")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Authors Chan HS , Ko FWS, Chan JWM , Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
Received 29 November 2022
Accepted for publication 15 March 2023
Published 6 April 2023 Volume 2023:18 Pages 507—519
DOI https://doi.org/10.2147/COPD.S394698
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Hok Sum Chan,1 Fanny Wai San Ko,2 Johnny Wai Man Chan,3 Kah Lin Choo,4 Loletta Kit Ying So,5 David Chi Leung Lam,6 Kit Man Sin,7 Wei Yin Wong,8 Yuk Lun Cheng,1 Maureen Mo Lin Wong9
1Department of Medicine, Alice Ho Miu Ling Nethersole Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 2Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 3Department of Medicine, Queen Elizabeth Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 4Department of Medicine, North District Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 5Department of Medicine, Pamela Youde Nethersole Eastern Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 6Department of Medicine, Queen Mary Hospital, University of Hong Kong, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 7Department of Medicine and Geriatrics, Tuen Mun Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 8Department of Medicine, Haven of Hope Hospital, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China; 9Department of Medicine and Geriatrics, Caritas Medical Centre, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China
Correspondence: Hok Sum Chan, Department of Medicine, 6/F, Block J, Alice Ho Miu Ling Nethersole Hospital, 11 Chuen On Road, Tai Po, NT, Hong Kong Special Administrative Region (HKSAR), People’s Republic of China, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a common cause for hospital admission. This study aims to review the hospital burden of COPD in Hong Kong (HK) and the trend from year 2006 to 2014.
Methods: A multi-center, retrospective study of the characteristics of COPD patients discharged from the public hospitals of HK from year 2006 to 2014. Anonymized data retrieval and analysis were performed. The demographic data of the subjects, use of health-care resources, ventilatory support, medications used and mortality of the subjects were analyzed.
Results: Total patient headcount (HC) and admission number reduced from 10,425 and 23,362 in year 2006 to 9613 and 19,771, respectively, in 2014. There was a progressive reduction of female COPD HC from 2193 (21%) in year 2006 to 1517 (16%) in 2014. The utilization of non-invasive ventilation (NIV) increased rapidly and peaked in 2010 (29%) and decreased thereafter. There was a rapid increase in the prescription of long-acting bronchodilators (from 15% to 64%). COPD and pneumonia were the top causes of death, but death due to pneumonia was rapidly increasing while death due to COPD was progressively decreasing over the period.
Conclusion: COPD HC and admission number (particularly in female patients) decreased progressively from year 2006 to 2014. There was also a decreasing trend of severity of disease as reflected by lower NIV use (after year 2010) and lower mortality rate due to COPD. Reduced smoking prevalence and tuberculosis (TB) notification rate in the community in the past might have reduced the incidence and severity of COPD and the hospital burden of disease. We observed an increasing trend of mortality due to pneumonia in COPD patients. Appropriate and timely vaccination programs are recommended for COPD patients as in the general elderly population.
Keywords: hospital burden, mortality, smoking, old tuberculosis, pneumonia
Introduction
Chronic obstructive pulmonary disease (COPD) is a common disease that imposes a high burden on health-care resources worldwide.1 The first large-scale study of the burden of COPD in Hong Kong (HK) was carried out in 2005.2 The crude mortality rate of COPD was 29.1/100,000, while the crude hospitalization rate was 193/100,000 in 2005. COPD ranked the second (after respiratory infections) as a respiratory cause for hospitalization (14.6%) and inpatient bed-days (20.5%). However, details of health-care utilization by COPD patients were not revealed in this earlier study in HK.2
About 90% of the hospital service in HK is provided by the Hospital Authority (HA). Besides admission and discharge data, essential clinical information (including primary and secondary diagnoses, procedure coding and medications) in HA were computerized and recorded in the clinical management system (CMS). Anonymized patient data could be retrieved and analyzed using the HA Clinical Data Analysis and Reporting System (CDARS) software program.3–5 Previous published data of 14 public hospitals in HK showed that it is possible to review the health-care utilization of an anonymized COPD patient cohort (N = 9776) in year 2012 using CDARS.3 The present study aimed to assess the trend of hospital burden of COPD from 2006 to 2014 – including the demographic data, use of health-care resources, mortality and survival. HK has a population of over 7 million and the present study included the medical departments of all acute public hospitals (N = 15) and chest hospitals (N = 4) in HK. We believed that the information from this study would be useful for the planning of health-care resources.
Methods
Study Design and Patient Recruitment
This was a multi-centered retrospective study of COPD patients discharged from the medical departments of all acute regional hospitals (N = 15) and all chest hospitals (N = 4) of the HA in HK, during the period from 1st January 2006 to 31st December 2014. A list of the participating hospitals is shown in Appendix. Anonymized data retrieval was performed with the HA CDARS.3–5 All patients with the principal diagnosis of “chronic bronchitis” (ICD-9 codes 491, 491.2, 491.21), “emphysema” (ICD-9 codes 492, 492.8) and “COPD” (ICD-9 code 496) on discharge in year 2006 to 2014 were included. These ICD codes were grouped under a “COPD Clinical Data Framework (CDF)” in the CMS to facilitate data retrieval. For patients with spirometry data available, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria of post bronchodilator forced expiratory volume in 1 second / forced vital capacity ratio (FEV1/FVC) <70% was used for the diagnosis of COPD.1 The inclusion criteria were: (1) COPD CDF (ICD-9 codes described earlier) as the principal diagnosis on discharge; (2) over 40 years of age and (3) discharged from the medical departments of the respective hospitals. The exclusion criteria were: (1) 40 years of age or less and (2) patients discharged from specialties other than Medicine.
Group data for each year included: (1) number of individual patient [headcount (HC)] with principal discharge diagnosis of COPD; (2) demographic data (gender and age); (3) total number of hospital admissions (with COPD as principal diagnosis); (4) length of hospital stay (LOS); (4) number of attendance at Accident & Emergency Department (A&E) and number of Specialist Out-Patient Department (SOPD) visits; (5) treatment modalities including NIV (ICD code 93.9) and invasive mechanical ventilation (IMV) (ICD code 96.70, 96.71, 96.72); (6) comorbidity of “old tuberculosis (TB)” was identified for subjects with secondary diagnosis of “late effect of respiratory TB (ICD code 137.0)” in the index COPD admissions or in previous admissions related or unrelated to COPD; (7) prescription of one or more long acting bronchodilators [long acting beta-agonists (LABA) and/or long-acting anti-muscarinic agent (LAMA)]; (8) prescription of inhaled corticosteroid (ICS); (9) mortality of the recruited patients in the same and subsequent years; (10) the cause of death was retrieved from the death registry and the principal diagnosis for the episode of hospital discharge which ended up in death.
Data Administration and Research Ethics Approval
The present research project was endorsed by the Central Committee of COPD [CC(COPD)] of the HA Head Office (HAHO). The hospitals in HK under the HA were distributed in 7 clusters as listed in Appendix.
Cluster representatives in CC(COPD) were invited as co-investigators of the present research project. As there is no central ethics committee of HAHO, research ethics approval was sought from the research ethics committee of all the hospital clusters. The cluster representatives were responsible for the submission of research ethics application for their respective cluster. A full list of the cluster representatives in CC(COPD) and the full names of the respective research ethics committees are listed in Appendix 2. As this was a retrospective study and the dataset retrieved by the HA computer system (CDARS) was anonymized with no personal information, patient informed consent was not required. The present research project was approved by the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (the leading research Ethics Committee of the New Territories East Cluster) and the research ethics committees of all the other participating clusters. The cluster representatives, besides being co-investigators in this research project, were also the data controller of their respective cluster, and co-authors of the present manuscript.
Definition
The subjects with admission for COPD in 2006 were defined as the 2006 cohort. The subjects with the 1st admission for COPD in 2007 but no admission in 2006 were defined as the 2007 cohort, and so on. The 2014 cohort had no previous hospital admissions in 2006 to 2013.
Statistics
The CDARS provided simple statistical analysis with means and standard deviations (SD) of the whole group and subgroups defined by different parameters. Additional statistical evaluations, for example, comparisons between subgroups, were performed using the SPSS version 22 software package (IBM Corporation, Armonk, NY, USA). Data were expressed as mean ± SD. Comparisons between various groups and between time frames were made by one-way analysis of variance and the Tukey post hoc tests. To test for any trend across time frames, the chi-squared tests for linear trend were used for categorical data (please refer to Tables and Figures for details). A p-value of less than 0.05 was considered statistically significant.
Results
HC with COPD as Principal Discharge Diagnosis
From year 2006 to 2014, the number of HC of COPD peaked in the year 2007 with 11,046 HC admitted in that year (Table 1, Supplementary Table 1). Thereafter, the HC of COPD showed a slow reduction to below 11,000/year. In 2013 and 2014, the number of HC further dropped to below 10,000/year. There was a trend of reduction in HC for both male and female patients (Table 2), but the reduction was more marked for female patients. The number of female HC reduced from 2193 (21%) in 2006 to 1517 (15.8%) in 2014 (Table 2). There was a smaller reduction in the HC for male patients over the years (8232 in 2006 to 8096 in 2014) and consequently the percentage of male HC increased from 79.0% in 2006 to 84.2% in 2014 (p < 0.0001) (Table 1 and Table 2).
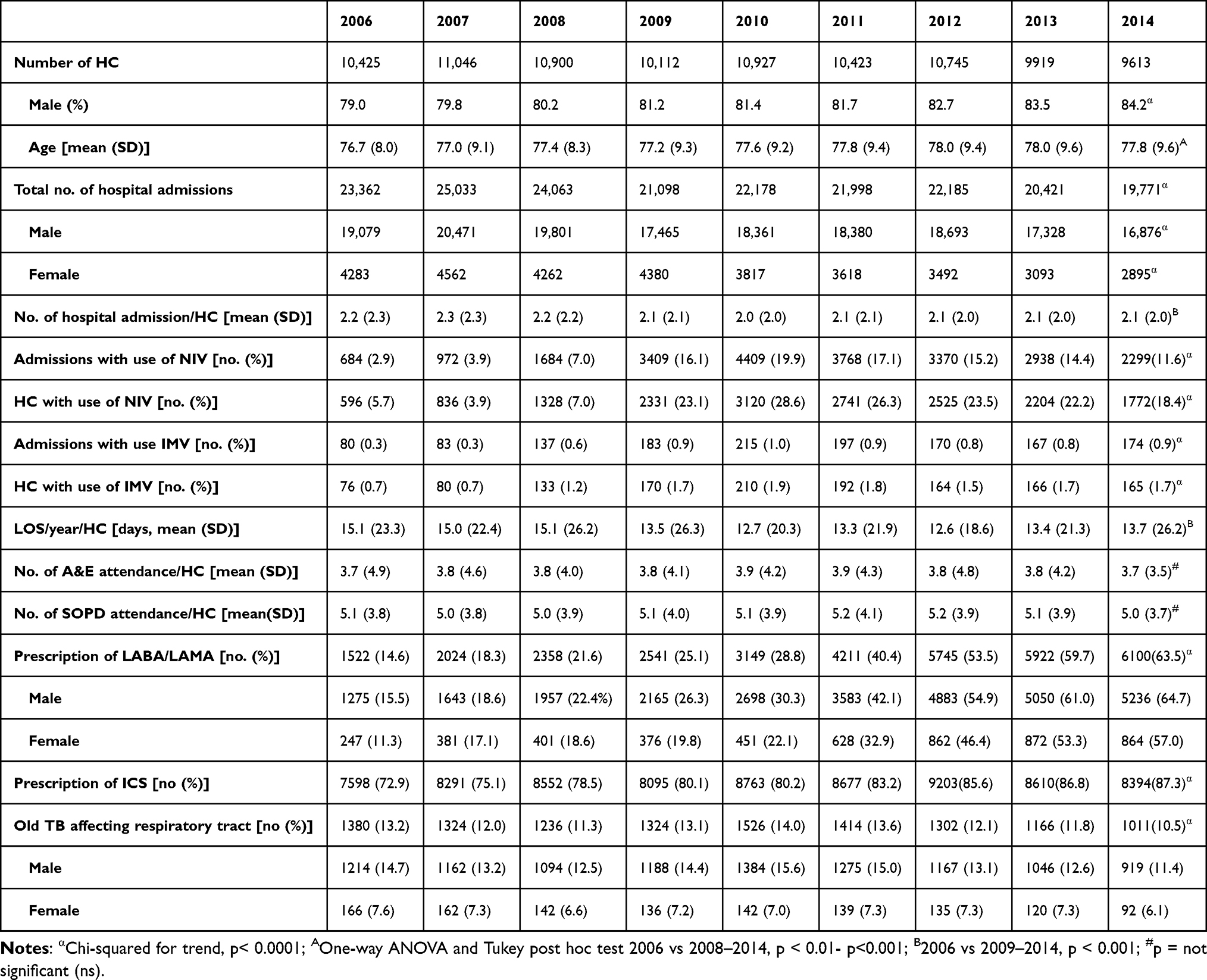 |
Table 1 Trend of Demographic Data and Use of Healthcare Resources by COPD Patients from 2006 to 2014 |
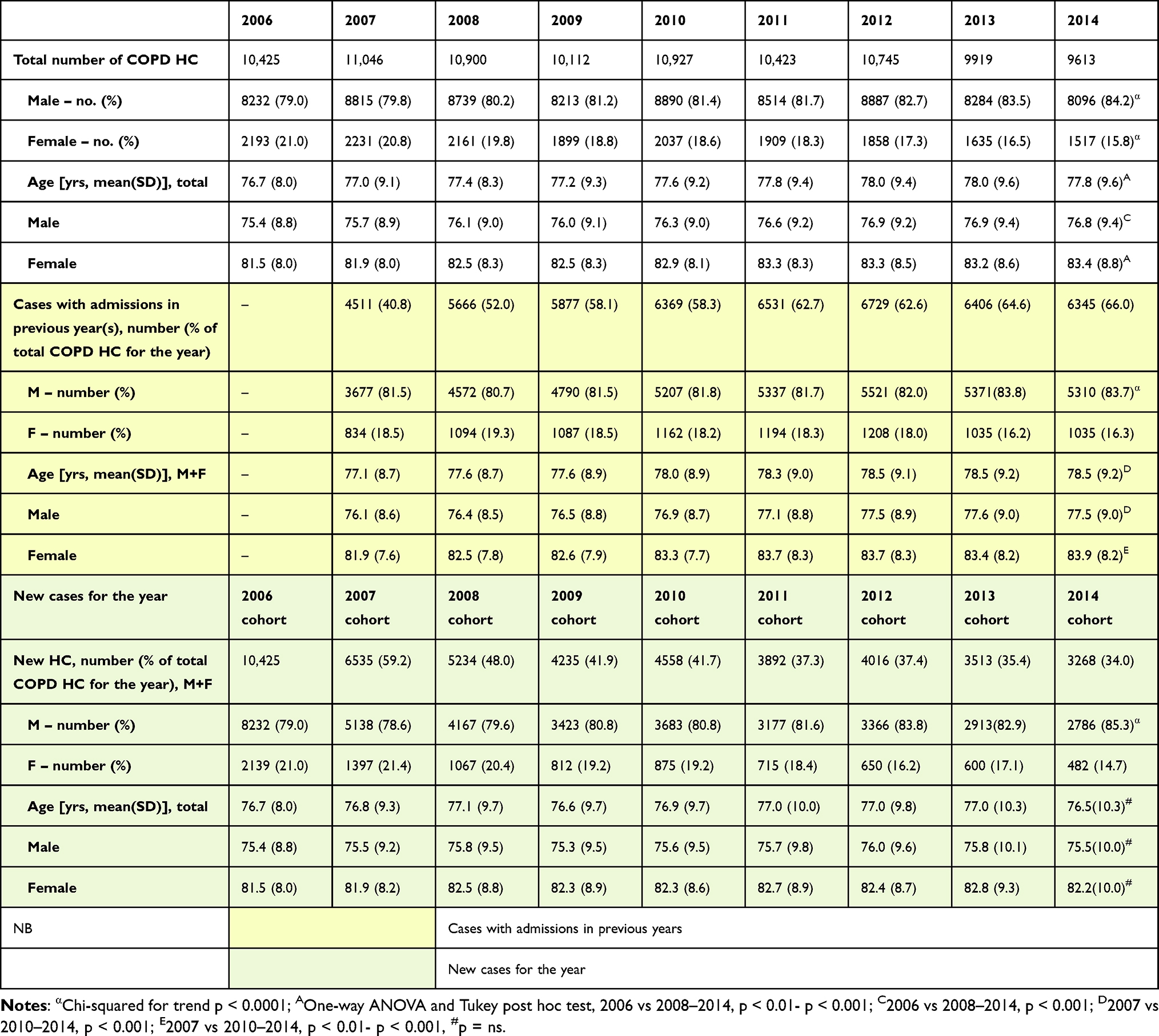 |
Table 2 Trend of Age and Sex Distribution of the New COPD Patients in Each Year Compared with the Whole COPD Population with Hospital Admissions from 2006 to 2014 |
Use of Healthcare Resources
The yearly number of COPD admissions peaked in year 2007 with 25,033 admissions in that year (Table 1). Thereafter, the yearly COPD admissions gradually reduced. In 2014, the number of admissions dropped to below 20,000. The number of hospital admission/HC/year showed a small but statistically significant reduction from 2.2 (2.3) [mean (SD)] in year 2006 to 2.1 (2.0) in 2014 (p < 0.001) (Table 1, Supplementary Table 2). The hospital length of stay (LOS)/HC/year was reduced from 15.1 (23.3) days in year 2006 to 13.7 (26.2) days in 2014 (p < 0.001) (Table 1, Supplementary Table 3).
The utilization of NIV was low in year 2006 (2.9% of admission, 5.7% of HC), but it reached a peak in 2010 with 19.9% of admission, 28.6% of HC, being given NIV (p < 0.0001) (Table 1). The utilization of IMV was low throughout the period, but it also showed a peak in year 2010 with 1% of admission and 1.9% of HC being given IMV. The percentage of admissions and HC requiring NIV and IMV gradually dropped after the peak in 2010. In 2014, the percentage of admissions requiring NIV and IMV dropped to 11.6% and 0.9%, respectively (p < 0.0001).
The number of AED attendance was stable at around 3.7 to 3.9 episodes/HC/year. The number of SOPD attendance was also stable at around 5.0–5.2 episodes/HC/year. There was no significant trend in the number of A&E or SOPD attendance/HC/year over the years from 2006 to 2014 (Table 1, Supplementary Tables 4 and 5).
The prescription of one or more long-acting bronchodilators (LABA and/or LAMA) increased rapidly from 15% in 2006 to 64% in 2014 (p < 0.0001) (Table 1). The prescription of ICS was common and there was a gradual increase over the years from 72.9% in year 2006 to 87.3% in 2014 (p < 0.0001).
Old TB and the Use of NIV
Old TB is a common comorbidity of patients with COPD in HK, with over 10% of the patients having old TB from year 2006 to 2014 (p < 0.0001) (Table 1). The number and proportion of patients with old TB as a comorbidity showed a peak in 2010 with 14.0% of HC having old TB as a comorbidity, but the number and percentage declined from 2011 onwards. In 2016, only 10.5% of COPD HC had old TB as a comorbidity (p < 0.0001).
Subgroup analysis of patients with COPD and history of old TB (Table 3) showed that this group of patients was at risk of requiring NIV treatment during acute COPD exacerbations. The application of NIV peaked in year 2010 with 3120 (28.6%) of HC requiring NIV. Subgroup analysis showed that in year 2010, 20.5% of the COPD HC requiring NIV had history of old TB, and 41.9% of HC with COPD and history of old TB required the use of NIV in that year. Thereafter, both the use of NIV and history of old TB declined. In year 2014, 18.4% of COPD HC (with and without TB) and 25.5% of HC with COPD and old TB required NIV, respectively (p < 0.0001).
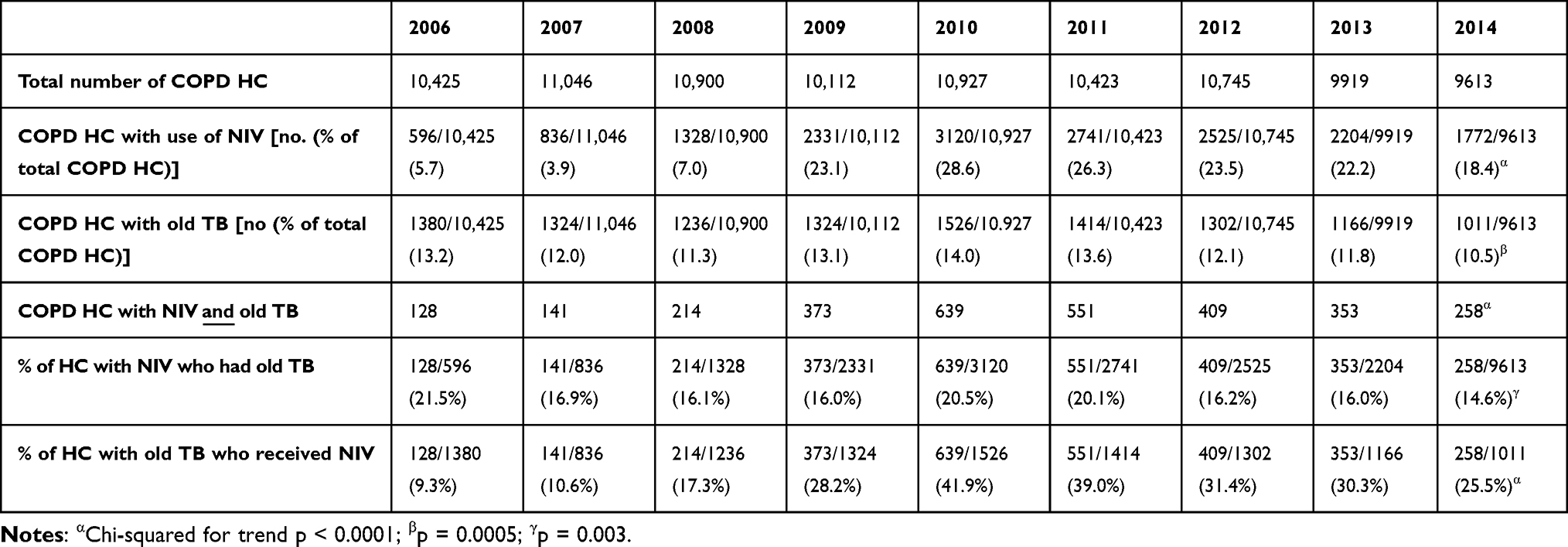 |
Table 3 Subgroup Analysis of Patients with COPD and Old TB and Requirement of NIV |
Effect of Demographic Factors on COPD Admissions
The age of the COPD HC showed a small (but statistically significant) increasing trend for all patients, male (M) and female (F) from year 2006 to 2014. The mean age was (all: 76.7, M: 75.4, F: 81.5 years of age) in 2006 vs 2014 (all: 77.8, M: 76.8, F: 83.4 years of age) (p < 0.001) (Table 2, Supplementary Tables 6–8).
The COPD HC with the first admission or repeated admissions in each year from 2007 to 2014 were analyzed (Table 2). The HC with the first admission in 2007 (defined as 2007 cohort) and the subsequent years (2008 to 2014 cohorts) showed a trend of reducing numbers over the years. A total of 6535 HC were admitted in year 2007 (2007 cohort, 59.2% of total COPD HC), having no admission in year 2006. In year 2014, 3268 HC (2014 cohort, 34.0% of total HC) had their first admission in 2014 with no previous admissions from year 2006–2013. The falling trend of new cases requiring hospital admission was seen for both males and females, but more marked for females. As a result, the percentage of male HC who were new admissions increased from 78.6% in year 2007 to 85.3% in 2014 (p < 0.0001) (Table 2).
On the other hand, the number of patients with admissions in previous years (ie, repeated admissions) increased from 4511 (40.8% of total HC) in 2007 to 6345 (66.0% of total HC) in 2014. This trend of repeated admissions in subsequent years was particularly seen in male patients with HC that slowly increased from 3677 (81.5%) in year 2007 to a peak of 5521 (82.0%) in 2012 and remained high at over 5300 per year (84%) in 2013 and 2014 (p < 0.0001) (Table 2). The HC of female patients with repeated admissions showed no significant fluctuations, but because of the increasing number of male HC with repeated admissions, the proportion of female HC with repeated admissions reduced from 18.5% in year 2007 to 16.3% in 2014 (Table 2).
The age of patients with repeated admissions showed a small but a significant increasing trend for all, male and female HC (mean age of all: 77.1, M: 76.1, F: 81.9 years of age) in year 2007 to 2014 (all: 78.5, M: 77.5, F: 83.9 years of age) (p < 0.01- p < 0.001) (Table 2, Supplementary Tables 9–11). There was no significant trend in the age of the patients with the first admission in the years from 2007 (mean age of all: 76.8, M: 75.5, F: 81.9 years of age) to 2014 (mean age of all: 76.5, M: 75.5, F: 82.2 years of age) (Table 2, Supplementary Table 12).
The trends of hospital admissions originating from different cohorts are shown graphically in Figure 1. Despite the falling number of new cases of COPD requiring hospital admissions, the total number of COPD HC with hospital admission in each year was largely maintained by the repeated admissions of COPD HC who survived over the years.
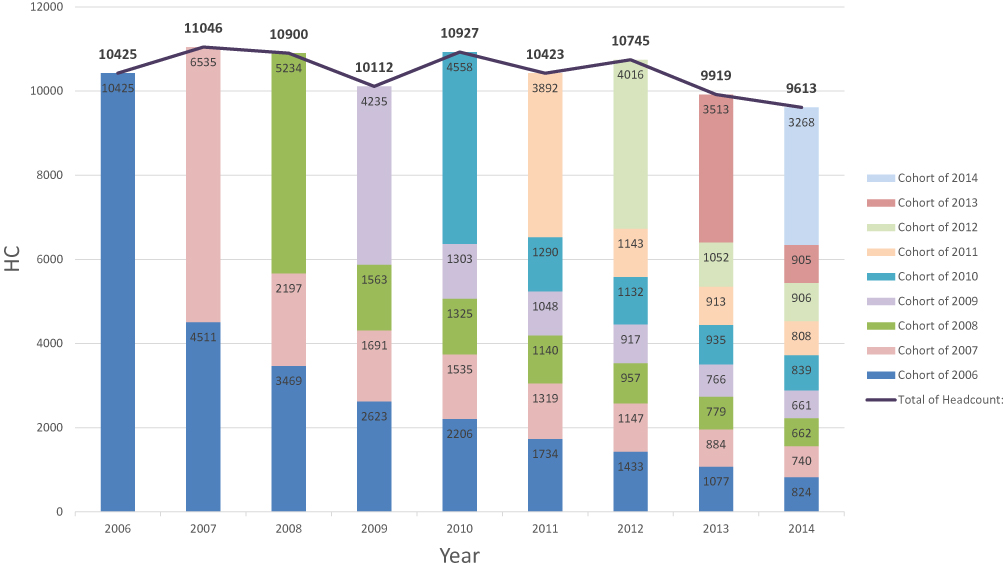 |
Figure 1 Trend of COPD admission HC in each year and the year that they were first admitted to HA hospital (year of cohort). |
In summary, the new cases of COPD requiring hospital admission in each year was falling in number from year 2006 to 2014, and the age of the new COPD HC in each year was similar. On the other hand, the patients with repeated admissions were increasing in age over the years, compatible with their continued survival throughout the study period from year 2006 to 2014.
First Year Mortality and Cause of Death
The first year total mortality rate was around 17–18% with no significant variation over the years (Table 4). However, the mean age of death showed a gradual increase from year 2006 (all 79.6, M 78.2, F 84.3 years of age) to year 2014 (all 81.3, M 80.3, F 86.3 years of age) (Table 4, Supplementary Tables 13–15).
 |
Table 4 Trend of Mortality, Sex and Age at Death and the Top 10 Causes of Death from 2006 to 2014 |
Over 60% of the deaths were due to COPD or pneumonia over the period from year 2006 to 2014 (Table 4). However, there were significant reductions in the total number and proportion of deaths due to COPD from 800 (43.1%) in year 2006 to 418 (25.9%) in 2014 (p < 0.0001). Deaths due to pneumonia increased from 387 (20.8%) in 2006 to 681 (42.2%) in 2014 (p < 0.0001). The other less common causes of death were lung cancer, malignancies other than lung, ischemic heart disease, heart failure, respiratory failure, etc. The proportion of deaths who were male increased from 76% in year 2006 to 84% in 2014 (p < 0.0001) (Table 4), corresponding with the percentage increase in male COPD HC in the same period (Table 1).
Subgroup analysis of the death cases due to COPD and pneumonia (Table 5) showed that male patients accounted for over 70% of the deaths due to COPD (p = 0.004) or pneumonia (p < 0.0001). The age of the patients who died from pneumonia (both male and female) were about 2 years older than patients who died from COPD over the whole study period. Age at death of the patients who died of COPD showed no significant change over the years (Table 5, Supplementary Table 16). On the other hand, a trend of increasing age at death was seen for patients who died of pneumonia, but only statistically significant in male patients (Table 5, Supplementary Tables 17 and 18).
 |
Table 5 Subgroup Analysis of Death Cases Due to COPD and Pneumonia |
Cumulative Survival of COPD HC Originating from Different Cohorts
The cumulative survival of the COPD HC as at 31 Dec of each year was calculated by subtracting the number of fatal cases in each year from the original cohort as shown in Figure 2. Combining the HC originating from other years, the cumulative survival of the COPD patients ever admitted to HA hospitals after year 2006 was gradually accumulating in the community, up to and seemed to plateau off at 19,060 as on 31 Dec 2014. These patients might or might not be admitted to hospital after their first admission, but they were still surviving in the community according to the death registry.
 |
Figure 2 Cumulative survival of COPD patients originating from cohorts of different years. |
Discussion
COPD is the 4th leading cause of death in the world in 1990,6 but it became the 3rd leading cause of death worldwide in 2019.7 However, earlier report from HK showed a progressive decline in mortality and hospitalization rate due to COPD between 1997 and 2005.2 Cigarette is the major cause of COPD in HK like most western populations. It was postulated that the general trend of reduction in mortality and hospitalization rates of COPD in HK from year 1997–2005 reflected the decline in the prevalence of smoking locally since 1980.8 We have extended the study to look for the hospital burden of COPD in HK, the trend from year 2006 to 2014, and to study the COPD cohorts in each year in greater detail.
The important observations of COPD patients discharged from public hospitals in HK from year 2006 to 2014 were:
- The number of COPD admissions peaked in year 2007 with 25,033 discharges, but gradually declined to 19,771 in 2014.
- Progressive decline of COPD HC requiring hospital admissions, particularly females, so that the proportion of females in the HC was reduced from 21% in year 2006 to 16% in year 2014. There was noticeable decline of both male and female HC in 2013 and 2014.
- There was a slight (but statistically significant) reduction in the number of hospital admission/HC in each year. There was no significant change in the number of A&E and SOPD attendance/HC in each year.
- The utilization of NIV increased rapidly from 2006 and reached a peak in 2010 with 29% of HC requiring NIV, but the usage declined in year 2011 to 2014.
- There was a rapid increase in the prescription of LABA and/or LAMA from 15% to 64%. The prescription of ICS (with or without LABA/LAMA) was high throughout the period (73% to 87%).
- The first year mortality rate in each year was stable at around 17%, but death due to COPD was decreasing and death due to pneumonia was increasing.
- The mean age of COPD patients with hospital admissions and age at death was slowly increasing for both males and females. The age at death of COPD patients was close to that of the general population for both gender.
- The number of new cases of COPD requiring hospital admission reduced over the years. COPD admissions were largely contributed by patients with repeated admissions, particularly male patients.
- The cumulative survival of the COPD HC ever admitted to HA hospital in and after 2006 was gradually increasing in the community and seemed to plateau off to just over 19,000 HC at the end of 2014.
The population in HK increased from over 6.8 million in 2006 to over 7.2 million in 2014. The male: female ratio was around 1:1.06.9 The important finding of the present study is that the trend of progressive decline in mortality and hospitalization rate due to COPD between 1997 and 2005, as revealed in previous report,2 was continued in year 2006 to 2014. We have observed a decreasing trend of the number of COPD admissions, as well as the number of individual COPD patients (HC) requiring hospital admission. We have also observed a trend of decreasing severity of the disease as evidenced by the decreasing need of NIV during admissions for COPD exacerbations and decreasing mortality due to COPD.
As cigarette smoking is the major cause of COPD in HK as in most western population, the gradual decline in COPD admissions and HC (especially in female throughout the whole period and both gender in 2013 and 2014) was likely related to decline in the prevalence of smoking.2,8 As the effect of smoking may take up to 15–25 years,10,11 we have searched for the smoking pattern in HK about 20 years before our study period. Survey in year 1982 showed that 39.7% of male age 15 or above were daily smokers, compared with 5.6% for females. The corresponding figures for the 1988 survey were 30.0% and 2.9%, respectively.12 The lower percentage of smokers, especially in females, might explain the decreasing number of COPD HC, especially females, more than 20 years later. As in 2017, the prevalence of smoking in HK was 10.0% (male 18.1%, female 2.7%),13 we would expect the problem of COPD to reduce further in future.
The proportion of HC requiring use of NIV increased rapidly from 5.7% in 2006 to a peak of 28.6% in 2010. Thereafter, the percentage dropped gradually to 18.4% in 2014. The initial rapid rise in NIV utilization from 2006 to 2010 was probably the result of promotion of the technique among general and respiratory physicians. To the best of our knowledge, the only territory-wide report of NIV use in COPD patients admitted to hospital in HK was 23% in year 2012.3 There was no change in the practice or coding for NIV in COPD patients over the years. The decline in utilization of NIV from 28.6% of admissions in year 2010 to 18.4% in year 2014 probably reflected in a decrease in the severity of the COPD disease rather than a change in policy or practice.
Subsequent to the finding of decreasing number and severity of COPD patients admitted to hospital from 2010 onwards, we had tried to look for other factors besides reducing prevalence of smoking in the community. TB is a well-known contributory factor of COPD.14–16 Notification rate of TB gradually declined from 1995 (101/100,000 population) to 2014 (65/100,000 population) in HK with small fluctuations in between.17 There was a trend of modest decline in the number and proportion of HC with TB as comorbidity of COPD from 13.2% in 2006 to 10.5% in 2014 (p < 0.0001) (Table 1). However, we observed a small peak of old TB affecting the respiratory tract as a comorbidity of COPD (14.0%) in year 2010, which coincided with the small peak in the utilization of NIV (Table 3). In the PLATINO study18 it was reported that a history of pulmonary TB was associated with more severe GOLD stages of COPD. A more recent report had shown that COPD patients with history of TB had reduced respiratory functions, increased PaCO2 and died earlier compared to the patients without history of TB.19 In our present study, the number of COPD patients with past history of old TB who received NIV also showed a peak in 2010. Almost 42% of COPD with past history of old TB received NIV in year 2010 (Table 3). We may perhaps postulate that chronic effect of old TB was an important contributory factor for severe COPD, so that a significant proportion of these patients required NIV during an acute COPD exacerbation. Reduction of TB in the community might be one of the explanations for the reducing number and proportion of patients requiring NIV after 2010. As the notification rate of TB in HK continues to fall over the years, from 65 in 2014 to 57.5/100,000 population in 2017,17 further studies are warranted to study the effect of decreasing prevalence of TB on the prevalence and severity of COPD in HK.
For the inhalers used for COPD, a previous multicenter study in 2005 with 153 patients from HK showed that the use of LABA or LAMA was the lowest among the countries studied (LABA 2.6%, tiotropium 1.9%, and LABA/ICS 12.5%).20 In the present study, the prescription of LABA and/or LAMA experienced a dramatic increase from 14.6% in 2006 to 63.5% in 2014. We also observed a high proportion of COPD patients being prescribed ICS (with or without LABA/LAMA) with an increasing trend from 72.9% in 2006 to 87.3% in 2014. As most of the LABAs in HK were marketed in combination with an ICS, the marked increase in the prescription of LABA might explain the modest increase of ICS prescription for COPD patients. With the recognition that ICS might increase the incidence of pneumonia21 and the restricted prescription of ICS to group E COPD patients with high eosinophil counts,1 it is interesting to know whether the high usage of ICS in COPD patients in HK may decrease in recent years. Further studies are required to find out whether the more common prescriptions of LABA/LAMA with or without ICS have contributed to the lower COPD admission/HC and lowering mortality related to COPD.
To explore the potential confounding impact of air pollution in this study, available data on air quality in HK from the Environmental Protection Department of HK22 were reviewed. It appeared that the air quality of HK showed some, though may not be significant, improvement over the study period. Thus, we believed that this largely static air quality over the study period may not have significant impact in the observed small changes in the number of COPD admissions per HC over the same study period.
While the major cause of reduction in COPD HC was likely due to the reduction in smoking habit (especially in female subjects), the cause of the reducing number of hospital admission/HC was multi-factorial. There was no change in the regulation or requirement from HA on the admission or timing of hospitalization for patients with COPD. Patient support programs organized by some hospitals, more common prescription of LAMA/LABA (with or without ICS), and perhaps the improving air quality in HK may have contributed to the reduction of hospital admission per HC. Further prospective studies are required to find out whether and how much these interventions have resulted in reduction of COPD admissions.
The mean age at death of patients with COPD increased gradually over the years for both male and female (Table 4), from a mean age of 78 years in males and 84 years of age in females in 2006, to 80 in males and 86 years of age in females, respectively, in year 2014. These mean age were very close to the expectation of life for the general population in HK of 81 for males and 87 years of age for females, respectively.9 In addition, we observed a changing pattern with increasing number of deaths due to pneumonia and reducing number of deaths due to COPD (Table 5). To the best of our knowledge, there was no change in the coding practice for COPD or pneumonia over the study period. Patients (for both gender) who died from pneumonia were about 2 years older than those who died from COPD. Retrieval of the leading causes of death of the general population in HK showed that in 2001, 45.1/100,000 population died of pneumonia (the 2nd leading cause of death, after malignant neoplasms of any organ).23 In 2014, the figure for pneumonia was 103.8/100,000 and in 2021, the figure further increased to 132.6/100,000 population (almost 3 times the figure in 2001). Pneumonia remained the 2nd leading cause of death in 2021 (after malignant neoplasms of any organ).23 Therefore, the increasing number of deaths due to pneumonia was a phenomenon in the general population, and not just a phenomenon in COPD patients. The exact cause of the increasing number of deaths due to pneumonia was unknown, but most likely related to a decline in immunity with ageing. Augmentation of the vaccination program in the general public and particularly in COPD patients may help to reduce deaths related to pneumonia. The reducing number of deaths due to COPD might be due to patients having less severe disease, probably related to reduced smoking and TB notification in the community. The prescription of ICS was common over the period but by itself could not account for the increasing number of death due to pneumonia.21
The improving trend COPD that we observed in HK with a population of 7.2 million may not be an isolated incidence. Cigarette smoking is a major cause of COPD in HK as in most western population. Our experience showed that the control of smoking about 20 years earlier can significantly reduce the number of new patients with COPD who require hospital admission (group E in the GOLD strategy 2023).1 We have also observed that in this group E COPD patients, with adequate treatment and support, their life expectancy can be close to that of the general population. We have observed an increasing trend of mortality due to pneumonia in the general and COPD population in the elderly. It is of paramount importance to strengthen the vaccination program for the elderly population, whether they have underlying COPD or not.
In developing countries where TB is still prevalent, our experience showed that the combination of “COPD” and “late effect of respiratory TB” can result in severe COPD, especially those who required assisted ventilation (NIV/IMV). With adequate TB control programs, it is hoped that the number of subjects with co-existing COPD and old TB can be reduced and possibly leading to reduction in number of patients with severe COPD.
The major limitation of the present study is that the data depends on the accuracy and completeness in the coding of discharge diagnoses and procedures. As the coding for principal and secondary diagnoses and procedures (especially NIV and IMV) were compulsory in the CMS and there was regular checking by audit teams of HA, we believed that this information was mostly correct and reliable. Information of individual patients which required case record review such as radiographic changes and lung function parameters were outside the scope of this study. Further studies are required to confirm some of the observations and postulations made in the present study.
Conclusion
COPD is a common cause of hospital admission and healthcare burden. We have demonstrated a progressive decline in the admission number, HC and severity of disease of COPD patients requiring hospital admission in HK from year 2006 to 2014. The decreasing trend was particularly observed in female patients. The utilization of NIV increased rapidly from year 2006 and reached a peak in 2010. The decreasing trend of COPD admission number and HC probably reflected the decreasing trend of smoking habit in the community. The decreasing TB notification in the community might reduce the co-incidence of COPD with old TB, especially those with severe disease requiring NIV during acute exacerbations. The number of new cases of COPD requiring hospital admission was decreasing, and increasing percentage of COPD admissions were due to re-admissions, especially male patients. The mortality rate of COPD patients remained quite stable but the age at death of COPD patients was slowly increasing. The age at death of COPD patients was close to the general population for both male and female. Pneumonia and COPD were common causes of mortality. Increasing percentage of death due to pneumonia might reflect the older age and declining immunity of the COPD patients, a phenomenon which is also observed in the general population in HK. The cumulative survival of COPD patients who were ever admitted to hospital showed a gradual accumulation in the community but seemed to plateau at around 19,000 HC in year 2014. Control of smoking, TB notification and air quality in the community, better planned ambulatory care of the COPD patients, optimal use of LABA/LAMA combination (with/without ICS) may reduce or delay their COPD admission and lighten the burden on the healthcare system in future. Comprehensive and timely vaccination for targeted viruses and bacteria might reduce the pneumonia risks in COPD patients as in the elderly population.
Acknowledgments
We would like to thank Ms. Reling Tse of Medial Records Office for generating the patient statistics from CDARS. We would also like to thank Dr Thomas Mok, Dr KS Lau, Dr Wilson Yee, Dr YC Yeung, Dr Veronica Chan, Dr CH Chau, Dr FY Kong, Dr Jane Cheung, Dr PY Tse as co-ordinators for the hospitals involved in this study and the HK Lung Foundation for sponsoring this project.
Disclosure
All authors reported no conflicts of interest in this work and received no personal fee from any grant or commercial companies.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease; 2023. Available from: https://goldcopd.org/2023-gold-report2/.
2. Chan-Yeung M, Lai CK, Chan KS, et al. The burden of lung disease in Hong Kong: a report from the Hong Kong Thoracic Society. Respirology. 2008;13(Suppl 4):S133–65. doi:10.1111/j.1440-1843.2008.01394.x
3. Chan HS, Fo FWS, Chan JWM, et al. Comorbidities, mortality, and management of chronic obstructive pulmonary disease patients who required admissions to public hospitals in Hong Kong - computerized data collection and analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1–13. doi:10.2147/COPD.S163659
4. Wong MC, Jiang JY, Tang JL, Lam A, Fung H, Mercer SW. Health services research in the public healthcare system in Hong Kong: an analysis of over 1 million antihypertensive prescriptions between 2004–2007 as an example of the potential and pitfalls of using routinely collected electronic patient data. BMC Health Serv Res. 2008;8:138–146. doi:10.1186/1472-6963-8-138
5. Yip TC, Chan HL, Wong VW, Tse YK, Lam KL, Wong LH. Impact of age and gender on risk of hepatocellular carcinoma after hepatitis B surface antigen seroclearance. J Hepatol. 2017;67:902–908. doi:10.1016/j.jhep.2017.06.019
6. Lozano NM, Foreman K, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380:2095–2128. doi:10.1016/S0140-6736(12)61728-0
7. World Health Organisation. Fact sheets - chronic obstructive pulmonary disease. Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
8. Social Survey Section, Census and Statistics department, Hong Kong. Thematic household survey. Report No. 26; 2006. Available from: http://www.censtatd.gov.hk.
9. Census and Statistics department, the Government of the HKSAR. Population by sex and age group. Available from: http://www.censtatd.gov.hk.
10. Berend N. Epidemiolical survey of chronic obstructive pulmonary disease and alpha-1-antitrypsin deficiency in Australia. Respirology. 2001;6:S21–25. doi:10.1046/j.1440-1843.2001.00308.x
11. Rycroft CE, Heyes A, Lnaza L, Becker K. Eidemiology of chronic obstructive pulmonary disease: a literature review. Int J Chron Obstruct Pulmon Dis. 2012;7:457–494. doi:10.2147/COPD.S32330
12. Social data collected by the general household survey: special topics. Report No. V, 1989. Available from: http://www.censtatd.gov.hk.
13. Social Survey Section, Census and Statistics department, Hong Kong. Thematic household survey. Report No. 64, 2018. Available from: http://www.censtatd.gov.hk.
14. Lee SH, Hwang ED, Lim JE, et al. The risk factors and characteristics of COPD among nonsmokers in Korea: an analysis of KNHANES IV and V. Lung. 2016;194:353–361. doi:10.1007/s00408-016-9871-6
15. Amaral AF, Coton S, Kato B, et al. Tuberculosis associates with both airflow obstruction and low lung function: BOLD results. Eur Respir J. 2015;46:1104–1112. doi:10.1183/13993003.02325-2014
16. Alwood BW, Myer L, Bateman ED. A systematic review of the association between pulmonary tuberculosis and the development of chronic airflow obstruction in adults. Respiration. 2013;86:76–85. doi:10.1159/000350917
17. Center for Health Protection HKSAR. Tuberculosis Notification; 2016. Available from: http://www.chp.gov.hk/tc/static/24012.html.
18. Medezes AM, Hallal PC, Petrez-Padilla R, et al. Tuberculosis and airflow obstruction: evidence from the PLATINO study in Latin America. Eur Respir J. 2007;30:1180–1185. doi:10.1183/09031936.00083507
19. Yakar HI, Gunen H, Pehlivan E, Aydogan S. The role of tuberculosis in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:323–329. doi:10.2147/COPD.S116086
20. Miravitlles M, Murio C, Tirado-Conde G, et al. Geographic differences in clinical characteristics and management of COPD: the EPOCA study. Int J Chron Obstruct Pulmon Dis. 2008;3:1–12. doi:10.2147/COPD.S4257
21. Crim C, Calvery PMA, Anderson JA, et al. Pneumonia risk in COPD patients receiving corticosteroids alone or in combination: TORCH study results. Eur Respir J. 2009;34:641–647. doi:10.1183/09031936.00193908
22. Environmemtal Protection Department of HK. Pollutant long term trends (1990–2020); Available from: https://www.epd.gov.hk.
23. Centre for Health Protection. Death rate by leading causes of death, 2001–2021. Available from: https://www.chp.gov.hk/en/statistics/data/10/27/117.html#.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.