Back to Journals » Patient Preference and Adherence » Volume 17
Developing a Suite of Resources to Improve Patient Adherence to Compression Stockings: Application of Behavior Change Theory
Authors Bar L ![]() , Marks D
, Marks D ![]() , Brandis S
, Brandis S
Received 16 September 2022
Accepted for publication 13 December 2022
Published 6 January 2023 Volume 2023:17 Pages 51—66
DOI https://doi.org/10.2147/PPA.S390123
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Laila Bar,1,2 Darryn Marks,3 Susan Brandis1
1Department of Occupational Therapy, Bond University, Faculty of Health Science and Medicine, Robina, Queensland, Australia; 2Department of Occupational Therapy, Gold Coast University Hospital, Southport, Queensland, Australia; 3Department of Physiotherapy, Bond University, Faculty of Health Science and Medicine, Robina, Queensland, Australia
Correspondence: Laila Bar, Department of Occupational Therapy, Level 4, Bond Institute of Health and Sport, 2 Promethean Way, Robina, Queensland, 4226, Australia, Tel +61 413 855 090, Email [email protected]
Purpose: Poor patient adherence to compression stockings remains a difficult and pervasive problem for clinicians, with costly repercussions for patients and health-care systems. The purpose of this paper was to describe the application of behavior change theory to the systematic development of a suite of resources, aimed at improving patient adherence to wearing compression stockings.
Methods: Employing a non-empirical approach, behavior-change theory was used to develop an innovative intervention as part of a multi-phase project. Target behaviors, barriers and potential enablers were identified in relation to stocking adherence. An impact-likelihood matrix for behavior prioritization was used to identify possible areas for intervention within occupational therapy outpatient clinics. Selection of suitable resources and their consequent development were based on a narrative and problem-solving process by a panel of clinical experts.
Results: Of 14 potential domains embedded in the Theoretical Domains Framework, the key target behaviors and barriers were associated with eight domains. Michie’s Behavior Change Wheel revealed recommendations in six subdivisions and of these, four intervention functions were selected by the panel, based on their potential impact and likelihood of adoption in clinical practice. Findings led to the development of a suite of resources comprising a new questionnaire, a clinical decision tree, augmented by clinical answer sheets corresponding to each of the barriers.
Conclusion: Application of behavior change theory informed the design of a behavior change intervention comprising an integrated suite of resources for novice and experienced clinicians.
Practice Implications: These novel resources have potential to improve patient adherence to compression stockings and consequently generate health-care savings through reduced need for wound care products, and medical interventions with translation to other settings and conditions requiring compression stockings. Patient outcomes will likely be improved with reduced pain, improved quality of life and earlier resumption of usual occupations.
Keywords: compression stockings, adherence, behavior change theory, Behavior Change Wheel, COM-B model, Theoretical Domains Framework, venous leg ulcers
Plain Language Summary
The best way to treat and prevent venous leg ulcers is by wearing compression stockings every day. However, some people do not wear their stockings as much as they should, demonstrating “low adherence” to compression stockings. Using behavior change theory, three new resources have been developed to attempt to improve patient adherence. These include a new questionnaire to determine individual patient barriers, a decision tree to guide clinicians in addressing the barriers, and answer sheets listing recommendations to address each barrier.
Background
Clinically prescribed compression stockings are considered best practice, for chronic venous insufficiency (CVI), to heal and prevent venous leg ulcers (VLU).1–3 VLUs are wounds in the lower legs, occurring due to higher pressure within veins, often related to higher body mass index and/or impaired mobility.3 They are a significant problem for those over the age of 65, with international prevalence studies reporting rates between 1.5 and 3.0 per 1000 people.4 With demographics trending towards sedentary lifestyles and an ageing population, VLUs will likely remain a significant burden on society.5 VLUs have negative impacts at the individual level, contributing to pain, reduced quality of life and work productivity,6 while also burdening health-care systems due to wound management costs and hospitalization.7
Compression stockings must be worn consistently,3 since low adherence contributes to delayed healing8 and recurrence of VLU.9,10 Unfortunately, worldwide adherence rates are low, reported to be between 12% and 52%.11 Adherence to wearing compression stockings is a complex multi-faceted phenomenon, with over 200 barriers identified in the literature.10,12 Many of these barriers relate to patients’ lack of understanding of why stockings are required, difficulty with getting them on and off, and discomfort whilst wearing them.13,14
To determine each patient’s specific barriers to adherence, a suitable questionnaire is required. This is supported by Michie,15 a behavior theorist, who recommends that the reasons contributing to a “problem behavior”, such as poor adherence to medical advice, should be identified, prior to implementing any intervention. Several purpose-made questionnaires16–20 designed to determine patient-reasons for discontinuing compression therapy have been developed, however these do not adequately address the multi-dimensional aspects of adherence. Further, they lack sufficiently detailed questions for meaningful and personalized intervention planning. For example, Allaert’s 2019 study16 evaluated the psychometric properties of a self-questionnaire on adherence, Benigni17 investigated difficulties with donning stockings through a survey, and Shannon20 assessed adherence to wider clinical recommendations for preventing VLUs, but none of these included prior negative experiences,21 low mood22 or low self-belief23,24 as potential barriers. In relation to the comfort of a stocking, Allaert’s16 only question was “I find it uncomfortable (heat, cold, pressure)” and Clarke-Moloney18 simply asked “How do you find the feel/sensation’ of the stocking on your leg?”
Unidimensional interventions that aim to improve behaviors associated with adherence to compression stockings have often been unsuccessful and none have demonstrated consistent superiority over others.25 In contrast, research into improving adherence in other chronic health conditions including diabetes mellitus26 and chronic kidney disease,27 demonstrates more positive impacts from personalized and multidimensional approaches. A recent scoping review25 of adherence to wearing compression stockings found that, while personalized and multi-dimensional interventions show promise, further high-quality research is required. It recommended that the design of a multidimensional behavior change intervention to improve adherence with compression stockings, must accommodate the multitude of adherence barriers and be sufficiently flexible to deliver tailored personal interventions.
Many authors15,28,29 have employed theory in the development of other clinical interventions (prototypes) for behavior change, to promote clarity around planning, design, implementation, and evaluation. Theory can provide structure to complex knowledge, allowing for generalization across populations and settings.15,30,31 This is particularly relevant in the context of the adherence phenomenon, where patients often present with several barriers at the same time, requiring a complex intervention.28,32
In consideration of an overarching framework to guide resource development, a design thinking approach33 was given due consideration, since it aligns with the intent to implement a collaborative and human-centered approach to a real-world problem. However, since this framework encompasses prototype testing, it was considered beyond the scope of this paper. Behavior change theory allows for a more concentrated focus on development of a behavior change intervention.
Behavior change interventions can be defined as “coordinated sets of activities designed to change specified behavior patterns aiming to promote uptake of clinical services to support healthy lifestyles”.34 While there are several broad theoretical approaches available for developing interventions generally in health-care settings,15,35–37 more specific theories have also been used in the context of promoting adherence to medical recommendations.30,38 This section describes justification for the selection of a specific behavior change theoretical model.
A 2011 systematic analysis34 of 19 frameworks of behavior change interventions concluded that none covered the full range of intervention functions required for effective behavior change. Subsequently, Michie developed the Behavior Change Wheel (BCW).34 This is an iteration of the popular Theoretical Domains Framework (TDF).39 The BCW claims to be more flexible than the TDF alone, however the TDF is often used alongside it.40
The BCW has at its core, a “behavior system” involving three essential conditions: capability (C), opportunity (O) and motivation (M) to influence behavior (B). These form the basis of Michie’s COM-B model34 of behavior change. It proposes that at any given moment, a particular behavior will occur only when the person has the capability and opportunity to engage in a certain behavior, and when they are more motivated to perform that behavior than any other.34,41
The BCW on its own has demonstrated success and broad applicability in behavior change programs. A 2015 scoping30 review of adherence promotion theories in pelvic floor muscle training critiqued 12 theoretical models/theories and identified Michie’s BCW as helpful in informing future research into adherence interventions. BCW has also been used successfully to improve adherence to medical advice in diabetes management42,43 and heart failure.44 Furthermore, Gould et al45 employed the BCW to systematically inform an intervention for health provider care of Australian indigenous pregnant women regarding smoking cessation. Similarly, a theory-based 2018 study46 used the BCW to embed particular clinical behaviors into adult hearing aid fitting consultations, while Sinnott et al47 described the use of the BCW to develop an intervention for use by general practitioners to improve medication management in multimorbidity.
Use of the COM-B model together with the 14 domains of the TDF facilitates a more detailed transition from a behavioral analysis of the problem to the selection of the most contextually and effective intervention functions, including modes of delivery.41,45,46 The successful application of BCW and the TDF to other complex chronic conditions requiring multifactorial solutions argues well for its extension to the development of programs to improve adherence to compression stockings for the management of venous leg ulcers. Therefore, this paper describes the application of behavior change theory, specifically the COM-B model described by Michie in the BCW, supplemented by the additional details embedded in the TDF.
Methods
Michie’s BCW was used to guide selection of intervention functions to address barriers to target behaviors, identified using the COM-B model and TDF domains; a target behavior being one that has been chosen, or “targeted” for change.48
Initially, a local metropolitan hospital expert clinical panel was established by the lead investigator. Individuals were approached for inclusion based on their clinical relatedness to the topic and availability for subsequent collaborative phases of brainstorming, reframing, and refinement of ideas to inform the selection of appropriate resources for development. The final panel, connecting through email and personal interviews, consisted of occupational therapists, vascular nurse practitioners, vascular surgeons, and university academic staff.
The steps involved in resource development reflect similar BCW methodology described by earlier authors.46,47,49 Figure 1 illustrates the steps undertaken by the panel through the stages of defining the problem through to identification of appropriate behavior change techniques and their mode of delivery.
 |
Figure 1 Overview of steps used in resource development using the BCW approach. |
Firstly, the problem behaviors were defined, informing selection of target behaviors according to COM-B defined terms. The source (clinician or patient) of the desired behavior was then described alongside its linking TDF domain.39,50 “Clinicians” comprises occupational therapists and occupational therapy assistants, and “patients” are adults who are referred to outpatient clinics for compression stockings, with a history of venous leg ulcers and reduced adherence to stockings. To avoid repetition, affirming language was used. For example, “the patient can’t put stockings on and off by himself” became, “the patient can put stockings on and off by himself.” The dominant barriers to the target behavior were identified and linked to potential enablers within the context of occupational therapy (OT) outpatient clinics. Potential recipients of a new intervention were considered, and included hospital administrators, vascular surgeons, vascular nurse practitioners, general practitioners, patients, and clinicians.
The second step was to select, develop, and tailor the intervention functions to achieve the target behavior. The COM-B model was applied to the target behaviors and barriers. Potential strategies were linked to the desirable patient behavior. COM-B intervention functions with potential to elicit behavior change51,52 were considered by the panel in relation to each barrier, considering contextual relevance, and anticipated target acceptability. Kneebone’s Impact-Likelihood Matrix for behavior prioritization53 (Figure 2) prompted analysis of their likely impact and ease of implementation and was adapted with permission. Interventional strategies most likely to have a greater impact on stocking adherence were identified as those requiring the least effort and having the highest likelihood of adoption by clinicians.
 |
Figure 2 The impact-likelihood matrix for behavior prioritization.53 Notes: Reprinted from Kneebone SL, Fielding K. The impact-likelihood matrix: a policy tool for behaviour prioritisation. Environ Sci Technol. 2017;70:9–20, Copyright (2017), with permission from Elsevier.53 |
This process led to the third step, where the specific details about the resources to be developed were determined using a narrative and problem-solving process.
In development of the first resource (a questionnaire), barriers to stocking adherence were grouped thematically, and a list of possible questions considered capable of revealing these barriers was assembled by the lead investigator. These questions were then refined through consultation with the local expert clinical panel to provide a level of satisfactory detail. Recognizing, for example that there are multiple reasons for lack of comfort in stockings, this new questionnaire comprises 11 questions that relate to this issue alone.
In designing the second resource (a decision tree), the COM-B component and TDF domains were considered in relation to the source of the enabling behavior, linking each barrier to multiple levels of existing local resources, including videos and handouts.
Potential clinical recommendations regarding each question (barrier) on the questionnaire were explored in development of the third resource (clinical answer sheets) through a review of the literature, supplemented by several phases of feedback from the expert clinical panel. These were revised until a consensus was reached regarding the final version of each corresponding answer sheet.
Results
The following section presents the results from the application of behavior change theory as described above. Initially, the expert clinical panel agreed that only patients and clinicians were appropriate recipients of the intervention. The step of defining the problem and specifying the target behaviors found that, of 14 potential TDF domains, the target patient- and clinician-behaviors and barriers were associated with the following eight domains: Knowledge, skill, environmental context and resources, social/professional role, memory/attention/decision process, beliefs about consequences, beliefs about capabilities, and social influences. Table 1 presents this information.
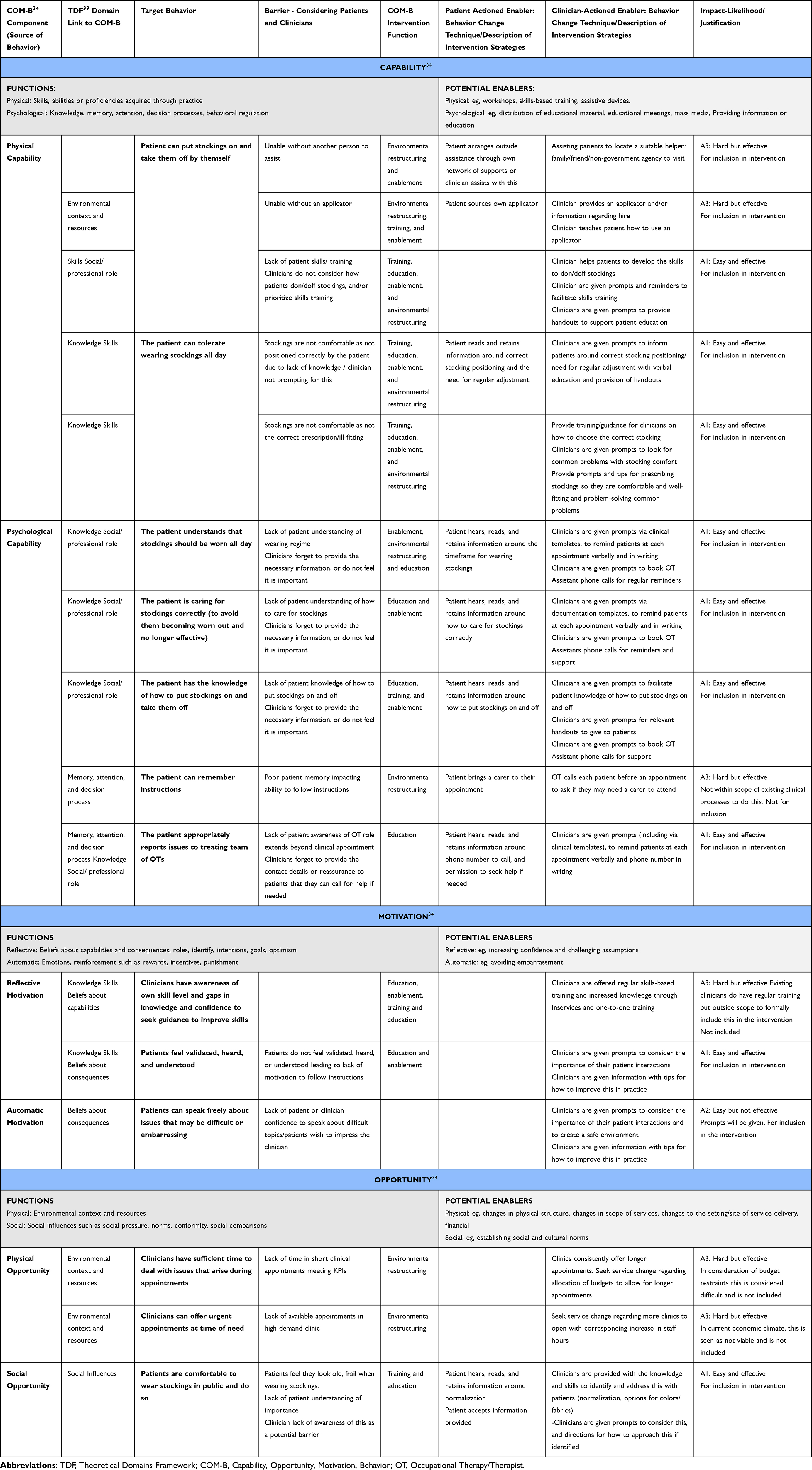 |
Table 1 Mapping of Barriers and Enablers to the Wearing of Compression Stockings, Linked to Michie’s COM-B Functions, Grouped by TDF Domains, and Rated on Their Justification for Inclusion |
The second step resulted in the selection, development, and tailoring of the intervention, while also identifying intervention functions to achieve the target behavior. Application of the COM-B model to the target behaviors and barriers revealed recommendations in six sub-divisions isolating potential facilitators across multiple domains. The intervention functions were identified and prioritized and are also included in Table 1. Nine possible COM-B intervention functions were considered by the panel for contextual relevance and acceptability. Five intervention functions were excluded (persuasion, incentivization, coercion, restriction, and modelling) considered difficult to implement due to practical limitations of prebooked outpatient appointments which are inflexible (30- or 60-minute appointments) and patients are routinely only reviewed every six months. Those considered feasible were education, training, environmental restructuring, and enablement. Of 16 potential contextually relevant patient- or clinician-actioned enablers mapped onto a prioritization tool, four were excluded. Justification for omission is described in Table 1.
This process identified the need to develop a suite of resources to comprehensively address the variability and combined complexity of the intervention strategies and enablers identified. These resources were modelled around published evidence, strengthened by the expert panel’s shared knowledge and experience.54,55 A new patient questionnaire, sufficiently specific to determine individual patient barriers to adherence was created. Secondly, a decision tree was designed to assist clinician’s efforts to systematically address each patient barrier to the target behavior. Finally, recommendations to address each barrier were agreed upon, and assembled conveniently as “clinical answer sheets”. This suite of resources is shown in Figure 3.
 |
Figure 3 The suite of resources. |
The “Barriers to Compression Questionnaire” comprises 24 questions, thematically grouped into five categories. It prompts the treating clinician to make clinical observations and ask probing questions to identify participant-specific barriers to adherence. Each question requires a “yes” or “no” response. If a “yes” response is recorded, the clinician or participant rates the significance of this score on a Likert scale of 1 (mild) to 5 (severe). Table 2 demonstrates the link between each barrier, the question relating to the barrier, the relevant COM-B component and the TDF domain and source of enabling behavior.
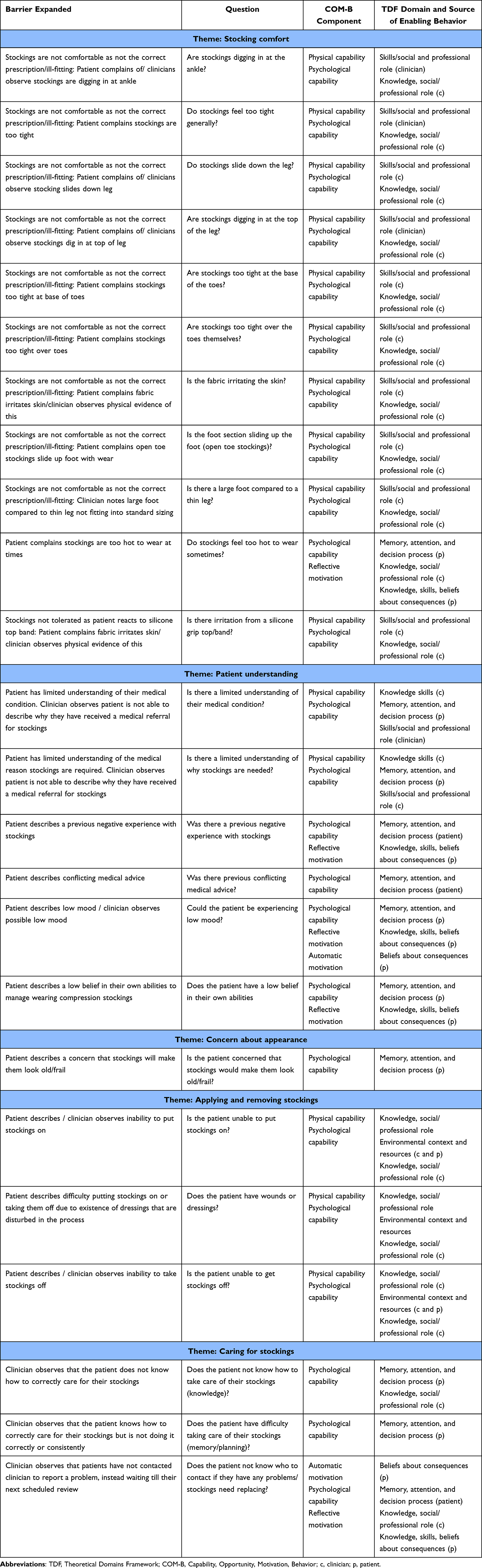 |
Table 2 Barrier Identification Expanded for Detail, Linked with Its COM-B34 Component, TDF39 Domain and Source of the Enabling Behavior |
The clinical decision tree links each barrier to multiple levels of resources. For example, if a patient’s primary barrier is related to lack of skills in applying compression stockings, the decision tree will link to the relevant clinical answer sheet, recommend targeted skills-based training and/or enablement via assistive devices, and suggest pertinent patient handouts and videos. If the barrier relates to discomfort whilst wearing stockings, then the answer sheet will suggest a modified stocking type/sizing based on the reason for the discomfort and suggest further resources if appropriate.
A separate clinical answer sheet corresponds to each of the 24 questions. Clinicians are instructed to identify their patients’ top three barriers before designing and implementing a treatment plan, as per usual clinical practice.56
To illustrate the process from identification of a barrier through to selection of a behavior change intervention, using appropriate intervention functions, three examples are shown in Figure 4.
 |
Figure 4 Three examples demonstrating links between barriers, intervention function and intervention prompted by the clinical decision tree. |
Discussion
This paper describes the application of an evidence-based, behavior theory-driven methodology for improving patient adherence to wearing compression stockings. It presents a suite of resources developed using Michie’s BCW and the TDF. A recent scoping review25 found that multidimensional approaches showed greater impact on adherence to stockings but have not yet been developed for testing. These new resources were developed to meet this gap.
These resources have potential to demonstrate positive impacts on health economics and patient outcomes. It is predicted that the development of a program to improve stocking adherence may have greater impact on this population than any improvement in medical or wound treatments.57 In a review of the health economics regarding compression stockings, a 2018 Australian study58 highlighted the important contribution of compression therapy in the management of VLUs. This study proposed that the provision of compression stockings to affected individuals nationally would initially cost the health system an additional AUS$270 million over 5 years but ultimately save AUS$1.4 billion over the same period of time. Further supporting the allocation of government funding, Pacella59 reported that when patients were reimbursed for any costs related to compression stockings, their health-related quality of life improved. Importantly however, this economic modelling assumes that patients are adhering to compression stocking regimes.3 Given the well documented low adherence to best-practice treatment with subsequent negative impacts on wound healing and recurrence,13,14 improving compression stocking adherence may contribute to substantial cost savings and favorable patient outcomes3,18 by allowing their full benefits to be realized.
It is also anticipated that these new resources will be transferable to other settings with a role in providing compression stockings for medical conditions where adherence is similarly low, such as lymphoedema, deep vein thrombosis, scarring and burns,60 suggesting potential impact beyond venous leg ulcers.
The clinical information and guidance provided within these resources has the potential to influence clinician skill, confidence, and job satisfaction. Many may consider the specialized area of compression stockings outside their scope of practice57 while clinical frustration related to the care of patients who are considered non-adherent to other forms of medical advice, has been linked to clinician stress, burnout, and general dissatisfaction with the health profession.61 Competence in influencing patient adherence may therefore impact clinician satisfaction in caring for this patient cohort with potential generation of interest in gaining further expertise in this clinical area.
Strengths and Limitations
The strength of this new suite of resources lies in the breath of analysis completed prior to their development and the multifactorial aspects considered. The underpinning theory-based approach is augmented by input from highly experienced local clinical experts. The developed resources meet the requirements of an innovative personalized and multidimensional approach to intervention, as recommended by earlier authors.14
A substantial evidence base supports the selection of behavior change theory to guide the development of a new intervention. Other models were considered, for example, a design thinking approach,33,62 however this is a relatively new framework. The BCW and TDF have been employed extensively42–44 to explore barriers and enablers to behavior change for other medical recommendations and they provide the scope to encompass the complexity surrounding compression stocking adherence.
Several limitations are acknowledged. Complex problems lend themselves to non-empirical approaches; however, empirical methods are required to draw conclusions and test their efficacy. Repeatability of research methodology is hindered by variability of site-specific factors including local clinical context, patient demographics and panel expertise. Further challenges exist because of the novelty of the resources and absence of similar comparative models. It is also acknowledged that the developed resources are required to be used together which, in consideration of their combined complexity, would require a behavior change for the clinicians using it. A paper-based delivery format could be considered cumbersome and, therefore, implementation of developed resources require attention regarding their delivery method.
Directions for Future Research
Given the known benefits of medical software applications, including increased access to point-of-care tools, better clinician communication, portability of information resources63 and improved clinical decision-making,64 the combined resources could be delivered on an App platform. A pilot study to investigate user acceptability, feasibility, and potential early proof of concept of these resources is recommended. This could then inform a larger randomized controlled trial with health-economics analysis, to test if these resources can improve stocking adherence and determine if there is a cost-benefit related to their use.
Conclusion
Behavior change theory was used to inform the design of a behavior change intervention to improve adherence to compression stockings. An analysis using Michie’s BCW34 and the TDF39 considered expert opinion and available literature, to determine barriers to wearing compression stockings, and identify potential intervention methods. These were rated on their ease of implementation and target acceptability within occupational therapy clinics, culminating in the development of a suite of resources including a questionnaire, a clinical decision tree, and clinical answer sheets for novice and experienced clinicians to improve patient stocking adherence.
Abbreviations
BCW, Behavior Change Wheel; COM-B, Capability, Opportunity, Motivation, Behavior; CVI, Chronic Venous Insufficiency; OT, Occupational Therapist; TDF, Theoretical Domains Framework.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weller CD, Buchbinder R, Johnston RV. Interventions for helping people adhere to compression treatments for venous leg ulceration. Cochrane Database Syst Rev. 2016;3:CD008378.
2. O’Meara S, Cullum N, Nelson EA, Dumville JC. Compression for venous leg ulcers. Cochrane Database Syst Rev. 2012;11:CD000265.
3. Health Quality Ontario. Compression stockings for the prevention of venous leg ulcer recurrence: a health technology assessment. Ont Health Technol Assess Ser. 2019;19(2):1–86.
4. Nelson EA, Bell-Syer SE. Compression for preventing recurrence of venous ulcers. Cochrane Database Syst Rev. 2014;9:CD002303.
5. Alavi A, Sibbald RG, Phillips TJ, et al. What’s new: management of venous leg ulcers. J Am Acad Dermatol. 2016;74(4):643–664. doi:10.1016/j.jaad.2015.03.059
6. Margolis DJ, Allen-Taylor L, Hoffstad O, Berlin JA. The accuracy of venous leg ulcer prognostic models in a wound care system. Wound Repair Regen. 2004;12(2):163–168. doi:10.1111/j.1067-1927.2004.012207.x
7. Barnsbee L, Cheng Q, Tulleners R, Lee X, Brain D, Pacella R. Measuring costs and quality of life for venous leg ulcers. Int Wound J. 2019;16(1):112–121. doi:10.1111/iwj.13000
8. Harrison MB, Graham ID, Friedberg E, Lorimer K, Vandevelde-Coke S. Regional planning study. Assessing the population with leg and foot ulcers. Can Nurse. 2001;97(2):18–23.
9. Samson RH, Showalter DP. Stockings and the prevention of recurrent venous ulcers. Dermatol Surg. 1996;22(4):373–376. doi:10.1111/j.1524-4725.1996.tb00334.x
10. Van Hecke A, Grypdonck M, Defloor T. A review of why patients with leg ulcers do not adhere to treatment. J Clin Nurs. 2009;18(3):337–349. doi:10.1111/j.1365-2702.2008.02575.x
11. Finlayson K, Edwards H, Courtney M. The impact of psychosocial factors on adherence to compression therapy to prevent recurrence of venous leg ulcers. J Clin Nurs. 2010;19(9–10):1289–1297. doi:10.1111/j.1365-2702.2009.03151.x
12. Muller S, Kohlmann T, Wilke T. Validation of the adherence barriers questionnaire: an instrument for identifying potential risk factors associated with medication-related non-adherence. BMC Health Serv Res. 2015;15:153.
13. Finlayson K, Edwards HE, Courtney MD. Venous leg ulcer recurrence: deciphering long-term adherence to preventative treatments and activities. Wound Pract Res. 2014;22:84–98.
14. Van Hecke A, Grypdonck M, Beele H, Vanderwee K, Defloor T. Adherence to leg ulcer lifestyle advice: qualitative and quantitative outcomes associated with a nurse-led intervention. J Clin Nurs. 2011;20(3–4):429–443. doi:10.1111/j.1365-2702.2010.03546.x
15. Michie S, Johnston M, Francis JJ, Hardeman W, Eccles M. From theory to intervention: mapping theoretically derived behavioural determinants to behaviour change techniques. Appl Psychol. 2008;57:660–680. doi:10.1111/j.1464-0597.2008.00341.x
16. Allaert FA, Rastel D, Graissaguel A, Sion D, Hamel-Desnos C. Design and evaluation of the psychometric properties of a self-questionnaire on patient adherence to wearing elastic compression stockings. Phleb. 2019;34(1):25–31. doi:10.1177/0268355518762824
17. Benigni JP, Branchoux S, Bacle I, Taieb C. Difficulty associated with donning medical compression stockings: results from a survey comparing two different compression stockings. Womens Health. 2013;9(3):291–300.
18. Clarke-Moloney M, Keane N, O’Connor V, et al. Randomised controlled trial comparing European standard class 1 to class 2 compression stockings for ulcer recurrence and patient compliance. Int Wound J. 2014;11(4):404–408. doi:10.1111/j.1742-481X.2012.01108.x
19. Heinen M, Borm G, van der Vleuten C, Evers A, Oostendorp R, van Achterberg T. The lively legs self-management programme increased physical activity and reduced wound days in leg ulcer patients: results from a randomized controlled trial. Int J Nurs Stud. 2012;49(2):151–161. doi:10.1016/j.ijnurstu.2011.09.005
20. Shannon MM, Hawk J, Navaroli L, Serena T. Factors affecting patient adherence to recommended measures for prevention of recurrent venous ulcers. J Wound Ostomy Continence Nurs. 2013;40(3):268–274. doi:10.1097/WON.0b013e318285081a
21. Chitambira F. Patient perspectives: explaining low rates of compliance to compression therapy. Wound Pract Res. 2019;27(4):168–174.
22. Raju S, Hollis K, Neglen P. Use of compression stockings in chronic venous disease: patient compliance and efficacy. Ann Vasc Surg. 2007;21(6):790–795. doi:10.1016/j.avsg.2007.07.014
23. Brown A. Evaluating the reasons underlying treatment nonadherence in VLU patients: introducing the VeLUSET Part 1 of 2. J Wound Care. 2014;23(1):37,40,42–34. doi:10.12968/jowc.2014.23.1.37
24. Brown A. Two-Component Compression: Concordance, Evidence and Clinical Use. Wounds UK; 2014.
25. Bar L, Brandis S, Marks D. Improving adherence to wearing compression stockings for chronic venous insufficiency and venous leg ulcers: a scoping review. Patient Prefer Adherence. 2021;15:2085–2102. doi:10.2147/PPA.S323766
26. Delamater AM. Improving patient adherence. Clin Diabetes. 2006;24(2):71–77. doi:10.2337/diaclin.24.2.71
27. Pagels AA, Hylander B, Alvarsson M. A multi-dimensional support programme for patients with diabetic kidney disease. J Ren Care. 2015;41(3):187–194. doi:10.1111/jorc.12114
28. Willmott T-TS. Are we speaking the same language? Call for action to improve theory application and reporting in behaviour change research. BMC Public Health. 2021;21(479):2–8.
29. Michie S, Prestwich A. Are interventions theory-based? Development of a theory coding scheme. Health Psychol. 2010;29(1):1–8. doi:10.1037/a0016939
30. McClurg D, Frawley H, Hay-Smith J, et al. Scoping review of adherence promotion theories in pelvic floor muscle training. Neurourol Urodyn. 2015;34(7):606–614. doi:10.1002/nau.22769
31. Ryan P. Integrated theory of health behavior change: background and intervention development. Clin Nurse Spec. 2009;23(3):161–170. doi:10.1097/NUR.0b013e3181a42373
32. McAllister S, Simpson A, Tsianakas V, et al. Developing a theory-informed complex intervention to improve nurse-patient therapeutic engagement employing experience-based co-design and the behaviour change wheel: an acute mental health ward case study. BMJ Open. 2021;11(5):e047114. doi:10.1136/bmjopen-2020-047114
33. Chan K. A design thinking mindset beyond the public health model: design thinking for public health. World Med Health Policy. 2018;10:111–119. doi:10.1002/wmh3.253
34. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
35. French SD, Green SE, O’Connor DA, et al. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implement Sci. 2012;7:38. doi:10.1186/1748-5908-7-38
36. Lippke S, Zielgelmann JP. Theory-based health behaviour change: developing, testing and applying theories for evidence-based interventions. Appl Psychol. 2008;57:698–716. doi:10.1111/j.1464-0597.2008.00339.x
37. Grol RP, Bosch MC, Hulscher ME, Eccles MP, Wensing M. Planning and studying improvement in patient care: the use of theoretical perspectives. Milbank Q. 2007;85(1):93–138. doi:10.1111/j.1468-0009.2007.00478.x
38. McGregor SLT. Understanding and Evaluating Research: A Critical Guide. Thousand Oaks: SAGE Publications Inc; 2019.
39. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implant Sci. 2017;12. doi:10.1186/s13012-017-0605-9
40. De Leo A, Bayes S, Bloxsome D, Butt J. Exploring the usability of the COM-B model and Theoretical Domains Framework (TDF) to define the helpers of and hindrances to evidence-based practice in midwifery. Implement Sci Commun. 2021;2(1):7. doi:10.1186/s43058-020-00100-x
41. West RM, Michie S. A brief introduction to the COM-B model of behaviour and the PRIME theory of motivation. Qeois. 2020. doi:10.32388/WW04E6.22020
42. Moore AP, Rivers CA, Stanton-Fay S, Harding R, Goff LM. Designing the healthy eating and active lifestyles for diabetes (HEAL-D) self-management and support programme for UK African and Caribbean communities: a culturally tailored, complex intervention under-pinned by behaviour change theory. BMC Public Health. 2019;19(1):1146. doi:10.1186/s12889-019-7411-z
43. MacPherson MM, Cranston KD, Locke SR, Bourne JE, Jung ME. Using the behavior change wheel to develop text messages to promote diet and physical activity adherence following a diabetes prevention program. TBM. 2021;11:1593–1595.
44. Herber OR, Atkins L, Stork S, Wilm S. Enhancing self-care adherence in patients with heart failure: a study protocol for developing a theory-based behaviour change intervention using the COM-B behaviour model (ACHIEVE study). BMJ Open. 2018;8(9):e025907. doi:10.1136/bmjopen-2018-025907
45. Gould GS, Bar-Zeev Y, Bovill M, et al. Designing an implementation intervention with the behaviour change wheel for health provider smoking cessation care for Australian indigenous pregnant women. Implement Sci. 2017;12(1):114. doi:10.1186/s13012-017-0645-1
46. Barker F, Lusignan S, Deborah C. Improving collaborative behaviour planning in adult auditory rehabilitation: development of the I-PLAN intervention using the behaviour change wheel. Ann Behav Med. 2018;52(6):489–500. doi:10.1007/s12160-016-9843-3
47. Sinnott C, Mercer SW, Payne RA, Duerden M, Bradley CP, Byrne M. Improving medication management in multimorbidity: development of the MultimorbiditY COllaborative Medication Review And DEcision Making (MY COMRADE) intervention using the Behaviour Change Wheel. Implement Sci. 2015;10:132. doi:10.1186/s13012-015-0322-1
48. Martin G, Pear J. Behavior Modification: What is It and How to Do It.
49. Cassidy C, Steenbeek A, Langille D, Martin-Misener R, Curran J. Designing an intervention to improve sexual health service use among university undergraduate students: a mixed methods study guided by the behaviour change wheel. BMC Public Health. 2019;19(1):1734. doi:10.1186/s12889-019-8059-4
50. Tavender EJ, Bosch M, Gruen RL, et al. Developing a targeted, theory-informed implementation intervention using two theoretical frameworks to address health professional and organisational factors: a case study to improve the management of mild traumatic brain injury in the emergency department. Implement Sci. 2015;10:74. doi:10.1186/s13012-015-0264-7
51. Dyson J, Cowdell F. How is the theoretical domains framework applied in designing interventions to support healthcare practitioner behaviour change? A systematic review. Int J Qual Health Care. 2021;33(3). doi:10.1093/intqhc/mzab106
52. Wenke R, Weir K, Mickan S. What influences allied health clinician participation in research in the public hospital: a qualitative theory-informed approach. BMJ. 2020;10(8):e036183.
53. Kneebone SL, Fielding K. The impact-likelihood matrix: a policy tool for behaviour prioritisation. Environ Sci Technol. 2017;70:9–20.
54. Elven M, Hochwalder J, Dean E, Soderlund A. A clinical reasoning model focused on clients’ behaviour change with reference to physiotherapists: its multiphase development and validation. Physiother Theory Pract. 2015;31(4):231–243. doi:10.3109/09593985.2014.994250
55. Tonelli MR. In defense of expert opinion. Acad Med. 1999;74(11):1187–1192. doi:10.1097/00001888-199911000-00010
56. Berman PS. Case Conceptualization and Treatment Planning: Exercises for Integrating Theory with Clinical Practice. Thousand Oaks: Sage Publications Inc; 1997.
57. Van Hecke A, Grypdonck M, Defloor T. Interventions to enhance patient compliance with leg ulcer treatment: a review of the literature. J Clin Nurs. 2008;17(1):29–39. doi:10.1111/j.1365-2702.2006.01863.x
58. Cheng Q, Gibb M, Graves N, Finlayson K, Pacella RE. Cost-effectiveness analysis of guideline-based optimal care for venous leg ulcers in Australia. BMC Health Serv Res. 2018;18(1):421. doi:10.1186/s12913-018-3234-3
59. Pacella R. Solutions to the chronic wound problem in Australia: a call to action. Wound Pract Res. 2018;26:84–98.
60. Crofton E, Meredith P, Gray P, O’Reilly S, Strong J. Non-adherence with compression garment wear in adult burns patients: a systematic review and meta-ethnography. Burns. 2020;46(2):472–482. doi:10.1016/j.burns.2019.08.011
61. Osborn R, Moulds D, Schneider EC, Doty MM, Squires D, Sarnak DO. Primary care physicians in ten countries report challenges caring for patients with complex health needs. Health Aff. 2015;34(12):2104–2112. doi:10.1377/hlthaff.2015.1018
62. Hendricks S, Conrad N, Douglas TS, Mutsvangwa T. A modified stakeholder participation assessment framework for design thinking in health innovation. Healthc. 2018;6(3):191–196. doi:10.1016/j.hjdsi.2018.06.003
63. Mickan S, Tilson JK, Atherton H, Roberts NW, Heneghan C. Evidence of effectiveness of health care professionals using handheld computers: a scoping review of systematic reviews. J Med Internet Res. 2013;15(10):e212. doi:10.2196/jmir.2530
64. Ventola CL. Mobile devices and apps for health care professionals: uses and benefits. PT. 2014;39(5):356–364.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Influencing Adherence to Dietary Interventions Among Patients with Gestational Diabetes Mellitus in China: A Qualitative Study Based on the COM-B Model
Jia CL, Wang LJ, Li LH, Lu YJ, Yang Y
Journal of Multidisciplinary Healthcare 2025, 18:4653-4663
Published Date: 5 August 2025
Barriers to Adherence to Remote Pelvic Floor Muscle Training Among Postpartum Women: A Qualitative Study Guided by the COM-B Model
Zhou D, Ni X, Ding M, Shi H
Patient Preference and Adherence 2026, 20:612714
Published Date: 22 May 2026