Back to Journals » Patient Preference and Adherence » Volume 17
A Conceptual Model of Home-Based Cardiac Rehabilitation Exercise Adherence in Patients with Chronic Heart Failure: A Constructivist Grounded Theory Study
Authors Yang Z ![]() , Sun L, Sun Y, Dong Y, Wang A
, Sun L, Sun Y, Dong Y, Wang A
Received 10 January 2023
Accepted for publication 21 March 2023
Published 24 March 2023 Volume 2023:17 Pages 851—860
DOI https://doi.org/10.2147/PPA.S404287
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zhen Yang,1 Longfeng Sun,2 Yuanhui Sun,1 Yu Dong,1 Aiping Wang1
1Department of Public Service, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China; 2Department of Geriatrics, The First Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China
Correspondence: Aiping Wang, Department of Public Service, The First Affiliated Hospital of China Medical University, No. 155, Nanjing North Street, Heping District, Shenyang, 110001, Liaoning Province, People’s Republic of China, Tel +86 13998890800, Email [email protected]
Purpose: This study aimed to explore a conceptual model of home-based cardiac rehabilitation exercise adherence and reveal its internal behavioral logic.
Patients and Methods: A constructivist grounded theory design was adopted to explore the conceptual model of home-based cardiac rehabilitation exercise adherence. Semi-structured interviews were completed to collect qualitative data for constructing the conceptual model. The theoretical saturation and validation strategies were adopted to demonstrate the adequacy of qualitative data. A three-level coding procedure with constant comparisons was completed to analyze this qualitative data.
Results: A total of 21 patients with chronic heart failure were recruited in this study. As a result of this study, 32 initial codes, 12 category codes, and four core categories were extracted, namely, seeking supports, rehabilitation exercise, exercise monitoring and information feedback. According to the internal behavioral logic, the conceptual model of home cardiac rehabilitation exercise adherence was finally formed. In this closed-chain model, seeking supports is the initial adherence behavior, and rehabilitation exercise is the core adherence behavior, and exercise monitoring is the key adherence behavior, and information feedback is the driving adherence behavior.
Conclusion: The conceptual model of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure was developed, revealing its internal behavioral logic and providing theoretical references for developing relevant clinical research tools with comprehensive coverage and identifying weak links.
Keywords: cardiac rehabilitation, adherence, qualitative study, conceptual model, quality of life
Introduction
Chronic heart failure is a persistent clinical syndrome caused by abnormal cardiac structure and/or function and confirmed by objective evidence.1 It was reported that the clinical prognostic burden of chronic heart failure, such as disability and adverse cardiovascular events, remains severe despite advances in treatment.2,3 Therefore, it is necessary to explore effective interventions to control chronic symptoms and improve the clinical prognosis for patients with chronic heart failure.
Cardiac rehabilitation is the synthesis of all methods (exercise, nutrition, medicine, psychology and lifestyle) to ensure that patients with heart disease obtain the best physical, mental and social functions and lead an active life through their efforts.4 It was confirmed that exercise-centered cardiac rehabilitation can significantly enhance ventricular remodeling and diastolic function of patients with cardiovascular diseases and improve their clinical prognosis.5–7 Also, cardiac rehabilitation is recommended by various academic organizations as grade IA evidence to enhance cardiac performance.8,9 However, long-term outpatient rehabilitation exercise brings a heavy economic burden due to the chronic nature of the disease.10 As a meaningful alternative model,11–13 the home-based cardiac rehabilitation exercise provides the same benefits as centralized cardiac rehabilitation exercise in improving cardiopulmonary performance, clinical prognosis, and reducing cardiovascular risk.14–16 Also, a series of studies shown that home-based cardiac rehabilitation has a significant cost-effectiveness and can improve exercise endurance and quality of life, promote mental health, and reduce readmission rates in patients with chronic heart failure.17–19
However, these benefits rely on long-term adherence to home-based cardiac rehabilitation exercises. Unfortunately, the proportion of patients with chronic heart failure who are chronically adherent to home-based cardiac rehabilitation exercise is still suboptimal.20 It was reported that only 52% of patients with chronic heart failure participate in home-based cardiac rehabilitation exercise after completing centralized cardiac rehabilitation,21 and reduced adherence to the home-based group compared with the group in supervised training.22 Similarly, due to the chronic nature of the disease and limited exercise endurance, 43% to 63% of patients with chronic heart failure were reluctant to perform routine cardiac rehabilitation exercises.23,24 Long-term (24 months) home-based cardiac rehabilitation exercise adherence was relatively low (34%) even with strict interventions.25 At present, there is no suitable solution to the unsustainability of home-based cardiac rehabilitation exercise due to the lack of a perfect supervision mechanism and unclear influencing factors. Therefore, these findings demonstrate the need to explore the conceptual model of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure to understand its internal behavioral logic.
Home-based cardiac rehabilitation exercise adherence is a complex issue that is not well understood from an individual behavioral perspective. This study aimed to construct an exploratory model of home-based cardiac rehabilitation exercise adherence to explore further its internal behavioral logic. This study may provide a basis for developing clinical research tools with comprehensive coverage and exploring weak links in exercise adherence.
Materials and Methods
Constructivist Grounded Theory
A constructivist grounded theory study exploring a conceptual model of home-based cardiac rehabilitation exercise adherence was conducted from May to August 2022. Symbolic interactionism and pragmatism underpinned this study. Constructivist grounded theory epistemologically emphasizes the interrelationship between researchers and participants to construct shared meaning.26 The humanity of the researchers is considered as part of the research effort by placing the researchers squarely within the methodology to impart acknowledgment of their experience, expertise and values as significant contributors to the process and outcomes. In contrast, the constructivist approach asserts theoretical sensitivity is driven by the rich co-creative experience of participants, researchers, the literature and the data. Based on the experiences and behaviors of participants, this study employs grounded theory to comprehensively understand home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure. Meanwhile, the interactive process and potential consequences of exercise adherence will be discussed and explained.
Participants and Samples
Eligible patients with chronic heart failure participated in the interviews. Inclusion criteria were: (a) 18 years of age or older, and (b) ongoing home-based cardiac rehabilitation. Exclusion criteria were: (a) communication disorders, and (b) mental disorders, and (c) patients who refused to participate in this study. In this study, a total of 21 patients with chronic heart failure participated in semi-structured interviews. Participants covered 9 men and 12 women and ranged in age from 53 to 73 years with a mean age of (61.71±6.98) years. The mean course of disease was (5.19±2.32) years. In terms of education level, there are 5 patients with primary education, 9 patients with secondary education and 7 patients with higher education. In terms of monthly income, there are eight patients with less than 3000 CNY, eight patients with between 3000 CNY and 6000 CNY, and 5 patients with more than 6000 CNY.
Theoretical Saturation and Validation
In the initial phase, purposive sampling was adopted to recruit participants to provide a wealth of information related to the research topic. After initial thematic saturation, the categories were preliminarily formed. In the second phase, theoretical sampling was adopted to collect qualitative data to further elaborate on the categories and attributes. The sampling procedure was stopped when the collected data could not further reveal the core category and attributes, and no new theoretical insights were generated.22 In the third phase, the expert interviews were completed for theoretical saturation validation to ensure the integrity and reliability of the findings. Compared to the previous codes, no new codes emerged.
Study Instruments
Socio-Demographic Characteristics Questionnaire
After a thorough literature review and rigorous panel discussion, the socio-demographic characteristics questionnaire was developed with age, gender, education level, disease duration (year), and monthly income (CNY).
Interview Outline
Based on the existing knowledge of the topic and the purpose of this study, the initial interview outline was developed following a literature review and panel discussion. Subsequently, three eligible patients with chronic heart failure were invited to participate in pre-interviews via a purposive sampling, and the final interview outline was revised and developed (Table 1).
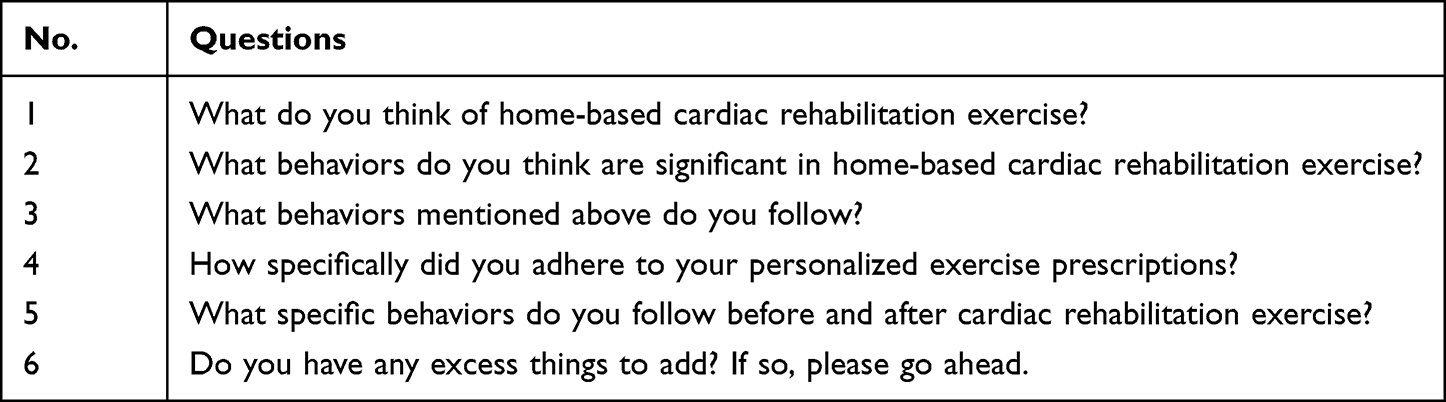 |
Table 1 Interview Outline of This Study |
Research Team
It is generally believed that the interviewers are also powerful tools in the qualitative study.27 Our research team consists of: (a) a female academic professor responsible for study design and quality control, (b) two Ph.D. candidates with expertise in qualitative research (one male and one female) responsible for collecting and analyzing qualitative data, and (c) a female professor with qualitative experience responsible for negotiating and determining coding themes.
Data Collection
In this study, the researchers established good relationships with participants, and the two principal researchers conducted face-to-face semi-structured interviews with the participants. A comfortable interview place was determined with preference of the participants. Also, the researchers informed the participants of the purpose, significance, voluntary nature, and data protection of this study. The researcher sought permission to record the process and assured that these records and transcripts were only available to the research team. After signing formal informed consent, participants were interviewed neutrally. After the interviews, the researchers wrote a reflective diary to improve the interaction process and record the most vivid and emotional thoughts. In this study, interviews and transcripts were conducted in Chinese. The interview transcripts were translated into English by two bilingual experts. To ensure homogeneity, translated texts were reviewed and discussed by the research team.
Data Analysis
In this study, a qualitative analysis procedure consisting of open coding, axial coding and selective coding was completed based on the strategy of constant comparisons and combined with Corbin and Strauss theory.28 In the open coding phase, the transcripts were conceptualized, and the concepts were clustered into subcategories. In the axial coding phase, the relationships among various subcategories were discovered and established as critical categories of axis coding. In the selective coding phase, the interrelationships among the major categories were further interpreted to form the core categories. In this procedure, the differences in coding were rigorously negotiated until a consensus was reached. None of the participants were involved in the data analysis, but the codes were checked by the participants to ensure that they captured the views of the participants. In addition, writing a reflective diary is an effective program to improve the theoretical sensitivity and conceptual ability of the researchers. NVivo 12.0 software was adopted to analyze transcripts and synthesize descriptions.
Rigour
Rigour was demonstrated by the application of four criteria for trustworthiness proposed by Charmaz:29 credibility, resonance, originality, and usefulness. In terms of credibility, writing the reflective diary and following the qualitative guidance improved the credibility of this study. Triangulation of data analysis ensured the reliability of the conceptual categories. In terms of resonance, the codings were validated by experts to ensure theoretical saturation, and the participants received their transcripts for review. In terms of originality, based on the interview outline, the internal behavioral logic of home-based cardiac rehabilitation exercise adherence was explored, and the related theoretical model was developed to extend the existing contents. In terms of usefulness, the internal behavioral logic of home cardiac rehabilitation exercise adherence was adequately described to establish the reproducibility and transferability of this study.
Ethical Consideration
All participants signed an informed consent form after receiving an explanation regarding the purpose and significance of the study, voluntary nature of participation, and the management and protection of data. All procedures were performed in accordance with the 1964 Helsinki declaration. This protocol was approved by the Ethics Review Committee of the First Affiliated Hospital of China Medical University (No. 2021. 503).
Results
The conceptual model of home-based cardiac rehabilitation exercise adherence was formed by three-level coding with continuous comparison (Table 2). The conceptual model has four categories of home-based cardiac rehabilitation exercise adherence, consisting of seeking supports, rehabilitation exercise, exercise monitoring and information feedback. These categories are not parallel, but chained (Figure 1). In this closed-chain model, seeking supports is the initial adherence behavior, and rehabilitation exercise is the core adherence behavior, and exercise monitoring is the key adherence behavior, and information feedback is the driving adherence behavior.
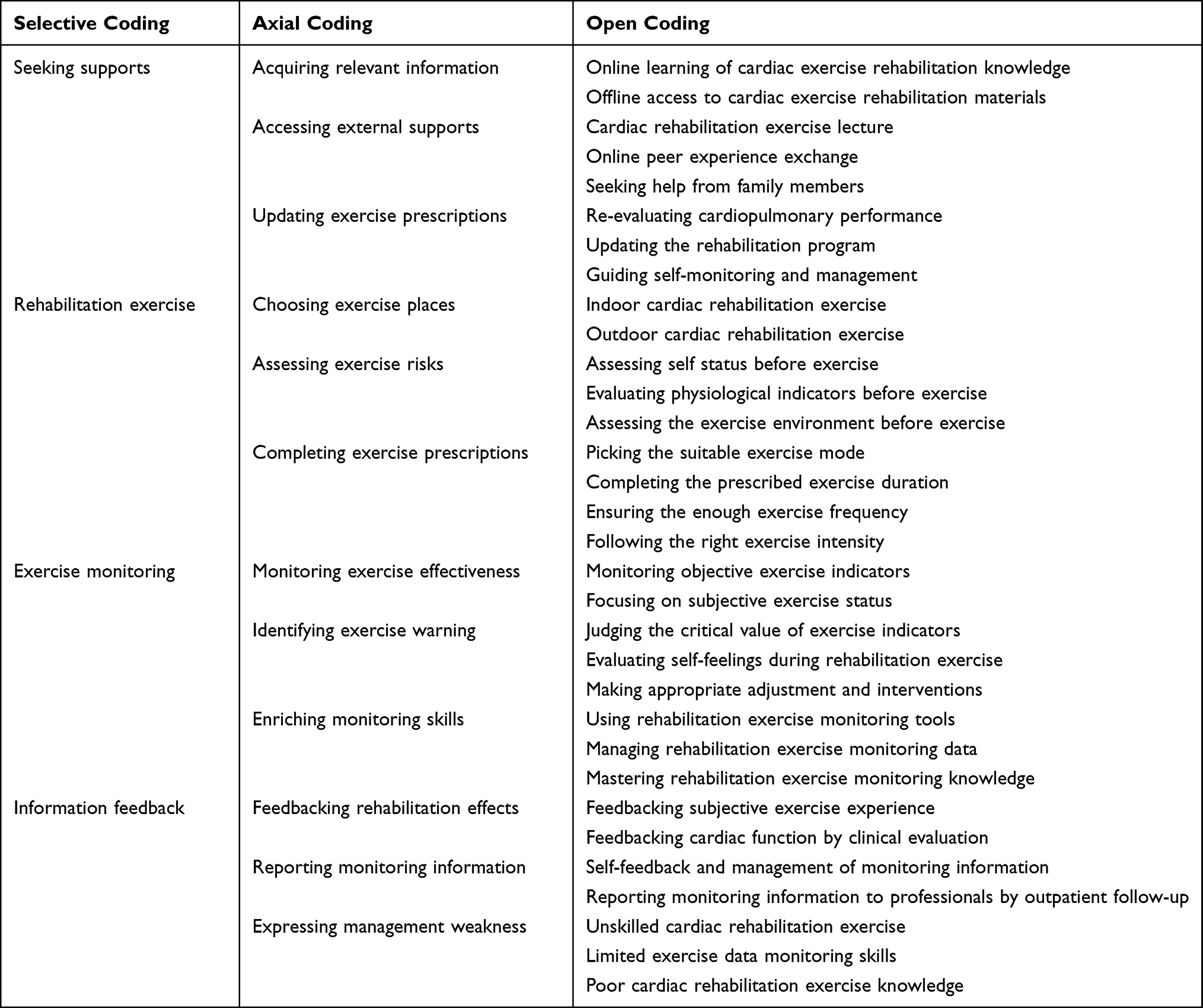 |
Table 2 The Three-Level Coding Result of This Study |
 |
Figure 1 A conceptual model of home-based cardiac rehabilitation exercise adherence. |
Seeking Supports
Patients with chronic heart failure actively seek relevant supports on the home-based cardiac rehabilitation exercise, including consulting relevant materials, obtaining information support, and optimizing exercise prescriptions. In daily life, they searched cardiac rehabilitation materials through online and offline resources to learn cardiac rehabilitation exercise knowledge and strengthen exercise behavior. In addition, they benefited from relevant lectures and information support from peers, and actively carried out cardiac rehabilitation exercise with the help of family members. In outpatient follow-up, they sought cardiac rehabilitation professionals to assess cardiopulmonary performance, guiding home-based self-monitoring and management, and updating their cardiac rehabilitation exercise program.
P:I read relevant books almost daily to enrich my knowledge of diseases. I also make full use of the quality resources on the Internet.
F:I often listen to related disease lectures held by the community to seek some advice, and where I can meet peers to communicate and share with them.
T:I go to the clinic every month to ask the professionals for guidance on home-based self-monitoring, otherwise I would be very worried about whether I am doing it correctly.
B:At each outpatient visit, I seek professionals to optimize my exercise program to achieve home-based cardiac rehabilitation.
Rehabilitation Exercise
As a result of this study, home-based cardiac rehabilitation exercise in patients with chronic heart failure consisted of selecting exercise places, assessing exercise risks, and completing exercise prescriptions. Patients with chronic heart failure choose appropriate exercise places to carry out cardiac rehabilitation exercise according to climate and preferences. In addition, they evaluated exercise risk before exercise, including subjective status, physiological indicators and exercise environments to ensure exercise suitability. As a core adherence behavior, they strictly followed the home-based cardiac rehabilitation exercise program, consisting of exercise intensity, exercise style, exercise duration and exercise frequency.
Q:I will choose a suitable place according to the weather conditions and my preference. If it is sunny, I prefer to do sports outdoors.
K:Before formal exercise, I have to evaluate my subjective state and blood pressure to ensure the safety of exercise. Otherwise, I always feel uneasy.
D:Blood pressure and heart rate are two key indicators that I need to measure before exercise to ensure the suitability and safety of exercise.
I:I will strictly follow the exercise advice given by professionals, including exercise intensity, exercise style and exercise frequency.
Exercise Monitoring
Exercise monitoring is essential for patients with chronic heart failure to ensure exercise safety during home-based cardiac rehabilitation exercise. Patients with chronic heart failure actively monitored objective exercise indicators and subjective exercise status to ensure the effectiveness of home-based cardiac rehabilitation exercise. In addition, to ensure safety, they identified exercise early warning by judging the critical value of exercise indicators and self-feelings during rehabilitation exercise to make appropriate adjustments and interventions. In cardiac rehabilitation exercise, patients constantly enrich their monitoring skills, including using intelligent monitoring tools, managing exercise monitoring data, and mastering exercise monitoring knowledge.
A:I always pay careful attention to my subjective feelings during the exercise. Once I feel uncomfortable, I will stop immediately and ask my family for help.
G:It is very necessary to monitor the exercise data during rehabilitation exercise. Only when I know the indicators of blood pressure and heart rate at any time can I rest assured.
S:I know the outliers of relevant indicators and can timely identify and adjust myself and ask for help in the process of exercise.
N:I often learn exercise monitoring knowledge and master effective monitoring skills and manage exercise data skillfully on the Internet.
Information Feedback
As a result of this study, information feedback is the driving adherence behavior for patients with chronic heart failure, including feedbacking exercise effects, reporting monitoring information and expressing management weakness. They reported monitoring information to professionals during outpatient follow-up and gave themselves feedback to make reasonable adjustments further rehabilitation exercise. In addition, they provided professionals with subjective experiences of rehabilitation exercise, and the rehabilitation exercise effects were confirmed by objective medical evaluation. Also, they expressed the self-management weaknesses to seek relevant advices, including unskilled rehabilitation exercise, limited monitoring skills, and poor exercise knowledge.
E:I usually give professionals feedback on relevant home-based monitoring data to see if they are normal during outpatient visits.
L:I do not know if cardiopulmonary performance is effective based on home cardiac exercise during this period, so cardiopulmonary performance needs to be measured at each regular outpatient visit to ensure the effectiveness of the exercise.
H:I will record relevant monitoring data every time to give myself a feedback after exercise, so as to facilitate self-adjustment and management.
C:I have a poor knowledge and skills of cardiac rehabilitation exercise, so I always give feedback to a professional for advice.
Discussion
In this study, semi-structured interviews were completed to develop a conceptual model of home-based cardiac rehabilitation exercise adherence. Data integration resulted in 4 core categories: (a) seeking supports, (b) rehabilitation exercise, (c) exercise monitoring, and (d) information feedback. Compared with previous studies,30,31 the conceptual model was developed by grounded theory rather than conceptual exploration. It reveals the internal behavioral logic of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure in Chinese culture, which is beneficial to the rational thinking of cardiac rehabilitation professionals.
Seeking supports is an initial positive behavior for improving self-management and adherence.32 According to the knowledge-attitude-behavior theory,33 acquiring and learning relevant disease knowledge in patients with chronic heart failure is conducive to strengthening their belief in cardiac rehabilitation and promoting their cardiac rehabilitation exercise behavior. However, consistent with the findings of related studies,34,35 this active learning behavior only occurred in highly educated patients with chronic heart failure in this study. Therefore, educational supports from cardiac rehabilitation professionals are particularly necessary for patients with chronic heart failure with low education. According to the information-motivation-behavior skills model,36 patients with chronic heart failure significantly benefit from information and family supports in improving home-based cardiac rehabilitation exercise skills and adherence. In regular outpatient follow-up, as the prerequisite for optimizing exercise prescriptions,37 cardiopulmonary evaluation provide strong evidence for exercise endurance and meaningful guidance for self-monitoring and management in patients with chronic heart failure. However, non-adherence to outpatient follow-up and regular cardiopulmonary evaluation seriously affects the effectiveness of home-based cardiac rehabilitation exercise in patients with chronic heart failure.38 At present, educational supports and mHealth intervention may be relatively appropriate solutions.
As the recommended A level evidence, exercise is the core of cardiac rehabilitation.8,9 To ensure exercise safety, it is essential for patients with chronic heart failure to select appropriate home-based exercise venues according to preferences and conditions prior to exercise.39 Also, evaluating exercise risk is a vital guarantee for exercise safety,40 and provides a reliable reference for patients to adjust the appropriate home-based exercise intensity and styles. Therefore, patients with chronic heart failure should evaluate physiological indicators, exercise environment and current states before home-based exercise to ensure the appropriateness of exercise. Home-based cardiac rehabilitation exercise following medical prescriptions is key to ensuring the effectiveness of cardiac rehabilitation. Studies showed that cardiac rehabilitation exercise has significant effects on cardiopulmonary performance and clinical prognosis in patients with chronic heart failure.41,42 However, fewer patients with chronic heart failure are able to comply long-term with rehabilitation exercise prescriptions for many obstacles such as limited means of transportation and heavy financial burden.43,44 Therefore, home-based cardiac rehabilitation exercise based on shared decision-making should be adopted to solve this problem.
Exercise monitoring is the key adherence behavior of home-based cardiac rehabilitation exercise for patients with cardiovascular disease.45 As two crucial self-monitoring forms, monitoring objective indicators with intelligent equipments and focusing on subjective status during exercise can significantly ensure the safety and effectiveness of exercise. However, it was reported that patients with chronic heart failure have poor ability to recognize exercise early warning, and only by judging the critical value of exercise indicators and self-feelings to adopt appropriate exercise intensity during home-based cardiac rehabilitation exercise.46 Accordingly, it is necessary for patients with chronic heart failure to receive the relevant technical supports and education from cardiac rehabilitation professionals to promote the ability to identify exercise risk warnings and adherence behavior. In addition, there are great differences in exercise monitoring among patients with chronic heart failure for the heterogeneity of education level. In a qualitative study, patients with chronic heart failure reported difficulties in using exercise monitoring tools, managing exercise data, and mastering monitoring knowledge during a based on home-based cardiac rehabilitation exercise.47 Therefore, the relevant monitoring training should be completed to improve their exercise monitoring knowledge and self-management ability.
Information feedback is a driving adherence behavior during cardiac rehabilitation exercise, which is beneficial to update exercise program and guide exercise monitoring.48 Outpatient follow-up is one of the basic forms of information feedback. Patients with chronic heart failure provided monitoring information to cardiac rehabilitation professionals for receiving strong supports and guidance during outpatient follow-up. And, the most direct way to demonstrate the effectiveness of home-based cardiac rehabilitation exercise is to assess cardiopulmonary performance through clinical means.48 However, the chronic nature of the disease and economic constraints determine their non-adherence to outpatient follow-up.38 In addition, the subjective rehabilitation experience of patients is helpful for cardiac rehabilitation professionals to make relevant clinical decisions to guide exercise monitoring and self-management. As the intervenable targets, patients with chronic heart failure often have deficiencies in motor skills, data monitoring, and disease knowledge. Addressing these issues depends on awareness of patient adherence to outpatient follow-up, education and support from professionals, and outpatient insurance.
Limitations
This study explored a conceptual model lacking empirical evidence and needs to be continually revised and improved by the quantitative designs in future studies. Theoretical saturation is a relative concept, and with further interviews, the densities and dimensions of the categories of this interpretive understanding might be enriched. In this study, participants ranged in age from 53 to 73, and younger participants were not included. Also, the classification and prognostic indicators of patients with chronic heart failure were not investigated. In future studies, younger patients with chronic heart failure with disease classification and prognostic indicators should be included to complement the results of this study.
Conclusion
In this study, the conceptual model of home-based cardiac rehabilitation exercise adherence was developed, revealing the internal behavioral logic of home-based cardiac rehabilitation exercise adherence in patients with chronic heart failure. In future studies, relevant measurement tools could be developed to assess and identify weak links according to this model, and then to construct intervention programs based on the intervenable targets.
Acknowledgments
The authors are grateful to patients with chronic heart failure who participated in this study, and also to the health providers for their strong support in sampling.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McDonagh TA, Adamo M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2022;24(1):4–131. doi:10.1002/ejhf.2333
2. Lorenzovici L, Bârzan-Székely A, Farkas-Ráduly S, et al. Burden of chronic heart failure in Romania. Healthcare. 2022;10(1):107. doi:10.3390/healthcare10010107
3. Butler J, Djatche LM, Sawhney B, et al. Clinical and economic burden of chronic heart failure and reduced ejection fraction following a worsening heart failure event. Adv Ther. 2020;37(9):4015–4032. doi:10.1007/s12325-020-01456-1
4. Dalal HM, Doherty P, Taylor RS. Cardiac rehabilitation. BMJ. 2015;351:h5000. doi:10.1136/bmj.h5000
5. Lee JH, Kim J, Sun BJ, Jee SJ, Park JH. Effect of cardiac rehabilitation on left ventricular diastolic function in patients with acute myocardial infarction. J Clin Med. 2021;10(10):2088. doi:10.3390/jcm10102088
6. Grall S, Bouteau R, Hamel JF, et al. Left ventricular remodeling in ST-segment elevation myocardial infarction patients with depressed left ventricular ejection fraction after cardiac rehabilitation. JACC Cardiovasc Imaging. 2019;12(5):938–939. doi:10.1016/j.jcmg.2018.11.018
7. Kamiya K, Sato Y, Takahashi T, et al. Multidisciplinary cardiac rehabilitation and long-term prognosis in patients with heart failure. Circ Heart Fail. 2020;13(10):e006798. doi:10.1161/CIRCHEARTFAILURE.119.006798
8. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA guideline for the management of heart failure: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2022;145(18):e895–e1032.
9. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
10. Bakhshayeh S, Sarbaz M, Kimiafar K, Vakilian F, Eslami S. Barriers to participation in center-based cardiac rehabilitation programs and patients’ attitude toward home-based cardiac rehabilitation programs. Physiother Theory Pract. 2021;37(1):158–168. doi:10.1080/09593985.2019.1620388
11. Clark RA, Conway A, Poulsen V, Keech W, Tirimacco R, Tideman P. Alternative models of cardiac rehabilitation: a systematic review. Eur J Prev Cardiol. 2015;22(1):35–74. doi:10.1177/2047487313501093
12. Stefanakis M, Batalik L, Papathanasiou J, Dipla L, Antoniou V, Pepera G. Exercise-based cardiac rehabilitation programs in the era of COVID-19: a critical review. Rev Cardiovasc Med. 2021;22(4):1143–1155. doi:10.31083/j.rcm2204123
13. Antoniou V, Xanthopoulos A, Giamouzis G, et al. Efficacy, efficiency and safety of a cardiac telerehabilitation programme using wearable sensors in patients with coronary heart disease: the TELEWEAR-CR study protocol. BMJ Open. 2022;12(6):e059945. doi:10.1136/bmjopen-2021-059945
14. Imran HM, Baig M, Erqou S, et al. Home-based cardiac rehabilitation alone and hybrid with center-based cardiac rehabilitation in heart failure: a systematic review and meta-analysis. J Am Heart Assoc. 2019;8(16):e012779. doi:10.1161/JAHA.119.012779
15. Schopfer DW, Whooley MA, Allsup K, et al. Effects of home-based cardiac rehabilitation on time to enrollment and functional status in patients with ischemic heart disease. J Am Heart Assoc. 2020;9(19):e016456. doi:10.1161/JAHA.120.016456
16. Ramachandran HJ, Jiang Y, Tam WWS, Yeo TJ, Wang W. Effectiveness of home-based cardiac telerehabilitation as an alternative to Phase 2 cardiac rehabilitation of coronary heart disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29(7):1017–1043. doi:10.1093/eurjpc/zwab106
17. Nagatomi Y, Ide T, Higuchi T, et al. Home-based cardiac rehabilitation using information and communication technology for heart failure patients with frailty. ESC Heart Fail. 2022;9(4):2407–2418. doi:10.1002/ehf2.13934
18. Krishnamurthi N, Schopfer DW, Shen H, Whooley MA. Association of mental health conditions with participation in cardiac rehabilitation. J Am Heart Assoc. 2019;8(11):e011639. doi:10.1161/JAHA.118.011639
19. Batalik L, Filakova K, Sladeckova M, Dosbaba F, Su JJ, Pepera G. The cost-effectiveness of exercise-based cardiac telerehabilitation intervention: a systematic review. Eur J Phys Rehabil Med. 2023. doi:10.23736/S1973-9087.23.07773-0
20. Nielsen J, Duncan K, Pozehl B. Patient-selected strategies for post cardiac rehabilitation exercise adherence in heart failure. Rehabil Nurs. 2019;44(3):181–185. doi:10.1097/rnj.0000000000000127
21. Schopfer DW, Nicosia FM, Ottoboni L, Whooley MA. Patient perspectives on declining to participate in home-based cardiac rehabilitation: a mixed-methods study. J Cardiopulm Rehabil Prev. 2020;40(5):335–340. doi:10.1097/HCR.0000000000000493
22. McKelvie RS, Teo KK, Roberts R, et al. Effects of exercise training in patients with heart failure: the Exercise Rehabilitation Trial (EXERT). Am Heart J. 2002;144(1):23–30. doi:10.1067/mhj.2002.123310
23. Kulnik ST, Sareban M, Höppchen I, et al. Outpatient cardiac rehabilitation closure and home-based exercise training during the first COVID-19 lockdown in Austria: a mixed-methods study. Front Psychol. 2022;13:817912. doi:10.3389/fpsyg.2022.817912
24. Krishnamurthi N, Schopfer DW, Ahi T, et al. Predictors of patient participation and completion of home-based cardiac rehabilitation in the veterans health administration for patients with coronary heart disease. Am J Cardiol. 2019;123(1):19–24. doi:10.1016/j.amjcard.2018.09.024
25. Whellan DJ, O’Connor CM, Lee KL, et al. Heart failure and a controlled trial investigating outcomes of exercise training (HF-ACTION): design and rationale. Am Heart J. 2007;153(2):201–211. doi:10.1016/j.ahj.2006.11.007
26. Charmaz K. Constructing Grounded Theory.
27. Schwarze ML, Kaji AH, Ghaferi AA. Practical guide to qualitative analysis. JAMA Surg. 2020;155(3):252–253. doi:10.1001/jamasurg.2019.4385
28. Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual Sociol. 1990;13:3–21. doi:10.1007/BF00988593
29. Charmaz K. Constructing Grounded Theory: A Practical Guide Through Qualitative Analysis. London: Sage Publications; 2006.
30. Niebauer J, Mayr K, Tschentscher M, Pokan R, Benzer W. Outpatient cardiac rehabilitation: the Austrian model. Eur J Prev Cardiol. 2013;20(3):468–479. doi:10.1177/2047487312446137
31. Grace SL, Turk-Adawi KI, Contractor A, et al. Cardiac rehabilitation delivery model for low-resource settings. Heart. 2016;102(18):1449–1455. doi:10.1136/heartjnl-2015-309209
32. Ma C, Yang Q, Huang S. Translation and psychometric evaluation of the Chinese version of the information needs in cardiac rehabilitation tool. J Cardiopulm Rehabil Prev. 2019;39(5):331–337. doi:10.1097/HCR.0000000000000411
33. Williamson TM, Rouleau CR, Aggarwal SG, Arena R, Hauer T, Campbell TS. The impact of patient education on knowledge, attitudes, and cardiac rehabilitation attendance among patients with coronary artery disease. Patient Educ Couns. 2021;104(12):2969–2978. doi:10.1016/j.pec.2021.04.024
34. Jankowski P, Pajak A, Lysek R, et al. Cardiac rehabilitation in real life. Medicine. 2015;94(32):e1257. doi:10.1097/MD.0000000000001257
35. Zhou Y, Li J, Du S, et al. Cardiac rehabilitation knowledge in patients with coronary heart disease in Baoding city of China: a cross-sectional study. Int J Nurs Sci. 2017;4(1):24–28. doi:10.1016/j.ijnss.2016.12.011
36. Li M, Zhu H. Application of intervention of information motivation behavior skill (IMB) model in the cardiac rehabilitation of patients with coronary heart disease. Pak J Med Sci. 2022;38(6):1627–1632. doi:10.12669/pjms.38.6.5721
37. Achttien RJ, Staal JB, van der Voort S, et al. Exercise-based cardiac rehabilitation in patients with chronic heart failure: a Dutch practice guideline. Neth Heart J. 2015;23(1):6–17. doi:10.1007/s12471-014-0612-2
38. Ozemek C, Squires RW. Enrollment and adherence to early outpatient and maintenance cardiac rehabilitation programs. J Cardiopulm Rehabil Prev. 2021;41(6):367–374. doi:10.1097/HCR.0000000000000645
39. Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. 2022;55:117–126. doi:10.1016/j.hrtlng.2022.04.016
40. Lelis JD, Chaves G, Ghisi GLM, Grace SL, Britto RR. validity of the incremental shuttle walk test to assess exercise safety when initiating cardiac rehabilitation in low-resource settings. J Cardiopulm Rehabil Prev. 2019;39(3):E1–E7. doi:10.1097/HCR.0000000000000412
41. Bozkurt B, Fonarow GC, Goldberg LR, et al. Cardiac rehabilitation for patients with heart failure: JACC Expert Panel. J Am Coll Cardiol. 2021;77(11):1454–1469. doi:10.1016/j.jacc.2021.01.030
42. Chen YW, Wang CY, Lai YH, et al. Home-based cardiac rehabilitation improves quality of life, aerobic capacity, and readmission rates in patients with chronic heart failure. Medicine. 2018;97(4):e9629. doi:10.1097/MD.0000000000009629
43. Park LG, Schopfer DW, Zhang N, Shen H, Whooley MA. Participation in cardiac rehabilitation among patients with heart failure. J Card Fail. 2017;23(5):427–431. doi:10.1016/j.cardfail.2017.02.003
44. Rengo JL, Savage PD, Barrett T, Ades PA. Cardiac rehabilitation participation rates and outcomes for patients with heart failure. J Cardiopulm Rehabil Prev. 2018;38(1):38–42. doi:10.1097/HCR.0000000000000252
45. Medina Quero J, Fernández Olmo MR, Peláez Aguilera MD, Espinilla Estévez M. Real-time monitoring in home-based cardiac rehabilitation using wrist-worn heart rate devices. Sensors. 2017;17(12):2892. doi:10.3390/s17122892
46. Scotto CJ, Waechter D, Rosneck J. Patients’ perception of monitoring during cardiac rehabilitation: taking the message home. J Nurs Care Qual. 2009;24(3):263–268. doi:10.1097/01.NCQ.0000356909.79829.4e
47. Busnatu ȘS, Pană MA, Lăcraru AE, et al. Patient perception when transitioning from classic to remote assisted cardiac rehabilitation. Diagnostics. 2022;12(4):926. doi:10.3390/diagnostics12040926
48. Gude WT, van Engen-Verheul MM, van der Veer SN, de Keizer NF, Peek N. How does audit and feedback influence intentions of health professionals to improve practice? A laboratory experiment and field study in cardiac rehabilitation. BMJ Qual Saf. 2017;26(4):279–287. doi:10.1136/bmjqs-2015-004795
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Support Life Club: A New Model Based on Social Media Group Chats and Social Activities That Can Improve Adherence and Clinical Outcomes in Patients Receiving Cardiac Rehabilitation
Zhang S, Zuo H, Meng X, Hu D
Patient Preference and Adherence 2022, 16:1907-1917
Published Date: 3 August 2022
Quality of Life and Adherence to Healthcare Services During the COVID-19 Pandemic: A Cross-Sectional Analysis
Hassan SUN, Zahra A, Parveen N, Khatoon F, Bangi NA, Hosseinzadeh H
Patient Preference and Adherence 2022, 16:2533-2542
Published Date: 13 September 2022
Can Pharmacists’ Counseling Improve the Use of Inhalers and Quality of Life? A Prospective “Pre” and “Post” Education Analysis in Mardan, Pakistan
Gul S, Rehman IU, Goh KW, Ali Z, Rahman AU, Khalil A, Shah I, Khan TM, Ming LC
Journal of Asthma and Allergy 2023, 16:679-687
Published Date: 6 July 2023
Predictive Models of Psychological Distress, Quality of Life, and Adherence to Medication in Breast Cancer Patients: A Scoping Review
Pezzolato M, Spada GE, Fragale E, Cutica I, Masiero M, Marzorati C, Pravettoni G
Patient Preference and Adherence 2023, 17:3461-3473
Published Date: 19 December 2023
Adherence to Cardiac Rehabilitation in Patients with Acute Myocardial Infarction After PCI: A Scoping Review
Li P, Zhang W, Wu B
Journal of Multidisciplinary Healthcare 2024, 17:4165-4176
Published Date: 28 August 2024