Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Association Between Monocyte-to-High Density Lipoprotein-Cholesterol Ratio and COPD Among US Adults: Findings from NHANES 1999–2018
Authors Li X, Chi X, Chen X, Huang M, Pan M, Peng Z, Ruan W, Wei Y, Deng J, Mai Z, Tang M, Sha H, Zhang J
Received 11 June 2025
Accepted for publication 19 November 2025
Published 8 January 2026 Volume 2026:21 546197
DOI https://doi.org/10.2147/COPD.S546197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xiaohua Li,* Xianhong Chi,* Xinyan Chen, Mingsi Huang, Mianluan Pan, Zhimin Peng, Weibin Ruan, Yaqin Wei, Jiehua Deng, Ziqing Mai, Mengxin Tang, Haojun Sha, Jianquan Zhang
Department of Respiratory and Critical Medicine, the Eighth Affiliated Hospital, Sun Yat-Sen University, Shenzhen, Guangdong Province, 518000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianquan Zhang, Email [email protected]
Background: The monocyte to high-density lipoprotein–cholesterol ratio (MHR) has been significantly associated with inflammation. However, there is a paucity of research exploring the association between MHR and the susceptibility to chronic obstructive pulmonary disease (COPD).
Methods: The study cohort comprised participants from ten cycles of the National Health and Nutrition Examination Survey, covering the period from 1999 to 2018. COPD was identified through self-reported diagnoses. Mobile Examination Center weights were applied in accordance with guidelines from National Center for Health Statistics. The multivariate logistic regression analysis was conducted to determine the association between MHR and COPD. Restricted cubic spline curves were employed to investigate the potential dose–response relationship between COPD and MHR. Subgroup analyses and interaction tests were finally performed.
Results: The study included a total of 39,646 participants, including 2,876 COPD participants. After controlling for all potential covariates, weighted logistic regression analysis demonstrated a significant association between MHR and COPD. When MHR was treated as a categorical variable, the risk of COPD increased significantly after adjusting for all potential covariates. The dose–response curve suggested a non-linear relationship between MHR and COPD risk. Subgroup analysis revealed significant interactive effects between MHR and COPD among individuals with varying BMI, marital status and smoking status.
Conclusion: MHR was significantly associated with COPD among US adults. There is a need for further longitudinal cohort studies to explore the relationship between MHR and COPD.
Keywords: chronic obstructive pulmonary disease, monocyte-to-high density lipoprotein–cholesterol ratio, NHANES, inflammation, monocytes, HDL-C
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent chronic respiratory disease characterized by irreversible and progressive airflow limitation. Despite advancements in medical technology and treatment strategies for COPD, the incidence and mortality rates remain significantly high.1 As awareness of the importance of disease prevention grows, early intervention is recognized as crucial for enhancing the prognosis of individuals with COPD. In 2022, the Global Initiative for Chronic Obstructive Lung Disease (GOLD) introduced the concept of “pre-chronic obstructive pulmonary disease”, underscoring the necessity for early detection of COPD in clinical practice.2 Nevertheless, there is a notable absence of effective and convenient tools for assessing the risk of COPD development, highlighting an urgent need to identify and address the risk factors associated with COPD to advance public health outcomes.
Inflammatory biomarkers may be among the most promising candidates to address this gap. The inflammatory response is integral to the pathogenesis and progression of COPD, particularly through mechanisms involving oxidative stress3–7 and the aberrant activation of the immune system induced by inflammation.8 These processes contribute significantly to both the onset and exacerbation of COPD. Traditional biomarkers,9 such as C-reactive protein (CRP),10 fibrinogen11 and white blood cell counts,12 are frequently linked to the inflammatory response in COPD.13 However, these markers often lack adequate sensitivity and specificity, limiting their utility in the early detection of the population with high risk of COPD. Recently, novel inflammation-related biomarkers, including the Dietary Inflammatory Index,14–16 the Triglyceride–Glucose ratio17 and the ratio of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol,15 have been extensively investigated. These biomarkers are significantly associated with various diseases and potential for risk stratification.3 The monocyte to high-density lipoprotein cholesterol ratio (MHR) is an emerging composite inflammatory marker that holds unique promise. It simultaneously reflects pro-inflammatory and anti-inflammatory pathways and offers the practical advantages of being cost-effective and readily obtainable from routine blood tests. Previous research have indicated that MHR is associated with cardiovascular diseases,18–20 gallstones,21 kidney stone22 and metabolic syndrome.23 However, there has been limited research investigating the association between MHR and COPD. Therefore, this study aims to further investigate this association utilizing nationally representative data from the National Health and Nutrition Examination Survey (NHANES) covering the period from 1999 to 2018, to provide more valuable evidence.
Materials and Methods
Study Design and Data Source
This population-based study analyzed publicly available data from the 1999–2018 two-year cycles of NHANES. NHANES is conducted by the National Center for Health Statistics (NCHS), a branch of the Centers for Disease Control and Prevention (CDC) in the United States. The survey aims to assess the health and nutritional status of adults and children nationwide. Utilizing a complex, multistage probability sampling design, NHANES collects and analyzes data representative of the US civilian, non-institutionalized population. The data is accessible for research purposes, with usage permission granted by NCHS. Participants complete household interviews and are invited to visit a Mobile Examination Center (MEC) for comprehensive examinations, which include physical assessments, specialized measurements, and laboratory tests. Additional information about NHANES can be found at https://www.cdc.gov/nchs/nhanes/?CDC_AAref_Val=https://www.cdc.gov/nchs/nhanes/index.htm.
Study Population Selection
We extracted NHANES data from ten consecutive cycles with a sample size of 101,316. The selection of the age range was referenced to the previous study.24 Data were progressively excluded based on the following criteria: 1) age < 20 or ≥ 80 years; 2) missing information on diagnosis of COPD; and 3) missing information on blood monocyte counts or high-density lipoprotein cholesterol (HDL-C). Detailed information is shown in Figure 1.
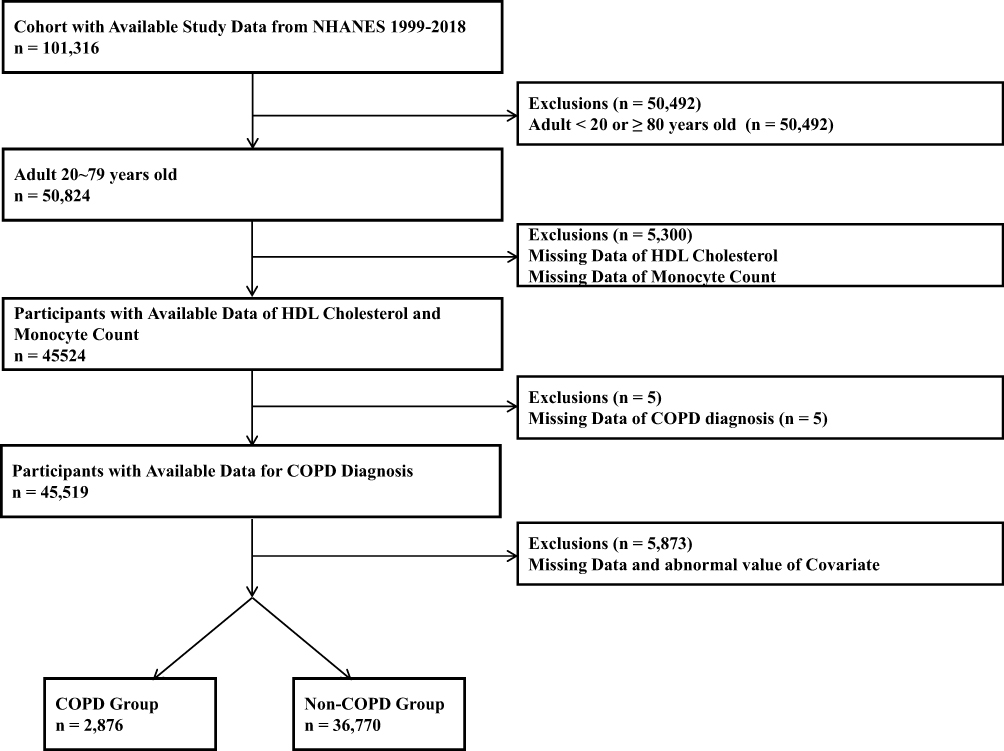 |
Figure 1 The flowchart of population selection. |
Definition of COPD Diagnosis
This study diagnosed COPD through a self-reported questionnaire, asking participants whether they had ever been diagnosed with COPD, emphysema, or chronic bronchitis by doctors or healthcare professional. To be specific, COPD was identified based on participants’ responses to three specific self-reported questions from the NHANES questionnaire, which were designed and quality-controlled by NHANES personnel. The questions were: (1) Ever told you that you had emphysema? (2) Ever told you that you had chronic bronchitis? (3) Ever told you that you had COPD? Participants who responded “Yes” to any of these questions were classified as having a self-reported physician diagnosis of COPD and were assigned to the COPD group. Those who answered “No” to all three questions were categorized into the Non-COPD group. The self-reported method has been widely adopted in the national and large-scale studies.25,26
Measurement of MHR
Monocyte counts and HDL-C levels were measured according to the protocols specified in the NHANES Laboratory/Medical Technologist Procedures Manual. The complete blood count parameters were derived using the Beckman Coulter method of counting and sizing. White blood cell differentials were determined using Volume, Conductivity, and Scatter technology.
HDL-C levels are measured through a selective chemical reaction. After non-HDL cholesterol is removed, HDL-C reacts with specific enzymes to produce a colored compound, the intensity of which is measured at 600 nm to determine concentration. To extract the level of HDL-C, a magnesium/dextran sulfate solution is first added to the specimen to form water-soluble complexes with non-HDL-C fractions. With addition of some reagents, HDL-C are converted by PEG-cholesterol esterase. The HDL-C is acted upon by PEG-cholesterol oxidase, and the chemical products under the action of peroxidase form a purple/blue pigment that is measured photometrically at 600 nm. Detailed descriptions are available on the NHANES website. Subsequently, we calculated the MHR based on the extracted data and stratified all MHR level into four quantiles (the first quantile (Q1), the second quantile (Q2), the third quantile (Q3), the fourth quantile (Q4)) according to their quartile boundaries. The formula for the calculation of MHR is as follows:

Covariates
The following additional baseline risk factor data were collected: (1) demographic characteristics: age, gender, race, education, marital status, and poverty income ratio (PIR); (2) physical examinations parameters: body mass index (BMI); (3) Presence of diabetes, hypertension, cancer and asthma; (4) laboratory findings: monocyte counts and HDL-C levels; (5) The PIR was calculated by dividing the family’s income by the federal poverty threshold appropriate for the family size and composition. Based on PIR values, participants were classified into three income groups based on previous studies:27 low-income (PIR < 2), middle-income (PIR = 2–4), and high-income (PIR > 4). BMI was determined by the formula weight (kg) divided by height squared (m2) and categorized into “Underweight” (BMI < 18 kg/m2), “Normal weight” (BMI = 18–24.9 kg/m2), “Overweight” (BMI= 25-29.9 kg/m2), and “Obesity” (BMI ≥ 30 kg/m2). Education was dichotomized into “Less than high school” and “High school and above”. Age was stratified into three groups: “20–39 years”, “40–59 years”, and “60–79 years”. Marital status was classified into two categories “Married or Living with partner” and “living alone” (“Widowed”/“Divorce”/“Separated”/“Never married”). Race was composed by “Mexican American”, “Other Hispanic”, “Non-Hispanic White”, “Non-Hispanic Black” and “Other Race”. According to the participants’ response to the question “Have you smoked at least 100 cigarettes in your entire life?”, smoking status was, respectively, classified as “Yes” and “No”. Individuals were inquired about whether a doctor or other healthcare professional has ever diagnosed them with chronic comorbidities including diabetes, asthma, cancer, hypertension. If the response was affirmative, it was determined that the person had the comorbidity mentioned above.
Statistical Analysis
To account for the complex sampling design of NHANES, which includes weighting, clustering, and stratification, appropriate survey methodologies were employed. MEC weights were applied in accordance with guidelines from NCHS. Continuous variables with a normal distribution were expressed as mean ± standard deviation and analyzed using the t-test. Non-normally distributed continuous variables were presented as median with interquartile ranges (25th, 75th percentiles) and assessed using the Kruskal–Wallis H-test. Categorical variables were reported as counts (n) and percentages (%) and analyzed using the chi-square test.
To investigate the association between MHR levels and the prevalence of COPD, the multivariate logistic regression analyses were performed while adjusting for potential confounders. Model I was adjusted for age, gender, race, marital status, education, PIR, Model II was adjusted for all variables in Model I, BMI and smoking, and Model III was adjusted for all variables in Model II, diabetes, hypertension, asthma and cancer.
To account for potential nonlinear dose–response relationships between COPD and MHR, we employed restricted cubic spline (RCS) modeling using model III. We set the candidate knots ranging from 3 to 8, and performed 5-fold cross-validation to train the model under each knot’s configuration, followed by prediction and Area Under the Curve (AUC) calculation. Finally, the knots demonstrating the highest average AUC value was selected, and an RCS plot was drawn in Figure 2.
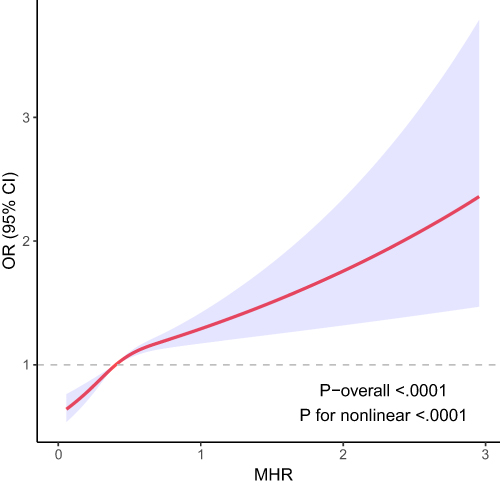 |
Figure 2 The Non-Linear Association Between MHR and COPD by RCS. |
Subgroup analyses were conducted to explore potential differences among the different populations in model III and to assess the potential modifying effects by testing the corresponding multiplicative interaction terms. Finally, forest plots (Figure 3) were used to show the result of the subgroup analyses.
 |
Figure 3 The forest plot for subgroup analysis under adjusting for all covariates. |
All statistical analyses were performed using R software version 4.4.0 (http://www.r-project.org), Zstats 1.0 (www.zstats.net) and SPSS 26.0 software, and double-sided P < 0.05 was defined as statistical significance.
Result
Baseline Characteristics of Participants
As shown in Table 1, 39,646 participants were enrolled in the present study from the NHANES database between 1999 and 2018. The weighted prevalence of COPD was 7.25%, with 2,876 individuals with COPD. When participants were categorized into quartiles based on MHR levels (Q1: < 0.293; Q2: 0.293–0.404; Q3: 0.404–0.550; Q4: ≥ 0.550), a clear trend of increasing MHR was observed across quartiles in the COPD group, while levels remained relatively stable in the non-COPD group. In Table 2, participants with COPD had higher MHR levels than those without COPD. Tables 1 and 2 demonstrate statistically significant differences for most covariates across groups, with the exception of asthma and cancer in Table 2. (P > 0.05).
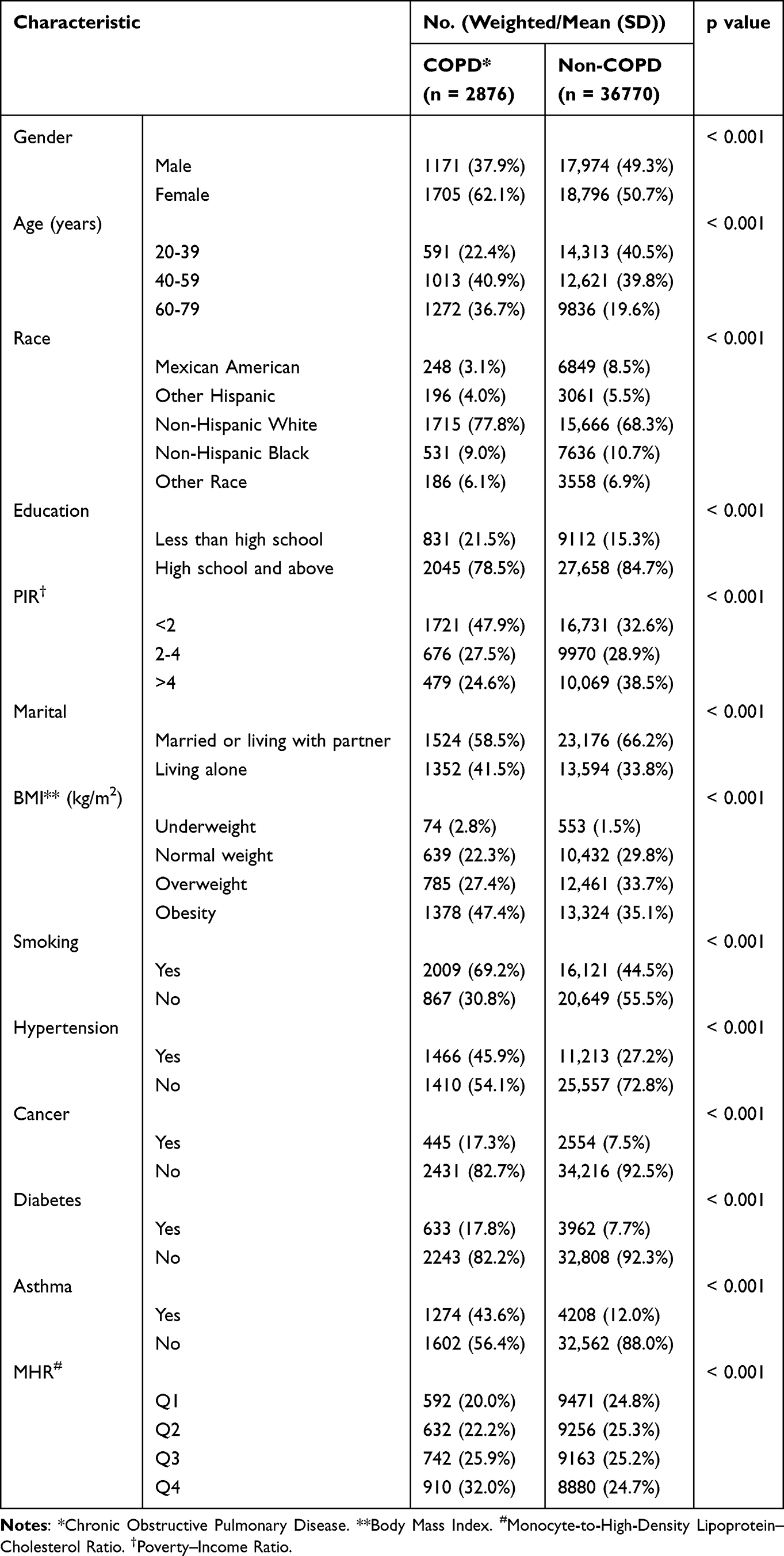 |
Table 1 Baseline Characteristic, Classified by COPD, for the Association Between COPD and MHR Among US Population with Age 20–79 Years, NHANES 1999–2018 |
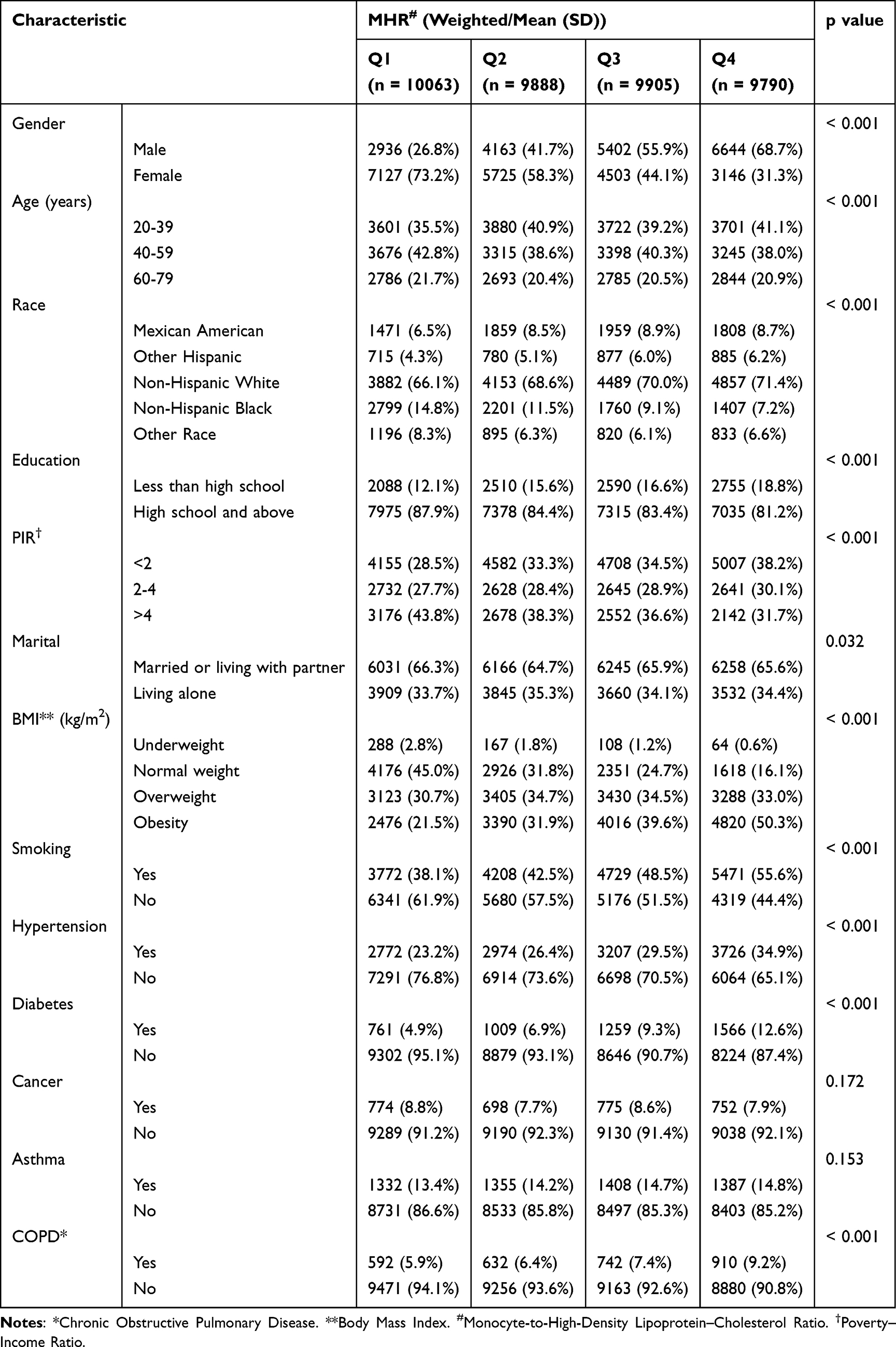 |
Table 2 Baseline Characteristic, Classified by MHR, for the Association Between COPD and MHR Among US Population with Age 20–79 Years, NHANES 1999–2018 |
Multivariable Logistic Regression Analysis of the Association Between MHR and COPD
The independent association between MHR and COPD was analyzed via three weighted logistic regression models, as shown in Table 3. After adjusting for potential covariates across three models, the continuous MHR showed a significant positive correlation with risk of COPD in all models. Notably, in the fully adjusted model (Model III), participants in the highest MHR quartile (Q4) had a 36% greater risk of COPD compared to those in the lowest quartile (Q1) (OR: 1.36, 95% CI: 1.19–1.54, p < 0.001).
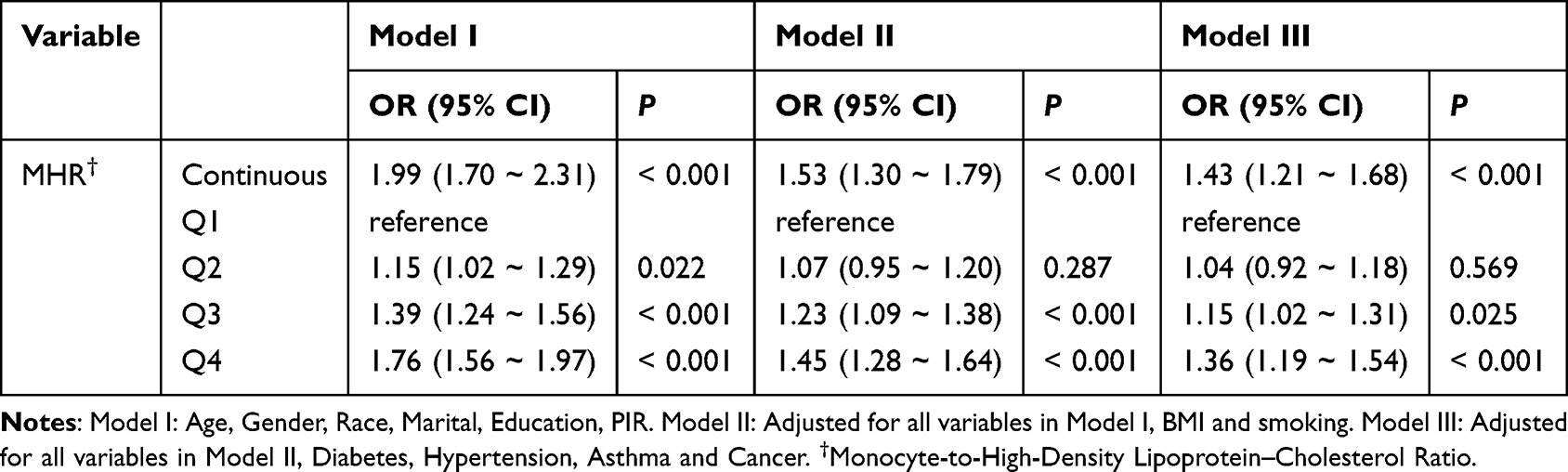 |
Table 3 Multivariate Logistic Regression Models for the Association Between MHR Level and COPD Prevalence, NHANES 1999–2018 |
The Non-Linear Association Between MHR and COPD
The study utilized RCS plots to visualize the dose–response relationship between MHR and COPD, revealing a nonlinear association. The curve demonstrated a positive correlation between MHR and COPD prevalence odds beyond a certain cutoff point, after which the relationship remained positive but stabilized. The difference in the curve before and after this threshold was statistically significant (Figure 2).
Subgroup Analysis
To further evaluate the robustness of the association between MHR and the risk of COPD, the multi-subgroup analyses and interaction tests were conducted across various covariates. Figure 3 shows the forest plot for subgroup analysis under adjusting for all covariates we included in the study. Our subgroup analyses demonstrated stability in the positive association between MHR and COPD risk, as evidenced by non-significant interaction terms across most subgroups. This robustness suggests the observed relationship is consistent across diverse demographic (age, gender, race, education, PIR) and comorbidities (diabetes, hypertension, asthma and cancer). In addition, the relationship between MHR and COPD was significantly different in the subgroups stratified by BMI, marital status and smoking status, indicating that the association between elevated MHR and higher COPD risk was more pronounced among overweight individuals (p for interaction = 0.045, OR: 1.99, 95% CI: 1.46–2.70, p < 0.001), those living alone (p for interaction = 0.041, OR: 1.77, 95% CI: 1.37–2.29, p < 0.001) and the smoking subgroup (p for interaction < 0.001, OR: 1.76, 95% CI: 1.45–2.14, p < 0.001). Detailed data can be found in Figure 3.
Discussion
This study utilized data from ten cycles of NHANES (1999–2018) to investigate the association between MHR and COPD. Our findings indicate that after adjusting for potential covariates, there is a positive association between MHR and COPD risk. Individuals with higher MHR levels had 36% higher odds of COPD prevalence compared to those with lower levels. Furthermore, when analyzed as a continuous variable, each unit increase in MHR was associated with a 43% elevation in COPD odds. Subgroup interaction analysis results revealed consistent interaction results across all subgroups, except for BMI, marital status and smoking status, where significant interactions were observed. Therefore, the potential mechanisms underlying the relationship between MHR and COPD in “overweight”, “living alone” and “smoking” subgroups warrant further in‐depth research and exploration.
In this study, COPD patients were predominantly characterized as female, elderly (≥ 60 years), obese, low-income (PIR < 2), and with smoking history, aligning with established research.28,29 Gender differences in COPD susceptibility are particularly pronounced among non-smokers, with females showing higher vulnerability to disease onset and progression.30,31 Aging synergistically amplifies COPD risk through cumulative exposure to smoking, environmental pollutants, and socioeconomic challenges compounded by comorbidities.32 This underscores the compounded impact of sociodemographic and clinical risk factors on COPD burden, highlighting the need for multidimensional management strategies.
Recent advances have highlighted the clinical relevance of novel biomarkers in disease prediction and management. As a composite inflammatory metabolic marker, the MHR uniquely integrates peripheral monocyte counts and HDL-C levels, providing a multidimensional perspective on the interplay between inflammation and lipid metabolism. Compared to individual parameters, MHR shows enhanced predictive capacity for clinical outcomes.33,34 Evidence demonstrates its association with renal function decline,33 cardiovascular mortality risk,34 the occurrence of cardio-renal syndrome and deep vein thrombosis35,36 as well as diabetes-related metabolic inflammation, particularly when combined with hs-CRP assessment for systemic inflammation evaluation.37 These findings support the role of an elevated MHR as a marker of monocyte-mediated inflammation and HDL-C dysfunction, which aligns with the association we observed between MHR and the risk of COPD.
In addition, our RCS analysis showed a significant nonlinear relationship between MHR and COPD (overall P-value < 0.001, nonlinear P-value < 0.001), suggesting a dose–response relationship between MHR and COPD risk. However, the mechanisms are not fully elucidated. Monocytes, constituting about 10% of peripheral leukocytes,38–40 are recruited to the lungs and drive COPD pathology.41 Clinically, elevated circulating monocytes (especially non-classical42) correlate with disease severity43 and exacerbations.44 HDL-C, typically an anti-inflammatory regulator of monocytes,45 displays paradoxical effects in COPD. Some studies report reduced HDL-C levels linked to impaired lung function,46 whereas others describe elevated but dysfunctional HDL-C with compromised protective effects.47,48 This HDL-C paradox suggests context-dependent anti-/pro-inflammatory roles in COPD progression.35 We propose that the MHR quantifies a critical immunometabolic balance. Its disruption likely triggers the persistent inflammatory cascade central to COPD pathogenesis.
As shown in Figure 3, the positive association between increased MHR and increased COPD risk was more pronounced in “overweight”, “living alone” and “smoking” subgroup. Smoking is a well-established risk factor that promotes COPD progression by triggering systemic inflammation, dyslipidemia, and accelerated emphysema development. It is acknowledged that high BMI is a key factor in the development of various chronic diseases. However, the “obesity paradox” suggests that the risk of developing COPD and its acute exacerbations may not increase but instead decrease in these patients. A large retrospective study of US veterans found that overweight and obese patients are more likely to be misdiagnosed with COPD, consequently receiving inappropriate treatments and having other more critical etiologies overlooked.49 In this context, MHR, as a biomarker, may help refine risk stratification for this population. Although direct evidence linking living alone to COPD is lacking, studies suggest that living alone is often associated with psychosocial factors, such as stress or limited social support, poorer dietary and nutritional status, which may indirectly exacerbate disease risk.50 Therefore, integrating our findings with previous evidence indicates that the association between MHR and COPD is stronger in the overweight, living-alone, and smoking subgroups. Collectively, these subgroup findings suggest that MHR may have particular utility for risk stratification and targeted prevention efforts in these specific, high-risk populations.
This study has several notable strengths. First, the analysis of a large, nationally representative cohort from NHANES (n = 39,646) enhances the generalizability and robustness of our findings. Second, we employed advanced statistical methodologies, including RCS, to identify non-linear thresholds in the MHR-COPD relationship and conducted comprehensive multivariable adjustments to control for a wide range of potential confounders. Finally, our subgroup analyses provided valuable insights by identifying specific populations where the association is most pronounced.
This study has several limitations. First, the use of self-reported COPD diagnoses, though previously validated,25 is susceptible to recall bias. Second, the cross-sectional design precludes causal inference, and reverse causality remains possible whereby COPD status may influence MHR levels. Third, despite adjusting for key covariates, residual confounding from unmeasured or imprecisely measured factors such as diet, physical activity, and medication use, cannot be ruled out. Additionally, the analysis of data spanning 1999–2018 may not fully reflect contemporary epidemiological patterns. Finally, the predominantly U.S.-based sample limits generalizability to other populations or healthcare settings.
Conclusions
In conclusion, this study revealed a positive correlation between MHR and COPD risk. Individuals with higher MHR may warrant prioritized attention regarding COPD risk. Our findings provide some insight into the role of MHR in the pathogenesis of COPD and firstly establish MHR as a statistically significant independent risk factor for COPD, albeit with a modest effect. Additionally, there is a need for further longitudinal cohort studies to explore the deeper mechanisms and potential applications of the relationship between MHR and COPD.
Abbreviation
AUC, Area Under the Curve; BMI, Body Mass Index; CDC, Centers for Disease Control and Prevention; COPD, Chronic Obstructive Pulmonary Disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HDL-C, High-Density Lipoprotein–Cholesterol; HsCRP, High-sensitivity C-reactive Protein; MHR, Monocyte-to-High-Density Lipoprotein–Cholesterol Ratio; MEC, Mobile Examination Center; NCHS, National Center for Health Statistics; PIR, Poverty–Income Ratio; RCS, Restricted cubic spline; ROS, Reactive Oxygen Species.
Data Sharing Statement
The datasets generated during and analyzed during the current study are available in the National Health and Nutrition Examination Survey (NHANES) repository, https://www.cdc.gov/nchs/nhanes/index.htm.
Ethics Approval and Consent to Participate
NHANES was approved by the CDC/NCHS Ethics Review Board and all individuals signed informed consent to participate in NHANES. The study is exempt based on national guidelines such as item 1 and 2 of Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects dated February 18, 2023, China.
Acknowledgments
We deeply appreciate the NHANES that shared high quality data for our analysis and researches.
Funding
This work was supported by grants from the Natural Science Foundation of Guangdong province [grant numbers 2024A1515011073, 2023A1515012987]; the Science and Technology Innovation Commission of Shenzhen [grant numbers JCYJ20250604142716021]; the Shenzhen Clinical Research Center for respiratory disease [grant number HXKTZJQ202501]; the Public Health Welfare Research Projects of Shenzhen Futian District [grant number FTWS2025099]; the Science and Technology Department of Guangxi Zhuang Autonomous Foundation of Guangxi Key Research and Development Program [grant numbers 2024AB17061]; the Science and Technology Innovation Commission of Shenzhen [grant numbers JCYJ20230807110914029]; the Public Health Welfare Research Projects of Shenzhen Futian District [grant numbers FTWS2022019].
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–13. doi:10.1016/S2213-2600(20)30105-3
2. Agustí A, Celli BR, Criner GJ, et al. Global initiative for chronic obstructive lung disease 2023 report: GOLD executive summary. Respirology. 2023;28(4):316–338. doi:10.1111/resp.14486
3. Xu J, Zeng Q, Li S, et al. Inflammation mechanism and research progress of COPD. Front Immunol. 2024;15:1404615. doi:10.3389/fimmu.2024.1404615
4. Chang C, Huang K, Xu X, et al. MiR-23a-5p alleviates chronic obstructive pulmonary disease through targeted regulation of RAGE-ROS pathway. Respir Res. 2024;25(1):93. doi:10.1186/s12931-024-02736-y
5. Teyani RL, Moghaddam F, Moniri NH. ROS-mediated regulation of β2AR function: does oxidation play a meaningful role towards β2-agonist tachyphylaxis in airway obstructive diseases? Biochem Pharmacol. 2024;226:116403. doi:10.1016/j.bcp.2024.116403
6. Zhu Y, Dutta S, Han Y, et al. Oxidative stress promotes lipid-laden macrophage formation via CYP1B1. Redox Biol. 2025;79:103481. doi:10.1016/j.redox.2024.103481
7. Strzelak A, Ratajczak A, Adamiec A, et al. Tobacco smoke induces and alters immune responses in the lung triggering inflammation, allergy, asthma and other lung diseases: a mechanistic review. Int J Environ Res Public Health. 2018;15(5). doi:10.3390/ijerph15051033
8. Lugg ST, Scott A, Parekh D, et al. Cigarette smoke exposure and alveolar macrophages: mechanisms for lung disease. Thorax. 2022;77(1):94–101. doi:10.1136/thoraxjnl-2020-216296
9. Shah KPK, Bhat HP, Kadam M, et al. Assessment of the BODE index and its association with inflammatory mediators in chronic obstructive pulmonary disease (COPD) patients. Cureus. 2024;16(10):e72172. doi:10.7759/cureus.72172
10. Agustí A, Edwards LD, Rennard SI, et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 2012;7(5):e37483. doi:10.1371/journal.pone.0037483
11. Mannino DM, Tal-Singer R, Lomas DA, et al. Plasma fibrinogen as a biomarker for mortality and hospitalized exacerbations in people with COPD. Chronic Obstr Pulm Dis. 2015;2(1):23–34. doi:10.15326/jcopdf.2.1.2014.0138
12. Thomsen M, Ingebrigtsen TS, Marott JL, et al. Inflammatory biomarkers and exacerbations in chronic obstructive pulmonary disease. JAMA. 2013;309(22):2353–2361. doi:10.1001/jama.2013.5732
13. Ellingsen J, Janson C, Bröms K, et al. CRP, fibrinogen, white blood cells, and blood cell indices as prognostic biomarkers of future COPD EXACERBATION FREQUENCY: the TIE cohort study. J Clin Med. 2024;13(13). doi:10.3390/jcm13133855
14. Sedighi M, Saber A, Bagheri A, et al. The associations between diet-induced inflammation and the improvement or worsening of hepatic steatosis and fibrosis: a longitudinal analysis of RaNCD cohort study. Nutr Metab. 2025;22(1):5. doi:10.1186/s12986-025-00897-1
15. Wu R, Gong H. The association between non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol ratio and chronic obstructive pulmonary disease: the mediating role of dietary inflammatory index. Front Nutr. 2024;11:1427586. doi:10.3389/fnut.2024.1427586
16. Chen C, Yang T, Wang C. The dietary inflammatory index and early COPD: results from the national health and nutrition examination survey. Nutrients. 2022;14(14). doi:10.3390/nu14142841
17. Wang X, Cui X, Fan H, et al. Elevated triglyceride-glucose (TyG) index predicts poor clinical outcomes in critically Ill AECOPD patients: a retrospective study. Int J Chron Obstruct Pulmon Dis. 2024;19:2217–2228. doi:10.2147/COPD.S477268
18. Wu Y, Meng Y, Yi W, et al. The ratio of monocyte count and high-density lipoprotein cholesterol mediates the association between urinary tungsten and cardiovascular disease: a study from NHANES 2005-2018. Environ Sci Pollut Res Int. 2023;30(36):85930–85939. doi:10.1007/s11356-023-28214-4
19. Jiang M, Yang J, Zou H, et al. Monocyte-to-high-density lipoprotein-cholesterol ratio (MHR) and the risk of all-cause and cardiovascular mortality: a nationwide cohort study in the United States. Lipids Health Dis. 2022;21(1):30. doi:10.1186/s12944-022-01638-6
20. Yan S, Sha S, Wang D, et al. Association between monocyte to high-density lipoprotein ratio and coronary heart disease in US adults in the national health and nutrition examination surveys 2009-2018. Coron Artery Dis. 2023;34(2):111–118. doi:10.1097/MCA.0000000000001208
21. Liu X, Yan G, Xu B, et al. Association between monocyte-to-high-density lipoprotein-cholesterol ratio and gallstones in U.S. adults: findings from the national health and nutrition examination survey 2017-2020. Lipids Health Dis. 2024;23(1):173. doi:10.1186/s12944-024-02166-1
22. Wang Z, Zhao G, Cao Y, et al. Association between monocyte to high-density lipoprotein cholesterol ratio and kidney stone: insights from NHANES. Front Endocrinol. 2024;15:1374376. doi:10.3389/fendo.2024.1374376
23. Liang Y, Liu Y, Tan Q, et al. Systemic immune-inflammation mediates the association between Klotho protein and metabolic syndrome: findings from a large-scale population-based study. Lipids Health Dis. 2024;23(1):360. doi:10.1186/s12944-024-02339-y
24. Liu S, Ben X, Liang H, et al. Association of acrylamide hemoglobin biomarkers with chronic obstructive pulmonary disease in the general population in the US: NHANES 2013-2016. Food Funct. 2021;12(24):12765–12773. doi:10.1039/D1FO02612G
25. Ford ES, Croft C, Mannino DM, et al. COPD surveillance--United States, 1999-2011. Chest. 2013;144(1):284–305. doi:10.1378/chest.13-0809
26. Liu Y, Greenlund KJ, VanFrank B, et al. Smoking cessation among U.S. Adult smokers with and without chronic obstructive pulmonary disease, 2018. Am J Prev Med. 2022;62(4):492–502. doi:10.1016/j.amepre.2021.12.001
27. Liu M, Aggarwal R, Zheng Z, et al. Cardiovascular health of middle-aged U.S. Adults by income level, 1999 to March 2020: a serial cross-sectional study. Ann Intern Med. 2023;176(12):1595–1605. doi:10.7326/M23-2109
28. Chen H, Luo X, Du Y, et al. Association between chronic obstructive pulmonary disease and cardiovascular disease in adults aged 40 years and above: data from NHANES 2013-2018. BMC Pulm Med. 2023;23(1):318. doi:10.1186/s12890-023-02606-1
29. Yan Z, Xu Y, Li K, et al. Heavy metal levels and flavonoid intakes are associated with chronic obstructive pulmonary disease: an NHANES analysis (2007-2010 to 2017-2018. BMC Public Health. 2023;23(1):2335. doi:10.1186/s12889-023-17250-x
30. Lamprecht B, MA M, Vollmer WM, et al. COPD in never smokers: results from the population-based burden of obstructive lung disease study. Chest. 2011;139(4):752–763. doi:10.1378/chest.10-1253
31. Montserrat-Capdevila J, Godoy P, Marsal JR, et al. Prevalence and characteristics of chronic obstructive pulmonary disease in non-smokers. Aten Primaria. 2019;51(10):602–609. doi:10.1016/j.aprim.2017.10.012
32. Agustí A, Melén E, DeMeo DL, et al. Pathogenesis of chronic obstructive pulmonary disease: understanding the contributions of gene-environment interactions across the lifespan. Lancet Respir Med. 2022;10(5):512–524. doi:10.1016/S2213-2600(21)00555-5
33. Xu L, Li D, Song Z, et al. The association between monocyte to high-density lipoprotein cholesterol ratio and chronic kidney disease in a Chinese adult population: a cross-sectional study. Ren Fail. 2024;46(1):2331614. doi:10.1080/0886022X.2024.2331614
34. Pruc M, Kubica J, Banach M, et al. Prognostic value of the monocyte-to-high-density lipoprotein-cholesterol ratio in ACS patients: a systematic review and meta-analysis. Kardiol Pol. 2024. doi:10.33963/v.phj.102773
35. Lin J, Li Z, Xu J, et al. Independent and joint associations of monocyte to high-density lipoprotein-cholesterol ratio and body mass index with cardiorenal syndrome: insights from NHANES 2003-2020. Lipids Health Dis. 2024;23(1):153. doi:10.1186/s12944-024-02149-2
36. Selvaggio S, Brugaletta G, Abate A, et al. Platelet‑to‑lymphocyte ratio, neutrophil‑to‑lymphocyte ratio and monocyte to HDL cholesterol ratio as helpful biomarkers for patients hospitalized for deep vein thrombosis. Int J Mol Med. 2023;51(6). doi:10.3892/ijmm.2023.5255
37. Wu D, Lan Y, Xu Y, et al. Association of cumulative monocyte to high-density lipoprotein ratio with the risk of type 2 diabetes: a prospective cohort study. Cardiovasc Diabetol. 2022;21(1):268. doi:10.1186/s12933-022-01701-7
38. Auffray C, Sieweke MH, Geissmann F. Blood monocytes: development, heterogeneity, and relationship with dendritic cells. Annu Rev Immunol. 2009;27:669–692. doi:10.1146/annurev.immunol.021908.132557
39. PB N, Marcovecchio P, Hamers AA, et al. Nonclassical monocytes in health and disease. Annu Rev Immunol. 2019;37:439–456. doi:10.1146/annurev-immunol-042617-053119
40. Sampath P, Moideen K, Ranganathan R, et al. Monocyte subsets: phenotypes and function in tuberculosis infection. Front Immunol. 2018;9:1726. doi:10.3389/fimmu.2018.01726
41. Wohnhaas CT, Baßler K, Watson CK, et al. Monocyte-derived alveolar macrophages are key drivers of smoke-induced lung inflammation and tissue remodeling. Front Immunol. 2024;15:1325090. doi:10.3389/fimmu.2024.1325090
42. Wacleche VS, Tremblay CL, Routy JP, et al. The biology of monocytes and dendritic cells: contribution to HIV pathogenesis. Viruses. 2018;10(2). doi:10.3390/v10020065
43. Cornwell WD, Kim V, Fan X, et al. Activation and polarization of circulating monocytes in severe chronic obstructive pulmonary disease. BMC Pulm Med. 2018;18(1):101. doi:10.1186/s12890-018-0664-y
44. Lin CH, Li YR, Lin PR, et al. Blood monocyte levels predict the risk of acute exacerbations of chronic obstructive pulmonary disease: a retrospective case-control study. Sci Rep. 2022;12(1):21057. doi:10.1038/s41598-022-25520-8
45. Wang W, Xu H, Shi Y, et al. Genetic deletion of apolipoprotein A-I increases airway hyperresponsiveness, inflammation, and collagen deposition in the lung. J Lipid Res. 2010;51(9):2560–2570. doi:10.1194/jlr.M004549
46. Gunay S, Sariaydin M, Acay A. New predictor of atherosclerosis in subjects with COPD: atherogenic indices. Respir Care. 2016;61(11):1481–1487. doi:10.4187/respcare.04796
47. Van Lenten BJ, Ham SY, de Beer FC, et al. Anti-inflammatory HDL becomes pro-inflammatory during the acute phase response. Loss of protective effect of HDL against LDL oxidation in aortic wall cell cocultures. J Clin Invest. 1995;96(6):2758–2767. doi:10.1172/JCI118345
48. Han CY, Tang C, Guevara M, et al. Serum amyloid A impairs the antiinflammatory properties of HDL. J Clin Invest. 2016;126(2):796. doi:10.1172/JCI86401
49. Collins BF, Ramenofsky D, Au DH, et al. The association of weight with the detection of airflow obstruction and inhaled treatment among patients with a clinical diagnosis of COPD. Chest. 2014;146(6):1513–1520. doi:10.1378/chest.13-2759
50. Odencrants S, Bjuström T, Wiklund N, et al. Nutritional status, gender and marital status in patients with chronic obstructive pulmonary disease. J Clin Nurs. 2013;22(19–20):2822–2829. doi:10.1111/jocn.12222
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
AMPK/SIRT1 Deficiency Drives Adjuvant-Induced Arthritis in Rats by Promoting Glycolysis-Mediated Monocytes Inflammatory Polarization
Wang DD, He CY, Wu YJ, Xu L, Shi C, Olatunji OJ, Zuo J, Ji CL
Journal of Inflammation Research 2022, 15:4663-4675
Published Date: 15 August 2022
α-Mangostin Inhibited M1 Polarization of Macrophages/Monocytes in Antigen-Induced Arthritis Mice by Up-Regulating Silent Information Regulator 1 and Peroxisome Proliferators-Activated Receptor γ Simultaneously

Wu YJ, Zhang SS, Yin Q, Lei M, Wang QH, Chen WG, Luo TT, Zhou P, Ji CL
Drug Design, Development and Therapy 2023, 17:563-577
Published Date: 23 February 2023
Dental Pulp Stem Cells Ameliorate Elastase-Induced Pulmonary Emphysema by Regulating Inflammation and Oxidative Stress
Gao X, Liu Z, Wang Z
Journal of Inflammation Research 2023, 16:1497-1508
Published Date: 8 April 2023
Emerging Anti-Inflammatory COPD Treatments: Potential Cardiovascular Impacts
Cazzola M, Calzetta L, Rogliani P, Matera MG
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:2481-2495
Published Date: 21 November 2024
Exercise Prescription Training in Chronic Obstructive Pulmonary Disease: Benefits and Mechanisms
Liu S, Yang A, Yu Y, Xu B, Yu G, Wang H
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:1071-1082
Published Date: 15 April 2025