Back to Journals » Biologics: Targets and Therapy » Volume 19
Beyond Monotherapy: Exploring the Efficacy and Safety of Dual Biologic Strategies in Rheumatic Diseases
Authors Hassan F ![]() , Jeries H, Daood R, Naffaa ME
, Jeries H, Daood R, Naffaa ME ![]()
Received 3 September 2025
Accepted for publication 21 October 2025
Published 8 November 2025 Volume 2025:19 Pages 665—680
DOI https://doi.org/10.2147/BTT.S565137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Fadi Hassan,1,2 Helana Jeries,1,2 Rula Daood,1,2 Mohammad E Naffaa1,2
1Rheumatology Unit, Galilee Medical Center, Naharyia, Israel; 2Azrieli Faculty of Medicine, Bar-Ilan University, Safed, Israel
Correspondence: Fadi Hassan, Rheumatology Unit, POB 21, Galilee Medical Center, Road 89, Naharyia, Israel, Tel +97249107038, Fax +97249107593, Email [email protected]
Abstract: Although numerous biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) are available, substantial number of rheumatic patients fail to achieve therapeutic goals with sequential monotherapy. Dual biologic therapy (DBT) may overcome treatment resistance by concomitantly inhibiting multiple inflammatory pathways. In rheumatoid arthritis, DBT shows moderate efficacy improvements but consistently higher serious infection rates compared to monotherapy, particularly with rituximab and JAK inhibitor combination-based regimens. In psoriatic arthritis, studies demonstrate possible benefits especially with combinations targeting alternate pathways, eg, apremilast with biologics or IL-17/IL-23 inhibitors with TNF blockers, though safety concerns exist. The multi-domain nature of PsA makes DBT particularly attractive in achieving global disease control. In axSpA, evidence of efficacy is also limited but encouraging in treatment-refractory disease. However, major research gaps persist. Data remain limited and largely heterogeneous, with limited disease-specific studies and a paucity of randomized controlled trials (RCTs). Most available reports derive from small case series or single-center experiences, limiting the generalizability of findings. Geographic variation further complicates interpretation, as infection risk, treatment accessibility, and pharmacovigilance capacity differ markedly between developed and resource-limited regions. Therefore, this narrative review aims to summarize current evidence while emphasizing the unmet clinical and research needs surrounding DBT, highlighting the necessity for systematic reviews, large-scale registries, and context-specific studies to inform safe and equitable clinical application worldwide. While DBT may be beneficial in carefully selected patients with treatment-refractory disease, current evidence does not consistently demonstrate increased efficacy. Thus, DBT should be reserved for refractory cases where benefits outweigh risks.
Keywords: dual biologic therapy, rheumatoid arthritis, psoriatic arthritis, axial spondyloarthritis, treatment resistance, refractory disease, biologics
Introduction
The introduction of biologic and targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs) has revolutionized the management of immune-mediated inflammatory diseases (IMIDs).1 In clinical practice, b/tsDMARDs are typically used as monotherapies or in combination with conventional synthetic DMARDs (csDMARDs). When a b/tsDMARD fails to achieve the therapeutic goal, switching to another b/tsDMARD, usually with a different mechanism, is the standard approach.2,3 Current treatment guidelines from major rheumatology societies, including the European Alliance of Associations for Rheumatology (EULAR) and the American College of Rheumatology (ACR), consistently endorse a sequential treatment strategy using a single biologic agent (often in combination with a csDMARD), and do not recommend dual biologic therapy (DBT). These guidelines emphasize switching between biologic classes rather than combining them, reflecting the limited evidence base and persisting safety concerns associated with DBT. Consequently, the concomitant use of two b/tsDMARDs has generally been avoided due to safety concerns. Nevertheless, despite the increasing number of available b/tsDMARDs, a substantial proportion of rheumatic patients fail to achieve the treatment goal, even when switching to other b/tsDMARDs with different mechanisms of action.4–8 This therapeutic resistance represents a substantial challenge in the daily clinical practice. One approach to overcome this challenge can be achieved using concomitant inhibition of multiple inflammatory pathways or cytokines by utilizing DBT. This strategy may improve clinical outcomes by providing deeper inhibiting of the inflammatory process.1,9 The concept of DBT has emerged over the past two decades as a promising approach in patients with difficult-to-treat disease. DBT has been also investigated beyond the field of rheumatology, particularly in resistant cases of osteoporosis, asthma, atopic dermatitis and inflammatory bowel disease (IBD).10 Although early experiences with DBT were limited due to safety concerns, growing knowledge of cytokine pathways and careful patient selection have renewed interest in this strategy, particularly given the substantial number of patients failing to achieve treatment goals using standard sequential approach.9
This review summarizes current evidence on DBT in rheumatic diseases, focusing on efficacy and safety. We outline mechanisms of treatment resistance that limit the effectiveness of sequential biologic monotherapy, and present the rationale for DBT as a means to target overlapping or complementary inflammatory pathways. Clinical evidence is reviewed with emphasis on rheumatoid arthritis (RA), psoriatic arthritis (PsA), and axial spondyloarthropathy (axSpA), followed by a discussion of strategies beyond DBT for difficult-to-treat disease.
Resistance Mechanisms to Biologics Monotherapy
Multiple mechanisms have been proposed to explain this therapeutic failure of sequential b/tsDMARD monotherapy approach, including immunological and genetic factors, as well as patient-related non-immunological factors. A key mechanism involves the formation of anti-drug antibodies (ADAs), particularly in response to immunogenic monoclonal antibody-based agents such as infliximab and adalimumab. These ADAs can either neutralize the drug directly or enhance its clearance from circulation, resulting, in both cases, in subtherapeutic drug levels and reduced efficacy.11 This mechanism is further supported by the finding that methotrexate co-administration decreases immunogenicity and enhances the drug survival of biologic agents, emphasizing the important role of combining a csDMARD with a b/tsDMARD.12
The various cytokine pathways and the connections between them constitute another key mechanism underlying resistance to b/tsDMARD therapy. The inflammatory milieu in rheumatic diseases is composed of a vast network of overlapping and, often, compensatory signaling cascades. Consequently, targeting single cytokine, such as TNF, may be inadequate for achieving disease control in patients with complex immune activation, as TNF represents only one downstream cytokine within a broader inflammatory framework.13 Notably, alternative mediators such as IL-6 and granulocyte-macrophage colony-stimulating factor (GM-CSF) have been identified as compensatory pathways contributing to therapeutic failure in TNF inhibitor non-responders.14
At the cellular level, immune dysregulation, affecting effector T cell subsets, regulatory T cells (Tregs), and myeloid compartments, can limit b/tsDMARD efficacy. Resistance is linked to persistent Th17 polarization and impaired Treg function despite targeted cytokine blockade.15 Pharmacogenomic and transcriptomic data reveal molecular heterogeneity, with interferon-regulated gene signatures predicting poor TNF inhibitor response and supporting alternative targets.16 Additionally, polymorphisms in cytokine genes, receptor loci, and Fcγ receptors (eg, FCGR3A) may influence efficacy and immunogenicity, informing precision medicine approaches.17
Finally, non-immunological factors may also play an important role in resistance. Factors such as poor medication adherence, obesity, and altered pharmacokinetics can substantially modulate treatment outcomes. Notably, increased body mass index has been associated with lower serum drug levels and reduced therapeutic response, particularly with fixed-dose biologic regimens.18
Unmet Needs and Rationale for Combining Biologics
Mechanistic and clinical evidence support DBT by showing the redundancy and interplay of cytokine networks in rheumatic diseases. Preclinical studies indicate that dual blockade of distinct pathways may yield additive or synergistic immunomodulatory effects, potentially overcoming monotherapy limitations. In a Lewis rat adjuvant arthritis model, Feige et al showed that combining an interleukin-1 receptor antagonist (IL-1Ra) with polyethylene glycol–conjugated soluble TNF receptor type I (PEG sTNF-RI) produced significantly greater reductions in inflammation, weight loss, bone erosion, and histopathologic damage than either monotherapy.19 Isobologram analysis confirmed true pharmacological synergy, suggesting that lower doses of each agent could be used without loss of efficacy. Dillon et al evaluated acazicolcept (ALPN-101), a dual CD28/ Inducible T Cell Costimulator (ICOS) antagonist, in a collagen-induced arthritis model.20 Unlike constitutively expressed CD28, ICOS is rapidly upregulated after T cell activation and drives Th1, Th2, and Th17 responses. By blocking two non-redundant costimulatory pathways, acazicolcept achieved greater suppression of joint inflammation, cytokine production, and disease severity than abatacept or ICOS monotherapy. Another experimental study investigated the combination of etanercept with a Transient Receptor Potential Vanilloid 2 (TRPV2) agonist in preclinical mice model of collagen-induced arthritis.21 TRPV2 is a non-selective cation channel expressed by fibroblast-like synoviocytes that suppresses their invasive properties by preventing Rac1 and RhoA activation. The dual treatment achieved sustained suppression of disease severity and more pronounced reduction in joint damage compared to either monotherapy. Moreover, the DBT group showed the most significant protection in histologic scores for synovial inflammation, hyperplasia, cartilage erosions, and bone erosions. Together, these preclinical studies provide a strong mechanistic rationale for combining biologic agents with complementary or synergistic immunologic targets in the treatment of immune-mediated inflammatory diseases.
Clinical experience shows that disease domains in PsA and axSpA often respond variably to different biologics, highlighting monotherapy limitations and supporting for DBT strategy. IL-17A inhibitors are effective for joint and skin disease but may exacerbate IBD, whereas vedolizumab, a gut-selective α4β7 integrin antagonist, controls IBD without systemic immunosuppression.22 Case reports and series describe vedolizumab combined with TNF inhibitors or IL-17 blockers in patients with coexisting SpA and IBD, achieving control of both articular and gastrointestinal inflammation without increased infection risk.22–25 Vedolizumab is the most frequently used gut-selective agent in DBT for IBD, often paired with other bDMARDs in refractory disease, with real-world data suggesting preserved or enhanced efficacy.22–24,26 Other selective agents, such as ustekinumab (IL-12/23 inhibitor), have also been safely combined with TNF inhibitors or vedolizumab in complex cases.25,26 Similarly, apremilast, a PDE4 inhibitor with minimal immunosuppressive effects, has emerged as an attractive candidate for DBT. Furthermore, IL-17 inhibitors themselves, despite their known pro-inflammatory risk in gut mucosa, have been used in DBT regimens with other biologics or targeted synthetic DMARDs (tsDMARDs), particularly in patients with severe, multi-domain PsA or PsA coexisting with atopic dermatitis or asthma.
In summary, these findings indicate that the thoughtful selection of biologics with complementary efficacy and safety profiles, particularly those with minimal systemic immunosuppression, may allow for personalized and effective DBT approaches in complex and difficult to treat immune-mediated diseases.
Rheumatoid Arthritis
Up to 30–40% of RA patients respond inadequately to sequential biologic monotherapy, and 15–20% remain persistently refractory.5 This unmet need has driven investigation of biologic combinations as a potential strategy to enhance efficacy (Table 1).
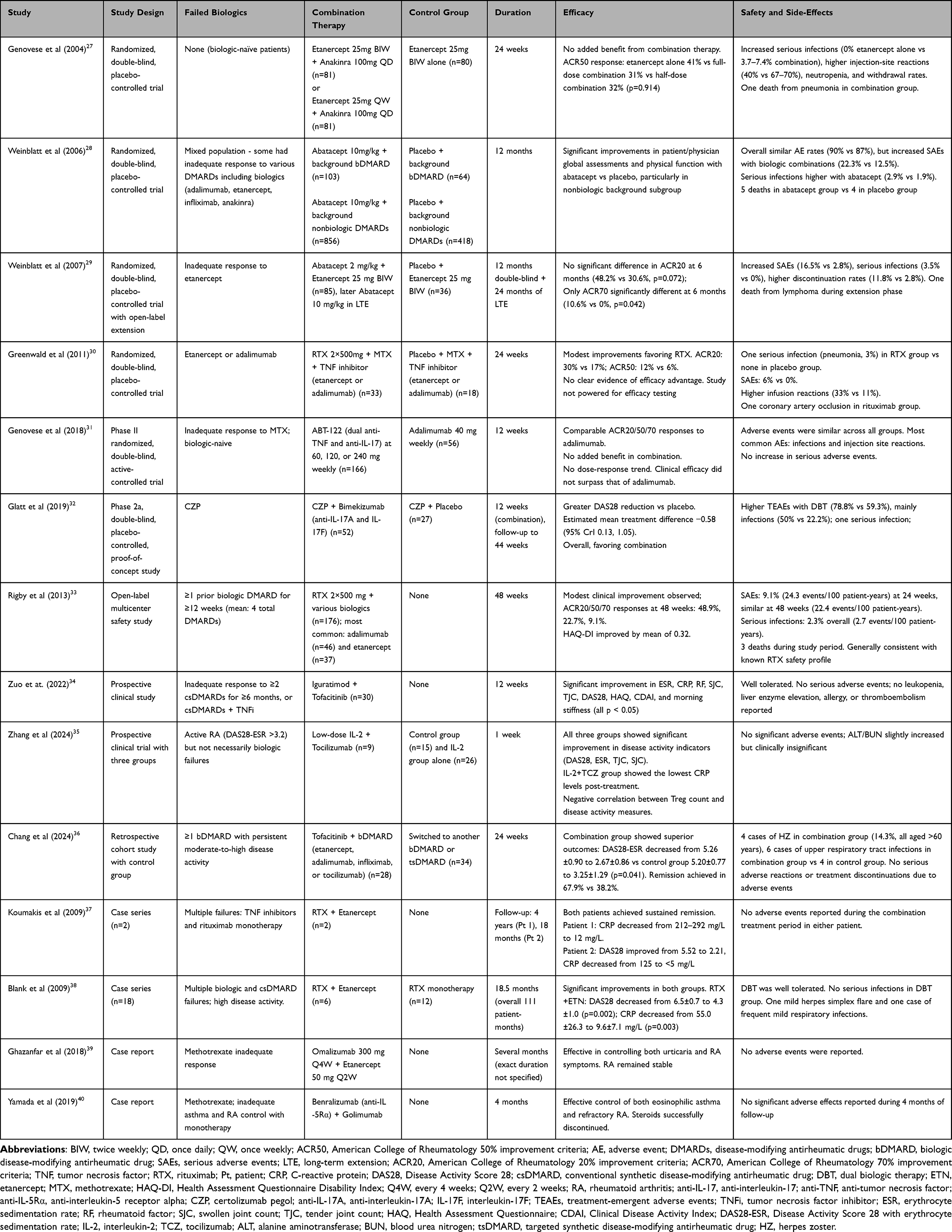 |
Table 1 Summary of Dual Biologic Therapy in Treatment-Refractory Rheumatoid Arthritis |
Early DBT trials in RA raised safety concerns. In 2004, Genovese et al combined etanercept with anakinra in methotrexate-refractory RA, finding modest efficacy gains but higher serious infection rates (3.7% with half-dose and 7.4% with full-dose DBT vs 0% with etanercept alone).27 In 2006, Weinblatt et al tested abatacept plus etanercept. Although ACR50/70 rates were numerically higher, differences were not significant, and serious infections (3.5% vs 0%) and serious adverse events (16.5% vs 2.8%) were more frequent with DBT.28
Despite these early concerns, interest in DBT continued. In a pivotal study, Cohen et al demonstrated the efficacy of rituximab (a B-cell depleting agent) in RA patients who had failed anti-TNF therapy.41 This study was followed by studies assessing the safety of rituximab in combination with other biologics. Greenwald et al reported on a cohort receiving rituximab in DBT regimen with TNF inhibitors.30 While no unexpected safety signals were observed within 24 hours of infusion, the DBT group experienced markedly higher rate of serious infections (8.5%) compared to TNF inhibitor–only group (1.5%), including one fatal case. The study was not powered to detect efficacy differences, and no significant improvement in ACR20/50/70 response rates was observed in the DBT group compared to TNF inhibitor monotherapy, further questioning the benefit of this strategy. Rigby et al extended these findings in an open-label study showing that rituximab (2 × 500mg) could be co-administered with a variety of other biologics across 18 different DBT regimens in a real-world cohort.33 Although the overall incidence of serious infections remained low at 2.7 events per 100 patient-years over 48 weeks of follow-up, only modest improvements in disease activity were reported, with ACR20 responses increasing from 30.7% at 24 weeks to 48.9% at 48 weeks. The absence of a control arm and the heterogeneous treatment regimens, ranging from rituximab plus adalimumab monotherapy to complex multi-DMARD combinations, limited the ability to draw any firm conclusions regarding added efficacy beyond that achievable with single biologic therapy.
In 2018, Genovese et al introduced novel approach to dual biologic therapy with ABT-122 molecule, a bispecific dual variable domain immunoglobulin targeting both TNF and IL-17A.31 The rationale for this dual targeting was based on preclinical evidence showing synergistic effects of TNF and IL-17A in osteoclastogenesis and bone destruction, and clinical observations that patients failing TNF inhibition often have elevated circulating Th17 cells and increased IL-17 levels. In this Phase II, randomized, double-blind study, 222 biologic-naive patients with active RA and inadequate response to methotrexate were assigned to ABT-122 at three dosing regimens (60 mg every other week, 120 mg every other week, or 120 mg every week) or adalimumab 40 mg every other week for 12 weeks. Despite the theoretical advantages of dual cytokine inhibition, ABT-122 demonstrated no meaningful clinical superiority over TNF inhibition monotherapy, with ACR20 response rates at week 12 of 62%, 75%, and 80% respectively across the ABT-122 dose groups versus 68% with adalimumab. The safety profile was comparable across all treatment groups, with treatment-emergent adverse events occurring in 37–42% of ABT-122 patients versus 43% with adalimumab, and no serious infections reported with ABT-122. Importantly, mechanistic analyses suggested that the anti-TNF component was the primary driver of ABT-122’s efficacy, supporting emerging evidence that IL-17A may not be a major contributor to RA pathophysiology, ultimately leading to discontinuation of ABT-122 development for RA treatment.
In 2018, a case report documented the successful combined use of omalizumab (anti-IgE monoclonal antibody) and etanercept in a patient with coexisting chronic spontaneous urticaria and RA.40 The patient, previously unresponsive to conventional therapy, achieved clinical remission of both conditions without significant adverse events. Although it is based on single case report, the observed improvement suggests that a DBT strategy may have therapeutic potential in selected patients with treatment-resistant disease.
In 2024, Chang et al published a retrospective study evaluating the DBT of tofacitinib (5 mg twice daily) with various bDMARDs in 28 RA patients with inadequate response to biologic monotherapy.36 The most commonly used biologics in DBT were adalimumab (11 patients) and etanercept (8 patients), followed by tocilizumab (6 patients) and infliximab (3 patients). At 24 weeks, 67.9% of patients achieved DAS28-ESR remission compared to 38.2% in the control group of 34 patients who utilized the sequential approach with switching to another single b/tsDMARD. The DBT group demonstrated significantly superior ACR20/50/70 response rates (85.71%, 75%, and 39.29% vs 75.0%, 53.57%, and 21.43%, respectively). Notably, four patients (14.3%) in the DBT group developed herpes zoster, three with adalimumab plus tofacitinib and one with tocilizumab plus tofacitinib, all occurring in patients over 60 years of age. All patients recovered with antiviral treatment without requiring treatment discontinuation. Despite the retrospective design and limited sample size, these results provide preliminary evidence supporting the potential efficacy of combining JAK inhibitors with bDMARDs in selected difficult-to-treat RA cases, though monitoring for infectious complications, particularly in elderly patients, is needed.
In conclusion, evidence for DBT in RA is inconsistent. Benefits in refractory cases are modest, while serious infection risk, particularly with full-dose combinations, is consistently higher. Its Therefore, DBT should be considered cautiously and reserved for selected patients.
Psoriatic Arthritis (PsA)
PsA is a heterogeneous inflammatory disease involving multiple domains including peripheral arthritis, axial disease, enthesitis, dactylitis, skin/nail psoriasis, and extra-articular features such as uveitis and IBD. Management is often difficult due to the diverse presentations and variable domain responses.6 Although b/tsDMARDs have improved outcomes, many patients remain uncontrolled despite monotherapy or sequential switching, especially those with concurrent multi-domain activity. This has driven interest in DBT to simultaneously target multiple pathogenic pathways in refractory PsA (see Table 2). Consequently, there is a growing interest in the use of DBT to target multiple pathogenic pathways simultaneously in refractory cases of PsA (see Table 2).
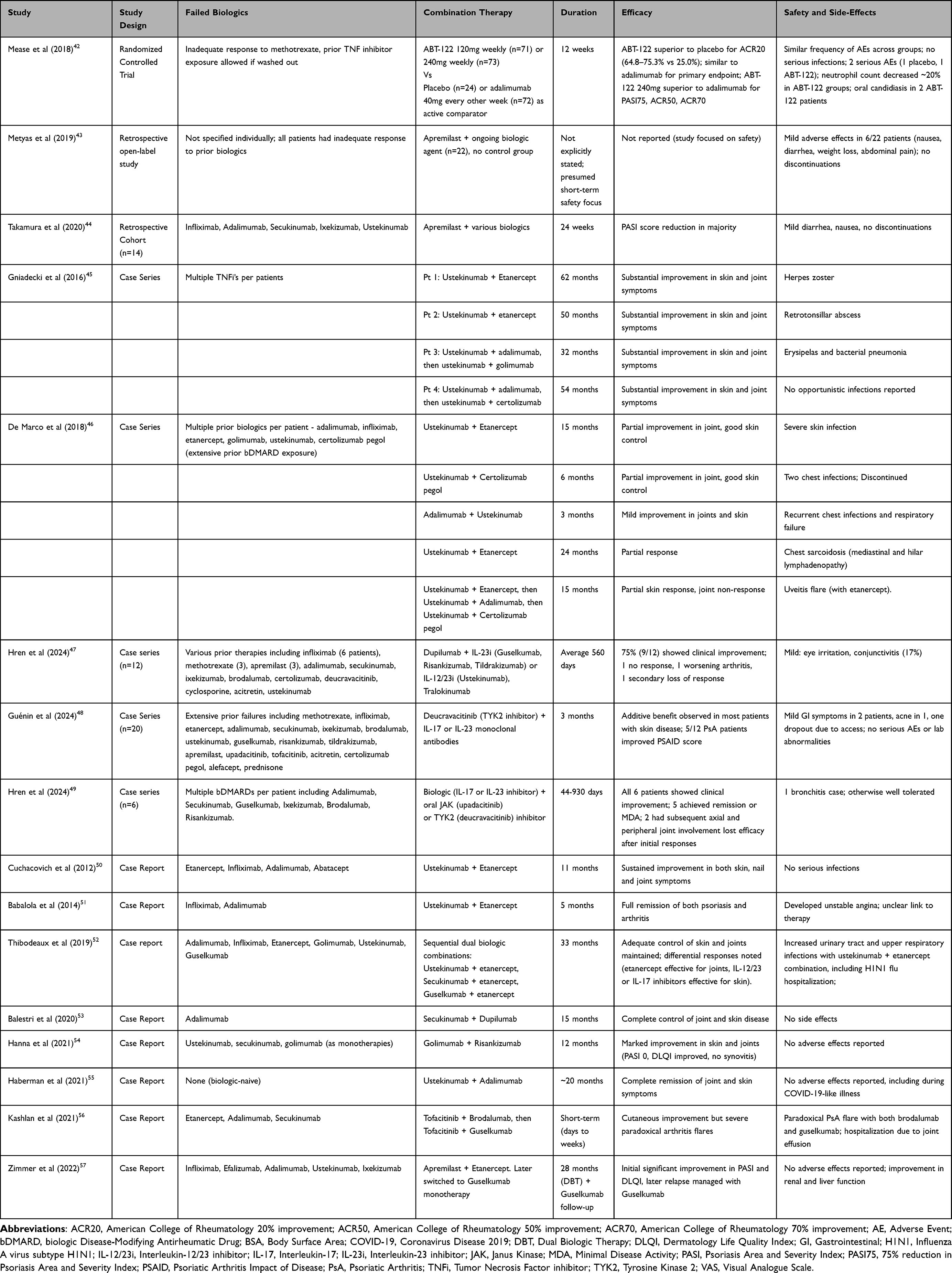 |
Table 2 Summary of Dual Biologic Therapy in Treatment-Refractory Psoriatic Arthritis |
Apremilast Regimens – Apremilast, an oral phosphodiesterase-4 (PDE4) inhibitor, has been suggested as a potential candidate in DBT approach. Owing to its minimal immunosuppressive effect, apremilast presents a compelling option for combination with other biologics, potentially enhancing efficacy without substantially increasing infection risk. A retrospective open-label study by Metyas et al evaluated 22 patients with plaque psoriasis and PsA who had inadequate response to ongoing biologic therapy and were subsequently given apremilast as an add-on treatment.43 The study reported that while 6 patients experienced mild adverse effects (nausea, diarrhea, weight loss, abdominal pain), none required treatment discontinuation. Importantly, no serious infections or significant safety concerns were observed, suggesting a favorable safety profile for the combination. In a second retrospective cohort study by Takamura et al, 14 patients with psoriasis (including three with PsA) who had experienced secondary loss of efficacy to their current biologic therapy were treated with apremilast in addition to their existing biologic agent (including TNF-α, IL-17, and IL-23 inhibitors).44 All patients had tried an average of 2.9 systemic medications before dual therapy. The study demonstrated a significant reduction in PASI score from 3.2±0.4 at baseline to 1.6±0.3 after 24 weeks of DBT. PASI-75 and PASI-50 response rates were achieved in 29% and 50% of patients, respectively. Side effects were generally mild, including diarrhea (4 patients), nausea (1 patient), and weight loss exceeding 5% of body weight (2 patients), with no treatment discontinuations due to adverse events. Notably, response rates were superior when apremilast was combined with TNF-α or IL-23 inhibitors compared to IL-17 inhibitors, suggesting differential efficacy based on the underlying biologic mechanism of action. Additionally, a case report by Zimmer et al described a 62-year-old man with PsA, diabetic nephropathy, and liver cirrhosis who had previously failed multiple biologics.57 Despite experiencing a relapse of joint symptoms while on etanercept monotherapy, the addition of apremilast led to significant improvement and long-term disease control. Over 28 months of DBT, the patient achieved stable remission of both cutaneous and articular symptoms, with no serious infections or adverse events reported. Notably, liver enzyme levels and renal function also improved during the course of treatment.
Overall, apremilast appears to be well-tolerated and potentially beneficial add-on therapy to DBT for PsA. However, evidence is still limited by small sample sizes, short follow-up, highlighting the need for prospective trials.
IL-12/23 Inhibitor Regimens — Ustekinumab has been used in DBT for PsA with multi-domain involvement or inadequate monotherapy response, often combined with TNF inhibitors. Case reports by Cuchacovich et al and Babalola et al describe complete remission with ustekinumab–etanercept combinations and no adverse events during follow-up.50,51, However, safety issues have emerged across multiple reports. Gniadecki et al reported three PsA patients achieving marked PASI and pain VAS improvements but developing herpes zoster, bacterial pneumonia or retrotonsillar abscess.45 De Marco et al found similar efficacy in six patients, but recurrent infections, including erysipelas and pneumonia, necessitated treatment discontinuation in some.46 Overall, while TNFi–ustekinumab DBT may benefit select refractory PsA patients, evidence is limited to uncontrolled case series, and infection risk, bacterial and viral, appears consistent. Thus, such regimens should be reserved for cases where anticipated benefit clearly outweighs safety concerns.
IL-17 and IL-23 Inhibitor Regimens – Combining IL-17 or IL-23 inhibitors with other bDMARDs in PsA has been explored for complex or refractory cases, though evidence remains limited. In a Phase II trial of 240 PsA patients with inadequate methotrexate response, ABT-122 (dual TNF-α/IL-17A blockade) achieved ACR20 rates of 64.8–75.3% and PASI75 up to 77.6%, with no serious infections and similar adverse events across arms. However, no efficacy advantage over adalimumab was observed.42 Case reports and small series describe TNF inhibitor combinations (eg, ustekinumab + etanercept, secukinumab + etanercept, guselkumab + etanercept), showing periods of disease control but occasional infections, particularly with ustekinumab + TNFi.52 Other reports, such as risankizumab + golimumab for 12 months, noted marked improvement without adverse effects.54, A retrospective series of 12 patients on dupilumab plus IL-17/IL-23 inhibitors, including four PsA cases, found 75% clinical improvement, no severe infections, but conjunctivitis in 17%.47 Overall, IL-17/IL-23–based DBT may benefit select refractory PsA patients, especially with non-overlapping mechanisms. While no consistent pattern of serious infections, data is limited and further research is needed.
JAK inhibitor regimens – Studies combining JAK inhibitors with other biologics in PsA remain limited. Kashlan et al described a patient with long-standing PsA and psoriasis who was maintained on tofacitinib but experienced significant cutaneous disease.56 Brodalumab (IL-17 receptor A inhibitor) was added, leading to rapid skin improvement, but paradoxical PsA flare within a week occurred, prompting discontinuation. Subsequently, guselkumab was initiated with another PsA flare requiring hospitalization and steroid therapy. Thus, despite efficacy in skin disease, dual therapy involving JAK inhibitor and IL-17/23 blocker may precipitate paradoxical joint inflammation or unmask subclinical arthritis. The timing of flares after initiating the combination, while previously stable on tofacitinib, supports drug-induced phenomenon, rather than simple disease progression.
Hren et al reported a case series of six patients with treatment-refractory PsA and psoriasis who were managed with a DBT regimen of IL-17 or IL-23 inhibitor combined with oral JAK1 or TYK2 inhibitor.49 All patients had failed multiple prior therapies, and DBT resulted in significant improvement in both joint and skin symptoms, with several achieving minimal disease activity. However, treatment responses were variable, efficacy declined in two cases after several months, and one patient developed bronchitis during therapy. Although no serious infections or hospitalizations were observed, the limited sample size, retrospective nature, and short follow-up duration constrain the ability to draw definitive conclusions regarding safety.
In PsA, DBT may benefit treatment-refractory patients, especially with multi-domain involvement. Combinations such as apremilast with TNF or IL-23 inhibitors, ustekinumab with TNF inhibitors, and IL-17/IL-23 inhibitors with JAK inhibitors have improved both articular and cutaneous outcomes. However, infection risk, particularly with ustekinumab or JAK inhibitors, warrant cautious use, weighing potential benefit against harm (Table 3).
 |
Table 3 Infection Risk Comparison Between DBT and Biologic Monotherapy |
Axial Spondyloarthropathies (axSpA)
Despite improved outcomes with b/tsDMARDs, many axSpA patients still experience inadequate control with sequential switching strategy offering limited efficacy.58 These limitations have prompted growing interest in DBT (Table 4).
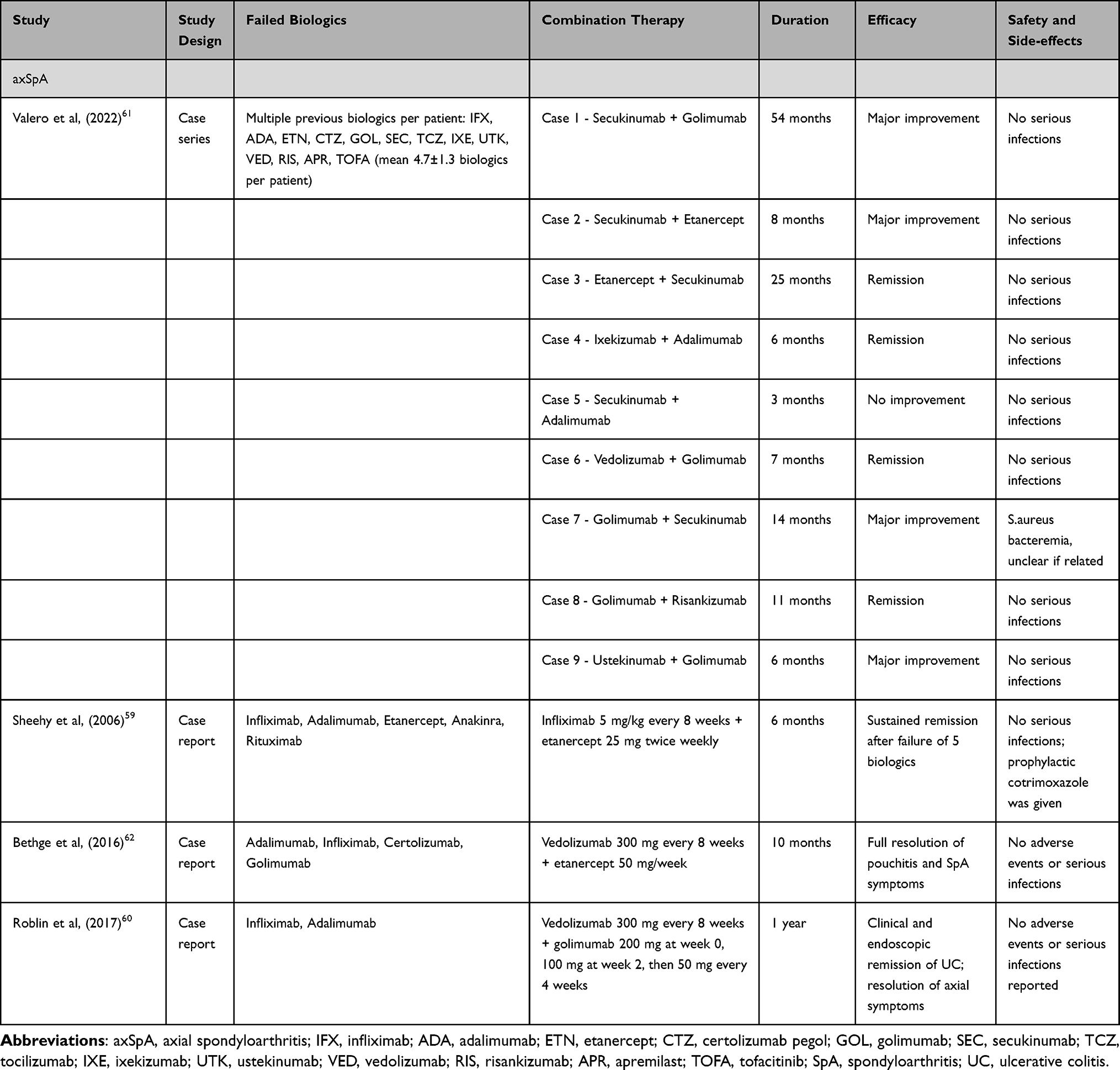 |
Table 4 Summary of Dual Biologic Therapy in Treatment-Refractory Axial Spondyloarthropathy |
One of the earliest reported cases of DBT in axSpA was described by Sheehy et al in 2006.59, A 28-year-old man with HLA-B27–associated arthritis who failed multiple conventional DMARDs and five biologic agents, including infliximab, adalimumab, etanercept, anakinra, and rituximab (all used sequentially with methotrexate). He was subsequently treated with simultaneous administration of infliximab (5 mg/kg every 8 weeks) and etanercept (25 mg twice weekly), resulting in dramatic clinical improvement, normalization of inflammatory markers (ESR and platelet count fell rapidly to normal levels) and sustained remission for at least six months without infectious complications or other adverse effects. Prophylactic cotrimoxazole was administered for Pneumocystis jirovecii pneumonia prevention, and methotrexate was discontinued due to potential interaction with cotrimoxazole.
Further support for DBT in axSpA comes from a case report of 56-year-old male with long-standing seronegative axSpA and refractory pouchitis.62 After secondary loss of response to several TNF inhibitors, vedolizumab was initiated, leading to remission of pouchitis but worsening of axial skeletal symptoms. The addition of etanercept led to rapid and sustained control of both intestinal and joint manifestations without any adverse events during 10 months of DBT. Similarly, Roblin et al reported a 48-year-old woman with HLA-B27–positive AS and ulcerative colitis who flared on vedolizumab monotherapy.62 The addition of golimumab achieved remission of both diseases, with no serious infections reported over one year. In both cases, vedolizumab’s gut-selective mechanism likely contributed to the favorable safety profile.
A 2022 retrospective case series provided further real-world evidence by examining nine patients with long-standing, multidomain SpA who had failed a median of five prior b/tsDMARDs.61 Various DBT regimens were used, including dual TNF and IL-17A blockade and combinations involving IL-12/23, IL-23, and vedolizumab. Eight of the nine patients achieved major clinical improvement, and four reached full remission based on standardized disease activity indices. Notably, most had failed the individual agents previously, suggesting synergistic benefit. Only one serious infection (Staphylococcus aureus bacteremia in a high-risk patient) occurred and was not definitively attributed to DBT.
In axSpA, DBT use is limited to small case series and reports, suggesting possible improvement or remission after monotherapy failure. While safety appears acceptable, the limited data means both its true efficacy and risk of serious adverse events remain uncertain.
Future Directions
While DBT might be considered a therapeutic option for multiple b/tsDMARDs-refractory cases, current evidence regarding efficacy and safety is limited. Some studies report no clear advantage over monotherapy in terms of efficacy, while others suggest an increased risk of infections and other adverse events. These uncertainties highlight the need for better, and perhaps more sophisticated, treatment strategies aiming to increase the efficacy and safety in those difficult-to-treat patients.
Biomarkers for Response - The development of predictive biomarkers for treatment response represents a promising strategy for optimizing biologic therapy selection and potentially reducing the need for DBT. In RA, serum metabolomic profiling has identified distinct panels capable of predicting response to specific biologics with high accuracy. Takahashi et al reported that five metabolites - betonicine, glycerol-3-phosphate, N-acetylalanine, hexanoic acid, and taurine - predicted TNF inhibitor response with 85.7% sensitivity and 100% specificity, whereas three metabolites - citric acid, quinic acid, and 3-aminobutyric acid -predicted abatacept response with 100% sensitivity and 90.9% specificity.63
Genetic markers have also shown promise in treatment stratification. In psoriasis, Dand et al demonstrated that HLA-C*06:02–negative patients were significantly more likely to respond to adalimumab compared to ustekinumab (6-month OR = 2.95; P = 5.85 × 10−7), with an even stronger association observed among those with psoriatic arthritis (OR = 5.98; P = 6.89 × 10−5).64 Similarly, proteomic profiling in psoriatic arthritis has identified a 57-protein synovial biomarker panel - including S100-A8, immunoglobulin kappa chain C, fibrinogen, haptoglobin, and annexins - that predicted response to adalimumab and successfully predicted abatacept response in 86% of patients in a blinded validation cohort.65
While these genetic and biomarkers are promising, further research and validation are required before such approaches can be integrated into routine clinical practice.
Induction of Immune Tolerance – Autoimmune diseases result from loss of immune homeostasis, where autoreactive lymphocytes escape tolerance mechanisms and drive pathogenic inflammation.66 Inducing immune tolerance has been achieved in both neonatal and adult animals, such as with short courses of anti-CD4 antibodies, without impairing overall immunity.67,68 However, greater MHC disparity, genetic heterogeneity, and environmental impact make tolerance induction more challenging in humans. Current strategies include antigen-independent approaches (eg, CD4⁺ T cell targeting with abatacept, which can delay RA onset and reduce progression) and antigen-specific methods such as peptide immunotherapy, tolerogenic dendritic cells, regulatory T cell therapies, in vivo Treg expansion, and microbiome modulation.69 Early intervention may offer the best opportunity for durable tolerance, though these strategies remain experimental at this stage.
Chimeric Antigen Receptor-T (CAR-T) Cell Therapy — Originally developed for hematologic malignancies, CAR-T therapy engineers a patient’s T cells ex-vivo to express chimeric antigen receptors, enabling targeted destruction of antigen-expressing cells with reduced collateral damage.70,71 These modified cells can proliferate and persist in-vivo, offering durable responses. Advances include multi-antigen targeting, enhanced signaling domains, safety switches, and CAR-Tregs for immunosuppressive applications, highlighting its potential benefits and future application.
Summary
Although DBT may offer clinical benefit patients with treatment-refractory rheumatic disease, it has not consistently demonstrated superior efficacy over monotherapy and often carries higher risk of serious infections. Risk may be reduced by combining two agents with differing immunosuppressive profiles, including at least one with minimal systemic effects, to target distinct pathways while limiting infection risk. Thus, DBT should be reserved for selected severe, multi-refractory cases, with careful benefit–risk assessment.
Acknowledgment
During the preparation of this work the author(s) used ChatGPT for spelling and grammar checks. After using this tool/service, the author(s) reviewed and edited the content as needed and take(s) full responsibility for the content of the publication.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this work.
Disclosure
The authors have no conflict of interest to declare.
References
1. El-Gabalawy H, Guenther LC, Bernstein CN. Epidemiology of immune-mediated inflammatory diseases: incidence, prevalence, natural history, and comorbidities. J Rheumatol Suppl. 2010;85:2–10. doi:10.3899/jrheum.091461
2. Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79:700–712. doi:10.1136/annrheumdis-2020-217159
3. Smolen JS, Landewé RBM, Bergstra SA, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2022 update. Ann Rheum Dis. 2023;82:3–18. doi:10.1136/ard-2022-223356
4. Ouardi NE, Maghraoui AE, Djossou HJ, et al. Discontinuation of biologic therapy in patients with rheumatoid arthritis and ankylosing spondylitis: analysis from a multicenter cohort study. Rheumatol Int. 2023;43(1):79–87. doi:10.1007/s00296-022-05237-7
5. Nagy G, Roodenrijs NMT, Welsing PM, et al. EULAR definition of difficult-to-treat rheumatoid arthritis. Ann Rheum Dis. 2021;80(1):31–35. doi:10.1136/annrheumdis-2020-217344
6. Coates LC, de Wit M, Buchanan-Hughes A, Smulders M, Sheahan A, Ogdie AR. Residual disease associated with suboptimal treatment response in patients with psoriatic arthritis: a systematic review of real-world evidence. Rheumatol Ther. 2022;9(3):803–821. doi:10.1007/s40744-022-00443-y
7. Singla S, Ribeiro A, Torgutalp M, Mease PJ, Proft F. Difficult-to-treat psoriatic arthritis (D2T PsA): a scoping literature review informing a GRAPPA research project. RMD Open. 2024;10(1):e003809. doi:10.1136/rmdopen-2023-003809
8. Chmielińska M, Felis-Giemza A, Olesińska M, Paradowska-Gorycka A, Szukiewicz D. The failure of biological treatment in axial spondyloarthritis is linked to factors related to increased intestinal permeability and dysbiosis: a prospective observational cohort study. Rheumatol Int. 2024;44(8):1487–1499. doi:10.1007/s00296-024-05614-4
9. Winthrop KL, Weinblatt ME, Bathon J, et al. Unmet need in rheumatology: reports from the Targeted Therapies meeting 2019. Ann Rheum Dis. 2020;79(1):88–93. doi:10.1136/annrheumdis-2019-216151
10. Furer V, Elkayam O. Dual biologic therapy in patients with rheumatoid arthritis and psoriatic arthritis. Rambam Maimonides Med J. 2023;14(2):e0007. doi:10.5041/RMMJ.10494
11. Pizano-Martinez O, Mendieta-Condado E, Vázquez-Del Mercado M, et al. Anti-drug antibodies in the biological therapy of autoimmune rheumatic diseases. J Clin Med. 2023;12(9):3271. doi:10.3390/jcm12093271
12. Krieckaert CL, Nurmohamed MT, Wolbink GJ. Methotrexate reduces immunogenicity in Adalimumab-treated rheumatoid arthritis patients in a dose-dependent manner. Ann Rheum Dis. 2012;71(11):1914–1915. doi:10.1136/annrheumdis-2012-201544
13. McInnes IB, Schett G. Cytokines in the pathogenesis of rheumatoid arthritis. Nat Rev Immunol. 2007;7(6):429–442. doi:10.1038/nri2094
14. Hamilton JA. GM-CSF in inflammation and autoimmunity. Trends Immunol. 2002;23(8):403–408. doi:10.1016/S1471-4906(02)02260-3
15. Nistala K, Wedderburn LR. Th17 and regulatory T cells: rebalancing pro- and anti-inflammatory forces in autoimmune arthritis. Rheumatology. 2009;48(6):602–606. doi:10.1093/rheumatology/kep028
16. Farutin V, Prod’homme T, McConnell K, et al. Molecular profiling of rheumatoid arthritis patients reveals an association between innate and adaptive cell populations and response to anti-tumor necrosis factor. Arthritis Res Ther. 2019;21(1):216. doi:10.1186/s13075-019-1999-3
17. Li X, Kimberly RP. Targeting the Fc receptor in autoimmune disease. Expert Opin Ther Targets. 2014;18(3):335–350. doi:10.1517/14728222.2014.877891
18. Hetland ML, Christensen IJ, Tarp U, et al. Direct comparison of treatment responses, remission rates, and drug adherence in patients with rheumatoid arthritis treated with Adalimumab, etanercept, or infliximab: results from eight years of surveillance in the Danish DANBIO registry. Arthritis Rheum. 2010;62(1):22–32. doi:10.1002/art.27227
19. Feige U, Hu YL, Gasser J, Campagnuolo G, Munyakazi L, Bolon B. Anti-interleukin-1 and anti-tumor necrosis factor-α synergistically inhibit adjuvant arthritis in Lewis rats. Cell Mol Life Sci. 2000;57(10):1457–1470. doi:10.1007/PL00000629
20. Dillon SR, Evans LS, Lewis KE, et al. Non-redundant roles of T cell costimulation pathways in inflammatory arthritis revealed by dual blockade of ICOS and CD28 with acazicolcept (ALPN-101). Arthritis Rheumatol. 2023;75(8):1344–1356. doi:10.1002/art.42484
21. Laragione T, Harris C, Gulko PS. Combination therapy of a TRPV2 agonist with a TNF inhibitor achieves sustained suppression of disease severity and reduced joint damage. Clin Exp Immunol. 2023;211(3):233–238. doi:10.1093/cei/uxac124
22. Privitera G, Onali S, Pugliese D, et al. Dual targeted therapy: a possible option for the management of refractory inflammatory bowel disease. J Crohns Colitis. 2020;14(10):1136–1147.
23. McCormack MD, Wahedna NA, Aldulaimi D, Hawker P. Emerging role of dual biologic therapy for the treatment of inflammatory bowel disease. World J Clin Cases. 2023;11(12):2621–2630. doi:10.12998/wjcc.v11.i12.2621
24. Goessens L, Colombel JF, Outtier A, et al. Safety and efficacy of combining biologics or small molecules for inflammatory bowel disease or immune-mediated inflammatory diseases: a European retrospective observational study. United Eur Gastroenterol J. 2021;9(10):1136–1147. doi:10.1002/ueg2.12170
25. Hirten RP, Iacucci M, Shah S, Ghosh S, Colombel JF. Combining biologics in inflammatory bowel disease and other immune mediated inflammatory disorders. Clin Gastroenterol Hepatol. 2018;16(9):1374–1382. doi:10.1016/j.cgh.2018.02.024
26. Burgevin A, Caron B, Sasson A, et al. Comparative safety of ustekinumab and vedolizumab in older patients with inflammatory bowel disease: a bicentric cohort study. J Clin Med. 2022;11(23):6967. doi:10.3390/jcm11236967
27. Genovese MC, Bathon JM, Martin RW, et al. Combination therapy with etanercept and anakinra in the treatment of patients with rheumatoid arthritis. Arthritis Rheum. 2004;50(5):1412–1419. doi:10.1002/art.20221
28. Weinblatt ME, Moreland LW, Westhovens R, et al. Safety of the selective co-stimulation modulator Abatacept in rheumatoid arthritis. Arthritis Rheum. 2006;54(9):2807–2816. doi:10.1002/art.22070
29. Weinblatt M, Schiff M, Goldman A, et al. Selective costimulation modulation using Abatacept in patients with active rheumatoid arthritis while receiving etanercept: a randomised clinical trial. Ann Rheum Dis. 2007;66(2):228–234. doi:10.1136/ard.2006.055111
30. Greenwald MW, Shergy WJ, Kaine JL, et al. Evaluation of the safety of rituximab in combination with a tumor necrosis factor inhibitor in patients with rheumatoid arthritis. Arthritis Rheum. 2010;62(9):2625–2632. doi:10.1002/art.27555
31. Genovese MC, Weinblatt ME, Aelion JA, et al. ABT-122, a bispecific dual variable domain immunoglobulin targeting tumor necrosis factor and interleukin-17A, in patients with rheumatoid arthritis with an inadequate response to methotrexate: a randomized, double-blind study. Arthritis Rheumatol. 2018;70(11):1710–1720. doi:10.1002/art.40580
32. Glatt S, Taylor PC, McInnes IB, et al. Efficacy and safety of bimekizumab as add-on therapy for rheumatoid arthritis in patients with inadequate response to certolizumab pegol: a proof-of-concept study. Ann Rheum Dis. 2019;78(8):1033–1040. doi:10.1136/annrheumdis-2018-214943
33. Rigby WF, Tony HP, Oelke K, et al. Safety of rituximab in combination with other biologic DMARDs in rheumatoid arthritis: an open-label study. J Rheumatol. 2013;40(5):599–604. doi:10.3899/jrheum.120924
34. Zou X, Bai XJ, Zhang LQ. Effectiveness of tofacitinib combined with iguratimod in the treatment of difficult-to-treat moderate-to-severe rheumatoid arthritis. Beijing Da Xue Xue Bao Yi Xue Ban. 2023;55(6):1013–1021. doi:10.19723/j.issn.1671-167X.2023.06.009
35. Zhang SX, Chen HR, Wang J, et al. The efficacy and safety of short-term and low-dose IL-2 combined with tocilizumab to treat rheumatoid arthritis. Front Immunol. 2024;15:1359041. doi:10.3389/fimmu.2024.1359041
36. Chang J, Wang G. A retrospective study of efficacy of tofacitinib combined with bDMARDs in the treatment of rheumatoid arthritis patients with inadequate response to bDMARDs. Int J Rheum Dis. 2024;27(9):e15311. doi:10.1111/1756-185X.15311
37. Koumakis E, Wipff J, Avouac J, Kahan A, Allanore Y. Severe refractory rheumatoid arthritis successfully treated with combination rituximab and anti-tumor necrosis factor-α-blocking agents. J Rheumatol. 2009;36(9):2125–2126. doi:10.3899/jrheum.090160
38. Blank N, Max R, Schiller M, Briem S, Lorenz HM. Safety of combination therapy with rituximab and etanercept for patients with rheumatoid arthritis. Rheumatology. 2009;48(4):440–441. doi:10.1093/rheumatology/ken491
39. Ghazanfar MN, Thomsen SF. Combined treatment with omalizumab and etanercept in a patient with chronic spontaneous urticaria and rheumatoid arthritis. J Dermatol Treat. 2019;30(4):387–388. doi:10.1080/09546634.2018.1515465
40. Yamada H, Hida N, Kurashima Y, Satoh H, Saito T, Hizawa N. A case of severe eosinophilic asthma and refractory rheumatoid arthritis well controlled by combination of IL-5Rα antibody and TNFα inhibitor. Allergol Int. 2019;68(4):536–538. doi:10.1016/j.alit.2019.04.003
41. Cohen SB, Emery P, Greenwald MW, et al. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: results of a multicenter, randomized, double-blind, placebo-controlled, Phase III trial at 24 weeks. Arthritis Rheum. 2006;54(9):2793–2806. doi:10.1002/art.22025
42. Mease PJ, Genovese MC, Weinblatt ME, et al. Phase II study of ABT-122, a TNF- and IL-17A-targeted dual variable domain immunoglobulin, in patients with psoriatic arthritis with an inadequate response to methotrexate. Arthritis Rheumatol. 2018;70(11):1778–1789. doi:10.1002/art.40579
43. Metyas S, Tomassian C, Messiah R, Gettas T, Chen C, Quismorio A. Combination therapy of apremilast and biologic agent as a safe option of psoriatic arthritis and psoriasis. Curr Rheumatol Rev. 2019;15(3):234–237. doi:10.2174/1573397115666181130094455
44. Takamura S, Sugai S, Taguchi R, Teraki Y. Combination therapy of apremilast and biologics in patients with psoriasis showing biologic fatigue. J Dermatol. 2020;47(3):290–294. doi:10.1111/1346-8138.15193
45. Gniadecki R, Bang B, Sand C. Combination of anti-tumour necrosis factor-α and anti-interleukin-12/23 antibodies in refractory psoriasis and psoriatic arthritis: a long-term case-series observational study. Br J Dermatol. 2016;174(5):1145–1146. doi:10.1111/bjd.14270
46. De Marco G, McGonagle D, Mathieson HR, et al. Combined inhibition of tumour necrosis factor-α and interleukin-12/23 for long-standing, refractory psoriatic disease: a differential role for cytokine pathways? Rheumatology. 2018;57(11):2053–2055. doi:10.1093/rheumatology/key199
47. Hren MG, Guenin S, Khattri S. Use of dual biologic therapy targeting the Th2 and Th17 axes simultaneously to treat patients with atopic dermatitis and concomitant psoriasis, psoriatic arthritis, or inflammatory bowel disease. J Am Acad Dermatol. 2024;91(1):138–140. doi:10.1016/j.jaad.2024.03.007
48. Guenin S, Andrews E, Lebwohl MG. Safety and efficacy of dual tyrosine kinase 2 inhibitor and monoclonal antibody therapy for psoriasis and psoriatic arthritis. Br J Dermatol. 2024;190(3):451–453. doi:10.1093/bjd/ljad473
49. Hren MG, Khattri S. Treatment of recalcitrant psoriasis and psoriatic arthritis with a combination of a biologic plus an oral JAK or TYK2 inhibitor: a case series. Ann Rheum Dis. 2024;83(10):1392–1393. doi:10.1136/ard-2024-225800
50. Cuchacovich R, Garcia-Valladares I, Espinoza LR. Combination biologic treatment of refractory psoriasis and psoriatic arthritis. J Rheumatol. 2012;39(1):187–193. doi:10.3899/jrheum.110295
51. Babalola O, Lakdawala N, Strober BE. Combined biologic therapy for the treatment of psoriasis and psoriatic arthritis: a case report. JAAD Case Rep. 2014;1(1):3–4. doi:10.1016/j.jdcr.2014.09.002
52. Thibodeaux Q, Ly K, Reddy V, Smith MP, Liao W. Dual biologic therapy for recalcitrant psoriasis and psoriatic arthritis. JAAD Case Rep. 2019;5(10):928–930. doi:10.1016/j.jdcr.2019.08.015
53. Balestri R, Magnano M, Girardelli CR, Bortolotti R, Rech G. Long-term safety of combined biological therapy in a patient affected by arthropathic psoriasis and atopic dermatitis. Dermatol Ther. 2020;33(4):e13498. doi:10.1111/dth.13498
54. Hanna S, Youssef P, Lowe P. Novel combination biologic therapy for recalcitrant psoriasis and psoriatic arthritis in a medically complex patient. Australas J Dermatol. 2022;63(1):e63–6. doi:10.1111/ajd.13752
55. Haberman RH, Castillo R, Scher JU. Induction of remission in biologic-naive, severe psoriasis and PsA with dual anti-cytokine combination. Rheumatology. 2021;60(7):e225–6. doi:10.1093/rheumatology/keaa880
56. Kashlan R, Slater K, Garber ME, Kartono F. Paradoxical psoriatic arthritis flare with the initiation of brodalumab and guselkumab. JAAD Case Rep. 2021;10:47–49. doi:10.1016/j.jdcr.2021.01.014
57. Zimmer S, Goldust M, Bhargava S, Wegner J, Grabbe S, Staubach-Renz P. Combination therapy of recalcitrant severe psoriasis with psoriatic arthritis, diabetes nephropathy, and liver cirrhosis. J Cosmet Dermatol. 2022;21(5):2226–2228. doi:10.1111/jocd.14367
58. Noureldin B, Barkham N. The current standard of care and the unmet needs for axial spondyloarthritis. Rheumatology. 2018;57(suppl_6):vi10–vi17. doi:10.1093/rheumatology/key217
59. Sheehy C, Murphy E, Barry M. Effective co-administration of infliximab and etanercept following the failure of sequential anti-TNF agents in a patient with HLA-B27-associated arthropathy. Rheumatology. 2006;45(10):1314–1315. doi:10.1093/rheumatology/kel211
60. Roblin X, Paul S, Ben-Horin S. Co-treatment with golimumab and vedolizumab to treat severe UC and associated spondyloarthropathy. J Crohns Colitis. 2018;12(3):379–380. doi:10.1093/ecco-jcc/jjx142
61. Valero C, Baldivieso JP, Gonzalez-Alvaro I, Tomero E, Castañeda S, García-Vicuña R. Effectiveness and safety of combined biological therapy in patients with refractory multidomain spondyloarthritis. Ann Rheum Dis. 2022;81(6):899–901. doi:10.1136/annrheumdis-2021-221812
62. Bethge J, Meffert S, Ellrichmann M, Conrad C, Nikolaus S, Schreiber S. Combination therapy with vedolizumab and etanercept in a patient with pouchitis and spondylarthritis. BMJ Open Gastroenterol. 2017;4(1):e000127. doi:10.1136/bmjgast-2016-000127
63. Takahashi S, Saegusa J, Onishi A, Morinobu A. Biomarkers identified by serum metabolomic analysis to predict biologic treatment response in rheumatoid arthritis patients. Rheumatology. 2019;58(12):2156–2164. doi:10.1093/rheumatology/kez199
64. Dand N, Duckworth M, Baudry D, et al. HLA-C*06:02 genotype is a predictive biomarker of biologic treatment response in psoriasis. J Allergy Clin Immunol. 2019;143(6):2120–2130. doi:10.1016/j.jaci.2018.11.038
65. Ademowo OS, Hernandez B, Collins E, et al. Discovery and confirmation of a protein biomarker panel with potential to predict response to biological therapy in psoriatic arthritis. Ann Rheum Dis. 2016;75(9):1688–1695. doi:10.1136/annrheumdis-2014-205417
66. Rayner F, Isaacs JD. Therapeutic tolerance in autoimmune disease. Semin Arthritis Rheum. 2018;48(3):558–562. doi:10.1016/j.semarthrit.2018.09.008
67. Billingham RE, Brent L, Medawar PB. Actively acquired tolerance of foreign cells. Nature. 1953;172(4379):603–606. doi:10.1038/172603a0
68. Waldmann H, Cobbold S. How do monoclonal antibodies induce tolerance? A role for infectious tolerance? Annu Rev Immunol. 1998;16:619–644. doi:10.1146/annurev.immunol.16.1.619
69. Emery P, Durez P, Dougados M, et al. Impact of T-cell costimulation modulation in patients with undifferentiated inflammatory arthritis or very early rheumatoid arthritis: a clinical and imaging study of Abatacept (the ADJUST trial). Ann Rheum Dis. 2010;69(3):510–516. doi:10.1136/ard.2009.119016
70. Gill S, Maus MV, Porter DL. Chimeric antigen receptor T cell therapy: 25 years in the making. Blood Rev. 2016;30(3):157–167. doi:10.1016/j.blre.2015.10.003
71. Ohno R, Nakamura A. Advancing autoimmune rheumatic disease treatment: CAR-T cell therapies—evidence, safety, and future directions. Semin Arthritis Rheum. 2024;67:152479. doi:10.1016/j.semarthrit.2024.152479
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is Tofacitinib Effectiveness in Patients with Rheumatoid Arthritis Better After Conventional Than After Biological Therapy? – A Cohort Study in a Colombian Population
Santos-Moreno P, Martinez S, Ibata L, Villarreal L, Rodríguez-Florido F, Rivero M, Rojas-Villarraga A, Galarza-Maldonado C
Biologics: Targets and Therapy 2022, 16:107-117
Published Date: 13 July 2022
Demographic, Physical, and Psychological Determinants of Patient Experience with Subcutaneous Self-Injection in Patients with Rheumatoid Arthritis: Structural Equation Modeling Approach
Onishi A, Kaizu M, Shirasugi I, Yagyu T, Ueda Y, Sakai Y, Miura Y, Saegusa J
Patient Preference and Adherence 2023, 17:1551-1559
Published Date: 3 July 2023
Health Disparities in Rheumatology in the United States
Wright GC, Zueger PM, Copley-Merriman C, Khan S, Costello J, Krumbach A, Reddy P, Tanjinatus O, Wells AF
Open Access Rheumatology: Research and Reviews 2025, 17:1-12
Published Date: 9 January 2025
The Effects of Disease-Modifying Antirheumatic Drugs on Cardiovascular Risk in Inflammatory Joint Diseases: Current Evidence and Uncertainties
Garmish O, Smiyan S, Hladkykh F, Koshak B, Komorovsky R
Vascular Health and Risk Management 2025, 21:593-605
Published Date: 4 August 2025
Central Sensitization and Nociplastic Pain: Shared Mechanisms in Fibromyalgia, Osteoarthritis, and Inflammatory Arthritis
Hladkykh FV, Liadova TI, Matvieienko MS, Komorovsky R, Smiyan S, Student V
Journal of Pain Research 2026, 19:571311
Published Date: 26 March 2026