Back to Journals » Drug Design, Development and Therapy » Volume 20
Benzodiazepine Use Among Patients Receiving Methadone Maintenance Treatment: A Descriptive Study
Authors Liu Y ![]() , Hong Q, Shen W
, Hong Q, Shen W ![]() , Li L
, Li L ![]() , Li Z, Zhou W, Xie X
, Li Z, Zhou W, Xie X ![]()
Received 7 November 2025
Accepted for publication 12 February 2026
Published 24 February 2026 Volume 2026:20 579917
DOI https://doi.org/10.2147/DDDT.S579917
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yan Zhu
Yue Liu,1,2 Qingxiao Hong,2 Wenwen Shen,1,2 Longhui Li,2 Zimeng Li,3 Wenhua Zhou,2 Xiaohu Xie2
1Department of Psychiatry, Affiliated Kangning Hospital of Ningbo University, Ningbo, Zhejiang, 315201, People’s Republic of China; 2Zhejiang Key Laboratory of Drug Addiction and Brain Health, Ningbo, Zhejiang, 315201, People’s Republic of China; 3Department of Clinical Medicine, Hangzhou Medical College, Hangzhou, Zhejiang, 310000, People’s Republic of China
Correspondence: Xiaohu Xie; Wenhua Zhou, Zhejiang Key Laboratory of Drug Addiction and Brain Health, No. 1, Zhuangyu South Road, Zhuangshi Street, Zhenhai District, Ningbo, Zhejiang, 315201, People’s Republic of China, Email [email protected]; [email protected]
Purpose: This study aimed to investigate the patterns and characteristics of benzodiazepine (BZD) use among patients receiving methadone maintenance treatment (MMT).
Methods: A total of 80 participants (40 with and 40 without BZD use) were recruited from the MMT clinic of the Affiliated Kangning Hospital of Ningbo University between April 2024 and March 2025. All participants were assessed using the BZD Use Questionnaire (BUQ), the Chinese version of Barratt impulsiveness scale (BIS-C), the Self-rating Anxiety Scale (SAS), the Self-rating Depression Scale (SDS), and the Quality of Life Scale for Drug Addicts (QOL-DA).
Results: Among 80 initially selected participants, 71 (BZD group: n=39; non-BZD group: n=32) were included in the final analysis after exclusions for invalid data. In univariate comparisons, the BZD group had a significantly higher prevalence of comorbid mental, sleep, and chronic disorders, higher scores on impulsivity (total, motor, and non-planning), anxiety, and depression scales, and lower scores on the total score as well as the psychological and symptoms/side effects domains of the QOL-DA (all P < 0.05). However, after adjusting for potential confounders, multivariate regression analyses indicated that BZD use was independently associated with higher anxiety levels (β = 0.279, P < 0.05) and greater total impulsivity (β = 0.439, P < 0.001). Regarding impulsivity subscales, BZD use was independently associated with non-planning (β = 0.265, P < 0.05) and motor impulsivity (β = 0.345, P < 0.05), but not with attentional impulsivity. No significant independent associations were found between BZD use and depression or any domain of quality of life (all P > 0.05).
Conclusion: BZD use was independently associated with higher levels of impulsivity and anxiety after controlling for key comorbidities, but not with depression or QOL. The causal direction between BZD use and increased impulsivity/anxiety in MMT patients remains unclear, potentially reflecting either pharmacological effects or pre-existing higher levels of impulsivity or anxiety.
Keywords: methadone maintenance treatment, benzodiazepines, impulsivity, anxiety, depression, quality of life
Introduction
Opioid use disorder (OUD) is a chronic, relapsing brain disease characterized by compulsive drug seeking and use despite harmful consequences, accompanied by profound neurochemical and molecular changes.1 It poses a major public health challenge, being closely associated with increased morbidity, mortality, and criminal behaviour. OUD is also strongly linked to injection drug use, a major driver of blood-borne viral infections such as hepatitis C virus (HCV) and human immunodeficiency virus (HIV).2 Methadone maintenance treatment (MMT), a substitution therapy for OUD, is one of the most widely implemented and effective interventions for preventing relapse, reducing opioid-related crime, and curbing the transmission of infectious diseases such as HIV/AIDS.3
Benzodiazepines (BZDs), first introduced in the 1960s (eg, chlordiazepoxide), quickly gained clinical popularity due to their improved safety profile over barbiturates.4 They are commonly prescribed for both psychiatric and non-psychiatric conditions, including anxiety, insomnia, seizures, and pain.5 However, long-term use leads to the development of tolerance and dependence,4 and continuous prescription is generally discouraged. Despite this, BZD misuse remains a global concern.6 Individuals with a personal or family history of substance use disorders are particularly vulnerable to BZD misuse.7 Co-use of BZDs with opioids is a major clinical risk factor for overdose.8 Although BZDs are mild respiratory depressants when used alone, their concurrent use with opioids can lead to profound respiratory suppression.9 Notably, individuals who filled prescriptions for a BZD in addition to an opioid had a nearly 15-fold greater risk of drug-related death than individuals not prescribed either drug.10
Recent data indicate a sharp rise in emergency visits and overdose fatalities linked to combined opioid–BZD use, exceeding the rates attributed to either substance alone.11,12 Substantial evidence demonstrates that this combination heightens the risk of severe respiratory and fatal outcomes.9,13 Patients with OUD undergoing methadone or buprenorphine maintenance therapy are especially susceptible to BZD misuse,14 with usage rates as high as 66% in some methadone clinics.15 In an Israeli cohort, lifetime BZD misuse among MMT patients was 66.3%, with current misuse rates at 50.8%, and approximately half of users initiated BZD use after entering the methadone program.10
BZD users in MMT programs often differ physiologically from general BZD users, presenting with older age, multiple comorbidities (eg, HCV or HIV from previous syringe sharing), and impaired hepatic, renal, pulmonary, and immune function.16,17 Such physiological vulnerabilities amplify the risk of adverse reactions, particularly respiratory depression and fatal overdose when opioids are concurrently used.9 In China, national MMT guidelines explicitly prohibit the concomitant use of BZDs.18
Accumulating evidences suggest that impulsivity may be a behavioral marker of the propensity to take addictive drugs.19,20 Patients with opioid, cocaine, or amphetamine use disorders exhibit significantly higher impulsivity than healthy controls.21–23 Impulsivity also predicts treatment retention and relapse risk; higher impulsivity is associated with shorter durations in maintenance therapy.24,25
Unlike illicit drugs such as opioids and cocaine, BZDs are prescription medications with recognised clinical applications. However, many former opioid users in MMT programs continue to experience persistent psychological and physical distress — such as anxiety, depression, pain, and protracted withdrawal symptoms — even after opioid cessation. Consequently, some may self-medicate with BZDs to alleviate these symptoms without medical supervision.26
However, it remains unclear whether MMT patients using BZDs exhibit distinct patterns of impulsivity, anxiety, depression, and quality of life (QOL) compared with non-users. We hypothesized that concurrent BZD users would demonstrate higher levels of impulsivity, anxiety, and depression, along with lower QOL, than non-users. To test this hypothesis and clarify these associations, this study aimed to retrospectively examine the characteristics of MMT patients concurrently using BZDs through the administration of standardized psychological and behavioural assessments.
Materials and Methods
Participants
This study was approved by the Ethics Committee of the Affiliated Kangning Hospital of Ningbo University (Approval No.: NBKNYY-2024-LC-12) and conducted in accordance with the Declaration of Helsinki. This study was registered at the Chinese Clinical Trial Registry (ChiCTR2400086237). All participants provided written informed consent prior to enrollment. Participants were recruited from the MMT clinic of the Affiliated Kangning Hospital of Ningbo University between April 2024 and March 2025.
Inclusion Criteria
Participants were eligible if they met all of the following conditions: (1) enrollment in MMT for more than 12 months; (2) age between 18 and 60 years; (3) absence of severe physical or psychiatric disorders; (4) no impairment in verbal communication; and (5) use of BZDs within the preceding six months.
Exclusion Criteria
Participants were excluded if they (1) had severe physical or psychiatric illnesses interfering with participation; (2) exhibited intellectual disabilities or language disorders; or (3) engaged in concurrent use of other addictive substances (eg, methamphetamine, cannabis).
The source population comprised 158 patients identified from the clinic registry. Using a structured questionnaire, we classified them as 73 BZD users and 85 non-users, with a target sample size of 40 per group based on practical feasibility, available resources, and precedents from similar cross-sectional studies. To obtain two equally sized and comparable groups while minimizing selection bias, we implemented a sequential, randomization-based recruitment procedure. Separate random sequences were computer-generated for the BZD user list (n=73) and the non-user list (n=85). Based on an estimated 75–80% combined consent and eligibility rate from previous similar studies in this clinic, we planned to contact the first 50 individuals from each randomized list. Invitations were issued strictly according to this pre-generated random order; if a contacted individual was unreachable, declined, or was ineligible, the next sequentially listed individual was immediately invited. This process continued until 40 eligible participants were enrolled per group or the list was exhausted. Recruitment was completed after inviting the 48th individual in the BZD user list and the 52nd in the non-user list. Neither group exhausted its full list, resulting in a final sample of 80 participants (40 per group). Throughout the process, the research team was blinded to the allocation sequence to minimize selection bias.
Medication
All participants had received MMT for more than 12 months. Methadone doses remained stable after the induction phase, ranging from 25 mg to 140 mg daily. Dosing followed an individualized titration principle aimed at achieving optimal control of withdrawal symptoms and cravings, ensuring subjective tolerability, and preventing adverse effects on consciousness or occupational functioning.
In this study, any self-reported use of BZDs within the six months prior to assessment was operationally defined as misuse, based on Chinese MMT guidelines which prohibit concomitant BZD use due to the well-established risk of severe respiratory depression from BZD-opioid interactions.
Measurements
We assessed BZD use characteristics, impulsivity, anxiety, depression, and QOL in 80 MMT patients using validated instruments administered by trained psychologists.
BZD Use Questionnaire (BUQ)
The BUQ, an interviewer-administered tool utilizing open-ended questions, documented BZD use characteristics and patterns. Data collection covered (1) demographic information (eg, gender, age) and (2) use characteristics (eg, route of administration, reasons for use); complete data are shown in Tables 1 and 2.
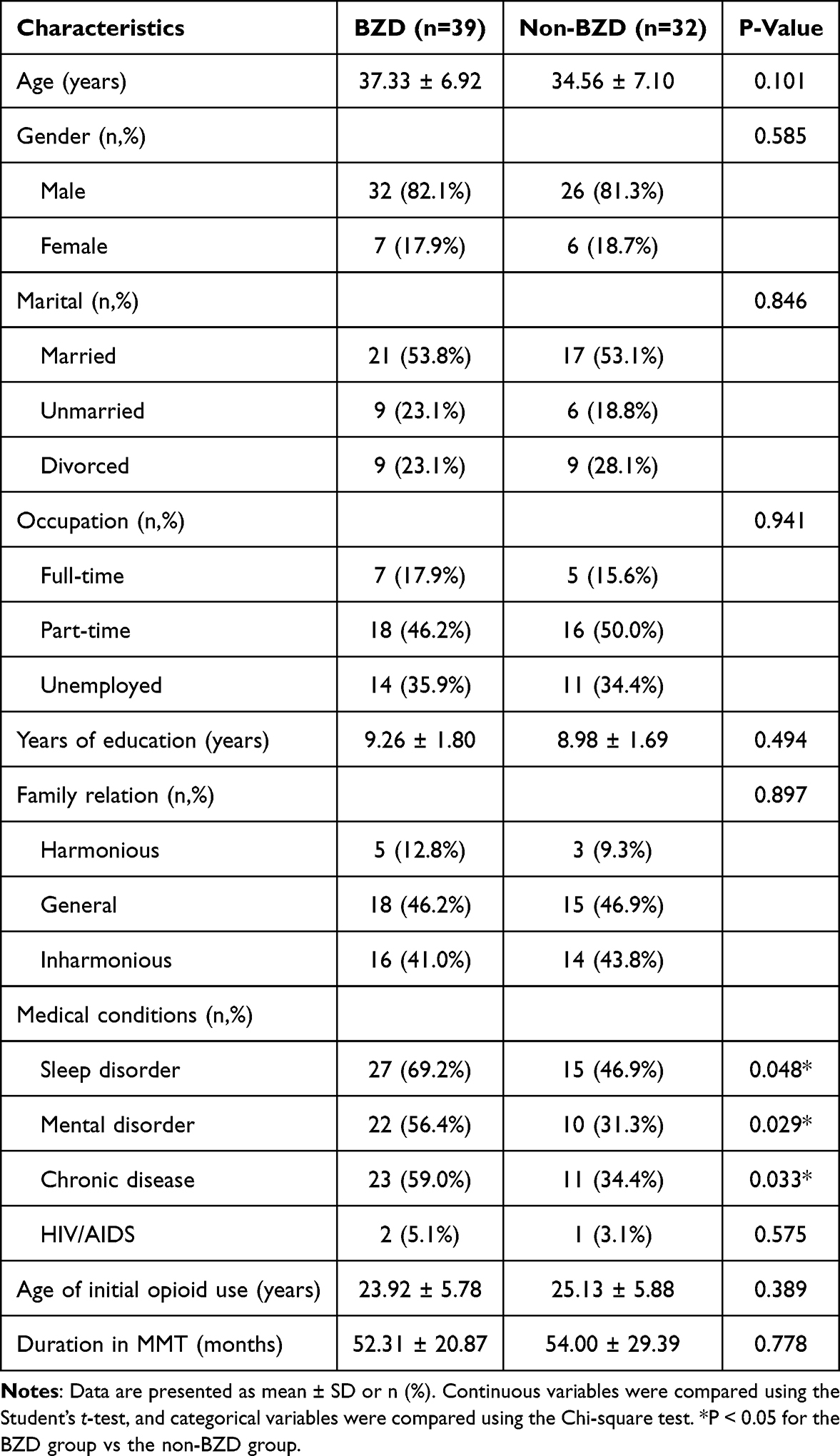 |
Table 1 Demographic Characteristics of the Study Participants |
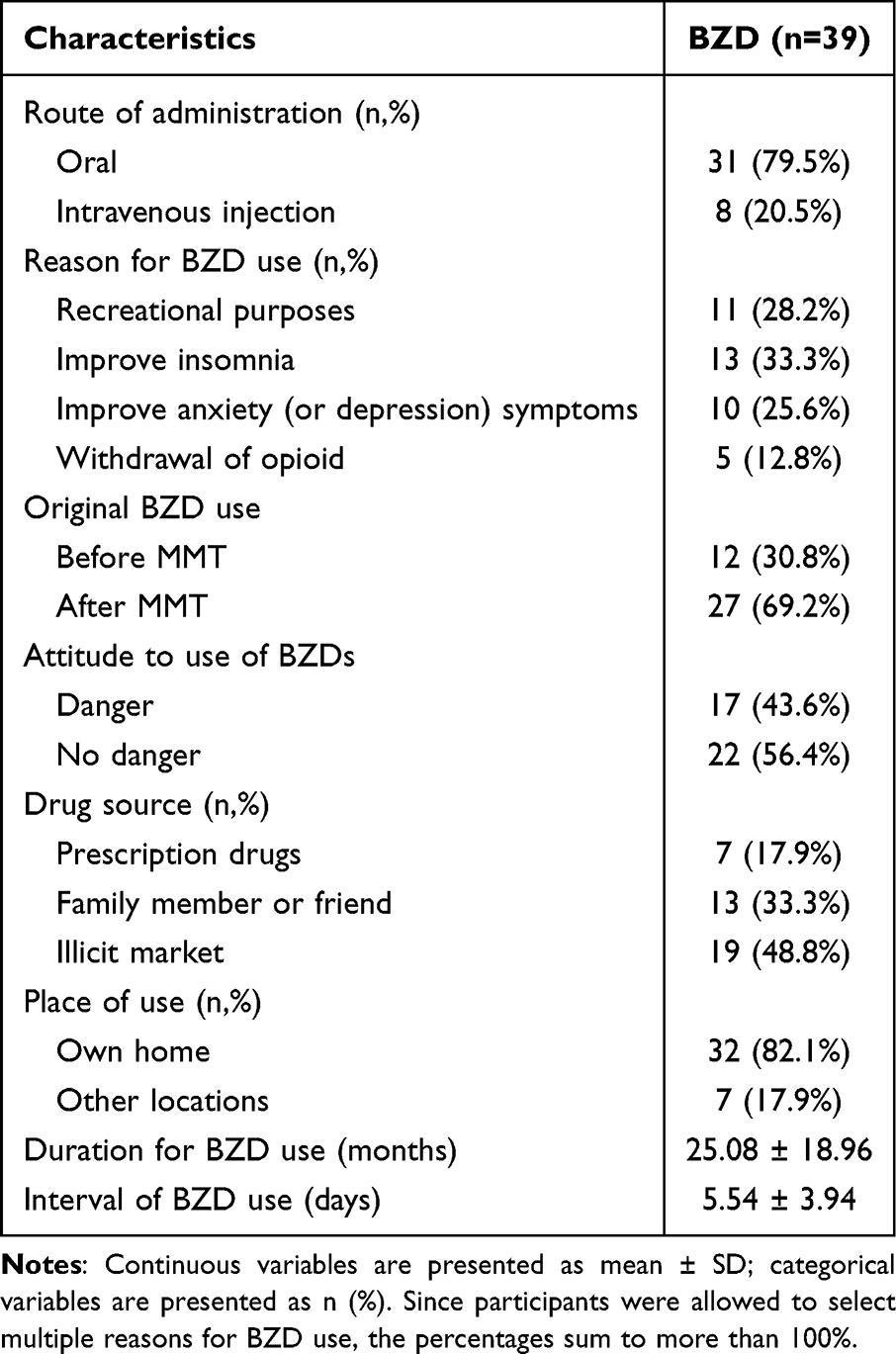 |
Table 2 Characteristics of BZD Use among Study Participants |
The diagnosis of comorbid conditions—primarily including mental disorders, sleep disorders, and chronic diseases—was based on participant self-report and clinical records from methadone maintenance clinics. To enhance the reliability of the data, electronic health records from these clinics were used, with participants’ informed consent, to cross-verify and supplement self-reported diagnoses for specific conditions.
Chinese Version of Barratt Impulsiveness Scale-11 (BIS-11-C)
The Barratt Impulsiveness Scale (BIS) is a self-report instrument measuring impulsive personality traits.27 The Chinese version, adapted by Zhou Liang et al,28 demonstrates strong reliability and validity in Chinese populations. BIS-11-C includes 30 items forming three dimensions—attentional, non-planning, and motor impulsiveness. Higher scores indicate greater impulsivity.29
Self-Rating Anxiety Scale (SAS)
Developed by Zung in 1971,30 the SAS comprises 20 items rated on a four-point Likert scale (1–4), reflecting symptom frequency over the preceding week. The raw score is multiplied by 1.25 to obtain a standardized score: <50 indicates no anxiety; 50–59 mild; 60–69 moderate; ≥70 severe anxiety. The Chinese version has shown good psychometric properties.31,32
Self-Rating Depression Scale (SDS)
The SDS is a 20-item self-report measure of depressive symptoms.33,34 Each item is rated from 1 to 4, with the raw score multiplied by 1.25 to yield a standard score: <53 indicates no depression; 53–62 mild; 63–72 moderate; ≥73 severe depression. The Chinese version demonstrates good reliability and validity.31,32
Quality of Life Scale for Drug Addicts (QOL-DA)
The QOL-DA assesses quality of life in patients with substance use disorders.35 It contains 41 items across four domains—physical function, psychological function, symptoms/side effects, and social function—rated on a five-point Likert scale (from 1 to 5). Higher scores indicate better QOL.
Data Analysis
Statistical analyses were conducted using SPSS version 26.0. Descriptive analyses were performed to determine proportions of BZD use characteristics. The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed data were compared between groups using independent-sample t-tests, while the Mann–Whitney U-test was applied for variables that violated the normality assumption, specifically years of education, age of initial opioid use, and duration in MMT. Categorical variables were analyzed using the chi-square test. A p-value < 0.05 was considered statistically significant.
To assess the independent relationships between BZD use and various outcomes, we conducted separate multiple linear regression analyses for the following: anxiety (SAS), depression (SDS), impulsivity (BIS-11), and quality of life (QOL-DA). In each model, BZD use (yes/no) served as the primary predictor. Based on clinical relevance, all models were adjusted for the following potential confounders: sex, age, duration in MMT, and the presence of mental disorders, sleep disorders, and chronic diseases. Model fit was assessed using adjusted R2 and omnibus F-tests. The significance of individual predictors was evaluated with t-tests, applying a two-sided alpha level of 0.05.
Results
Demographic Characteristics
A total of 80 participants were recruited; 71 provided valid data (39 in the BZD group, 32 in the non-BZD group). Four cases were excluded due to coding errors, and five due to logical inconsistencies or >15% missing data. No significant differences were observed between groups in age, gender, marital status, education, or other demographic characteristics (P > 0.05). The sample was predominantly male (81.7%). Nearly half were unmarried or divorced (46.5%), and 35.2% were unemployed (Table 1).
No significant between-group differences were found for age at initial opioid use, duration in MMT, or HIV co-infection (P > 0.05). However, participants in the BZD group showed a significantly higher prevalence of mental disorders (P = 0.029), sleep disorders (P = 0.048), and chronic conditions such as hepatitis B/C, cardiovascular/cerebrovascular diseases (P = 0.033) (Table 1).
BZD Use Characteristics
Among BZD users, 71.8% reported self-medicating for opioid withdrawal-related symptoms (eg, anxiety, depression, insomnia), while 28.2% reported recreational use for euphoria. Oral and intravenous routes were both reported, with intravenous use accounting for 20.5%. Drug sources included medical prescriptions (17.9%), friends/family, and the illicit market. The mean interval between BZD uses was 5.54 ± 3.94 days (Table 2).
Comparison of Impulsivity, SAS and SDS
In the overall sample, 52.1% and 40.9% of participants met the criteria for clinically significant anxiety (defined as an SAS score ≥50) and depression (defined as an SDS score ≥53), respectively.31,32 Group comparisons using independent-samples t-tests indicated that the BZD group scored significantly higher than the non-BZD group in impulsivity: total BIS score (77.87 ± 11.49 vs 68.06 ± 10.72, P = 0.004), non-planning impulsivity (25.97 ± 7.68 vs 21.94 ± 5.7, P = 0.017), and motor impulsivity (28.95 ± 7.04 vs 24.81 ± 7.45, P = 0.019). Similarly, SAS scores (54.36 ± 13.99 vs 47.81 ± 13.13, P = 0.047) and SDS scores (47.67 ± 14.29 vs 40.00 ± 13.94, P= 0.026) were significantly higher in the BZD group (Table 3).
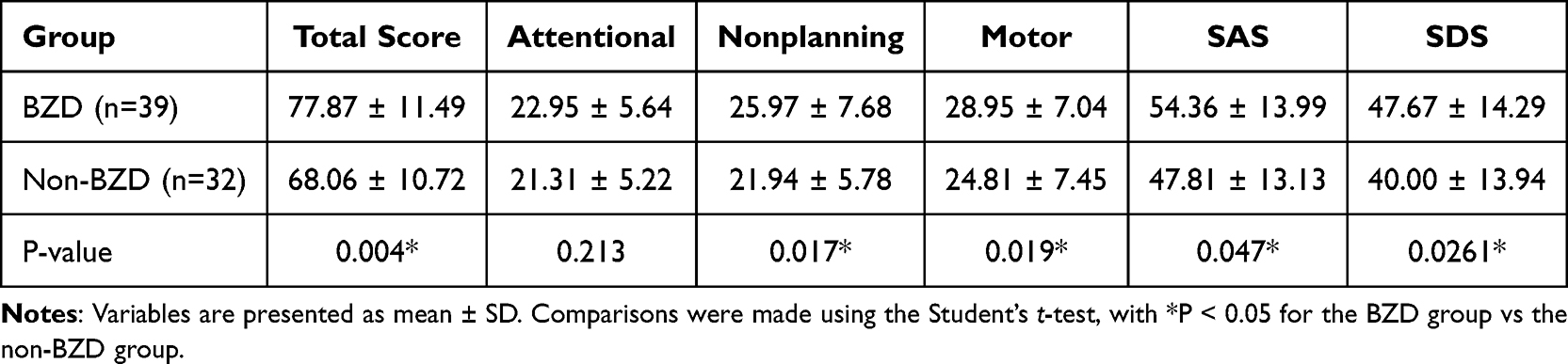 |
Table 3 Comparison of BIS, SAS, and SDS Scores Between the Two Groups |
Multicollinearity diagnostics, conducted prior to regression analysis, showed no concerns with all variance inflation factors below 2 (Table 4), supporting the inclusion of all predictors in the models. The overall regression models for anxiety (SAS), depression (SDS), impulsivity (BIS-11), and quality of life (QOL-DA) were statistically significant (P < 0.05). As detailed in Table 5, multivariate regression analysis revealed that BZD use was independently associated with higher levels of anxiety (β = 0.279, P < 0.05) and greater total impulsivity (β = 0.439, P < 0.001). Analysis of impulsivity subscales revealed positive associations with non-planning impulsivity (β = 0.265, P < 0.05) and motor impulsivity (β = 0.345, P < 0.05), but not with attentional impulsivity. No significant associations were observed between BZD use and depression or any domain of QOL (all P > 0.05).
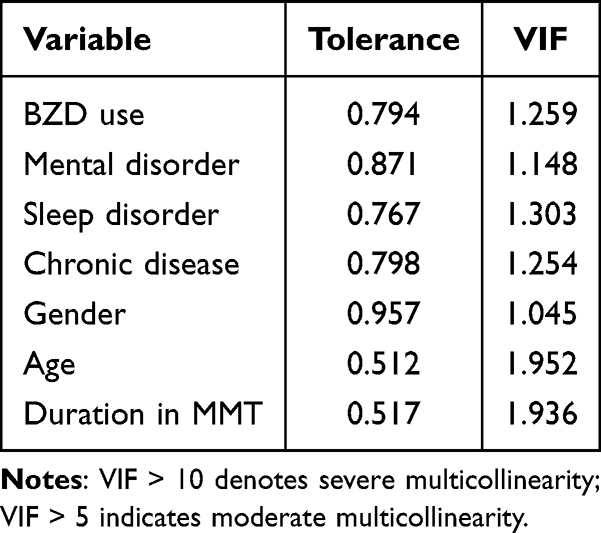 |
Table 4 Multicollinearity Diagnostics: Tolerance and Variance Inflation Factor (VIF) |
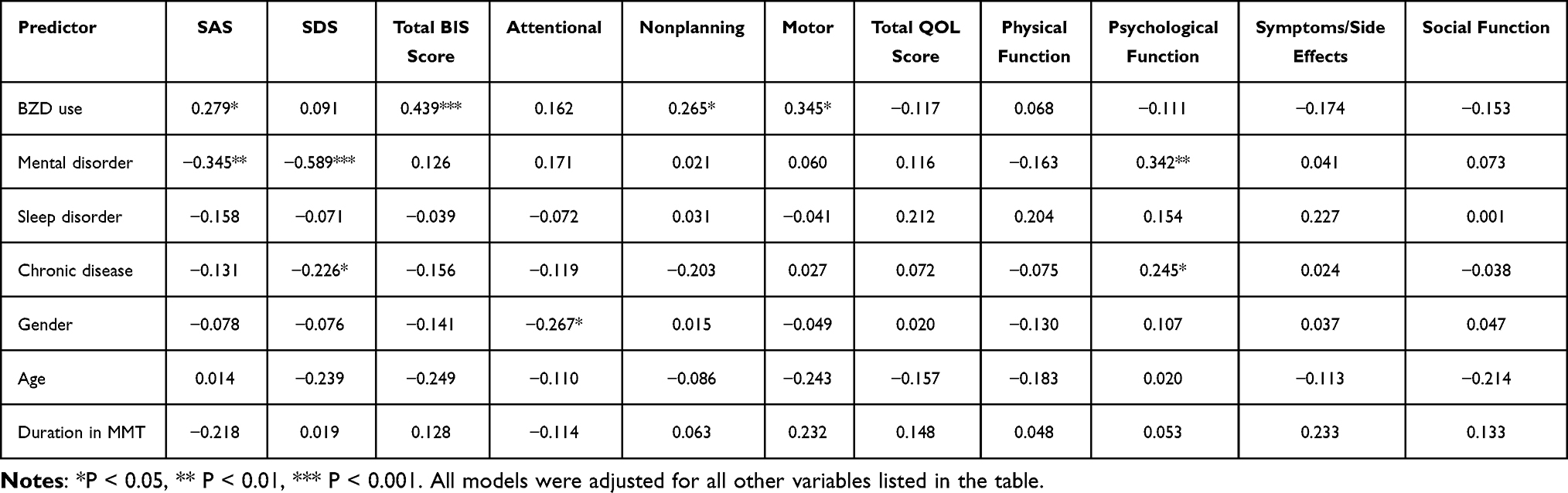 |
Table 5 Multiple Regression Analyses Examining Associations Between BZD Use and Various Outcomes (Standardized Coefficients, β) |
Comparison of QOL-DA
Group comparisons using independent-samples t-tests indicated that, compared with the non-BZD group, the BZD group reported significantly lower QOL-DA total scores (134.31 ± 20.44 vs 145.19 ± 22.72, P = 0.037), as well as lower psychological function (P = 0.014) and symptoms/side effects (P = 0.022) subscale scores. No significant differences were found in physical or social function (P > 0.05) (Table 6). However, subsequent multivariate regression analysis, adjusting for potential confounders, revealed no significant independent association between BZD use and any domain of QOL (all P > 0.05) (Table 5).
 |
Table 6 Comparison of QOL-DA Scores Between the Two Groups |
Discussion
The use and misuse of BZDs are highly prevalent among individuals receiving MMT. Previous studies have reported prevalence rates of up to 50% among this population.15 Furthermore, more than half of BZD users undergoing MMT reportedly began using BZDs only after entering the program.10 In our MMT clinic, the prevalence of BZD misuse was 54.7%, with 69.2% of BZD users initiating use after starting MMT. These findings are consistent with previous research. We propose that the physical and psychological discomfort associated with opioid withdrawal may serve as a primary motivation for initiating BZD use following enrollment in MMT. This underscores the critical need for timely interventions to manage post-withdrawal symptoms and prevent secondary substance misuse.
A particularly noteworthy finding of this study was that 28.2% of participants reported current recreational BZD misuse, despite having initially used them for symptom relief. Several factors may explain the high prevalence of recreational misuse among MMT patients. First, unlike heroin, methadone lacks euphoric effects; thus, some individuals may combine it with BZDs to alleviate cravings or achieve a “high.”10 Second, there remains a common misconception that BZDs are relatively safe or non-addictive. Third, unintentional misuse often begins with self-medication for sleep disturbances, withdrawal symptoms, or psychological distress (eg, anxiety, depression) but can evolve into habitual recreational use over time.
Association Between BZDs and Impulsivity
Impulsivity is a multidimensional neuropsychological construct commonly defined as the tendency to act prematurely without adequate consideration of consequences.21,36 While prior research on impulsivity and addiction has largely focused on cocaine, opioids, and amphetamines, the misuse of prescription drugs—particularly BZDs—has attracted increasing attention in recent years. Evidence suggests that individuals with a history of heroin use receiving opioid substitution therapy (eg, methadone or buprenorphine) are especially vulnerable to BZD misuse.37
A central finding of this study is that BZD use maintained an independent association with higher levels of overall impulsivity, non-planning impulsivity, and motor impulsivity, even after controlling for key confounders including comorbid conditions such as mental disorders, sleep disorders, and chronic diseases. Two potential explanations can be considered. First, individuals with higher baseline impulsivity may be more susceptible to co-using BZDs, as impulsivity is a well-established risk factor for substance misuse. Alternatively, BZD use itself may exacerbate impulsivity through its neurochemical effects on inhibitory control. However, this hypothesis requires longitudinal investigation to determine causality.
Associations Between BZDs, Anxiety, and Depression
Anxiety and depression are highly prevalent among individuals with OUD undergoing MMT. In our study, the prevalence rates of anxiety and depression were 52.1% and 40.9%, respectively—figures consistent with prior literature.38,39
Although BZDs have been widely prescribed for their anxiolytic properties,40 our study revealed that BZD use was independently associated with higher anxiety levels, even after accounting for key comorbidities including mental, sleep, and chronic disorders. This seemingly paradoxical result may be explained by two factors. First, BZDs may be used in an addictive manner (at high doses and irregularly) in non-medical contexts, which can cause adverse physiological effects and thereby limit the manifestation of their anti-anxiety properties. Second, concurrent polysubstance use can exacerbate both physical and psychological distress, impair quality of life, and disrupt social and familial support systems, all of which may aggravate pre-existing anxiety symptoms. Alternatively, the observed association could reflect reverse causality: individuals with more severe anxiety symptoms may be more likely to initiate or escalate BZD use as a form of self-medication. This explanation does not preclude the aforementioned mechanisms, since maladaptive use patterns could develop over time. Longitudinal studies are needed to disentangle the temporal and causal relationships between BZD use and anxiety symptomatology in this clinical population.
Furthermore, our results revealed an important finding: the significant difference in depression scores between BZD users and non-users observed in unadjusted analyses was no longer present after controlling for relevant comorbidities and other confounding factors, indicating no independent association between BZD use and depression levels. This contrasts with some previous reports that identify BZD use as a risk factor for depression and link its cessation to symptomatic improvement in MMT patients.41,42 Several considerations may explain these discrepant findings. Methodological variations, particularly in the selection of adjusted confounders, likely play a role. Additionally, residual confounding by unmeasured factors (eg, disease severity, social support) or limited statistical power due to our sample size may have obscured a more complex association.
Nevertheless, our analysis suggests that among this highly comorbid MMT population, comorbidities—including mental disorders, sleep disorders, and chronic somatic diseases—act as significant confounders in the relationship between BZD use and depression. The elevated symptom burden observed among BZD users appears to be largely attributable to their greater baseline psychiatric and somatic comorbidity, rather than to a direct effect of BZD use. These findings highlight the necessity of rigorously adjusting for such comorbidities in similar research.
Association Between BZDs and QOL
QOL encompasses both physical and psychological well-being.43 Although initial unadjusted analysis indicated lower QOL scores among BZD users, this association was not independent of confounding factors. The link appears to be driven by a greater baseline burden of comorbidities—such as mental and chronic somatic disorders—in BZD users, rather than by a direct pharmacological effect. Consequently, interventions aimed at enhancing QOL in this clinically complex population should focus on the integrated management of these underlying medical and mental conditions.
External Validity and Generalizability
The findings of this study must be interpreted within the context of its specific population, as all participants were recruited from a Chinese clinical setting. Substantial inter-individual variability in drug metabolism is well-documented across different ethnic and ancestral groups, with pronounced differences frequently observed between populations of European and East Asian descent.44 Such ethnic disparities in pharmacokinetics and pharmacogenomics can directly influence drug exposure, therapeutic efficacy, and safety profiles.45 Therefore, these factors may limit the broader extrapolation of our clinical findings to other populations, implying that when designing multi-regional trials or considering generalizability, it is imperative to account for these variations.
Future Prospects
At present, the psychiatric mechanisms underlying drug-related addictive behaviors remain incompletely characterized. It has often been implicitly assumed that the same symptomatic domains targeted by the therapeutic use of BZDs also contribute to the development of dependence.46 Given this complexity, early identification and intervention are essential for addressing both unintentional and recreational BZD use within the MMT population.
To translate these insights into practice, several pragmatic measures are recommended for MMT settings. First, implementing routine screening for BZD use and comorbid mental health conditions in MMT clinics is a critical step for early detection. Second, delivering structured psychoeducation regarding the risks of BZD misuse is warranted. Finally, skills-based interventions should be introduced to enhance patients’ emotion regulation, reduce impulsivity, and equip them with strategies to manage drug-related cues.
The present study provides empirical evidence to inform the development of effective clinical and behavioral strategies aimed at improving treatment outcomes. Future research should focus on designing and evaluating targeted interventions that reduce impulsivity, alleviate anxiety and depression, and enhance quality of life. Furthermore, longitudinal studies are warranted to determine whether such interventions can decrease concurrent BZD misuse, improve treatment adherence, and ultimately enhance the long-term prognosis of patients receiving MMT.
Limitations
Several limitations of this study should be acknowledged. First, as a cross-sectional study based on self-reported data, the findings may be influenced by recall bias or social desirability bias, particularly for stigmatized behaviors such as illicit substance use. Second, the relatively small sample size may limit the statistical power and generalizability of the results. Future studies with larger samples are needed to confirm these findings. Third, methodological constraints prevented us from examining the potential effects of BZD dosage and specific drug types, both of which may differentially influence clinical outcomes. Further research incorporating these variables is warranted to provide a more comprehensive understanding of BZD use among MMT patients.
Conclusion
Even after adjustment for key comorbidities (including mental, sleep, and chronic somatic disorders), BZD use maintained independent associations with elevated levels of overall, non-planning, and motor impulsivity, as well as with higher anxiety. In contrast, the apparent links between BZD use and worse depression or QOL were attenuated and became statistically non-significant after accounting for relevant confounders. These findings suggest that BZD use was independently associated with higher levels of impulsivity and anxiety after controlling for key comorbidities, whereas the apparent links with depression and QOL are largely confounded by coexisting clinical conditions.
Notably, the causal direction between BZD use and elevated impulsivity/anxiety in MMT patients remains unclear. This association may be driven either by the pharmacological effects of BZDs directly exacerbating these symptoms, or by pre-existing higher levels of impulsivity or anxiety increasing the propensity to initiate or continue BZD use.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval and Informed Consent
This study was approved by the ethics committee of Affiliated Kangning Hospital of Ningbo University in accordance with the Declaration of Helsinki. The ethics trial no. is NBKNYY-2024-LC-12. Informed consent was obtained from all subjects.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Key Research and Development Program of China (No. 2023YFC3304202), the National Natural Science Foundation of China (No. 82471516), the Ningbo Top Medical and Health Research Program (No. 2022030410), and Ningbo Natural Science Foundation Project (No. 2023J029).
Disclosure
The authors declare that they have no conflicts of interest regarding this manuscript.
References
1. Dowell D, Arias E, Kochanek K. et al. Contribution of Opioid-Involved Poisoning to the Change in Life Expectancy in the United States, 2000–2015. JAMA. 2017;318(11):1065–12. doi:10.1001/jama.2017.9308
2. Tsui JI, Burt R, Thiede H, et al. Utilization of Buprenorphine and Methadone among Opioid users who Inject Drugs. Subst Abuse. 2018;39(1):83–88. doi:10.1080/08897077.2017.1363844
3. Nosyk B, Fischer B, Sun H, et al. High levels of opioid analgesic co-prescription among methadone maintenance treatment clients in British Columbia, Canada: results from a population‐level retrospective cohort study. Am J Addiction. 2014;23(3):257–264. doi:10.1111/j.1521-0391.2014.12091.x
4. Wick JY. The History of Benzodiazepines. Consult Pharm. 2013;28(9):538–544. doi:10.4140/TCP.n.2013.538
5. Edinoff AN, Nix CA, Hollier J, et al. Benzodiazepines: uses, Dangers, and Clinical Considerations. Neurol Int. 2021;13(4):594–607. doi:10.3390/neurolint13040059
6. Hashmi AM, Han JY, French-Rosas L, et al. Benzodiazepine Use and Abuse. Psychiat Ann. 2018;48(8):360–365. doi:10.3928/00485713-20180718-02
7. El-Guebaly N, Sareen J, Stein MB. Are There Guidelines for the Responsible Prescription of Benzodiazepines? Can J Psychiat. 2010;55(11):709–714. doi:10.1177/070674371005501104
8. Pierce J, Moser S, Hassett AL, et al. Influence of Abuse History on Concurrent Benzodiazepine and Opioid Use in Chronic Pain Patients. J Pain. 2019;20(4):473–480.
9. Boon M, Van Dorp E, Broens S, et al. Combining opioids and benzodiazepines: effects on mortality and severe adverse respiratory events. Ann Palliat Med. 2020;9(2):542–557. doi:10.21037/apm.2019.12.09
10. Schmitz A. Benzodiazepine use, misuse, and abuse: a review. Ment Health Clin. 2016;6(3):120–126. doi:10.9740/mhc.2016.05.120
11. Jones CM, McAninch JK. Emergency Department Visits and Overdose Deaths From Combined Use of Opioids and Benzodiazepines. Am J Prev Med. 2015;49(4):493–501. doi:10.1016/j.amepre.2015.03.040
12. Gladden RM, O’Donnell J, Mattson CL, et al. Changes in Opioid-Involved Overdose Deaths by Opioid Type and Presence of Benzodiazepines, Cocaine, and Methamphetamine-25 States, July-December 2017 to January-June 2018. MMWR. 2019;68(34):737–744. doi:10.15585/mmwr.mm6834a2
13. Park TW, Larochelle MR, Saitz R, et al. Associations between prescribed benzodiazepines, overdose death and buprenorphine discontinuation among people receiving buprenorphine. Addict. 2020;115(5):924–932. doi:10.1111/add.14886
14. Lintzeris N, Nielsen S. Benzodiazepines, methadone and buprenorphine: interactions and clinical management. Am J Addict. 2010;19(1):59–72. doi:10.1111/j.1521-0391.2009.00007.x
15. Eibl JK, Wilton AS, Franklyn AM, et al. Evaluating the Impact of Prescribed Versus Nonprescribed Benzodiazepine Use in Methadone Maintenance Therapy: results From a Population-based Retrospective Cohort Study. J Addict Med. 2019;13(3):182–187. doi:10.1097/ADM.0000000000000476
16. Cheng Z, Chen G, Dai M, et al. New Psychoactive Substances Abuse Among Patients with Access to Methadone Maintenance Treatment in Jiangsu Province: a Case-Control Study. Chin J Epidemiol. 2018;39(5):625–630.
17. Li J, Li X. Current status of drug use and HIV/AIDS prevention in drug users in China. J Food Drug Anal. 2013;21(4):S37–S41. doi:10.1016/j.jfda.2013.09.031
18. Mo L. Community Medication Maintenance Treatment Clinic Work Manual. Xinjiang, China: Xinjiang People’s Medical Publishing House; 2014.
19. Belin D, Mar AC, Dalley JW, et al. High Impulsivity Predicts the Switch to Compulsive Cocaine-Taking. SCI. 2008;320(5881):1352–1355. doi:10.1126/science.1158136
20. Cunningham KA, Anastasio NC. Serotonin at the nexus of impulsivity and cue reactivity in cocaine addiction. Neuropharmacology. 2014;76:460–478. doi:10.1016/j.neuropharm.2013.06.030
21. Yaghubi M, Zargar F, Akbari H. Comparing Effectiveness of Mindfulness-Based Relapse Prevention with Treatment as Usual on Impulsivity and Relapse for Methadone-Treated Patients: a Randomized Clinical Trial. Addict Health. 2017;9(3):156–165.
22. Luba R, Carpenter KM, Evans S, et al. Impulsivity and Treatment Outcomes in Individuals with Cocaine Use Disorder: examining the Gap between Interest and Adherence. Subst Use Misuse. 2023;58(8):1014–1020. doi:10.1080/10826084.2023.2201851
23. Liu Y, Liu N, Shen W, et al. The Abuse Characteristics of Amphetamine-Type Stimulants in Patients Receiving Methadone Maintenance Treatment and Buprenorphine Maintenance Treatment. Drug Des Dev Ther. 2021;15:2109–2116.
24. Lopez-Torrecillas F, Graña JL, Herruzo C, et al. Impulsivity and Compulsivity Related to Substance Use Disorders. Frontiers in Psychiatry. 2025;16:159989
25. Stevens L, Roeyers H, Dom G, et al. Impulsivity in Cocaine-Dependent Individuals with and without Attention-Deficit/Hyperactivity Disorder. Eur Addict Res. 2015;21(3):131–143. doi:10.1159/000369008
26. Park TW, Sikov J, DellaBitta V, et al. It could potentially be dangerous. but nothing else has seemed to help me: patient and clinician perspectives on benzodiazepine use in opioid agonist treatment. J Subst Abuse Treat. 2021;131:108455. doi:10.1016/j.jsat.2021.108455
27. Patton JH, Stanford MS, Barratt ES. Factor structure of the barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768–774. doi:10.1002/1097-4679(199511)51:6<768::AID-JCLP2270510607>3.0.CO;2-1
28. Zhou L, Xiao S, He X. Reliability and Validity of Chinese Version of Barratt Impulsiveness Scale-11. Chin J Clin Psychol. 2006;14(4):343–344.
29. Haden SC, Shiva A. Trait impulsivity in a forensic inpatient sample: an evaluation of the barratt impulsiveness scale. Behav Sci Law. 2008;26(6):675–690. doi:10.1002/bsl.820
30. Cao X, Feng M, Ge R, et al. Relationship between self-management of patients with anxiety disorders and their anxiety level and quality of life: a cross-sectional study. PLoS One. 2023;18(5):e0284121.
31. Dou X, Lu J, Yu Y, et al. The impact of depression and anxiety on mobile phone addiction and the mediating effect of self-esteem. Sci Rep. 2024;14(1):23004.
32. Yang Y, Ma Y, Zhou R, et al. Internet gaming addiction among children and adolescents with non-suicidal self-Injury: a network perspective. J Affect Disorders Rep. 2023;14:100609. doi:10.1016/j.jadr.2023.100609
33. Dunstan DA, Scott N. Clarification of the cut-off score for Zung’s self-rating depression scale. BMC Psychiatry. 2019;19(1):1–7.
34. Zielińska M, Łuszczki E, Szymańska A, et al. Food addiction and the physical and mental health status of adults with overweight and obesity. Peer J. 2024;12(6):e1763.
35. Xu X, Wang G, Huang X, et al. The current situation and influencing factors of life quality of drug addicts under compulsory rehabilitation. J Prev Med Inf. 2021;37(4):545–552.
36. Overmeyer R, Endrass T. Disentangling associations between impulsivity, compulsivity, and performance monitoring. Psychophysiology. 2024;61(6):e14539.
37. Liu Y, Hong Q, Xie X, et al. Benzodiazepine Use Among Individuals with Opioid Use Disorder: a Narrative Review. Subst Abuse Rehabil. 2025;16:283–291. doi:10.2147/SAR.S550775
38. Malik E, Adelson M, Sason A, et al. Outcome of Patients With High Depressive Symptoms on Admission to Methadone Maintenance Treatment. J Dual Diagn. 2019;15(4):281–290. doi:10.1080/15504263.2019.1656353
39. Lee K, Yen CF. The relationships among withdrawal symptoms and depression in IV injection and non-injection groups in a population of heroin users. Heroin Addict Rel Cl. 2024;26(1):1592–1638.
40. Parikh SV, Quilty LC, Ravitz P, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 Clinical Guidelines for the Management of Adults with Major Depressive Disorder. Can J Psychiatry. 2016;61(9):524–539. doi:10.1177/0706743716659418
41. Schreiber S, Peles E, Adelson M. Association between improvement in depression, reduced benzodiazepine (BDZ) abuse, and increased psychotropic medication use in methadone maintenance treatment (MMT) patients. Drug Alcohol Depend. 2008;92(1):79–85. doi:10.1016/j.drugalcdep.2007.06.016
42. Lim B, Sproule BA, Zahra Z, et al. Understanding the effects of chronic benzodiazepine use in depression: a focus on neuropharmacology. Int Clin Psychopharmacol. 2020;35(5):243–245.
43. Hussein T, Haya HT, Bahjat AS. Quality of Life and its Relation to Self-Esteem for a Sample of Drugs Addicts. Inf Sci Lett. 2023;12(7):2779–2790.
44. Zhou Q, Liu Z, Chen Y. Ethnic Differences in Drug Metabolism and Transport: focus on East Asian Populations. Annu Rev Pharmacol Toxicol. 2022;62:165–187.
45. Ramamoorthy A, Pacanowski M, Bull J, et al. Racial/ethnic differences in drug disposition and response: review of recently approved drugs. Clin Pharmacol Ther. 2015;97(3):263–267. doi:10.1002/cpt.61
46. Pacini M, Maremmani AGI, Maremmani I. Benzodiazepine abuse in a private outpatient treatment setting-psychiatric common grounds and typization of BDZ-bound addictive behavior. Heroin Addict Rel Cl. 2018;20:36–37.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relation Among Anxiety, Depression, Sleep Quality and Health-Related Quality of Life Among Patients with Systemic Lupus Erythematosus: Path Analysis
Chen HJ, Wang H, Qiu LJ, Ling HY, Wu LL, Wang TR, Zhou Y, Xue Y, Ye DQ, Wang B
Patient Preference and Adherence 2022, 16:1351-1358
Published Date: 25 May 2022
A Cross-Sectional Study on the Relationship Between Rosacea Severity and Quality of Life or Psychological State
Yang F, Zhang Q, Song D, Liu X, Wang L, Jiang X
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2807-2816
Published Date: 20 December 2022
Correlation Analysis Between Disease Activity and Anxiety, Depression, Sleep Disturbance, and Quality of Life in Patients with Inflammatory Bowel Disease
Yu R, Liu C, Zhang J, Li J, Tian S, Ding F, Liu Z, Wang T, Liu Z, Jiang C, Shi J, Wu K, Dong W
Nature and Science of Sleep 2023, 15:407-421
Published Date: 26 May 2023
Analyzing Role Overload, Mental Health, and Quality of Life Among Jordanian Female Healthcare Professionals: A Cross-Sectional Study
Alnazly EK, Allari R, Alshareef BE, Abu Al-khair F
International Journal of Women's Health 2023, 15:1917-1930
Published Date: 4 December 2023
Modulatory Effects of XIAOPI Formula on CXCL1 and Selected Outcomes in Triple-Negative Breast Cancer: A Randomized Controlled Clinical Trial
Guo L, Hong SC, Wang X, Wang SQ, Wang N, Wei XQ, Situ HL, Wang ZY
Breast Cancer: Targets and Therapy 2024, 16:289-303
Published Date: 31 May 2024