Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Peripheral Blood NLR, PLR, and EXACT-PRO Scores in Patients with Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Prospective Observational Cohort Study
Authors Lai XM, Xie XY, Zhang JC
Received 30 October 2025
Accepted for publication 1 March 2026
Published 12 March 2026 Volume 2026:21 578000
DOI https://doi.org/10.2147/COPD.S578000
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xue-Mei Lai, Xin-Yun Xie, Jia-Chun Zhang
Department of Respiratory Medicine, Chengdu Sixth People’s Hospital, Chengdu, Sichuan Province, 610000, People’s Republic of China
Correspondence: Jia-Chun Zhang, Department of Respiratory Medicine, Chengdu Sixth People’s Hospital, No. 39 of Donghong Road, Chenghua District, Chengdu, Sichuan Province, 610000, People’s Republic of China, Tel +86 13980789271, Email [email protected]
Objective: This study examined the correlation between changes in peripheral blood neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) before and after treatment, and Exacerbations of Chronic Pulmonary Disease Tool - Patient Reported Outcome (EXACT-PRO) scores in patients with acute exacerbations of COPD (AECOPD), to assess the clinical utility of EXACT-PRO in measuring disease severity.
Methods: Hospitalized patients diagnosed with AECOPD underwent pulmonary function testing, and peripheral blood NLR and PLR levels were recorded before and after treatment. Participants completed the EXACT-PRO, COPD Assessment Test (CAT), and modified Medical Research Council (mMRC) Dyspnea Scale questionnaires. Patients with AECOPD were classified into mild, moderate, and severe groups according to the 2026 GOLD classification criteria. Baseline characteristics were compared across the three groups. Pearson’s correlation analysis was performed to evaluate the relationship between changes in NLR, PLR, and EXACT-PRO scores. ROC curves of post-treatment NLR and EXACT-PRO scores were further constructed to evaluate the discriminative performance of NLR, and a scatter plot was used to visually illustrate the correlation between the two variables.
Results: After applying the exclusion criteria to the initial cohort of 112 patients, a total of 60 patients with AECOPD were ultimately included in the analysis. According to the 2026 GOLD classification criteria, 13 patients were classified as mild, 29 as moderate, and 18 as severe. Blood samples were collected within 24 hours of hospital admission before treatment and on the day of discharge after treatment. Post-treatment NLR levels showed a statistically significant reduction compared to pre-treatment levels (p < 0.05, 95% CI: 1.12– 5.60). A positive correlation was observed between post-treatment NLR levels and EXACT-PRO scores.
Conclusion: Peripheral blood NLR levels demonstrated potential clinical relevance in patients with AECOPD and may support the development of a simple and effective quantitative tool for assessing disease severity.
Keywords: acute exacerbation of chronic obstructive pulmonary disease, EXACT-PRO score, lymphocytes, neutrophils
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic respiratory condition characterized by persistent airflow limitation, frequently accompanied by clinical manifestations such as cough, expectoration, and increased production of purulent sputum.1 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) represents a critical phase in the disease course and is recognized as a major contributor to the increased mortality rate observed in patients with COPD.2,3 Current clinical guidelines for the prevention and treatment of COPD emphasize the utility of both the COPD Assessment Test (CAT) and the modified Medical Research Council (mMRC) Dyspnea Scale in evaluating disease severity. However, these indicators are either subjective in nature or fail to reflect the dynamic inflammatory process during the acute phase in a timely manner. Therefore, identifying biomarkers that can objectively and rapidly reflect the inflammatory status and clinical severity of AECOPD is of great importance for guiding precision treatment.
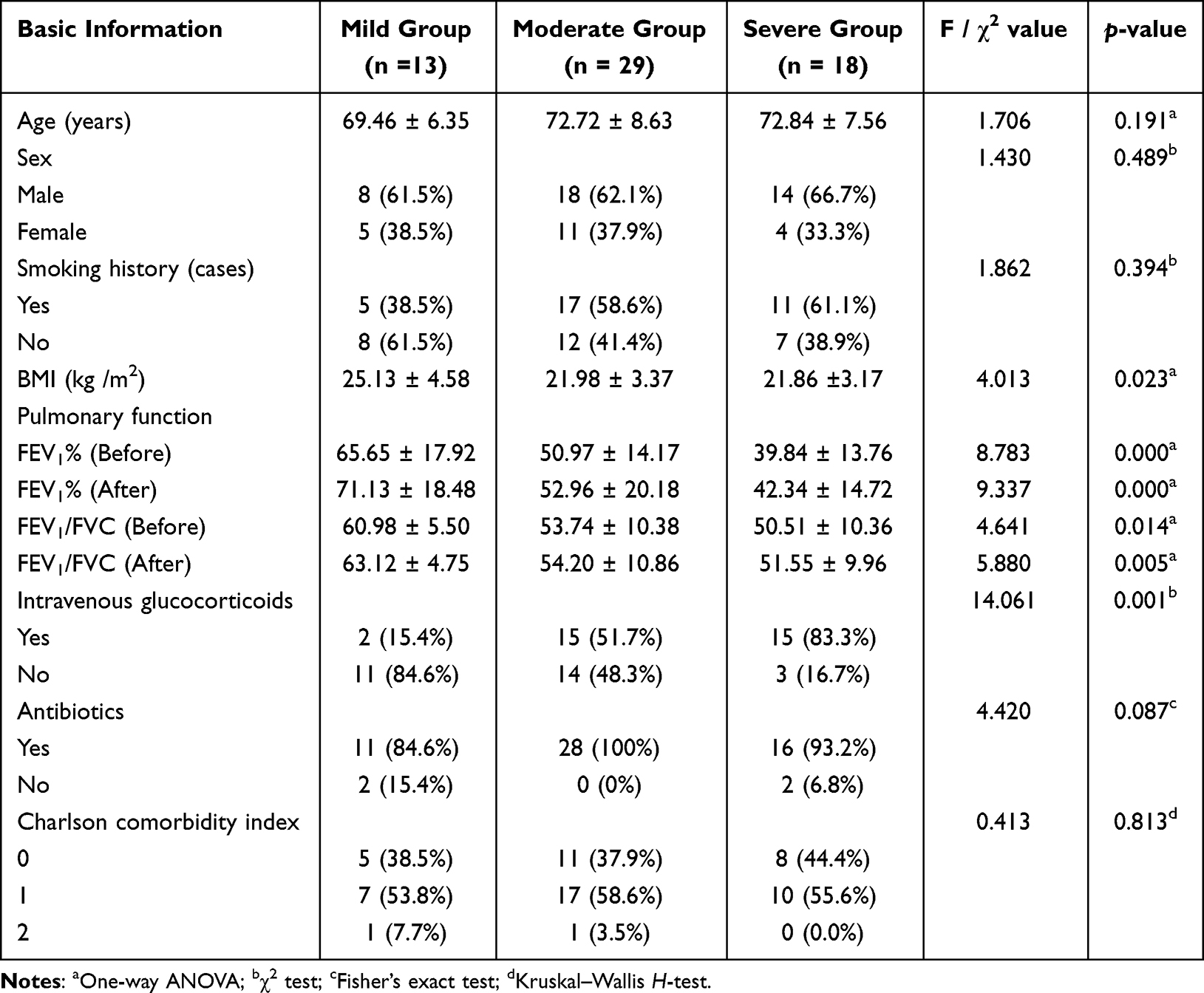 |
Table 1 Comparison of Baseline Characteristics Between Mild, Moderate and Severe AECOPD Groups (n = 60) |
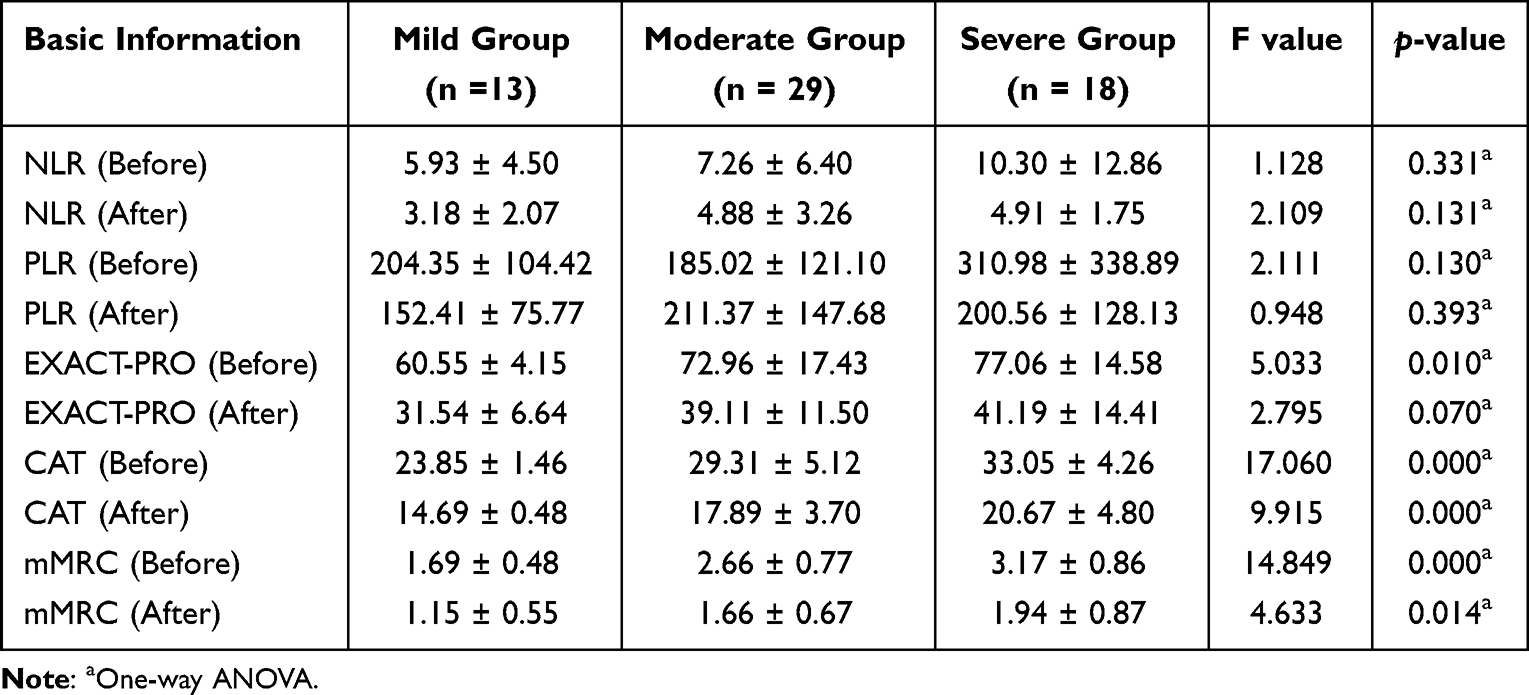 |
Table 2 The Crrelation Results Between Various Inflammatory Indicators and Scoring Scales Before and After Treatment |
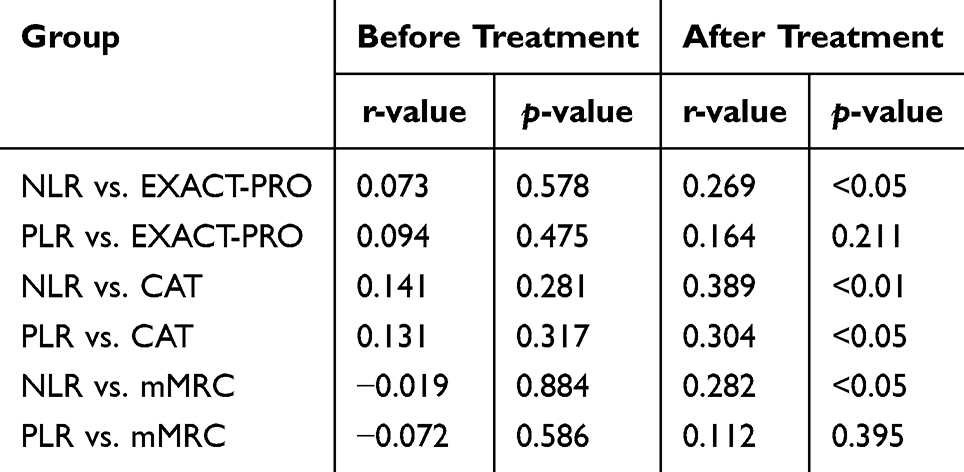 |
Table 3 Correlation Results Between Inflammatory Biomarkers and Symptom Scores Before and After Treatment |
Infiltration of inflammatory cells and the subsequent release of pro-inflammatory mediators may accelerate disease progression and adversely affect clinical outcomes. Among various biomarkers, the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) in peripheral blood have been identified as important indicators of systemic inflammation and immune response in patients experiencing AECOPD.4,5 Routine monitoring of NLR and PLR may facilitate the assessment of disease activity and guide therapeutic decision-making. In recent years, the clinical utility of these hematological parameters in the management of AECOPD has garnered increasing attention. Meanwhile, patient-reported outcome instruments designed to quantify symptom burden during acute exacerbations, such as the Exacerbations of Chronic Pulmonary Disease Tool (EXACT-PRO), are used to assess COPD severity and the risk of acute exacerbation. This tool incorporates multiple dimensions of symptomatology, including the degree of breathlessness, severity of persistent cough, and sputum characteristics, and is widely used internationally for treatment evaluation and disease monitoring.6
Most existing studies have focused on the associations between NLR/PLR and traditional indicators (eg. CAT and mMRC) or single clinical outcomes. An important knowledge gap remains: the dynamic relationship between these objective inflammatory markers and the multidimensional EXACT-PRO score has not been clearly established. In particular, there is a lack of studies in hospitalized patients with AECOPD that systematically evaluate the associations between pre- and post-treatment changes in NLR/PLR and EXACT-PRO scores. Clarifying this relationship may help integrate objective inflammatory monitoring with subjective symptom perception, providing a more comprehensive and complementary assessment framework for AECOPD and addressing the limitations of relying on a single evaluation tool.7,8
Accordingly, this study aims to fill this gap. Using a prospective observational design, the primary objective was to examine the associations between NLR/PLR and EXACT-PRO during hospitalization for AECOPD, and to further explore the predictive value of NLR/PLR for symptom improvement. The findings provide new evidence to support the integration of biological markers with patient-reported outcomes to optimize the clinical assessment and management of AECOPD.
Materials and Methods
Clinical Data
Case Source and Data Collection
This study was a single-center, prospective observational study. Participants were enrolled using a consecutive sampling approach and included patients hospitalized in the Department of Respiratory Medicine at Chengdu Sixth People’s Hospital (Donghong Branch) between June 20, 2023, and December 31, 2024, with a confirmed diagnosis of AECOPD. Demographic characteristics, clinical assessments, and treatment-related data were systematically collected for all patients who met the inclusion criteria.
Data Collection
Data were collected at two time points. Pre-treatment data were obtained after hospital admission and before the initiation of any AECOPD-specific therapy. Post-treatment data were collected on the day of discharge. Blood samples were analyzed within 1 hour of collection. Complete blood counts were measured using a BC-5390 CRP automated hematology analyzer, and arterial blood gas analysis was performed with a RADIOMETER ABL9 analyzer. All samples were confirmed to be free of hemolysis. Absolute neutrophil counts, absolute lymphocyte counts, and platelet counts were recorded, and the following indices were calculated: NLR = absolute neutrophil count ÷ absolute lymphocyte count; PLR = platelet count ÷ absolute lymphocyte count. Comorbid chronic conditions were systematically assessed and quantified using the Charlson Comorbidity Index.
Diagnostic Criteria
COPD diagnosis was based on the 2026 Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines. A post-bronchodilator ratio of forced expiratory volume in one second to forced vital capacity ratio (FEV1/FVC) of less than 0.7 on spirometry was considered indicative of incompletely reversible airflow limitation, consistent with a COPD diagnosis.9 The final diagnosis was established by integrating spirometric findings with the patient’s clinical presentation, following the exclusion of alternative respiratory conditions.
Inclusion and Exclusion Criteria
Inclusion criteria
Patients were eligible for inclusion if they met the following conditions:10 ① Fulfilled the diagnostic criteria for AECOPD as defined by the 2023 Global Initiative for Chronic Obstructive Lung Disease (GOLD), characterized by a worsening of respiratory symptoms (such as dyspnea, cough, and/or sputum production) beyond normal day-to-day variation; ② Age ≥ 40 years; ③ Hospitalization duration exceeding 24 hours; ④ Able to read, write, and communicate effectively, and capable of completing questionnaires such as the EXACT-PRO independently or with the assistance of the researchers; ⑤ Voluntary participation with signed informed consent.
Exclusion criteria
Patients were excluded under the following conditions: ① Presence of severe comorbidities, including immunodeficiency, hematologic disorders, or malignancies; ② Severe hepatic or renal dysfunction, or clinically significant cardiovascular or cerebrovascular diseases; ③ History of psychiatric illness, cognitive impairment, or inability to communicate verbally and complete questionnaires independently; ④ received systemic corticosteroids or other medications that could significantly affect white blood cell counts within 48 hours prior to baseline blood sample collection; ⑤ Discontinuation of treatment or voluntary request for discharge; ⑥ Transfer to other medical specialties or referral to external institutions.
Patient Grouping
Based on spirometric findings, patients diagnosed with AECOPD were classified into mild, moderate, and severe groups according to the 2026 GOLD classification criteria.9 Mild: Dyspnea VAS <5, respiratory rate <24/min, heart rate <95 bpm, resting SpO2 ≥92% with ≤3% variation, and CRP <10 mg/L (if measured); Moderate: Dyspnea VAS ≥5, respiratory rate ≥24/min, heart rate ≥95 bpm, resting SpO2 <92% or >3% variation, and CRP ≥10 mg/L; arterial blood gas may show PaO2 70–80 mmHg. Severe: Meets moderate criteria, with arterial blood gas showing PaO2 ≤60 mmHg and/or PaCO2 >45 mmHg with pH <7.35. Clinical symptoms and signs were subsequently recorded and compared across the different severity groups.
EXACT-PRO, CAT, and mMRC Questionnaire Assessment
Data collection was conducted through structured questionnaires administered by clinicians and nursing staff. All patients diagnosed with AECOPD completed the EXACT-PRO, the CAT, and the mMRC Dyspnea Scale.
The EXACT-PRO is a standardized patient-reported outcome measure designed to evaluate the frequency, severity, and duration of acute exacerbations in patients with COPD. It comprises 14 items, each scored on a scale from 0 to 5, yielding a total possible score ranging from 0 to 100. Higher scores indicate greater symptom burden. The questionnaire evaluates domains including cough and sputum (frequency of cough, volume and viscosity of sputum, difficulty with expectoration), chest symptoms (chest tightness, discomfort, and oppression), dyspnea (shortness of breath, degree of shortness of breath, shortness of breath during personal care, and indoor and outdoor activities), fatigue or weakness, panic or anxiety, and sleep disturbances. Respondents were instructed to complete the questionnaire nightly before sleep.11
The CAT is an 8-item instrument used to assess the overall health status of patients with COPD. It evaluates symptoms such as dyspnea, cough, sputum production, chest tightness, activity limitation, sleep quality, energy levels, and psychological well-being. The total score ranges from 0 to 40, with disease severity classified as follows: mild (0–10), moderate (11–20), severe (21–30), and very severe (31–40). Respiratory dysfunction remains one of the most prevalent clinical manifestations among patients with COPD. Pulmonary function testing serves as the diagnostic gold standard for evaluating respiratory impairment and is critical in assessing respiratory diseases.12
The mMRC dyspnea scale is primarily utilized to grade the severity of breathlessness. It consists of five levels, scored from 0 to 4, with higher scores indicating severe dyspnea.7
Statistical Analysis
All statistical analyses were performed using SPSS software version 26.0. and GraphPad Prism version 10. Continuous variables were presented as mean ± standard deviation ( ). Paired sample t-tests were used to compare pre- and post-treatment values within the same group. One-way ANOVA was used to compare mean values between the mild, moderate and severe AECOPD groups. Categorical variables were expressed as frequencies and percentages, and comparisons were conducted using the chi-square (χ2) test and Fisher’s exact test. Pearson’s correlation analysis was performed to evaluate the association between quantitative variables. Categorical variables were analyzed using the Kruskal–Wallis H-test. A p-value of less than 0.05 was considered to indicate statistical significance.
). Paired sample t-tests were used to compare pre- and post-treatment values within the same group. One-way ANOVA was used to compare mean values between the mild, moderate and severe AECOPD groups. Categorical variables were expressed as frequencies and percentages, and comparisons were conducted using the chi-square (χ2) test and Fisher’s exact test. Pearson’s correlation analysis was performed to evaluate the association between quantitative variables. Categorical variables were analyzed using the Kruskal–Wallis H-test. A p-value of less than 0.05 was considered to indicate statistical significance.
Results
Basic Patient Characteristics
After applying exclusion criteria to the initial 112 patients (lung cancer, n = 15; coronary heart disease, n = 10; renal insufficiency, n = 10; department transfer, n = 5; hospital transfer, n = 2; voluntary withdrawal, n = 10), a total of 60 patients were finally enrolled, including 40 males (66.7%) and 20 females (33.3%), all diagnosed with AECOPD. Among them, 13 patients were classified into the mild group, 29 patients were classified into the moderate group and 18 patients into the severe group based on pulmonary function test results (Figure 1).
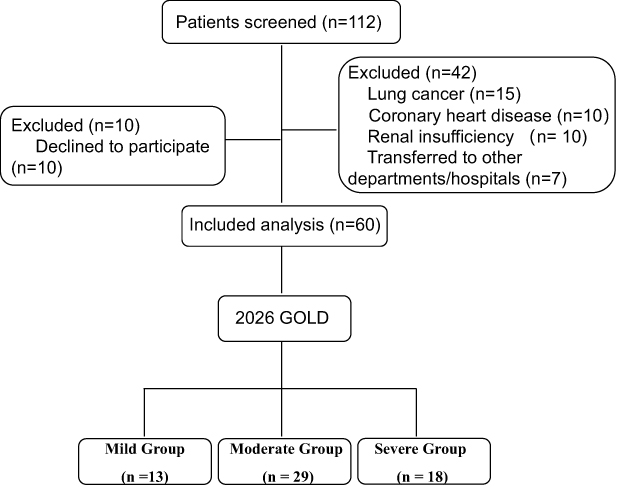 |
Figure 1 Study flowchart. |
No statistically significant differences were observed between the three groups with respect to age, sex distribution, smoking history, body mass index (BMI), use of antibiotics, or combined complications situation (p > 0.05). However, pulmonary function parameters, including FEV1% Pred and FEV1/FVC (Before and After), administration of intravenous glucocorticoids were significantly lower in the severe group compared to the mild and moderate group (p < 0.001). Detailed baseline characteristics are presented in Table 1.
Baseline and statistical analyses were performed for NLR, PLR, EXACT-PRO, CAT, and mMRC scores before and after treatment across the three patient groups. No significant differences were observed in pre- and post-treatment NLR or PLR among the groups (p > 0.05). However, the severity of AECOPD was associated with significant differences in baseline EXACT-PRO, CAT, and mMRC scores (p < 0.05). Post-hoc multiple comparisons for EXACT-PRO revealed significant differences between mild and severe patients (mild vs. severe: p = 0.043, 95% CI: −24.53 to −0.30) and between moderate and severe patients (moderate vs. severe: p = 0.009, 95% CI: −29.71 to −3.31), while no significant difference was observed between mild and moderate patients (Table 2).
Peripheral Blood NLR and PLR Levels Before and After Treatment
As illustrated in Figure 2, peripheral blood NLR levels in patients with AECOPD demonstrated a statistically significant reduction following treatment when compared to pre-treatment values (p<0.05, 95% CI: 1.12–5.60). In contrast, no statistically significant change was observed in PLR levels before and after treatment.
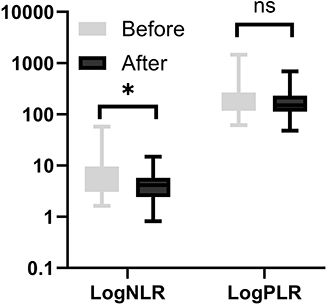 |
Figure 2 Blood NLR and PLR levels in AECOPD patients before and after treatment. *p < 0.05 vs. pre-treatment; ns, p > 0.05. |
EXACT-PRO, CAT, and mMRC Scores Before and After Treatment
As shown in Figure 3, scores from the EXACT-PRO, the CAT, and the mMRC Dyspnea Scale significantly decreased after treatment in the AECOPD cohort (p < 0.001), indicating symptomatic improvement.
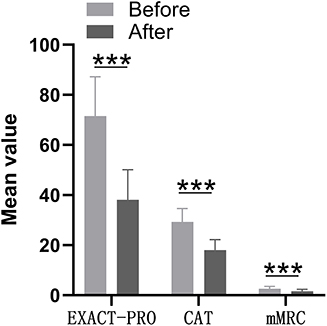 |
Figure 3 EXACT-PRO, CAT, and mMRC scores in AECOPD patients before and after treatment. ***p < 0.001 vs. pre-treatment. |
Correlation Between Inflammatory Biomarkers and Symptom Scores
Correlation analysis indicated that, prior to treatment, neither NLR nor PLR showed a statistically significant association with EXACT-PRO, CAT, or mMRC scores. However, post-treatment measurements revealed a statistically significant positive correlation between NLR and the EXACT-PRO, CAT, and mMRC scores. PLR demonstrated a positive correlation only with the CAT scores after treatment. Detailed correlation coefficients are presented in Table 3. Next, the correlation between pre-treatment NLR and EXACT-PRO scores was visualized (Figure 4), which showed a significant positive association (r = 0.269, p < 0.05, 95% CI: 0.038–0.487). EXACT-PRO scores ≥50 were categorized as severe and <50 as non-severe.13 ROC analysis indicated that post-treatment NLR predicted severity with an area under the curve of 0.732. The optimal NLR cutoff was 5.39, corresponding to a sensitivity of 63.6% and specificity of 77.6% (Figure 5).
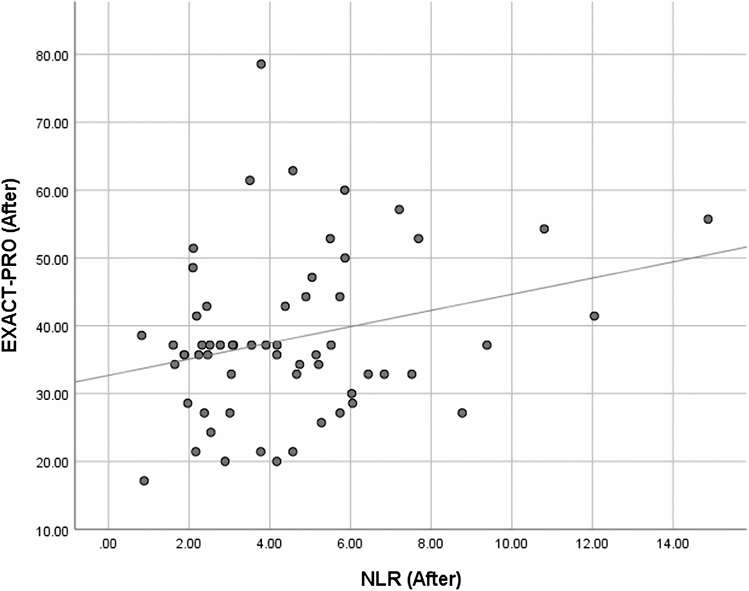 |
Figure 4 Correlation between post-treatment NLR and EXACT-PRO scores in AECOPD patients. |
 |
Figure 5 ROC curve of post-treatment NLR for predicting EXACT-PRO severity in AECOPD patients. |
Discussion
This study explored the association between systemic inflammatory markers (NLR and PLR) and patient-reported outcomes (EXACT-PRO, CAT, and mMRC) in the assessment of AECOPD severity. Our key findings are as follows. First, baseline symptom scores (EXACT-PRO, CAT, and mMRC) effectively discriminated between GOLD-defined AECOPD severity groups, highlighting their clinical value as initial screening tools for disease severity. Second, post-treatment NLR levels decreased significantly compared with baseline, whereas changes in PLR were not statistically significant, suggesting that NLR may be more sensitive to the resolution of acute systemic inflammation. Third, post-treatment NLR showed positive correlations with all three symptom scores, while no such associations were observed before treatment. ROC analysis further indicated that post-treatment NLR, with a cutoff value of 5.39, demonstrated moderate predictive value for identifying a high symptom burden (EXACT-PRO ≥ 50), with an AUC of 0.732. Notably, the significant association between inflammatory markers, particularly NLR, and symptom scores was observed only after treatment, but not at baseline. This phenomenon may be explained by the complex pathophysiological state during the acute phase of AECOPD. Before treatment, patients are exposed to intense systemic stress and high inflammatory burden, while symptom severity is simultaneously influenced by multiple factors, including airway obstruction, infection, respiratory muscle fatigue, and psychological distress. In this context, inflammation represents only one of several drivers of symptoms, which may obscure its direct association with symptom scores. Following treatment with systemic corticosteroids and bronchodilators, rapid alleviation of airway spasm and systemic inflammation may reduce this multifactorial interference, allowing the relationship between residual inflammation and symptom burden to become more evident. This finding is partially consistent with a report demonstrating that once inflammation is initially controlled, residual inflammatory levels are more closely associated with patients’ functional status.14
Our findings both align with and diverge from previous studies. Numerous investigations have confirmed the value of NLR and PLR as markers of inflammation and prognosis in patients with AECOPD,15–17 and the significant post-treatment reduction in NLR observed in our study supports this evidence. However, the reported associations between these inflammatory markers and patient-reported outcomes remain inconsistent across the literature. For example, some studies have identified a relationship between baseline NLR and CAT scores, whereas no such association was observed at baseline in our cohort. These discrepancies may be attributable to heterogeneity in study populations (eg., differences in severity distribution and comorbidity profiles), variations in the timing and intensity of therapeutic interventions, and the use of different symptom assessment instruments. Notably, this study employed the EXACT-PRO, a tool specifically designed to capture symptom burden during acute exacerbations, which may assess symptom dimensions distinct from those measured by more general instruments such as the CAT. Post hoc analyses indicated that EXACT-PRO demonstrated greater discriminatory ability between mild and severe AECOPD compared with other symptom scores, further supporting its potential advantage in acute-phase assessment. Although observational in design, our findings suggest a potential clinical application for NLR. As an easily accessible and objective biomarker, post-treatment NLR, with a reference cutoff of 5.39, may assist clinicians in identifying an “inflammatory phenotype” of patients who continue to experience a high symptom burden despite standard therapy. For such patients, clinical decision-making may involve more detailed inflammatory assessments (eg., CRP or cytokine profiling) or cautious adjustment of anti-inflammatory strategies, such as the duration or intensity of systemic corticosteroid treatment, to facilitate more precise, individualized management. These results provide preliminary support for future exploration of dynamic treatment models guided by both symptom burden and inflammatory status.
This study has several limitations that should be acknowledged. First, the overall sample size was relatively small, and the unequal distribution of patients across severity subgroups may have reduced statistical power and the robustness of subgroup analyses. Second, as a single-center observational study, there was heterogeneity in treatment regimens, particularly regarding the timing and dosage of systemic corticosteroid use. Although efforts were made to account for these factors in the analysis, residual confounding cannot be fully excluded. Third, data were collected at only two clinically practical time points (at hospital admission and at discharge), which limited our ability to capture the dynamic trajectories of inflammatory markers and symptom burden throughout the treatment course. Fourth, the dichotomization of symptom severity using an EXACT-PRO cutoff of ≥50, while based on the observed data distribution, requires validation in larger cohorts to determine its optimal clinical threshold.
Conclusion
This prospective study demonstrates that, following standardized treatment for AECOPD, a reduction in the peripheral blood NLR occurs in parallel with improvements in patient-reported symptoms, as reflected by decreases in EXACT-PRO, CAT, and mMRC scores. Moreover, post-treatment NLR levels were positively correlated with symptom scores, suggesting that dynamic monitoring of NLR may serve as a potential objective adjunct for evaluating treatment response and residual symptom burden in patients with AECOPD. Notably, no significant association was observed between baseline NLR and symptom scores, and the PLR showed no consistent correlation with symptom measures throughout the observation period. These findings indicate that the strength of the relationship between inflammatory biomarkers and clinical symptoms may vary according to both the treatment phase and the type of biomarker, and therefore should not be generalized indiscriminately. However, given the single-center observational design, limited sample size, and incomplete control of treatment-related heterogeneity, NLR cannot yet be regarded as an independent basis for clinical decision-making, and its association with symptom burden should be interpreted with caution. To further validate the clinical utility of NLR, future large-scale, multicenter prospective cohort studies are warranted, with standardized timing of biomarker and symptom assessments and systematic adjustment for key confounders such as systemic corticosteroid use. Ultimately, interventional studies are needed to determine whether management strategies guided by a dual “inflammation–symptom” framework can meaningfully improve patient outcomes, thereby opening new avenues for precision medicine in AECOPD.
Abbreviations
AECOPD, Acute exacerbation of chronic obstructive pulmonary disease; EXACT-PRO, Exacerbations of Chronic Pulmonary Disease Tool - Patient Reported Outcome; COPD, chronic obstructive pulmonary disease; NLR, neutrophil/lymphocyte ratio; PLR, platelet / lymphocyte ratio; CAT, COPD assessment test; mMRC, modified Medical Research Council; GOLD, Global Initiative for Chronic Obstructive Lung Disease; FEV1/FVC, Forced expiratory volume in one second/forced vital capacity; FEV1, Forced expiratory volume in one second; FVC, forced vital capacity; FEV1% Pred, forced expiratory volume in one second predicted value ratio; BMI, Body Mass Index.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Chengdu Sixth People’s Hospital (No. 2024-009). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff who implemented the intervention and evaluation components of the study.
Funding
2022 Sichuan Youth Innovation Research Project (N0.Q22089).
Disclosure
The authors declare that they have no competing interests.
References
1. Celli BR, Fabbri LM, Aaron SD, et al. Differential diagnosis of suspected chronic obstructive pulmonary disease exacerbations in the acute care setting: best practice. Am J Respir Crit Care Med. 2023;207(9):1134–10. PMID: 36701677; PMCID: PMC10161746. doi:10.1164/rccm.202209-1795CI
2. Albert RK, Connett J, Bailey WC, et al; COPD Clinical Research Network. Azithromycin for prevention of exacerbations of COPD. N Engl J Med. 2011; 365(8):689–698. Erratum in: N Engl J Med. 2012 Apr 5;366(14):1356. PMID: 21864166; PMCID: PMC3220999. doi:10.1056/NEJMoa1104623
3. Su YC, Jalalvand F, Thegerström J, Riesbeck K. The interplay between immune response and bacterial infection in copd: focus upon non-typeable Haemophilus influenzae. Front Immunol. 2018;9:2530. PMID: 30455693; PMCID: PMC6230626. doi:10.3389/fimmu.2018.02530
4. Liao QQ, Mo YJ, Zhu KW, et al. Platelet-to-Lymphocyte Ratio (PLR), Neutrophil-to-Lymphocyte Ratio (NLR), Monocyte-to-Lymphocyte Ratio (MLR), and Eosinophil-to-Lymphocyte Ratio (ELR) as biomarkers in patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2024;19:501–518. PMID: 38414718; PMCID: PMC10898603. doi:10.2147/COPD.S447519
5. Li J, Zhou Y, Xu QX, Pang YY, Li XQ. The changing characteristics of inflammatory indicators in patients with pulmonary thromboembolism. Chin J General Pract. 2019;17(5):733–737. doi:10.16766/j.cnki.issn.1674-4152.000778
6. Wang MH, Bi LC, Yin LY, Li SY, Li JS. Application of early identification tools for acute exacerbation of chronic obstructive pulmonary disease; 2021. doi:10.3969/j.issn.1005-9202.2021.10.056
7. Wang LM, Ji S, Fei GH. The clinical significance of the study on the correlation between blood ACE2 levels and NLR changes in AECOPD patients and CAT. Acta Universitatis Medicinalis Anhui. 2019;8:5. doi:10.19405/j.cnki.issn1000-1492.2019.08.028
8. Yang PP, Xu K, Li X. The value of EXACT-PRO in assessing the severity of COPD and the risk of acute exacerbation in patients. Chongqing Medicine. 2021;50(12):6. doi:10.3969/j.issn.1671-8348.2021.12.008
9. Venkatesan P. GOLD COPD report: 2023 update. Lancet Respir Med. 2023;11(1):18. Epub 2022 Nov 30. PMID: 36462509. doi:10.1016/S2213-2600(22)00494-5
10. Xie DB, Kong XQ, Zeng Q. Analysis of the distribution characteristics and drug resistance of pathogenic bacteria in sputum of 120 middle-aged and elderly patients with acute exacerbation of chronic obstructive pulmonary disease in a certain hospital. Anti-Infect Pharm. 2020;17(10):4. doi:10.13493/j.issn.1672-7878.2020.10-014
11. Jones PW, Chen WH, Wilcox TK, Sethi S, Leidy NK; EXACT-PRO Study Group. Characterizing and quantifying the symptomatic features of COPD exacerbations. Chest. 2011;139(6):1388–1394. Epub 2010 Nov 11. PMID: 21071529. doi:10.1378/chest.10-1240
12. Kim S, Oh J, Kim YI, et al. Differences in classification of COPD group using COPD assessment test (CAT) or modified Medical Research Council (mMRC) dyspnea scores: a cross-sectional analyses. BMC Pulm Med. 2013;13:35. PMID: 23731868; PMCID: PMC3680333. doi:10.1186/1471-2466-13-35
13. Nishimura K, Nakamura S, Kusunose M, et al. Comparison of patient-reported outcomes during acute exacerbations of chronic obstructive pulmonary disease. BMJ Open Respir Res. 2018;5(1):e000305. doi:10.1136/bmjresp-2018-000305
14. Kohli P, Pinto-Plata V, Divo M, et al. Functional capacity, health status, and inflammatory biomarker profile in a cohort of patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil Prev. 2015;35(5):348–355. doi:10.1097/HCR.0000000000000123
15. Luo Z, Zhang W, Chen L, Xu N. Prognostic value of neutrophil:lymphocyte and platelet:lymphocyte ratios for 28-day mortality of patients with AECOPD. Int J Gen Med. 2021;14:2839–2848. doi:10.2147/IJGM.S312045
16. Fu Y, Wang Y, Wang Y, et al. Biomarkers (NLR, PLR, SII) for Frequent COPD exacerbations: diagnostic and clinical management implications in a retrospective study. Int J Chron Obstruct Pulmon Dis. 2025;20:987–998. doi:10.2147/COPD.S510118
17. Xu Y, Zhang L, Zhu L, et al. Prognostic value of biomarkers in chronic obstructive pulmonary disease: a comprehensive review. Int J Chron Obstruct Pulmon Dis. 2025;20:3123–3134. doi:10.2147/COPD.S531935
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Value of Preoperative Systemic Immune-Inflammation Index as a Predictor of Prolonged Hospital Stay in Orthopedic Surgery: A Retrospective Study
Alsabani MH, Alotaibi BA, Olayan LH, Alghamdi AS, Alshammasi MA, Alqasir BA, Alrashidi SM, Alshugair MS, Al Harbi MK
International Journal of General Medicine 2023, 16:4773-4782
Published Date: 25 October 2023
Predictive Role of White Blood Cell Differential Count for the Development of Acute Exacerbation in Korean Chronic Obstructive Pulmonary Disease
Yoon EC, Koo SM, Park HY, Kim HC, Kim WJ, Kim KU, Jung KS, Yoo KH, Yoon HK, Yoon HY
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:17-31
Published Date: 4 January 2024
Abnormal Expression of Peripheral Blood Leukocyte Surface Markers in Retinopathy of Prematurity Patients
Guo R, Cheng F, Meng XJ, Fan JM, Lu YL, Ma XH, Qiao X, Li JH
Journal of Multidisciplinary Healthcare 2025, 18:651-661
Published Date: 7 February 2025
Dynamic Neutrophil-to-Lymphocyte Ratio at 3-4 weeks of Intensity-Modulated Radiotherapy Combined with Normal Liver Volume Predicts Radiation-Induced Hepatic Toxicity in Hepatocellular Carcinoma: A Retrospective Study
Chen L, Li J, Wang X, Chen S, Wu Y, Li J, Liang S
Journal of Inflammation Research 2025, 18:7879-7892
Published Date: 17 June 2025
Relationship Between Lymphocyte-Associated Inflammatory Markers and Post-Stroke Cognitive Impairment
Hu QY, Liu J, Cui CH, Guo MF, Shi YT, Zhang XM, Jia BF, Li XY, Sun SJ
Journal of Inflammation Research 2025, 18:13347-13358
Published Date: 25 September 2025