Back to Journals » Journal of Pain Research » Volume 18
A Review of Movement and Functional Impairments in Fibromyalgia: Implications for Targeted Treatment
Authors Quodling N ![]() , Hoffman N, Carrick FR, Jemni M
, Hoffman N, Carrick FR, Jemni M
Received 3 June 2025
Accepted for publication 17 September 2025
Published 25 October 2025 Volume 2025:18 Pages 5587—5597
DOI https://doi.org/10.2147/JPR.S543775
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor King Hei Stanley Lam
Nicole Quodling,1,2 Norman Hoffman,1 Frederick Robert Carrick,1,3– 5 Monèm Jemni1,6,7
1Department of Neurology, Carrick Institute, Cape Canaveral, FL, 32920, USA; 2Coelevate Chiropractic, Walkerville, SA, 5081, Australia; 3Neurology University of Central Florida College of Medicine, Orlando, FL, 23816, USA; 4Burnett School of Biomedical Science, University of Central Florida, Orlando, FL, 32827, USA; 5MGH Institute for Health Professions, Boston, MA, 02129, USA; 6Centre for Mental Health Research in Association with the University of Cambridge, Cambridge, CB2 1TN, UK; 7Faculty of Physical Education, Ningbo University, Ningbo, 315000, People’s Republic of China
Correspondence: Nicole Quodling, Coelevate Chiropractic, 103 Walkerville Terrace, Walkerville, SA, 5081, Australia, Email [email protected]
Abstract: Fibromyalgia (FM) is a complex and disabling chronic pain condition characterized by widespread musculoskeletal pain, persistent fatigue, cognitive dysfunction, and sleep disturbances. It affects approximately 1– 10% of the general population, with a strong female predominance. Beyond pain, patients often experience hypersensitivity to stimuli such as light, touch, and temperature - a phenomenon attributed to central sensitization. Despite its high prevalence, FM remains poorly understood. The condition is believed to arise from abnormal central sensory processing in interaction with peripheral pain generators and psycho-neuro-endocrine dysfunction. Pharmaceutical therapies provide limited relief, with many patients experiencing minimal improvements in function or quality of life and multiple medications being associated with reduced quality of life indices. Importantly, FM is increasingly associated with deficits in motor control, including impaired balance, altered gait, and reduced postural stability. These functional impairments contribute to sedentary behaviour and disability, yet remain underexplored in the literature compared to pain-related symptoms. This review aims to synthesise the current evidence on motor control deficits, balance dysfunction, gait abnormalities, and psychological and rehabilitative strategies in FM. By understanding these multifactorial impairments, this work seeks to support more holistic, multidisciplinary approaches to FM management.
Keywords: central sensitization, movement disorder, gait, balance, posture, exercise
Introduction
Fibromyalgia (FM) is a disabling chronic pain syndrome characterized by multiple symptoms, including medically unexplained widespread pain, fatigue, cognitive, mood and sleep disorders.1–11 FM is considered a diagnosis of exclusion, leading to a significant delay in diagnosis, of up to 5 years, with the number of physicians visited in the interim reported as 3.7,12 The subjective nature of FM and the absence of validated diagnostic tests negatively impact its management, contributing to greater disease severity, fatigue, pain, poor treatment response and frustration.13 Efficient FM diagnosis and treatment depend on eliciting valid biomarkers,12 and defining subgroups.10,14 Motor control deficits in balance and postural control have been demonstrated in patients with FM,8,15 as have symptoms of central sensitization, characterized by hypersensitivity to bright light, touch, noise, temperature, and mechanical pressure.4,7,16 The prevalence of FM in the general population is estimated to be between 1 and 10%,1,4,5,7,9,17 with a female predominance.5,7,12,13 FM patients report higher levels of pain and fatigue than other chronic pain syndromes, negatively impacting social contacts, employment abilities, daily activities, and mental health,4,11 associated with reduced quality of life,4,5,7,10,11,17 and presenting a societal burden.6,18 FM has an unknown aetiology but has been described as a complex hyperalgesic pain syndrome in which abnormalities of central sensory processing interact with peripheral pain generators.1,5,7 Despite the importance of comorbid symptoms, most research has traditionally focused on pain-related outcomes.3 However, recommended pharmaceutical therapies generally achieve only 30% effectiveness in relieving symptoms and 20% effectiveness in improving function. Multiple position statements recommend that medications be accompanied by exercise and coping skills approaches.18
The symptoms of FM may lead to a sedentary lifestyle by reducing physical abilities, which can lead to adverse effects on the functional capacity of the patient.19 Patients with chronic pain often have deficits in motor performance, including restricted movement or altered motor planning,20 leading to posture, gait and balance insufficiencies.19,21 Despite the evidence of altered gait and postural parameters in FM, little is known about how these abnormalities are linked to clinical variables such as pain, fatigue, stiffness, or depression.19 Understanding the underlying disease process will provide insights for targeted therapeutic approaches.7,10 This review aims to synthesise current evidence on motor control deficits, balance, and postural dysfunction in FM, and to evaluate multidisciplinary strategies to improve functional capacity and quality of life.
Materials and Methods
A systematic literature search was conducted across four databases—PubMed, Medline, Scopus, and Web of Science—up to February 2025. The search combined the terms “fibromyalgia” AND “movement disorder”, with related terms including “gait”, “balance”, “posture”, and “exercise”. Boolean operators and filters for peer-reviewed, human studies published in English were applied where applicable. After removing duplicates, 52 studies remained for screening. There was no formal risk-of-bias assessment for each included paper. Studies were excluded if they did not address movement-related variables (eg, gait, postural control, balance) or if they focused exclusively on non-human models. One rodent-based study was excluded on this basis. Following title and abstract screening, 23 studies met the inclusion criteria for full review. The inclusion criteria were: (1) participants diagnosed with FM; (2) outcome measures related to movement, posture, gait, motor control, or physical activity. Case reports with <5 participants, and studies without clear functional or biomechanical measures were excluded. The results of the search are displayed in Figure 1.22
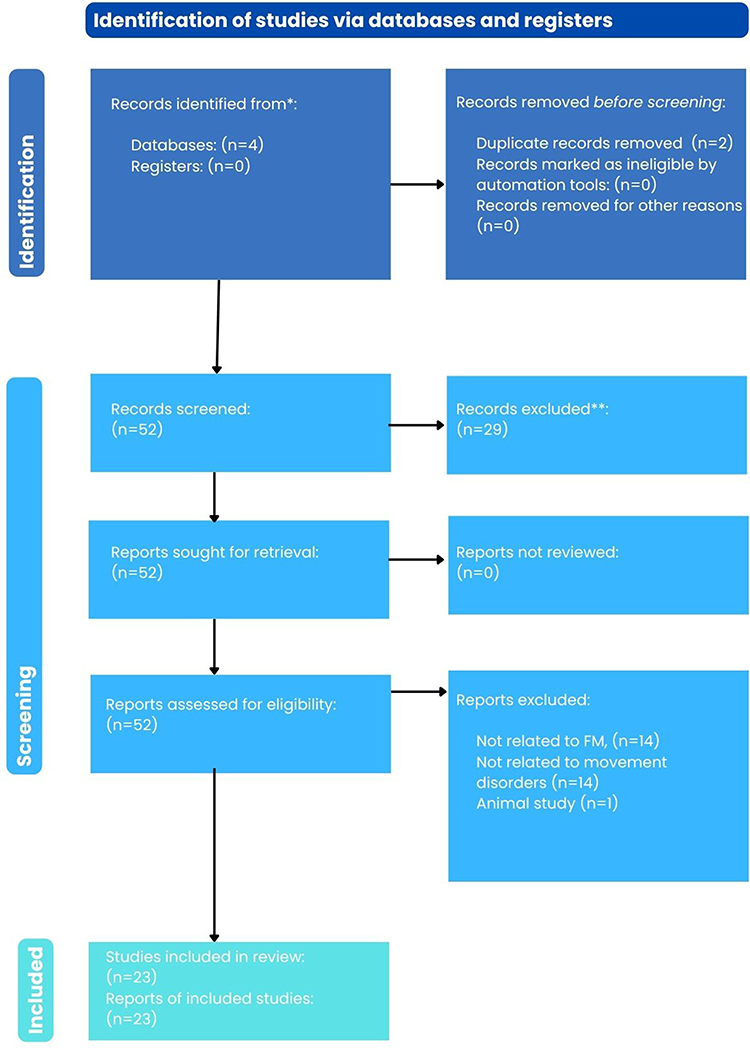 |
Figure 1 PRISMA Framework database21 and articles search. |
Twenty-three studies met the inclusion criteria. The findings are summarised using a narrative synthesis, thematically based on their relevance to key domains of motor function and functional impairment in FM. These include (1) pain and fatigue, (2) kinesiophobia and psychological factors, (3) gait and balance, (4) sensorimotor integration and reaction time, and (5) biomechanical deficits and physical conditioning (Figure 2). Key characteristics of each study were extracted and summarised in table form to enable efficient narrative synthesis (Table 1).
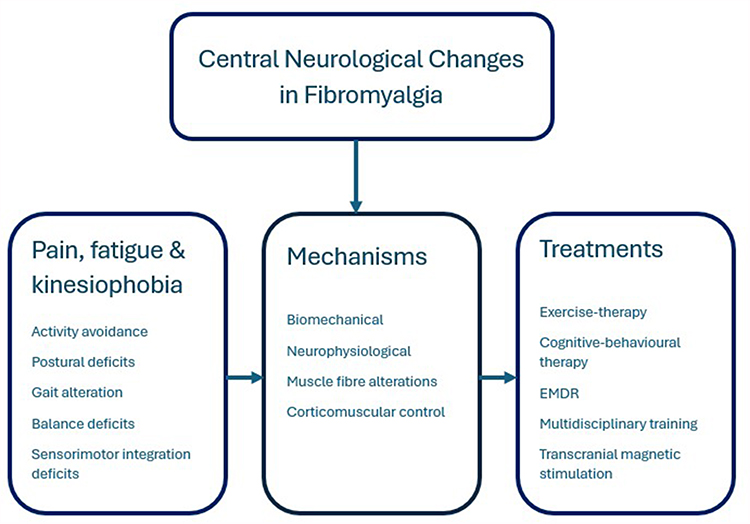 |
Figure 2 Central Neurological Changes in Fibromyalgia. |
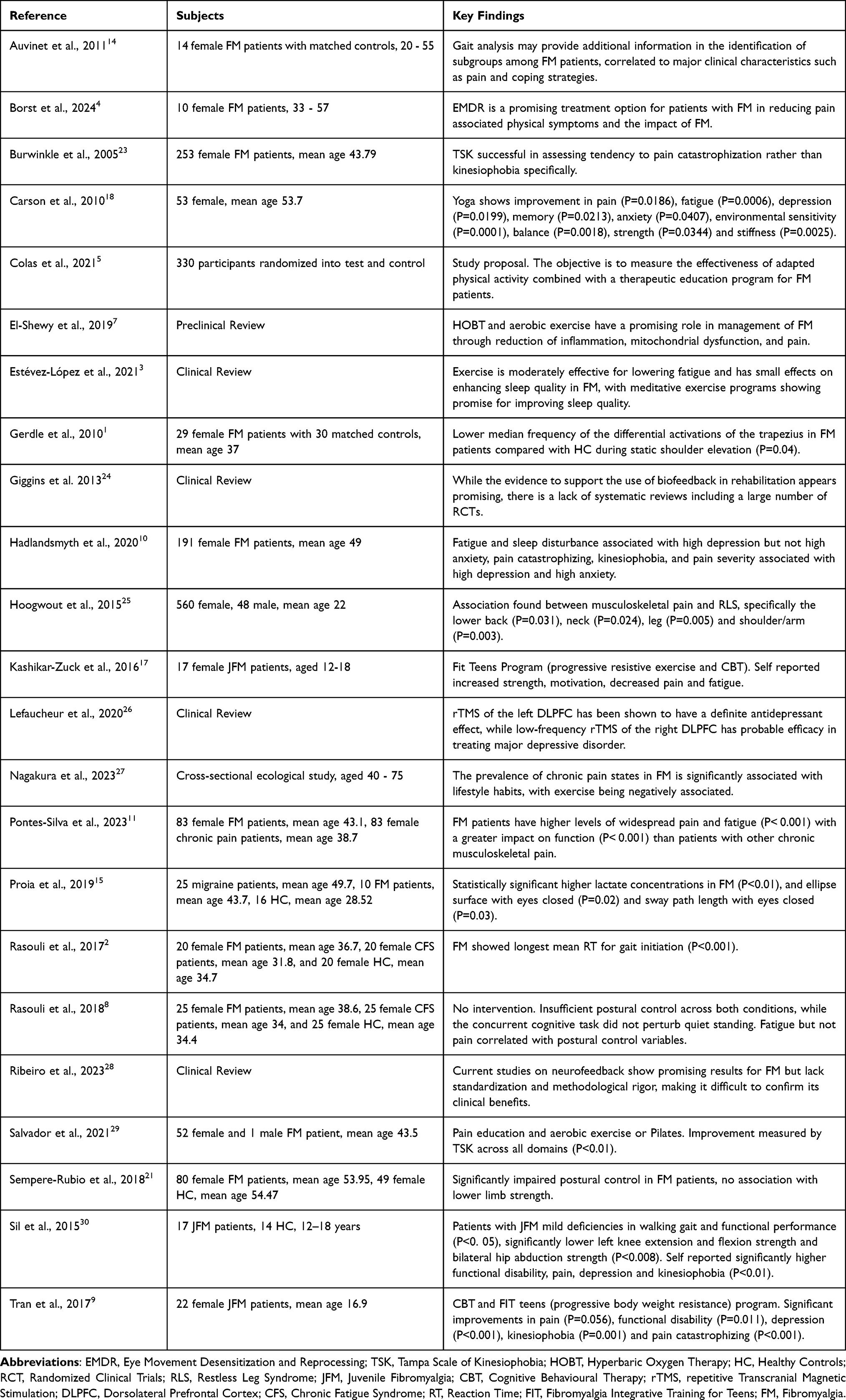 |
Table 1 Summary of Methodology and Findings |
Results
Pain and Fatigue
Pain was listed as a factor and/or measured in every paper elicited, confirming the weight pain is allocated as a symptom. Over 80% of FM patients report severe fatigue, which significantly impairs postural control and motor performance.3,8,21 Fatigue, more than pain, is correlated with balance deficits, attributed to impaired sensorimotor learning.8 Avoiding pain and fatigue presumably explains low levels of physical activity.8
Kinesiophobia and Psychological Factors
Kinesiophobia is defined as an excessive, irrational, and debilitating fear of movement and physical activity resulting from the feeling of vulnerability to painful or new injuries.23,29 Kinesiophobia was reported in patients with FM due to the association between pain, fatigue and movement, and was associated with reduced levels of physical activity, increased disability, and perpetuation of pain.17,29,30 Low levels of physical activity were correlated with poor motor control, lower movement velocity, and a higher body mass index (BMI), which are typical in FM populations. High BMI and inactivity may exacerbate motor deficits and perpetuate the cycle of disability.2,17
FM patients may also experience real pain flare-ups post-exercise, linked to metabolic dysfunction and impaired endogenous pain inhibition.17 FM has been characterized by an increase in lactate levels, which appeared to facilitate the response of neuronal voltage-insensitive sodium channels.15
Gait and Balance
Patients with FM present with slower gait speed, reduced stride length, delayed gait initiation, altered postural sway,2,21 and altered muscle activation patterns during walking.30 Specific deficiencies in gait include reduced stride length and alterations in dorsiflexion, eversion, and internal rotation at the knee during early stance.30 Gait analysis was proposed to provide additional information in identifying subgroups among FM patients.14 Stride frequency may differentiate FM patients from healthy controls (HC) and was correlated with diverted attention and reduced self-assessed coping skills. Stride regularity was correlated to quality of life measures and pain catastrophizing, prospectively predicting high levels of comorbid pain and depression.14 FM was associated with an increased BMI, which was positively correlated with decreased reaction time during gait initiation.2 However, gait and postural control deficits were observable even after adjusting for BMI, indicating disease-specific mechanisms.30 An overview of gait and balance deficits described in the literature is provided in Table 2.
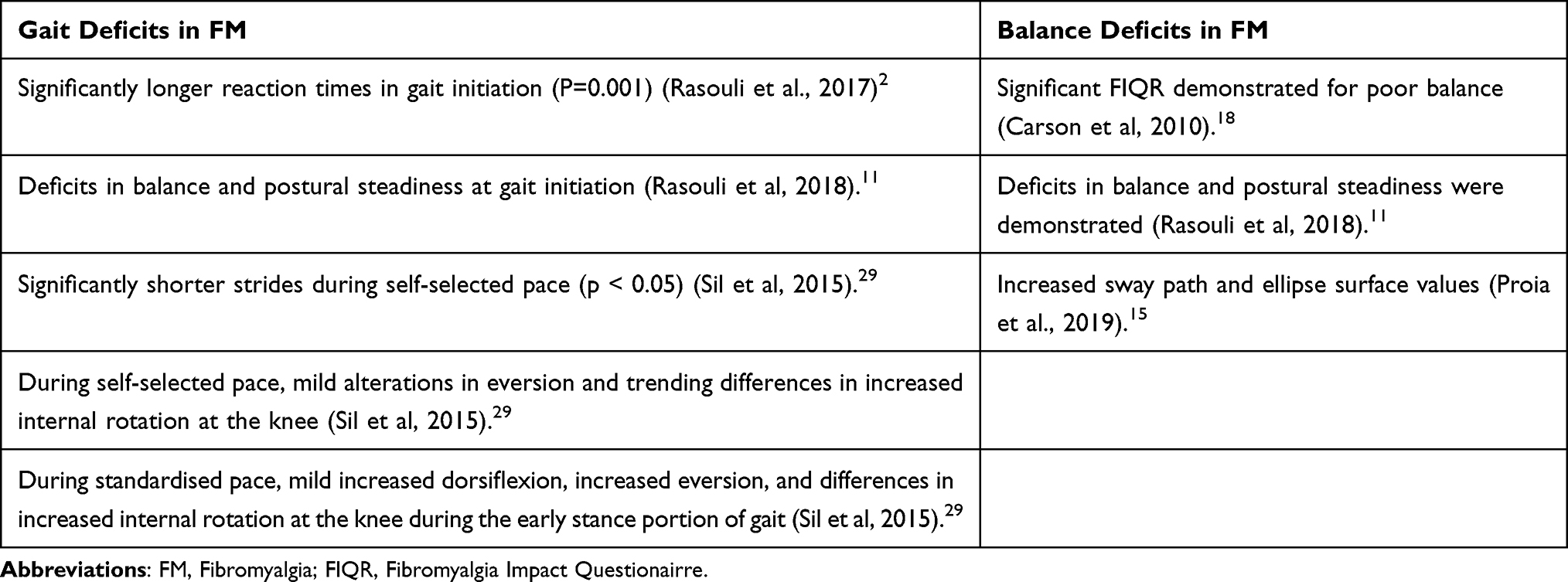 |
Table 2 Gait and Balance Deficits Observed in FM |
Sensorimotor Integration and Reaction Time
Longer response times in reaction time tasks were observed in FM, along with reduced psychomotor function, resulting in slower movement initiation and lower movement speed, especially in tasks with higher cognitive demands.2 FM patients demonstrate reduced differential muscle activation, likely due to impaired descending motor inhibition and altered neuromuscular strategies.1 These differences in neuromuscular control may serve as a substrate for ongoing functional limitations, not only in gait, but in functional performance and lower extremity strength. These deficits were accompanied by pain, functional disability, lowered mood, and kinesiophobia.30
Deficits in fine motor tasks, such as manual dexterity, reflect broader impairments in sensorimotor integration2 but may also be associated with dopamine dysregulation.25 Associations between restless leg syndrome and FM were identified, positively associated with both pain severity and the number of pain sites. Functional dysregulation of dopaminergic circuitry was suggested as a common underlying pathway, and may account for comorbid depressive symptoms and anxiety disorders.25 Further, activity in certain basal ganglionic areas has been correlated with motivation versus physical fatigue, namely widespread throughout the basal ganglia in the former and in the putamen for the latter.27
Biomechanical Deficits and Physical Conditioning
The pathogenesis of FM was hypothesised to include muscle abnormalities, including a reduction in type II muscle fibres, low levels of adenosine triphosphate, and damage to nerve fibres, leading to abnormal muscle metabolism, resulting in weakness, fatigue, and muscle pain.7 FM patients show reduced muscle strength and altered joint mechanics during functional movements like jumping.21,30 Observed biomechanics include reduced trunk flexion, increased hip flexion, and poor proximal stabilization, all of which contribute to fall risk.30
These findings reveal a multifactorial profile of motor and postural dysfunction in FM, shaped by pain processing abnormalities, psychological distress, deconditioning, and altered biomechanics. Collectively, these impairments suggest the need for integrative, multidisciplinary management approaches. Central neurological changes observed in FM and proposed treatments are represented in Figure 2.
The Role of Exercise
Regular moderate to vigorous physical activity and weight-bearing exercises are recommended for pain management in patients with FM,5,21 but adherence to these recommendations is often poor.9,17,30 Aerobic or resistance training programs may be challenging for patients with FM due to poor movement confidence and competence17 and increased baseline lactate concentrations.15 Moderate exercise, integrative neuromuscular training, Tai Chi, and Virtual Reality (VR) based exergaming show promise in improving postural stability and physical functioning.5,24
Force plate systems provide feedback on balance, movement, and gait and have been shown to reduce the incidence of falls.24 Although there is a growing number of studies regarding the effect of neurofeedback on FM in the literature, the level of evidence is still uncertain.28
The Role of Psychological Support
As there has been an association between traumatic life experiences, post-traumatic stress disorder (PTSD) symptoms, and the development and persistence of FM,3 evidence-based interventions for PTSD, such as Eye Movement Desensitization and Reprocessing (EMDR), have been investigated.4 Stiffness in muscles and joints and self-reported fatigue have been shown to significantly decrease in patients with FM following a series of EMDR sessions.4 Cognitive behavioural therapy (CBT) for FM is effective in reducing symptoms of depression, functional disability, and catastrophizing and increasing pain-coping efficacy,9,17 but does not result in greater engagement in more vigorous activity or exercise when applied in isolation.17 CBT combined with adapted physical activity appears more effective than either intervention alone.9,17 Thus, our current understanding underscores the need to address multiple domains of care, including physical, psychological and neurological treatment.
Transcranial Magnetic Stimulation of the Motor Cortex
Quality of life has been shown to be improved in patients with FM treated with high-frequency repetitive transcranial magnetic stimulation (HF-rTMS) of the motor cortex, with evidence of an impact on fatigue.26 HF-rTMS of the left dorsolateral prefrontal cortex (DLPFC) is more effective in reducing pain. In contrast, HF-rTMS of the left motor cortex is more effective in improving quality of life.26 rTMS is well tolerated with few minor side effects.26 A more systematic assessment of the optimal time window for treating patients with rTMS is needed, ideally based on individual markers of responsiveness.26
Discussion
The use of Gait Analysis as a Stratification Tool in Fibromyalgia Biomechanical assessments of gait are increasingly used to identify functional deficits.30 Insufficient postural control is generally characterized by a larger amplitude and lower frequency in the slow component representing postural sway, and a larger amplitude in the fast component, attributed to adjusting ankle torque. A mismatch between the magnitude and frequency of the controlling ankle torque thereby induces postural sway in patients.8 Gait in FM patients may be achieved preferentially by recruiting hip flexors instead of ankle plantar flexors, increasing metabolic demands and contributing to fatigue.19 Kinesiophobia may also contribute to altered gait, due to decreased walking speed, weakened muscle strength, and reduced performance in physical tasks.30
Gait analysis provides relevant information about physical and cognitive status and pain behaviour, and needs to be considered as a complementary exam in the assessment of FM. Stride frequency is a sensitive and specific gait marker for distinguishing FM patients from controls.14 Subgrouping FM patients on the basis of stride frequency measurement could facilitate the prescription of physical activity for patients with normal stride frequency, and encourage the prescription of a slowly progressive physical activity program for those who demonstrate reduced stride frequency on assessment. Stride regularity, in contrast, has been associated with the unsteadiness of gait, and has been linked to neurodegeneration and diminished executive function and attention.14 Reduced stride regularity values may characterise a subgroup of FM patients with poor affect and cognitive abilities. Stride regularity measurement could therefore help in the orientation of behavioural therapy in this subgroup. However, further studies are needed to better understand the implications of gait analysis in FM.14
Falls Risk and the Quality of Life
Balance confidence, decreased muscle strength and altered biomechanics can negatively affect patients’ quality of life by increasing the risk of falling, fall-related injuries and fear of falling,9,17,19,30 with poor perceived balance reported as one of the most debilitating symptoms.31 Balance training is generally not included in FM treatment; however, by identifying and quantifying consistent balance abnormalities in FM patients, the specificity and effectiveness of treatments may be improved.31
Additionally, many drugs to relieve pain for FM, such as opiates, muscle relaxants, and antidepressants, may impair balance. More information is needed on the side effects of medication prescribed for FM and their potential contribution to falls and balance impairment, since multiple medications are known to increase fall risk.31
The Contribution of Comorbid Obesity
Another area for further study of postural stability in FM patients is the role of BMI. A progressive decline in physical activity can contribute to excessive weight gain, with obesity being a common comorbidity with FM compared to HC.31 A high BMI has been associated with negative consequences for both fine and gross motor skills.2 However, the literature is mixed in implicating obesity concerning motor control and postural stability.2,17,30 It is likely that muscle strength does not increase in proportion to total weight in obese individuals; therefore, obese persons may not be able to generate the adequate force required to quickly regain postural control.31 Increased BMI has been associated with increased time to diagnosis in FM patients.13
Emerging Themes and Best Practice
Exercise
Pharmacological management often relies on the prescription of analgesics, antidepressants, and/or antiepileptics, but these therapies are not always effective and frequently cause undesirable effects.5 Nonpharmacological therapies have been advocated as a first-line treatment for patients suffering from FM, including exercise, which is the only strong therapy-based recommendation.3,5 Tailored exercise programs are needed for FM patients,3,17 but thus far, finding the most appropriate type of exercise that is both tolerable and sustainable for these patients has been challenging.17, The effects of pain and fatigue on motor function are often under-recognised.8 Patients with FM demonstrate dysfunctional pain inhibition, whereby they do not show endogenous hypoalgesia following exercise17 and may experience discrepancy between their perceived capability and actual ability to engage in exercise.3 Pain can trigger inhibitory mechanisms in affected and surrounding muscles, contributing to decreased motor output.2 FM patients exhibit reduced blood flow and degenerative changes in the muscles, presumably due to local hypoxia, creating higher levels of free radicals that induce apoptosis, reduce ATP and increase lactate concentrations in muscle cells, leading to muscle weakness and pain.7,15 Another hypothesis suggests that hypervascularisation of tender points increases oxygen availability in muscle fibres, leading to a prevalent use of aerobic metabolism with low lactate production.15
More than 80% of people with FM experience poor sleep quality with severe fatigue impacting depression,3 pain perception, physical functioning10 and exercise adherence.2,17,21 Reduced attentional and cognitive capacity resulting primarily from fatigue, may interfere with sensorimotor processing and contribute to reduced postural control displayed by patients with FM.8 This, along with co-occurring joint hypermobility, requires that exercise be performed with neutral joint positioning17 to avoid potential repetitive use injury.32 Exercise has low to moderate effects on fatigue for FM patients; however, at this juncture, the literature is scarce and there are no precise recommendations regarding frequency, intensity or type.5
Establishing fundamental movement skills and confidence should be the first step in facilitating engagement in activities of daily living and physical activity.9,30 Mind-body disciplines may fulfil the need for both exercise and coping skills components of FM treatment,7,18 and have been shown to improve balance.32 The addition of VR and therapeutic exergames offer patients opportunities to engage in meaningful, intensive, and enjoyable tasks related to their real-life interests and daily activities.24
Psychological
The influence of psychological factors is already well described in patients with chronic musculoskeletal pain contributing to decreased movement.10,29 Kinesiophobia and pain catastrophizing are prevalent in FM and are strongly associated with decreased physical performance, reduced postural control, and muscle weakness,9,17,29 further compounding activity avoidance and contributing to functional deficits and physical deconditioning.30 Providing patients with EMDR,4 CBT,9,12,17 biofeedback24 or rTMS26,33 may enable them to gain control over physical processes, allowing for improved functional task performance and increased autonomy in their rehabilitation.24 An integrative strategy combining pain-coping skills, enhanced with tailored, enjoyable exercise that includes sensory and motor challenges specifically designed to improve confidence in movement and enhance activity participation, holds promise in managing FM.2,17,30 However, recommendations for exercise have been based on reviews that provided evidence of the benefits of exercise for pain but were unclear for other symptoms.3,6
Optimal rehabilitation of FM requires an objective assessment of physical impairments during postural control, gait and motor planning to structure individual, multidisciplinary interventions and provide feedback on their efficacy.14,19 Motor assessment can be used to assess the effectiveness of training programs in improving physical functioning in patients with FM.30 Tailoring a flexible program which allows for modifications in consultation with the patient, with an emphasis on graded exercise and positive coping strategies, may be effective in ensuring that initial muscle soreness does not hinder compliance.17 Despite its clinical relevance, fatigue is rarely a primary measure of potential interventions.33 While pain is recommended as the primary outcome measure for chronic pain treatment interventions, functional deficits have long been reported by patients with FM and warrant investigation and appropriate, evidence-based intervention.33
Limitations and Gaps in the Literature
Limitations of this research are related to methodological inconsistencies, study heterogeneity, low subject numbers and the reliance on self-reported data. Due to the paucity of studies, papers referring to juvenile FM (JFM) were included where relevant. There is a need for stratified clinical trials and better functional assessments.
Of the studies investigated, only 5 provided an intervention, each showing positive results, however, each study was limited by small subject numbers. The search for better treatments is ongoing and directed towards multidisciplinary, patient-centred care, ideally focused on identified pathology.34 Despite the increase in the amount of research in recent years, there is still a paucity of information regarding optimal exercise dosing and subgroup-specific responses in FM. Future research is required to address the subgrouping of FM patients, appropriate exercise dosing and the efficacy of combined therapies.
Conclusions
FM is a disabling chronic pain syndrome characterized by multiple symptoms, including motor control deficits. Poor balance confidence, which may result from fatigue, decreased muscle strength, altered biomechanics or medication, has been associated with an increased number of falls and is reported as one of the most debilitating symptoms of FM. This, along with pain, may lead to a sedentary lifestyle, reducing physical abilities, further compounding the patient’s functional capacity. Most research has traditionally focused on pharmaceutical pain-related outcomes, and the effects of pain and fatigue on motor function are often under-recognised. Identifying and quantifying consistent motor dysfunction, including reaction time, hypermobility, gait, balance, and postural abnormalities in FM, may provide insight into broader deficits, such as proprioception and sensorimotor integration, and indicate how the specificity and effectiveness of treatments may be improved.
Regular moderate to vigorous physical activity and weight-bearing exercises are recommended for pain management in patients with FM, but compliance is notoriously poor, associated with hyperalgesia, pain catastrophizing, kinesiophobia and fundamental movement competence. Graded exercise, which includes motor planning and balance and can be assessed by measurable subjective and objective outcomes, including self-report, biomechanical, and balance evaluations, warrants further investigation. CBT combined with adapted physical activity seems more effective than either approach alone and may help reduce kinesiophobia and pain catastrophizing, enabling better adherence to exercise. Future research must evaluate the combination of psychological support with optimal and personalised graded exercise dosing.
AI Declaration
The authors acknowledge the use of Grammarly, Review Suggestions feature, and Clarivate Academic AI Platform as a feature of EndNote 2025.
Acknowledgments
The authors want to thank the Carrick Institute and Coelevate Chiropractic staff members for their continuing support along the way.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gerdle B, Grönlund C, Karlsson SJ, Holtermann A, Roeleveld K. Altered neuromuscular control mechanisms of the trapezius muscle in fibromyalgia. BMC Musculoskeletal Disord. 2010;11:42. doi:10.1186/1471-2474-11-42
2. Rasouli O, Fors EA, Borchgrevink PC, Öhberg F, Stensdotter AK. Gross and fine motor function in fibromyalgia and chronic fatigue syndrome. J Pain Res. 2017;10:303–309. doi:10.2147/JPR.S127038
3. Estévez-López F, Maestre-Cascales C, Russell D, et al. Effectiveness of exercise on fatigue and sleep quality in fibromyalgia: a systematic review and meta-analysis of randomized trials. Arch. Phys. Med. Rehabil. 2021;102(4):752–761. doi:10.1016/j.apmr.2020.06.019
4. Borst M, Moeyaert M, van Rood Y. The effect of eye movement desensitization and reprocessing on fibromyalgia: a multiple-baseline experimental case study across ten participants. Neuropsychol. Rehabil. 2024;34(10):1422–1454. doi:10.1080/09602011.2024.2314883
5. Colas C, Goutte J, Creac’h C, et al. Efficiency of an optimized care organization in fibromyalgia patients: the from intent to move (FIMOUV) study protocol of a randomized controlled trial. Front Public Health. 2021;9:554291. doi:10.3389/fpubh.2021.554291
6. Nagakura Y, Hayashi M, Kajioka S. Analysis of Japanese nationwide health datasets: association between lifestyle habits and prevalence of neuropathic pain and fibromyalgia with reference to dementia-related diseases and Parkinson’s disease. Scandinavian J Pain. 2023;23(4):662–669. doi:10.1515/sjpain-2023-0010
7. El-Shewy KM, Kunbaz A, Gad MM, et al. Hyperbaric oxygen and aerobic exercise in the long-term treatment of fibromyalgia: a narrative review. Biomed Pharmacothe. 2019;109:629–638. doi:10.1016/j.biopha.2018.10.157
8. Rasouli O, Fors EA, Vasseljen O, Stensdotter AK. A concurrent cognitive task does not perturb quiet standing in fibromyalgia and chronic fatigue syndrome. Pain res manag. 2018;2018:9014232. doi:10.1155/2018/9014232
9. Tran ST, Guite JW, Pantaleao A, et al. Preliminary outcomes of a cross-site cognitive-behavioral and neuromuscular integrative training intervention for juvenile fibromyalgia. Arthritis Care Res. 2017;69(3):413–420. doi:10.1002/acr.22946
10. Hadlandsmyth K, Dailey DL, Rakel BA, et al. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J Health Psychol. 2020;25(6):819–829. doi:10.1177/1359105317736577
11. Pontes-Silva A, de Sousa AP, Dibai-Filho AV, de Souza MC, DeSantana JM, Avila MA. Do the instruments used to assess fibromyalgia symptoms according to American College of Rheumatology criteria generate similar scores in other chronic musculoskeletal pain? BMC Musculoskeletal Disord. 2023;24(1):467. doi:10.1186/s12891-023-06572-x
12. Qureshi AG, Jha SK, Iskander J, et al. Diagnostic challenges and management of fibromyalgia. Cureus. 2021;13(10):e18692. doi:10.7759/cureus.18692
13. Moshrif A, Mosallam A, Abu-Zaid MH, Gouda W. Evaluating the effect of delayed diagnosis on disease outcome in fibromyalgia: a multi-center cross-sectional study. J Pain Res. 2023;16:1355–1365. doi:10.2147/JPR.S381314
14. Auvinet B, Chaleil D, Cabane J, et al. The interest of gait markers in the identification of subgroups among fibromyalgia patients. BMC Musculoskeletal Disord. 2011;12:258. doi:10.1186/1471-2474-12-258
15. Proia P, Amato A, Contrò V, et al. Relevance of lactate level detection in migrane and fibromyalgia. Eur J Trans Myol. 2019;29(2):8202. doi:10.4081/ejtm.2019.8202
16. Quodling N, Hoffman N, Carrick FR, Jemni M. Sensory processing in medically unexplained pain syndrome. A systematic review. Front Pain Res. 2025;6(1584227). doi:10.3389/fpain.2025.1584227
17. Kashikar-Zuck S, Tran ST, Barnett K, et al. A qualitative examination of a new combined cognitive-behavioral and neuromuscular training intervention for juvenile fibromyalgia. Clin J Pain. 2016;32(1):70–81. doi:10.1097/AJP.0000000000000221
18. Carson JW, Carson KM, Jones KD, Bennett RM, Wright CL, Mist SD. A pilot randomized controlled trial of the Yoga of Awareness program in the management of fibromyalgia. Pain. 2010;151(2):530–539. doi:10.1016/j.pain.2010.08.020
19. Costa ID, Gamundí A, Miranda JG, França LG, De Santana CN, Montoya P. Altered Functional Performance in Patients with Fibromyalgia. Front. hum. neurosci, 2017;14. doi:10.3389/fnhum.2017.00014
20. Park SH, Michael AM, Baker AK, Lei C, Martucci KT. Altered functional networks during gain anticipation in fibromyalgia. medRxiv. 2023. doi:10.1101/2023.04.28.23289290
21. Sempere-Rubio N, López-Pascual J, Aguilar-Rodríguez M, et al. Characterisation of postural control impairment in women with fibromyalgia. PLoS One. 2018;13(5):e0196575. doi:10.1371/journal.pone.0196575
22. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
23. Burwinkle T, Robinson JP, Turk DC. Fear of movement: factor structure of the Tampa scale of kinesiophobia in patients with fibromyalgia syndrome. J Pain. 2005;6(6):384–391. doi:10.1016/j.jpain.2005.01.355
24. Giggins OM, Persson UM, Caulfield B. Biofeedback in rehabilitation. J Neuroeng Rehabil. 2013;10:60. doi:10.1186/1743-0003-10-60
25. Hoogwout SJ, Paananen MV, Smith AJ, et al. Musculoskeletal pain is associated with restless legs syndrome in young adults. BMC Musculoskeletal Disord. 2015;16:294. doi:10.1186/s12891-015-0765-1
26. Lefaucheur JP, Aleman A, Baeken C, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014-2018). Clin Neurophysiol. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
27. Nakagawa S, Takeuchi H, Taki Y, et al. Basal ganglia correlates of fatigue in young adults. Sci Rep. 2016;6:21386. doi:10.1038/srep21386
28. Ribeiro TF, Carriello MA, Paula EP Jr, Garcia AC, da Rocha GL, Teive HAG. Clinical applications of neurofeedback based on sensorimotor rhythm: a systematic review and meta-analysis. Front Neurosci. 2023;17:1195066. doi:10.3389/fnins.2023.1195066
29. Salvador EMES, Franco KFM, Miyamoto GC, Franco YRDS, Cabral CMN. Analysis of the measurement properties of the Brazilian-Portuguese version of the Tampa Scale for Kinesiophobia-11 in patients with fibromyalgia. Braz. J. Phys. Ther. 2021;25(2):168–174. doi:10.1016/j.bjpt.2020.05.004
30. Sil S, Thomas S, DiCesare C, et al. Preliminary evidence of altered biomechanics in adolescents with juvenile fibromyalgia. Arthritis Care Res. 2015;67(1):102–111. doi:10.1002/acr.22450
31. Jones KD, King LA, Mist SD, Bennett RM, Horak FB. Postural control deficits in people with fibromyalgia: a pilot study. Arthritis Res Therap. 2011;13(4):R127. doi:10.1186/ar3432
32. Black WR, DiCesare CA, Wright LA, et al. The effects of joint hypermobility on pain and functional biomechanics in adolescents with juvenile fibromyalgia: secondary baseline analysis from a pilot randomized controlled trial. BMC Pediatric. 2023;23(1):557. doi:10.1186/s12887-023-04353-y
33. Fitzgibbon BM, Hoy KE, Knox LA, et al. Evidence for the improvement of fatigue in fibromyalgia: a 4-week left dorsolateral prefrontal cortex repetitive transcranial magnetic stimulation randomized-controlled trial. Eur. J. Pain. 2018;22(7):1255–1267. doi:10.1002/ejp.1213
34. Gracely RH, Schweinhardt P. Programmed symptoms: disparate effects united by purpose. Curr Rheumatol Rev. 2015;11(2):116–130. doi:10.2174/1573397111666150619095125
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multimorbidity Patterns and Associations with Gait, Balance and Lower Extremity Muscle Function in the Elderly: A Cross-Sectional Study in Northwest China
Yang K, Yang S, Chen Y, Cao G, Xu R, Jia X, Hou L, Li J, Bi C, Wang X
International Journal of General Medicine 2023, 16:3179-3192
Published Date: 28 July 2023
Balance and Gait Disorders in the Aged Population. Causes, Assessment and Management: A Literature Review
Manckoundia P, Mourey F, Larosa F, Renoncourt T
Clinical Interventions in Aging 2025, 20:1945-1962
Published Date: 11 November 2025
Efficacy of Tai Chi and Roliball Exercise on Balance, Mobility, and Cognitive Function in Community-Dwelling Older Adults: A Randomized Controlled Trial
Yang Y, Li E, Hua Y, Yang X, Zhao Z, Zhu X, Li X, Tang J
Clinical Interventions in Aging 2025, 20:1975-1992
Published Date: 12 November 2025
Biopsychosocial Factors Affecting Disability in Individuals with Chronic Nonspecific Low Back Pain: A Cross-Sectional Study
Canli İ, Özüdoğru A
Journal of Pain Research 2026, 19:590191
Published Date: 13 March 2026