Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Characteristics of Current Smokers versus Former Smokers with COPD and Their Associations with Smoking Cessation Within 4.5 Years: Results from COSYCONET
Authors Alter P ![]() , Stoleriu C, Kahnert K, Henke MO, Bals R, Trudzinski FC
, Stoleriu C, Kahnert K, Henke MO, Bals R, Trudzinski FC ![]() , Watz H, Speicher T, Söhler S
, Watz H, Speicher T, Söhler S ![]() , Welte T
, Welte T ![]() , Rabe KF
, Rabe KF ![]() , Wouters EFM, Vogelmeier CF, Jörres RA
, Wouters EFM, Vogelmeier CF, Jörres RA ![]()
Received 14 September 2023
Accepted for publication 13 November 2023
Published 6 December 2023 Volume 2023:18 Pages 2911—2923
DOI https://doi.org/10.2147/COPD.S436669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Peter Alter,1 Cosmina Stoleriu,2 Kathrin Kahnert,3,4 Markus Oliver Henke,5 Robert Bals,6 Franziska C Trudzinski,7 Henrik Watz,8 Tim Speicher,1 Sandra Söhler,1 Tobias Welte,9 Klaus F Rabe,10,11 Emiel FM Wouters,12,13 Claus F Vogelmeier,1 Rudolf A Jörres14
1Department of Medicine, Pulmonary, Critical Care and Sleep Medicine, Philipps University of Marburg (UMR), Member of the German Center for Lung Research (DZL), Marburg, Germany; 2Asklepios Lungenklinik Gauting, Comprehensive Pneumology Center Munich (CPC-M), Member of the German Center for Lung Research (DZL), Gauting, Germany; 3Department of Medicine V, LMU University Hospital, LMU Munich, Comprehensive Pneumology Center Munich (CPC-M), Member of the German Center for Lung Research (DZL), Munich, Germany; 4MediCenterGermering, Germering, Germany; 5Klinik für Innere Medizin und Pneumologie, Krankenhaus Martha-Maria, Munich, Germany; 6Department of Internal Medicine V, Pulmonology, Allergology, Intensive Care Medicine, Saarland University Hospital, Homburg, Germany; 7Department of Pneumology and Critical Care Medicine, Thoraxklinik, University of Heidelberg, Translational Lung Research Center Heidelberg (TLRC-H), Member of the Center for Lung Research (DZL), Heidelberg, Germany; 8Pulmonary Research Institute at LungenClinic Grosshansdorf, Airway Research Center North (ARCN), Member of the German Center for Lung Research (DZL), Grosshansdorf, Germany; 9Clinic for Pneumology, Hannover Medical School, Member of the German Center for Lung Research (DZL), Hannover, Germany; 10LungenClinic Grosshansdorf, Airway Research Center North (ARCN), Member of the German Center for Lung Research (DZL), Grosshansdorf, Germany; 11Department of Medicine, Christian-Albrechts-University, Kiel, Germany; 12Department of Respiratory Medicine, Maastricht University Medical Centre, Maastricht, Netherlands; 13Ludwig Boltzmann Institute for Lung Health, Vienna, Austria; 14Institute and Outpatient Clinic for Occupational, Social and Environmental Medicine, LMU University Hospital, LMU Munich, Comprehensive Pneumology Center Munich (CPC-M), Member of the German Center for Lung Research (DZL), Munich, Germany
Correspondence: Peter Alter, Department of Medicine, Pulmonary, Critical Care and Sleep Medicine, Philipps University of Marburg (UMR), Member of the German Center for Lung Research (DZL), Baldingerstrasse 1, Marburg, 35033, Germany, Tel +49 6421 5866140, Email [email protected]
Background: Many patients with chronic obstructive pulmonary disease (COPD) continue smoking. We used data from the “real-life” COSYCONET COPD cohort to evaluate whether these patients differed from patients with COPD who either had ceased smoking prior to inclusion or ceased during the follow-up time of the study.
Methods: The analysis was based on data from visits 1– 5 (covering 4.5 years), including all patients with the diagnosis of COPD who were either ex-smokers or smokers and categorized as GOLD 1– 4 or the former GOLD 0 category. We compared the characteristics of smokers and ex-smokers at baseline (visit 1), as well as the course of lung function in the follow-up of permanent ex-smokers, permanent smokers and incident ex-smokers (smokers at visit 1 who ceased smoking before visit 5). We also identified baseline factors associated with subsequent smoking cessation.
Results: Among 2500 patients who were ever-smokers, 660 were current smokers and 1840 ex-smokers at baseline. Smokers were younger than ex-smokers (mean 61.5 vs 66.0 y), had a longer duration of smoking but fewer pack-years, a lower frequency of asthma, higher forced expiratory volume in 1 sec (FEV1, 59.4 vs 55.2% predicted) and higher functional residual capacity (FRC, 147.7 vs 144.3% predicted). Similar results were obtained for the longitudinal subpopulation, comprising 713 permanent ex-smokers, 175 permanent smokers, and 55 incident ex-smokers. When analyzing the time course of lung function, higher FRC, lower FEV1 and the presence of asthma (p < 0.05 each) were associated with incident cessation prior to visit 5, while less airway obstruction was associated with smoking continuation.
Conclusion: These findings, which were consistent in the cross-sectional and longitudinal analyses, suggest that lung hyperinflation was associated with being or becoming ex-smoker. Possibly, it is perceived by patients as one of the factors motivating their attempts to quit smoking, independent from airway obstruction.
Keywords: COPD, smoking, smoking cessation, airway obstruction, lung hyperinflation
Introduction
Despite tobacco smoking being recognized as a major cause of chronic obstructive pulmonary disease (COPD),1,2 a surprisingly high number of patients with COPD continue to smoke.3 Even in longitudinal study cohorts, in which one could expect above-average insight into the causes and driving factors of COPD, a significant proportion continues smoking.4 Many studies have compared non-smoking healthy subjects, smokers without the diagnosis of COPD,5 and COPD patients who were ex-smokers or current smokers,6–9 while the number of studies specifically comparing smokers and ex-smokers with COPD is limited.10,11
Given the high percentage of current smokers among COPD patients, the question naturally arises as to how patients who have stopped smoking differ from those who continue smoking. The second question is whether clinical and functional characteristics are associated with an increased or decreased likelihood to stop smoking in the future. To address these questions, the COPD cohort COSYCONET (COPD and Systemic Consequences – Comorbidities Network)4 seems well suited, as it comprises a large number of patients, a follow-up over several years, and a broad panel of clinical and functional indices. The present analysis used data from this cohort with a follow-up time of 4.5 years, to address the topic in four ways. We performed (1) a cross-sectional comparison of ex-smokers and current smokers at baseline, (2) a cross-sectional comparison of patients who remained ex-smokers, or ceased smoking within the follow-up period, or remained smokers, (3) a longitudinal description of the time course of lung function during follow-up for these groups, and (4) we sought to identify baseline characteristics associated with the transition from smoker to ex-smoker during the follow-up.
Methods
Study Population
COSYCONET is an ongoing, long-term, observational multi-center cohort of patients with COPD. Patients of Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades 1 to 4 were included, as well as patients of the former GOLD grade 0 referring to patients with chronic bronchitis without fulfilling the spirometric criterion forced expiratory volume in 1 s to forced vital capacity ratio (FEV1/FVC) <0.7.12 Details of the COSYCONET study design, baseline characteristics, and in- and exclusion criteria have been described previously.4 Follow-up visits were conducted at 6, 18, 36 and 54 months after enrolment (visits 2 to 5). The analysis comprised two study populations, first that of visit 1 for cross-sectional analysis, and second that of patients remaining in the study until visit 5 for longitudinal analysis. COSYCONET was approved by the ethics committees of all study centers and conducted in accordance with the Declaration of Helsinki. All participants provided their written informed consent. ClinicalTrials.gov: NCT01245933.
Assessments
Baseline characteristics including age, sex, body mass index (BMI) and post-bronchodilator lung function values. We measured FEV1 and FVC following recommendations and used Global Lung Function Initiative (GLI) equations to express the results as % predicted in order to facilitate interpretation.13 Body plethysmography was used to determine functional residual capacity (FRC) and residual volume (RV), using European Coal and Steel Community (ECSC) reference values.14 Single-breath diffusing capacity for carbon monoxide (CO) included the transfer factor (TLCO) and its coefficient (KCO, ratio of TLCO to alveolar volume), expressed as % predicted relative to GLI reference values.15 In addition, 6-minute walking distance (6MWD) was assessed following a standard protocol,4 expressed as percent of published predicted values.16
Patients were categorized into spirometric GOLD grades 0 (FEV1/FVC ≥0.7) or 1 to 4 (FEV1/FVC <0.7), and as GOLD groups A, B or E based on symptoms assessed via the modified Medical Research Council (mMRC) dyspnea scale.2 Besides the COPD Assessment Test (CAT),17–19 we used the Saint George’s Respiratory Questionnaire (SGRQ) including its Activity, Impact and Symptoms domains20 for the assessment of disease-related quality of life.21 The assessment of self-reported comorbidities was based on patient-reported physician-based diagnoses22,23 and included asthma, cardiac failure and coronary artery disease; the latter two were combined into cardiac disease.24 These two comorbidities were chosen, as their presence might be hypothesized to be associated with the likelihood of smoking cessation. The ankle-brachial index (ABI) was used as a marker of peripheral vascular state.25
Smoking History and Status
A detailed smoking history was assessed upon enrolment. History included total years of smoking, pack-years, the age at initiation and since quitting, as well as whether parents had smoked or there were other smokers in the household. Patients were categorized at baseline into current and ex-smokers; never-smokers were excluded from the present analysis and have been characterized in this cohort previously.26 Smoking status was assessed at each visit until visit 5. Based on this, the group of incident ex-smokers could be defined as patients who were smokers at visit 1 and reported smoking cessation at visit 5.
Study Questions
First, baseline characteristics of active and previous smokers at enrolment were compared. Second, we used the follow-up data and compared baseline characteristics in the three groups of permanent ex-smokers, permanent smokers, and incident ex-smokers. This was done in order to test the consistency of our findings between data upon inclusion and data after follow-up. Third, the course of lung function over follow-up was analyzed for these three groups. Fourth, factors at baseline were identified that were associated with smoking cessation during follow-up.
Statistical Analysis
For descriptive purposes, mean values and standard deviations (SD) or numbers and percentages are given, depending on the type of data. Differences between two groups were analyzed using non-parametric Mann–Whitney-U statistics, in case of categorical variables using Fisher’s exact for 2 × 2 tables. In case of more than three groups or categories, chi-square statistics were computed, or the Kruskal–Wallis test was applied, with Bonferroni-adjusted post hoc comparisons via the Mann–Whitney-U-test. Mixed linear models (GLM) with repeated-measures design and logit link (equivalent to longitudinal logistic regression analysis) were used to examine the time course of lung function in relation to smoking status. To identify predictors of smoking cessation during follow-up, binary logistic regression analysis was used, taking patient characteristics at visit 1 as predictors and the transition from smoker to incident ex-smoker until visit 5 as binary outcome. For all computations, the software package IBM SPSS Statistics (Version 26.0.0.0, Armonk, NY, USA) was employed.
Results
Study Population
COSYCONET enrolled 2741 patients with a diagnosis of COPD at visit 1, with GOLD grades available for 2721 patients (Figure 1). A total of 217 patients were never-smokers, with smoking history not available for 4 patients; these were excluded. The remaining 2500 patients comprised 660 active smokers and 1840 ex-smokers, with 363 categorized as former GOLD 0. At visit 5, 943 patients remained in the study.
 |
Figure 1 Flow chart of study population. Grey boxes indicate the study populations. |
Comparison of Ex-Smokers and Current Smokers at Baseline
Smoking History
On average, current smokers had a lower number of pack-years (p < 0.001) but a longer duration of smoking (p < 0.001) and started smoking at a younger age (p = 0.013) than ex-smokers (Table 1). Ex-smokers had ceased smoking on average (SD) 13.2 (12.7) years prior to enrolment. The status of active versus ex-smoker significantly (p < 0.001) was associated with the number of parents who had smoked. When none had smoked, the percentage of active smokers was 21.1%, when one had smoked, 26.2%, and when both had smoked, 34.6%. The proportion of current smokers was also higher if other persons in the household smoked (46.0% vs 21.7%, p < 0.001).
 |
Table 1 Patient Characteristics at Visit 1 |
Clinical and Functional Characteristics
Current smokers were more likely to be female than ex-smokers (p < 0.001, Table 1), were on average about 4.5 years younger than ex-smokers (p < 0.001) and had a lower BMI (p < 0.001). There were also differences in the distribution of GOLD grades and groups (p < 0.001), with grades 3 and 4 and group E being less common in active smokers.
FEV1% predicted, FVC % predicted, FEV1/FVC, FRC % predicted and RV % predicted were all significantly higher in smokers, while KCO % predicted was lower (p < 0.05 each, Table 1). There were no significant differences in TLCO % predicted. ABI was significantly lower in smokers compared to ex-smokers (p = 0.005). CAT total score did not significantly differ between groups (Table 1). SGRQ total score (p = 0.004) and the Activity domain (p < 0.001) were lower (ie, better) in current smokers than ex-smokers, whereas the Symptoms domain was higher (ie, worse; p < 0.001). There were no significant differences in the proportion of asthma or cardiac disease. 6MWD % predicted did not differ between smokers and ex-smokers (p = 0.23).
Comparison of Baseline Characteristics of Permanent Ex-Smokers, Permanent Smokers and Incident Ex-Smokers
Smoking Status
None of the ex-smokers at visit 1 started smoking during follow-up. Among the 943 patients at visit 5, 713 were permanent ex-smokers, 175 permanent smokers, and 55 incident ex-smokers (Table 2). Among the incident ex-smokers, the numbers of patients who had stopped smoking at visits 2, 3, 4 and 5, were 15, 40, 48, and 55, respectively.
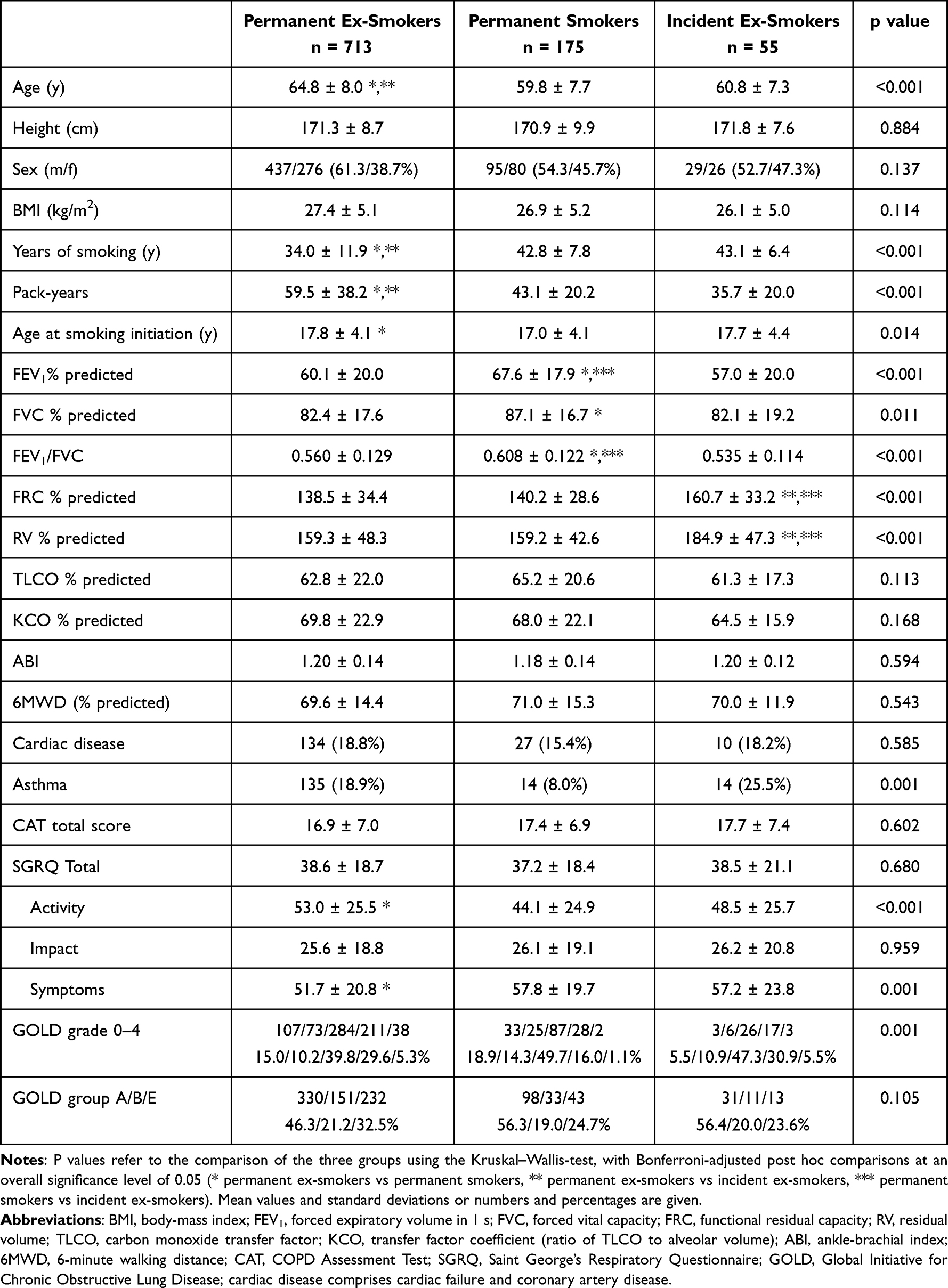 |
Table 2 Patient Characteristics at Visit 1 of the Longitudinal Cohort with Follow-Up Until Visit 5 |
According to post-hoc comparisons, the average smoking pack-years at baseline were higher in the permanent ex-smokers than the two other groups, while their total years of smoking were smallest (p < 0.001). With two smoking parents, the proportion of permanent smokers was higher and that of permanent ex-smokers lower than if either none or one of the parents had smoked (p = 0.020). In addition, the proportion of permanent smokers was highest if other persons in the household were current smokers (p < 0.001), whereas the likelihood of quitting smoking was highest when no other persons in the household smoked (p = 0.032).
Clinical and Functional Characteristics
Groups did not significantly differ in the distributions of sex or GOLD groups, but there was a difference (p < 0.001) in spirometric GOLD grades, with grades 3 and 4 being less frequent in permanent smokers. Age was highest in the group of permanent ex-smokers (p < 0.001). FEV1% predicted, FVC % predicted, FEV1/FVC, FRC % predicted and RV % predicted differed significantly between the three groups (p < 0.05 each), while BMI, TLCO % predicted, KCO % predicted, 6MWD % predicted and ABI did not. The results of adjusted pairwise comparisons are indicated in Table 2.
The three groups also did not differ significantly in terms of CAT score or SGRQ total score or Impact domain. In contrast, the SGRQ Symptom domain was highest (ie, worst) and the Activity domain lowest (ie, best) in the permanent smokers (p < 0.001). Asthma was much more frequent in incident ex-smokers compared to permanent smokers (p = 0.001; Table 2).
Time Course of FEV1 and FRC During Follow-Up for Permanent Ex-Smokers, Permanent Smokers, or Incident Ex-Smokers
FEV1% predicted and FRC % predicted were selected to monitor the time course of lung function (Figure 2A and B, respectively). The initially higher value of FEV1% predicted in permanent smokers was maintained over 4.5 years; incident ex-smokers had the highest average FRC % predicted, especially upon inclusion.
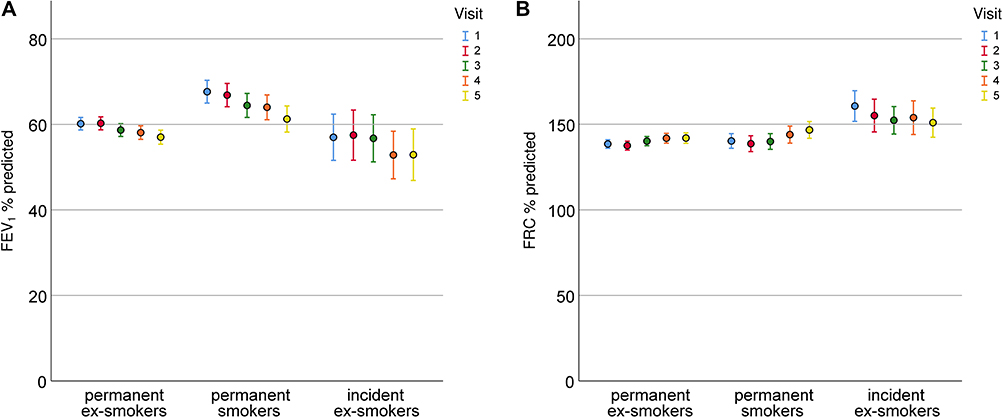 |
Figure 2 (A) Time course of FEV1% predicted in permanent ex-smokers, permanent smokers and incident ex-smokers over visits 1 to 5. (B) Time course of FRC % predicted in permanent ex-smokers, permanent smokers and incident ex-smokers over visits 1 to 5. Mean values and 95% confidence intervals are shown. Only patients remaining in the study until visit 5 were included in this graph. |
Analysis by a generalized linear model including visit, age and group as well as an interaction between visit and group confirmed that in the group of permanent smokers, the FEV1 rate of decline over time was greater than in permanent ex-smokers (p < 0.001), while it was similar to that of incident ex-smokers. Regarding FRC % predicted, the elevated baseline values in incident ex-smokers was confirmed (p < 0.001), with its rate of decline over time differing from those of the other two groups (p < 0.001 each).
Identification of Predictors of Smoking Cessation During Follow-Up
Using logistic regression analysis, we aimed to identify characteristics at visit 1 that were related to smoking cessation or maintenance at visit 5. In order to avoid complications from the inclusion of correlated predictors, a stepwise approach was used, comprising the separate analysis of different sets of potentially relevant predictors. We first included the SGRQ domains and GOLD groups as simultaneous predictors. These variables had no predictive value for smoking cessation. In the next step, lung function variables were analyzed, using FEV1% predicted, FRC % predicted, RV % predicted and TLCO % predicted as simultaneous predictors, together with age, sex and BMI, to cover different aspects of respiratory function. Only FEV1% predicted and FRC % predicted were significantly (p < 0.05) associated with smoking cessation. When using comorbidities as predictors, only asthma was significant (p = 0.001).
Finally, we combined the four lung function parameters, age, sex, BMI and asthma diagnosis in order to reveal whether they were statistically independent predictors. FEV1% predicted (p = 0.016), FRC % predicted (p = 0.012) and a history of asthma (p = 0.002) were again significantly associated with smoking cessation (Figure 3). The odds for smoking cessation within 4.5 years were increased by factor 4.26 (95% CI: 1.69, 10.72) in individuals with a diagnosis of asthma at visit 1, by 1.37 (1.07, 1.74) for a 10% higher value in FRC % predicted, and by 1.38 (1.06, 1.78) for a 10% lower value in FEV1% predicted.
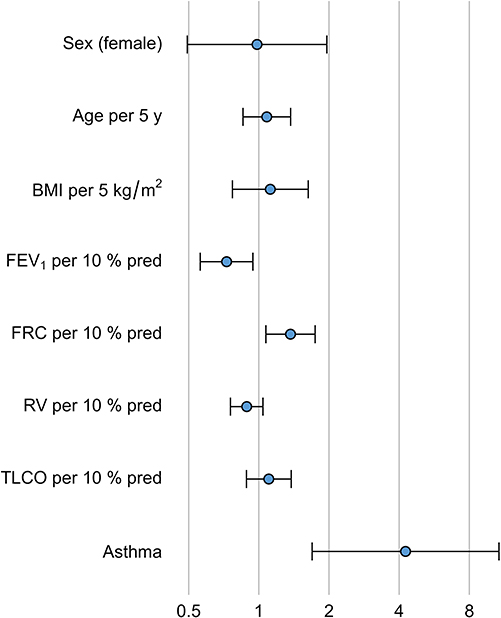 |
Figure 3 Variables associated with smoking cessation within the follow-up period of 4.5 y. Only patients who were smokers at visit 1 were included, and odds ratios and their 95% % confidence intervals are given for the various predictors at visit 1. BMI = body mass index, FEV1 = forced expiratory volume in 1 s, FRC = functional residual capacity, RV = residual volume, TLCO = diffusing capacity of the lung for carbon monoxide. The odds ratios refer to characteristics of patients at visit 1 in terms of the number of units as indicated and relative to the mean of the whole study population. |
Discussion
This study addressed the question which characteristics are shown by patients with COPD who still smoke. For this purpose, we compared patients who continued smoking with those who either had stopped smoking in the past or during a 4.5-year follow-up. When comparing smokers with ex-smokers upon inclusion, smokers had better spirometric lung function and reported more respiratory symptoms in terms of the SGRQ symptoms domain, but less burden from the disease as reflected in the Activity domain. Compared to ex-smokers, their smoking was less intense as indicated by the lower number of pack-years with longer duration of smoking.
Over the follow-up period, patients who were still smoking 4.5 years after inclusion showed the lowest airway obstruction in terms of FEV1 upon inclusion and over the follow-up time, whereas obstruction was similar in those who quitted and those who had quitted before. In contrast, lung hyperinflation in terms of FRC was similar in permanent smokers and permanent ex-smokers. Those who quit during the study (incident ex-smokers) showed the highest degree of hyperinflation at all visits, with a slight improvement over time (see Figure 2). In addition, the comorbidity asthma correlated with a higher probability of becoming ex-smoker. It therefore seemed that patients with COPD who continued smoking were those with less airway obstruction and lower frequency of asthma, whereas patients who stopped smoking had higher lung hyperinflation and obstruction and more often asthma.
The fact that so many patients with COPD continue to smoke seems especially astonishing in patients who participate in a long-term study, such as COSYCONET, as one might assume a greater-than-average awareness of the role of smoking in these patients. None of the ex-smokers upon inclusion became smokers, while during the follow-up 24% of 230 smokers stopped smoking and remained ex-smokers. We did not have detailed information on the participation in smoking cessation programs over the follow-up, but at the time of visit 5, 16% of permanent ex-smokers, 26% of permanent smokers and 33% of incident ex-smokers reported to have ever participated in a smoking cessation program, with no significant difference between permanent smokers and incident ex-smokers (Fisher’s exact test). The observation that the majority of these cessations (49/55) occurred until visit 3, ie in the first third of the 4.5-year follow-up period, seems to support the assumption that the participation in the cohort study was a large motivating factor in cessation.
The observation that patients who quitted smoking during the observation period showed markedly higher lung hyperinflation than those who continued smoking is of special interest. These patients also showed more hyperinflation than those who had already ceased smoking. On the other hand, they had a similar degree of airway obstruction as those who already had ceased smoking upon inclusion. The association between a high degree of lung hyperinflation and a higher likelihood to quit smoking was confirmed by the multiple regression analysis, while other potential determinants, ie elevated residual volume and impaired diffusing capacity, did not play a role.
In the absence of imaging data, we cannot determine whether hyperinflation also indicated a higher degree of lung emphysema, but the observation of a lower KCO in smokers and a tendency for lower KCO in permanent smokers would be compatible with this assumption. In addition, upon inclusion, ABI showed worse values in current smokers than ex-smokers. While KCO was adjusted for age by the use of predicted values, this was not the case for ABI. To elucidate the difference, we performed an additional regression analysis of the baseline data using the two groups of smokers vs ex-smokers, age, sex and FEV1% predicted as predictors. As a result, the small unadjusted difference in ABI of 0.021 units (Table 1) increased to 0.035 units when accounting for the covariates including age and airway obstruction, which are known to have an association with ABI.25 Thus, the vascular impairment in smokers was more pronounced than indicated by the raw data, in line with the hypothesis that smoking has particularly adverse effects on the vascular system, as reflected by ABI and KCO in our study.
Importantly, the association of elevated FRC and lower FEV1 with smoking cessation during follow-up was consistent with the findings regarding the baseline data (Figure 2, Table 1). It is important to note that in COPD not only obstruction but especially hyperinflation is a key determinant of dyspnea, particularly upon exertion, and that in many studies a reduction in lung hyperinflation by medical intervention has been found to be linked to improvements of dyspnea and exercise capacity.27–29
We do not believe that the lack of data on the patients’ psychological characteristics or their participation in smoking cessation programs invalidates our findings, since it is unlikely that the willingness to participate in such programs, or their success, or unknown social or psychological factors were, just by chance, correlated precisely with hyperinflation and obstruction. It seems more likely that the functional parameters were major determinants of the patients’ perceptions of their disease state and that these perceptions were linked to the attempts and success of cessation. Our finding is novel in demonstrating the independent role of lung hyperinflation as potential objective marker of the likelihood of smoking cessation, beyond the degree of airway obstruction.
When tentatively introducing three categories of education as covariates into the comparisons of groups,26 no significant associations were found (data not shown). However, the presence of smokers in the household was associated with smoking cessation, even within the follow-up time of 4.5 years. Given the fact that smoking cessation occurred more often when none of the other persons in the household smoked, the role of social factors in the continuation of habits such as smoking is underlined. The differences in the age at which smoking had been started were small and could not explain or predict smoking habits in the cohort. Among comorbidities, only asthma was associated with smoking cessation during follow-up. We do not know whether this was due to the medical information gained by the patients through participation in the study, but this might be a possibility.
The differences in the distribution of GOLD grades and groups were consistent with the general results that smokers at baseline and permanent smokers over the follow-up experienced fewer limitations from their COPD. In both the cross-sectional and the longitudinal analyses, the CAT sum score did not significantly differ between groups. The SGRQ Activity domain was higher (ie, worse) in the incident ex-smokers compared to the permanent smokers, and also higher in ex-smokers than current smokers, suggesting some association between smoking cessation and disease-related quality of life. This, however, was not strong enough to be significant in the multiple logistic regression analysis. Interestingly, exacerbation risk in terms of GOLD group E did not play a role.
Criteria for the diagnosis and categorization of COPD are well established.1,2 Especially, for the analysis of smoking habits, however, it seems reasonable to extend this population by including subjects with symptoms and clinical characteristics of COPD, even though they do not satisfy the functional criterion required by the classical definition.30 This comprises the group of patients “at risk” or “GOLD 0”31,32 in general and its subgroup with “preserved ratio impaired spirometry” (PRISm),12 among which patients with early COPD may be found.33 We therefore included these patients in the current analysis. The numbers of patients categorized as PRISm or GOLD 0 were, however, too low to allow for a meaningful separate analysis over the follow-up period.
Limitations
This study comprised cross-sectional and longitudinal elements, the major results of which were consistent. Despite this, a larger study population and a longer follow-up time would have allowed an analysis of the associations between patient characteristics and smoking habits in more detail, potentially including the interference with medication. In addition, more detailed information on attempts to quit smoking from previous times as well as during the follow-up might have been helpful, as well as information on the Fagerstrom test to quantify the degree of nicotine dependence. The asthma diagnosis was based on patient-reported physicians’ diagnoses and medication,24 and this approach has been successfully used in previous analyses of COSYCONET data.34 Despite this, it might have been helpful to have had additional markers such as blood eosinophils, but such data were not available in sufficient completeness in the present study population.
Conclusion
Based on data from a large “real-life” COPD cohort, we found that patients who continued smoking were younger and had a longer duration of smoking but fewer pack-years than ex-smokers. They also had less airway obstruction, but more lung hyperinflation. Consistent with this, in the follow-up a higher degree of hyperinflation was associated with a higher likelihood of smoking cessation, independent from airway obstruction. In addition, the presence of asthma was relevant, while a low degree of airway obstruction was associated with continuation of the smoking habit. These findings suggest that lung hyperinflation may be perceived by patients as major functional deterioration that favors smoking cessation in addition to airway obstruction.
COSYCONET Study Group
Andreas, Stefan (Lungenfachklinik, Immenhausen); Bals, Robert (Universitätsklinikum des Saarlandes); Behr, Jürgen and Kahnert, Kathrin (Klinikum der Ludwig-Maximilians-Universität München); Bahmer, Thomas (Universitätsklinikum Schleswig Holstein) and Bewig, Burkhard (Städtisches Krankenhaus Kiel); Ewert, Ralf and Stubbe, Beate (Universitätsmedizin Greifswald); Ficker, Joachim H. (Klinikum Nürnberg, Paracelsus Medizinische Privatuniversität Nürnberg); Grohé, Christian (Ev. Lungenklinik Berlin); Held, Matthias (Klinikum Würzburg Mitte gGmbH, Standort Missioklinik); Behr, Jürgen and Henke, Markus (Asklepios Fachkliniken München-Gauting); Herth, Felix (Thoraxklinik Heidelberg gGmbH); Kirsten, Anne-Marie and Watz, Henrik (Pneumologisches Forschungsinstitut an der Lungenclinic Grosshansdorf GmbH); Koczulla, Rembert (Schön Klinik Berchtesgadener Land); Kronsbein, Juliane (Berufsgenossenschaftliches Universitätsklinikum Bergmannsheil, Bochum); Kropf-Sanchen, Cornelia (Universitätsklinikum Ulm); Herzmann, Christian (Forschungszentrum Borstel); Pfeifer, Michael (Klinik Donaustauf); Randerath, Winfried J. (Wissenschaftliches Institut Bethanien e. V., Solingen); Seeger, Werner (Justus-Liebig-Universität Gießen); Studnicka, Michael (Uniklinikum Salzburg); Taube, Christian (Ruhrlandklinik gGmbH Essen); Timmermann, Hartmut (Hamburger Institut für Therapieforschung GmbH); Alter, Peter; Schmeck, Bernd and Vogelmeier, Claus (Universitätsklinikum Gießen und Marburg GmbH, Standort Marburg); Welte, Tobias (Medizinische Hochschule Hannover); Wirtz, Hubert (Universitätsklinikum Leipzig).
The study was based on patients recruited within the COSYCONET framework (ClinicalTrials.gov, Identifier: NCT01245933). For further information see Karch A, Vogelmeier C, Welte T, Bals R, Kauczor HU, Biederer J, Heinrich J, Schulz H, Glaser S, Holle R et al.: The German COPD cohort COSYCONET: Aims, methods and descriptive analysis of the study population at baseline. Respir Med 2016, 114:27–37.
Data Sharing Statement
COSYCONET is an ongoing, long-term, multi-center observational study the data of which are not intended to be available without demand. If there is interest in the analysis of specific questions, however, there is a formalized procedure for submitting an application to the study office, which will be evaluated by the steering committee on scientific grounds. There is no limitation for this application except proven expertise in COPD studies.
Ethics Approval and Consent to Participate
The study protocol was approved by the central ethical committee in Marburg (Ethikkommission FB Medizin Marburg) and the respective local ethical committees: Bad Reichenhall (Ethikkommission Bayerische Landesärztekammer); Berlin (Ethikkommission Ärztekammer Berlin); Bochum (Ethikkommission Medizinische Fakultät der RUB); Borstel (Ethikkommission Universität Lübeck); Coswig (Ethikkommission TU Dresden); Donaustauf (Ethikkommission Universitätsklinikum Regensburg); Essen (Ethikkommission Medizinische Fakultät Duisburg-Essen); Gießen (Ethikkommission Fachbereich Medizin); Greifswald (Ethikkommission Universitätsmedizin Greifswald); Großhansdorf (Ethikkommission Ärztekammer Schleswig-Holstein); Hamburg (Ethikkommission Ärztekammer Hamburg); MHH Hannover/Coppenbrügge (MHH Ethikkommission); Heidelberg Thorax/Uniklinik (Ethikkommission Universität Heidelberg); Homburg (Ethikkommission Saarbrücken); Immenhausen (Ethikkommission Landesärztekammer Hessen); Kiel (Ethikkommission Christian-Albrechts-Universität zu Kiel); Leipzig (Ethikkommission Universität Leipzig); Löwenstein (Ethikkommission Landesärztekammer Baden-Württemberg); Mainz (Ethikkommission Landesärztekammer Rheinland-Pfalz); München LMU/Gauting (Ethikkommission Klinikum Universität München); Nürnberg (Ethikkommission Friedrich-Alexander-Universität Erlangen Nürnberg); Rostock (Ethikkommission Universität Rostock); Berchtesgadener Land (Ethikkommission Land Salzburg); Schmallenberg (Ethikkommission Ärztekammer Westfalen-Lippe); Solingen (Ethikkommission Universität Witten-Herdecke); Ulm (Ethikkommission Universität Ulm); Würzburg (Ethikkommission Universität Würzburg). The study was performed in accordance with the declaration of Helsinki, and all participants gave their written informed consent.
Acknowledgments
We are grateful to all COSYCONET study centers, especially to all study nurses, for their excellent and enduring work in data collection, as well as to all patients who were willing to participate in this study over an extended period of time. We also thank David Young for helpful comments on the manuscript.
Author Contributions
All authors of this manuscript meet all of the following criteria required for authorship, as they 1) made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas, 2) have drafted or written, or substantially revised or critically reviewed the article, 3) have agreed on the “International Journal of COPD” as the Journal to which the article was submitted, 4) reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage, and 5) agree to take responsibility and be accountable for the contents of the article.
Funding
COSYCONET is supported by the German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET) and performed in collaboration with the German Center for Lung Research (DZL). The project is funded by the BMBF with grant number 01 GI 0881 and is supported by unrestricted grants from AstraZeneca GmbH, Bayer Schering Pharma AG, Boehringer Ingelheim Pharma GmbH & Co. KG, Chiesi GmbH, GlaxoSmithKline, Grifols Deutschland GmbH, MSD Sharp & Dohme GmbH, Mundipharma GmbH, Novartis Deutschland GmbH, Pfizer Pharma GmbH, Takeda Pharma Vertrieb GmbH & Co. KG, Teva GmbH for patient investigations and laboratory measurements. For the present study, an additional grant for data management was given by Novartis Pharma GmbH. The funding body had no involvement in the design of the study or the collection, analysis or interpretation of the data.
Disclosure
Dr Robert Bals reports grants from BMBF, during the conduct of the study; personal fees/grants from CSL Behring, DFG, GSK, and Schwiete Stifung, outside the submitted work. Prof. Dr Tobias Welte reports grants from German Ministry of Research and Education, during the conduct of the study; personal fees from AstraZeneca, Berlin-Chemie, Chiesi, GSK, Novartis, outside the submitted work. Prof. Dr Klaus Rabe reports personal fees from AstraZeneca, Boehringer Ingelheim, Berlin Chemie, Chiesi Pharmaceuticals, GSK, CSL Behring, Sanofi & Regeneron and shareholder of rnatics, outside the submitted work. Dr Claus Vogelmeier reports personal fees and/or grants from Aerogen, AstraZeneca, Boehringer Ingelheim, CSL Behring, Chiesi, GlaxoSmithKline, Grifols, Insmed, MedUpdate, Menarini, Novartis, Nuvaira, Roche, and Sanofi, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report gold executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1164/rccm.201701-0218PP
2. Agusti A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: gold executive summary. Am J Respir Crit Care Med. 2023;207(7):819–837. doi:10.1164/rccm.202301-0106PP
3. Radaeli A, Nardin M, Azzolina D, Malerba M. Determinants of smoking status in a sample of outpatients afferent to a tertiary referral hospital. Int J Environ Res Public Health. 2019;16(21):4136. doi:10.3390/ijerph16214136
4. Karch A, Vogelmeier C, Welte T, et al. The German COPD cohort COSYCONET: aims, methods and descriptive analysis of the study population at baseline. Respir Med. 2016;114:27–37. doi:10.1016/j.rmed.2016.03.008
5. Lederer DJ, Enright PL, Kawut SM, et al. Cigarette smoking is associated with subclinical parenchymal lung disease: the multi-ethnic study of atherosclerosis (mesa)-lung study. Am J Respir Crit Care Med. 2009;180(5):407–414. doi:10.1164/rccm.200812-1966OC
6. Tupper OD, Kjeldgaard P, Løkke A, Ulrik CS. Predictors of COPD in symptomatic smokers and ex-smokers seen in primary care. Chron Respir Dis. 2018;15(4):393–399. doi:10.1177/1479972318761655
7. Zhang PD, Zhang XR, Zhang A, et al. Associations of genetic risk and smoking with incident COPD. Eur Respir J. 2022;59(2):2101320. doi:10.1183/13993003.01320-2021
8. Salvi SS, Barnes PJ. Chronic obstructive pulmonary disease in non-smokers. Lancet. 2009;374(9691):733–743. doi:10.1016/S0140-6736(09)61303-9
9. Yang IA, Jenkins CR, Salvi SS. Chronic obstructive pulmonary disease in never-smokers: risk factors, pathogenesis, and implications for prevention and treatment. Lancet Respir Med. 2022;1010:497–511.
10. Josephs L, Culliford D, Johnson M, Thomas M. Improved outcomes in ex-smokers with COPD: a UK primary care observational cohort study. Eur Respir J. 2017;49(5):1602114. doi:10.1183/13993003.02114-2016
11. Wilson D, Adams R, Appleton S, Ruffin R. Difficulties identifying and targeting COPD and population-attributable risk of smoking for COPD: a population study. Chest. 2005;128128:2035–2042.
12. Wan ES, Fortis S, Regan EA, et al. Investigators CO: longitudinal phenotypes and mortality in preserved ratio impaired spirometry in the copdgene study. Am J Respir Crit Care Med. 2018;198(11):1397–1405. doi:10.1164/rccm.201804-0663OC
13. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40:1324–1343.
14. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, Yernault JC. Lung volumes and forced ventilatory flows. report working party standardization of lung function tests, European community for steel and coal official statement of the European respiratory society. Eur Respir J Suppl. 1993;16(Suppl 16):5–40. doi:10.1183/09041950.005s1693
15. Stanojevic S, Graham BL, Cooper BG, et al. Global lung function initiative twg, global lung function initiative t: official ers technical standards: global lung function initiative reference values for the carbon monoxide transfer factor for caucasians. Eur Respir J. 2017;50(3):1700010. doi:10.1183/13993003.00010-2017
16. Troosters T, Gosselink R, Decramer M. Six minute walking distance in healthy elderly subjects. Eur Respir J. 1999;14(2):270–274. doi:10.1034/j.1399-3003.1999.14b06.x
17. Jones PW, Harding G, Berry P, Wiklund I, Chen W-H, Kline Leidy N. Development and first validation of the COPD Assessment Test. Eur Respir J. 2009;34(3):648–654. doi:10.1183/09031936.00102509
18. Jones PW, Tabberer M, Chen WH. Creating scenarios of the impact of COPD and their relationship to COPD Assessment Test (CAT) scores. BMC Pulm Med. 2011;11(42). doi:10.1186/1471-2466-11-42
19. von Siemens S M, Alter P, Lutter JI, et al. CAT score single item analysis in patients with COPD: results from COSYCONET. Respir Med. 2019;159:105810.
20. Jones PW, Quirk FH, Baveystock CM, Littlejohns P. A self-complete measure of health status for chronic airflow limitation the St. George’s Respiratory Questionnaire. Am Rev Respir Dis. 1992;145:1321–1327.
21. Wacker ME, Jörres RA, Karch A, et al. Assessing health-related quality of life in COPD: comparing generic and disease-specific instruments with focus on comorbidities. BMC Pulm Med. 2016;16(70). doi:10.1186/s12890-016-0238-9
22. Alter P, Mayerhofer BA, Kahnert K, et al. Prevalence of cardiac comorbidities, and their underdetection and contribution to exertional symptoms in COPD: results from the COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. 2019;14:2163–2172. doi:10.2147/COPD.S209343
23. Alter P, Kahnert K, Trudzinski FC, et al. Disease progression and age as factors underlying multimorbidity in patients with COPD: results from COSYCONET. Int J Chron Obstruct Pulmon Dis. 2022;17:1703–1713.
24. Lucke T, Herrera R, Wacker M, et al. Systematic analysis of self-reported comorbidities in large cohort studies - a novel stepwise approach by evaluation of medication. PLoS One. 2016;11(10):e0163408. doi:10.1371/journal.pone.0163408
25. Houben-Wilke S, Jorres RA, Bals R, et al. Peripheral artery disease and its clinical relevance in patients with chronic obstructive pulmonary disease in the COPD and systemic consequences-comorbidities network study. Am J Respir Crit Care Med. 2017;195(2):189–197. doi:10.1164/rccm.201602-0354OC
26. Lutter JI, Jorres RA, Welte T, et al. Impact of education on COPD severity and all-cause mortality in lifetime never-smokers and longtime ex-smokers: results of the cosyconet cohort. Int J Chron Obstruct Pulmon Dis. 2020;15:2787–2798.
27. Tzani P, Crisafulli E, Nicolini G, et al. Effects of beclomethasone/formoterol fixed combination on lung hyperinflation and dyspnea in COPD patients. Int J Chron Obstruct Pulmon Dis. 2011;6:503–509. doi:10.2147/COPD.S23746
28. Thomas M, Decramer M, O’Donnell DE. No room to breathe: the importance of lung hyperinflation in COPD. Prim Care Respir J. 2013;22:101–111.
29. Soffler MI, Hayes MM, Schwartzstein RM. Respiratory sensations in dynamic hyperinflation physiological and clinical applications. Respir Care. 2017;62:1212–1223.
30. Mayerhofer B, Jorres RA, Lutter JI, et al. Deterioration and mortality risk of COPD patients not fitting into standard gold categories: results of the cosyconet cohort. Respiration. 2021;100(4):308–317. doi:10.1159/000513010
31. Pauwels RA, Buist AS, Calverley PM, From the global strategy for the diagnosis, management and prevention of COPD, global initiative for Chronic Obstructive Lung Disease (GOLD). Am J Respir Crit Care Med. 2001;163:1256–1276.
32. Pauwels RA, Buist AS, Ma P, Jenkins CR, Hurd SS, Committee GS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: national heart, lung, and blood institute and world health organization global initiative for Chronic Obstructive Lung Disease (GOLD): executive summary. Respir Care. 2001;46(8):798–825.
33. Han MK, Agusti A, Celli BR, et al. From GOLD 0 to Pre-COPD. Am J Respir Crit Care Med. 2021;203(4):414–423. doi:10.1164/rccm.202008-3328PP
34. Alter P, Kahnert K, Trudzinski CF, et al. Clinical factors linked to the type of respiratory medication in COPD: results from the COSYCONET cohort. Ther Adv Respir Dis. 2023;17. doi:10.1177/17534666231208584
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
An Exploration of Smoking Patterns Among People with Serious Mental Illness Attending an Outpatient Clinic in Qatar
Zolezzi M, Al-Rawi S, Eltorki Y
Neuropsychiatric Disease and Treatment 2022, 18:2847-2854
Published Date: 7 December 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies
Byanova KL, Abelman R, North CM, Christenson SA, Huang L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2795-2817
Published Date: 29 November 2023
The Effects of Smoking and Airway Restriction on Subclinical Atherosclerosis
Yeşildağ M, Keskin Z, Yavşan DM, Bekci TT, Osmanoglu UO
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1217-1226
Published Date: 24 April 2025
Insights Into Electronic-Cigarette Perspectives: Smokers’ Knowledge Attitudes and Practices at Hamad Medical Corporation, 2020
Chehab M, Abdu Y, Alkubaisi NJ, Al Mulla A, Bougmiza MI
Substance Abuse and Rehabilitation 2025, 16:223-237
Published Date: 30 August 2025