Back to Journals » International Journal of Women's Health » Volume 17
Association Between the C-Reactive Protein–Albumin–Lymphocyte Index and Endometriosis: Insights from the 1999–2006 National Health and Nutrition Examination Survey
Authors Xu X, Cheng H, Ye X, Chang X
Received 7 August 2025
Accepted for publication 31 October 2025
Published 7 November 2025 Volume 2025:17 Pages 4267—4280
DOI https://doi.org/10.2147/IJWH.S558997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Everett Magann
Xinyu Xu, Hongyan Cheng, Xue Ye, Xiaohong Chang
Department of Obstetrics and Gynecology, People’s Hospital, Peking University, Beijing, People’s Republic of China
Correspondence: Xiaohong Chang, Department of Obstetrics and Gynecology, People’s Hospital, Peking University, Beijing, People’s Republic of China, Email [email protected]
Objective: The C-reactive protein–albumin–lymphocyte (CALLY) index serves as an integrated indicator, reflecting the interplay between systemic inflammation, immune competence, and nutritional health. While validated in other chronic diseases, its relevance to endometriosis remains unexplored. We aimed to assess its association with endometriosis using nationally representative data.
Methods: This cross-sectional analysis used data from four cycles of the National Health and Nutrition Examination Survey (NHANES, 1999– 2006), including 4,602 US adults. The CALLY index was derived by integrating measurements of C-reactive protein (CRP) levels, serum albumin concentrations, and lymphocyte counts. Associations with endometriosis were estimated using weighted multivariable logistic regression across three progressively adjusted models. The discriminatory ability of CALLY was assessed using receiver operating characteristic (ROC) analyses and compared against that of other commonly used inflammatory biomarkers. Smoothed curve fitting and subgroup/interaction analyses assessed pattern and heterogeneity.
Results: Log-transformed CALLY values (ln CALLY) levels showed a statistically significant inverse relationship with endometriosis prevalence (OR = 0.87; 95% CI: 0.79– 0.96). Individuals in the top quartile of ln CALLY (Q4) had a 40% lower risk of endometriosis than those in the bottom quartile (Q1) (OR = 0.60, 95% CI: 0.41– 0.87). Compared to other commonly used indices, CALLY exhibited superior discriminatory performance, achieving an AUC of 0.7219 (95% CI: 0.6970– 0.7468) in the fully adjusted model. Curve fitting indicated that higher CALLY index levels were linked to a reduced likelihood of endometriosis. Subgroup analysis further confirmed the consistency and independence of this relationship (all p values for interactions > 0.05).
Conclusion: A significant inverse association was observed between the CALLY index and endometriosis prevalence among American adults, supporting its potential as a novel inflammatory marker for identifying individuals at elevated risk. However, as a cross-sectional study, causality cannot be inferred. Future prospective cohorts across diverse populations are needed to evaluate its clinical utility for risk prediction and early identification.
Keywords: endometriosis, CALLY index, NHANES, association, nutrition, inflammation
Introduction
Endometriosis is an estrogen-dependent disorder characterized by the ectopic growth of endometrial-like tissue outside the uterine cavity and is commonly associated with pain and infertility.1 Statistically, endometriosis impacts approximately 10% (190 million) of women of reproductive age globally, significantly affecting reproductive health, quality of life, and overall well-being.2 Although endometriosis is highly prevalent, the absence of uniform diagnostic standards and the wide variability in clinical presentation often contribute to considerable delays in both diagnosis (up to 10 years) and treatment.3 In addition, endometriosis exhibits malignancy-like features such as implantation, invasiveness, and recurrence, and endometriosis-associated ovarian cancer from its malignant transformation has become a serious clinical problem.4,5 Therefore, early identification of individuals at high risk for endometriosis is crucial for timely clinical intervention. Although various emerging biomarker modalities—including omics-based approaches such as metabolomics—are under investigation to facilitate earlier detection, none have yet demonstrated sufficient reproducibility or clinical feasibility for widespread clinical implementation.6 This underscores the ongoing need for clinically accessible and systemically integrative biomarkers that may serve as alternative or complementary tools in the early detection of endometriosis.
The pathogenesis of endometriosis remains incompletely understood, despite advances in research. Emerging research indicates that immunological dysfunction, persistent inflammatory responses, and nutritional status are critical contributors to its development and progression. Patients exhibit an aberrant immunological microenvironment that enables retrograde menstruation-derived endometrial cells to evade immune surveillance. Moreover, circulating pro-inflammatory cytokines and altered immune-cell subsets contribute to a chronic, systemic inflammatory state extending beyond the pelvic cavity.2,7–9 Inflammatory biomarkers obtained from complete blood count data—such as the systemic inflammation index (SII), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic inflammation response index (SIRI), derived NLR (dNLR), neutrophil-percentage-to-albumin ratio (NPAR), and pan-immune-inflammation value (PIV)—have been widely investigated for their associations with endometriosis.10–12 However, findings remain inconsistent across populations and study designs, owing to variability in sample sizes, diagnostic criteria, and analytical analytical approaches. Moreover, these indices typically reflect only a single dimension of systemic response—such as inflammation or immune status—limiting their predictive value and clinical utility. In addition, growing evidence suggests that nutritional factors also influence the severity and clinical presentation of endometriosis, with targeted dietary interventions showing potential in symptom management.13,14 Overall, the dynamic interaction between immunity, inflammation, and nutrition forms a complex vicious cycle that contributes to disease progression.
The CALLY index, a novel composite biomarker integrating C-reactive protein, albumin, and lymphocyte count, was first proposed by Iida et al in 2022 and has since been validated as a prognostic indicator in various malignancies.15,16 Its clinical utility has since extended to cardiovascular, respiratory, and critical care conditions.17–19 In an observational study, the CALLY index outperformed other traditional prognostic indicators, such as SII, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and modified Glasgow prognostic score, in terms of predicting the accuracy of mortality risk in patients with colorectal cancer.20 In contrast to conventional indices that reflect only a single physiological process, the CALLY index captures the interplay among systemic inflammation, nutritional status, and immune function—three interrelated biological processes increasingly recognized as integral to the pathophysiology of endometriosis. This integrative marker therefore offers a biologically grounded, multidimensional measure that aligns with the complex systemic nature of endometriosis. However, no prior research has examined the potential link between CALLY levels and the risk of developing endometriosis. This research aimed to contribute to the early diagnosis and prevention of endometriosis by examining the potential association between the CALLY index and this condition, using data from the National Health and Nutrition Examination Survey (NHANES).
Materials and Methods
Data Sources and Study Population
This study utilized data from the NHANES database, a comprehensive, cross-sectional survey program conducted by the National Center for Health Statistics (NCHS) in 1999, offering nationally representative insights.21 To gather comprehensive health data through questionnaire interviews, physical examinations, and laboratory testing, NHANES utilizes a sophisticated multistage probability sampling approach. The survey was conducted biennially, and each participant signed an informed consent form to comply with the requirements of the Centers for Disease Control and Prevention Institutional Review Board.
For this analysis, we examined data from four successive NHANES cycles, conducted between 1999 and 2006, as endometriosis-related questionnaire responses were only available during this period. A total of 41,474 individuals participated in the survey over this timeframe. Only female participants (n=6,626) between the ages of 20 and 55 were included in the analysis. In addition, participants with missing data were excluded, including those who had, (1) missing endometriosis-related interview survey data (n=1069), (2) missing data on CBC-derived inflammatory-related indicators (n=356), and (3) missing data on important covariates (n= 594). The final analytic sample consisted of 4,602 participants after applying all exclusion criteria (Figure 1). The specific distribution of excluded participants due to missing values in covariates is also illustrated in Figure 1 to provide additional transparency regarding data completeness.
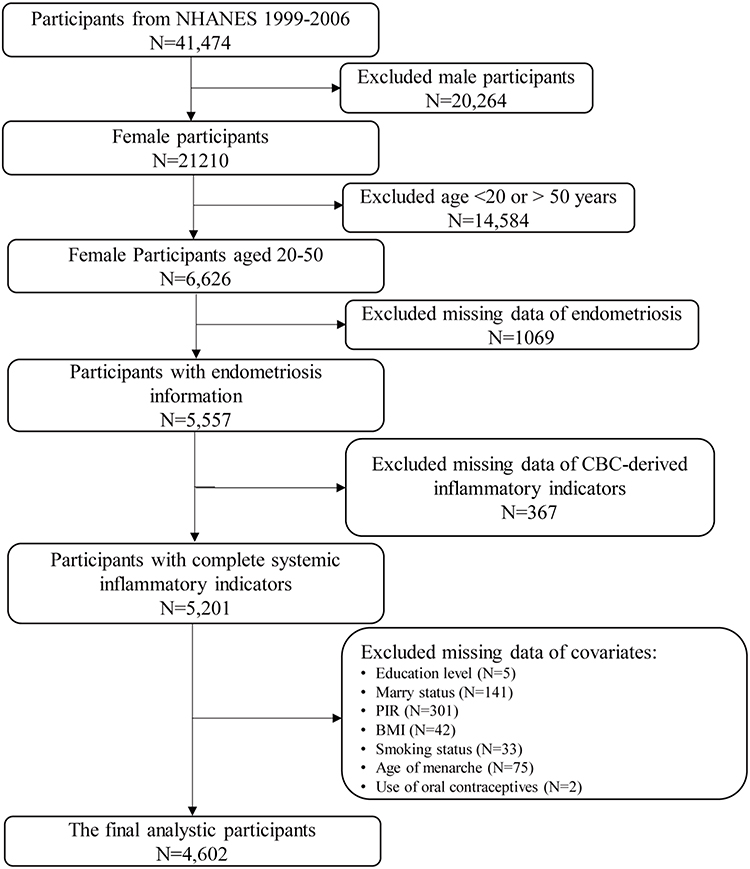 |
Figure 1 Flowchart of participant inclusion and exclusion in the current study. Abbreviations: NHANES, National Health and Nutrition Examination Surveys; CBC, complete blood count; PIR, poverty income ratio; BMI, body mass index. |
Endometriosis Definition
In this study, the identification of endometriosis was based on participants’ responses to two specific questions from the reproductive health survey: (1) RHQ360: “Have you ever been told by a healthcare professional that you have endometriosis?” and (2) RHQ370: “What was your age when you were initially diagnosed with endometriosis?”.22,23 Female participants who answered “yes” to RHQ360 or indicated their age at diagnosis in RHQ370 were classified as having endometriosis. The others were grouped as controls, indicating no diagnosis of endometriosis.
CBC-Derived Inflammation-Related Indicators Measurement
This research investigated several key biomarkers associated with immunity, nutrition, and inflammation, including leukocytes, neutrophils, lymphocytes, monocytes, platelets, albumin, and CRP. To investigate how these biomarkers relate to endometriosis, we calculated several composite indices: CALLY, SIRI, NPAR, dNLR, and PIV.24–28 The CALLY index was calculated as (albumin × lymphocyte count)/(CRP × 10), following the formula proposed by Iida et al (2022).29 In their original study, lymphocyte counts were expressed in units of cells per microliter, requiring a scaling factor of 104. In our dataset, however, lymphocyte counts are already reported in thousands per microliter (×103/μL). Therefore, we used a simpler scaling factor of 10 to ensure that the resulting index remains on a comparable scale. Complete Blood Count (CBC) was obtained using the Beckman Coulter® counting and quantification method and reported as ×103 cells/μL. Serum albumin levels were measured using the Roche Cobas 6000 chemistry analyzer with bromocresol purple reagent and presented as g/dL. Additionally, CRP levels in serum were quantified using a Behring Nephelometer with latex-enhanced nephelometry for measurement and expressed in mg/dL. Because the CALLY, SIRI, NPAR, dNLR, and PIV data had a right-skewed distribution, the data was normalized using the natural logarithmic transformation (ln).




Covariate Definition
In order to reduce the impact of possible confounding variables, this study included a range of covariates in the statistical models. These covariates included sociodemographic variables, lifestyle, and health status. Covariates specifically include age (years), race/ethnicity, marital status, education level, poverty-to-income ratio (PIR), body mass index (BMI), smoking status, age of menarche, and use of oral contraceptives. Racial and ethnic classifications included non-Hispanic White, non-Hispanic Black, Mexican American, and other races. Marital status was categorized into three distinct groups: married or living with a partner, separated/divorced/widowed, and never married. Educational level was categorized as less than high school, high school, and college or higher. Family economic status was conducted with PIR, and stratified into low (<1.3), middle (1.3–3.0), and high (>3.0) income levels. BMI classifications were classified as normal weight (< 25 kg/m2), overweight (25–30 kg/m2), and obesity (> 30 kg/m2) by clinical significance. Smoking behavior was evaluated using serum cotinine levels, with values <3.0 ng/mL indicating nonsmokers or non-current smokers, and ≥3.0 ng/mL indicating current smokers. Age at menarche, a critical marker of female reproductive health, was divided into two categories: <13 years and ≥13 years. Oral contraceptive use status was another disease-related covariate derived from the questionnaire RHQ420 and was categorized as either “ever used” or “never used.”
Statistical Analysis
In this study, secondary analyses were performed on publicly accessible data, and descriptive statistics were utilized to describe the participants’ baseline characteristics. Continuous variables are reported as the mean ± standard deviation, and categorical data are shown as frequencies and percentages. Considering the complex multistage probability sampling design of NHANES, we followed the NCHS guidelines by using weights from 4‑year fasting data (WTSAF4YR) for participants from 1999–2002 and weights from 2‑year fasting data (WTSAF2YR) for participants from 2003–2006. The relationship between CBC-derived inflammatory biomarkers and endometriosis was examined using weighted multifactorial logistic regression. To account for confounding factors, three separate logistic regression models were applied. Model I did not adjust for any covariates and analyzed only the effects of CBC-derived inflammatory-related indicators and endometriosis; Model II adjusted for sociodemographic variables (age, race/ethnicity, and education level); and Model III further adjusted for additional covariates, including PIR, marital status, BMI, smoking status, age at menarche, and oral contraceptive use status. The purpose of these models was to thoroughly account for confounding variables and provide a clearer understanding of how inflammatory markers are linked to endometriosis. To minimize the influence of extreme values, the natural logarithm of CALLY (ln CALLY) was separated into quartiles and analyzed as a categorical variable. Smooth curve fitting methods were applied to investigate the possible linear and nonlinear associations between ln CALLY levels and the presence of endometriosis. To further evaluate model performance, we calculated variance inflation factor (VIF) values for all variables included in Models 2 and 3, and additionally performed receiver operating characteristic (ROC) curve analyses to evaluate and compare the predictive performance of inflammatory indices, including CALLY, SIRI, NPAR, dNLR, and PIV, for endometriosis. A separate sensitivity analysis was conducted using random forest imputation for missing covariate data to examine the impact of missingness on the overall results.
Furthermore, subgroup analyses and interaction tests were employed to evaluate how specific population characteristics might affect the relationship between CALLY and the likelihood of developing endometriosis. The analyses were performed across categories including age (<35 years or ≥35 years), race/ethnicity (non-Hispanic White, non-Hispanic Black, Mexican American, and other races), marital status (married/living with a partner, separated/divorced/widowed, and never married), smoking status (non-smoker or non-current smoker or current smoker), age at menarche (<13 years or ≥13 years), and oral contraceptive use (ever or never).
The statistical analyses in this study were executed utilizing the R software package (http://www.r-project.org) and EmpowerStats (http://www.empowerstats.com). A two-sided p-value of less than 0.05 was considered to indicate statistical significance.
Results
Characteristics of the Participants
Following stringent exclusion criteria, this study included 4602 participants from the NHANES dataset spanning 1999 to 2006, with 338 individuals (7.34%) being diagnosed with endometriosis by their physicians (Figure 1). The sociodemographic information and laboratory data for the participants are summarized in Table 1. The cohort of endometriosis patients had an average age of 40.04 ± 8.52, significantly higher than the 35.43 ± 10.03 years observed in the non-endometriosis group (P < 0.001). BMI did not exhibit a meaningful association with endometriosis occurrence (P = 0.967). Race/ethnicity, marital status, education level, PIR, smoking status, age of menarche, and use of oral contraceptives were significantly associated with endometriosis (P < 0.05). More specifically, women with endometriosis were significantly more likely to be non-Hispanic White, have attained higher levels of education (college or higher), be married or cohabiting, have a higher PIR, not smoke, experience earlier menarche, and use oral contraceptives (p < 0.05).
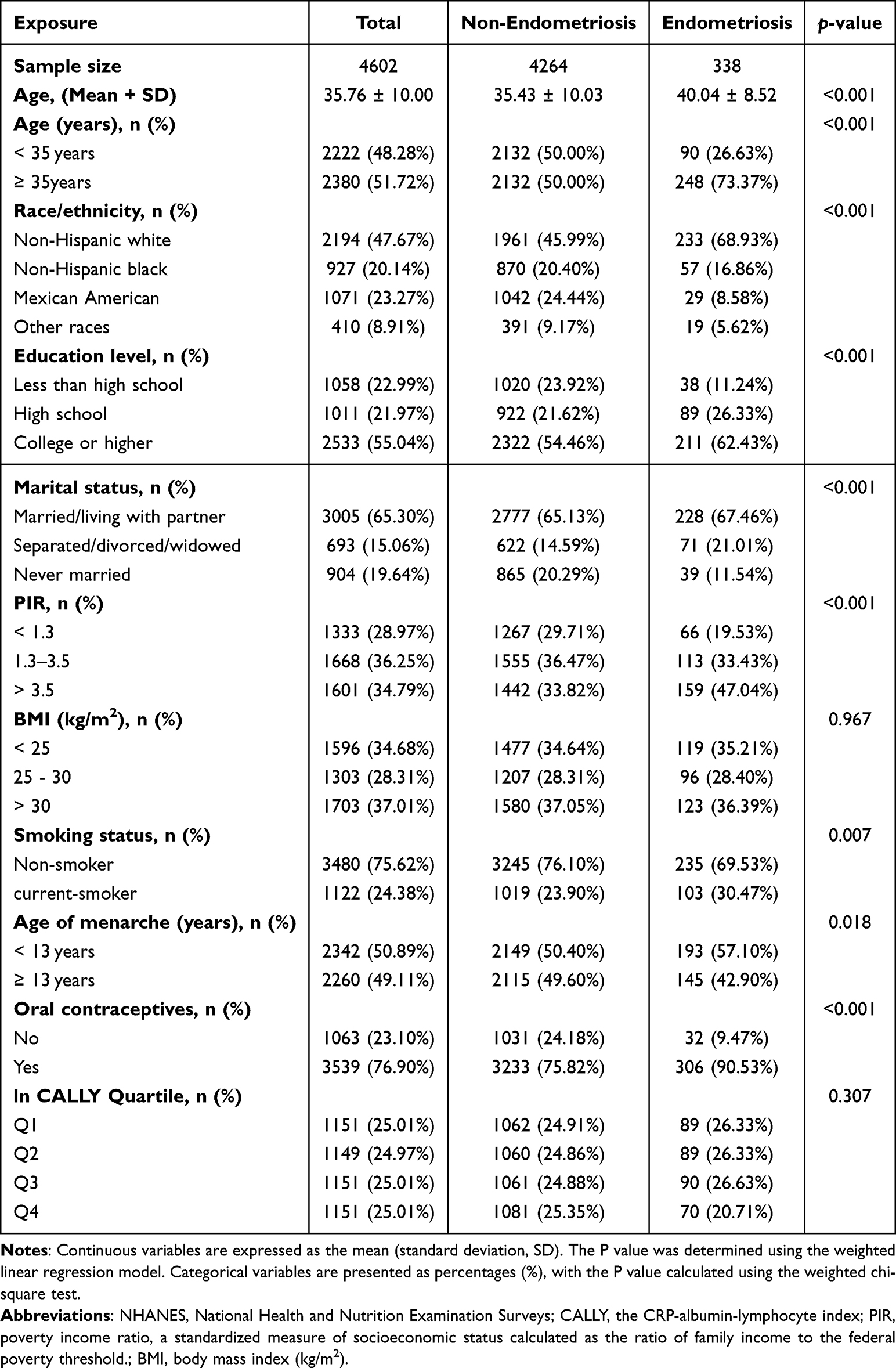 |
Table 1 Basic Characteristics of Study Participants from NHANES 1999–2006 |
Association Between CALLY and Endometriosis Prevalence
Since the distribution of these inflammation-related indicators was significantly skewed, a natural log transformation was applied prior to performing statistical analyses to ensure data normalization. Presented in Table 2, the findings from weighted multivariable logistic regression analysis explore the link between CBC-derived systemic inflammatory indicators and the prevalence of endometriosis. The results from both Model 1 (OR = 0.93, 95% CI: 0.86, 1.01) and Model 2 (OR = 0.89, 95% CI: 0.82, 0.97) revealed an inverse association, and this trend remained statistically relevant even in the fully adjusted model (OR = 0.87, 95% CI: 0.79, 0.96). This indicates that higher ln CALLY levels were associated with approximately 13% lower odds of endometriosis. Conversely, ln SIRI, ln NPAR, ln DNLR, and ln PIV did not reveal notable associations with endometriosis in the fully adjusted model.
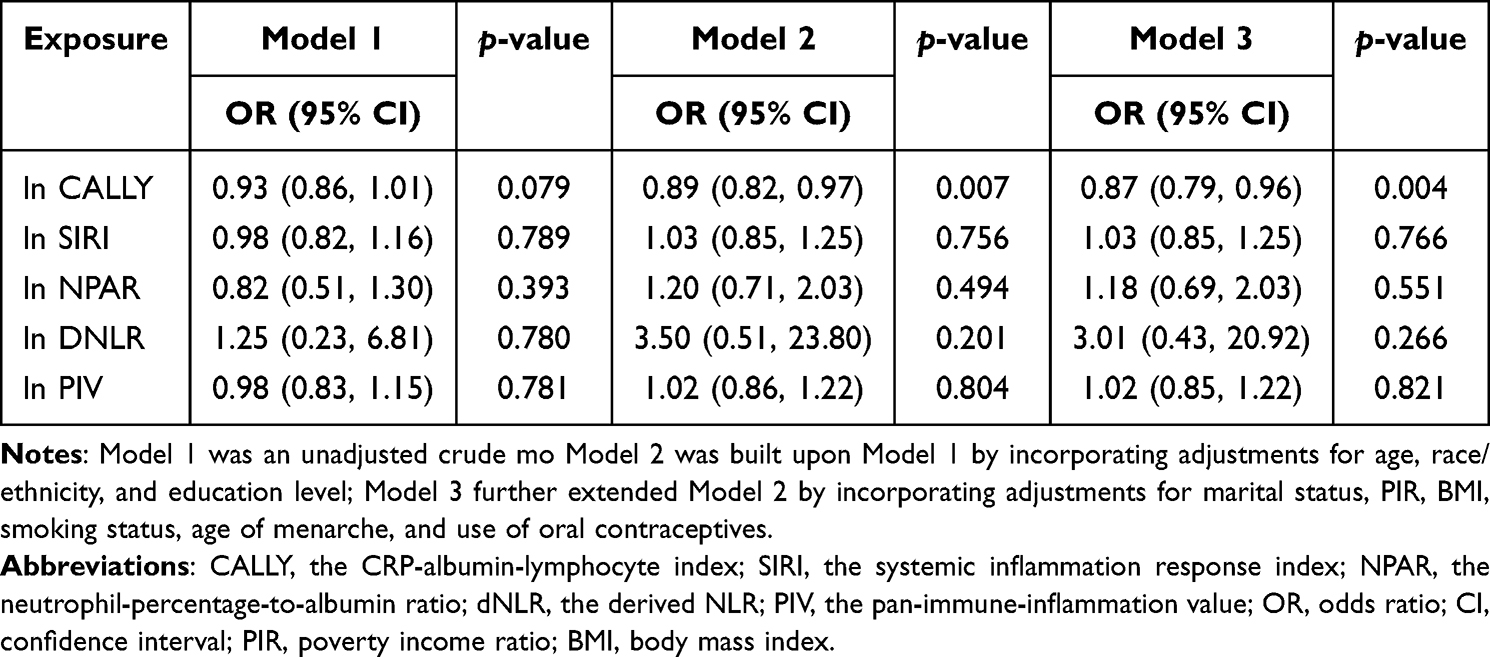 |
Table 2 Weighted Multivariate Logistic Analysis CBC-Derived Inflammatory Indicators and Endometriosis |
We divided the value of ln CALLY into quartiles. Table 3 investigates how different quartiles of ln CALLY relate to the frequency of endometriosis. After applying full adjustments in Model 3, individuals in the highest quartile of ln CALLY (Q4) demonstrated a significant link to endometriosis (OR = 0.60, 95% CI: 0.41–0.87, p = 0.008). More precisely, each additional unit of ln CALLY within the highest quartile (Q4) was associated with a 40% reduction in the likelihood of endometriosis, compared to individuals in the lowest quartile (Q1). When comparing quartile 1 with quartiles 2–4, an increasing trend in OR values was observed as ln CALLY levels rose (P for trend = 0.010). While only the highest quartile (Q4) reached statistical significance in the fully adjusted model, the significant P for trend and the gradually decreasing OR values across quartiles suggest a potential dose–response relationship between higher CALLY levels and lower endometriosis risk. To further evaluate the potential influence of missing data, a sensitivity analysis was performed using random forest imputation for covariates. After imputation, the multivariable logistic regression models were re-estimated based on the expanded sample (n = 5,201). The direction, magnitude, and statistical significance of the associations between ln CALLY and endometriosis remained essentially unchanged, supporting the robustness of our findings (Table S2). Figure 2 illustrates that smoothed curve fitting revealed a significant decrease in endometriosis risk as ln CALLY levels rose. To address concerns regarding potential multicollinearity among covariates, we assessed multicollinearity among covariates included in Models 2 and 3. All variance inflation factor (VIF) values were below 5, with mean VIFs of 1.06 and 1.22 respectively, indicating no concerning multicollinearity (Table S1).
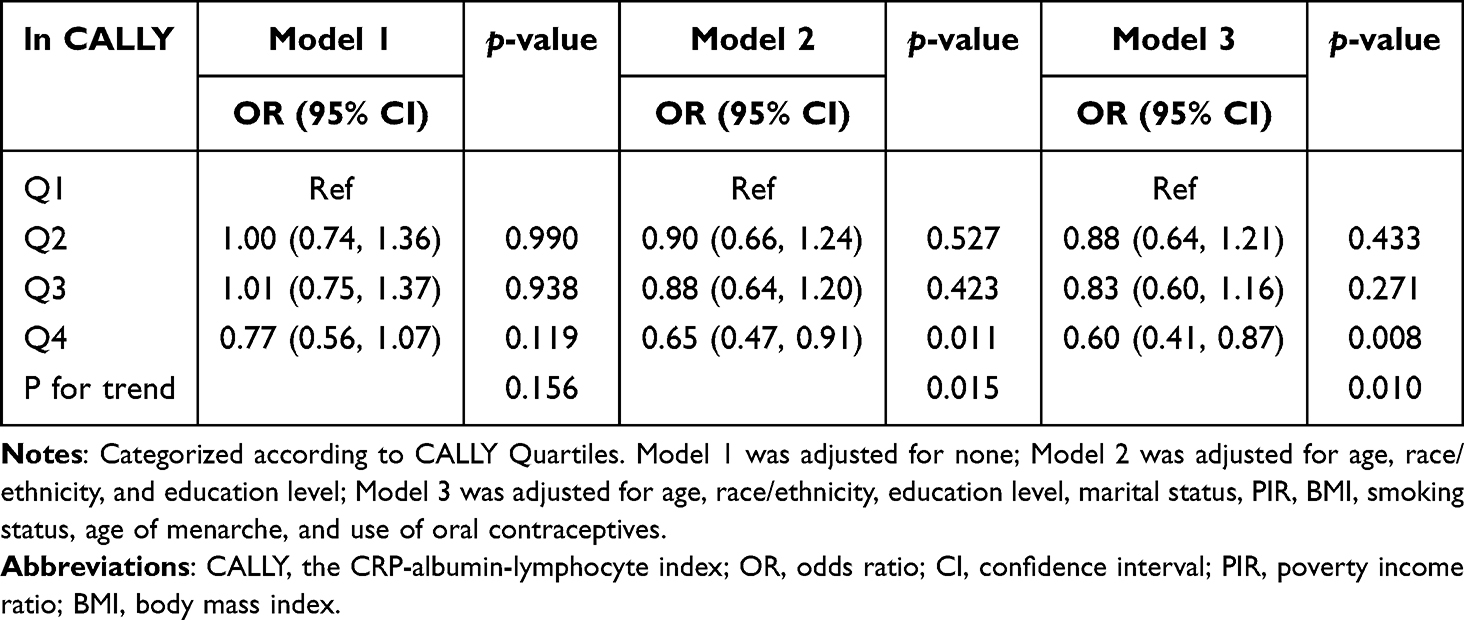 |
Table 3 Cross-Sectional Association Between Ln CALLY Index and Endometriosis |
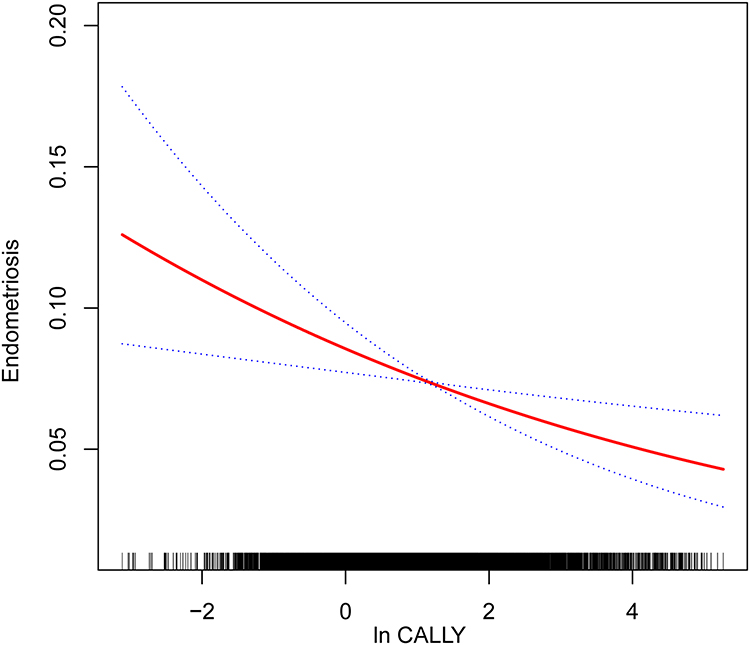 |
Figure 2 Smooth curve fitting diagram of the CALLY index and endometriosis in fully adjusted models. Abbreviations: CALLY, C-reactive protein–albumin–lymphocyte index. |
Subgroup Analysis and Interaction
Figure 3 illustrates the findings from subgroup analysis and interaction testing, revealing how ln CALLY influences endometriosis risk across varying population characteristics. Specifically, no substantial interactions were observed between ln CALLY and variables such as age (P = 0.7442), race/ethnicity (P = 0.5244), education level (P = 0.5323), marital status (P = 0.7122), PIR (P = 0.8765), BMI (P = 0.8267), smoking status (P = 0.1348), age of menarche (P = 0.6046), and use of oral contraceptives (P = 0.0978). These results suggest that the relationship between ln CALLY and endometriosis did not show statistically significant differences across different subgroups.
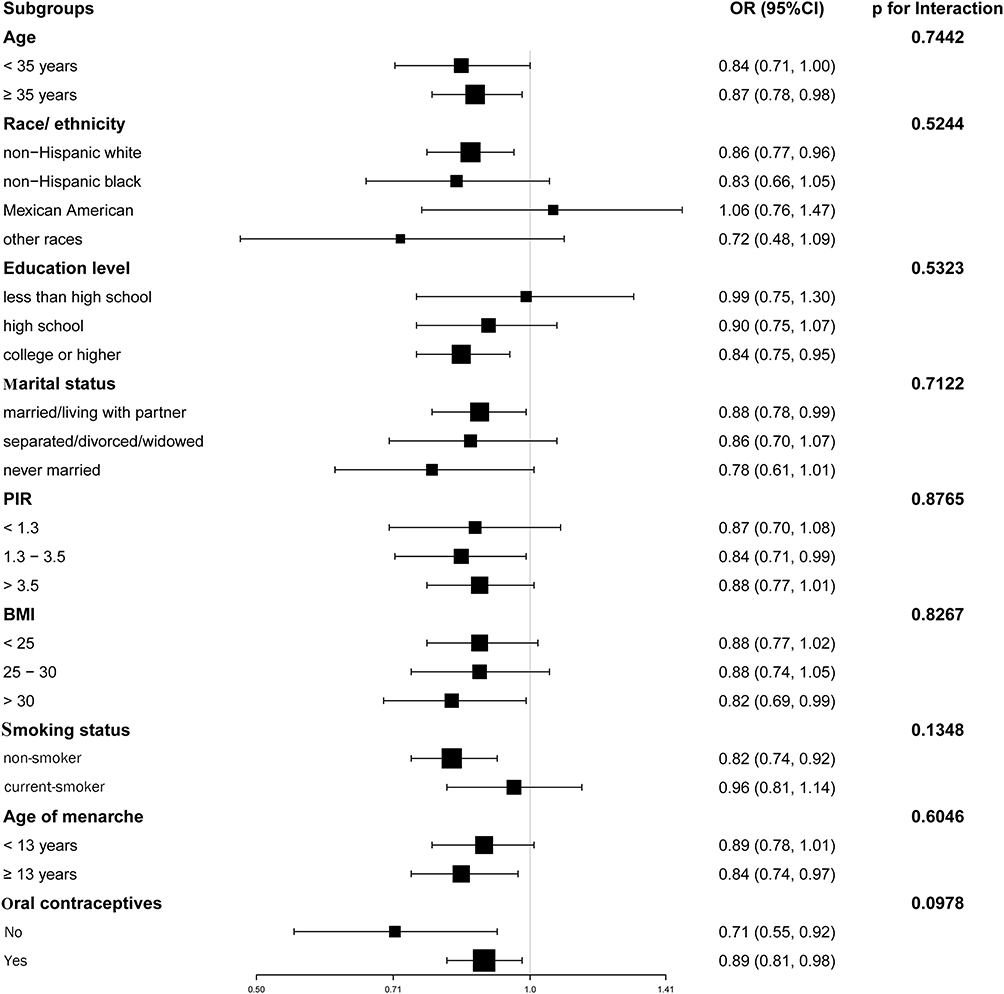 |
Figure 3 Subgroup analysis of the associations between endometriosis and ln CALLY. Abbreviations: PIR, poverty income ratio; BMI, body mass index; OR, odds ratio; CI, confidence interval. Notes: The forest plot displays odds ratios (ORs) and 95% confidence intervals (CIs) for the association between ln CALLY and endometriosis across subgroups. P for interaction values are displayed on the right to assess whether the associations significantly differ across subgroups. |
ROC Analysis
To evaluate the predictive accuracy of the CALLY index and other indices, ROC analyses were conducted across Models 1 to 3. As shown in Figure 4, the AUC of CALLY increased from 0.5247 (95% CI: 0.4939–0.5555) in Model 1 to 0.7025 (95% CI: 0.6769–0.7281) in Model 2, and 0.7219 (95% CI: 0.6970–0.7468) in Model 3, indicating improved discriminatory performance with progressively adjusted models. Similarly, other indices such as SIRI, NPAR, dNLR, and PIV also exhibited progressively higher AUCs across these models, though none surpassed CALLY in predictive ability. Full results are presented in Table 4.
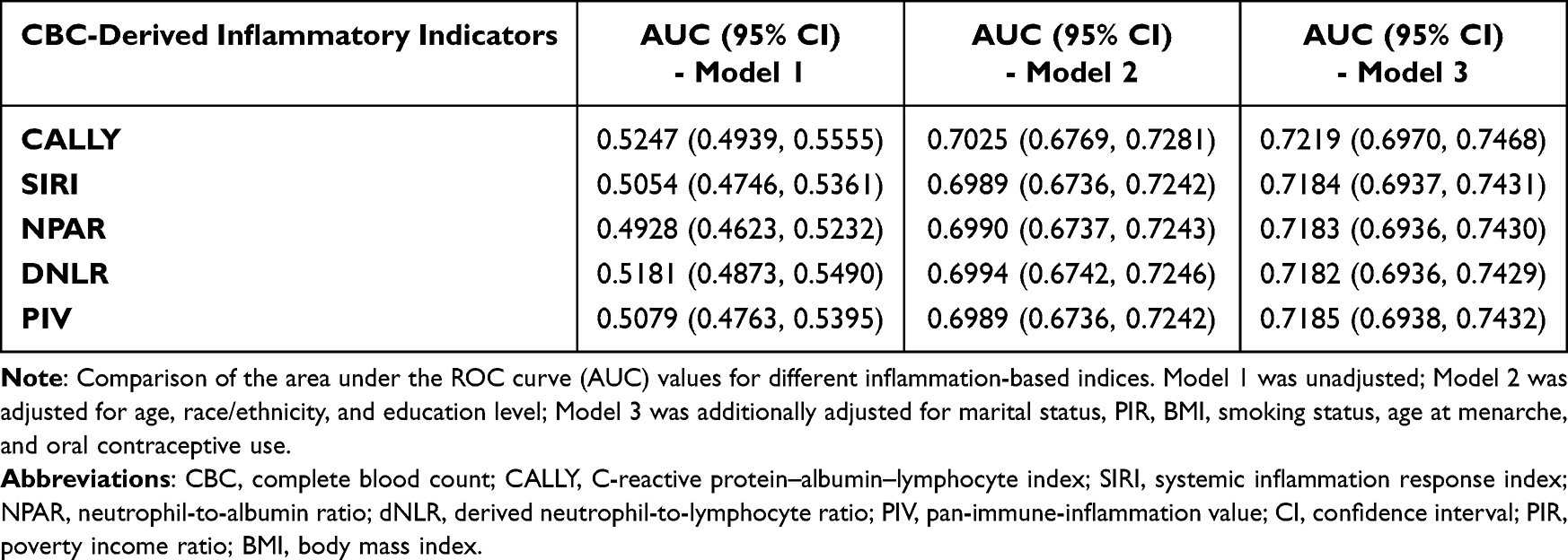 |
Table 4 Comparison of AUC Values Between CALLY and Other Inflammation Marks |
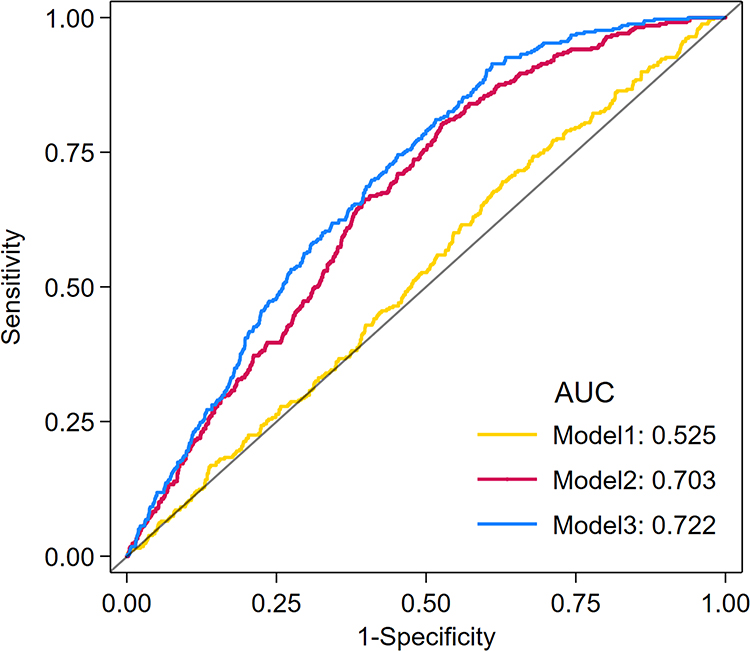 |
Figure 4 ROC curves of the CALLY index for predicting endometriosis across three logistic regression models. Abbreviations: CALLY, C-reactive protein–albumin–lymphocyte index; ROC Curve, receiver operating characteristic curve; AUC, area under the curve; PIR, poverty income ratio; BMI, body mass index. Notes: Comparison of the area under the curve (AUC) values of the CALLY index across three logistic regression models. Model 1, unadjusted model; Model 2 was built upon Model 1 by incorporating adjustments for age, race/ethnicity, and education level; Model 3 further extended Model 2 by incorporating adjustments for marital status, PIR, BMI, smoking status, age at menarche, and oral contraceptive use. |
Discussion
To our knowledge, this is the first study using nationally representative US data to investigate the association between the CALLY index and endometriosis. This research provides an in-depth analysis of the association between the CALLY index and endometriosis among adult females in the US, using NHANES data from 1999 to 2006. Among 4,602 participants, endometriosis was notably less common in those with higher CALLY levels, suggesting a clear negative association. This relationship remained robust when the index was analyzed in quartiles and was consistently observed across various subgroups in interaction analyses.
Chronic low-grade inflammation is a key contributor to the pathophysiology of endometriosis, adversely affecting ovarian and pelvic function and increasing risks of chronic pain, infertility, and malignant transformation.30,31 CRP, a nonspecific biomarker of inflammation and tissue damage with significant pro-inflammatory effects, is primarily synthesized and secreted by liver cells in response to interleukin-6 stimulation. An investigation revealed that serum hs-CRP concentrations were markedly elevated among individuals diagnosed with endometriosis when contrasted with healthy controls, further emphasizing the critical role of chronic inflammation in the pathophysiology of endometriosis.32 According to Lermann et al, although hs-CRP and CRP concentrations appeared higher among endometriosis patients relative to individuals without the condition, the observed variation was not statistically significant.33 This inconsistency may be attributed to differences in study populations, testing procedures, illness subtypes, disease stages, and/or sample sizes. Given that CRP levels can be influenced by various factors, its utility as a standalone diagnostic marker is limited. Therefore, the CALLY index was proposed to integrate CRP with other serum markers to comprehensively predict the risk of endometriosis.
Nutritional deficiency is considered a key risk factor for endometriosis progression, promoting ectopic cell proliferation, estrogen biosynthesis, angiogenesis, inflammation, and resistance to apoptosis.34 There is accumulating evidence that targeted nutritional interventions can alter various molecular processes, such as estrogen activity, prostaglandin metabolism, inflammation, and oxidative stress, which may alleviate clinical manifestations and enhance quality of life among those affected by endometriosis.35 As a principal marker of an individual’s nutritional condition, albumin is mainly produced in the liver and contributes significantly to antioxidant protection mechanisms.36 As reported by Signorile et al at the Centro Italiano Endometriosi, serum samples from 20 patients with endometriosis were analyzed using Luminex technology, revealing significantly lower albumin levels compared with healthy controls.37 A Pakistani study reported that serum albumin concentrations were marginally elevated in the control group compared to individuals with endometriosis, although this variation did not reach statistical significance.38 This study clarifies the association between the CALLY index—which integrates serum albumin—and endometriosis, highlighting albumin’s potential relevance in disease development and the need for further mechanistic research.
Extensive evidence suggests that immunological dysfunction creates a microenvironment that allows ectopic endometrial cells to evade immune surveillance, thereby promoting their proliferation, adhesion, angiogenesis, and eventual implantation.39,40 Lymphocyte subsets are essential for maintaining immune balance and clearing aberrant cells, serving as direct indicators of immune function. A study from Iran reported significantly lower lymphocyte counts in patients with endometriosis compared to those with other benign gynecological tumors.41 Similarly, Ottolina et al observed decreased lymphocyte levels in women with ovarian endometriosis, with more pronounced reductions in advanced stages.42 Another study from Türkiye found lower lymphocyte counts in endometriosis patients than in controls, although the difference was not statistically significant.43 Furthermore, the functional imbalance and interactions of lymphocyte subsets are also involved in the pathophysiology of endometriosis. Several studies have demonstrated that the Th1/Th2 balance in peripheral blood and peritoneal fluid shifts toward Th2 immunity in endometriosis patients, a disruption that can promote immune tolerance and disease progression.44,45 The regulatory T cells (Tregs), which suppress inflammation and maintain immune homeostasis, are reportedly elevated in peritoneal fluid and ectopic lesions, although their concentrations in the normal endometrium and peripheral blood remain controversial.46 Despite physiological and pathological fluctuations, lymphocyte count remains a clinically relevant marker of immune function, especially when combined with other inflammation-related indicators.47,48
Recently, growing attention has been directed toward exploring the association between CBC-derived inflammatory indicators and endometriosis, but findings remain inconsistent due to differences in populations, sample sizes, and methodologies. A retrospective study from Romania found that increased levels of neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) may correspond to both pelvic pain and advanced stages of endometriosis, while Yavuzcan et al found no significant differences in these markers, possibly reflecting regional or individual variability.49,50 A clinical study from China showed increased SII, SIRI, NLR, and PIV in endometriosis patients.12 Conversely, a cross-sectional analysis identified a positive association between SII and disease occurrence, though the relationship was influenced by demographic and reproductive factors.10 This study comprehensively analyzed the relationship between endometriosis, CALLY index, and other inflammatory markers. The results showed that the CALLY index—incorporating inflammation, nutritional status, and immune function—was independently associated with endometriosis, whereas SIRI, NPAR, dNLR, and PIV did not demonstrate significant predictive value.
Beyond the inflammatory and immune mechanisms discussed above, we also observed demographic differences in disease distribution. For instance, affected women tended to be older, possibly due to diagnostic delays or increased healthcare engagement with age.3 Earlier menarche was also more prevalent, which may reflect prolonged exposure to menstruation and retrograde flow.51 Additionally, the higher reported prevalence among non-Hispanic White women may be partially attributed to racial disparities in symptom recognition and diagnostic access.52 While not central to our analysis, these patterns underscore the importance of demographic context in interpreting disease burden.
One of the main strengths of this study lies in the use of nationally representative data from the NHANES program, enhancing the generalizability of the findings. Additionally, this study introduces the CALLY index as an innovative and minimally invasive indicator that allows for a multidimensional assessment of endometriosis prevalence. The application of weighted multivariate logistic regression models and subgroup analysis reinforced the credibility and robustness of the findings. Nonetheless, several limitations should be acknowledged. First, endometriosis diagnosis was based on self-reported data rather than clinical confirmation, which may introduce recall bias or misclassification. Second, the lack of disease staging data in NHANES limited severity-specific analyses and may have reduced the interpretability and generalizability of our findings, given the considerable biological heterogeneity of endometriosis across stages. Third, due to the cross-sectional design of this research, it cannot establish a direct cause-and-effect link between the CALLY index and endometriosis but can only illustrate their association. Given this limitation, future prospective cohort studies are warranted to validate the temporal and causal relationship between CALLY levels and the development of endometriosis. Additionally, the results of this study require additional validation in a larger and more diverse population because it relied on participants from the NHANES database from 1996 to 2006, which only represents the US population. Moreover, given the multifactorial nature of endometriosis—including retrograde menstruation, metaplasia, stem cell migration, hormonal and environmental influences—future studies should adopt multidimensional risk assessment frameworks.53 Accordingly, the CALLY index may, in future applications, be considered alongside other emerging biomarkers to support more comprehensive and integrative strategies for endometriosis risk prediction.6 Despite these limitations, this research represents a pioneering effort to elucidate how endometriosis may be linked to CALLY values, providing a practical and affordable tool for identifying high-risk populations, particularly as a cost-effective adjunct for early detection in healthcare settings with limited diagnostic resources.
Conclusion
In summary, the findings suggest that lower CALLY values tend to coincide with higher endometriosis burden, underscoring the relevance of integrating nutritional evaluation, systemic inflammation control, and immune profiling into patient management strategies. This finding emphasizes the considerable value of employing the CALLY index in clinical settings to screen for individuals with an elevated likelihood of endometriosis. However, these findings should be considered preliminary, and further validation in large-scale, prospective, and multi-center studies is essential to confirm their clinical utility and elucidate underlying mechanisms.
Data Sharing Statement
Publicly available datasets were analyzed in this study. The data can be found in: https://www.cdc.gov/nchs/nhanes/index.htm.
Ethics Approval and Consent to Participate
This study follows the guidelines of the Declaration of Helsinki. The Research Ethics Review Board of the National Center for Health Statistics granted approval for the NHANES data collection (NCHS). All participants provided written informed consent. Based on Item 1 and Item 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects, dated February 18, 2023, China, our study is exempt from additional ethical approval. The relevant legislation details are as follows: Article 32: Research involving human data or biological samples, where no harm is caused to individuals and no sensitive personal information or commercial interests are involved, may be exempt from ethical review. This is to reduce unnecessary burdens on researchers and to facilitate the progress of life science and medical research involving humans. (1) Research using publicly available data that has been legally obtained, or data generated through observation without interference with public behavior. (2) Research using anonymized data.
Acknowledgments
We extend our profound gratitude to the dedicated staff and principal investigators of the NHANES. Our deepest appreciation is reserved for the study participants whose invaluable contributions have been instrumental in advancing scientific knowledge and public health understanding.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by The National Natural Science Foundation of China (No.82471683) and The National Key R&D Program (No.2022YFC2704001).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009
2. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839–852. doi:10.1016/s0140-6736(21)00389-5
3. De Corte P, Klinghardt M, von Stockum S, Heinemann K. Time to diagnose endometriosis: current status, challenges and regional characteristics-a systematic literature review. BJOG. 2025;132(2):118–130. doi:10.1111/1471-0528.17973
4. Chen F, Zhu M, Li W. Advances in research on malignant transformation of endometriosis-associated ovarian cancer. Front Oncol. 2024;14:1475231. doi:10.3389/fonc.2024.1475231
5. Iyshwarya BK, Mohammed V, Veerabathiran R. Genetics of endometriosis and its association with ovarian cancer. Gynecol Obstetrics Clin Med. 2021;1(4):177–185. doi:10.1016/j.gocm.2021.09.001
6. Pandey S. Metabolomics for the identification of biomarkers in endometriosis. Arch Gynecol Obstet. 2024;310(6):2823–2827. doi:10.1007/s00404-024-07796-5
7. Blanco LP, Salmeri N, Temkin SM, Shanmugam VK, Stratton P. Endometriosis and autoimmunity. Autoimmun Rev. 2025;24(4):103752. doi:10.1016/j.autrev.2025.103752
8. Nishimoto-Kakiuchi A, Sato I, Nakano K, et al. A long-acting anti-IL-8 antibody improves inflammation and fibrosis in endometriosis. Sci Transl Med. 2023;15(684):eabq5858. doi:10.1126/scitranslmed.abq5858
9. Brinca AT, Peiró AM, Evangelio PM, et al. Follicular fluid and blood monitorization of infertility biomarkers in women with endometriosis. Int J Mol Sci. 2024;25(13). doi:10.3390/ijms25137177
10. Peng L, Luo X, Cao B, Wang X. Exploring the link: systemic immune-inflammation index as a marker in endometriosis-Insights from the NHANES 2001-2006 cross-sectional study. PLoS One. 2024;19(6):e0304591. doi:10.1371/journal.pone.0304591
11. Li MM, Tang XH, Wang LM. Study on the predictive significance of PLR, SII and RPR in ovarian endometriotic cyst. Zhonghua Fu Chan Ke Za Zhi. 2023;58(9):672–679. doi:10.3760/cma.j.cn112141-20230504-00200
12. Zhou Y, Liu G, Yuan L, Qiao Y, Chen Q. Evaluating systemic immune-inflammation indices as predictive markers for endometriosis diagnosis: a retrospective observational study. J Reprod Immunol. 2025;167:104416. doi:10.1016/j.jri.2024.104416
13. Huijs E, Nap A. The effects of nutrients on symptoms in women with endometriosis: a systematic review. Reprod Biomed Online. 2020;41(2):317–328. doi:10.1016/j.rbmo.2020.04.014
14. Abulughod N, Valakas S, El-Assaad F. Dietary and nutritional interventions for the management of endometriosis. Nutrients. 2024;16(23). doi:10.3390/nu16233988
15. Zhu D, Lin YD, Yao YZ, Qi XJ, Qian K, Lin LZ. Negative association of C-reactive protein-albumin-lymphocyte index (CALLY index) with all-cause and cause-specific mortality in patients with cancer: results from NHANES 1999-2018. BMC Cancer. 2024;24(1):1499. doi:10.1186/s12885-024-13261-y
16. Takeda Y, Sugano H, Okamoto A, et al. Prognostic usefulness of the C-reactive protein-albumin-lymphocyte (CALLY) index as a novel biomarker in patients undergoing colorectal cancer surgery. Asian J Surg. 2024;47(8):3492–3498. doi:10.1016/j.asjsur.2024.03.054
17. Fan X, Qing D, Zhao J, et al. The relationship between CALLY index and stroke in hypertensive patients: insights from NHANES. Front Nutr. 2025;12:1592641. doi:10.3389/fnut.2025.1592641
18. Liu Y, Wei Y. Association between the CALLY index, vitamin D, and asthma: insights from NHANES. Front Allergy. 2025;6:1557677. doi:10.3389/falgy.2025.1557677
19. Saridas A, Cetinkaya R. The prognostic value of the CALLY index in sepsis: a composite biomarker reflecting inflammation, nutrition, and immunity. Diagnostics. 2025;15(8). doi:10.3390/diagnostics15081026
20. Yang M, Lin SQ, Liu XY, et al. Association between C-reactive protein-albumin-lymphocyte (CALLY) index and overall survival in patients with colorectal cancer: from the investigation on nutrition status and clinical outcome of common cancers study. Front Immunol. 2023;14:1131496. doi:10.3389/fimmu.2023.1131496
21. National Center for Health Statistics. National Health and Nutrition Examination Survey (NHANES). Available from: https://www.cdc.gov/nchs/nhanes/index.htm.
22. Xu H, Zou H, Wen Q, Xing X, Xu N, Wu S. Association between endometriosis and arthritis: results from NHANES 1999-2006, genetic correlation analysis, and Mendelian randomization study. Front Immunol. 2024;15:1424648. doi:10.3389/fimmu.2024.1424648
23. Chen W, Xiao K, Zhou C, Cheng J, Zeng Z, Zhang F. Association of composite dietary antioxidant index and endometriosis risk in reproductive-age women: a cross-sectional study using big data-machine learning approach. Front Nutr. 2025;12:1572336. doi:10.3389/fnut.2025.1572336
24. Toda M, Musha H, Suzuki T, Nomura T, Motoi F. Impact of C-reactive protein-albumin-lymphocyte index as a prognostic marker for the patients with undergoing gastric cancer surgery. Front Nutr. 2025;12:1556062. doi:10.3389/fnut.2025.1556062
25. Briciu V, Leucuta DC, Muntean M, et al. Differences in the inflammatory response and outcome among hospitalized patients during different waves of the COVID-19 pandemic. Front Immunol. 2025;16:1545181. doi:10.3389/fimmu.2025.1545181
26. Ji Y, Xie Q, Wei W, et al. Association between blood inflammatory status and the survival of tuberculosis: a five-year cohort study. Front Immunol. 2025;16:1556857. doi:10.3389/fimmu.2025.1556857
27. Atefi A, Ghanaatpisheh A, Fereidouni M, Habibi G, Takrimi Niarad F, Aboutaleb E. Neutrophil to albumin ratio as a novel associated factor for depression; results from NHANES 2017-2018. J Affect Disord. 2025;379:72–78. doi:10.1016/j.jad.2025.02.013
28. Xu H, Cai X, Niu H, Cai X, He P, Ouyang Y. Association of PIV value with early mortality in ICU patients with sepsis-associated acute kidney injury from the MIMIC IV database. Sci Rep. 2025;15(1):11212. doi:10.1038/s41598-025-96320-z
29. Iida H, Tani M, Komeda K, et al. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB. 2022;24(1):101–115. doi:10.1016/j.hpb.2021.06.414
30. Orisaka M, Mizutani T, Miyazaki Y, et al. Chronic low-grade inflammation and ovarian dysfunction in women with polycystic ovarian syndrome, endometriosis, and aging. Front Endocrinol. 2023;14:1324429. doi:10.3389/fendo.2023.1324429
31. Park W, Lim W, Kim M, et al. Female reproductive disease, endometriosis: from inflammation to infertility. Mol Cells. 2025;48(1):100164. doi:10.1016/j.mocell.2024.100164
32. Kokot I, Piwowar A, Jędryka M, Sołkiewicz K, Kratz EM. Diagnostic significance of selected serum inflammatory markers in women with advanced endometriosis. Int J Mol Sci. 2021;22(5). doi:10.3390/ijms22052295
33. Lermann J, Mueller A, Körber F, et al. Evaluation of high-sensitivity C-reactive protein in comparison with C-reactive protein as biochemical serum markers in women with endometriosis. Fertil Steril. 2010;93(7):2125–2129. doi:10.1016/j.fertnstert.2009.01.072
34. Shimura K, Tarumi Y, Fujii M, et al. Low-nutrient environment-induced changes in inflammation, cell proliferation, and PGC-1α expression in stromal cells with ovarian endometriosis. Reprod Sci. 2023;30(4):1094–1102. doi:10.1007/s43032-022-01089-5
35. Cuffaro F, Russo E, Endometriosis AA. Pain, and related psychological disorders: unveiling the interplay among the microbiome, inflammation, and oxidative stress as a common thread. Int J Mol Sci. 2024;25(12). doi:10.3390/ijms25126473
36. Belinskaia DA, Voronina PA, Shmurak VI, et al. The universal soldier: enzymatic and non-enzymatic antioxidant functions of serum albumin. Antioxidants. 2020;9(10). doi:10.3390/antiox9100966
37. Signorile PG, Baldi A. Prototype of multiplex bead assay for quantification of three serum biomarkers for in vitro diagnosis of endometriosis. J Cell Physiol. 2016;231(12):2622–2627. doi:10.1002/jcp.25410
38. Hasan A, Rahim A, Afzal M, Naveed AK, Ayub S, Jahan S. Serum Albumin and C3 Complement Levels in Endometriosis. J Coll Physicians Surg Pak. 2019;29(8):702–705. doi:10.29271/jcpsp.2019.08.702
39. Sadłocha M, Toczek J, Major K, Staniczek J, Stojko R. Endometriosis: molecular pathophysiology and recent treatment strategies-comprehensive literature review. Pharmaceuticals. 2024;17(7). doi:10.3390/ph17070827
40. Zhang W, Li K, Jian A, Zhang G, Zhang X. Prospects for potential therapy targeting immune‑associated factors in endometriosis (Review). Mol Med Rep. 2025;31(3). doi:10.3892/mmr.2024.13422
41. Moini A, Ghanaat M, Hosseini R, Rastad H, Hosseini L. Evaluating hematological parameters in women with endometriosis. J Obstet Gynaecol. 2021;41(7):1151–1156. doi:10.1080/01443615.2020.1845634
42. Ottolina J, Bartiromo L, Dolci C, et al. Assessment of coagulation parameters in women affected by endometriosis: validation study and systematic review of the literature. Diagnostics. 2020;10(8). doi:10.3390/diagnostics10080567
43. Günday Ö K, Yılmazer M. Combined delta neutrophil index and red blood cell distribution width as a new biomarker to predict endometriosis. J Turk Ger Gynecol Assoc. 2024;25(1):30–37. doi:10.4274/jtgga.galenos.2023.2022-11-4
44. Olkowska-Truchanowicz J, Białoszewska A, Zwierzchowska A, et al. Peritoneal fluid from patients with ovarian endometriosis displays immunosuppressive potential and stimulates th2 response. Int J Mol Sci. 2021;22(15). doi:10.3390/ijms22158134
45. Lin KR, Li PX, Zhu XH, et al. Peripheral immune characteristics and subset disorder in reproductive females with endometriosis. Front Immunol. 2024;15:1431175. doi:10.3389/fimmu.2024.1431175
46. de Barros IBL, Malvezzi H, Gueuvoghlanian-Silva BY, et al. “What do we know about regulatory T cells and endometriosis? A systematic review”. J Reprod Immunol. 2017;120:48–55. doi:10.1016/j.jri.2017.04.003
47. Cristofaro MG, Ferragina F, Tolino F, Barca I. Systemic inflammatory markers as prognostic factors in oral squamous cell carcinoma of the tongue. Biomedicines. 2025;13(3). doi:10.3390/biomedicines13030754
48. Rocco A, Sgamato C, Pelizzaro F, et al. Systemic inflammatory response markers improve the discrimination for prognostic model in hepatocellular carcinoma. Hepatol Int. 2025;19:915–928. doi:10.1007/s12072-025-10806-6
49. Gorun OM, Ratiu A, Citu C, et al. The role of inflammatory markers NLR and PLR in predicting pelvic pain in endometriosis. J Clin Med. 2024;14(1). doi:10.3390/jcm14010149
50. Yavuzcan A, Cağlar M, Ustün Y, et al. Evaluation of mean platelet volume, neutrophil/lymphocyte ratio and platelet/lymphocyte ratio in advanced stage endometriosis with endometrioma. J Turk Ger Gynecol Assoc. 2013;14(4):210–215. doi:10.5152/jtgga.2013.55452
51. Ban M, Jiao J, Zhou J, Cui L, Wang H, Chen ZJ. Association of age at menarche and different causes of infertility: a retrospective study of 7634 women undergoing assisted reproductive technology. J Ovarian Res. 2025;18(1):40. doi:10.1186/s13048-025-01629-y
52. Bougie O, Nwosu I, Warshafsky C. Revisiting the impact of race/ethnicity in endometriosis. Reprod Fertil. 2022;3(2):R34–R41. doi:10.1530/RAF-21-0106
53. Awad Hegazy A. A new look at the theoretical causes of endometriosis: narrative review. Int J Reprod Biomed. 2024;22(5):343–356. doi:10.18502/ijrm.v22i5.16433
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Anorexia of Aging: Metabolic Changes and Biomarker Discovery
Picca A, Calvani R, Coelho-Júnior HJ, Landi F, Marzetti E
Clinical Interventions in Aging 2022, 17:1761-1767
Published Date: 2 December 2022
Construction and Validation of a Novel Nomogram Predicting Recurrence in Alpha-Fetoprotein-Negative Hepatocellular Carcinoma Post-Surgery Using an Innovative Liver Function-Nutrition-Inflammation-Immune (LFNII) Score: A Bicentric Investigation
Zhang BL, Liu J, Diao G, Chang J, Xue J, Huang Z, Zhao H, Yu L, Cai J
Journal of Hepatocellular Carcinoma 2024, 11:489-508
Published Date: 6 March 2024
Prognostic Value of the SII-PNI Score in Unresectable HCC Treated with Transcatheter Arterial Chemoembolization Combined with Lenvatinib and PD-1 Inhibitors
Wei SM, Zeng ZX, Pan RJ, Wu JY, Wu JY, Luo MC, Li YN, Li H, Liu DY, Ou XY, Zhang ZB, Zhou JY, Li B, Zhuang SW, Yan ML
Journal of Inflammation Research 2025, 18:7545-7557
Published Date: 10 June 2025
Association Between Remnant Cholesterol and Endometriosis Findings from NHANES 1999–2006
Su L, Wang X, Zhang J, Xu R, Ren Y, Wang S
International Journal of Women's Health 2025, 17:5709-5718
Published Date: 30 December 2025