Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Level of Awareness About Chronic Obstructive Pulmonary Disease Among Active Smokers
Authors Al-Otaibi HM ![]() , Homoud MM, Alqarni MM, Alsobhi GJ, Al-Otaibi GZ, Alnahdi NA
, Homoud MM, Alqarni MM, Alsobhi GJ, Al-Otaibi GZ, Alnahdi NA
Received 24 November 2025
Accepted for publication 9 March 2026
Published 29 March 2026 Volume 2026:21 580239
DOI https://doi.org/10.2147/COPD.S580239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Hajed M Al-Otaibi,1,2 Mazen M Homoud,1,2 Manal M Alqarni,3 Ghadeer J Alsobhi,4 Ghala Zaam Al-Otaibi,2 Nehal A Alnahdi5
1Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia; 2Respiratory Therapy Unit, King Abdulaziz University Hospital, King Abdulaziz University, Jeddah, Saudi Arabia; 3Department of Respiratory Therapy, King Abdullah Specialized Children’s Hospital, Jeddah, Saudi Arabia; 4Department of Respiratory Therapy, Prince Mohammed Bin Abdulaziz Hospital, National Guard Health Affairs, Madinah, Saudi Arabia; 5Department of Respiratory Therapy, Dr. Erfan & Bagedo General Hospital, Jeddah, Saudi Arabia
Correspondence: Hajed M Al-Otaibi, Department of Respiratory Therapy, Faculty of Medical Rehabilitation Sciences, King Abdulaziz University, Jeddah, Saudi Arabia, Tel +00966599914319, Email [email protected]
Background: Smoking is considered the primary cause of chronic obstructive pulmonary disease (COPD). It has been shown that approximately half of smokers develop COPD at some point in their lives. Several studies have examined COPD awareness in the general population. However, data on awareness among active smokers remain limited. This study aims to assess the level of COPD awareness among current smokers.
Methods: A cross-sectional study was conducted among active smokers. Recruitment was performed via non-probability convenience sampling through commonly used social media platforms. An online survey was utilized to collect data on sociodemographic characteristics, health status, COPD awareness levels, and smokers’ perceptions after learning about COPD. Multivariable logistic regression was performed to identify determinants of COPD awareness.
Results: The total number of respondents was 455 active smokers. Of those, 342 (75%) were male. The mean age of participants was 35 ± 11 years. Although COPD-related symptoms were reported by 324 participants (71.2% of the total sample), only 91 participants (20%) indicated being aware of COPD. The most common symptoms reported were sputum production (209 participants, 46%), shortness of breath (167 participants, 36.7%), and cough (166 participants, 36.4%). Multivariable logistic regression analysis for determinants of COPD awareness showed that none of the predictors (sex, years of smoking, level of education, and COPD-related symptoms) were statistically significant. Among COPD-related symptoms, coughing (adjusted odds ratio (aOR) = 0.62, 95% confidence interval (CI): 0.35– 1.08, p = 0.089) and sputum production (aOR = 1.48, 95% CI: 0.86– 2.55, p = 0.160) showed trends toward association with COPD awareness but were still not statistically significant. The most common sources of knowledge about COPD were healthcare providers (34%) and social media platforms (31.8%).
Conclusion: The level of COPD awareness is low among active smokers, which might hinder early diagnosis and delay timely interventions. Healthcare providers and social media may promote awareness. Therefore, the advocacy role of healthcare providers may need encouragement, and Social media platforms may support culturally tailored COPD awareness campaigns.
Keywords: chronic obstructive pulmonary disease, smoking, awareness, social media, COPD
Introduction
Tobacco smoking is recognized as one of the leading causes of preventable diseases and premature death across the world. Based on 2019 data, more than 1 billion people worldwide are active smokers. While tobacco use prevalence differs between countries, it exceeds 20% among males in over 150 countries and among females in 42 countries. Tobacco consumption results in more than 8 million deaths each year.1
Almost four out of five active smokers reside in low- and middle-income nations.2 The most widely used tobacco product is cigarettes, but other forms of tobacco like cigars, shisha, and electronic cigarettes are also used. Smoking is widely known to have adverse effects on health and contributes to cardiovascular diseases, metabolic disorders, and various forms of cancers.2 Moreover, smoking has a significant economic impact and results in over 1 trillion US dollars in annual healthcare costs and productivity losses worldwide.2
Chronic respiratory diseases are a major burden on global health systems and quality of life, and the annual mortalities exceed 4 million deaths globally.3 The most common chronic respiratory diseases are chronic obstructive pulmonary disease (COPD) and asthma. COPD is one of the most prevalent and severe smoking-related respiratory diseases. It is the leading cause of death from chronic respiratory diseases.3 The Global Initiative for Chronic Obstructive Lung Disease (GOLD) reported that COPD affects over 390 million people globally and is the third greatest cause of death, accounting for over 3.2 million deaths each year.4 More recent data showed that the prevalence of COPD was estimated to be 580 million, and this number is projected to rise to 592 million by 2050.5
Tobacco smoking is the leading cause of COPD,6 and the relationship between tobacco smoking and COPD was confirmed more than 30 years ago.7 This relation resembles the relationship between tobacco smoking and cancers.7 Smoking was reported to be the leading cause of deaths related to COPD.8 Recent studies show that the mortality risk is higher for current and former smokers in the COPD population.9 Furthermore, it has been shown that COPD causes a significant reduction in life expectancy among current smokers.10 Smoking cessation and increased public awareness are key strategies for reducing the burden of COPD.11
Several studies have investigated the awareness of the general population about COPD. An early Chinese study investigated COPD awareness among individuals aged 40 years and above. The authors reported an awareness rate of 9%, while only 5% had knowledge related to COPD among more than 75,000 people surveyed.12 An editorial from Portugal published in 2024 reported that only 32% of the surveyed sample (n = 1,500) had heard of or were aware of COPD.13 In Syria, the reported COPD awareness rate was 25% among participants who were not healthcare providers. There were no significant differences in awareness based on age group, gender, or geographic locations.14 Data from Africa indicated low COPD awareness among smokers, with major knowledge gaps regarding its causes, risk factors, prevention, and treatability. Community tailored awareness campaigns and improved facility based COPD education were recommended.15 Similarly, evidence from Japan demonstrated persistent gaps in COPD related knowledge among adult active smokers.16 In Saudi Arabia, a low awareness rate of COPD has also been reported. A recent study investigating the awareness rate among the general population found that 77% of the surveyed sample (n = 15,002) were unaware of COPD. A sub-analysis of smokers showed a similar level of unawareness.17
Low levels of COPD awareness among smokers may have several important consequences. First, it may be associated with delayed diagnosis and limited opportunities for early intervention. It may also reduce smokers’ motivation to engage in smoking cessation programs, as their perceived vulnerability to COPD may be low. Overall, these consequences may contribute to increased COPD related morbidity and greater healthcare utilization.
The majority of studies have investigated COPD awareness rates among the general population, but data on awareness among active smokers is limited. In most studies, COPD awareness among active smokers was assessed as a subgroup analysis rather than as a primary outcome. Therefore, the present investigation examined the awareness and perception of COPD among active smokers.
Materials and Methods
A cross-sectional study design was employed using a questionnaire developed from items previously published in similar research with modification and subsequent translation into Arabic. To ensure translation accuracy, the questionnaire was reviewed and modified by bilingual Arabic and English speakers. The modifications was intended to ensure clarity of the questionnaire statements by correcting grammatical and vocabulary issues that could potentially mislead participants or affect their interpretation of the items, while also ensuring cultural appropriateness and contextual relevance to the target population. Accordingly, this modification and review process supported the content validity of the questionnaire by ensuring clarity, relevance, and cultural appropriateness of the survey items. Following this, a pilot test was conducted with 10 participants, who reported that the questions were clear and straightforward, and no modifications to the content were required. The questionnaire was then sent electronically and distributed through social media platforms via WhatsApp, Snapchat, Twitter, Telegram, etc., to invite eligible individuals to participate; eligible participants were current (active) smokers aged ≥18 years. Individuals who did not meet the inclusion criteria (ie., non-smokers, ex-smokers, users of smokeless tobacco, or individuals aged <18 years) were excluded from the study. Participant recruitment followed a non-probability sampling approach, primarily convenience sampling. A snowball recruitment was encouraged by asking and encouraging participants to share the survey link within their social networks. Participants’ responses were screened, prior to analysis, to identify and remove duplicate entries, and incomplete questionnaires were excluded. This process was implemented to minimize potential bias and to ensure the accuracy and reliability of the survey outcomes.
Data Collection Tool
A structured questionnaire with multiple sections was utilized to conduct the survey. In addition to collecting participants’ demographics and smoking history, the questionnaire covered current health status, COPD-related symptoms, and participants’ level of awareness and perception of COPD. The first section addressed current health status and COPD-related symptoms. The second section focused on whether participants had a confirmed diagnosis of COPD or were undergoing treatment for the disease. The third section assessed public awareness of smoking-related respiratory disorders, while the fourth explored attitudes toward COPD.
Demographic Characteristics
Participants provided demographic information such as gender, age, weight, and height to capture fundamental physiological characteristics. Smoking history was documented to evaluate exposure risk. Educational level was recorded to examine its relationship with COPD awareness.
Current Health Status and Symptoms
Participants were asked about the presence of common lifestyle-related chronic conditions, including various cardiopulmonary diseases, hypertension, and diabetes mellitus. They also reported COPD-related symptoms using the Modified Medical Research Council questionnaire, which covers cough, sputum production, dyspnea, wheezing, and chest-pain episodes. Additionally, participants indicated whether they had ever been diagnosed with COPD.
Awareness of COPD and Changes in Attitudes
Awareness of COPD was evaluated in relation to participants’ knowledge of COPD symptoms, their educational level, and their sources of information. Participants were also asked to express their willingness to quit smoking after being made aware that smoking is the primary cause of COPD. This question aimed to evaluate how knowledge of the direct link between smoking and COPD might influence participants’ motivation to change their smoking behavior and adopt healthier lifestyle choices.
Statistical Analysis
Descriptive statistics, including frequencies, percentages, means, and standard deviations (SDs), were used to summarize the data. Categorical variables were summarized as frequencies and percentages. Comparisons between participants who were aware of COPD and those who were unaware were performed. Age was compared between groups using an independent samples t-test. Categorical variables, including sex, education level, and respiratory symptoms (cough, sputum production, dyspnea, wheezing and chest pain), were analyzed using Chi-square test of independence or Fisher’s exact test when appropriate. Years of smoking were compared using the Mann–Whitney U-test due to non-normal distribution. Spearman’s rank correlation coefficient test was performed to assess the presence of any significant relationship between variables. Multivariable logistic regression analysis was performed to identify determinants of COPD awareness among participants. The independent variables included sex, years of smoking, educational level, and the presence of COPD-related symptoms (cough, sputum production, dyspnea, wheezing, and chest pain). Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported and a p-value of ≤ 0.05 was considered indicative of statistical significance. The data were analyzed using the Statistical Package for the Social Sciences for Windows version 27.0 (Chicago, IL, USA).
Ethical Approval
The study received ethical approval from the King Abdulaziz University Hospital (KAUH) Ethics Committee ((Approval No. 115–22) Non-Intervention (Cross sectional)). The study followed the principles of the Declaration of Helsinki. Participants reviewed the form and provided electronic informed consent prior to starting the survey.
Results
A total of 455 respondents completed the online questionnaire. Of those, 342 (75%) were male. The mean age of participants was 35 ± 11 years. The average height and weight were 167 ± 19 cm and 76 ± 18 kg, respectively. The educational levels of participants varied across the sample. The majority held a bachelor’s degree (n = 301; 66.2%), followed by a high school certificate (n = 97; 21.3%). A smaller proportion of respondents possessed postgraduate qualifications (n = 38; 8.4%).
Only 91 out of 455 participants (20% of the sample) reported being aware of COPD. There were no statistically significant differences between participants who were aware of COPD and those who were unaware with respect to age, sex, educational level, or years of smoking (all p > 0.05).
Participants reported experiencing symptoms commonly associated with COPD. The most frequently reported symptom was sputum production, which was noted by 209 (46%) participants. In contrast, wheezing was the least commonly reported symptom and was identified by 120 (26.4%) participants. There were no statistically significant differences between participants who were aware of COPD and those who were unaware with respect to reported respiratory symptoms, including cough, sputum production, dyspnea, wheezes, and chest pain (all p > 0.05). Notably, only 3 participants (0.6%) reported a confirmed medical diagnosis of COPD. Table 1 presents COPD-related symptoms and comorbidities among the participants.
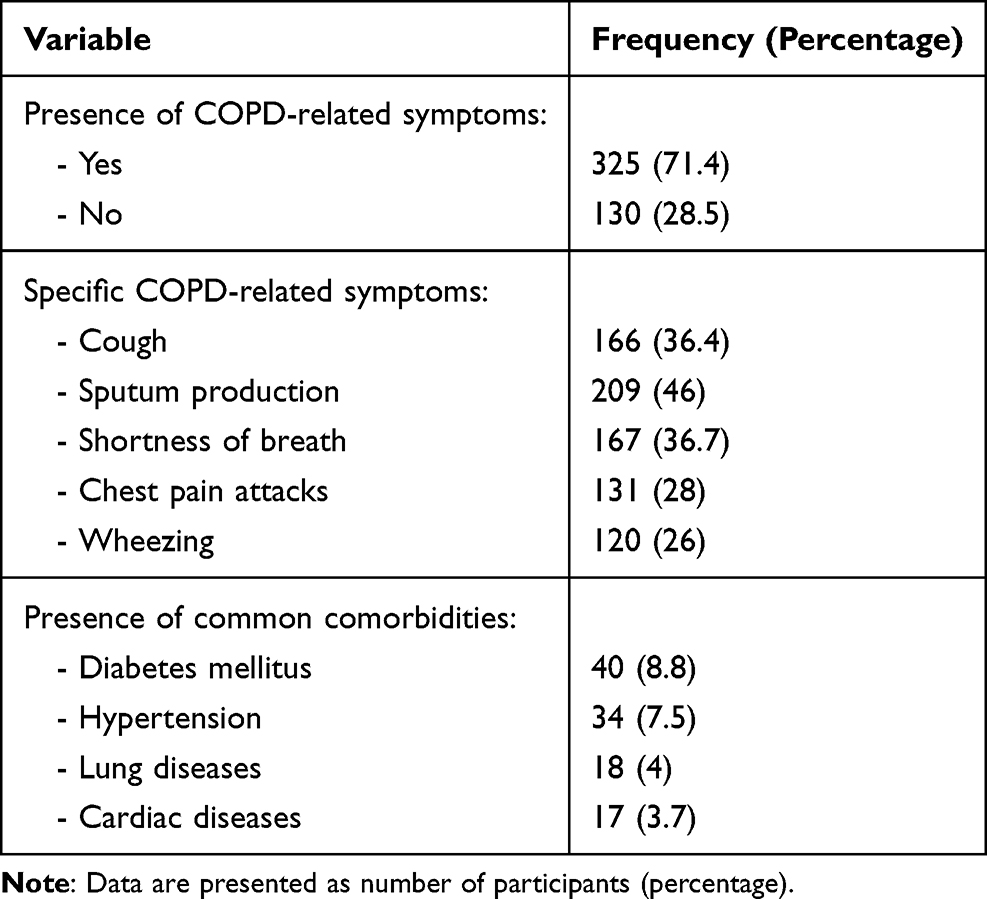 |
Table 1 COPD-Related Symptoms and Comorbidity |
Among all respondents, 431 (94.7%) participants reported having smoked tobacco for at least one year. Participants had a mean smoking duration of 13.8 ± 11.1 years. The majority of participants (n = 320; 70%) reported smoking conventional cigarettes, 150 participants (33%) reported smoking hookah, and 108 (23.7%) participants smoked more than one form of tobacco. In terms of tobacco consumption patterns, the majority of conventional cigarette smokers (44%) reported smoking between 1 and 10 cigarettes per day. Among smokers of alternative tobacco products, 56.9% of participants who reported electronic cigarette use, and 85.3% of hookah smokers indicated usage frequency of less than twice daily. Table 2 presents the type and history of tobacco use.
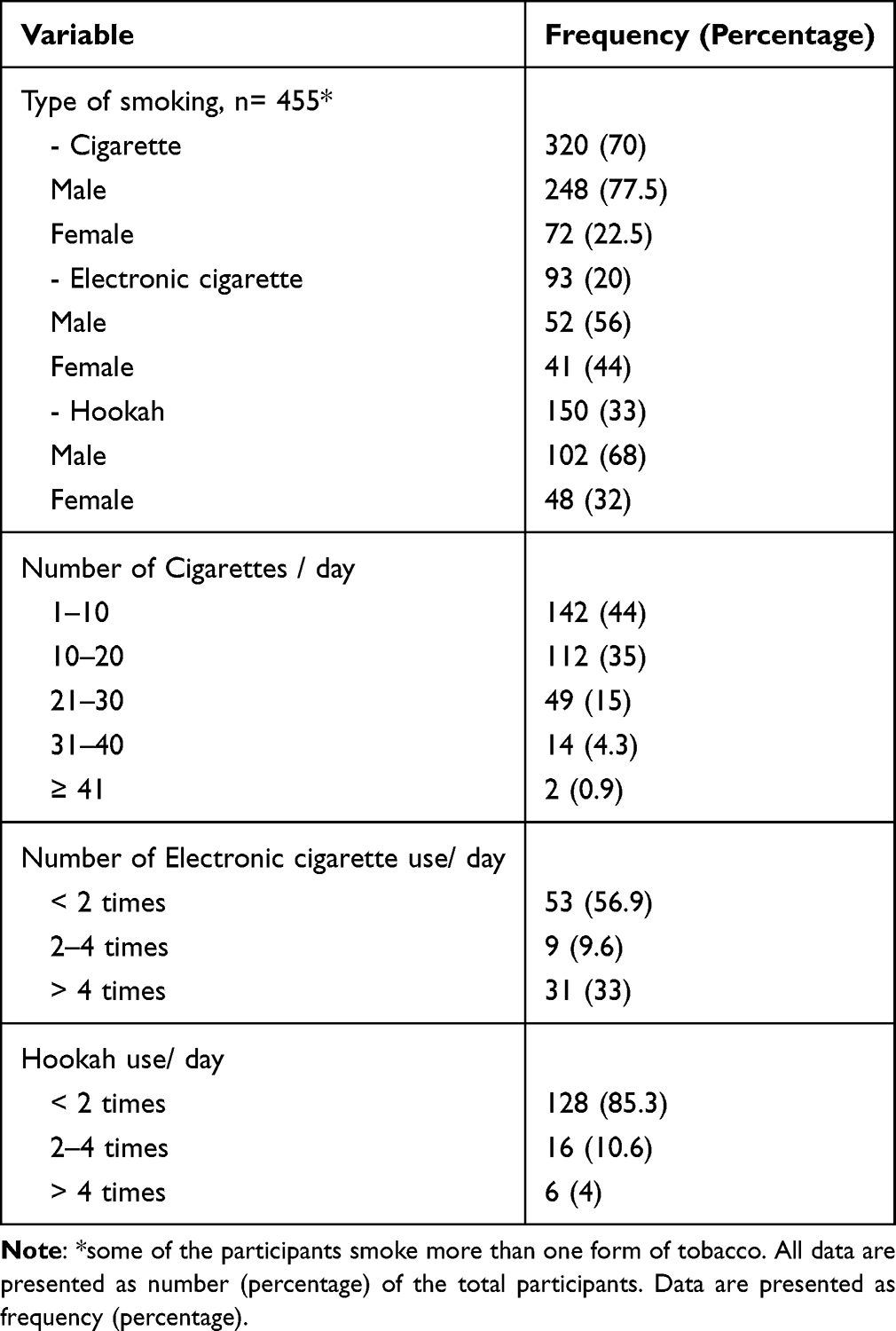 |
Table 2 Type and History of Tobacco Use |
The awareness rate among participants who experienced COPD related symptoms was evaluated, in addition to their level of education and source of information. The current data show that awareness of COPD among participants experiencing COPD-related symptoms ranged from 38% to nearly 46%. Awareness was highest for those with chest pain (45.8%) and lowest for those with sputum production (38%).
Spearman’s ranking correlation coefficient test showed no significant relationship between the number of symptoms and COPD awareness (p=0.928). The raw data indicate that educational level had little impact on COPD awareness, with no more than 30% of participants across all education levels reporting awareness of COPD. Spearman’s ranking correlation analysis showed that the correlation between the educational level and awareness of COPD was weak (R2 = 0.019) and not statistically significant (p=0.693). The primary sources of information about COPD were healthcare providers (34%) and social media (32%). Table 3 presents the number of participants who reported being aware of COPD, stratified by symptoms, educational level, and sources of information.
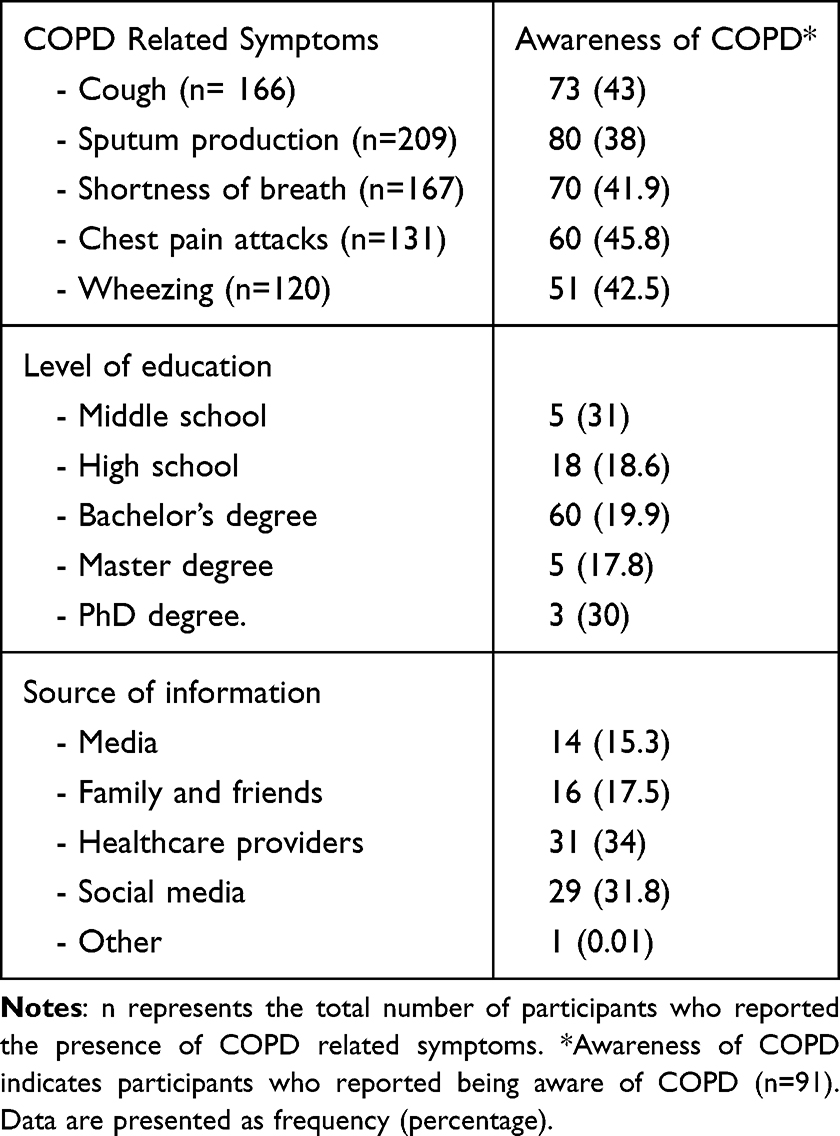 |
Table 3 COPD Awareness Categorized by Symptoms, Education, and Information Sources, N= 325 |
Multivariable logistic regression analysis for determinants of COPD awareness showed that none of the predictors (sex, years of smoking, level of education, and COPD-related symptoms) were significantly associated with COPD awareness. The logistic regression analysis showed that sex (male vs. female) was not a significant predictor (adjusted odds ratio (aOR) = 0.99, 95% confidence interval (CI): 0.50–1.95, p = 0.965). Years of smoking (aOR = 0.99, 95% CI: 0.97–1.02, p = 0.646) and level of education (aOR = 1.10, 95% CI: 0.79–1.55, p = 0.571) were statistically insignificant predictors of COPD awareness. Among COPD-related symptoms, cough (aOR = 0.62, 95% CI: 0.35–1.08, p = 0.089) and sputum production (aOR = 1.48, 95% CI: 0.86–2.55, p = 0.160) showed trends toward association with COPD awareness but were still not statistically significant. Dyspnea, wheezes, and chest pain were also not significant (aOR =1.19, 95% CI: 0.68–2.10, p=0.537; aOR =0.99, 95% CI: 0.54–1.83, p= 0.983; aOR =0.80, 95% CI: 0.45–1.41, p= 0.438, respectively).
The majority of participants who indicated awareness of COPD-related symptoms reported having either very poor or poor knowledge. Nearly half of the respondents rated their awareness of all COPD-related symptoms as very poor or poor. Table 4 represents the level of awareness based on the COPD-related symptoms.
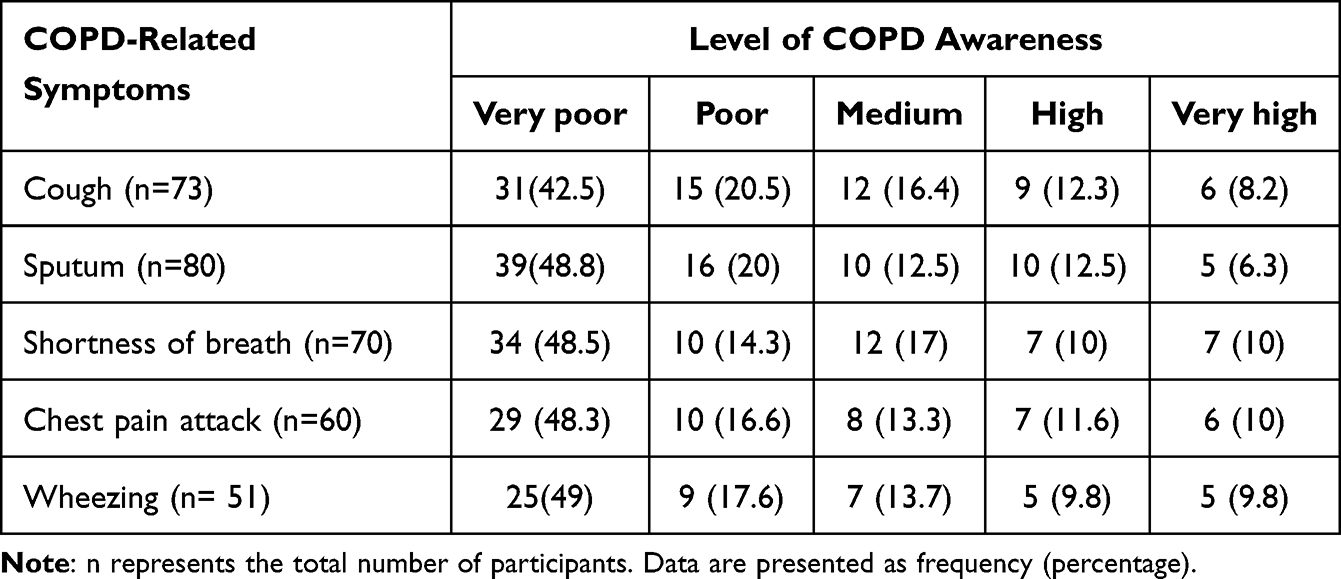 |
Table 4 Level of COPD Awareness According to COPD-Related Symptoms |
After learning that smoking is the primary cause of COPD, 332 (72.9%) participants showed willingness to quit smoking. Participants were stratified according to their COPD-related symptoms and age in order to evaluate their willingness to cease smoking. A majority of participants expressed willingness to quit smoking. However, Spearman’s ranking correlation coefficient test showed a weak positive relationship between the number of symptoms and willingness to quit smoking but with a negligible effect size (R2 = 0.041), and it was statistically insignificant (p=0.395). Table 5 presents the participants’ willingness to quit smoking in relation to their COPD-related symptoms and age groups.
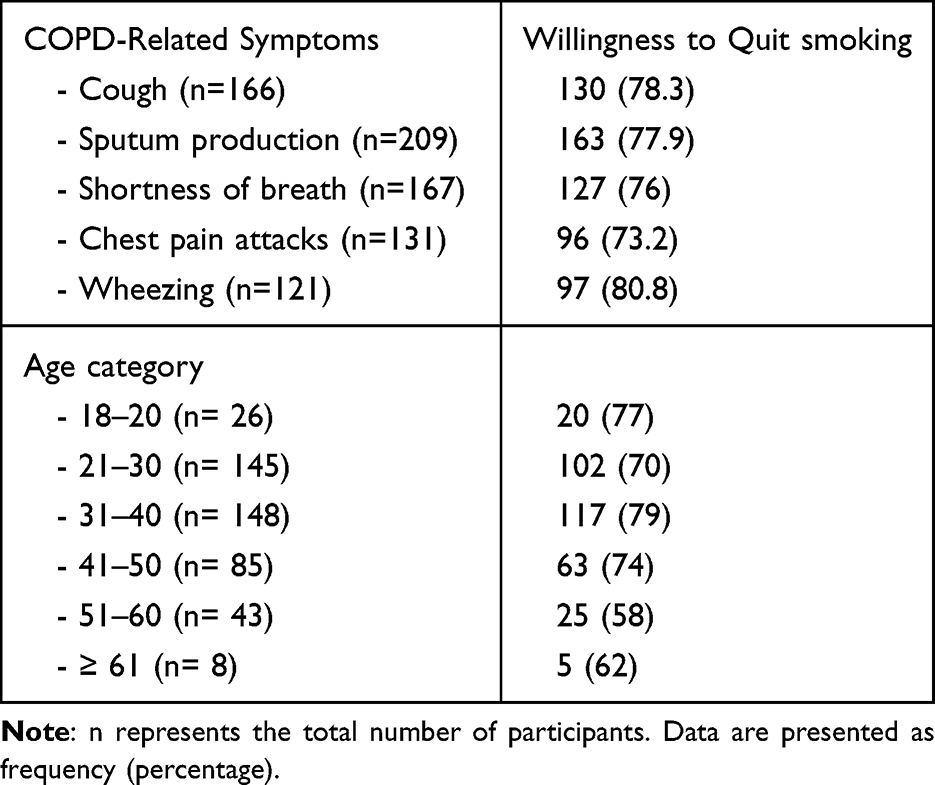 |
Table 5 Willingness to Quit Smoking by COPD Symptoms and Age Category, N= 455 |
Discussion
The present data show that two-thirds of the active smokers experienced one or more of the symptoms commonly associated with COPD, but only 20% of the participants were aware of COPD. The majority of participants who reported awareness of COPD described their awareness level as very poor or poor. The awareness rate of COPD was similar across all educational levels. The most common sources of information were healthcare providers and social media. More importantly, the majority of participants expressed willingness to quit smoking tobacco after learning that it is the primary cause of COPD, and the trend was observed across all age groups.
Moreover, multivariable analysis did not identify any independent predictors significantly associated with COPD awareness among active smokers. The lack of statistically significant independent predictors in the multivariable regression model may be attributed to several factors. It may reflect the multifactorial nature of COPD awareness among smokers, which is influenced by smokers’ characteristics, health literacy, and access to reliable sources of health information. It also may be due to modest effect sizes, limited variability in the level of awareness among participants, and probably unmeasured confounding factors.
Recently published data from Iraq indicated that participants demonstrated a high level of knowledge about COPD. A large proportion of the participants (1,033) correctly answered questions designed to assess their knowledge about COPD.18 Similarly, data from Slovenia showed that nearly half of participants were familiar with COPD.19 In contrast, data from Syria showed that only 25% of non-healthcare-provider participants were aware of COPD.14
A regional study from Saudi Arabia showed that the majority of participants (72%) never heard about COPD.20 Moreover, a large-scale study involving 15,002 participants aimed at evaluating the knowledge of the general population in Saudi Arabia reported that the majority of participants were not aware of COPD.17 Both studies from Saudi Arabia aimed to evaluate awareness among the general population. The current study aimed to evaluate the level of awareness among active smokers and found that only 20% were aware of COPD. Similarly, Almuzaini et al reported an awareness rate of 22% among smokers,20 while Alqahtani et al found that 73% of active smokers were unaware of the disease.17 All three studies consistently indicate that awareness of COPD among active smokers remains low. The consistent findings across these studies highlight a persistent knowledge gap among active smokers, which may reduce opportunities for disease screening, delay diagnosis and enrollment in smoking-cessation programs.
Studies have shown that smokers are significantly more likely to experience respiratory-related symptoms compared to non-smokers.21 Although there is evidence suggesting that smokers recognize COPD-related symptoms better than non-smokers, their overall knowledge remains limited.22 The present data show that majority of smokers experienced one or more symptoms related to COPD. Similarly, data presented by Alqahtani et al showed that almost one third of their participants complained of at least one respiratory related symptoms (smokers and ex-smokers constituted 15% of their sample).17 This might imply that active smokers are unable to assess or recognize their symptoms. Overall, our participants demonstrated an unsatisfactory level of awareness regarding COPD-related symptoms, and even among those who reported being aware of COPD, most rated their level of awareness as poor or very poor.
It is unsurprising that social media is the primary source of information for the majority of the population. Recent data from Spain showed that the majority of participants acquired knowledge about COPD through social media platforms, the internet, and other media sources.23 Similar findings were reported in Saudi Arabia, where online social platforms and other media were found to contribute significantly to COPD awareness.17 The present findings indicate that digital and traditional media are among the primary sources of health information for active smokers. These findings highlight the importance of utilizing modern media platforms to disseminate health information and shape public knowledge. Interactive and culturally appropriate media, combined with targeted messaging, have the potential to improve awareness and cognitive knowledge among smokers.
Evidence suggests that health campaigns delivered through social media platforms have the potential to increase public awareness, enhance engagement, and may positively influence health-related behaviors.24–26 This may be attributed to the broader reach and visibility of social media platforms. Higher levels of user interaction and engagement have the potential to further amplify message dissemination and increase influence. Thus, digital and traditional media appear to play major factors in promoting public awareness. Therefore, delivering COPD awareness campaigns through social media platforms may be more effective than traditional approaches, as it enables timely dissemination of up-to-date health information to a wider audience. A well-structured, objective-oriented health promotion campaign with clearly defined key performance indicators can be easily implemented through these platforms.
The perception that tobacco smoking poses few health risks may be one of the reasons people continue to smoke. Therefore, increasing awareness of the link between tobacco use and respiratory diseases could be a key factor in motivating smokers to quit. It has been reported that almost half of the smokers are unaware that smoking tobacco is a leading cause of COPD.17 Similarly, half of active smokers are unaware that smoking tobacco causes cardiovascular disease or stroke.24 These findings are supported by evidence indicating that active smokers tend to perceive tobacco use as being associated with fewer health risks compared to former smokers and individuals who have never smoked.24 The present data show that the majority of participants expressed a willingness to quit smoking once they became aware that it is the primary cause of COPD and learned more about the disease. A similar trend was observed even when the data were stratified by COPD-related symptoms or by age group. Thus, a lack of awareness or uncertainty regarding the harmful effects of tobacco use and its associated health risks may be one factor that reduces willingness to quit smoking. Lack of awareness may result in the absence of the fundamental motivation necessary to initiate smoking cessation. Therefore, promoting awareness among the general public, particularly current smokers, may help support intention to quit.
The present investigation is not without limitations. The survey has several inherent limitations, including recall bias, non-response bias, as well as cross-sectional design. Selection bias may have occurred due to the use of a non-probability sampling approach, particularly the convenience sampling plan. This may have led to underrepresentation of certain groups, particularly individuals who are less active on social media or those with limited interest in the topic. Recall bias may have led to reporting errors and misclassification of COPD-related symptoms. Therefore, the present study findings should be interpreted cautiously, particularly their generalizability. However, the anonymous nature of the survey, cultural adaptation of the questionnaire, and screening of raw data for duplicate and incomplete responses may have helped mitigate some of these limitations. Nevertheless, the current data shed light on the knowledge and perceptions of active smokers regarding COPD. This study may also serve as motivation for further qualitative and quantitative research to gain deeper understanding of the impact of awareness promotion on smoking prevalence. Future longitudinal studies are needed to evaluate trends in COPD awareness over time and to identify contributing factors that influence public awareness. Targeted interventional studies are also needed to evaluate the effectiveness of well-structured, objective-based smoking and COPD awareness campaigns among high-risk populations.
Conclusion
The present investigation demonstrates a low level of COPD awareness among active smokers, a trend observed across all educational levels. These findings have important clinical implications, as poor COPD awareness may delay early detection and negatively influence disease management and quality of life. More importantly, promoting awareness through social media platforms has the potential to encourage quitting, and this effect has been noted across all age categories. Therefore, well-structured and frequent awareness campaigns are highly recommended.
Data Sharing Statement
The data of the present study can be obtained from the corresponding author upon a justified request.
Author Contributions
All authors contributed substantially to the work reported, including the conception and design of the study, data acquisition, execution, analysis, and interpretation. All authors participated in drafting the manuscript or revising it critically for important intellectual content. Additionally, all authors approved the final version to be published, agreed on the target journal, and accept responsibility and accountability for all aspects of the work.
Funding
The APC was funded by the Deanship of Scientific Research (DSR) at King Abdulaziz University. The authors, therefore, acknowledge with thanks the technical and financial support.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. GBD. Tobacco collaborators. Spatial, temporal, and demographic patterns in prevalence of smoking tobacco use and attributable disease burden in 204 countries and territories, 1990-2019: a systematic analysis from the global burden of disease study 2019. Lancet. 2021 Jun 19;397(10292):2337-2360. Lancet. 2021;397(10292):2336. doi:10.1016/S0140-6736(21)01282-4
2. World Health Organization. Tobacco. World Health Organization; 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/tobacco.
3. GBD. Chronic respiratory diseases collaborators. global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the global burden of disease study 2019. EClinicalMedicine. 2023;59:101936.
4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2024 report). GOLD; 2024. Available from: https://goldcopd.org/2024-gold-report-2/.
5. Boers E, Barrett M, Su JG, et al. Global burden of chronic obstructive pulmonary disease through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
6. Lu W, Aarsand R, Schotte K, et al. Tobacco and COPD: presenting the world health organization (WHO) tobacco knowledge summary. Respir Res. 2024;25:338. doi:10.1186/s12931-024-02961-5
7. Doll R, Peto R, Wheatley K, et al. Mortality in relation to smoking: 40 years’ observations on male British doctors. BMJ. 1994;309(6959):901–10. doi:10.1136/bmj.309.6959.901
8. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
9. Adebile TV, Asifat OA, Dey S, et al. Effect of smoking on mortality in individuals with COPD in the United States. Respir Care. 2025;70(5):559–565. doi:10.1089/respcare.12264
10. Shavelle RM, Strauss DR, Kush P, et al. Life expectancy and years of life lost in chronic obstructive pulmonary disease: findings from the NHANES III follow-up study. Int J Chron Obstruct Pulmon Dis. 2009;4:137–148. doi:10.2147/copd.s5237
11. Zhu Y, Shen T, Guo R, et al. Global, regional, and national burden of young COPD, 1990–2021, with forecasts to 2050: a systematic analysis for the global burden of disease study 2021. BMC Public Health. 2025;25(1):276. doi:10.1186/s12889-025-21414-2
12. Fan J, Wang N, Fang LW, et al. [Awareness of knowledge about chronic obstructive pulmonary disease and related factors in residents aged 40 years and older in China, 2014. Zhonghua Liu Xing Bing Xue Za Zhi. 2018;39(5):586–592. doi:10.3760/cma.j.issn.0254-6450.2018.05.009
13. Oliveira AS, Cortesão N, Gomes J, et al. Unmasking the hidden threat: COPD awareness and knowledge in Portugal. Pulmonology. 2024;30(3):207–209. doi:10.1016/j.pulmoe.2023.11.005
14. Hadakie R, Kakaje A, Al Kwatly K, et al. COPD awareness among the Syrian community: population-based study. Sci Rep. 2023;13(1):5997. doi:10.1038/s41598-023-32612-6
15. A JA, Haiderbhai M, Mwalimu J, et al. Analysis of knowledge regarding chronic obstructive pulmonary disease (COPD) among male smokers in Rwamishenye Ward, Bukoba District, Kagera Region, Tanzania: a cross-sectional study. Cureus. 2025;17(12):e100369. doi:10.7759/cureus.100369
16. De Fatima De Oliveira Graca Y, Yang L, Mingyu C, et al. Smoking attitudes, self-reported practices, and COPD knowledge among adults aged 20-59 years: insights from a Japanese sample. Tob Induc Dis. 2025. doi:10.18332/tid/200855
17. Alqahtani JS, Aldhahir AM, Siraj RA, et al. A nationwide survey of public COPD knowledge and awareness in Saudi Arabia: a population-based survey of 15,000 adults. PLoS One. 2023;18(7):e0287565. doi:10.1371/journal.pone.0287565
18. Alsajri AH, Al-Qerem W, Jarab A, et al. Assessing knowledge and awareness of asthma and chronic obstructive pulmonary disease among the Iraqi population. Int J Chronic Obstr. 2025;20:1749–1760. doi:10.2147/COPD.S517612
19. Farkas J, Lainscak M. Assessment of public awareness on chronic obstructive pulmonary disease in Slovenia. Eur Respir J. 2014;44(Suppl 58).
20. Almuzaini AS, Algeffari M, Alsohaibani A, et al. Awareness of chronic obstructive pulmonary disease and its risk factors among the adult population of the Qassim Region, Saudi Arabia. Cureus. 2023;15(9):e44743. doi:10.7759/cureus.44743
21. Walabyeki J, Adamson J, Buckley HL, et al. Experience of, awareness of and help-seeking for potential cancer symptoms in smokers and non-smokers: a cross-sectional study. PLoS One. 2017;12(8):e0183647. doi:10.1371/journal.pone.0183647
22. Sikjær MG, Hilberg O, Fløe A, et al. Lack of awareness towards smoking-related health risks, symptoms related to COPD, and attitudinal factors concerning smoking: an Internet-based survey conducted in a random sample of the Danish general population. Eur Clin Respir J. 2018;5(1):1506235. doi:10.1080/20018525.2018.1506235
23. Rodríguez Hermosa JL, Miravitlles M, López-Campos JL, et al. Smoking and COPD knowledge in the general spanish population: a CONOCEPOC study. J Clin Med. 2023;12(13):4473. doi:10.3390/jcm12134473
24. He T, Liu L, Huang J, et al. Health knowledge about smoking, role of doctors, and self-perceived health: a cross-sectional study on smokers’ intentions to quit. Int J Environ Res Public Health. 2021;18(7):3629. doi:10.3390/ijerph18073629
25. Ghahramani A, de Courten M, Prokofieva M. The potential of social media in health promotion beyond creating awareness: an integrative review. BMC Public Health. 2022;22(1):2402. doi:10.1186/s12889-022-14885-0
26. Kite J, Chan L, MacKay K, et al. A model of social media effects in public health communication campaigns: systematic review. J Med Internet Res. 2023;25:e46345. doi:10.2196/46345
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Chronic Obstructive Pulmonary Disease Prevalence and Associated Risk Factors in Adults Aged 40 Years and Older in Southeast China: A Cross-Sectional Study During 2019–2020
Chen J, Yin Y, Zhang Y, Lin X, Chen T, Yang Z, Wang D, Zhong W
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2317-2328
Published Date: 17 September 2022
Hospital Burden of Chronic Obstructive Pulmonary Disease in Hong Kong – The Trend from 2006 to 2014
Chan HS, Ko FWS, Chan JWM, Choo KL, So LKY, Lam DCL, Sin KM, Wong WY, Cheng YL, Wong MML
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:507-519
Published Date: 6 April 2023
Prevalence of Chronic Obstructive Pulmonary Disease in England from 2000 to 2019
Stone PW, Osen M, Ellis A, Coaker R, Quint JK
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:1565-1574
Published Date: 21 July 2023
A Long-Term Study of Adverse Outcomes Associated With Oral Corticosteroid Use in COPD

Tse G, Emmanuel B, Ariti C, Bafadhel M, Papi A, Carter V, Zhou J, Skinner D, Xu X, Müllerová H, Price D
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2565-2580
Published Date: 15 November 2023
COPD in People with HIV: Epidemiology, Pathogenesis, Management, and Prevention Strategies
Byanova KL, Abelman R, North CM, Christenson SA, Huang L
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2795-2817
Published Date: 29 November 2023