Back to Journals » Clinical Interventions in Aging » Volume 20
Balance and Gait Disorders in the Aged Population. Causes, Assessment and Management: A Literature Review
Authors Manckoundia P ![]() , Mourey F
, Mourey F ![]() , Larosa F, Renoncourt T
, Larosa F, Renoncourt T ![]()
Received 29 March 2025
Accepted for publication 26 August 2025
Published 11 November 2025 Volume 2025:20 Pages 1945—1962
DOI https://doi.org/10.2147/CIA.S531235
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Patrick Manckoundia,1,2 France Mourey,2 Fabrice Larosa,1 Thomas Renoncourt1,2
1Université Bourgogne Europe, CHU Dijon Bourgogne, Internal Medicine Geriatrics, Dijon, France; 2Université Bourgogne Europe, INSERM, CAPS UMR 1093, Dijon, France
Correspondence: Patrick Manckoundia, Service de Médecine Interne Gériatrie, Hôpital de Champmaillot CHU Dijon Bourgogne, 2, rue Jules Violle, Dijon Cedex, 21079, France, Tel +33 3 80 29 39 70, Email [email protected]
Abstract: With aging, compensatory mechanisms and physiological reserve may become insufficient to maintain balance and gait (BG), particularly when associated with stroke, Alzheimer’s disease, diabetes, osteoarticular diease, vestibular disorders, orthostatic hypotension (OH), heart rhythm disorders, or drug side effects. This leads to poorer postural-motor function and increased risk of falling (RoF). This review aims to highlight recent scientific advancements relative to BG disorders (BGDs) for gerontology professionals. When assessing older adults (OAs) with BGDs, a thorough assessment of patient history is needed to identify the origins. This should include the history of falls, an inventory of medications, and an analysis of the home environment. A comprehensive clinical examination is also required to guide etiological diagnoses. A clinical suspicion of cardiac arrhythmia/conduction disorders, for example, will be confirmed by electrocardiogram (ECG)/Holter ECG, whereas suspected OH (on questioning) will be confirmed by an OH test, and, in the presence of confusion, epilepsy will be confirmed by the electroencephalogram. Several tools, ranging from simple and quick to more complex and thorough, have been validated to evaluate BGDs in OAs. These tests involve activities of daily living tasks required to preserve independence. Emerging technologies for RoF assessment (ie, surface electromyography, force platforms, three-dimensional motion capture systems) while not yet used in routine geriatric practice, can improve early detection, monitoring, and rehabilitation. Optimal BGD management requires the implication of several health professionals. Rehabilitation programs such as the “Otago exercise programme” and “falls management exercise” have been validated. Assistive technologies (canes, walkers, grab bars, and orthopedic footwear or automated alert systems), and new technologies (virtual reality) can also be used. Additional steps include medication review and deprescribing, occupational therapy and home environment adaptations. Understanding and managing BGDs in OAs remains a major public health issue, and is vital for preserving independence in later life.
Keywords: balance, gait, posture, older adult, central nervous system
Introduction
Although with aging, balance and gait (BG) may become less efficient,1,2 older adults (OAs) can maintain adequate BG thanks to compensatory mechanisms and physiological reserve in the absence of chronic or acute disease. However, when aging is combined with illness, these reserves may become insufficient, leading to a breakdown of postural and locomotor functions and increasing the risk of falling (RoF). This concept, in which functional decompensation occurs once a threshold of insufficiency is surpassed, is known as the Bouchon model.3
Considering the importance of BG for maintaining independence, we propose a focused and updated overview of these disorders in OAs.1 Beyond summarizing established knowledge, we have highlighted recent advances in clinical assessment and multidisciplinary management. This includes both well-established clinical tests and recent digital tools such as sensor-based systems and wearable technologies that enhance diagnostic precision and RoF prediction.
This study aims to provide gerontology professionals with the latest scientific advances, particularly in the assessment and management of balance and gait disorders (BGDs). This includes both well-established clinical tests and more recent digital tools such as sensor-based systems and algorithmic approaches aimed at improving diagnostic accuracy and prediction of falls.
Methods
In this narrative review, we draw on foundational texts in geriatric practice and supplement our discussion with recent literature (<5 years) in English or French. In order to do so, we performed a targeted search using PubMed, ScienceDirect and Google Scholar. However, when specific clinical tools or interventions had not been robustly studied within this timeframe, key references published before 2020 were also included. Particular attention was given to major international guidelines.
Physiology of Balance and Gait
The simultaneous and coordinated action of afferents, the central nervous system (CNS) and effectors is essential for maintaining balance and walking.
As shown in Figure 1, the afferents provide individuals with information about their environment and position therein. They are also involved in perception and regulation of balance. They comprise the following three types of receptors:4
- Proprioceptive receptors, present in the muscles, joint capsules, skin and trunk,5,6 inform the CNS of the position and movements in space of body parts.6,7
- Vestibular receptors, located in the inner ear, which include the semicircular canals, informing the CNS of angular movements of the head and body, as well as the otoliths (utricle and saccule) providing information on linear accelerations and verticality (of the head and body).5–7 As with the proprioceptive system, this information allows balance to be controlled at multiple hierarchical levels of the CNS.4 Unlike the otoliths which affect balance and postural control, the semicircular canals are not involved in postural control.5
- Visual receptors, located in the retina, inform the CNS of the individual’s position in space and the environment.6 In addition to sophisticated analysis of the image generated (exteroceptive function), the central retina also controls the position of body segments during fine movements, while the peripheral retina analyzes the movement.5,6 Ultimately, due to its unique property as a telereceptor, the visual system allows for various actions including anticipation, obstacle avoidance and navigation, informing the CNS about body movements and postural oscillations.7
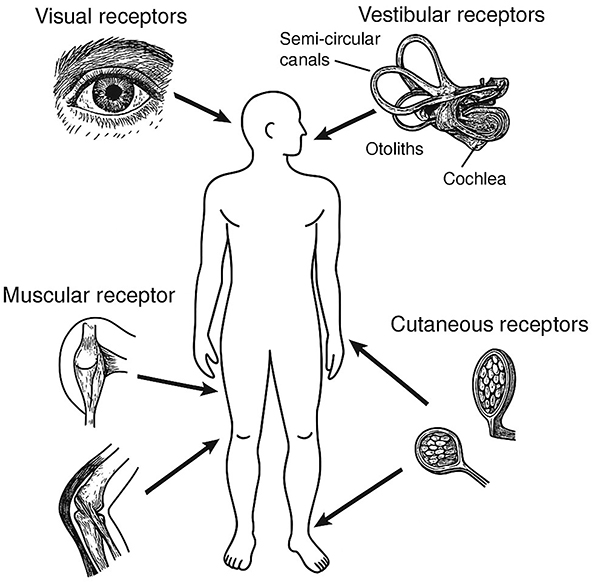 |
Figure 1 Sensory receptor involved in kinesthesia. From Berthoz A., *Le Sens du Mouvement* © Odile Jacob, 1997.8 |
The CNS receives messages from the afferents, which it processes.7 It then orders the effectors to perform various actions to maintain or adapt a posture, balance or walking by inducing, through the pyramidal and extrapyramidal pathways, motor reflexes stabilizing the gaze (visio-oculomotor and vestibulo-oculomotor reflexes) and posture (vestibulospinal reflexes). In addition to these reflexes, there are voluntary cognitive responses that allow the body to be sheathed and stabilized in a normal position.6,9 Each part of the CNS has a specific role within this organization (Table 1).
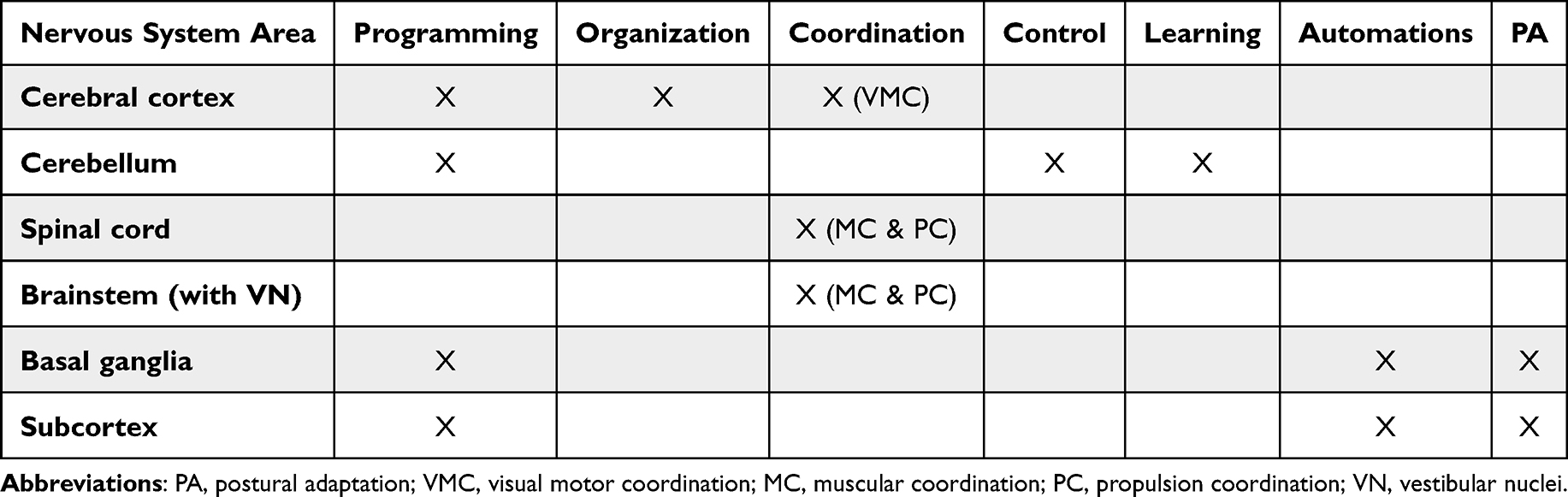 |
Table 1 Involvement of Different Components of the Central Nervous System in Maintaining or Adapting Posture, Balance and Walking |
The effectors are the third element of the system, comprising the muscles and skeleton (including the joints). They receive instructions from the CNS by the nerve impulse transiting through the somatic efferent pathways.6
The integrity of afferents, the CNS and effectors, essential for the precise and fine organization of BG, can decline with aging and be affected more or less severely by various pathological conditions.
Aging of Balance and Gait Functions
Even in the absence of associated pathologies, aging can have a negative impact on BG. Although the functional reserve diminishes, the threshold of insufficiency is never reached by aging alone.3
Afferent Nervous System Aging
With age, proprioceptive acuity decreases. Muscle spindles and joint mechanoreceptors, particularly Pacinian corpuscles, show marked reductions in density and conduction speed. Quantitative histological studies report that the number of Pacinian corpuscles may decrease by more than 30% at age 80, whereas the reduction of Ruffini endings is limited to approximately 10–15%.9 This relatively good preservation may explain why some low-threshold tactile feedback is maintained in advanced age, although integration at the cortical level remains impaired.10 Similar age-related degradation is observed in other proprioceptors, such as Golgi tendon organs located in the musculotendinous junction and sensitive to muscle contractions, and which show an estimated 30% decline in sensitivity. These organs are also found in muscle spindles, which are sensitive to muscle lengthening and exhibit a reduction of up to 30% in stretch reflex response with aging.9 Cutaneous receptors also exhibit a measurable decrease in both the size and functional efficiency of Pacinian and Meissner corpuscles over time, while Ruffini endings are less affected. These alterations degrade afferent encoding, resulting in delayed, low-amplitude or noisy sensory nerve signals, which become increasingly insufficient for accurate postural regulation in complex environments.11
Even without a vestibular condition, aging leads to a progressive loss of vestibular function. Vestibular hair cells are reduced by 20% to 40% after age 70, and there is a decrease in the number of nerve fibers and a decline in vestibular reflex efficiency.11,12 These changes impair the ability to stabilize the body during head movements or postural transitions.
In addition to presbyopia, aging induces anatomical and functional changes in the retina and visual pathways, increasing susceptibility to age-related eye diseases. Cataracts affect more than 70% of individuals over 75, while age-related macular degeneration affects 11–13% and glaucoma 7%.11 These conditions contribute to impaired visual acuity and field, damaged motion perception, reduced accommodation capacity, and decreased contrast sensitivity.5,6,13,14 Half of OAs experience decreased contrast sensitivity, which doubles the risk of recurring falls.15 These visual deficits interfere with anticipatory adjustments, obstacle detection, spatial navigation, and the CNS’s integration of body movement and postural sway, thereby promoting balance disorders.
Aging of the Central Nervous System
With age, the CNS undergoes structural and functional changes that profoundly affect postural control and gait regulation. Neuroimaging studies have shown progressive brain atrophy, particularly in the prefrontal cortex, basal ganglia, cerebellum and supplementary motor areas, which are all essential for motor planning, sensorimotor integration and postural adaptation.11 White matter hyperintensity, observed in up to 90% of OAs, impairs the transmission of signals between motor and sensory regions, contributing to slower reaction times and less efficient balance correction strategies.16 Functionally, aging leads to reduced neural plasticity, decreased motor unit recruitment and less automatic gait control, resulting in a higher reliance on attentional and executive resources for walking.17 This contributes to the “cognitive-motor interference” phenomenon, in which OAs exhibit disproportionate gait slowing or instability during dual-task conditions.11 In addition, there is evidence of impaired central sensory integration, with the CNS showing decreased ability to reweight sensory input in response to changing environmental demands.9 This reduced adaptability contributes to increased postural sway, delayed compensatory steps, and decreased ability to recover from perturbations.6
Impact of Aging on Effectors
Changes in muscle quality, including increased fat and decreased myocytes, associated with sarcopenia, all worsened by aging, are harmful for BG, especially as they can be exacerbated by a sedentary lifestyle and malnutrition.18 Osteoporosis, which increases in prevalence with age, exerts an indirect impact on BG primarily through structural and neuromuscular mechanisms. Vertebral compression fractures and associated hyperkyphosis are associated with a doubled RoF in OAs [odds ratio (OR)=2.1].19 These postural alterations shift the body’s center of mass forward and limit joint range, impairing anticipatory and reactive postural responses. Controlled trials show that women with osteoporosis-related kyphosis exhibit significantly greater mediolateral sway, reduced anteroposterior displacement, and slower gait velocities compared to controls.20 Furthermore, osteoporosis frequently coexists with sarcopenia (“osteosarcopenia”) which amplifies deficits in muscle strength and balance. Osteosarcopenic OAs have a 1.5 fold increased the RoF and fractures compared to those without.21 Muscle weakness associated with sarcopenia compromises postural stability and corrective muscle responses, particularly after destabilization. Lastly, fear of falling and concern over possible fractures often lead to reduced physical activity, resulting in deconditioning and reduced functional reserve, which further impairs gait and balance.10,22
Causes of Balance and Gait Disorders in Older Adults
BGDs reflect a dysfunction in the postural and motor regulation system secondary to certain pathological conditions, which have more pronounced effects in aging organisms. The main causes of BGDs are:
- Neurological pathologies that may be:
- Central: Stroke can lead to postural asymmetry, ataxia, and executive dysfunction, all of which limit adaptive responses. Alzheimer’s disease and related disorders cause executive, attentional, and visuospatial deficits, impairing navigation and postural anticipation. Cerebellar syndromes disrupt motor coordination and gait regularity. Normal-pressure hydrocephalus typically results in a magnetic gait, reduced postural adjustments, and frontal lobe dysfunction. Parkinsonian syndromes interfere with movement and postural adjustments through akinesia, axial rigidity, and delayed motor responses.1,6,23–26
- Or peripheral: The leading cause is diabetes, which induces a length-dependent sensory neuropathy that impairs plantar proprioception and delays postural corrections. Amyloidosis can cause a severe mixed axonal neuropathy, often with autonomic involvement. Both hypothyroidism and hyperthyroidism are associated with sensory or sensorimotor neuropathies through metabolic or immune-mediated mechanisms. Osteomalacia, particularly when related to severe vitamin D deficiency, leads to proximal muscle weakness and pain, impairing motor control. Deficiencies in vitamins B1, B6, or B12 can cause painful or proprioceptive sensory neuropathies, altering gait. Chronic exposure to alcohol or toxins (lead, solvents) is also implicated. Finally, lumbar stenosis causes neurogenic claudication, intermittent leg weakness and sensory loss, worsened by walking and relieved by rest.27–33
- (Neuro)muscular disorders, including myopathies and myositis, may result from dysthyroidism, osteomalacia or medication use.29,30,32–34 These conditions typically degrade gait through proximal weakness, reduced endurance, and impaired postural control. Malnutrition contributes to muscle wasting and worsens sarcopenia. Myasthenia gravis affects gait through muscle fatigability, while polymyalgia rheumatica causes pain, stiffness and fatigue in the pelvic girdle, limiting walking capacity.35,36
- Osteoarticular pathologies, including osteoarthritis, kyphosis, laxity of the lower limbs, osteoporosis, stiffness of the ankles or deformation of the feet (hallux valgus, hallux rigidus, claw toe, quintus varus, rheumatoid arthritis), degrade proprioception and cause chronic pain altering postural adaptation reflexes and modifying motor patterns.1,6,22
- Eye pathologies including cataracts, age-related macular degeneration or glaucoma (promoted by aging), particularly when there is a decrease in visual acuity and field.14
- Vestibular disorders such as toxic vestibular neuritis, Meniere’s disease or benign paroxysmal positional vertigo.23,37
- Cardiovascular pathologies, which promote a decrease in cerebral blood flow with or without discomfort, including arterial hypotension, particularly orthostatic hypotension (OH), cardiac arrhythmia, conduction disorders, sequelae of myocardial infarction or pulmonary embolism.1,6,38
- Deconditioning due to reduced physical activity may be secondary to various pathological conditions including depression, malnutrition, thyroid dysfunction, heart failure, respiratory failure and anemia.1,6
- Drugs that cause 1) low cerebral blood flow due to hypotension, bradycardia or cardiac rhythm disturbances, including antihypertensives, psychotropic medications, antiarrhythmics, acetylcholinesterase inhibitors or memantine,38–40 2) hypovigilance, including psychotropic medications,38 or 3) neuropathies or (neuro)muscular disorders, including corticosteroids, chloroquine/hydroxychloroquine, cimetidine, fibrates, statins, colchicine, D-penicillamine, certain antibiotics, beta-blockers, cyclosporine, certain anticonvulsants, certain chemotherapies or other molecules.30,34
- Toxins, including from alcohol use disorders.30
In OAs with motoric cognitive risk syndrome, although there are no objective cognitive or BG disorders, except gait speed decrease, there is an increased RoF.41
Assessment of Balance and Gait Disorders
BGDs affect independence and are associated with RoF, and the physical, psychological and social consequences of these disorders can have a functional or even vital effect. While BGDs can be relatively easy to diagnose thanks to the physical examination, the etiological diagnosis is more complex and requires a careful investigation including questioning the patient, a meticulous clinical examination, and relevant paraclinical examinations.
Detailed Interview
The anamnesis of OAs with BGDs and their close entourage aims to reconstruct as best as possible the chronology of events by specifying potential triggering factor(s) (illness, medication, stress, etc) and the context, which is often neglected but can make a valuable contribution. In addition to the age and onset (sudden or progressive) of the disorders, the personal and family history, especially neurological, osteoarticular, cardiovascular, ophthalmological, otolaryngological and BG, will be collected. The review of medications must be thorough, including treatments consumed through self-medication and any recent changes. Particular attention should be paid to well-recognized fall-risk–increasing drugs (FRIDs), such as benzodiazepines, antipsychotics, antidepressants, opioids, anticholinergics, antiepileptics, diuretics, alpha-blockers, and beta-blockers. These drugs may contribute to falls by inducing sedation, OH, balance disorders, slowed reaction time, and cognitive dysfunction.16,42,43 The use of at least one FRIDs has been shown to increase the incidence of falls by 13%, and by up to 22–33% for individuals taking multiple FRIDs.43 Several tools are available to assist clinicians in identifying potentially inappropriate medications, such as the STOPP/START criteria, the Beers criteria, or the REMEDI[e]S list.44–46 An history of falls (number and circumstances over the past 12 months) should be systematically obtained.47 Particular attention should be paid to so-called “near-falls”, defined as a loss of balance that does not result in a fall, which are increasingly recognized as strong predictors of future injurious falls. They often reflect declining postural reserves and subclinical gait impairment. Identifying near-falls allows for early detection of instability and therefore prevention of full-blown falls. The individual will be asked about their ability to rise from the floor. The interview will investigate the symptoms associated with BGDs, such as feelings of dizziness, nausea, lower limb weakness or postural instability.11 Footwear should be examined, as inappropriate/worn shoes may contribute to instability.15 In addition, an assessment of cognitive state and mood is crucial to detect even subtle depressive symptoms or cognitive impairment, which may exacerbate gait or balance difficulties.41 Broader functional status should be evaluated using activities of daily living (ADLs) and instrumental ADLs (IADLs). The use of a walking aid (cane, walker) or fall monitoring (alarm system, connected watch, videosurveillance) should be recorded,48 as should the presence of family/caregivers.47
Clinical Exam
The clinical examination is essential and should be as exhaustive as possible, emphasizing certain aspects described in Table 2.
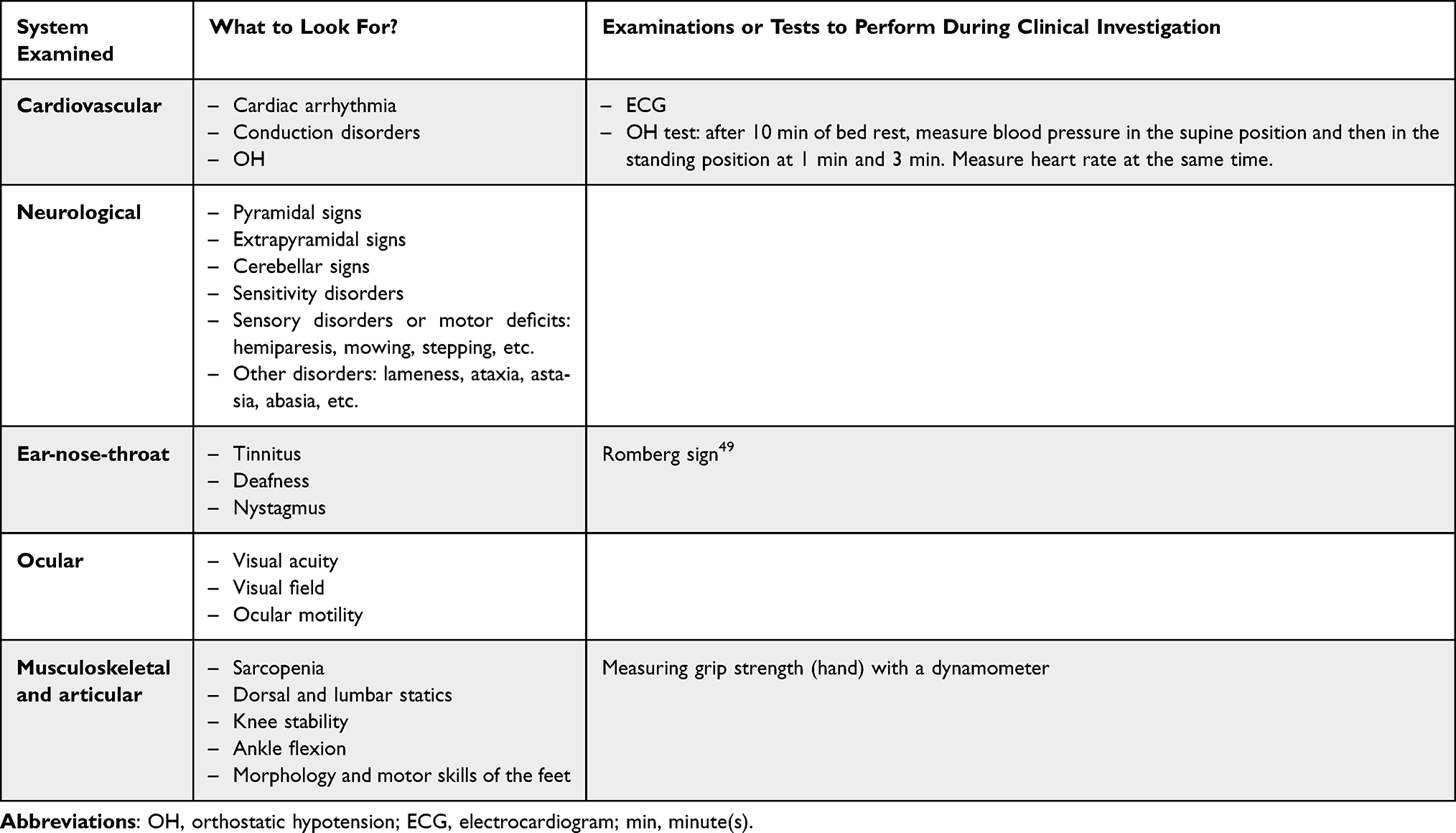 |
Table 2 Clinical Examination of Older Adult with Balance and/or Gait Disorders |
According to the results of the interview and clinical examination, additional paraclinical examinations may be relevant, including imaging. In case of a fall accompanied by prodromes, a cardiac cause (rhythm disorder, conduction disorder, etc) should be ruled out first with an electrocardiogram (ECG), supplemented by a Holter ECG (≥24 hours). An OH test can then be performed, OH being frequent and the cause of repeated falls. Repeated falls with abnormal movements or confusion indicate the need to perform an electroencephalogram to rule out epilepsy, which can be non-convulsive in OAs. A lesion of the CNS may also be suspected in case of confusion, requiring a brain computed tomography scan.
Posture and Motor Skills Assessment
Numerous clinical tests have been developed to assess balance, gait, and RoF in OAs. These tools, presented in Table 3 and Table 4 (for the mini motor test (MMT)) differ in their clinical objectives, time constraints, and diagnostic value.6,26,41,48–80
 |
Table 3 Tests That Can Be Used to Assess Balance and Gait in Older Adults |
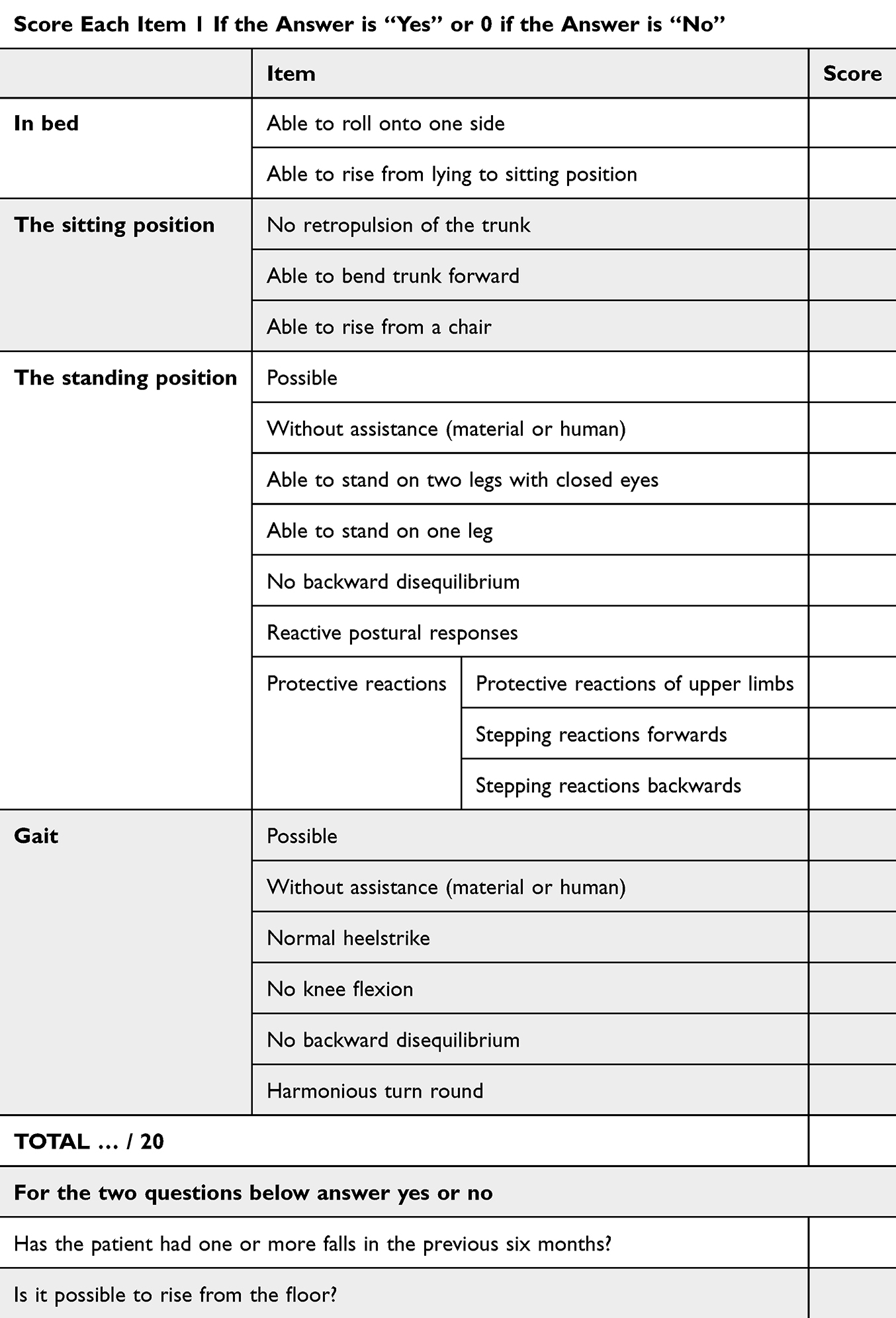 |
Table 4 The Mini Motor Test |
Emerging Technologies for Risk of Falling Assessment
Many technological tools have been developed to complement the clinical assessment of gait and balance disorders. These devices provide objective, reproducible, and sensitive measurements, capable of detecting subtle alterations in postural control or motor coordination that may be invisible during standard clinical evaluation.
- Surface electromyography (EMG) is used to analyze the timing and coordination of muscle group activation, particularly during anticipatory postural adjustments, gait initiation, and balance recovery strategies. Altered EMG patterns, such as delayed activation of ankle stabilizing muscles, have been observed in older adults compared to younger individuals, with average delays ranging from 30 to 120 ms depending on the muscle group involved.81 However, its use in routine clinical practice appears of limited practical value.
- Force platforms, either static or dynamic, measure center-of-pressure (CoP) displacement. Metrics such as total path length (>400 mm) or CoP velocity are robust predictors of RoF: a longer path length is associated with a 75% increase in the RoF, with an 8% rise per additional 10 mm.82 More recently, Liang et al demonstrated that combining CoP data with machine learning algorithms allows RoF classification based on the timed-up and go (TUG) test with an accuracy of 80–90% in older adults.83 However, predictive models remain difficult to generalize due to heterogeneous testing protocols.82
- Three-dimensional motion capture systems (eg, Vicon®) provide precise spatiotemporal and kinematic gait parameters under a variety of conditions. In a 2025 study involving 18 older adults, Vicon analysis showed that obstacle crossing significantly reduced gait speed (+15%) and increased head motion (+20%), negatively affecting postural stability.84 Visual search tasks were also shown to reduce speed, shorten step length (–8%), and decrease hip extension.84 These technologies can identify some of the fine markers of RoF that often elude traditional clinical examination.
- Wearable sensors (inertial measurement units, accelerometers, gyroscopes, or portable equivalents of Vicon®) can now be integrated into accessible devices such as smartphones and smartwatches. These systems provide objective gait data under real-life and extended conditions. One study showed that a single IMU sensor worn for one minute of walking could predict RoF with an accuracy of 81.6% in older adults.85 Smartphone-integrated systems also demonstrated good correlation with clinical reference standards for gait speed, stride regularity, and postural transitions.86 These tools enable remote, autonomous, and repeated assessments over time, helping to monitor subtle motor changes and support early intervention.
Although not yet widely adopted in routine geriatric practice, these tools are a major advance in the early detection of RoF, long-term monitoring, and personalized rehabilitation.
Management of Balance and Gait Disorders in Older Adults
The management of BGDs in OAs requires a coordinated multidisciplinary approach involving physicians, nurses, physiotherapists, occupational therapists, psychomotor therapists, and psychologists. Physicians evaluate underlying medical causes, prescribe appropriate interventions, and coordinate care programs. Nurses and nursing assistants contribute to clinical monitoring (including treatment) and daily support of OAs, as well as the prevention of risks related to BGDs (including patient education). Physiotherapists lead physical exercises and train gait, posture and balance. Occupational therapists assess functional capacities and adapt the home environment. Psychomotor therapists work on coordination, body schema, and movement safety. Psychologists are involved in the management of associated cognitive disorders and post-fall anxiety. This integrated model is built on targeted, evidence-based, and personalized strategies adapted to the patient’s needs and capacities.47 The key message here is the importance of multifactorial interventions, as no isolated approach has proven effective in preventing falls and their consequences.47
Important aspects of management are:
- Medication review and deprescribing: reducing FRIDs is a priority. A structured deprescribing approach has been shown to reduce RoF by 14% when included in a comprehensive management program.11,16 A collaborative process involving the patient, pharmacist, general practitioner, and geriatrician improves adherence: a recent study reported, for the first time, a 3-month maintenance rate of 86% for treatment changes following a joint discussion.87
- Physical exercise remains the most effective intervention for preventing falls. A meta-analysis reports a 20% relative reduction in falls (RR = 0.80) with programs combining muscle strengthening, balance training, and gait practice. The Otago Exercise Programme and Falls Management Exercise are the two commonly used validated models.88,89 The first is an individualized, home-based program led by a physiotherapist. The programme includes lower-limb strengthening, balance exercises, and active walking. It starts with an initial session and continues with monthly follow-up over 12 months. The second is a group-based program conducted in a dedicated setting, supervised by trained professionals. It focuses on progressive strengthening, dynamic balance, anticipatory postural reactions, and fall prevention strategies. An adapted physical activity professional may also be involved in delivering these sessions. These programs show optimal effectiveness at two to three sessions per week for at least six months, provided participants have sufficient physical and cognitive capacity.11,15
- Gait rehabilitation and targeted physiotherapy: physiotherapists play a central role in motor rehabilitation. However, isolated interventions focusing solely on gait retraining, posture or strength when not part of a structured and comprehensive program have not demonstrated significant benefit: the difference in fall rates is less than 5% compared to no intervention in trials included in current recommendations.15,47
- Sensory assessment: sensory deficits, particularly reduced visual acuity and age-related hearing loss (presbycusis), are frequently involved in the onset of falls in OAs. Systematic screening is essential, especially in cases of disorientation, complaints of instability, or unexplained falls. However, isolated interventions such as prescribing new glasses or cataract surgery have not shown significant benefit in reducing falls, and in some cases (eg, rapid and major changes in visual correction), may even temporarily worsen postural instability.11,15 With regard to hearing, presbycusis is associated with increased RoF and cognitive decline risk. Uncorrected hearing loss nearly doubles RoF, and exacerbates social isolation and cognitive impairment.90 Hearing aids may help to prevent functional decline and falls, provided the process is gradual, supported, and adapted to cognitive abilities. Their benefit is limited in longstanding or severe cases due to cochlear cell atrophy and a threshold beyond which recovery is no longer possible.
- Occupational therapy and home environment adaptation: assessing the home environment including stairs, lighting, obstacles, bedroom, toilet and bathroom allows for personalized fall prevention strategies. Although the effectiveness of environmental modifications alone is difficult to quantify, their value is widely acknowledged in secondary prevention, particularly after the first fall. Simple and low-cost interventions such as installing grab bars, removing rugs, or improving lighting are strongly recommended.9
- Assistive technologies: they play an increasingly important role in fall prevention, particularly among OAs living at home. Conventional tools such as canes, walkers, grab bars, and orthopedic footwear help improve stability and confidence during daily movement. Their effectiveness depends on appropriate indication, proper adjustment, and supervised use. In parallel, embedded technologies have rapidly evolved. Automated alert systems (eg, bracelets or pendants that detect prolonged inactivity or falls), smart mats, and motion sensors allow for early fall detection and reduce response time, thereby improving functional outcomes. Devices such as smartwatches now integrate accelerometers and gyroscopes capable of analyzing gait patterns, assessing stability, and even anticipating imbalance. Further innovations include instrumented insoles, smart clothing, and intelligent hearing devices with alert and geolocation features. While most of these technologies are well accepted by patients, their clinical effectiveness in reducing falls has yet to be confirmed in large-scale randomized trials. Nonetheless, they already offer undeniable added value in terms of perceived safety, autonomy, and home-based aging.91 These devices are also a means of implementing personalized digital monitoring of RoF, opening the prospect of predictive fall medicine combining biometric sensors, artificial intelligence, and adaptive rehabilitation programs. Virtual reality is an emerging rehabilitation tool, enabling users to perform or simulate motor tasks in a fully virtual environment. It can be used to analyze motor behavior and brain activity in a safe and controlled setting. While a habituation stage is essential due to the disorienting effects of immersive environments, several studies report significant benefits for balance and RoF and less dizziness, as measured by the one-leg stance test, TUG, Tinetti test, Berg balance scale, and functional reach test (FRT).24,92,93
Conclusion
BGDs are common in frail OAs and considering the increase in life expectancy thanks to medical progress and improved hygiene conditions, their prevalence will continue to rise. Once fatal medical situations can now be stabilized, leading to chronic conditions. It is thus necessary for health professionals managing OAs to fully understand BGDs, to thoroughly analyze each situation, and tailor care.
After interviewing to gather the OA’s history, including any previous falls, a medication inventory, in particular FRIDs, and the analysis of the home environment, a thorough clinical examination, possibly supplemented by paraclinical examinations, should be performed. These first steps are needed to obtain a clear picture of the situation and identify potential causes of BGDs. For example, a clinical suspicion of cardiac arrhythmia or conduction disorders requires an ECG or a Holter ECG. A suspicion of OH during interview will be confirmed by the OH test. In case of confusion, a lesion of the CNS may be suspected, requiring a brain computed tomography scan, or epilepsy, which must be confirmed by an electroencephalogram.
Among the many validated tools for assessing BGDs in OAs, some are easy and quick to administer (standing position, Five times sit-to-stand test, One-leg stance test, Gait speed, TUG, Dual-task test), while others are more complex and informative but take longer to complete (MMT, Tinetti test, Berg balance scale). All these tests involve tasks related to the daily activities necessary to preserve independent living. Emerging technologies such as surface electromyography, force platforms, and three-dimensional motion capture systems, although not yet used in routine geriatric practice, have considerably improved the early detection of RoF, monitoring, and rehabilitation of older adults with BGDs.
Regarding the management of BGDs, classic and validated and proven approaches such as motor rehabilitation must be associated with new technologies such as virtual reality. Automated alert systems such as fall detector bracelets or video surveillance can also be used.
Overall, the objective is to prevent falls and to limit or ideally avoid the loss of independence in OAs.
Abbreviations
ADLs, activities of daily living; BG, balance and gait; BGDs, balance and gait disorders, CNS, central nervous system; FRT, functional reach test; IADLs, instrumental activities of daily living; MMT, mini motor test; OA, older adult; OH, orthostatic hypotension; OR, odds ratio; RoF, risk of falling; SPPB, short physical performance battery; TUG, timed-up and go test.
Acknowledgments
The authors are grateful to Mrs. Suzanne RANKIN, a native English speaker, for editing and proofreading this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Manckoundia P, Mourey F, Pfitzenmeyer P. Marche et démences. Ann Readapt Med Phys. 2008;51(8):692–700. doi:10.1016/j.annrmp.2008.08.001
2. Herman T, Mirelman A, Giladi N, Schweiger A, Hausdorff JM. Executive control deficits as a prodrome to falls in healthy older adults: a prospective study linking thinking, walking, and falling. J Gerontol A Biol Sci Med Sci. 2010;65(10):1086–1092. doi:10.1093/gerona/glq077
3. Bouchon JP. 1 + 2 + 3 ou comment tenter d’être efficace en gériatrie ? Rev Prat. 1984;34:888–892.
4. Bioulac B, Burbaud P, Cazalets JR, Gross C. Fonctions motrices. EMC-Neurologie. 2004;1(1):1–15. doi:10.1016/S0246-0378(04)35622-8
5. Carini F, Mazzola M, Fici C, et al. Posture and posturology, anatomical and physiological profiles: overview and current state of art. Acta Biomed. 2017;88(1):11–16. doi:10.23750/abm.v88i1.5309
6. Manckoundia P. Troubles de la marche et de l’équilibre (voir item 107). Rev Prat. 2018;68(10):e403–e409.
7. Bronstein AM, Pavlou M. Balance. Handb Clin Neurol. 2013;110:189–208.
8. Berthoz A Le sens du mouvement. Paris (France): Odile Jacob; 1997.
9. Shaffer SW, Harrison AL. Aging of the somatosensory system: a translational perspective. Phys Ther. 2007;87(2):193–207. doi:10.2522/ptj.20060083
10. Tomlinson J, Zwirner J, Ondruschka B, Prietzel T, Hammer N. Innervation of the Hip joint capsular complex: a systematic review of histological and immunohistochemical studies and their clinical implications for contemporary treatment strategies in total hip arthroplasty. PLoS One. 2020;15(2):e0229128. doi:10.1371/journal.pone.0229128
11. Montero-Odasso M, Verghese J, Beauchet O, Hausdorff JM. Gait and cognition: a complementary approach to understanding brain function and the risk of falling. J Am Geriatr Soc. 2012;60(11):2127–2136. doi:10.1111/j.1532-5415.2012.04209.x
12. Alpini D, Cesarani A, Fraschini F, Kohen-Raz R, Capobianco S, Cornelio F. Aging and vestibular system: specific tests and role of melatonin in cognitive involvement. Arch Gerontol Geriatr Suppl. 2004;38(9):13–25. doi:10.1016/j.archger.2004.04.005
13. Campello L, Singh N, Advani J, Mondal AK, Corso-Díaz X, Swaroop A. Aging of the retina: molecular and metabolic turbulences and potential interventions. Annu Rev Vis Sci. 2021;7:633–664. doi:10.1146/annurev-vision-100419-114940
14. Kahiel Z, Grant A, Aubin MJ, Buhrmann R, Kergoat MJ, Freeman EE. Vision, eye disease, and the onset of balance problems: the Canadian Longitudinal Study on Aging. Am J Ophthalmol. 2021;231:170–178. doi:10.1016/j.ajo.2021.06.008
15. Lamb SE, Bruce J, Hossain A, et al; Prevention of Fall Injury Trial Study Group. Screening and intervention to prevent falls and fractures in older people. N Engl J Med. 2020;383(19):1848–1859. doi:10.1056/NEJMoa2001500
16. Seppala LJ, Petrovic M, Ryg J, et al. STOPPFall (Screening Tool of Older Persons Prescriptions in older adults with high fall risk): a Delphi study by the EuGMS task and finish group on fall-risk-increasing drugs. Age Ageing. 2021;50(4):1189–1199. doi:10.1093/ageing/afaa249
17. Faraji J, Metz GAS. Harnessing BDNF signaling to promote resilience in aging. Aging Dis. 2024;16(4):1813–1841. doi:10.14336/AD.2024.0961
18. Shur NF, Creedon L, Skirrow S, et al. Age-related changes in muscle architecture and metabolism in humans: the likely contribution of physical inactivity to age-related functional decline. Ageing Res Rev. 2021;68:101344. doi:10.1016/j.arr.2021.101344
19. van der Jagt-Willems HC, de Groot MH, van Campen JP, Lamoth CJ, Lems WF. Associations between vertebral fractures, increased thoracic kyphosis, a flexed posture and falls in older adults: a prospective cohort study. BMC Geriatr. 2015;15:34. doi:10.1186/s12877-015-0018-z
20. Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR. Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporos Int. 2005;16(8):1004–1010. doi:10.1007/s00198-004-1791-2
21. Huang T, Li C, Chen F, et al. Prevalence and risk factors of osteosarcopenia: a systematic review and meta-analysis. BMC Geriatr. 2023;23(1):369. doi:10.1186/s12877-023-04085-9
22. Khandelwal S, Lane NE. Osteoporosis: review of etiology, mechanisms, and approach to management in the aging population. Endocrinol Metab Clin North Am. 2023;52(2):259–275. doi:10.1016/j.ecl.2022.10.009
23. Bouccara D, Rubin F, Bonfils P, Lisan Q. Vertiges et troubles de l’équilibre: démarche diagnostique. Rev Med Interne. 2018;39(11):869–874. doi:10.1016/j.revmed.2018.02.004
24. Sana V, Ghous M, Kashif M, Albalwi A, Muneer R, Zia M. Effects of vestibular rehabilitation therapy versus virtual reality on balance, dizziness, and gait in patients with subacute stroke: a randomized controlled trial. Medicine. 2023;102(24):e33203. doi:10.1097/MD.0000000000033203
25. D’Amico RS, Praver M, Zanazzi GJ, et al. Subependymomas are low-grade heterogeneous glial neoplasms defined by subventricular zone lineage markers. World Neurosurg. 2017;107:451–463. doi:10.1016/j.wneu.2017.08.009
26. Stolze H, Kuhtz-Buschbeck JP, Drücke H, Jöhnk K, Illert M, Deuschl G. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J Neurol Neurosurg Psychiatry. 2001;70(3):289–297. doi:10.1136/jnnp.70.3.289
27. Tavares NMB, Silva JM, Silva MDMD, et al. Balance, gait, functionality and fall occurrence in adults and older adults with type 2 diabetes mellitus and associated peripheral neuropathy. Clin Pract. 2024;14(5):2044–2055. doi:10.3390/clinpract14050161
28. Chompoopong P, Mauermann ML, Siddiqi H, Peltier A. Amyloid neuropathy: from pathophysiology to treatment in light-chain amyloidosis and hereditary transthyretin amyloidosis. Ann Neurol. 2024;96(3):423–440. doi:10.1002/ana.26965
29. Ali AS, Akavaram NR. Neuromuscular disorders in thyrotoxicosis. Am Fam Physician. 1980;22(3):97–102.
30. Staff NP, Windebank AJ. Peripheral neuropathy due to vitamin deficiency, toxins, and medications. Continuum. 2014;20(5 Peripheral Nervous System Disorders):1293–1306. doi:10.1212/01.CON.0000455880.06675.5a
31. Wang J, Ullah S, Solano MA, Overley SC, Bumpass DB, Mannen EM. Changes in kinematics, kinetics, and muscle activity in patients with lumbar spinal stenosis during gait: systematic review. Spine J. 2022;22(1):157–167. doi:10.1016/j.spinee.2021.06.003
32. Kaffel D, Maatallah K, Ferjani HL, Triki W, Zarati D, Hamdi W. Profils cliniques, biologiques et étiologiques des ostéomalacies. Pan Afr Med J. 2020;37:215. doi:10.11604/pamj.2020.37.215.26407
33. Brzozowska MM, Banthia S, Thompson S, Narasimhan M, Lee J. Severe hypothyroidism complicated by myopathy and neuropathy with atypical demyelinating features. Case Rep Endocrinol. 2021;2021:5525156. doi:10.1155/2021/5525156
34. Le Quintrec JS, Le Quintrec JL. Drug-induced myopathies. Baillieres Clin Rheumatol. 1991;5(1):21–38. doi:10.1016/S0950-3579(05)80294-8
35. García Estévez DA, Pardo Fernández J. Myasthenia gravis. Update on diagnosis and therapy. Med Clin. 2023;161(3):119–127. doi:10.1016/j.medcli.2023.04.006
36. Bawa A, Banitsas K, Abbod M. A movement classification of polymyalgia rheumatica patients using myoelectric sensors. Sensors. 2024;24(5):1500. doi:10.3390/s24051500
37. Modi AD, Parekh A, Patel ZH. Methods for evaluating gait associated dynamic balance and coordination in rodents. Behav Brain Res. 2024;456:114695. doi:10.1016/j.bbr.2023.114695
38. Ang GC, Low SL, How CH. Approach to falls among the elderly in the community. Singapore Med J. 2020;61(3):116–121. doi:10.11622/smedj.2020029
39. Schoenberger JA. Drug-induced orthostatic hypotension. Drug Saf. 1991;6(6):402–407. doi:10.2165/00002018-199106060-00002
40. Aksoyalp ZŞ, Nemutlu-Samur D. Comparative post-marketing surveillance of memantine and cholinesterase inhibitors: cardiovascular adverse events with a focus on sex differences using the FDA adverse event reporting system database. Int J Geriatr Psychiatry. 2024;39(11):e70018. doi:10.1002/gps.70018
41. Li J, Yang D, He Q, Wu Q, Sun W, Sun W. Association of motoric cognitive risk syndrome with falls in older adults: findings from three longitudinal studies. BMC Geriatr. 2025;25(1):388. doi:10.1186/s12877-025-06062-w
42. Seppala LJ, van der Velde N, Masud T, et al. EuGMS task and finish group on Fall-Risk-Increasing Drugs (FRIDs): position on knowledge dissemination, management, and future research. Drugs Aging. 2019;36(4):299–307. doi:10.1007/s40266-018-0622-7
43. Godoi Rezende Costa Molino C, Forster CK, Wieczorek M, et al. Association of fall risk-increasing drugs with falls in generally healthy older adults: a 3-year prospective observational study of the DO-HEALTH trial. BMC Geriatr. 2024;24:980. doi:10.1186/s12877-024-05557-2
44. O’Mahony D, Cherubini A, Guiteras AR, et al. STOPP/START criteria for potentially inappropriate prescribing in older people: version 3. Eur Geriatr Med. 2023;14(4):625–632. doi:10.1007/s41999-023-00777-y
45. 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American Geriatrics Society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052–2081. doi:10.1111/jgs.18372
46. Roux B, Berthou-Contreras J, Beuscart JB, et al. REview of potentially inappropriate MEDIcation pr[e]scribing in Seniors (REMEDI[e]S): french implicit and explicit criteria. Eur J Clin Pharmacol. 2021;77(11):1713–1724. doi:10.1007/s00228-021-03145-6
47. Guirguis-Blake JM, Perdue LA, Coppola EL, Bean SI. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US preventive services task force. JAMA. 2024;332(1):58–69. doi:10.1001/jama.2024.4166
48. Kim JH, Lee SB. Evaluation of activities of daily living: current insights and future horizons. Ann Geriatr Med Res. 2025;29(2):143–158. doi:10.4235/agmr.24.0172
49. Cruz-Jentoft AJ, Bahat G, Bauer J, et al; Writing Group for the European Working Group on Sarcopenia in Older People 2 (EWGSOP2), and the Extended Group for EWGSOP2. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. Erratum in: Age Ageing. 2019;48(4):601. doi:10.1093/ageing/afy169
50. Maki BE, McIlroy WE. Postural control in the older adult. Clin Geriatr Med. 1996;12(4):635–658. doi:10.1016/S0749-0690(18)30193-9
51. Mehmet H, Yang AWH, Robinson SR. What is the optimal chair stand test protocol for older adults? A systematic review. Disabil Rehabil. 2020;42(20):2828–2835. doi:10.1080/09638288.2019.1575922
52. Tiedemann A, Shimada H, Sherrington C, Murray S, Lord S. The comparativeability of eight functional mobility tests for predicting falls in community-dwellingolder people. Age Ageing. 2008;37(4):430–435. doi:10.1093/ageing/afn100
53. Trommelen RD, Buttone LF, Dicharry DZ, Jacobs RM, Karpinski A. The use of five repetition sit to stand test (FRSTST) to assess fallrisk in the assisted living population. Phys Occup Ther Geriatrics. 2015;33(2):152–162. doi:10.3109/02703181.2015.1016646
54. Buatois S, Perret-Guillaume C, Gueguen R, et al. A simple clinical scale to stratify risk of recurrent falls in community-dwelling adults aged 65 years and older. Phys Ther. 2010;90(4):550–560. doi:10.2522/ptj.20090158
55. Mourey F, Camus A, d’Athis P, et al. Mini motor test: a clinical test for rehabilitation of patients showing psychomotor disadaptation syndrome (PDS). Arch Gerontol Geriatr. 2005;40(2):201–211. doi:10.1016/j.archger.2004.08.004
56. Ellrich N, Niermeyer K, Peto D, et al. Precision balance assessment in Parkinson’s disease: utilizing vision-based 3D pose tracking for pull test analysis. Sensors. 2024;24(11):3673. doi:10.3390/s24113673
57. Manckoundia P, Barthélémy E, Bonnot R, d’Athis P. Impact of an ambulatory physical activity program on balance and motor abilities of retirees: a prospective study. Int J Clin Pract. 2020;74(5):e13474. doi:10.1111/ijcp.13474
58. De Abreu DCC, Bandeira ACL, Magnani PE, et al. Standing balance test for fall prediction in older adults: a 6-month longitudinal study. BMC Geriatr. 2024;24:947. doi:10.1186/s12877-024-05380-9
59. Abellan van Kan G, Rolland Y, Andrieu S, et al. Gait speed at usual pace as a predictor of adverse outcomes in community-dwelling older people an International Academy on Nutrition and Aging (IANA) task force. J Nutr Health Aging. 2009;13(10):881–889. doi:10.1007/s12603-009-0246-z
60. Alexander NB, Ulbrich J, Raheja A, Channer D. Rising from the floor in older adults. J Am Geriatr Soc. 1997;45(5):564–569. doi:10.1111/j.1532-5415.1997.tb03088.x
61. Bergland A, Laake K. Concurrent and predictive validity of “getting up from lying on the floor”. Aging Clin Exp Res. 2005;17(3):181–185. doi:10.1007/BF03324594
62. Gatenio-Hefling O, Tzemah-Shahar R, Asraf K, Dilian O, Gil E, Agmon M. Revisiting the “Timed Up and Go” test: a 12-s cut-off can predict hospitalization associated functional decline in older adults. Geroscience. 2025;47(1):1039–1048. doi:10.1007/s11357-024-01280-3
63. Kojima G, Masud T, Kendrick D, et al. Does the timed up and go test predict future falls among British community-dwelling older people? Prospective cohort study nested within a randomised controlled trial. BMC Geriatr. 2015;15:38. doi:10.1186/s12877-015-0039-7
64. Lundin-Olsson L, Nyberg L, Gustafson Y. The mobility interaction fall chart. Physiother Res Int. 2000;5(3):190–201. doi:10.1002/pri.198
65. Hennah C, Doumas M. Dual-task walking on real-world surfaces: adaptive changes in walking speed, step width and step height in young and older adults. Exp Gerontol. 2023;177:112200. doi:10.1016/j.exger.2023.112200
66. Merendino A, Mourey F, Renoncourt T, et al. Psychomotor disadaptation syndrome: a scoping review. Eur Geriatr Med. 2025;16(3):807–826. doi:10.1007/s41999-025-01176-1
67. Tinetti ME. Performance-oriented assessment of mobility problems in elderly patients. J Am Geriatr Soc. 1986;34(2):119–126. doi:10.1111/j.1532-5415.1986.tb05480.x
68. Koo BB, Bergethon P, Qiu WQ, et al. Clinical prediction of fall risk and white matter abnormalities: a diffusion tensor imaging study. Arch Neurol. 2012;69(6):733–738. doi:10.1001/archneurol.2011.2272
69. Sakthivadivel V, Geetha J, Gaur A, Kaliappan A. Performance-oriented mobility assessment test and timed up and go test as predictors of falls in the elderly—a cross-sectional study. J Family Med Prim Care. 2022;11(11):7294–7298. doi:10.4103/jfmpc.jfmpc_1294_22
70. Giovannini S, Brau F, Galluzzo V, et al. Falls among older adults: screening, identification, rehabilitation, and management. Appl Sci. 2022;12:7934. doi:10.3390/app12157934
71. Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol A Biol Sci Med Sci. 2000;55(4):M221–M231. doi:10.1093/gerona/55.4.M221
72. Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health. 1992;83(S2):S7–S11.
73. Berg KO, Maki BE, Williams JI, Holliday PJ, Wood-Dauphinee SL. Clinical and laboratory measures of postural balance in an elderly population. Arch Phys Med Rehabil. 1992;73(11):1073–1080.
74. Bogle Thorbahn LD, Newton RA. Use of the Berg Balance Test to predict falls in elderly persons. Phys Ther. 1996;76(6):576–583. doi:10.1093/ptj/76.6.576
75. Dieterich M, Brandt T. Perception of verticality and vestibular disorders of balance and falls. Front Neurol. 2019;10:172. doi:10.3389/fneur.2019.00172
76. Manckoundia P, Mourey F, Pfitzenmeyer P, Van Hoecke J, Pérennou D. Is backward disequilibrium in the elderly caused by an abnormal perception of verticality? A pilot study. Clin Neurophysiol. 2007;118(4):786–793. doi:10.1016/j.clinph.2006.11.274
77. Barbieri G, Gissot AS, Pérennou D. Ageing of the postural vertical. Age. 2010;32(1):51–60. doi:10.1007/s11357-009-9112-5
78. Barra J, Pérennou D. Le sens de verticalité est-il vestibulaire? Neurophysiol Clin. 2013;43(3):197–204. doi:10.1016/j.neucli.2013.02.001
79. Duncan PW, Studenski S, Chandler J, Prescott B. Functional reach: predictive validity in a sample of elderly male veterans. J Gerontol. 1992;47(3):M93–M98. doi:10.1093/geronj/47.3.M93
80. Behrman AL, Light KE, Flynn SM, Thigpen MT. Is the functional reach test useful for identifying falls risk among individuals with Parkinson’s disease? Arch Phys Med Rehabil. 2002;83(4):538–542.
81. Duarte MB, da Silva Almeida GC, Costa KHA, et al. Anticipatory postural adjustments in older versus young adults: a systematic review and meta-analysis. Syst Rev. 2022;11(1):251. doi:10.1186/s13643-022-02116-x
82. Quijoux F, Vienne-Jumeau A, Bertin-Hugault F, et al. Center of pressure displacement characteristics differentiate fall risk in older people: a systematic review with meta-analysis. Ageing Res Rev. 2020;62:101117. doi:10.1016/j.arr.2020.101117
83. Liang HW, Ameri R, Band S, et al. Fall risk classification with posturographic parameters in community-dwelling older adults: a machine learning and explainable artificial intelligence approach. J Neuroeng Rehabil. 2024;21(1):15. doi:10.1186/s12984-024-01310-3
84. Jia S, Bello UM, Manduchi R, Cheong AMY. Effect of visual searching and obstacle crossing on gait performance in older adults. Sci Rep. 2025;15:22334. doi:10.1038/s41598-025-08174-0
85. Lockhart TE, Soangra R, Yoon H, et al. Prediction of fall risk among community-dwelling older adults using a wearable system. Sci Rep. 2021;11(1):20976.
86. Brognara L. Gait assessment using smartphone applications in older adults: a scoping review. Geriatrics. 2024;9(4):95. doi:10.3390/geriatrics9040095
87. Cornille C, Lenglet A, Decaudin B, et al. A multidisciplinary meeting for generating a personalized pharmaceutical plan for older adults at hospital discharge: the IATROPREV study. Br J Clin Pharmacol. 2025;91:2885–2891. doi:10.1002/bcp.70098
88. Yang Y, Wang K, Liu H, et al. The impact of Otago exercise programme on the prevention of falls in older adult: a systematic review. Front Public Health. 2022;10:953593. doi:10.3389/fpubh.2022.953593
89. Gumber L, Timmons S, Coupland C, et al. ‘It is designed for everybody to find their own level and to improve themselves’; views of older people and instructors of the Falls Management Exercise (FaME) programme. Age Ageing. 2022;51(2):afac023. doi:10.1093/ageing/afac023
90. Putter-Katz H, Horev N, Yaakobi E, Been E. Self-reported hearing measures can predict risk of falling and balance problems. Commun Med. 2025;5(1):173. doi:10.1038/s43856-025-00878-8
91. Kim U, Lim J, Park Y, Bae Y. Predicting fall risk through step width variability at increased gait speed in community dwelling older adults. Sci Rep. 2025;15:16915. doi:10.1038/s41598-025-02128-2
92. Zak M, Sikorski T, Krupnik S, et al. Physiotherapy programmes aided by VR solutions applied to the seniors affected by functional capacity impairment: randomised controlled trial. Int J Environ Res Public Health. 2022;19:6018. doi:10.3390/ijerph19106018
93. Lee K. Virtual reality gait training to promote balance and gait among older people: a randomized clinical trial. Geriatrics. 2020;6(1):1. doi:10.3390/geriatrics6010001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multimorbidity Patterns and Associations with Gait, Balance and Lower Extremity Muscle Function in the Elderly: A Cross-Sectional Study in Northwest China
Yang K, Yang S, Chen Y, Cao G, Xu R, Jia X, Hou L, Li J, Bi C, Wang X
International Journal of General Medicine 2023, 16:3179-3192
Published Date: 28 July 2023
A Review of Movement and Functional Impairments in Fibromyalgia: Implications for Targeted Treatment
Quodling N, Hoffman N, Carrick FR, Jemni M
Journal of Pain Research 2025, 18:5587-5597
Published Date: 25 October 2025
Biopsychosocial Factors Affecting Disability in Individuals with Chronic Nonspecific Low Back Pain: A Cross-Sectional Study
Canli İ, Özüdoğru A
Journal of Pain Research 2026, 19:590191
Published Date: 13 March 2026