Back to Journals » Patient Preference and Adherence » Volume 20
Barriers to Adherence to Remote Pelvic Floor Muscle Training Among Postpartum Women: A Qualitative Study Guided by the COM-B Model
Authors Zhou D, Ni X, Ding M, Shi H
Received 28 March 2026
Accepted for publication 15 May 2026
Published 22 May 2026 Volume 2026:20 612714
DOI https://doi.org/10.2147/PPA.S612714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ramón Morillo-Verdugo
Dan Zhou, Xiao Ni, Ming Ding, Huangfei Shi
Department of Obstetrics and Gynecology, Wuxi Ninth People’s Hospital Affiliated to Soochow University, Wuxi, Jiangsu, 214000, People’s Republic of China
Correspondence: Dan Zhou, Email [email protected]
Background: Pelvic floor muscle training (PFMT) is recognized as the first-line conservative intervention for postpartum pelvic floor rehabilitation. Remote pelvic floor muscle training, defined as a training modality conducted at home via mobile applications, online platforms, teleconsultation, or application-based reminders, without real-time on-site supervision, has expanded the accessibility of rehabilitation services; however, patient adherence remains suboptimal. Elucidating the barriers to adherence is critical for developing effective and well-accepted intervention strategies. This study, grounded in the Capability, Opportunity, Motivation–Behavior (COM-B) model, investigated various barriers to adherence among postpartum women engaged in remote pelvic floor muscle training.
Methods: A qualitative descriptive study was conducted at a pelvic floor rehabilitation clinic in Wuxi, China, between November and December 2025. Fifteen postpartum women aged 27– 36 years (6 weeks to 6 months postpartum) participated. The sample included primiparous and multiparous women, both vaginal and cesarean deliveries, and mixed symptomatic and asymptomatic participants. All had prior experience with at least one remote PFMT modality within the preceding six months. Semi-structured interviews were analyzed using directed content analysis guided by the COM-B model. Thematic saturation was reached after 12 interviews and confirmed with 3 additional interviews. Analytical rigor was ensured through independent double-coding of all transcripts, inductive code allowance, audit trail, and member checking.
Results: Eleven barriers were identified across the three COM‑B domains. Capability barriers comprised knowledge deficits, skill deficits, and physical discomfort. Opportunity barriers comprised caregiving burden, limited professional support, inadequate family support, and technological constraints. Motivation barriers comprised low perceived urgency, lack of perceived benefits, low self‑efficacy, and habit formation difficulties. Barriers did not operate in isolation: inadequate knowledge reduced perceived urgency, limited professional feedback amplified skill uncertainty and lowered self‑efficacy, caregiving burden simultaneously restricted opportunity and depleted physical and cognitive resources, and technological friction converted convenience into a motivational cost.
Conclusion: Postpartum women face multiple, interrelated barriers to remote PFMT adherence spanning all COM‑B domains. A blended care model that combines initial in‑person technique verification, low‑friction digital platforms with structured cues and progress tracking, periodic professional tele‑follow‑up, and family engagement components may more effectively address these barriers than standalone self‑guided remote delivery. These findings provide theory‑based, actionable guidance for designing hybrid postpartum rehabilitation services.
Keywords: postpartum women, pelvic floor muscle training, remote rehabilitation, adherence, COM-B model, qualitative study
Introduction
Pelvic floor dysfunction (PFD) encompasses urinary incontinence, pelvic organ prolapse, fecal incontinence, sexual dysfunction, and chronic pelvic pain, all of which may substantially impair women’s quality of life and psychosocial well-being.1 Pregnancy and vaginal childbirth are recognized as major risk factors for damage to the pelvic floor muscles, fascia, and pudendal nerves, thereby increasing the likelihood of postpartum pelvic floor symptoms and long-term dysfunction.2 A 2025 systematic review reported a pooled PFD prevalence of 23% to 67% in postpartum women,3 and among Chinese women who underwent vaginal delivery, a detection rate of 42.90% was identified at the 42-day postpartum follow-up.4 Given the considerable prevalence and health burden of PFD, early postpartum prevention and rehabilitation are critical components of women’s healthcare.
Pelvic floor muscle training (PFMT), which involves repeated voluntary contraction and relaxation of the pelvic floor muscles to enhance strength, endurance, and neuromuscular coordination, has been recommended as the first-line conservative treatment for the prevention and management of pelvic floor disorders.5 Evidence confirms that correct and consistent performance of PFMT can increase pelvic floor muscle strength, reduce symptom severity, and improve health-related quality of life.6,7 In postpartum women, PFMT also facilitates the recovery of pelvic floor function and reduces the risk of long-term dysfunction.8 However, these benefits are highly dependent on long-term adherence to prescribed training regimens. In practice, many postpartum women encounter difficulties in initiating and sustaining PFMT over an extended period, which directly limits the clinical effectiveness of rehabilitation.9,10 This gap between efficacy and actual adherence represents a critical implementation challenge, necessitating a systematic investigation of the barriers perceived by women.
With the rapid expansion of digital health and telemedicine, remote PFMT has become an increasingly feasible and attractive mode of postpartum rehabilitation.11,12 In this study, “remote PFMT” is defined as home-based training delivered via digital platforms, including mobile applications, asynchronous instructional videos, automated reminders, and remote teleconsultations, without concurrent in-person professional supervision.13 Unlike traditional face-to-face PFMT, which provides immediate tactile and verbal feedback, physical demonstration, and direct accountability through scheduled appointments, remote PFMT shifts the burden of technique self-assessment, motivation maintenance, and exercise scheduling almost entirely onto the postpartum woman in her home environment.14 This fundamental difference may simultaneously improve accessibility for women facing infant care demands, limited mobility, and geographic barriers to clinic attendance,15 while also introducing or amplifying barriers specific to unsupervised, digitally mediated rehabilitation. Nevertheless, adherence remains a major challenge in remote PFMT.16
Adherence to remote PFMT is a complex behavior shaped by multiple interrelated factors, including women’s knowledge, practical skills, beliefs about rehabilitation, emotional state, technological literacy, social support, and the broader care environment.17 However, the existing literature has largely focused on either the clinical efficacy of PFMT in controlled settings or the usability of individual digital health tools.18–20 What remains insufficiently understood is the in-depth, theory-grounded qualitative evidence on the specific barriers postpartum women face in maintaining adherence to PFMT when delivered remotely.
The Capability, Opportunity, Motivation-Behavior (COM-B) model offers a robust behavioral framework to dissect these adherence challenges (Figure 1).21 The COM-B model has been increasingly used in health behavior research to identify barriers and facilitators and to guide the development of targeted interventions.22–24 In the context of remote PFMT, capability encompasses the physical recovery and psychological knowledge required to correctly isolate and train pelvic floor muscles without direct supervision; opportunity reflects the home environment, including technological infrastructure, caregiving demands, and professional/family support; and motivation involves both reflective processes and automatic processes. Applying this framework to remote PFMT may help systematically elucidate why postpartum women struggle to maintain adherence.
 |
Figure 1 The COM-B conceptual framework (Note: This figure represents the theoretical model that guided the study design, data collection, and analysis; it does not depict original study findings). |
Therefore, this study aimed to explore the barriers to adherence to remote pelvic floor muscle training among postpartum women using a qualitative approach guided by the COM-B model, with the explicit purpose of generating theory-based evidence to inform the development of tailored intervention strategies and the design of hybrid digital–in-person postpartum rehabilitation services.
Methods
Study Design
This study employed a qualitative descriptive design to comprehensively illustrate the lived experiences of postpartum women regarding adherence to remote PFMT in straightforward, accessible language. This approach avoids complex theoretical abstractions and does not seek to develop a novel theoretical framework. Unlike phenomenology, which explores the intrinsic essence of lived experiences, and grounded theory, which generates emergent theories from empirical data, qualitative descriptive methodology is well-suited for applied clinical and digital health research. A primary strength of this design lies in its capacity to identify contextually relevant practical barriers, providing direct evidence to inform the development of targeted intervention protocols.
The study was guided by the COM-B model, which served as the theoretical framework for the development of the interview guide, data coding, and interpretation of findings. The study is reported in accordance with the Standards of Qualitative Research Reporting (SRQR) guidelines (Supplementary Material S1).25
Setting and Participants
Participants were recruited from the pelvic floor rehabilitation clinic at a Wuxi Hospital between November and December 2024. In the local postpartum care pathway, all women are recommended to undergo PFMT. Pelvic floor rehabilitation services are universally available, with remote PFMT programs prescribed either preventively (asymptomatic women) or therapeutically (symptomatic women). Inclusion criteria: (1) 6 weeks–12 months postpartum; (2) engaged in a remote PFMT program within the past 6 months; (3) aged ≥18; (4) fluent in Chinese. Exclusion criteria: (1) severe postpartum complications/neurological conditions; (2) exclusive face-to-face training. Purposive maximum-variation sampling was operationalized across six dimensions: parity, delivery mode, postpartum stage, symptom status, remote PFMT modality, and adherence level. Recruitment proceeded iteratively until thematic saturation was reached.
Recruitment Procedure
Potential participants were identified through pelvic floor rehabilitation clinics and approached by the research team either in person or via online messaging. Eligible women were informed about the purpose, procedures, and voluntary nature of the study. Those who agreed to participate provided written or electronic informed consent before the interview. Participants were assured that their personal information would be kept confidential and that they could withdraw from the study at any time without any consequences for their care.
Data collection and analysis were conducted concurrently. Recruitment ceased when thematic saturation was achieved, that is, when no new categories or meaningful insights emerged from subsequent interviews. Saturation was considered reached after 12 interviews, and 3 additional interviews were conducted to confirm saturation. A flow diagram summarizing the recruitment, eligibility assessment, participation, interview completion, and data analysis steps is provided in Supplementary Material S2.
Data Collection
Data were collected through semi-structured individual interviews conducted by a trained qualitative researcher, who had experience in qualitative interviewing and maternal health research. Before the formal interviews, the interview guide was developed based on the COM-B model and relevant literature on PFMT adherence, postpartum rehabilitation, and digital health behaviors. The guide was reviewed by 2 experts in maternal health and pilot-tested with 2 postpartum women to improve clarity and relevance (Supplementary Material S3).
Interviews were conducted by the lead researcher (DZ), a nurse researcher in obstetrics and gynecology, who had no prior therapeutic or clinical relationship with any participant. To minimize social desirability bias and mitigate potential power differentials, participants were explicitly informed that the interviewer was independent of their routine postpartum care team, that participation was strictly voluntary, and that negative, contradictory, or non-adherent experiences were equally valued and would not affect their clinical care. Interviews were scheduled over a four-week period, with sessions spaced 2–3 days apart to allow for iterative reflection and minor guide adjustments based on emerging data. Each interview was conducted in a private setting, either face-to-face or via encrypted video call, according to participant preference and logistical feasibility. Sessions lasted approximately 25–35 minutes and were audio-recorded with explicit consent. Field notes were taken during and immediately after the interviews to capture nonverbal cues, contextual information, and preliminary reflections. All interviews were conducted in Chinese, transcribed verbatim within 24–48 hours, and checked against the recordings for accuracy. Identifiable information was removed during transcription to ensure anonymity.
Data Analysis
Data were analyzed using directed content analysis, as described by Hsieh and Shannon,26 with the COM-B model serving as the initial coding framework. The analytic process was further organized according to the preparation, organizing, and reporting phases proposed by Elo and Kyngäs.27 To reduce the risk of merely allocating data to predetermined categories, the analysis explicitly allowed for inductive coding outside the COM‑B domains. When a code could not be readily classified into capability, opportunity, or motivation, it was retained and discussed among the research team to determine whether it represented a barrier not captured by the COM‑B model or could be reconciled through consensus. No major barrier was excluded solely because it did not fit the COM‑B framework; however, all identified barriers ultimately proved classifiable within the three domains.
All transcripts were read multiple times to achieve immersion. Meaning units related to barriers to adherence to remote pelvic floor muscle training were identified and openly coded. Codes were then mapped onto the three COM‑B domains, and through iterative comparison and abstraction, subthemes were developed within each domain. To enhance analytic rigor, two researchers (DZ and XN) independently coded all 15 transcripts. For the first five transcripts, coding was performed independently and then compared in joint meetings to harmonize the coding framework, resolve discrepancies, and refine code definitions. The remaining transcripts were coded independently using the refined framework, with regular consensus meetings to discuss emerging findings and ensure consistency across the dataset. Discrepancies that could not be resolved through discussion were referred to a third researcher (MD). NVivo 11.0 facilitated data management, coding, and retrieval.
Throughout the analysis, negative case analysis was undertaken by actively seeking participant accounts that appeared to diverge from emerging patterns; these instances prompted re‑examination and, where warranted, refinement of the subthemes. An audit trail was maintained, documenting key coding decisions, theme development, and modifications to the analytic framework. Saturation was considered achieved after 12 interviews, when no new subthemes or relevant properties emerged. Three additional interviews were conducted, confirming saturation.
Trustworthiness
To enhance the trustworthiness of the study, strategies addressing credibility, dependability, confirmability, and transferability were implemented throughout the research process.28 Detailed information is presented in Supplementary Material S4. Credibility was strengthened through purposive sampling with maximum variation, prolonged engagement with the data, and peer debriefing among the research team. The interviewer was involved in the entire research process, including participant recruitment, interviewing, transcription checking, and preliminary analysis, which facilitated familiarity with the data and a deeper understanding of participants’ experiences. Member checking was conducted with selected participants to confirm whether the preliminary findings accurately reflected their perspectives.
Ethical Considerations
This study was approved by the Ethics Committee of Wuxi Ninth People’s Hospital (KS2025009). All participants provided written informed consent before participation. Participants were informed of the purpose of the study, the voluntary nature of their participation, their right to withdraw at any time, and the measures taken to ensure confidentiality and anonymity. All audio files, transcripts, and research records were securely stored and accessible only to the research team. Informed consent obtained from all participants explicitly included permission to publish anonymized direct quotes and responses for academic dissemination.
Results
Participant Characteristics
A total of 15 postpartum women participated in the study (Table 1). Their ages ranged from 26 to 36 years, and the postpartum period ranged from 6 weeks to 6 months. The sample included both asymptomatic (n=8) and symptomatic (n=7) participants. Remote PFMT modalities varied: standalone app (n=7), app + video (n=4), app + teleconsultation (n=4). Adherence was self-reported based on frequency over the preceding 4 weeks: Low = <3 days/week (n=9); Moderate = 3–5 days/week (n=6); High = >5 days/week (n=0).
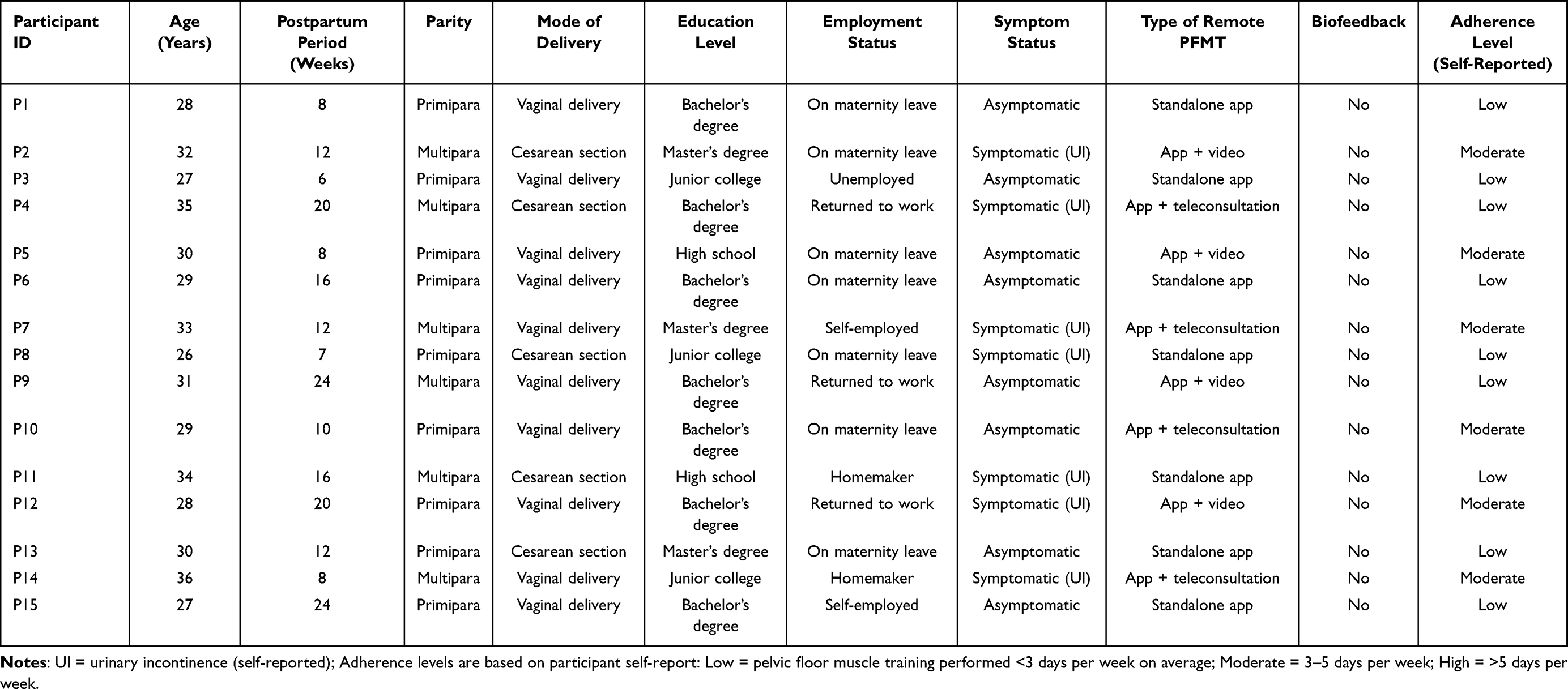 |
Table 1 Characteristics of Participants |
Overview of Findings
Analysis of the interview data identified multiple barriers to adherence to remote PFMT among postpartum women. These barriers were organized according to the three domains of the COM-B model: capability, opportunity, and motivation. Within these domains, 11 subthemes were identified (Table 2). These barriers were interrelated and often reinforced one another, jointly shaping women’s adherence behavior. To clarify the modality-specific impact of remote delivery, each barrier has been classified in Table 2 as either general to PFMT or specific to the remote delivery context.
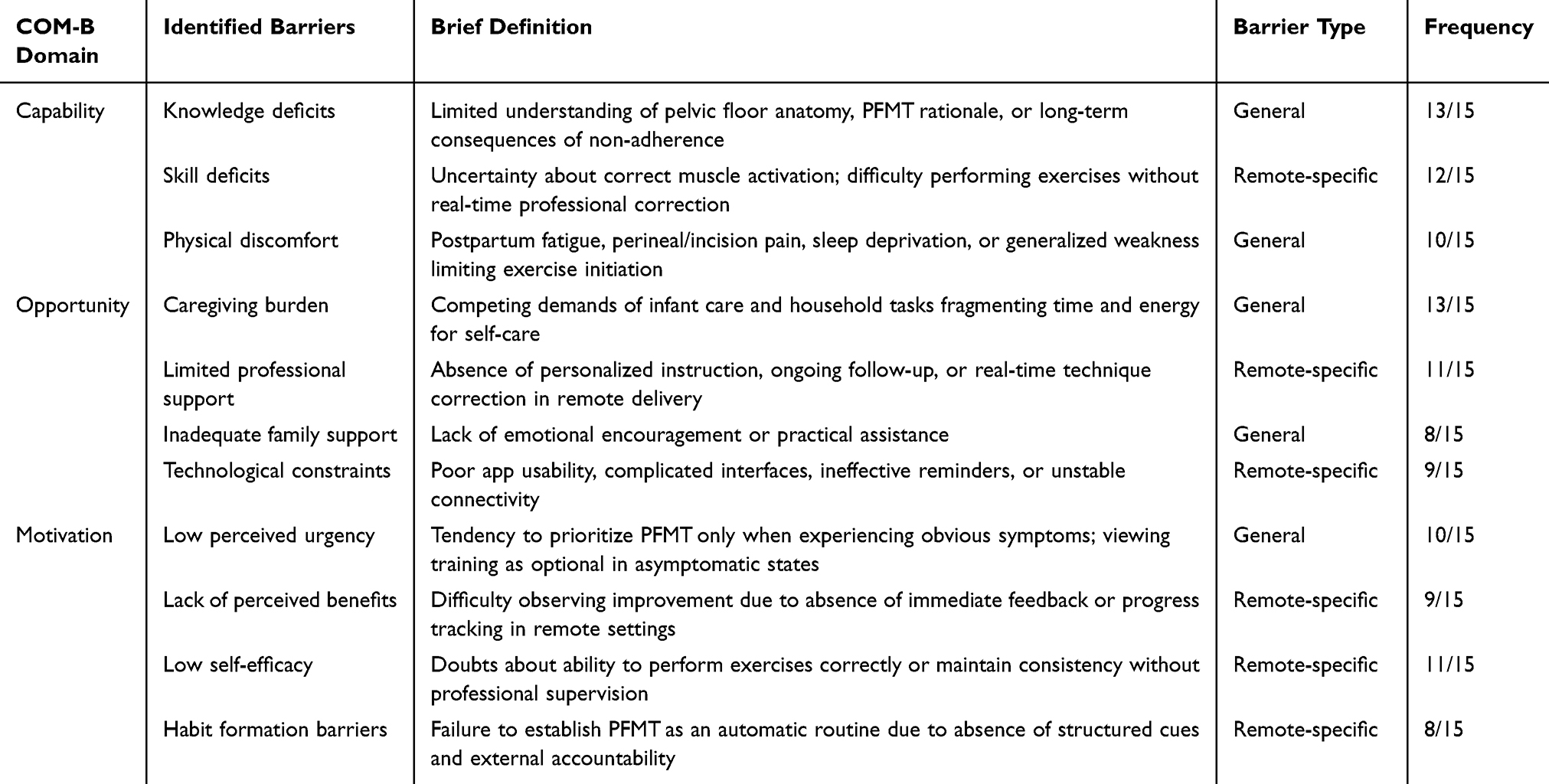 |
Table 2 COM-B-Based Barriers to Adherence to Remote Pelvic Floor Muscle Training Among Postpartum Women (n=15) |
Theme 1: Capability-Related Barriers
Subtheme 1.1: Knowledge Deficits
Many participants had limited knowledge of postpartum pelvic floor dysfunction and did not fully understand the preventive and therapeutic value of PFMT. Some women regarded PFMT as optional rather than necessary, especially in the absence of obvious symptoms.
I only knew that these exercises were somehow good for women after giving birth, but I didn’t know exactly what they were preventing. Since I didn’t have urine leakage or anything obvious, I felt it was not urgent. (P3)
No one explained clearly what might happen if I didn’t do the exercises. I thought as long as I rested well after childbirth, my body would recover naturally. (P9)
Subtheme 1.2: Skill Deficits
A prominent barrier raised by participants was uncertainty about whether they were performing PFMT correctly. Although remote programs provided instructional videos, text descriptions, or audio prompts, many women still found it difficult to identify the correct muscle groups and distinguish pelvic floor contractions from abdominal, gluteal, or thigh muscle movements.
The videos made it look simple, but when I did it myself, I really couldn’t tell whether I was tightening the right muscles. (P7)
I sometimes felt my abdomen becoming tense, and then I started wondering whether I was doing it wrong. Without someone checking me, I was never really sure. (P2)
Subtheme 1.3: Physical Discomfort
In addition to knowledge and skill-related barriers, women’s physical condition during the postpartum period also affected their capability to adhere to remote PFMT. Participants frequently described fatigue, sleep deprivation, perineal pain, incision discomfort, back pain, and generalized weakness as factors that limited their willingness or ability to exercise regularly.
After giving birth, I was physically drained every day. The baby woke up several times at night, and during the day I just wanted to rest whenever possible. (P10)
I had a cesarean section, and in the beginning I felt uncomfortable moving at all. Even if the training itself was not very hard, I didn’t feel ready to persist with it. (P4)
Theme 2: Opportunity-Related Barriers
Subtheme 2.1: Caregiving Burden
The most frequently described opportunity-related barrier was the overwhelming burden of childcare and domestic tasks. Participants portrayed the postpartum period as highly fragmented and unpredictable, with much of their time and energy devoted to feeding, soothing, bathing, and monitoring their infants. In addition, many were responsible for household duties or had to coordinate family-related tasks, leaving little uninterrupted time for self-care.
Looking after the baby takes up almost the whole day. Even if the exercise only takes a few minutes, it’s hard to find those few minutes when the baby is calm and no one needs me. (P5)
I would plan to do it, but then the baby would cry, or I had to feed her, or there was housework waiting. In the end, it was always postponed. (P1)
Subtheme 2.2: Limited Professional Support
Although remote PFMT increased accessibility, many participants perceived it as lacking the personalized guidance and accountability that face-to-face rehabilitation could provide. Women reported that they often needed more individualized instruction, ongoing follow-up, and real-time correction than the remote platform could offer.
The app could remind me, but it couldn’t tell me whether I was doing it correctly or whether I needed to adjust anything. (P6)
If a healthcare professional checked in with me regularly, I think I would take it more seriously. Doing it alone at home made it easy to give up. (P8)
Subtheme 2.3: Inadequate Family Support
Family support emerged as another important contextual factor influencing adherence. Some women reported that their spouses, parents, or other family members had limited understanding of postpartum pelvic floor recovery and did not recognize PFMT as a legitimate health priority. In such situations, women received little emotional encouragement or practical support, such as help with childcare or household work, to enable them to complete their exercises.
My family thought postpartum recovery mainly meant eating well and resting. They didn’t think these exercises were necessary, so no one really reminded or encouraged me. (P11)
If someone in the family could help hold the baby for a while, I might be able to do the training more regularly. But usually I had to manage everything myself. (P9)
Subtheme 2.4: Technological Constraints
Although remote PFMT was generally considered convenient, some participants experienced practical barriers related to the digital platform. These included poor usability of the app, complicated interfaces, lack of engaging content, ineffective reminders, unstable internet access, and difficulties navigating the program. Such problems reduced women’s willingness to use the platform consistently.
Sometimes I wanted to follow the program, but the app was not very intuitive, and I had to click through several steps. That made it feel troublesome. (P6)
Theme 3: Motivation-Related Barriers
Subtheme 3.1: Low Perceived Urgency
A key motivational barrier was the low perceived urgency of PFMT among women who did not experience clear or bothersome symptoms. Many participants associated rehabilitation with symptom relief rather than prevention. As a result, if they did not have urinary leakage, pelvic pressure, or other noticeable problems, they saw little immediate reason to continue the exercises.
Because I didn’t feel any obvious problem, I thought it was something I could do later or skip for a few days without much consequence. (P1)
If I had severe symptoms, I would probably insist more. But when everything seems normal, it’s easy to feel that the exercises are not essential. (P3)
Subtheme 3.2: Lack of Perceived Benefits
Another major barrier was that the effects of PFMT were often subtle, gradual, or not immediately observable. Many participants reported that because they could not see rapid improvement or tangible feedback, they questioned the usefulness of the exercises. This made it difficult to maintain interest and persistence over time.
I did it for a while, but I couldn’t tell if there was any real improvement. It’s hard to keep going when you don’t feel a clear result. (P8)
It’s not like taking medicine and feeling better quickly. This kind of training feels very slow, so after some time I lost patience. (P4)
Subtheme 3.3: Low Self-Efficacy
Some participants expressed doubts about their ability to integrate PFMT into their daily routines over the long term. Even when they acknowledged the potential benefits of training, they were uncertain whether they could remain consistent in the context of childcare demands, changing schedules, and eventual return to work.
At the beginning I was motivated, but I didn’t really believe I could keep it up for months. My days were too unpredictable. (P5)
Subtheme 3.4: Habit Formation Barriers
Habit formation was difficult for many participants. They reported that remote PFMT had not become an automatic part of their daily routine, largely because postpartum life was highly fragmented and unpredictable Forgetfulness, repeated interruptions, and the absence of stable cues made it difficult to establish a consistent exercise habit.
At first I felt enthusiastic, but later it became repetitive and easy to forget. Then I felt guilty for not doing it, and that made me even less willing to continue. (P11)
I wouldn’t say I deliberately refused to do it. It just kept slipping out of my mind because there were too many other things to think about. (P7)
Interactions Among Capability, Opportunity, and Motivation
Analysis revealed that barriers did not operate in isolation but formed mutually reinforcing cycles across COM‑B domains. Four key interaction pathways emerged. First, insufficient knowledge diminished reflective motivation: women who lacked a clear understanding of pelvic floor dysfunction and the preventive value of PFMT perceived the exercises as non‑urgent, particularly in the absence of symptoms. Second, limited professional support in remote programs amplified skill deficits and lowered self‑efficacy; without real‑time feedback, uncertainty about correct technique persisted, which in turn eroded women’s confidence and willingness to continue. Third, heavy caregiving responsibilities not only restricted the opportunity to exercise but also depleted the physical energy required for capability and disrupted the stable routines essential for automatic motivation and habit formation. Fourth, technological constraints such as unintuitive interfaces or cumbersome access steps introduced friction that transformed a convenient home‑based tool into an additional motivational burden.
Discussion
This qualitative study, guided by the COM-B model, identified eleven barriers to adherence to remote pelvic floor muscle training among postpartum women across the three behavioral domains: capability (knowledge deficits, skill deficits, physical discomfort), opportunity (caregiving burden, limited professional support, inadequate family support, technological constraints), and motivation (low perceived urgency, lack of perceived benefits, low self-efficacy, habit formation difficulties). These barriers did not operate in isolation but formed mutually reinforcing pathways that collectively undermined adherence behavior in the remote rehabilitation context.
Across all three COM-B domains, our findings further corroborate the barriers previously documented in studies of PFMT adherence, including knowledge deficits,29 physical discomfort,30 caregiving burden,31 and low perceived urgency.31 This indicating that many of these challenges are not unique to remote service delivery but are inherent characteristics of the postpartum rehabilitation process. However, our data also suggest that remote service delivery significantly alters how these barriers are experienced: in the absence of real-time professional feedback, skill deficiencies that could have been corrected during a single in-person consultation persist and progressively erode self-efficacy, a process that reflects a cascade from insufficient opportunity (limited professional support) to diminished capability (unvalidated technique) and subsequently to reduced motivation (low self-efficacy). This trajectory aligns with a mediating model recently validated by Wang et al, which posits that the effect of knowledge on PFMT adherence is exerted solely through self-efficacy;32 our study further demonstrates that, in the context of remote service delivery, opportunity constraints amplify this chain of mediation.
A key contribution of this study is the clear differentiation between inherent barriers commonly associated with conventional PFMT and those unique to remote PFMT delivery. Universal barriers, such as postpartum physical discomfort, competing demands of childcare responsibilities, and a lower perceived urgency among asymptomatic postpartum women regarding the need for training, are frequently reported and appear to be independent of the training modality. Nevertheless, these challenges are significantly amplified in a remote delivery context. While skill uncertainty exists in all forms of PFMT, it becomes a critical barrier specific to remote delivery in the absence of real-time professional guidance. These findings are consistent with prior research demonstrating that, for many women, correct voluntary contraction of the pelvic floor muscles is not an intuitive action, and a substantial proportion of individuals are unable to perform an effective contraction without instruction or feedback.33 Similarly, technological operational barriers, a lack of structured accountability mechanisms, and delayed progress feedback are challenges that are either uniquely introduced or substantially exacerbated by digital or home-based delivery models. Although digital interventions have demonstrated potential in supporting postpartum recovery,34 the findings of this study indicate that, when technology design or support is suboptimal, these factors can paradoxically become barriers. A feasibility study of the GoMAP application used by pregnant women undergoing PFMT reported high adherence and self-efficacy, suggesting that well-designed applications may be capable of overcoming certain technological obstacles.35 Adherence issues identified in remote delivery contexts cannot be adequately addressed through routine postpartum education alone. Instead, targeted strategies—including well-conceived digital solutions and tailored care pathways for different delivery modalities—are required to effectively manage these specific barriers.
The interaction patterns identified in this study—knowledge deficits weakening perceived urgency, caregiving burden simultaneously eroding opportunity and physical capability, technological friction converting convenience into motivational cost—underscore a central insight: adherence to remote PFMT is not determined by isolated deficits but by how barriers reinforce one another within a behavioral system. This systemic perspective, while consistent with the COM-B model’s theoretical assumptions,21 has rarely been demonstrated empirically in postpartum PFMT research. It carries a pragmatic implication: interventions that target only a single domain may fail because improvements in one area are neutralized by persistent barriers in others.
Implications for Intervention Design and Service Delivery
The findings of this study support a transition from a singular remote pelvic floor muscle training model to a hybrid care model. In this model, an initial in-person outpatient visit ensures the standardization of training movements, thereby addressing issues related to insufficient operational competence and low self-efficacy. A user-friendly digital platform provides structured training reminders and progress tracking, facilitating the formation of exercise habits and enhancing perceived subjective benefits. Regular online professional follow-up visits help maintain training adherence and correct movement deviations, compensating for deficiencies in professional guidance and skill acquisition. A psychoeducational module encourages the involvement of partners and other family members, fostering a supportive home environment and mitigating the lack of family support. Each of these measures directly corresponds to one or more barrier factors identified through the analyses in this study (Figure 2). Similar hybrid models have demonstrated feasibility in other domains of digital health for women.31 Furthermore, the APPEAL project study indicated that midwife-led health education combined with continuous support services significantly improved adherence to and practical effectiveness of pelvic floor muscle training.36
 |
Figure 2 COM-B Model of Adherence to Remote PFMT with Identified Barriers and Intervention Recommendations (Note: Green arrows indicate opportunity, Orange arrows indicate motivation, and blue arrows indicate capability). |
From a technical design perspective, the findings indicate that applications with non-intuitive operational interfaces and cumbersome usage steps lead to motivational attrition. This conclusion underscores the necessity of implementing user-centered design for postpartum women. Relevant platforms should streamline operational navigation, provide clear and immediate feedback on exercise completion, and ensure that reminder systems are sufficiently flexible to accommodate the unpredictable schedules associated with infant care. A collaborative design model involving end-users and pelvic floor rehabilitation therapists is recommended, ensuring that digital tools, while addressing existing usage barriers, do not inadvertently create new ones.
Limitations
This study has several limitations. First, recruitment from a single tertiary pelvic floor clinic may have selected women already engaged with postpartum rehabilitation services, potentially underrepresenting completely unengaged community populations. Second, the sample included mixed preventive and therapeutic participants; while this reflects real-world practice, symptom status likely influenced motivational reporting. Third, remote PFMT modalities varied, and although barrier patterns were consistent, modality-specific effects warrant dedicated investigation. Fourth, self-reported adherence and retrospective recall may introduce bias. Fifth, the barrier-focused interview design intentionally excluded facilitator exploration, limiting balanced intervention design insights. Sixth, reflexivity considerations were addressed but the interviewer’s clinical affiliation may have influenced participant disclosure. Finally, the sample size, though methodologically justified by saturation, limits subgroup comparisons by parity, delivery mode, or socioeconomic status. These constraints highlight the need for multi-center, longitudinal, and mixed-methods studies.
Conclusions
Postpartum women encounter multifaceted, interdependent barriers to remote PFMT adherence. Effective digital rehabilitation programs must move beyond content delivery to address capability verification, contextual opportunity constraints, and motivational sustainment through hybrid, theory-informed design. Future research should evaluate multi-component digital interventions targeting these COM-B domains across diverse postpartum populations.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Human Ethics Committee of Wuxi Ninth People’s Hospital Affiliated to Soochow University (KS2025009). Informed consent to participate was obtained from all of the participants. Informed consent obtained from all participants explicitly included permission to publish anonymized direct quotes and responses for academic dissemination.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Wuxi Association for Science and Technology Soft Science Program (No. KX-24-C063).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Billecocq S, Bo K, Dumoulin C, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for the conservative and non-pharmacological management of female pelvic floor dysfunction. Prog Urol. 2019;29(4):183–13. doi:10.1016/j.purol.2018.12.010
2. Dietz HP. Pelvic floor trauma in childbirth. Aust N Z J Obstet Gynaecol. 2013;53(3):220–230. doi:10.1111/ajo.12059
3. Deshmukh A, Ganvir S, Sathe T. Prevalence of pelvic floor dysfunction in postpartum women: a systematic review. J Neonatal Surg. 2025;14(8S):1019–1026.
4. Yu J, Wang L, Gan Q, Meng J. Risk factors of pelvic floor dysfunction in women with natural childbirth. South China J Prevent Med. 2024;50(4):299–303. doi:10.12183/j.scjpm.2024.0299
5. Palmer MH, Cockerell R, Griebling TL, Rantell A, van Houten P, Newman DK. Review of the 6th International Consultation on Incontinence: primary prevention of urinary incontinence. Neurourol Urodynamics. 2020;39(1):66–72. doi:10.1002/nau.24222
6. Bø K, Hilde G. Does it work in the long term?--A systematic review on pelvic floor muscle training for female stress urinary incontinence. Neurourol Urodyn. 2013;32(3):215–223. doi:10.1002/nau.22292
7. Boyle R, Hay-Smith EJC, Cody JD, Mørkved S. Pelvic floor muscle training for prevention and treatment of urinary and fecal incontinence in antenatal and postnatal women: a short version Cochrane review. Neurourol Urodyn. 2014;33(3):269–276. doi:10.1002/nau.22402
8. Sigurdardottir T, Steingrimsdottir T, Geirsson RT, Halldorsson TI, Aspelund T, Bø K. Can postpartum pelvic floor muscle training reduce urinary and anal incontinence? An assessor-blinded randomized controlled trial. Am J Obstet Gynecol. 2020;222(3):
9. Borello-France D, Burgio KL, Goode PS, et al. Adherence to behavioral interventions for stress incontinence: rates, barriers, and predictors. Phys Ther. 2013;93(6):757–773. doi:10.2522/ptj.20120072
10. Alewijnse D, Mesters I, Metsemakers J, Adriaans J, van den Borne B. Predictors of intention to adhere to physiotherapy among women with urinary incontinence. Health Educ Res. 2001;16(2):173–186. doi:10.1093/her/16.2.173
11. Asklund I, Nyström E, Sjöström M, Umefjord G, Stenlund H, Samuelsson E. Mobile app for treatment of stress urinary incontinence: a randomized controlled trial. Neurourol Urodyn. 2017;36(5):1369–1376. doi:10.1002/nau.23116
12. Sjöström M, Umefjord G, Stenlund H, Carlbring P, Andersson G, Samuelsson E. Internet-based treatment of stress urinary incontinence: a randomised controlled study with focus on pelvic floor muscle training. BJU Int. 2013;112(3):362–372. doi:10.1111/j.1464-410X.2012.11713.x
13. Chen SY, Tzeng YL. Path analysis for adherence to pelvic floor muscle exercise among women with urinary incontinence. J Nurs Res. 2009;17(2):83–92. doi:10.1097/JNR.0b013e3181a53e7e
14. Venegas M, Carrasco B, Casas-Cordero R. Factors influencing long-term adherence to pelvic floor exercises in women with urinary incontinence. Neurourol Urodyn. 2018;37(3):1120–1127. doi:10.1002/nau.23432
15. Harper RC, Sheppard S, Stewart C, Clark CJ. Exploring adherence to pelvic floor muscle training in women using mobile apps: scoping review. JMIR mHealth uHealth. 2023;11(1):e45947. doi:10.2196/45947
16. Villa-Del-Pino I, Jiménez-Rejano JJ, Rebollo-Salas M, Rodríguez-Domínguez ÁJ, Suárez-Serrano CM. Compliance and adherence to pelvic floor exercise therapy in people with pelvic floor disorders: a systematic review and meta-analysis. Life. 2025;15(4):613. doi:10.3390/life15040613
17. Wessels NJ, Loohuis AMM, van der Worp H, et al. Barriers and facilitators associated with app-based treatment for female urinary incontinence: mixed methods evaluation. JMIR mHealth uHealth. 2021;9(9):e25878. doi:10.2196/25878
18. Yang X, Zhang A, Sayer L, Bassett S, Woodward S. The effectiveness of group-based pelvic floor muscle training in preventing and treating urinary incontinence for antenatal and postnatal women: a systematic review. Int Urogynecol J. 2022;33(6):1407–1420. doi:10.1007/s00192-021-04960-2
19. Anglès-Acedo S, López-Frías L, Soler V, et al. The WOMEN-UP solution, a patient-centered innovative e-Health tool for pelvic floor muscle training: qualitative and usability study during early-stage development. Int J Environ Res Public Health. 2021;18(15):7800. doi:10.3390/ijerph18157800
20. Dufour S, Fedorkow D, Kun J, Deng SX, Fang Q. Exploring the impact of a mobile health solution for postpartum pelvic floor muscle training: pilot randomized controlled feasibility study. JMIR mHealth uHealth. 2019;7(7):e12587. doi:10.2196/12587
21. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
22. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
23. Keyworth C, Epton T, Goldthorpe J, Calam R, Armitage CJ. “It’s difficult, I think it’s complicated”: health care professionals’ barriers and enablers to providing opportunistic behaviour change interventions during routine medical consultations. Br J Health Psychol. 2019;24(3):571–592. doi:10.1111/bjhp.12368
24. Xu P, Jin Y, Guo P, et al. Barriers and enablers of pelvic floor rehabilitation behaviours in pregnant women with stress urinary incontinence: a qualitative analysis using the theoretical domains framework. BMC Pregnancy Childbirth. 2023;23(1):300. doi:10.1186/s12884-023-05633-2
25. O’Brien BC, Harris IB, Beckman TJ, Reed DA, Cook DA. Standards for reporting qualitative research: a synthesis of recommendations. Acad Med. 2014;89(9):1245–1251. doi:10.1097/ACM.0000000000000388
26. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
27. Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. doi:10.1111/j.1365-2648.2007.04569.x
28. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. doi:10.1016/j.nedt.2003.10.001
29. Gondim EJL, Moreira MA, Lima AC, de Aquino PS, Do Nascimento SL. Women know about perineal trauma risk but do not know how to prevent it: knowledge, attitude, and practice. Int J Gynaecol Obstet. 2023;161(2):470–477. doi:10.1002/ijgo.14526
30. Sitaraman L, Lewicky-Gaupp C, Rao SS. Postpartum anorectal and pelvic floor disorders: evaluation, treatment, and prevention. Curr Gastroenterol Rep. 2025;27(1):48. doi:10.1007/s11894-025-01000-7
31. Yount-Tavener SM, Fay RA. Maintaining a long-term practice of daily pelvic floor muscle exercises: what do childbearing women think? J Midwifery Womens Health. 2024;69(4):567–576. doi:10.1111/jmwh.13626
32. Wang J, Wu L, Fan G, Ji Y. The mediating effect of self-efficacy on adherence to pelvic floor muscle training: an analysis based on the COM-B model. Eur J Obstet Gynecol Reprod Biol. 2025;312:114514. doi:10.1016/j.ejogrb.2025.114514
33. Daniel DS, Goldenberg M, Kalichman L. Rehabilitative ultrasound imaging as visual biofeedback in pelvic floor dysfunction: a narrative review. Tomography. 2026;12(1):10. doi:10.3390/tomography12010010
34. Kwasnicki AJE, Rizk C, Western MJ, Zaidi H, Kwasnicki RM. Digital tools to support postpartum recovery: a systematic review. Women’s Health Rep. 2025;6(1):899–911. doi:10.1177/26884844251380146
35. Angélico C, Dos Sousa AJS, de Fernandes JGG, et al. Adherence and self-efficacy of pregnant women to perform pelvic floor muscle training through a health education application: a feasibility study. mHealth. 2025;11:17. doi:10.21037/mhealth-24-40
36. MacArthur C, Bick D, Salmon V, et al. Antenatal pelvic floor muscle exercise intervention led by midwives in England to reduce postnatal urinary incontinence: APPEAL feasibility and pilot randomised controlled cluster trial. BMJ Open. 2025;15(1):e091248. doi:10.1136/bmjopen-2024-091248
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Developing a Suite of Resources to Improve Patient Adherence to Compression Stockings: Application of Behavior Change Theory
Bar L, Marks D, Brandis S
Patient Preference and Adherence 2023, 17:51-66
Published Date: 6 January 2023
A Conceptual Model of Home-Based Cardiac Rehabilitation Exercise Adherence in Patients with Chronic Heart Failure: A Constructivist Grounded Theory Study
Yang Z, Sun L, Sun Y, Dong Y, Wang A
Patient Preference and Adherence 2023, 17:851-860
Published Date: 24 March 2023
Exploring Factors Influencing Dietary Management in Chinese Chronic Kidney Disease Patients Based on the COM-B Model: A Qualitative Study
Zhang N, Fan S, Wang S, Zhao Y, Liu H, Wei Y, Li Z, Wang W, Liu F
Risk Management and Healthcare Policy 2025, 18:1895-1910
Published Date: 12 June 2025
Factors Influencing Adherence to Dietary Interventions Among Patients with Gestational Diabetes Mellitus in China: A Qualitative Study Based on the COM-B Model
Jia CL, Wang LJ, Li LH, Lu YJ, Yang Y
Journal of Multidisciplinary Healthcare 2025, 18:4653-4663
Published Date: 5 August 2025