")
Back to Journals » International Journal of Women's Health » Volume 15
Analyzing Role Overload, Mental Health, and Quality of Life Among Jordanian Female Healthcare Professionals: A Cross-Sectional Study
Authors Alnazly EK , Allari R, Alshareef BE , Abu Al-khair F
Received 17 August 2023
Accepted for publication 28 November 2023
Published 4 December 2023 Volume 2023:15 Pages 1917—1930
DOI https://doi.org/10.2147/IJWH.S435857
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Eman Khamis Alnazly,1 Rabia Allari,1 Basma Eid Alshareef,2 Feda Abu Al-khair2
1Department of Primary Care Nursing, Al-Ahliyya Amman University, Amman, Jordan; 2Psychology Department, Al-Ahliyya Amman University, Amman, Jordan
Correspondence: Eman Khamis Alnazly, Department of Primary Care Nursing, Al-Ahliyya Amman University, Amman, Jordan, Email [email protected]
Purpose: To identify the role overload, mental health distress, and quality of life among Jordanian female healthcare professionals and explore their interrelationships.
Patients and Methods: This cross-sectional correlational research involved 412 female participants (physicians, nurses, and pharmacists) from the government and private sectors in Jordan. The Role Overload, Depression, Anxiety, and Stress Scale-21 (DASS-21) and the World Health Organization Quality of Life-Brief Version were used for data collection. Statistical analyses included descriptive statistics, Pearson correlation, multiple linear regression, multivariate analysis of variance, Tukey’s post hoc test, Spearman rho, and linear regression tests (p=0.05).
Results: Results indicate that 83.2% of participants experienced moderate to high role overload, with 72.9% displaying signs of moderate to extreme depression. Professionals working > 40 hours/week experienced elevated stress levels, while those with chronic illnesses exhibited higher mean scores for depressive symptoms (M= 16.91 vs M= 14.49, p=0.002) and stress (M= 20.55 vs M= 18.57, p=0.033). Professionals attending older individuals reported increased role overload (M= 3.66 vs M= 3.14, p< 0.001), higher stress (M=19.99 vs M=18.14, p=0.027), and lower physical (M=51.79 vs 55.41, p =0.025) and psychological (M=50.04 vs M=53.57, p=0.045) quality of life. Simple regression analysis revealed that role overload significantly predicted stress, depression, and anxiety. Role overload’s impact on depression scores (β = 2.108, t=5.234, p< 0.001), as well as anxiety (β =1.933, t=5.014, p< 0.001), was associated with an inverse correlation with both physical (β =1.671, R2= 3.4, p< 0.001) and psychological (β =1.914, R2= 1.4%, p=0.018) quality of life of healthcare professionals. Mental distress and role overload significantly predicted participants’ physical and psychological quality of life.
Conclusion: This study established a significant association between role overload, quality of life, and psychological health of female healthcare professionals in Jordan, with implications for enhancing their well-being.
Keywords: anxiety, depression, stress, quality of life, medics
Introduction
Role overload occurs when people perceive their energy, time, and competencies as insufficient to meet their role demands. Role overload is linked to various undesirable outcomes including psychological and physical distress.1,2 While engaging in multiple roles potentially affects emotional and psychological well-being, excessive demands from domestic tasks, jobs, and caregiving simultaneously can lead to increased stress, especially if role overload is long-term and builds up over time.2
Researchers have recently highlighted encouraging advancements in women’s workforce participation.3,4 Previous publications have primarily focused on investigating the effects of role overload on diverse outcomes. Role overload negatively impacts quality of life, health, job satisfaction, and employee performance.5–7 By contrast, Lin and Lang have argued that women’s role overload positively affects outcomes8 such as improvements in employee service levels.
Employing a quantitative survey to examine the well-being of mothers working as doctors and nurses in government hospitals, Khokhar et al9 demonstrated that the relationship between work time demands and job satisfaction was partially mediated by the relationship between family involvement and life satisfaction. The findings highlight the work-family conflicts that working women experience and their potential impact on well-being, including life satisfaction. Darolia et al10 surveyed working women in different sectors and reported that family distress was the strongest risk factor and predictor of mental health distress in working women.
The relationship between role overload and presenteeism is characterized by negative physical and physiological effects on working women. Hwang and Jung11 examined the mediating effects of mental and physical health problems on the relationship between work characteristics and presenteeism and identified differences between high and low work-life imbalance groups among women in the social and health sectors. They established that work demands had a significant and negative indirect effect on presenteeism, mediated by fatigue, muscle aches, sleeplessness, and physiological well-being. Physiological well-being was particularly affected in the high work-life imbalance group. Role overload affects job stress, satisfaction, and performance in married women. Mittal and Bhakar6 illustrated that role overload slightly increases job stress and performance and negatively impacts job satisfaction. The authors concluded that, although stress leads to body fatigue, minimal stress resulting from role overload slightly improves performance and decreases job satisfaction.
Zhou et al12 showed that work-family conflict arising from role overload contributes significantly to negative psychological impact among working women. The authors explored the sequential mediating effect of negative affect and perceived stress on the relationship between work-family conflict and mental health. They found negative relationships between the perception of family-to-work and work-to-family conflicts and mental health and noted that perceived stress and negative affect were negatively correlated with mental health.
The World Health Organization13 defines the quality of life as
an individual’s perception of their position in life in the context of the cultural and value systems in which they live and in relation to their goals, expectations, standards and concerns.13
This definition emphasizes that quality of life is subjective and includes positive and negative aspects.14 Researchers have shown that healthcare professionals are affected by role overload, which significantly affects their quality of life and has negative consequences for their mental health.15
Studies have been conducted in Jordan on the impact of role overload on the quality of life and mental health of female healthcare professionals. In a systematic review, researchers have proposed a significant link between role overload and quality of life among Jordanian personnel, highlighting that healthcare professionals in Arab countries such as Jordan experience significant burnout levels because of role overload specific to specialties, type of work, duration, and other personal factors.16
Jordan’s health system comprises a variety of health specialties, with a diverse category of health services provided by 106 public and private sector hospitals throughout the 12 governorates of Jordan. Approximately 44% of professionals in the health sector are females.17 Therefore, females are joining the healthcare workforce in increasing numbers and raising the proportion of females holding multiple roles. Each of these roles commonly places significant time and labor demands on them, causing researchers to hypothesize about a consequent adverse effect on women’s well-being.
Despite its crucial significance and relevance, the literature on the impact of work overload on the mental health and quality of life of women in healthcare remains limited. This study aims to understand the role overload, mental health distress, and quality of life experienced by Jordanian female healthcare professionals. Additionally, it seeks to explore the potential interrelationships among these variables and participants’ demographics.
Materials and Methods
Design
A cross-sectional correlational research design was used to examine the relationships between role overload, participants’ psychological well-being, and quality of life. Data were collected through self-report measures administered to the participants.
E-Survey
The survey was conducted online using Google Forms. The Checklist for Reporting Results of Internet E-Surveys18 was used.
Sampling
Female healthcare professionals were recruited from healthcare settings through convenience sampling. The sample size estimate was derived from the population of female healthcare professionals in Jordan, which is approximately 9700.19 The minimum sample size was determined using Raosoft online sample calculator.20 The results showed that at least 370 participants had a 3% margin of error and a 95% confidence level.
Participants and Settings
The target population comprised female Jordanian healthcare professionals (medical doctors, pharmacists, and nurses). The study was conducted between February 2022 and June 2023. Only those who met the inclusion criteria were eligible to participate in the scheduled survey. To facilitate the completion of the questionnaires, a research assistant contacted a liaison from different health institutions in the capital, Amman and Zarqa, Irbid, Karak, Aqaba, and other health service institutions all over Jordan. Participants included in the study were required to be Jordanian female healthcare professionals currently residing in the country, full-time or part-time employees with a minimum of one year of experience, and willing to participate in the planned study. Women healthcare professionals working only as needed and those who hired household helpers to assist with household chores were excluded from the study.
Study Tools
Sociodemographic Information
The surveys were conducted in English and included participant information such as age, number of children in the household, marital status, household size, caregiving for elderly persons, and level of education attained. Additional data are presented in Table 1.
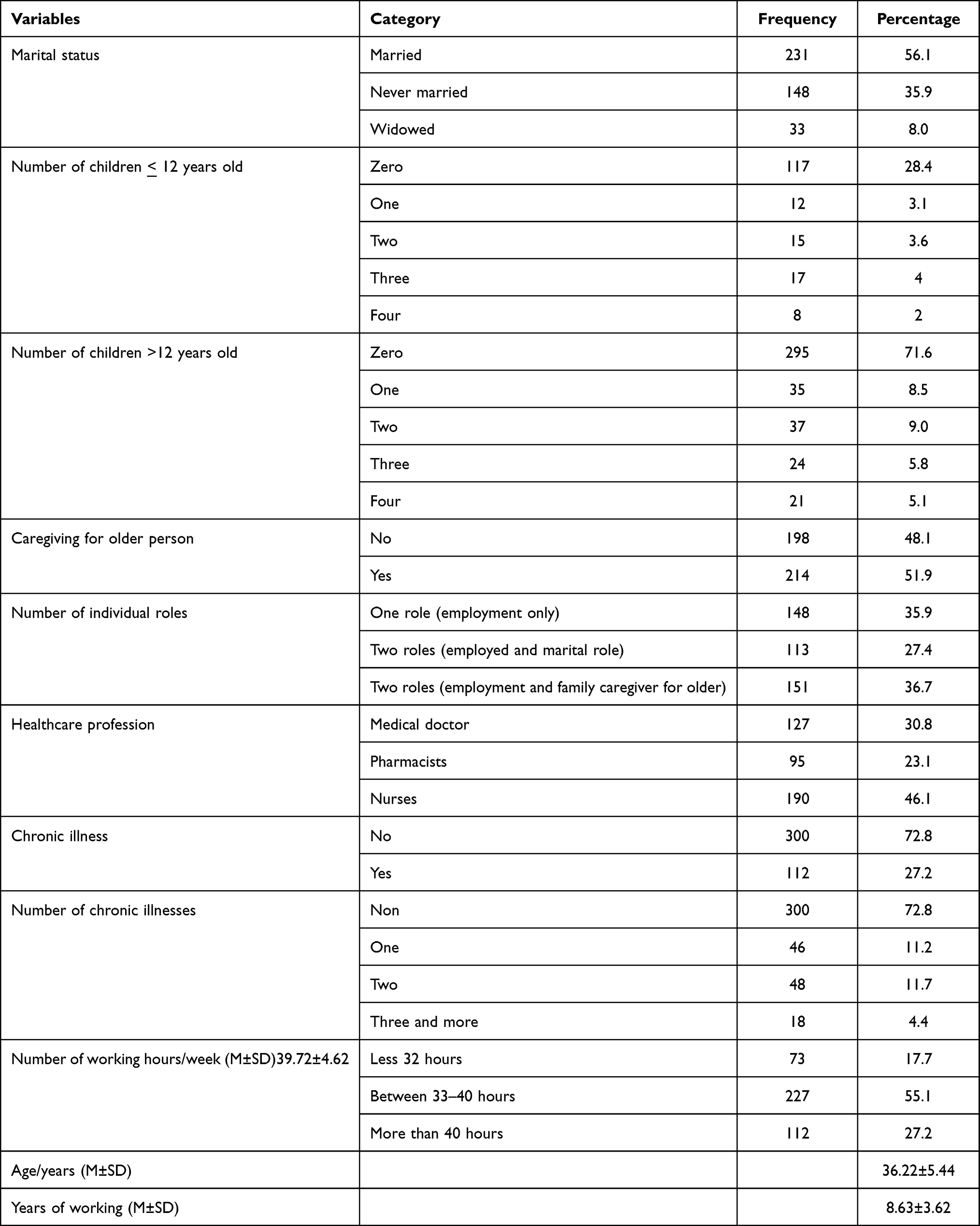 |
Table 1 Female Healthcare Professionals’ Socio-Demographical Characteristics |
Role Overload
Role overload is a three-item scale designed to measure role overload. These questionnaire items were adapted from the tool developed by Schaubroeck et al21 which has been widely used in previous studies. The tool uses a 5-point Likert scale, where one indicates strong disagreement and five indicates strong agreement.22 Higher scores indicate a higher level of role overload. The tool has been validated and is reliable, with a Cronbach’s alpha of 0.732 for role overload.22
DASS-21
Participants’ data on the symptoms of depression, anxiety, and stress over the past week were collected using the DASS-21. Participants were rated on the extent to which they experienced each symptom on a 4-point Likert scale ranging from 0 (never) to 3 (almost always) and involved summing up the scores of each subscale of depression, anxiety, or stress.23 The DASS-21 consists of 21 items divided into three categories: Categories 1, 3, 5, 10, 13, 16, 17, and 21 were used to evaluate depressive symptoms. Questions 2, 4, 7, 9, 15, 19, and 20 in Category 2 evaluated anxiety levels. Finally, items 1, 6, 8, 11, 12, 14, and 18 in Category 3 were used to evaluate the severity of depressive symptoms.24 The DASS-21 assessment tool was valid and reliable with Cronbach’s alpha values of 0.81, 0.89, and 0.78 for depression, anxiety, and stress, respectively.23
World Health Organization Quality of Life-BREF (WHOQOL-BREF)
The WHOQOL-BREF13 questionnaire was used to collect participants’ responses to the quality of life measures. The WHOQOL-BREF 5-point Likert scale evaluates the perceived quality of life of respondents over the past two weeks. It includes items on physical health, psychological well-being, social relationships, and environmental factors. In this study, the items for physical and psychological quality of life measures were included. The sum of participants’ responses on the Likert scale for physical and psychological items was used to assess the quality of life. The items of the WHOQOL-BREF are considered reliable and valid based on Cronbach’s alpha values of 0.759 for the physical domain and 0.742 for the psychological domain.25
Ethical Consideration
This study was approved by the Scientific Research Ethical Committee of the Faculty of Nursing/Al-Ahliyya Amman University (# 1/3/2021-2022) and was performed following the Declaration of Helsinki. When collecting data using questionnaires, pseudocodes were used instead of personal identifiers to ensure the confidentiality and privacy of participants.
Data Collection
Participants were recruited using various social media platforms and informed of the purpose of the study. The link to the cover letter and questionnaires for data collection included in the flyer was sent to the participants during the recruitment process. After consenting electronically, participants were required to complete electronic questionnaires using their smartphones or personal computers.
Data Analyses
Categorical data were expressed as frequencies and percentages, while scale data were expressed as means and standard deviations. Multivariate analysis of variance (MANOVA) was applied to investigate the mean differences in scale variables based on the participants’ categorical demographics. Subsequently, the Tukey post hoc test was used for multiple comparisons following significant F-model outcomes. Correlation between continuous variables was explored using Spearman’s rho and Pearson’s correlation. A simple linear regression test was used to examine the impact of role overload on women healthcare professionals’ mental distress and quality of life. Multiple linear regression was employed to explore the impact of role overload and mental distress on women healthcare professionals’ physical quality of life. SPSS IBM software version 28 was used to analyze the data, and statistical significance was set at a p-value of 0.05.
Results
A total of 412 Jordanian female healthcare professionals participated in this study with a mean age of 36.22 (SD=5.44) years. Most healthcare professionals were nurses (n=190, 46.1%) with a mean professional experience of 8.63 (SD=3.62) years. More than half of the participants were married (n=231, 53.9%), and n=45 (10.9%) had three or more children above the age of 12 years in their families. The percentage of women with one role (employed only) was roughly similar to that of those who had multiple roles (employed, married, and family caregivers for older members) (35.9% vs 36.7%, respectively). However, approximately half of the participants provided care to older adults (n=214, 51.9%) (see Table 1).
Participants’ health profile descriptive statistics revealed that n=112 (27.2%) had chronic diseases, with n=94 (22.9%) having one to two chronic diseases, and n=18 (4.4%) having more than three chronic diseases. Additionally, n=227 (55.1%) participants worked 33–40 hours per week. The means and standard deviations of the participants’ weekly working hours, age, and years of working experience are presented in Table 1.
The total score for each scale was computed and the results, presented in Table 2, indicate that most participants experienced high role overload (n=188, 45.6%). Most participants exhibited moderate depressive symptoms (n=119, 28.9%), while a significant portion displayed extremely severe anxiety levels (n=127, 30.8). MANOVA was employed to test group mean differences based on participants’ demographics (Table 3).
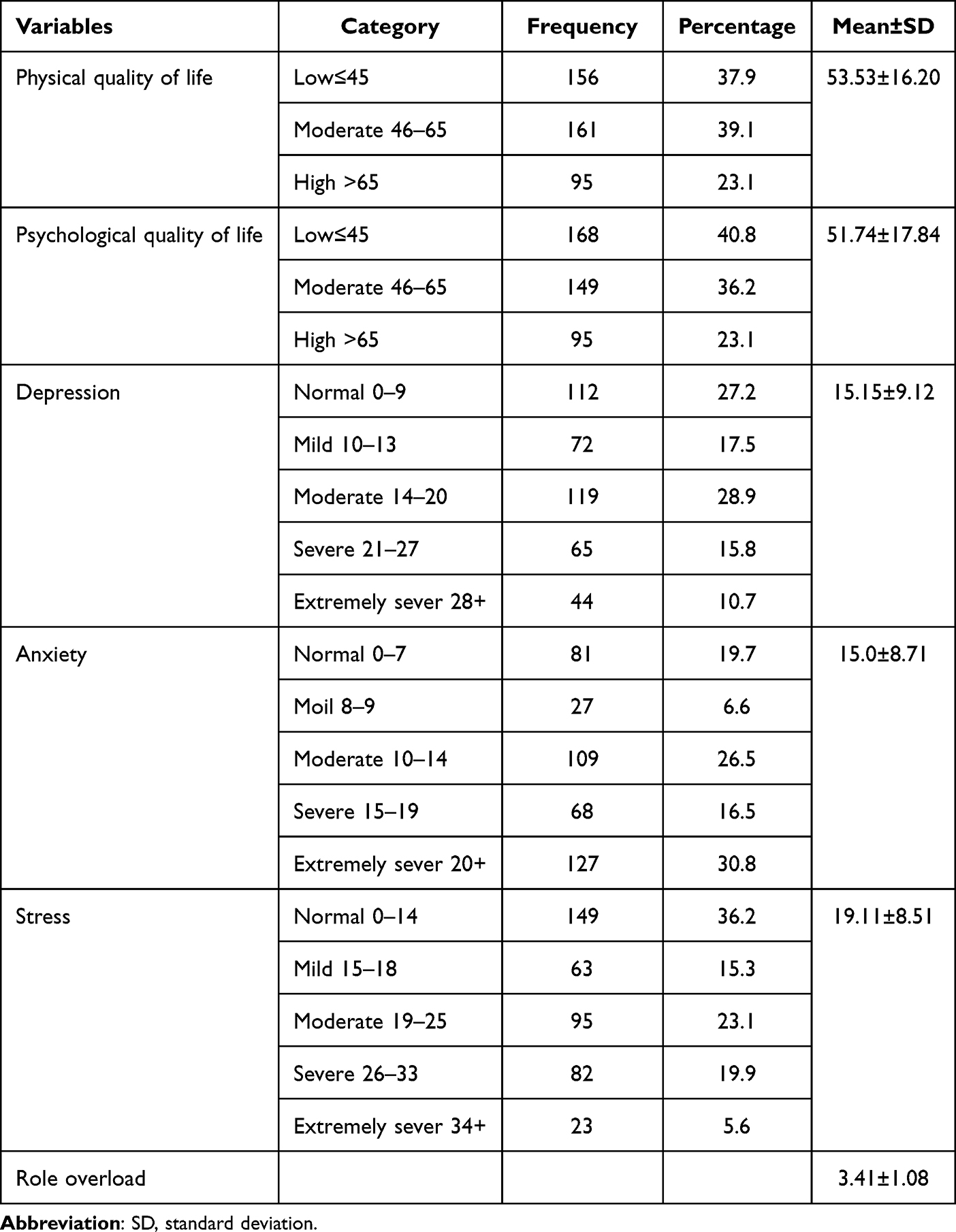 |
Table 2 Summary Statistics for Participants’ Scores of Role Overload, Depression, Anxiety, and Physical and Psychological Quality of Life |
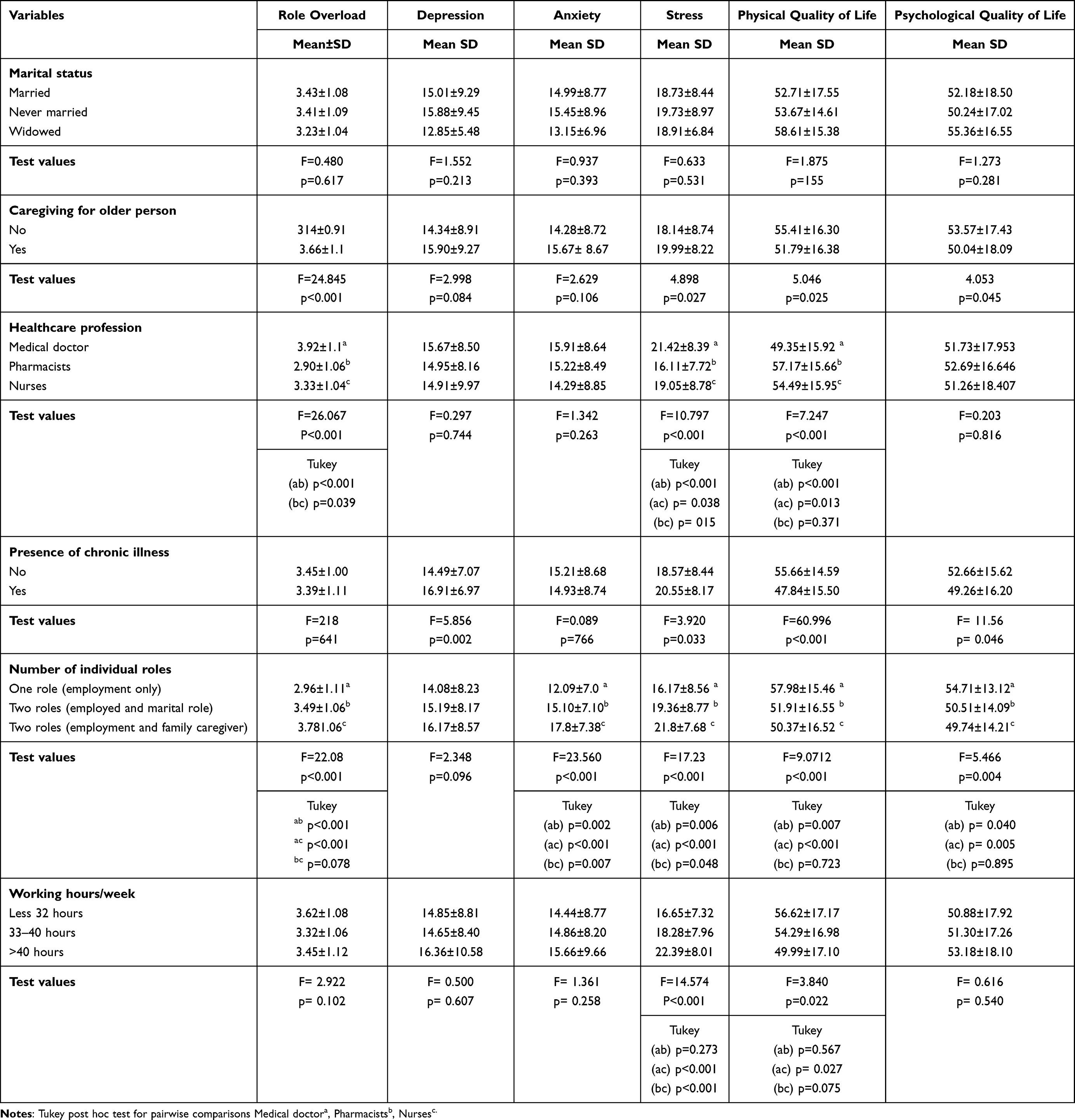 |
Table 3 MANOVA Output for Role Overload, Mental Distress, and Quality of Life Based on Their Demographic Characteristics |
Physicians exhibited significantly higher role overload mean scores (M=3.92) than pharmacists (M=2.90) and nurses (M=3.33) (p<0.001). Additionally, nurses had significantly higher overload mean scores than pharmacists (p=0.003). Similarly, physicians had significantly higher stress mean scores (M=21.42) than pharmacists (M=16.11) and nurses (M=19.05) (p<0.05). Furthermore, nurses had significantly higher stress mean scores than pharmacists (p=0.015). Additionally, physicians reported significantly lower mean scores for physical quality of life (M=49.35) than pharmacists (M=57.17) and nurses (M=54.49) (p<0.05). However, pharmacists’ and nurses’ mean scores were not significantly different for physical quality of life mean scores (p=0.371). Notably, no significant mean differences were found in depression, anxiety, and psychological quality of life between physicians, pharmacists, and nurses (p >0.05).
Participants engaged in two (M=3.49) or more roles (M=3.78) had significantly higher role overload mean scores than those with a single role (M=2.96) (p<0.001). Anxiety levels were significantly higher in individuals performing two (M=15.10) and more than two roles (M= 17.8) compared to individuals with one role (M=12.09) (p<0.01). Similarly, the stress score was significantly higher among participants performing two (M=19.36) or more than two roles (M=21.8) compared to the one-role group (M=16.17) (p<0.01). Additionally, participants with two (M=51.91) or more than two roles (M=50.37) reported a significantly lower physical quality of life than individuals with one role (M=57.98) (p<0.01) (see Table 3).
Participants working >40 hours/week experienced significantly higher stress mean scores (M=22.39) than those working 33–40 hours/week (M=18.28) and those working less than 32 hours/week (M=16.65) (p<0.001). Furthermore, participants working >40 hours/week exhibited significantly lower physical quality of life compared to those working <32 hours/week (p=0.027). Role overload, depression, anxiety, and psychological quality of life did not yield significant results (p>0.05) among the three categories.
The presence of chronic illnesses had significantly higher mean scores for depressive symptoms (M=16.91, compared to M=14.49, p=0.002), and stress (M=20.55, compared to M=18.57, p=0.033) than those without chronic illnesses. Furthermore, participants with chronic illnesses had significantly lower physical and psychological quality of life than those without chronic illnesses (p<0.05). However, the mean difference in the anxiety scale and role overload did not differ significantly between participants with and without chronic illnesses (p>0.05).
Women healthcare professionals who provide care to older persons reported significantly higher mean scores for role overload (M=3.66, compared to M=3.14, p<0.001), stress (M=19.99, compared to M=18.14, p=0.027), lower physical quality of life (M=51.79, compared to M=55.41, p=0.025), and lower psychological quality of life (M=50.04, compared to M=53.57, p=0.045) than those not caring for older persons. However, the mean anxiety scores were not significantly different between participants who provided care to older persons and those who did not (p>0.05). Additionally, role overload, depression, anxiety, and physical and psychological quality of life were not significantly different for participants’ marital status. Spearman correlation (rs) demonstrated that the number of children older than 12 years was significantly and positively correlated with role overload (rs= 0.258), anxiety (rs=0.234), and stress (rs=0.316) (p<0.001). However, significant negative correlations existed between the number of children aged above 12 years and physical (rs=−.227, p=0.008) and psychological (rs=−.285, p<0.001) quality of life. Pearson correlation (rp) indicated that healthcare professional age was significantly and negatively correlated with physical (rp=−256) and psychological (rp=−.293) (p <0.001) quality of life. Years of working did not show any significant correlation with role overload, mental distress, and quality of life (p> 0.05) (Table 4).
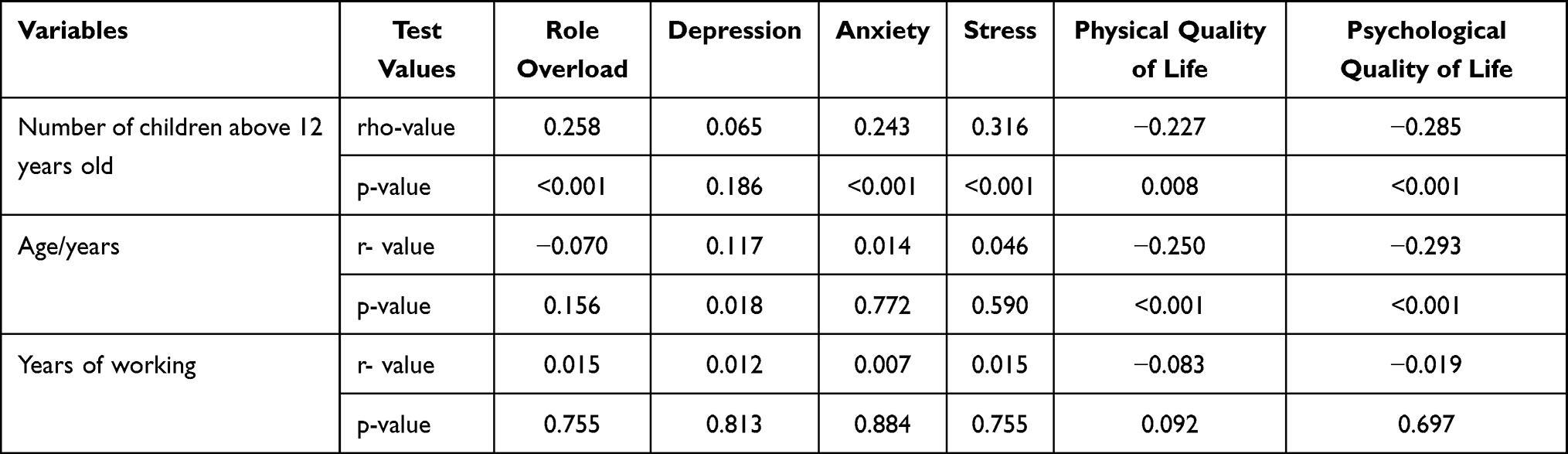 |
Table 4 Correlation Coefficients for Selected Variables |
Role overload was used as a predictor of mental distress and quality of life in simple linear regression models (Table 5). The regression results indicated that role overload was a significant predictor of stress, depression, and anxiety. A one-unit increase in participants’ role overload was associated with a corresponding increase of 2.3 units in stress (t=6.197, p<0.001), and the model explained 8.6% of the variations. The impact of role overload on depression score was the second highest with (β=2.108, t=5.234, p<0.001), indicating that a unit increase in role overload produces a corresponding increase of 2.108 units in depression. Similarly, the regression results indicated a direct positive relationship between role overload and anxiety (β=1.933, t=5.014, p<0.001), with a 5.8% variance explained by the model. By contrast, role overload demonstrated a significant inverse correlation with healthcare professionals’ physical (β=1.671, R2=3.4, p<0.001) and psychological (β=1.914, R2=1.4%, p=0.018) quality of life (see Table 5). The inverse correlation indicated that a unit increase in role overload resulted in a corresponding decrease in physical and psychological quality of life.
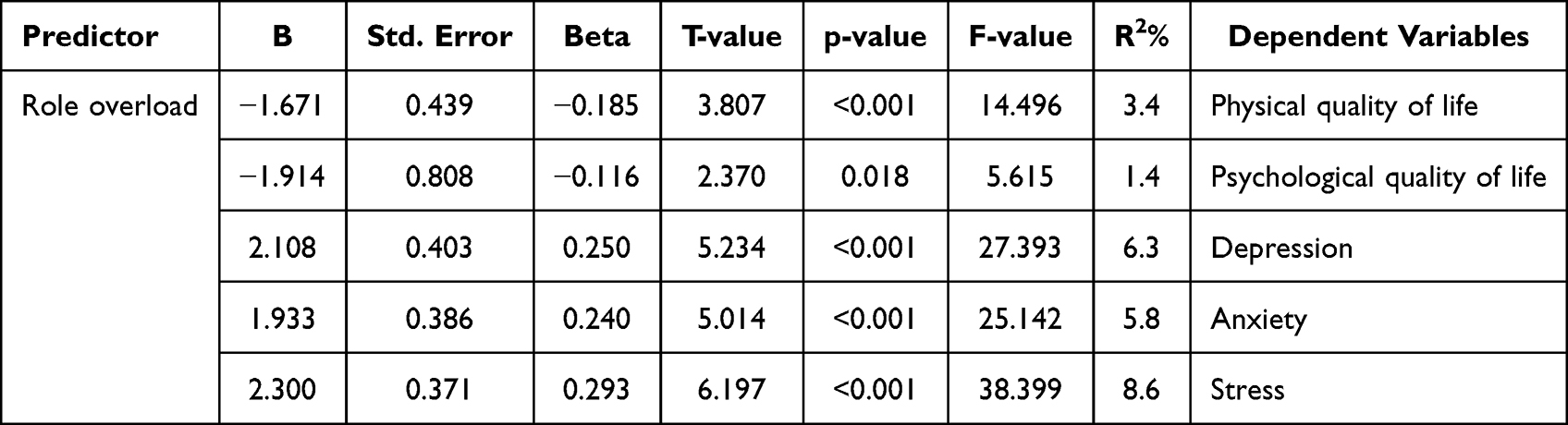 |
Table 5 Regression Results for the Impact of Role Overload on Healthcare Professionals’ Quality of Life and Mental Distress |
Multiple linear regression was used to evaluate the combined impact of participants’ role overload and mental distress on their quality of life. The overall ANOVA model was statistically significant (F=30.379, p<0.001 Adj-R2=22.2%), indicating that participants’ mental distress and role overload were significant predictors of physical quality of life. Generally, role overload and mental distress are negatively correlated with physical quality of life. However, the most predictive variable was anxiety with the lowest regression coefficient (β=−0.793, t=4.306, p<0.001). The second most predictive variable was depression (β=−0.465, t=3.691, p<0.001). Similarly, the participants’ physical quality of life was expected to decrease by −0.435 and −0.266 units for every additional unit increase in stress and role overload, respectively (p<0.05) (Table 6).
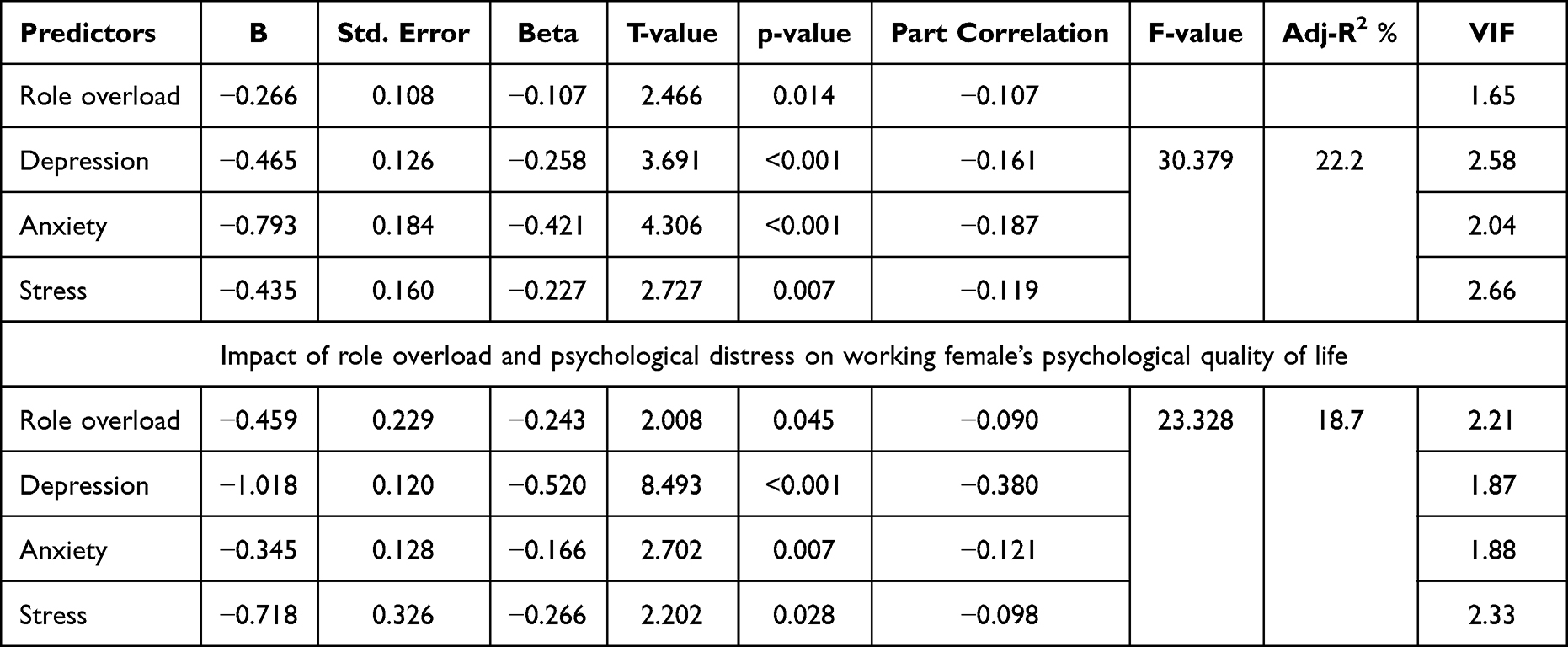 |
Table 6 Impact of Role Overload and Psychological Distress on Working Female’s Physical Quality of Life |
Similarly, role overload and mental distress were significant predictors of participants’ psychological quality of life (F=23.328, p<0.001, R2=18.7%). Depression was the most significant predictor of psychological quality of life (β=−1.018, t=8.493, p<0.001). Lastly, role overload was the weakest predictor of healthcare professionals’ psychological quality of life (β=−0.459, t=2.008, p=0.045) (Table 6), followed by anxiety (β=−0.345, t=2.702, p=0.007). The regression results indicated that a unit increase in depression produced a corresponding decrease of 1.018 units in participants’ psychological quality of life. Moreover, stress was associated with a reduction in the psychological quality of life score (β=−0.718, t=2.202, p=0.028) (Table 6).
Discussion
The overall findings of this cross-sectional study indicate that factors, including the type of health profession, number of roles, working hours, marital status, and caregiving for children/older adults, significantly impacts role overload, which in turn affects healthcare professionals’ mental well-being and quality of life. The descriptive results show that most participants experience moderate to high role overload, and the majority show signs of depression, ranging from moderate to extreme. Additionally, nearly half of the participants display severe or extremely severe anxiety symptoms and have a low quality of life. The results imply that a significant number of Jordanian women among healthcare professionals experience a high role overload that affects their psychological health through depression, stress, and anxiety, and lowers their quality of life. Similarly, a cross-sectional survey by Ugwu26 showed that role overload leads to chronic fatigue and has a negative psychological impact, making healthcare employees poorly engaged. Ugwu26 also showed that role overload was significantly associated with work engagement, implying that a unit increase in role overload led to a 0.45 unit decrease in work engagement. This finding suggests that role overload increases work demands either at home or at work, which exceeds a person’s ability and is likely to cause mental distress.
The ANOVA coupled with Tukey’s post hoc test for pairwise comparisons indicates that healthcare professionals working >40 hours/week experience significantly higher stress levels. Additionally, those with chronic illnesses exhibit higher mean scores for depressive symptoms and stress than those without chronic illnesses. Similarly, female healthcare professionals providing care to older people reported higher mean scores for role overload and stress and lower physical and psychological quality of life than those who do not provide such care. The findings suggest that the number of working hours, chronic illness, and caring for older persons impact women’s healthcare professionals’ role overload, mental health, and physical and psychological quality of life. The findings are also consistent with Alobaid et al’s3 systematic review of the factors and circumstances that affect female healthcare professionals’ lives and workplace environments. Alobaid et al3 showed that a lack of balance between the work and family roles of female health providers results in overload, which affects their quality of life. A cross-sectional study by Oliveira et al27 supports the findings by demonstrating that work overload impacts physical quality of life (M= 2.99 ± 0.92, p = 0.04), resulting in poor job satisfaction and work relationships. The findings of a recent study by Namdari et al28 revealed that nurses often experience strain in their family roles, which could negatively impact their professional performance. The results imply that family work role overload could significantly reduce nurses’ mental ability to provide care, impair professional communication, and lead to low morale in providing care, ultimately negatively influencing their overall professional performance. Namdari et al’s28 findings highlight the importance of addressing family role strain in nursing to minimize role overload and provide the best possible care to patients. The findings of this study highlight that role overload, resulting from multiple roles, has a potential impact on well-being, including mental health distress and quality of life. A lack of strategies to enhance the balance between multiple tasks to reduce the consequences of role overload will likely increase mental distress and lower their quality of life.
Spearman’s rho correlation test revealed a negative correlation between role overload, mental distress, and quality of life. The results imply that increased work stress or overload exacerbated by factors including the number of working hours, chronic illness, or caring for vulnerable persons results in poor quality of life and a rise in mental distress. The findings are also consistent with Babapour et al’s29 outcomes of a cross-sectional survey that investigated the association between work stress and nurses’ quality of life and behaviors. Babapour et al29 indicated a statistically significant and inverse correlation between work stress and nurses’ quality of life and behavior (r = −0.44, p < 0.001, medium effect; r = −0.26, p < 0.001, small effect). Similarly, in a cross-sectional survey, Rotenstein et al30 argued that burnout was one of the main psychological effects of role overload, leading to the intent to leave work. Rotenstein et al’s30 findings showed that work overload significantly correlated with burnout (adjusted risk ratio [ARR] 2.21 to 2.90) and intent to leave (ARR 1.73 to 2.10) across all clinical roles. Women who experience work overload that requires more effort are more likely to experience higher levels of mental distress. Professional women who experience role overload because of an increased workload experience more negative effects on their lives. Women should seek other resources in the workplace or home to reduce mental distress and improve their quality of life.
In this cross-sectional study, the results of a simple linear regression revealed that a unit increase in role overload increased participants’ stress levels (B=2.3 units, t=6.197, p<0.001), depression scores (B=2.108, t=5.234, p<0.001), and anxiety (B=1.933, t=5.014, p<0.001). The regression test also revealed an inverse relationship between role overload and quality of life; additional role overload decreased quality of life. The regression test results imply that increased role overload elevate the risk of mental distress and illnesses among professionals and lower their quality of life. These results align with the findings of Zhang et al,31 who investigated the effects of role overload on nurses’ performance. Zhang et al31 revealed that role overload results in poor work performance due to adverse impacts, such as stress and exhaustion, which affect the quality of care delivered. Tang and Vandenberghe1 also observed a significant association between role overload and psychological strain that interferes with work performance.
Strengths and Limitations
This study considered the impact of work overload on women’s mental health and quality of life in the healthcare sector, which has been largely ignored despite its crucial significance and relevance.16 Another strength is that the study’s findings revealed that role overload affected women healthcare professionals’ quality of life and psychological health. Therefore, this cross-sectional study produced significant findings that provide insights into improving the physical and mental health of women healthcare professionals.
However, this cross-sectional study had several limitations. Using a cross-sectional study approach provided restrictions in accounting for the measurement of changing variables over time, as the investigation was limited to a specific time. Additionally, the use of electronic self-administered questionnaires provided potential common biases such as social desirability and response bias, which could affect the reliability and validity of the findings. Additionally, the study is potentially gender biased because the participants were derived from the population of women healthcare professionals in Jordan; as such, caution should be taken when generalizing the results. Consequently, future research should be conducted in diverse settings using both male and female participants to improve the generalizability of the results.
Implications
Practice Implications
Administrative management in Jordan should recognize the effects of role overload and reduce the workload of women healthcare professionals to protect their mental health and improve their quality of life to enhance performance. Administrators should develop strategies such as creating teams to increase women healthcare professionals’ control over their workload. The findings can help design follow-up therapy programs to help Jordanian female healthcare professionals cope with personal and professional workloads and provide quality care to patients.
Theoretical Implications
This study contributes to the literature in three ways. First, although current medical research has identified some factors influencing the mental health and quality of life of women healthcare professionals, limited scholarly attention has been paid to role and personal stressors, particularly role overload. Second, this study expands the scope of role overload by examining other factors that influence its level, including socioeconomic characteristics, family responsibilities, existing interrelationships, and health status. This approach is crucial in determining the association between these factors and role overload for practical measures. Third, this study provides a definitive answer to the research question of whether role overload affects the mental health and quality of life of women healthcare professionals in Jordan.
Recommendations
Four recommendations were made based on the significant findings of this cross-sectional study. First, future studies should use longitudinal or experimental research to determine cause-and-effect relationships between the variables of interest over time, as the cross-sectional approach is limited to examining descriptive associations at a given point in time. A longitudinal research approach will also help overcome some of the biases of cross-sectional studies, such as non-responsive bias. Second, future research should employ multiple data sources because self-reported questionnaires constitute a potential bias. Third, to improve the generalizability of the findings, future research could involve more diverse populations from other health settings as this study was limited to female participants from Jordan. Finally, future research should incorporate other factors that influence the psychological well-being and quality of life of women healthcare professionals.
Conclusion
This study revealed a significant correlation between the level of role overload experienced by women healthcare professionals in Jordan, their mental health, and overall quality of life. In particular, the findings indicate that excessive role demands negatively impact the psychological well-being of women healthcare professionals, consequently lowering their quality of life. These findings have significant implications for the theoretical understanding of the challenges faced by women healthcare professionals in Jordan and the development of future health education programs that can effectively address these issues.
Data Sharing Statement
Data will be available from the corresponding author upon request.
Acknowledgments
We would like to express our thanks to the professional women who participated in the study for their time and patience. Without their participation, this project would not have been possible.
Author Contributions
All authors made a significant contribution to the work reported either in the conception, study design, execution, acquisition of data, analysis, and interpretation or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This project is funded by Al-Ahliyya Amman University, Amman, Jordan.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Tang WG, Vandenberghe C. Role overload and work performance: the role of psychological strain and leader-member exchange. Front Psychol. 2021;12:691207. doi:10.3389/fpsyg.2021.691207
2. Chen F, Lin Z, Bao L, Zimmer Z, Gultiano S, Borja BJ. Time-use profiles, Chronic role overload, and women’s body weight trajectories from middle to later life in the Philippines. J Health Soc Behav. 2019;60(1):119–136. doi:10.1177/0022146519827612
3. Alobaid AM, Gosling CM, Khasawneh E, McKenna L, Williams B. Challenges faced by female healthcare professionals in the workforce: a scoping review. J Multidiscip Healthc. 2020;13:681–691. doi:10.2147/JMDH.S254922
4. Mousa M, Boyle J, Skouteris H, et al. Advancing women in healthcare leadership: a systematic review and meta-synthesis of multi-sector evidence on organisational interventions. EClinicalmedicine. 2021;39:101084. doi:10.1016/j.eclinm.2021.101084
5. Iroegbu MN. Effect of organizational role conflict and job satisfaction on performance in the Nigerian customs service: an empirical examination. Int J Appl Psychol. 2013;3:174–181. doi:10.5923/j.ijap.20130306.05
6. Mittal M, Bhakar SS. Examining the impact of role overload on job stress, job satisfaction and job performance-a study among married working women in banking sector. Int J Manag Stud. 2018;V(2(7)):1–11. doi:10.18843/ijms/v5i2(7)/01
7. Purkait S. Impact of occupational stress on quality work life among employees in banking sector: a study in West Bengal region. Int J Adv Res. 2016;4(7):1215–1222. doi:10.21474/IJAR01/1026
8. Lin M, Ling Q. Is role stress always harmful? Differentiating role overload and role ambiguity in the challenge-hindrance stressors framework. Tourism Manag. 2018;68:355–366. doi:10.1016/j.tourman.2018.04.007
9. Khokhar AM, Nas Z, Zia-Ur-Rehman M. Working mother’s dilemma in Pakistan: analyzing their battle with work, family demands, and well-being. Sarhad J Manag Sci. 2020;6:259–278.
10. Darolia S, Rahi S, Sharma M. Work-family conflict and psychological distress as predictors of mental health among working women. Int J Soc Sci Review. 2019;7:805–808.
11. Hwang JH, Jung HS. The effects of work characteristics related to work-life imbalance on presenteeism among female workers in the health and social work sectors: mediation analysis of psychological and physical health problems. Int J Environ Res Public Health. 2021;18(12):6218. doi:10.3390/ijerph18126218
12. Zhou S, Da S, Guo H, Zhang X. Work-family conflict and mental health among female employees: a sequential mediation model via negative affect and perceived stress. Front Psychol. 2018;9:544. doi:10.3389/fpsyg.2018.00544
13. World Health Organization. Programme on mental health: WHOQOL user manual, 2012 revision; 2009 Gender and women’s mental health; 1998. Available from: https://apps.who.int/iris/handle/10665/77932.
14. Wong FY, Yang L, Yuen JW, Chang KK, Wong FK. Assessing the quality of life using WHOQOL-BREF: a cross-sectional study on the association between quality of life, neighborhood environmental satisfaction, and the mediating effect of health-related behaviors. BioMed Cent Public Health. 2018;18:1–14.
15. Chemali Z, Ezzeddine FL, Gelaye B, et al. Burnout among healthcare providers in the complex environment of the Middle East: a systematic review. BMC Public Health. 2019;19(1):1337. doi:10.1186/s12889-019-7713-1
16. Elbarazi I, Loney T, Yousef S, Elias A. Prevalence of and factors associated with burnout among health care professionals in Arab countries: a systematic review. BMC Health Serv Res. 2017;17(1):491. doi:10.1186/s12913-017-2319-8
17. High Health Council, Hashemite Kingdom of Jordan. The National Strategy for Health Sector in Jordan 2015–2019; 2015. Available from: http://www.hhc.gov.jo/uploadedimages/The%20National%20Strategy%20for%20Health%20Sector%20in%20Jordan%202015-2019.pdf.
18. Eysenbach G. Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res. 2004;6:e34. doi:10.2196/jmir.6.3.e34
19. Department of Statistics. Women statistics; 2021. Available from: http://dosweb.dos.gov.jo/population/woman-statistics/.
20. Raosoft. Incorporation: Raosoft sample size online calculator. Internet. c2004. Available from: http://www.raosoft.com/samplesize.html.
21. Schaubroeck J, Cotton JL, Jennings KR. Antecedents and consequences of role stress: a covariance structure analysis. J Organiz Behav. 1989;10(1):35–58. doi:10.1002/job.4030100104
22. Huang Q, Wang Y, Yuan K, Liu H. How role overload affects physical and psychological health of low-ranking government employees at different ages: the mediating role of burnout. Saf Health Work. 2022;13(2):207–212. doi:10.1016/j.shaw.2022.02.002
23. Marijanović I, Kraljević M, Buhovac T, et al. Use of the Depression, Anxiety and Stress Scale (DASS-21) questionnaire to assess levels of depression, anxiety, and stress in healthcare and administrative staff in 5 oncology institutions in Bosnia and Herzegovina during the 2020 COVID-19 pandemic. Med Sci Monit. 2021;27:930812. doi:10.12659/MSM.930812
24. Ali AM, Green J. Factor structure of the depression anxiety stress Scale-21 (DASS-21): unidimensionality of the Arabic version among Egyptian drug users. Subst Abuse Treat Prev Policy. 2019;14(1):40. doi:10.1186/s13011-019-0226-1
25. Alnabih AIA, Aldabbour B, Mat Tahir MFBM, Khamis NK. Quality of life and its demographic predictors among workers at a plastic factory in Malaysia: a cross-sectional study. Int J Public Health Sci. 2022;11:106–112. doi:10.11591/ijphs.v11i1.21275
26. Ugwu CC. Role overload and work engagement among nurses: moderating role of resilience. Sapientia Glob J Arts Humanit Dev Stud. 2022;5:221–235.
27. Oliveira JFD, Santos AMD, Primo LS, et al. Job satisfaction and work overload among mental health nurses in the south of Brazil. Cien Saude Colet. 2019;24(7):2593–2599. doi:10.1590/1413-81232018247.20252017
28. Namdari S, Nasiri A, Nakhaee S, Taheri F. Exploring the effects of nurses’ family-work conflict on patient care quality: a qualitative study. Mod Care J. 2019;16(1):e86130. doi:10.5812/modernc.86130
29. Babapour AR, Gahassab-Mozaffari N, Fathnezhad-Kazemi A. Nurses’ job stress and its impact on quality of life and caring behaviors: a cross-sectional study. BMC Nurs. 2022;21(1):75. doi:10.1186/s12912-022-00852-y
30. Rotenstein LS, Brown R, Sinsky C, Linzer M. The association of work overload with burnout and intent to leave the job across the healthcare workforce during COVID-19. J Gen Intern Med. 2023;38(8):1920–1927. doi:10.1007/s11606-023-08153-z
31. Zhang N, Xu D, Li J, Xu Z. Effects of role overload, work engagement and perceived organisational support on nurses’ job performance during the COVID-19 pandemic. J Nurs Manag. 2022;30(4):901–912. doi:10.1111/jonm.13598
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.