COPD (mean score 1.40) than in those without (mean score 0.67). Nevertheless, 98 (12.7%) of non-COPD participants had moderate or severe emphysema. Detected lung cancer cases, hemoglobin levels, and kidney function were similar across both groups.
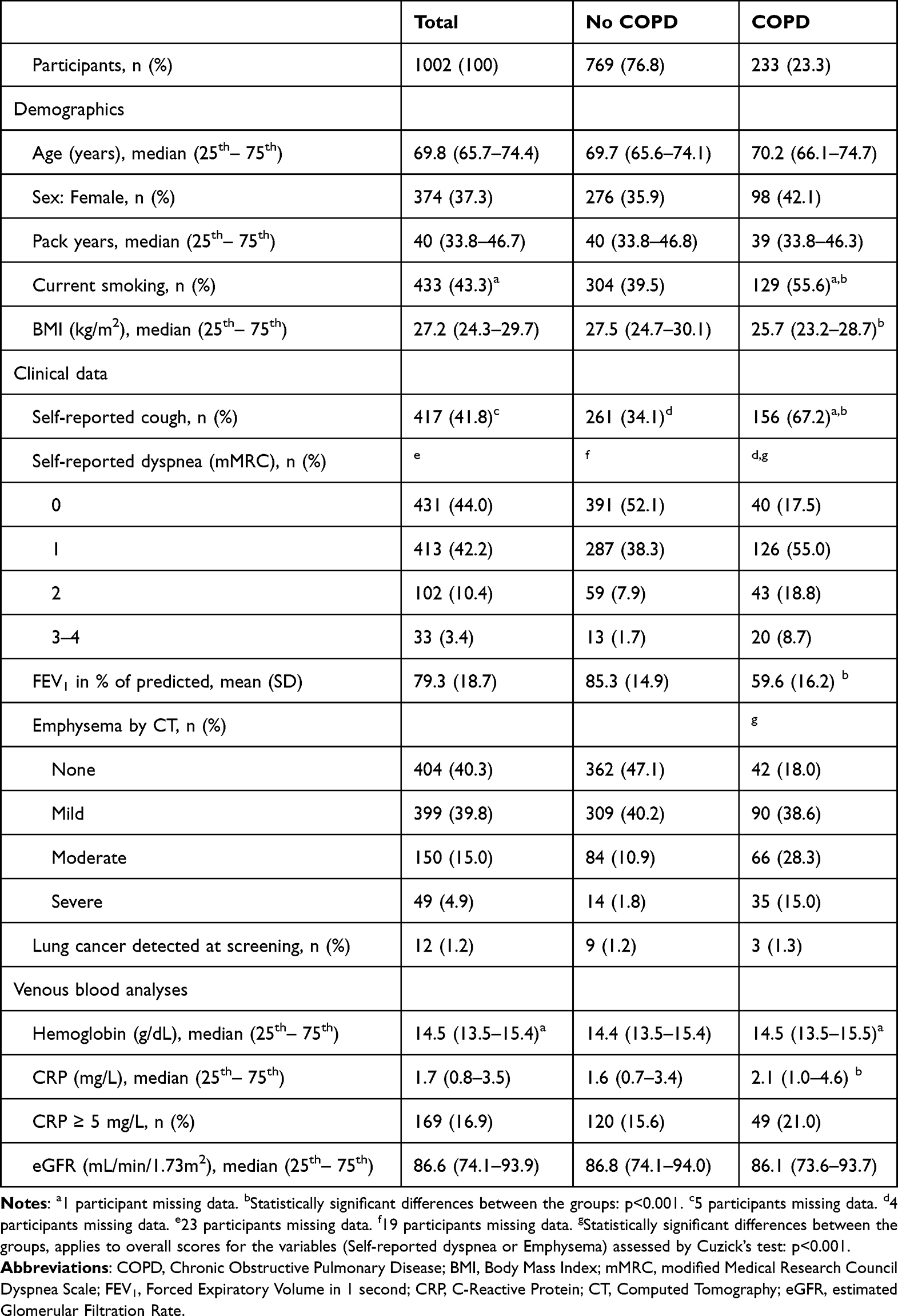 |
Table 1 Descriptive Demographic, Clinical and Laboratory Data for the Total Group and According to Presence of COPD |
Table 2 presents iron-related parameters stratified by the presence or absence of COPD or emphysema (moderate or severe). We observed a significantly higher proportion of participants with COPD meeting the TSat <20% criterion compared to those without COPD. In both groups, fewer participants met the ferritin < cutoff criterion. Combining the ferritin < cutoff and TSat <20% criteria resulted in a further decrease in the prevalence of iron deficiency, with no significant difference between the COPD and non-COPD groups. In similar analyses comparing participants with and without emphysema, no differences in iron deficiency prevalence were found between the groups. Overall iron deficiency prevalence was significantly higher when defined by TSat <20% compared to ferritin < cutoff (p<0.0001). The odds of being classified as iron deficient were nearly five times higher with the TSat <20% definition (OR=4.91, 95% CI: 3.38–7.33).
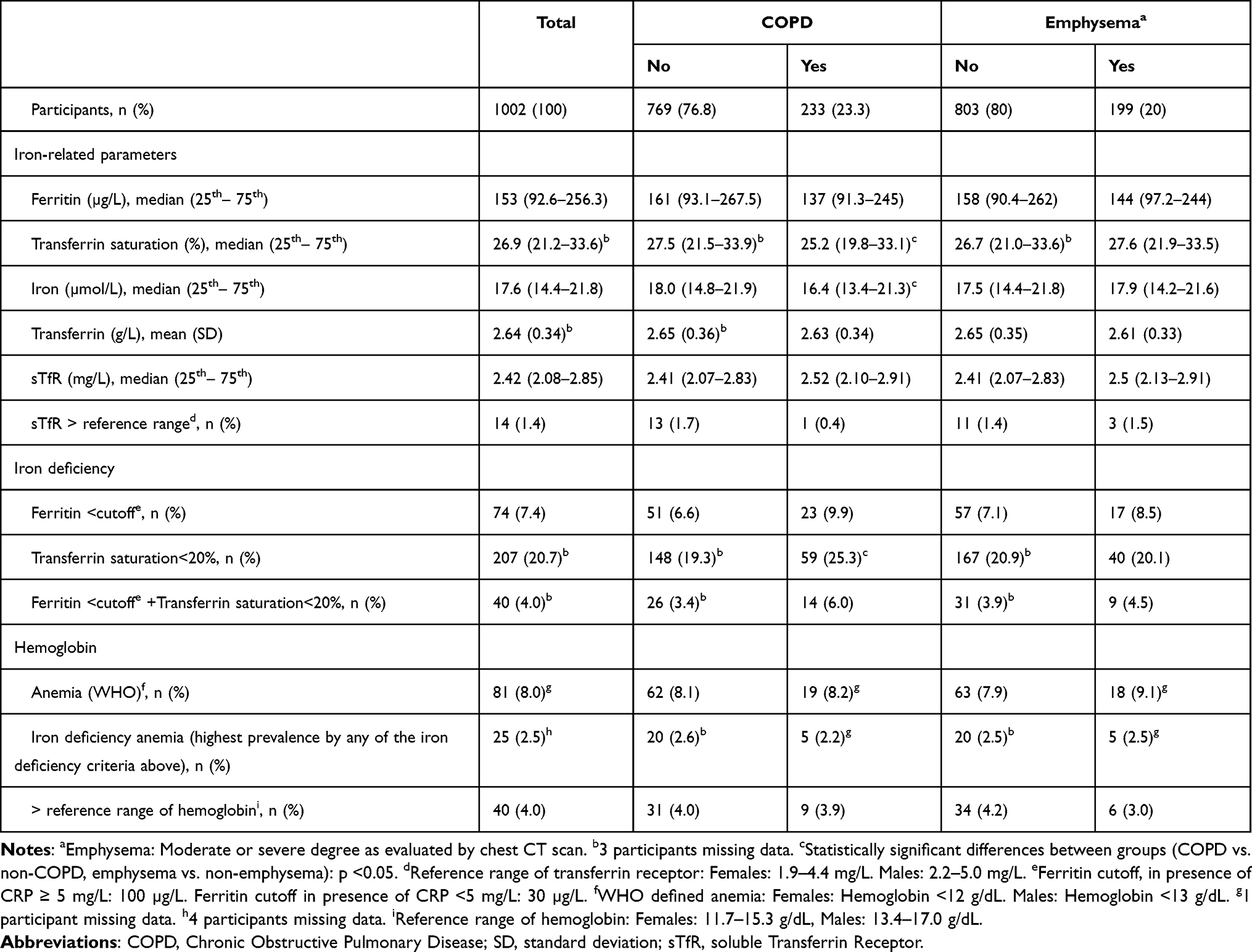 |
Table 2 Iron-Related Biomarkers and Iron Deficiency for the Total Population and Grouped According to COPD or Emphysema |
Participants were further categorized into four distinct groups: neither COPD nor emphysema (n=671, 67%); emphysema without COPD (n=98, 10%); COPD without emphysema (n=132, 13%); and COPD with emphysema (n=101, 10%). Figure 2 illustrates the prevalence of iron deficiency across these groups. Notably, the COPD without emphysema group exhibited the highest prevalence of iron deficiency based on the TSat <20% criterion, which was significantly greater than that in the group with neither COPD nor emphysema. No other statistically significant differences in biomarker-defined iron deficiency were observed between the groups.
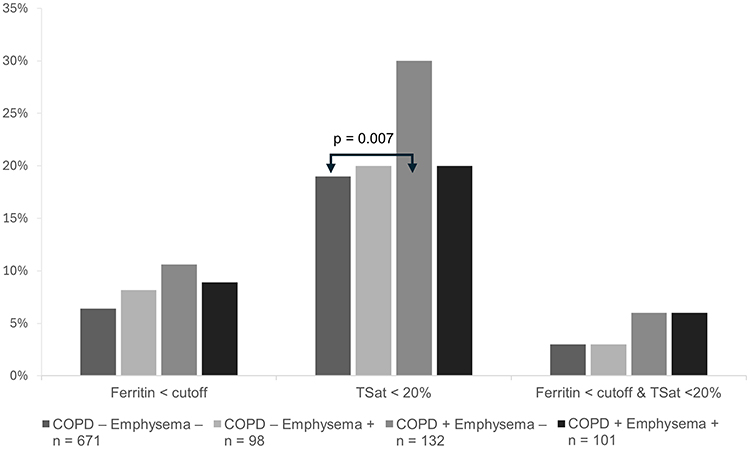 |
Figure 2 Bar chart illustrating the proportion with iron deficiency according to the different iron deficiency criteria in four different groups of participants, with or without COPD and/or with or without emphysema. Abbreviations: COPD, Chronic obstructive pulmonary disease; TSat, Transferrin Saturation. |
The overlap between the iron deficiency biomarkers ferritin < cutoff and TSat <20% was partial in both COPD and non-COPD participants (Supplemental Table 1). Among the 40 participants identified as having iron deficiency according to the combined criterion, this group represented 54% of those with ferritin < cutoff and 19% of those with TSat <20%.
The odds ratios from three separate bivariate and multivariable logistic regression models of iron deficiency criteria and relevant covariates are presented in Table 3. Adding the interaction terms CRP×COPD or CRP×emphysema did not improve model prediction as determined by the Akaike Information Criterion or the Bayesian Information Criterion, and these terms were not retained. In multivariable analyses, increasing age and sTfR, and female sex were significantly associated with ferritin < cutoff. For the outcome of TSat <20%, decreasing hemoglobin and increasing sTfR and CRP were significantly associated, while COPD was no longer significantly associated with it. Finally, for the combined criterion of ferritin < cutoff and TSat <20%, significantly associated covariates included increasing age and sTfR, and decreasing hemoglobin.
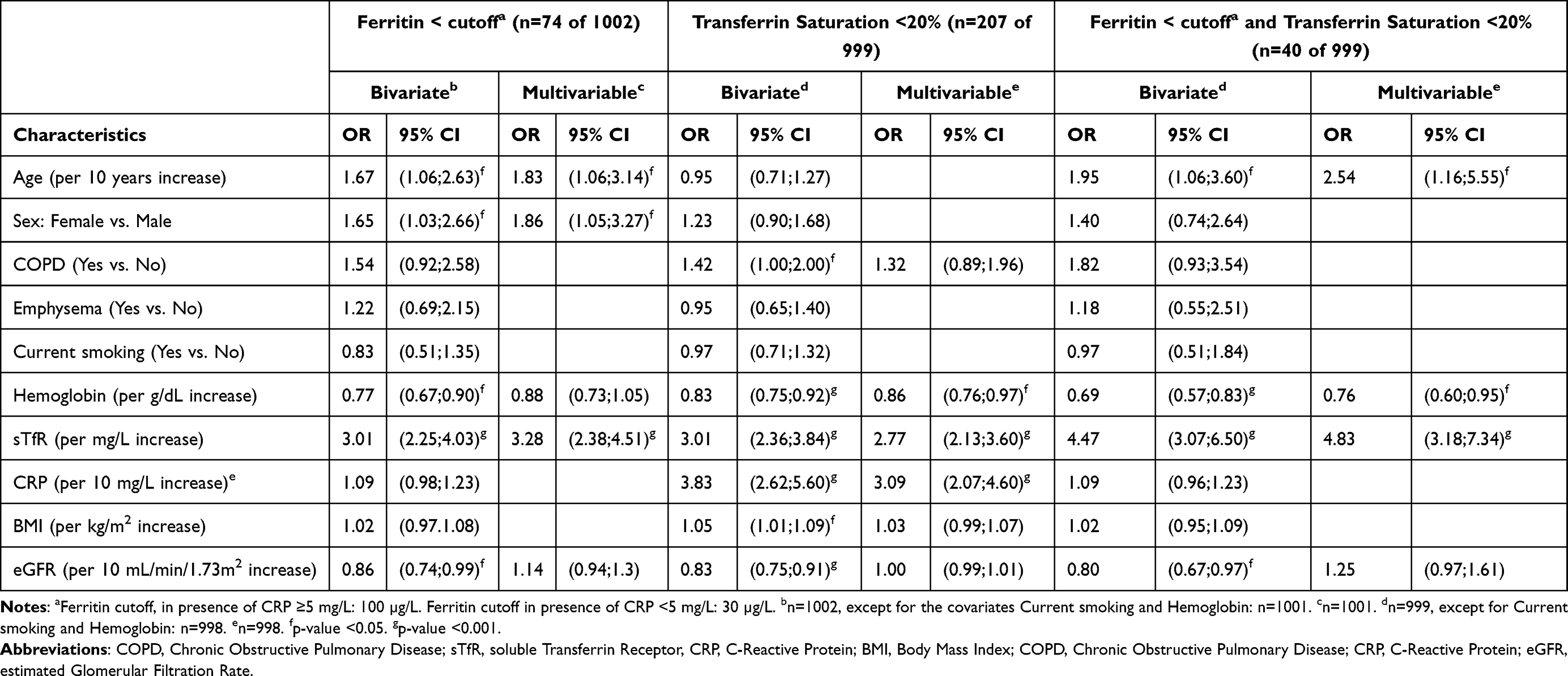 |
Table 3 Odds Ratios (OR) with Corresponding 95% Confidence Intervals (CI) for Three Diagnostic Criteria of Iron Deficiency, by Relevant Covariates Using Bivariate and Multivariable Logistic Regression. The Interaction Terms CRP × COPD and CRP × Emphysema Did Not Improve the Models and Were Thus Omitted. |
Anemia was identified in 8% of non-COPD participants (both with and without emphysema), 7% of COPD participants without emphysema, and 10% of COPD participants with emphysema (Supplemental Table 2). There were no statistically significant differences in anemia prevalence between these groups. One-third of all cases could be attributed to iron deficiency, with TSat <20% being the most frequently met criterion among these participants. Polycythemia was infrequently observed, occurring in 2–5% of participants across the groups, with the highest prevalence in the COPD group without emphysema; however, no statistically significant difference was observed between groups (Supplemental Table 2).
Discussion
The most significant findings are that iron deficiency, as indicated by TSat <20%, but not ferritin < cutoff, was more prevalent among lung cancer screening participants with COPD compared to non-COPD participants, while emphysema per se was not associated with biomarkers of iron deficiency.
First, the results of this study partially support previous research that points towards an association between COPD and increased prevalence of iron deficiency.4,11 Our data extend previous empirical evidence by assessing a large group of individuals from the general population with a history of heavy smoking. Furthermore, by including heavy smokers without COPD as a control group, we demonstrate that tobacco consumption alone is less likely to account for this association.
Our study suggests that one in four individuals with COPD and a heavy smoking history may have iron deficiency, highlighting the relevance of this issue for further investigation both in hospital settings and by family practitioners. Other comorbidities in COPD, such as cardiovascular disease, chronic kidney disease, and psychiatric conditions—which reportedly have similar prevalence rates to iron deficiency in this study—have received more attention to aid in identifying treatable traits that can improve patient outcomes.
A novel aspect of this study was including three different iron deficiency biomarkers and comparison of their prevalence. Across all three biomarkers, we found a higher absolute prevalence of iron deficiency in the COPD group compared to the non-COPD group. TSat <20% identified significantly more individuals as iron deficient than ferritin < cutoff. The overlap between TSat <20% and ferritin < cutoff, represented by the combined criterion, was limited. Research conducted on heart failure patients showed that combining TSat <20% and ferritin <128 µg/L best identified those with bone marrow-verified iron deficiency.13 Whether this also applies to COPD patients remains unclear.
Our population allowed us to investigate the association between iron deficiency biomarkers and COPD phenotypes, with emphysema being a novel approach. Aside from a minority of persons with genetic susceptibilities, emphysema arises from long-term exposure to tobacco smoke or related toxic agents. The permanently damaged alveolar architecture contributes to obstructive exhalation and reduced gas diffusion, leading to hyperinflated lungs with lower alveolar oxygen levels and, subsequently, hypoxemia, which stimulates increased erythropoiesis and consumes iron. We hypothesized that emphysema would be associated with iron deficiency; however, we found no evidence to support this hypothesis in our study. Additionally, we observed no increase in hemoglobin levels in the presence of emphysema compared to its absence. However, we cannot rule out that an association between emphysema and iron deficiency may exist in patients with more advanced pulmonary disease and pronounced hypoxemia.
Among other clinical and biochemical factors related to COPD phenotypes that we assessed, we report that increasing age was associated with iron deficiency defined as ferritin < cutoff or in combination with TSat <20%, which aligns with some findings but contradicts others.14,15 Female sex was associated with ferritin < cutoff, consistent with the latter study’s findings.15 As expected, lower hemoglobin and higher sTfR, both of which reflect processes involving iron supply, were linked to two or all three iron deficiency biomarkers.
sTfR has proven useful in distinguishing between anemia of iron deficiency and anemia of chronic inflammation.16 Although we found sTfR to be strongly associated with all three iron deficiency biomarkers, only 14 participants (1.4%) had an sTfR level above the reference range, and approximately 50% of them were anemic. Furthermore, all had TSat <20% and most had ferritin < cutoff. Previous research has shown that sTfR may not detect iron deficiency unless it has progressed significantly.17
Inflammation significantly impacts iron-related parameters as it leads to a decrease in plasma iron levels,18 resulting in lower TSat. Although no single test fully captures systemic inflammation, elevated CRP is commonly used as an indicator of its presence. In our multivariable analyses, increasing levels of CRP were associated with TSat <20%. As COPD is often characterized by chronic inflammation, the absence of a significant association between COPD and iron deficiency (TSat <20%) in multivariable analyses—compared to its presence in bivariate analyses—may be attributed to the inclusion of CRP in the model. The introduction of CRP likely accounted for some of the variance in iron status that might otherwise be attributed to COPD alone. While a formal interaction between CRP and COPD was not detected, it remains plausible that inflammation could modify the relationship between COPD and TSat <20%.
Inflammation also complicates the interpretation of ferritin levels. While plasma ferritin accurately reflects iron storage in absence of inflammation,19 ferritin levels increase during inflammation regardless of iron status.20 This is why a higher ferritin cutoff, commonly set at 100 µg/L, is used in inflammatory conditions. However, this cutoff may not be appropriate for individuals with low-grade inflammatory conditions.
The third aim of this study was to assess deviations in hemoglobin levels within the study population. We found no association between the prevalence of anemia or polycythemia and COPD or emphysema. Approximately one-third of the anemia cases were attributable to iron deficiency, defined as TSat <20%. A previous US population-based study found a similar prevalence of anemia among individuals aged 65 to 74 years, with one-third related to a nutrient deficiency.21 We do not have sufficient data to evaluate the causes of the remaining two-thirds of anemia cases.
The main strength and clinical relevance of this study lie in its analysis of associations between iron deficiency biomarkers, COPD, emphysema, and inflammation in a large cohort. It highlights the challenges clinicians face in diagnosing iron deficiency in COPD patients, where inflammatory processes may elevate ferritin levels and reduce TSat regardless of iron storage. Additionally, the correlation among iron deficiency biomarkers is limited. Even if the true prevalence of iron deficiency is estimated at 10% to 20%, it remains a clinically significant concern for COPD patients.
The study has several limitations. The cross-sectional nature of the data allows only for exploratory discussions of associations. We are uncertain about the status of non-responders in both the survey and the randomized study, which limits the generalizability of our findings to individuals from the general population willing to participate in screening programs. However, this is unlikely to have significantly affected the main results, as iron deficiency is not expected to bias participation rates. Additionally, blood samples were frozen prior to analysis, preventing assessments of reticulocyte hemoglobin and eosinophil count, which could have offered further insights. Bone marrow analysis for iron assessment could enhance our understanding of the relationship between iron status and deficiency biomarkers; however, the invasiveness of this procedure makes it difficult to obtain a sufficient sample size. Only ever-smokers were included in our cohort; therefore, the results may not be generalizable to individuals with COPD and/or emphysema due to non-smoking causes. Alternative investigations could include examining the impact of iron deficiency on functional outcomes, such as the relationship between exercise capacity and specific iron deficiency biomarkers, providing insights into the relevance of these biomarkers for this patient population.
Conclusion
In a large sample of individuals aged 60–79 years with a history of heavy smoking attending lung cancer screening, the prevalence of iron deficiency was significantly higher in COPD participants compared to those without. However, when accounting for radiological emphysema status, the significant difference remained only in participants without emphysema; emphysema did not contribute to iron deficiency in this study. Furthermore, TSat < 20% identified more individuals with iron deficiency than ferritin < cutoff. Anemia was present in 8% of the study population, with iron deficiency accounting for approximately one-third of these cases.
Abbreviations
COPD, Chronic obstructive pulmonary disease; CRP, C-Reactive Protein; TSat, Transferrin Saturation; sTfR, soluble Transferrin Receptor; TIDL, The Norwegian Early Lung Cancer Screening study; LDCT, Low-dose Computed Tomography; mMRC, modified Medical Research Council; FEV1, Forced Expiratory Volume in one second; FVC, Forced vital capacity; SD, standard deviation; BMI, Body Mass Index (kg/m2); eGFR, estimated glomerular filtration rate.
Acknowledgments
The main TIDL study was funded by The Norwegian Cancer Society (Kreftforeningen), while spirometry and biochemical analyses were funded by Akershus University Hospital. Morten K. Moe created Supplemental Figure 1. The AI-based tool GPT UiO 4o-mini, provided by the University of Oslo, has been used for language refinement.
Disclosure
The authors declare no conflicts of interest related to this work. Kirill Neumann has received fees from GSK and AstraZeneca for lecturing, from MSD for lecturing and serving on an advisory board, and from Janssen for serving on an advisory board. Gunnar Einvik has received honorarias for serving advisory boards for Sanofi and AstraZeneca. Prof. Dr. Haseem Ashraf reports grants from the Norwegian Cancer Society, during the conduct of the study.
References
1. Global Initiative for Chronic Obstructive Lung Disease. 2025-Report-v1.0-15Nov2024. Available from: https://goldcopd.org/2025-gold-report/.
2. Kemna E, Pickkers P, Nemeth E, van der Hoeven H, Swinkels D. Time-course analysis of hepcidin, serum iron, and plasma cytokine levels in humans injected with LPS. Blood. 2005;106(5):1864–11. doi:10.1182/blood-2005-03-1159
3. Semenza GL, Wang GL. A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Mol Cell Biol. 1992;12(12):5447–5454. doi:10.1128/mcb.12.12.5447-5454.1992
4. Nickol AH, Frise MC, Cheng HY, et al. A cross-sectional study of the prevalence and associations of iron deficiency in a cohort of patients with chronic obstructive pulmonary disease. BMJ Open. 2015;5(7):e007911. doi:10.1136/bmjopen-2015-007911
5. Hardang I, Søyseth V, Kononova N, Hagve T, Einvik C. COPD: iron deficiency and clinical characteristics in patients with and without chronic respiratory failure. Chronic Obstr Pulm Dis. 2024;2.
6. Tammemägi MC, Katki HA, Hocking WG, et al. Selection criteria for lung-cancer screening. N Engl J Med. 2013;368(8):728–736. doi:10.1056/NEJMoa1211776
7. Mahler DA. mMRC (Modified Medical Research Council) Dyspnea Scale. Available from: https://www.mdcalc.com/calc/4006/mmrc-modified-medical-research-council-dyspnea-scale#creator-insights.
8. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. An official American thoracic society and European respiratory society technical statement. Am J Respir Crit Care Med. 2019;200(8):e70–e88. doi:10.1164/rccm.201908-1590ST
9. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3–95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
10. Cappellini MD, Comin-Colet J, de Francisco A, et al. Iron deficiency across chronic inflammatory conditions: international expert opinion on definition, diagnosis, and management. Am J Hematol. 2017;92(10):1068–1078. doi:10.1002/ajh.24820
11. Robalo Nunes A, Tata M. The impact of anaemia and iron deficiency in chronic obstructive pulmonary disease: a clinical overview. Rev Port Pneumol. 2017;23(3):146–155. doi:10.1016/j.rppnen.2016.12.005
12. Grote Beverborg N, Klip IT, Meijers WC, et al. Definition of iron deficiency based on the gold standard of bone marrow iron staining in heart failure patients. Circ Heart Fail. 2018;11(2):e004519. doi:10.1161/CIRCHEARTFAILURE.117.004519
13. Grote Beverborg N, van der Wal HH, Klip IT, et al. Differences in clinical profile and outcomes of low iron storage vs defective iron utilization in patients with heart failure: results from the DEFINE-HF and BIOSTAT-CHF studies. JAMA Cardiol. 2019;4(7):696–701. doi:10.1001/jamacardio.2019.1739
14. Zacharski LR, Chow B, Shamayeva G, Lavori P. Effect of an interaction between age and ferritin level on clinical outcomes in Peripheral Arterial Disease (PAD). Blood. 2010;116(21):4302. doi:10.1182/blood.V116.21.4302.4302
15. Loría A, Hershko C, Konijn AM. Serum ferritin in an elderly population. J Gerontol. 1979;34(4):521–524. doi:10.1093/geronj/34.4.521
16. Punnonen K, Irjala K, Rajamäki A. Serum transferrin receptor and its ratio to serum ferritin in the diagnosis of iron deficiency. Blood. 1997;89(3):1052–1057. doi:10.1182/blood.V89.3.1052
17. Cook J, Skikne B, Baynes R. Serum transferrin receptor. Annu Rev Med. 1993;44(1):63–74. doi:10.1146/annurev.me.44.020193.000431
18. Nemeth E, Rivera S, Gabayan V, et al. IL-6 mediates hypoferremia of inflammation by inducing the synthesis of the iron regulatory hormone hepcidin. J Clin Invest. 2004;113(9):1271–1276. doi:10.1172/JCI200420945
19. Addison G, Beamish M, Hales C, Hodgkins M, Jacobs A, Llewellin P. An immunoradiometric assay for ferritin in the serum of normal subjects and patients with iron deficiency and iron overload. J Clin Pathol. 1972;25(4):326–329. doi:10.1136/jcp.25.4.326
20. Cook J, Finch C, Smith N. Evaluation of the iron status of a population. Blood. 1976;48(3):449–455. doi:10.1182/blood.V48.3.449.449
21. Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood. 2004;104(8):2263–2268. doi:10.1182/blood-2004-05-1812
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies
Byanova KL, Abelman R, North CM, Christenson SA, Huang L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2795-2817
Published Date: 29 November 2023
Characteristics of Current Smokers versus Former Smokers with COPD and Their Associations with Smoking Cessation Within 4.5 Years: Results from COSYCONET
Alter P, Stoleriu C, Kahnert K, Henke MO, Bals R, Trudzinski FC, Watz H, Speicher T, Söhler S, Welte T, Rabe KF, Wouters EFM, Vogelmeier CF, Jörres RA
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2911-2923
Published Date: 6 December 2023
The Effects of Smoking and Airway Restriction on Subclinical Atherosclerosis
Yeşildağ M, Keskin Z, Yavşan DM, Bekci TT, Osmanoglu UO
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1217-1226
Published Date: 24 April 2025
Level of Awareness About Chronic Obstructive Pulmonary Disease Among Active Smokers
Al-Otaibi HM, Homoud MM, Alqarni MM, Alsobhi GJ, Al-Otaibi GZ, Alnahdi NA
International Journal of Chronic Obstructive Pulmonary Disease 2026, 21:580239
Published Date: 29 March 2026