Back to Journals » Journal of Pain Research » Volume 19
Biopsychosocial Factors Affecting Disability in Individuals with Chronic Nonspecific Low Back Pain: A Cross-Sectional Study
Authors Canli İ ![]() , Özüdoğru A
, Özüdoğru A ![]()
Received 19 December 2025
Accepted for publication 11 March 2026
Published 13 March 2026 Volume 2026:19 590191
DOI https://doi.org/10.2147/JPR.S590191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
İrem Canli, Anıl Özüdoğru
Department of Physiotherapy and Rehabilitation, Kırşehir Ahi Evran University, School of Physical Therapy and Rehabilitation, Kırşehir, Turkey
Correspondence: İrem Canli, Department of Physiotherapy and Rehabilitation, Kırşehir Ahi Evran University, School of Physical Therapy and Rehabilitation, Kırşehir, Turkey, Tel +905348377384, Email [email protected]
Purpose: Chronic nonspecific low back pain (CNLBP) is a multifactorial condition influenced by clinical, physical, and psychological factors and is associated with pain, impaired balance, reduced muscle performance, kinesiophobia, and altered spinal mechanics. This cross-sectional study aimed to identify the clinical, psychological, and physical performance–related factors associated with disability in individuals with CNLBP.
Patients and Methods: A total of 252 individuals diagnosed with CNLBP were included in the study. Each individual was evaluated using the Oswestry Disability Index (ODI), Visual Analog Scale (VAS), Biodex balance device, Five Times Sit and Stand Test (FTSST), Tampa Kinesiophobia Scale (TKS), Timed Up and Go Test (TUG), goniometric measurement, Beck Depression Inventory (BDI), and spinal mouse. Relationships between variables were examined using multiple linear regression was performed to identify independent predictors of disability.
Results: Significant correlations were found between ODI and VAS, TKS, BDI, lumbar range of motion values, FTSST, static and dynamic balance values, TUG, and spinal evaluations. In addition, these related parameters explained 81.1% of the variance of ODI score, according to the results of linear regression analysis. In addition, according to the results of linear regression analysis, VAS activity, TKS, FTSST, lumbar extension angle, TUG, spinal posture score, spinal control score, static anteroposterior, and dynamic overall balance score were found to be independent predictors of ODI score. Our study showed that activity pain intensity, kinesiophobia level, lower extremity muscle strength, static anteroposterior and dynamic total balance score, lumbar extension angle, functional status, spinal posture, and spinal control score were predictors of disability level in individuals with CNLBP.
Conclusion: Activity pain, kinesiophobia, lower extremity strength, lumbar extension, functional status, spinal posture and control, and balance were independent predictors of disability in individuals with CNLBP. These factors should be considered when developing evaluation and treatment programs for CNLBP.
Keywords: pain, disability, balance, posture
Introduction
Low back pain (LBP) is one of the most common musculoskeletal problems worldwide, and a substantial proportion of cases progress to a chronic and nonspecific form. Approximately 10–40% of individuals with acute LBP develop chronic symptoms, and nearly 85% of chronic cases are classified as nonspecific.1 Although the exact pathophysiology of chronic nonspecific low back pain (CNLBP) remains unclear; however, it is widely accepted that biological, psychological, and social factors interact to influence its onset and persistence. CNLBP leads to reduced mobility, limitations in daily activities, and considerable physical, psychological, and economic burden.2
Disability is a key consequence of CNLBP and contributes significantly to its overall impact.3 While pain intensity is the primary predictor of disability in acute stages, psychosocial, functional, and biomechanical factors become increasingly influential as the condition becomes chronic.4 LBP has been identified as the leading cause of years lived with disability globally, reflecting its substantial public health burden.5 Moreover, disability related to chronic LBP results in decreased physical activity levels, diminished quality of life, and increased healthcare expenditures.6,7
Previous studies have primarily focused on pain severity or prevalence, yet the factors contributing to disability in individuals with CNLBP have not been thoroughly examined.8,9 Given that CNLBP-related disability is multifactorial, identifying the specific determinants that influence functional limitations is essential for developing effective rehabilitation strategies. Understanding these determinants also guides clinicians in tailoring evaluation and treatment programs based on individual needs.10 Accordingly, the present study aimed to investigate the clinical, psychological, and physical performance related factors associated with disability levels in individuals with CNLBP.
Materials and Methods
Study Design
The cross-sectional study was conducted between September 2024 and March 2025. Written and verbal informed consent was obtained from all participants, and the study was conducted in accordance with the principles of the Declaration of Helsinki. A limited number of comprehensive studies examining the factors affecting disability in individuals with CNLBP were found.
Participants
The participants were individuals who were diagnosed with CNLBP and referred to XXX for treatment. The inclusion criteria were to be between the ages of 18 and 65 years, to volunteer to participate in the study, and to have LBP complaints localized between the inferior gluteal region and the last costa and persisting for at least 3 months. Individuals with nerve root compression, uncontrolled metabolic, neurologic, cardiac, or hypertension diseases, inability to walk without a walking aid, or any other musculoskeletal disease that may affect the assessment results and balance were excluded.
Measurements
Sociodemographic data of the participants were collected face-to-face. Participants’ disability level, pain severity, balance level, lower extremity muscle strength, kinesiophobia level, functional status, range of motion, depression severity, and posture were evaluated by the same researcher. All assessments were conducted by a trained physiotherapist who was experienced in neuromuscular evaluation.
Outcome Measurements
Disability Level
The Turkish version of the Oswestry Disability Index (ODI) was used to assess the disability level of the participants. This scale is valid and reliable for assessing the level of disability in individuals with LBP (intraclass correlation coefficient [ICC] = 0.938). There are 6 options for each question in the questionnaire, which consists of a total of 10 questions. These options are scored from 0 to 5, and the result is obtained by taking the percentage of the score relative to the maximum score. Higher scores indicate an increased level of disability.11
Pain Severity
A visual analog scale (VAS) was used to assess the participants current pain intensity at night, at rest, and during activity. The scale has a 10 cm long line on which the patient can mark the intensity of pain. There, the patient was asked to indicate the degree of pain intensity between no pain (left side) and excruciating pain (right side).12
Kinesiophobia
The Tampa Kinesiophobia Scale (TKS), which is validated and reliable in Turkish, was used to assess the presence and level of kinesiophobia in the participants (ICC=0.867). This scale questions the increase in pain caused by movement, anxiety and fear of injury, and the and avoidance behavior resulting from pain. The scale consists of 17 items, and each item is scored on a Likert scale from 1 (strongly disagree) to 4 (strongly agree). A high score indicates a high level of kinesiophobia.13
Depression
The Turkish version of the Beck Depression Inventory (BDI) was used to assess the presence and severity of depression in the participants. The Turkish version has been shown to be valid and reliable, demonstrating excellent test–retest reliability (ICC= 0.93). This inventory has 21 items, and each of these items is scored between 0 and 3. A score between 0 and 63 is obtained from the scale. An increase in the score obtained from the scale indicates an increase in the severity of depression.14
Range of Joint Motion
Extension, flexion, and left and right lateral flexion movements were evaluated for the range of motion (ROM) values of the participants in the lumbar region. ROM values were recorded using a goniometer. The pivot point, fixed arm, and movable arm of the goniometer were placed at the points determined in accordance with the international evaluation principles. The range of motion was then measured while the patient was performing the active movement. The measured values were recorded in degrees.15
Lower Extremity Muscle Strength
The lower extremity muscle strength of the participants was evaluated with the five times sit and stand test (FTSST). The FTSST has been found to be reliable in patients with CNLBP and is a simple, rapid, and reproducible method used to assess lower extremity muscle strength.16 During the test, participants were asked to sit on a standard chair with their hands crossed over their chest and to sit and stand in this position five times. Test duration was measured in seconds with a stopwatch. A long duration in the FTSST indicates weak lower extremity muscle strength.16
Balance
The Biodex Balance System, which has proven its validity and reliability, was used to evaluate the balance levels of individuals with CNLBP (ICC = 0.82–0.95). The assessment was performed through the static and dynamic measurement modules of the device. The platform, which has an inclination of approximately 20° and a range of motion of 360°, measures the balance performance of individuals by moving in the mediolateral (M-L) and anteroposterior (A-P) directions. The device evaluates the degree of inclination of the platform in dynamic mode and the deviation of the center of pressure in static mode. The difficulty level of the test can be adjusted by changing the stability level of the platform. The stability level ranges from 0 (highest stability) to 12 (lowest stability), and in this study, ground stability was determined as level 6. High scores indicate poor balance and postural control.17
Functional Status
Functional status of individuals diagnosed with CNLBP was evaluated with the Timed Up-and-Go Test (TUG), which has proven to be reliable in individuals with CLBP (ICC= 0.92–0.99).18 Participants were asked to sit on a chair of standard height, then stand up and walk 3 meters forward, turn around, and sit back on the chair. The test time was recorded in seconds with a stopwatch. A prolonged test time indicates a negative impact on functional status.18
Spinal Evaluation
Spinal evaluation was performed using the Spinal Mouse® system (Idiag, Fehraltorf, Switzerland), a portable and computer-assisted device that provides reliable measurements of spinal posture, mobility, and postural endurance (ICC = 0.89–0.98).19 The device is guided manually along the spinous processes from C7 to S3 while participants maintain standardized postures. For spinal posture assessment, measurements were taken in a relaxed upright standing position to determine the sagittal alignment of the spine. Spinal mobility was evaluated by repeating the measurement while the participant performed maximum trunk flexion, allowing assessment of global lumbar and thoracic motion. Postural endurance was assessed by having participants hold a load equivalent to approximately 5% of their body weight with shoulders positioned at 90° flexion for 30 seconds, after which a second measurement was obtained without altering posture. All measurements were recorded automatically by the software, and higher scores indicated poorer spinal performance depending on the parameter evaluated.
Sample Size
Accordingly, using the G*Power program (Version 3.1.9.4.3, Heinrich-Heine Universität, Düsseldorf, Germany), a minimum sample size of 210 was calculated with a 95% confidence level, 80% power (β), and 5% type I error (α). Considering a 15% dropout rate, a minimum of 242 individuals was required.20
Statistical Analysis
Data were analyzed using the statistical software SPSS (Statistical Package for the Social Sciences Inc., Chicago, IL, USA, Ver. 22.0). The conformity of the numerical variables to normal distribution was evaluated using visual (histogram and probability plots) and analytical methods (Kolmogorov–Smirnov). Descriptive statistics for numerical variables were given as mean and standard deviation, while descriptive statistics for categorical variables were given as number (n) and percentage. The relationships between variables were calculated by Pearson Correlation Analysis. Pearson correlation coefficients between 0.7 and 1.0 were considered as high correlation, between 0.4 and 0.7 as moderate correlation, and less than 0.4 as low correlation.21 Multiple linear regression analysis was used to determine the independent determinants of disability level. The statistical significance level was accepted as p < 0.05.
Results
A total of 263 individuals were screened for eligibility; 3 declined participation and 9 did not meet the inclusion criteria. Thus, 252 participants (134 women, 118 men) were included in the analysis. The demographic characteristics of the participants are presented in Table 1.
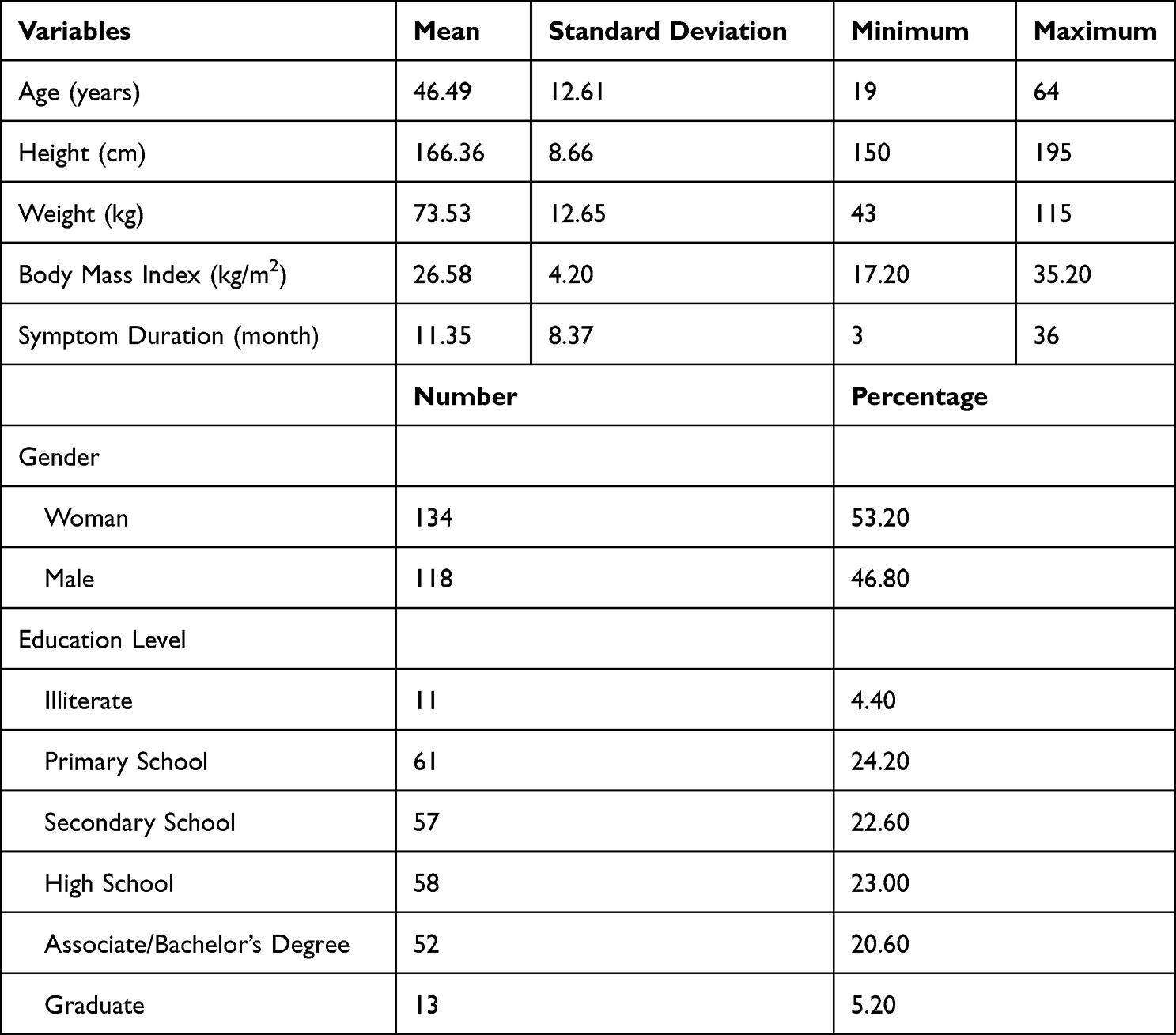 |
Table 1 Demographic Information of the Participants |
The clinical evaluation results, including disability level, pain intensity, balance parameters, spinal assessment scores, range of motion measurements, lower extremity muscle strength, kinesiophobia, depression severity, and functional status, are summarized in Table 2.
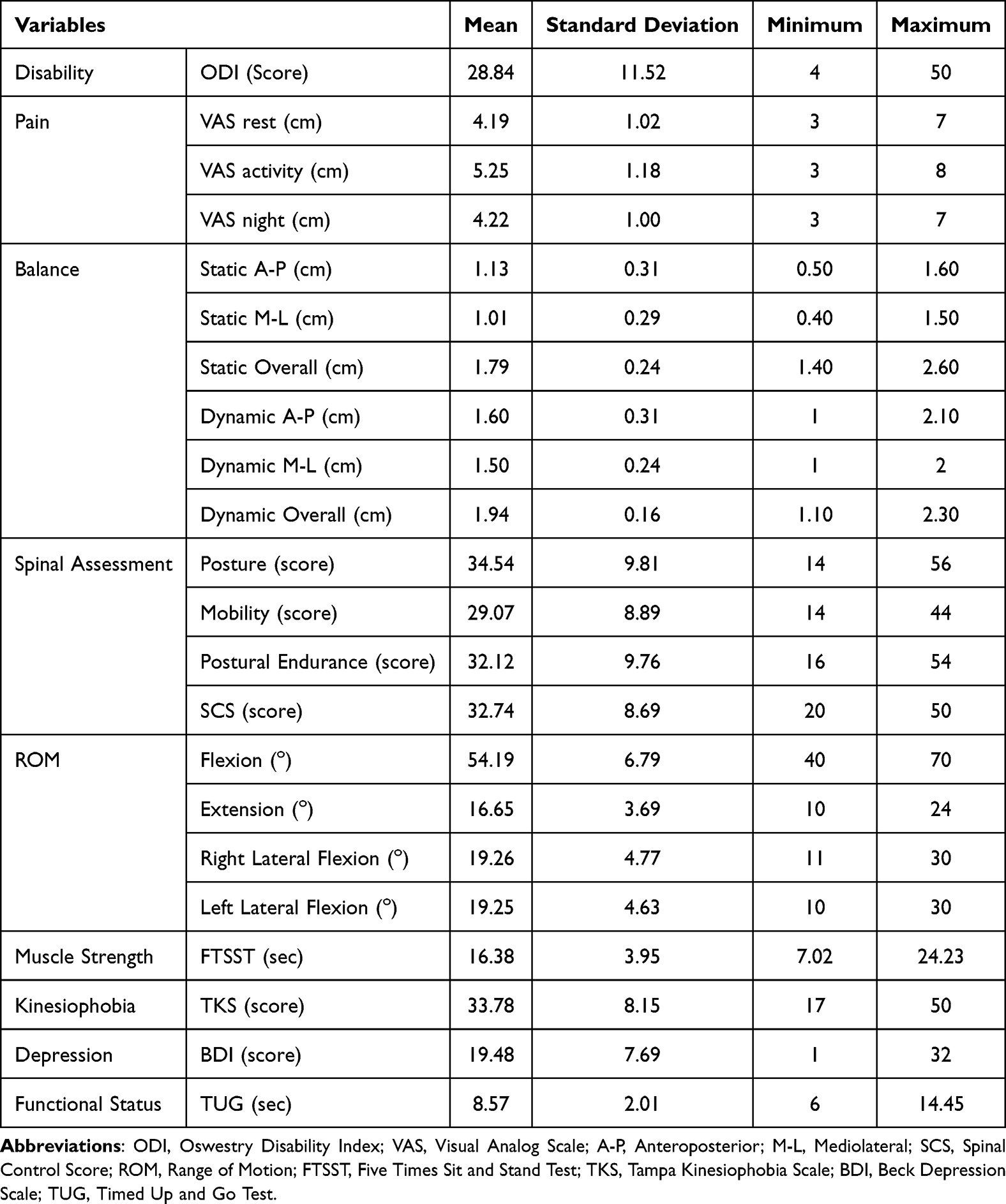 |
Table 2 Clinical Evaluation of the Participants |
The correlation analysis results between ODI and other variables are presented in Table 3. ODI demonstrated a moderate positive correlation with VAS (rest, activity, night), static and dynamic A–P balance scores, static M–L score, dynamic overall balance score, FTSST, TKS, and BDI. A moderate negative correlation was found between ODI and spinal posture and SCS. ODI showed a low but significant negative correlation with spinal mobility, postural endurance, and lumbar ROM values (flexion, extension, and lateral flexion). Dynamic M–L and dynamic total scores showed low positive correlations with ODI.
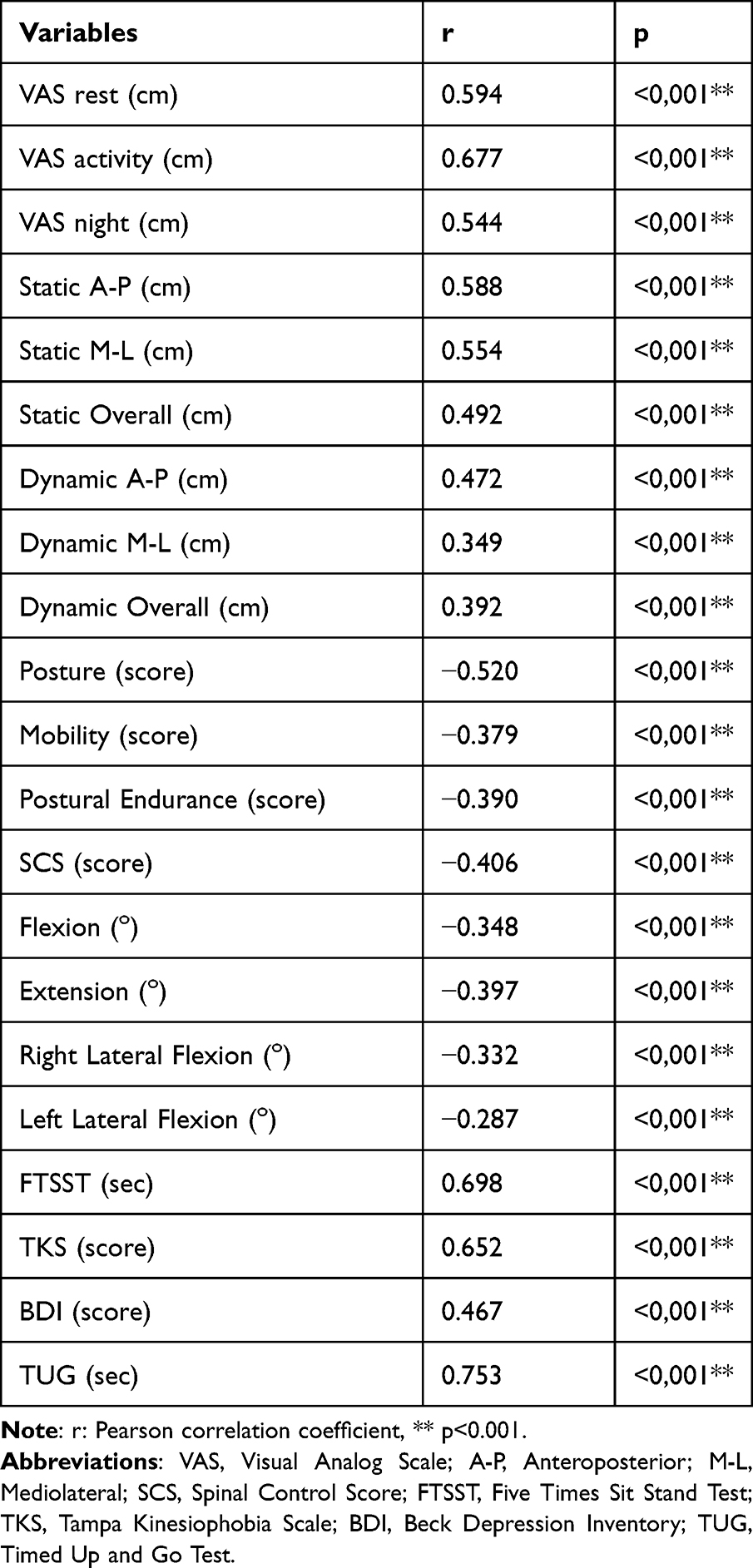 |
Table 3 Association Between Disability Scores and Other Parameters |
The results of the linear regression analysis conducted to determine the independent predictors of ODI are given in Table 4. According to the results of the analysis, VAS rest, VAS activity, VAS night, static A-P, static M-L, static total, dynamic A-P, dynamic M-L, dynamic total, posture, mobility, endurance, spinal control score, lumbar flexion, lumbar extension, lumbar right and left lateral flexion angles, FTSST, TKS, BDI, and TUG explained 81.1% of the variance of ODI score of individuals with CNLBP. Among these variables, VAS activity, static A–P, dynamic overall balance, spinal posture, spinal control score, lumbar extension angle, FTSST, TKS, and TUG emerged as independent predictors of disability level in individuals with CNLBP.
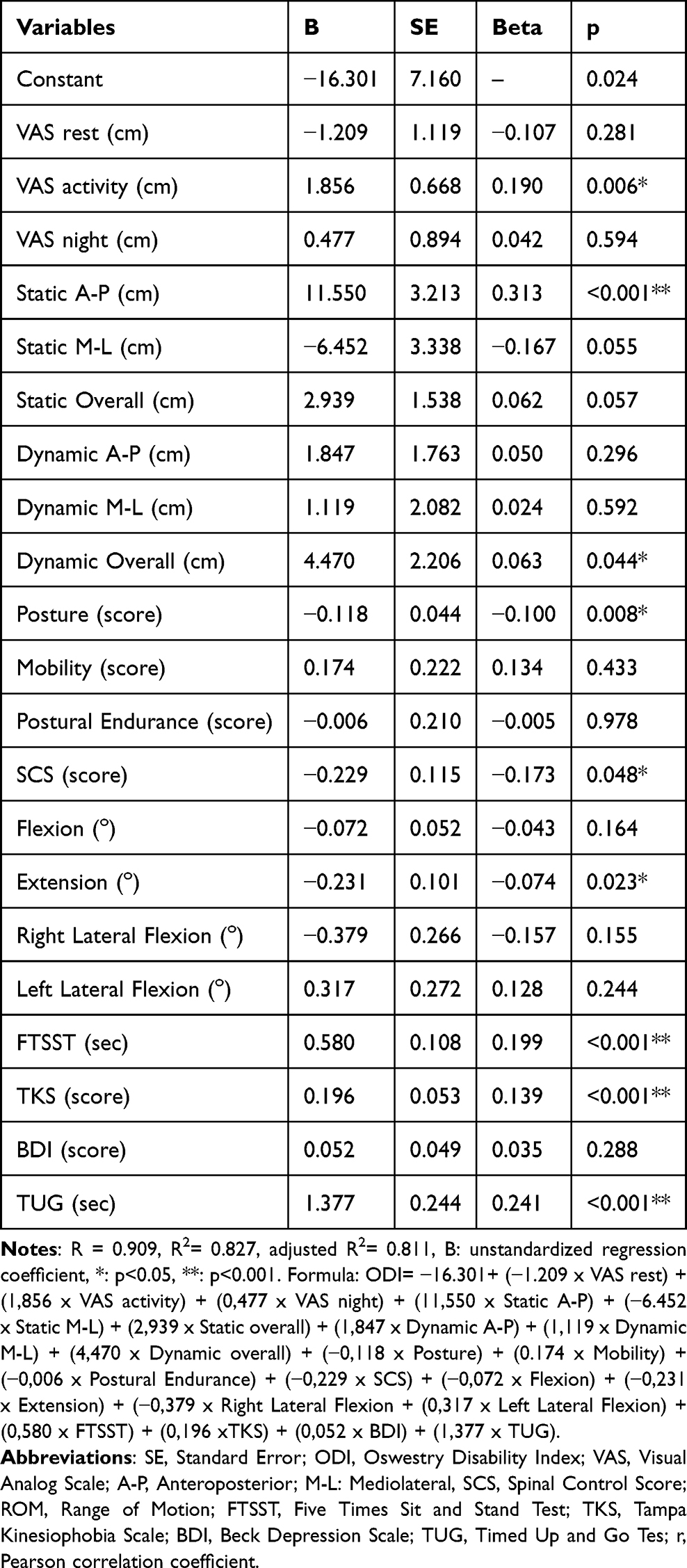 |
Table 4 Linear Regression Model of ODI |
Discussion
The present study investigated the factors associated with disability in individuals with chronic nonspecific low back pain (CNLBP) using a comprehensive set of physical, psychosocial, and functional assessments. The results demonstrated that disability level was significantly associated with pain intensity, kinesiophobia, depression, lumbar range of motion, lower extremity muscle strength, balance, functional status, and spinal parameters. Furthermore, activity-related pain, kinesiophobia, lower extremity muscle strength, static anteroposterior and dynamic overall balance, lumbar extension angle, functional status, spinal posture, and spinal control score emerged as independent predictors of disability. Together, these factors explained 81.1% of the variance in ODI scores, highlighting the multifactorial nature of disability in CNLBP.
Pain intensity showed a moderate positive association with disability, supporting previous findings suggesting that pain remains a major driver of functional limitation in CNLBP.1,22,23 Activity-related pain emerged as an independent predictor, indicating that pain during movement may be more strongly linked to disability than pain at rest. This relationship may reflect avoidance of daily activities, deconditioning, and behavioral changes that reinforce disability over time.24
These findings also have important clinical implications. The identification of activity-related pain, kinesiophobia, balance impairments, functional mobility limitations, lumbar extension angle, and spinal posture and control as independent predictors underscores the multidimensional nature of disability in CNLBP.8 The high amount of explained variance in the regression model (adjusted R2 = 0.811) indicates that evaluating these domains together provides a more realistic understanding of disability than focusing on pain alone. Therefore, rehabilitation programs should integrate approaches that target movement-related pain, address fear-avoidance beliefs, improve balance and functional mobility, and enhance spinal mobility and neuromuscular control. Such multidimensional strategies may yield more meaningful improvements in daily functioning and disability levels.
Balance impairments are frequently observed in individuals with LBP, likely due to altered proprioceptive input, decreased muscle feedback, and changes in postural control strategies.25,26 Consistent with this evidence, the present study found significant associations between disability and both static and dynamic balance parameters. Static anteroposterior and dynamic overall scores were independent predictors, suggesting that deficits in maintaining postural stability, particularly in challenging conditions, may contribute substantially to disability. Pain-related postural adaptations, shifts in the center of gravity, and reduced neuromuscular control may underlie this relationship.27
ROM was negatively correlated with disability, aligning with earlier studies reporting that restricted lumbar mobility is a key contributor to functional decline.28,29 Of the ROM parameters, lumbar extension emerged as an independent predictor. Reduced extension may reflect increased spinal stiffness, muscle shortening, altered loading patterns, or protective movement strategies, all of which can interfere with daily function and exacerbate disability.30
Lower extremity muscle strength was also strongly related to disability.31 Participants with poorer FTSST performance had higher disability scores, consistent with studies demonstrating that reduced hip and lower limb strength contributes to lumbopelvic instability and functional limitation.16,32 Muscle weakness in CNLBP may develop due to disuse, pain-induced inhibition, and altered movement patterns, further limiting physical capacity.33
Psychological factors also played a significant role.34 Kinesiophobia showed a moderate positive correlation with disability and was an independent predictor, consistent with literature emphasizing the role of fear-avoidance beliefs in the chronicity and severity of LBP.35–37 High levels of movement-related fear may lead to activity restriction, muscle deconditioning, and hypervigilance, all of which reinforce disability.38 Depression was associated with disability, in line with prior evidence39,40 although it was not an independent predictor in the regression model. Psychological distress may contribute to pain perception, behavioral avoidance, and reduced engagement in daily activities.41
Functional status, assessed by the TUG test, exhibited the strongest correlation with disability and was an independent predictor. Previous studies have similarly shown that reduced functional mobility is tightly linked to disability in CNLBP.42,43 Pain-induced alterations in gait, reduced lower limb strength, and impaired postural control may collectively limit mobility and daily functioning.
Proper lumbopelvic alignment is essential for coordinated neuromuscular control, and disruptions in this system may alter load distribution, movement strategies, and segmental interactions, contributing to postural changes commonly observed in individuals with LBP.44,45 Previous studies have shown that spinal posture, mobility, and endurance are closely related to disability in nonspecific LBP,46–48 suggesting that insufficient postural control may compromise spinal stability and functional capacity. Consistent with this evidence, our study identified a moderate negative association between disability and spinal posture, as well as low negative associations with spinal mobility and postural endurance. These findings indicate that reduced postural efficiency and diminished spinal control may increase mechanical stress on the spine over time, and the cumulative effects of improper loading may contribute to higher levels of disability.49
This study identified activity pain intensity, kinesiophobia level, lower extremity muscle strength, static anteroposterior and dynamic total balance scores, lumbar extension angle, functional status, spinal posture, and spinal control score as significant predictors of disability in individuals with CNLBP. These findings provide clinicians with a perspective beyond pain alone, highlighting the importance of comprehensive assessment. Recognizing the factors affecting disability and their relative impact can guide targeted evaluation and treatment strategies, helping to prioritize interventions that may improve functional outcomes and reduce disability in this population.
This study has several limitations. First, disability, pain, kinesiophobia, and depression were assessed using self-reported measures, which may be influenced by individual perception. Second, the absence of a healthy control group limits the ability to compare impairment levels. Third, other potential factors influencing disability in individuals with CNLBP, such as physical activity level, occupational characteristics, spinal deformities, and lifestyle factors, were not assessed. However, the use of objective tools for spinal and balance assessment is a notable strength. Future research should consider longitudinal and multicenter designs to better understand the causal pathways leading to disability and to verify the predictive relevance of the identified factors.
Conclusion
The current study examined the determinants affecting the level of disability in individuals with CNLBP. The results of the study showed that activity pain intensity, kinesiophobia level, lower extremity muscle strength, static anteroposterior and dynamic total balance score, lumbar extension angle, functional status, spinal posture, and spinal control score were predictors of disability level in individuals with CNLBP. Determining the parameters associated with disability in individuals with CNLBP may provide clinicians with a perspective beyond pain. Knowing the factors affecting disability and their levels may help determine which variables should be emphasized in treatment and evaluations.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available due to privacy or ethical restrictions. But are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Ethical approval was obtained by the Kırşehir Ahi Evran University, Health Sciences Scientific Research Ethics Committee (Number: 2024-15/133). Written and verbal informed consent was obtained from the participants before the study.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Sirbu E, Onofrei RR, Szasz S, Susan M. Predictors of disability in patients with chronic low back pain. Arch Med Sci. 2023;19(1):94. doi:10.5114/aoms.2020.97057
2. Ronai P, Sorace P. Chronic nonspecific low back pain and exercise. Strength Condition J. 2013;35(1):29–11. doi:10.1519/SSC.0b013e3182822bb1
3. Uçurum SG, Kalkan AC. The relationship between pain, kinesiophobia and quality of life in patients with low back pain. Ege J Med. 2018;57(3):131–135.
4. Froud R, Patterson S, Eldridge S, et al. A systematic review and meta-synthesis of the impact of low back pain on people’s lives. BMC Musculoskeletal Disord. 2014;15(1):1–14. doi:10.1186/1471-2474-15-50
5. Weinstein S, Yelin E, Watkins-Castillo S. United States bone and joint initiative: the burden of musculoskeletal diseases in the United States (BMUS) 2020. Rosemont, IL. 2021.
6. Becker A, Held H, Redaelli M, et al. Low back pain in primary care: costs of care and prediction of future health care utilization. Spine. 2010;35(18):1714–1720. doi:10.1097/BRS.0b013e3181cd656f
7. Kuzu Ş, Canli M, Valamur İ, Özüdoğru A, Alkan H, Hartavi A. Effects of aerobic exercise in addition to core stabilization exercises on functional capacity, physical performance and fall risk in geriatric individuals with chronic non-specific low back pain. BMC Sports Sci Med Rehabil. 2025;17(1):218. doi:10.1186/s13102-025-01271-7
8. Schiphorst Preuper H, Reneman M, Boonstra A, et al. Relationship between psychological factors and performance-based and self-reported disability in chronic low back pain. Euro Spine J. 2008;17(11):1448–1456. doi:10.1007/s00586-008-0772-0
9. Luo X, Pietrobon R, Sun SX, Liu GG, Hey L. Estimates and patterns of direct health care expenditures among individuals with back pain in the United States. Spine. 2004;29(1):79–86. doi:10.1097/01.BRS.0000105527.13866.0F
10. Urquhart DM, Bell R, Cicuttini FM, Cui J, Forbes A, Davis SR. Low back pain and disability in community-based women: prevalence and associated factors. Menopause. 2009;16(1):24–29. doi:10.1097/gme.0b013e31817e5ce0
11. Yakut E, Düger T, Öksüz Ç, et al. Validation of the Turkish version of the oswestry disability index for patients with low back pain. Spine. 2004;29(5):581–585. doi:10.1097/01.BRS.0000113869.13209.03
12. Faiz KW. VAS–visuell analog skala. Tidsskrift Den norske legeforening. 2014;134:323. doi:10.4045/tidsskr.13.1145
13. Yilmaz O, Yakut Y, Uygur F, Ulug N. Turkish version of the Tampa Scale for Kinesiophobia and its test-retest reliability. Turkish J Physiotherapy Rehabil Fizyoterapi Rehabilitasyon. 2011;22(1).
14. Ulusoy M, Sahin NH, Erkmen H. Turkish version of the beck anxiety inventory: psychometric properties. J Cognitive Psychotherapy. 1998;12(2):163.
15. Shamsi M, Mirzaei M, Khabiri SS. Universal goniometer and electro-goniometer intra-examiner reliability in measuring the knee range of motion during active knee extension test in patients with chronic low back pain with short hamstring muscle. BMC Sports Sci Med Rehabil. 2019;11(1):1–5. doi:10.1186/s13102-019-0116-x
16. Özüdoğru A, Canlı M, Ceylan İ, Kuzu Ş, Alkan H, Karaçay BÇ. Five times sit-to-stand test in people with non-specific chronic low back pain—a cross-sectional test–retest reliability study. Irish J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
17. Glave AP, Didier JJ, Weatherwax J, Browning SJ, Fiaud V. Testing postural stability: are the star excursion balance test and biodex balance system limits of stability tests consistent? Gait Posture. 2016;43:225–227. doi:10.1016/j.gaitpost.2015.09.028
18. Simmonds MJ, Olson SL, Jones S, et al. Psychometric characteristics and clinical usefulness of physical performance tests in patients with low back pain. Spine. 1998;23(22):2412–2421. doi:10.1097/00007632-199811150-00011
19. Mannion AF, Knecht K, Balaban G, Dvorak J, Grob D. A new skin-surface device for measuring the curvature and global and segmental ranges of motion of the spine: reliability of measurements and comparison with data reviewed from the literature. Euro Spine J. 2004;13(2):122–136. doi:10.1007/s00586-003-0618-8
20. Fransen M, Woodward M, Norton R, Coggan C, Dawe M, Sheridan N. Risk factors associated with the transition from acute to chronic occupational back pain. Spine. 2002;27(1):92–98. doi:10.1097/00007632-200201010-00022
21. Schober P, Boer C, Schwarte LA. Correlation coefficients: appropriate use and interpretation. Anesthes Analges. 2018;126(5):1763–1768. doi:10.1213/ANE.0000000000002864
22. Kocaman H, Alkan H, Ceylan İ, Canlı M, Yumuşak Ş. Investigation of factors associated with pain level in individuals with chronic non-specific low back pain. Hacettepe Univ Faculty Health Sci J. 2023;10(3):777–787. doi:10.21020/husbfd.1245196
23. Kuzu Ş, Özüdoğru A, Tuncay F. Effects of external and internal focus of attention exercises in chronic low back pain: a randomized controlled trial. Pain Manage Nurs. 2025;26:e448–e455. doi:10.1016/j.pmn.2025.02.011
24. Chung EJ, Hur Y-G, Lee B-H. A study of the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain. J Exercise Rehabil. 2013;9(6):532. doi:10.12965/jer.130079
25. Ruhe A, Fejer R, Walker B. Is there a relationship between pain intensity and postural sway in patients with non-specific low back pain? BMC Musculoskeletal Disord. 2011;12(1):1–8. doi:10.1186/1471-2474-12-162
26. Kelečić IL, Schuster S, Masharawi Y. Static balance and its association with pain and disability in females with low back pain-a pilot cross-sectional study. Phys Activity Rev. 2023;11(1).
27. Kim D-H, Park J-K, Jeong M-K. Influences of posterior-located center of gravity on lumbar extension strength, balance, and lumbar lordosis in chronic low back pain. J Back Musculoskeletal Rehabil. 2014;27(2):231–237. doi:10.3233/BMR-130442
28. La Touche R, Pérez-Fernández M, Barrera-Marchessi I, et al. Psychological and physical factors related to disability in chronic low back pain. J Back Musculoskeletal Rehabil. 2019;32(4):603–611. doi:10.3233/BMR-181269
29. Behennah J, Conway R, Fisher J, Osborne N, Steele J. The relationship between balance performance, lumbar extension strength, trunk extension endurance, and pain in participants with chronic low back pain, and those without. Clin Biomech. 2018;53:22–30. doi:10.1016/j.clinbiomech.2018.01.023
30. Rainville J, Nguyen R, Suri P. Effective conservative treatment for chronic low back pain. Elsevier. 2009;257–263.
31. Himmelreich H, Vogt L, Banzer W. Gluteal muscle recruitment during level, incline and stair ambulation in healthy subjects and chronic low back pain patients. J Back Musculoskeletal Rehabil. 2008;21(3):193–199. doi:10.3233/BMR-2008-21307
32. Penney T, Ploughman M, Austin MW, Behm DG, Byrne JM. Determining the activation of gluteus medius and the validity of the single leg stance test in chronic, nonspecific low back pain. Arch Phys Med Rehabil. 2014;95(10):1969–1976. doi:10.1016/j.apmr.2014.06.009
33. De Sousa CS, de Jesus FLA, Machado MB, et al. Lower limb muscle strength in patients with low back pain: a systematic review and meta-analysis. J Musculoskeletal Neuro Interact. 2019;19(1):69.
34. Kendall NAS. Psychosocial approaches to the prevention of chronic pain: the low back paradigm. Best Prac Res Clin Rheumatol. 1999;13(3):545–554. doi:10.1053/berh.1999.0044
35. Ishak NA, Zahari Z, Justine M. Kinesiophobia, pain, muscle functions, and functional performances among older persons with low back pain. Pain Res Treatment. 2017;2017(1):3489617. doi:10.1155/2017/3489617
36. Grotle M, Vøllestad NK, Brox JI. Clinical course and impact of fear-avoidance beliefs in low back pain: prospective cohort study of acute and chronic low back pain: II. Spine. 2006;31(9):1038–1046. doi:10.1097/01.brs.0000214878.01709.0e
37. Comachio J, Magalhães MO, Campos Carvalho e Silva APDM, Marques AP. A cross-sectional study of associations between kinesiophobia, pain, disability, and quality of life in patients with chronic low back pain. Adv Rheumatol. 2018;58(1):8. doi:10.1186/s42358-018-0011-2
38. Odole A, Ogunlana M, Dada O, Williams O. Kinesiophobia, self-efficacy and pain-related disability in patients with non-specific low back pain. African J Physiotherapy Rehabil Sci. 2018;8(1–2):38–43. doi:10.4314/ajprs.v8i1-2.6
39. Nassar N, Assaf N, Farrag D, Ibrahim D, Al-Sheekh A. Depression in patients with chronic low back pain. Egyptian Rheumatol Rehabil. 2019;46(1):48–54. doi:10.4103/err.err_32_18
40. Hung C-I, Liu C-Y, Fu T-S. Depression: an important factor associated with disability among patients with chronic low back pain. Int J Psychiatry Med. 2015;49(3):187–198. doi:10.1177/0091217415573937
41. Cankurtaran D, Aykın Yığman Z. Kronik Bel veya Boyun Ağrılı Hastalarda Anksiyete ve Depresyonun Ağrı Şiddeti ve Ağrı ile İlişkili Disabiliteye Etkisinin İncelenmesi. J Physical Med Rehabil Sci. 2022;25(2).
42. Di Iorio A, Abate M, Guralnik JM, et al. From chronic low back pain to disability, a multifactorial mediated pathway: the InCHIANTI study. Spine. 2007;32(26):E809–E815. doi:10.1097/BRS.0b013e31815cd422
43. Zhang S, Yang H, Luo B, Cheng Y, Niu S, Yang C. Factors affecting functional disability in patients with non-specific chronic low back pain: a cross-sectional study. Front Neurol. 2024;15:1367400. doi:10.3389/fneur.2024.1367400
44. Manchikanti L. Epidemiology of low back pain. Pain Physician. 2000;2;3(4;3):167–192. doi:10.36076/ppj.2000/3/167
45. Pinto RZA, Souza TR, Trede RG, Kirkwood RN, Figueiredo EM, Fonseca ST. Bilateral and unilateral increases in calcaneal eversion affect pelvic alignment in standing position. Manual Therapy. 2008;13(6):513–519. doi:10.1016/j.math.2007.06.004
46. Cox ME, Asselin S, Gracovetsky SA, et al. Relationship between functional evaluation measures and self-assessment in nonacute low back pain. Spine. 2000;25(14):1817–1826. doi:10.1097/00007632-200007150-00013
47. Abbott JH, Fritz JM, McCane B, et al. Lumbar segmental mobility disorders: comparison of two methods of defining abnormal displacement kinematics in a cohort of patients with non-specific mechanical low back pain. BMC Musculoskeletal Disord. 2006;7(1):45. doi:10.1186/1471-2474-7-45
48. Vanti C, Conti C, Faresin F, Ferrari S, Piccarreta R. The relationship between clinical instability and endurance tests, pain, and disability in nonspecific low back pain. J Manipulat Physiolog Therapeu. 2016;39(5):359–368. doi:10.1016/j.jmpt.2016.04.003
49. Tüzün Ç, Yorulmaz İ, Cindaş A, Vatan S. Low back pain and posture. Clin Rheumatol. 1999;18(4):308–312. doi:10.1007/s100670050107
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Review of Movement and Functional Impairments in Fibromyalgia: Implications for Targeted Treatment
Quodling N, Hoffman N, Carrick FR, Jemni M
Journal of Pain Research 2025, 18:5587-5597
Published Date: 25 October 2025
Balance and Gait Disorders in the Aged Population. Causes, Assessment and Management: A Literature Review
Manckoundia P, Mourey F, Larosa F, Renoncourt T
Clinical Interventions in Aging 2025, 20:1945-1962
Published Date: 11 November 2025