Back to Journals » Drug Design, Development and Therapy » Volume 20
Association Between Glucagon-Like Peptide-1 Receptor Agonists and Clinical Outcomes in Patients with Chronic Obstructive Pulmonary Disease and Obesity
Authors Huang SC, Wu JY ![]() , Kuo CY, Hsu WH, Tsai YW, Lai CC
, Kuo CY, Hsu WH, Tsai YW, Lai CC ![]()
Received 13 March 2026
Accepted for publication 3 June 2026
Published 8 June 2026 Volume 2026:20 609054
DOI https://doi.org/10.2147/DDDT.S609054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Solomon Tadesse Zeleke
Sheng-Chi Huang,1 Jheng-Yan Wu,2,3 Chia-Yu Kuo,1 Wan-Hsuan Hsu,4 Ya-Wen Tsai,5 Chih-Cheng Lai6,7
1Department of General Medicine, Chi Mei Medical Center, Tainan, Taiwan; 2Department of Nutrition, Chi Mei Medical Center, Tainan, Taiwan; 3Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan; 4Department of Internal Medicine, Chi Mei Medical Center, Tainan, Taiwan; 5Division of Preventive Medicine, Chi Mei Medical Center, Tainan, Taiwan; 6Department of Intensive Care Medicine, Chi Mei Medical Center, Tainan, Taiwan; 7School of Medicine, College of Medicine, National Sun Yat-Sen University, Kaohsiung, Taiwan
Correspondence: Chih-Cheng Lai, Department of Intensive Care Medicine, Chi Mei Medical Center, Tainan, Taiwan, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) frequently coexists with obesity, creating a vulnerable phenotype associated with increased exacerbations and mortality. Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have demonstrated benefits in weight management and cardiovascular protection, but their effects in patients with COPD and obesity remain unclear.
Methods: We conducted a retrospective cohort study using the TriNetX global research network. We identified adult patients with coexisting COPD and obesity who initiated GLP-1RA or other weight-loss medications. We performed 1:1 propensity-score matching to balance baseline characteristics between the study groups. The primary outcome was all-cause mortality. Secondary outcomes included COPD exacerbations, acute respiratory failure, pneumonia, and major adverse cardiovascular events (MACE).
Results: After propensity score matching, the study included 10,487 patients in each group. During follow-up, all-cause mortality occurred in 237 patients (0.8 per 100 person-years) in the GLP-1RA group compared with 519 patients (2.2 per 100 person-years) in the control group (hazard ratio [HR], 0.43; 95% confidence interval [CI], 0.37 to 0.50). GLP-1RA use was also associated with reduced risk of COPD exacerbations (HR, 0.79; 95% CI, 0.71 to 0.88), acute respiratory failure (HR, 0.55; 95% CI, 0.49 to 0.62), pneumonia (HR, 0.72; 95% CI, 0.64 to 0.81), and MACE (HR, 0.71; 95% CI, 0.64 to 0.79). Results remained consistent across multiple sensitivity analyses and subgroup analyses.
Conclusion: Among patients with coexisting COPD and obesity, GLP-1RA use was associated with lower risks of mortality and adverse respiratory and cardiovascular outcomes compared with other weight loss medication. However, given the observational nature of this study, these findings should be interpreted with caution, as residual confounding cannot be excluded. Randomized controlled trials are warranted to establish causality and confirm these findings.
Keywords: chronic obstructive pulmonary disease, obesity, glucagon-like peptide-1 receptor agonists, mortality, exacerbations, cardiovascular events
A Letter to the Editor has been published for this article.
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide, affecting more than 400 million individuals globally.1 Beyond its primary respiratory manifestations, COPD frequently coexists with multiple systemic comorbidities that substantially influence disease trajectory and patient outcomes.2 Among these comorbidities, obesity is particularly prevalent and clinically significant, affecting approximately 20% to 54% of patients with COPD.2–5 The relationship between obesity and COPD is complex. Obesity contributes to restrictive lung physiology, increases systemic inflammation, and impairs respiratory mechanics through increased chest wall load and reduced diaphragmatic excursion.6 The coexistence of obesity and COPD creates a vulnerable phenotype associated with adverse clinical outcomes. Observational studies have demonstrated that obese individuals with COPD experience more frequent exacerbations, higher hospitalization rates, increased health care resource use, and diminished quality of life compared with their nonobese counterparts.4,5
Given these challenges, effective weight management strategies are critically needed for patients with COPD and obesity. Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have revolutionized the management of type 2 diabetes (T2D) and obesity through their dual effects on glycemic control and weight reduction.7,8 Recent landmark trials have demonstrated that GLP-1RAs can achieve substantial weight loss of 10% to 20% of body weight, with additional cardiovascular and renal protective effects that extend beyond glycemic control and weight reduction alone.7,9–11 Several studies have also reported improved clinical outcomes among patients with COPD and comorbid T2D who received GLP-1RAs.12–15 However, whether these benefits extend to patients with COPD and obesity, independent of diabetes status, remains uncertain. To date, only one small randomized clinical trial involving 40 patients with COPD and obesity has directly evaluated GLP-1RA effects in this population; this trial reported that compared with placebo, liraglutide use resulted in significant weight loss, increased forced vital capacity and carbon monoxide diffusion capacity, and improved COPD Assessment Test score.16 While these preliminary findings are hypothesis-generating, they are insufficient to draw definitive conclusions given the small sample size, limited generalizability, and evaluation of a single agent. Furthermore, the respiratory safety profile of GLP-1RAs in this population, including the potential risks of respiratory adverse events, warrants careful evaluation before broad clinical adoption.
To address this knowledge gap, we conducted a large-scale, real-world comparative effectiveness study using the TriNetX global federated health research network to evaluate the association between GLP-1RA use and clinical outcomes in patients with coexisting COPD and obesity. We employed an active-comparator, new-user design, using other weight loss agents as the reference group. This comparator was selected because it represents a clinically relevant alternative for weight management in this population, and its use helps minimize indication bias and confounding by channeling that may arise when comparing treated patients against untreated controls. We assessed the effects of GLP-1RAs on all-cause mortality, COPD exacerbation, acute respiratory failure, pneumonia, and major adverse cardiovascular events (MACEs). We acknowledge that, as with all observational database studies, residual confounding, differences in adherence, and unmeasured clinical variables may limit causal inference. Accordingly, our findings are intended to complement evidence from controlled trials, and to provide hypothesis-generating real-world evidence to inform clinical decision-making in this understudied population.
Methods
Data Source
This retrospective cohort study utilized data from the TriNetX Global Collaborative Network, a federated health research platform comprising deidentified electronic medical records from approximately 186 million patients across over 168 healthcare organizations (HCOs) in North America, Europe, the Middle East, and the Asia-Pacific region.17 The TriNetX network includes data on demographics, diagnoses (ICD-10-CM), procedures (ICD-10-PCS and CPT codes), medications (RxNorm and VA Drug Classification), laboratory results (LOINC), and healthcare utilization. Unlike centralized databases, TriNetX employs a federated model that enables real-time querying of deidentified patient-level data while ensuring that raw data remain within the original institutions, thus upholding data security and regulatory compliance, including HIPAA and GDPR. Ethical approval was obtained from the Institutional Review Board of Chi Mei Medical Center, which also waived the requirement for informed consent, as only deidentified, aggregate-level data were analyzed. This study followed the principles of the Declaration of Helsinki and adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Study Population
We identified adult patients (≥18 years of age) with diagnoses of both COPD and obesity who initiated weight loss therapy between January 1, 2022, and November 30, 2025. The index date was defined as the date of first prescription for either a GLP-1RA or another weight loss medication during the study period.
Patients were classified into two groups: those who initiated GLP-1RA therapy (semaglutide, liraglutide, or tirzepatide) and those who initiated other weight loss medication including orlistat, setmelanotide, bupropion, naltrexone, phentermine, or topiramate. We excluded patients with a history of organ transplantation, end-stage renal disease requiring dialysis, or diabetes mellitus. We also excluded patients included individuals younger than 18 years; had a history of solid organ or tissue transplantation; had end-stage renal disease or dependence on renal dialysis; had received study drugs before the index date; or were lost to follow-up (Table S1).
Covariates
We collected data on demographic characteristics, baseline comorbidities and COPD-related variables including exacerbation history and inhaled therapies (short-acting beta-agonists [SABAs], long-acting beta-agonists [LABAs], long-acting muscarinic antagonists [LAMAs], and inhaled corticosteroids [ICSs]). All comorbidities were identified using ICD-10-CM codes documented in the electronic health records one year before the index date. BMI was calculated from the most recent height and weight measurements recorded within 180 days before the index date. Additional details on the categorization and codes used to define the covariates are shown in Table S2.
Outcomes
The primary outcome was all-cause mortality, ascertained from death records in the electronic health records. Secondary outcomes included COPD exacerbations, acute respiratory failure, pneumonia, and MACE (a composite of acute myocardial infarction, stroke, acute heart failure, ventricular arrhythmias, or cardiac arrest) (Table S3).
Statistical Analysis
We used propensity score matching to balance baseline characteristics between the two groups. The propensity score was estimated using a logistic regression model that included all demographic variables and comorbidities as covariates. We performed 1:1 nearest-neighbor matching without replacement using a caliper width of 0.1 of the standard deviation of the logit of the propensity score. Balance between groups after matching was assessed using standardized mean differences (SMDs), with values less than 0.1 indicating adequate balance.
We calculated incidence rates for each outcome. Incidence rates were calculated as the number of events divided by total person-years of follow-up, multiplied by 100. Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional-hazards regression models. The proportional-hazards assumption was assessed using Schoenfeld residuals. Follow-up began on the 90th day after index date and continued until the occurrence of the outcome of interest, death, loss to follow-up, or the end of the study period (November 30, 2025), whichever occurred first.
Sensitivity Analysis
To assess the robustness of our findings, we conducted several sensitivity analyses. First, we performed landmark analyses excluding events occurring within the first month after the index date and censoring follow-up at 1 year, 2 years, and 3 years to assess the consistency of associations over different time periods. Second, we analyzed a negative control outcome (acute appendicitis) to evaluate potential unmeasured confounding or surveillance bias. Third, we calculated E-values to quantify the minimum strength of association that an unmeasured confounder would need to have with both the exposure and outcome to fully explain the observed associations. All statistical tests were two-sided, and p values less than 0.05 were considered to indicate statistical significance. Analyses were performed using the TriNetX platform’s built-in analytics tools.
Subgroup Analysis
Prespecified subgroup analyses were conducted according to sex, age, comorbidity, history of prior COPD exacerbation, type of GLP-1RA, and BMI level. We also performed a subgroup analysis to examine whether the association between GLP-1RA use and the primary outcome varied by individual comparator weight loss medication. To this end, the control group was stratified by specific weight loss medications, including bupropion, topiramate, phentermine, and naltrexone. Separate propensity score–matched cohorts constructed for each comparison.
Results
Patient Selection
Based on the predefined inclusion and exclusion criteria, we identified 50,787 patients with coexisting COPD and obesity who initiated GLP-1RA or other weight loss medications (Figure 1). Of these, 13,133 patients initiated GLP-1RA therapy and 37,654 patients initiated other weight loss medication as control group. After 1:1 propensity score matching, the final analysis included 10,487 patients in each group.
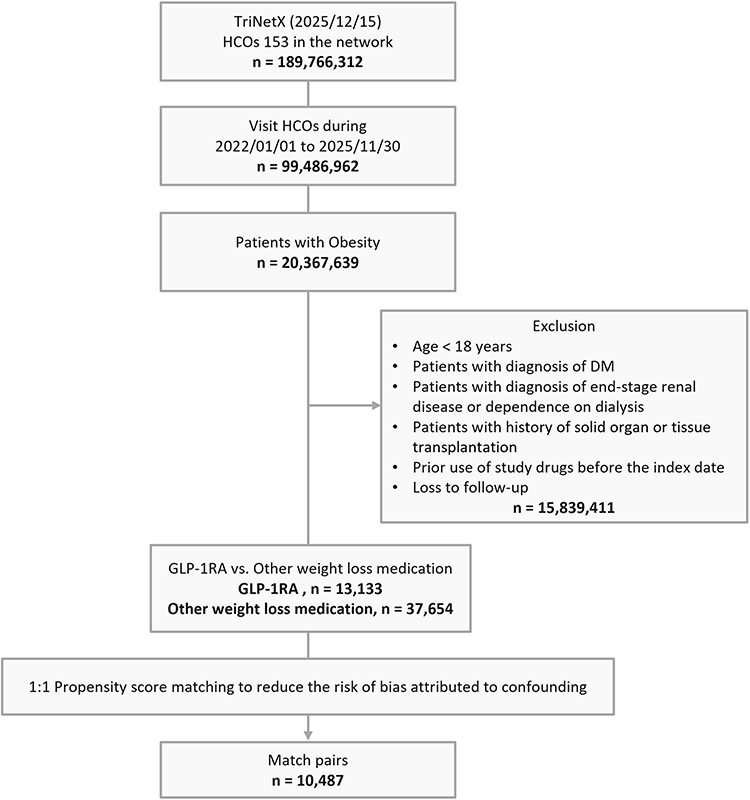 |
Figure 1 Study design and selection flow. Abbreviations: GLP1-RA, glucagon-like peptide-1 receptor agonist; HCO, healthcare organization; MASLD, metabolic dysfunction-associated steatotic liver disease. |
Baseline Characteristics
Before matching, patients in the GLP-1RA group were older (mean age 62.4 vs 59.6 years, SMD 0.253), had higher prevalence of several comorbidities including hypertension (79.3% vs 67.8%, SMD 0.264), hyperlipidemia (59.6% vs 46.3%, SMD 0.269), obstructive sleep apnea (55.1% vs 31.7%, SMD 0.486), ischemic heart disease (41.1% vs 28.9%, SMD 0.257), heart failure (28.7% vs 18.7%, SMD 0.236), diabetes mellitus (12.5% vs 6.0%, SMD 0.225), chronic liver disease (22.7% vs 15.2%, SMD 0.192), atrial fibrillation and flutter (17.8% vs 11.3%, SMD 0.185), chronic kidney disease (16.6% vs 10.5%, SMD 0.178), had lower prevalence of alcohol-related disorders (9.9% vs 13.1%, SMD 0.102), and had higher mean BMI (39.7 vs 35.7 kg/m2, SMD 0.533) compared with the control group (Table 1).
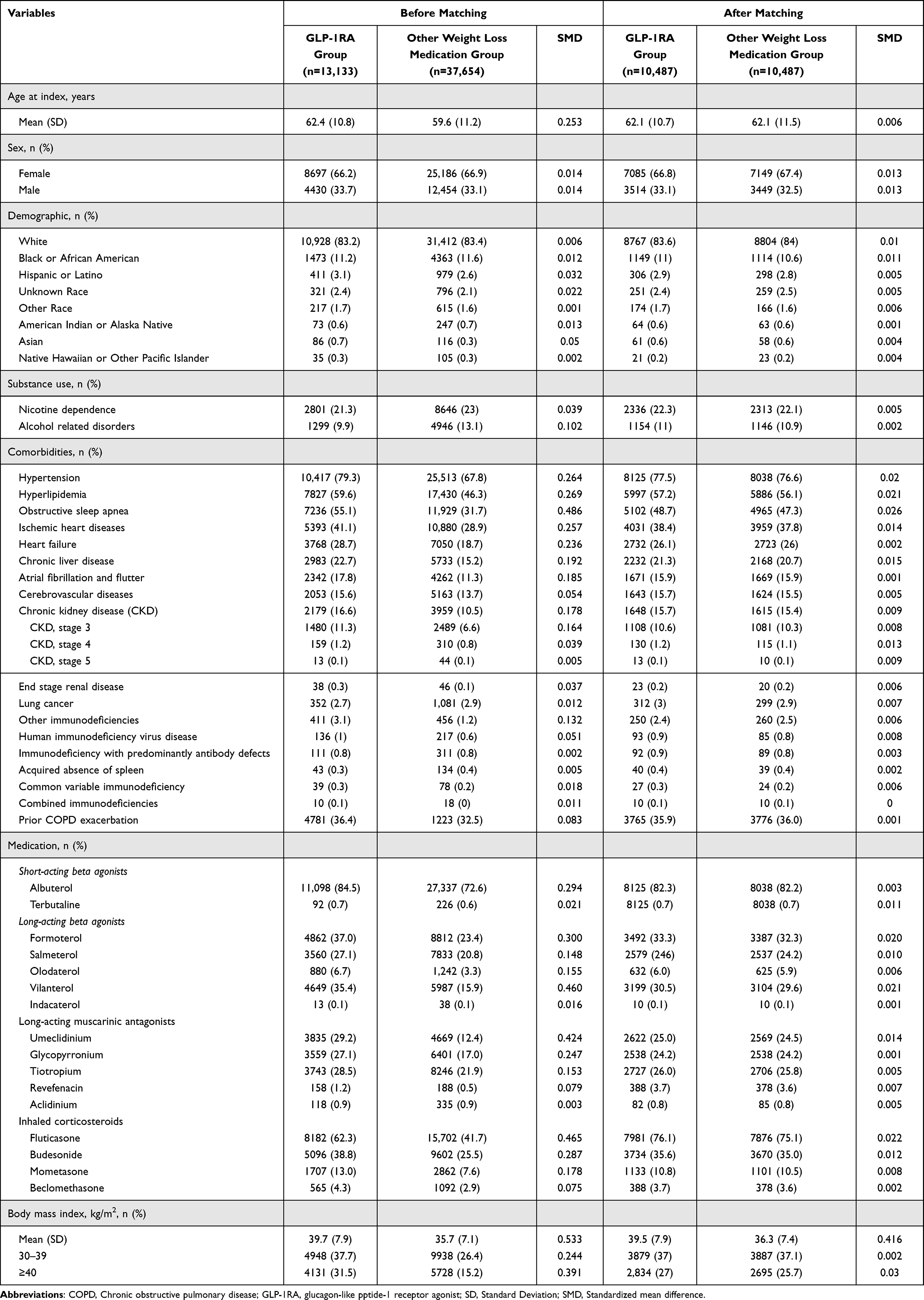 |
Table 1 Baseline Characteristics of Included Subjects Before and After Matching |
After matching, most baseline characteristics were adequately balanced between groups, with the matched cohort having a mean age of 62.1 years and being predominantly female (67%) and White (84%). Most of demographic and clinical features achieved acceptable balance, with SMDs less than 0.1. However, a notable residual imbalance persisted in BMI, with a mean of 39.5 kg/m2 in the GLP-1RA group compared with 36.3 kg/m2 in the control group (SMD = 0.416), indicating that propensity score matching did not fully balance this key clinical variable.
Primary Outcomes
After matching, the median follow-up duration was 530 days (Q1–Q3, 181–880 days) in GLP-1RA group and 467 days (Q1–Q3, 110–824 days) in other weight loss medication group. During the follow-up period, all-cause mortality occurred in 237 patients (0.8 per 100 person-years) in the GLP-1RA group compared with 519 patients (2.2 per 100 person-years) in the control group, corresponding to a 57% lower risk (HR, 0.43; 95% CI, 0.37–0.50; E-value, 4.1; 95% lower confidence limit [LCL], 3.4) (Table 2 and Figure 2).
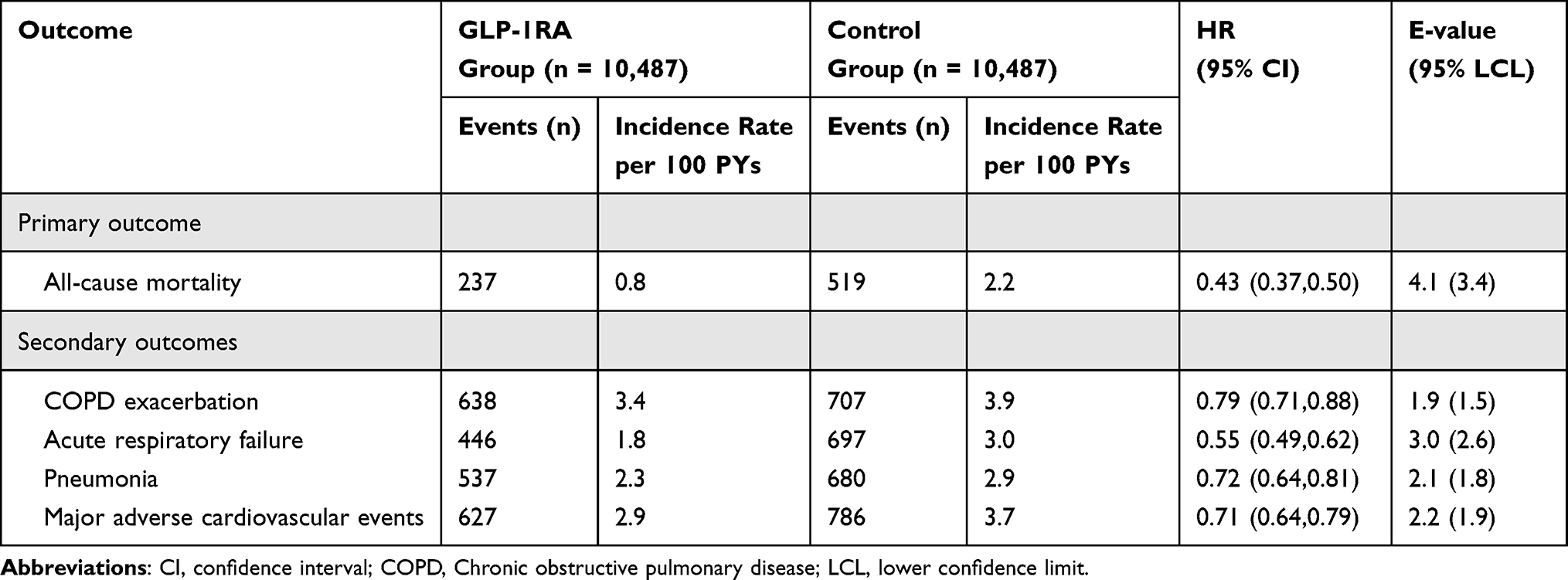 |
Table 2 Hazard Ratio of Outcomes Between the Glucagon-Like Peptide-1 Receptor Agonists (GLP-1 RA) and the Control (Other Weight Loss Medication) Groups |
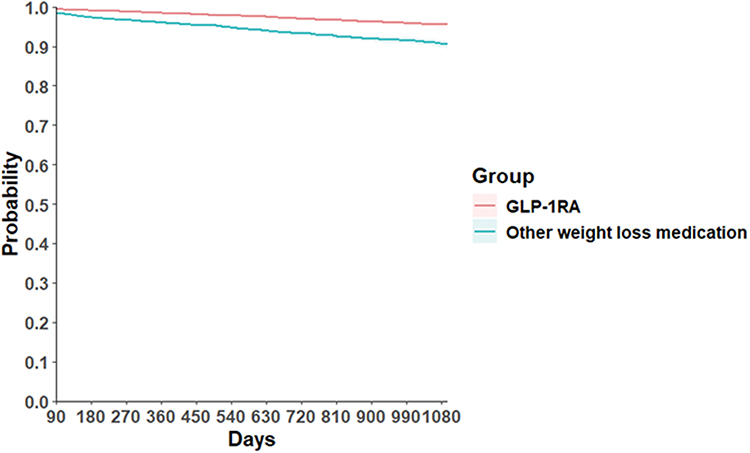 |
Figure 2 Kaplan–Meier curves for time to free of all-cause mortality comparing users of glucagon-like peptide-1 receptor agonists (GLP-1RAs) with users of other weight-loss medication. |
Subgroup analyses demonstrated consistent associations between GLP-1RA use and the lower risk of all-cause mortality across patient demographic and clinical characteristics (Figure 3). The mortality benefit was observed in both age groups (younger than 65 years and 65 years or older), and both sexes. The similar association was observed regardless of BMI category, including among patients with BMI ≥40, 35–40, 30–35, and <30 kg/m2, supporting the robustness of the primary findings despite the residual BMI imbalance after propensity score matching. The similar findings were observed n patients both with and without key comorbidities/conditions, including heart failure, and prior exacerbation. When examining individual GLP-1RA agents, tirzepatide showed the strongest association with a lower risk of mortality (HR, 0.27; 95% CI, 0.19–0.38), followed by semaglutide (HR, 0.44; 95% CI, 0.37–0.52), while liraglutide showed a numerically similar but statistically non-significant trend (HR, 0.66; 95% CI, 0.40–1.08). Subgroup analyses according to individual comparator weight loss medications demonstrated generally consistent associations between GLP-1RA use and all-cause mortality (Table S4). Compared with bupropion users, GLP-1RA users had a significantly lower risk of all-cause mortality (HR, 0.38; 95% CI, 0.33–0.45). Similar associations were observed when compared with topiramate users (HR, 0.51; 95% CI, 0.40–0.64) and phentermine users (HR, 0.65; 95% CI, 0.43–1.00). In contrast, compared with naltrexone users, GLP-1RA use was associated with a numerically lower but statistically non-significant risk of all-cause mortality (HR, 0.72; 95% CI, 0.51–1.03).
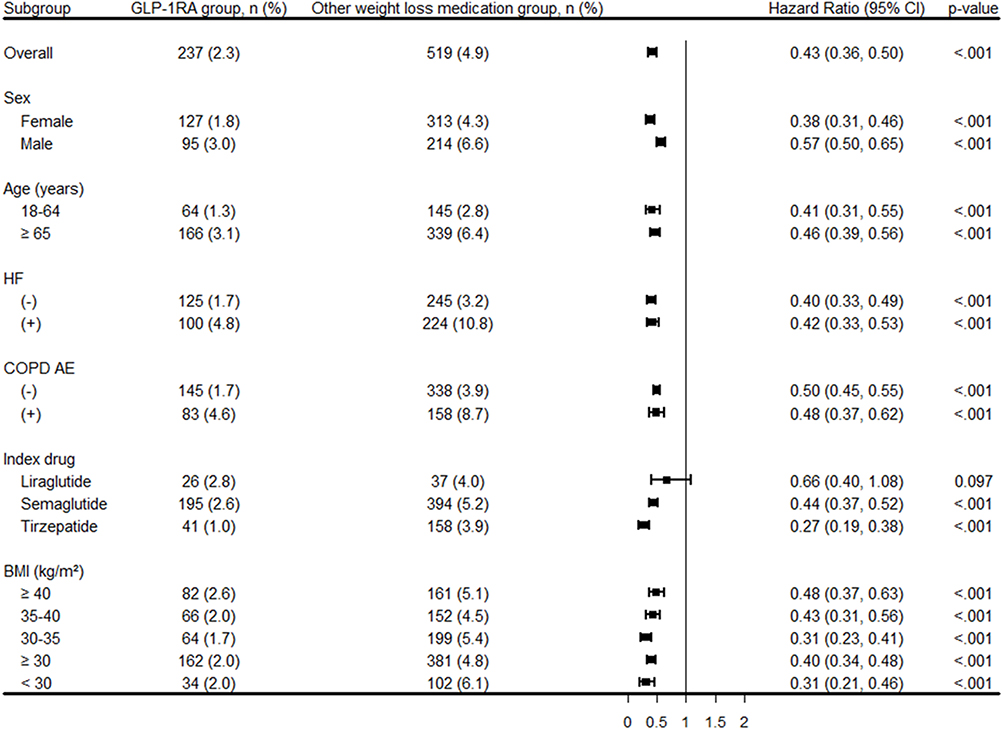 |
Figure 3 Subgroup analysis of the risk of all-cause mortality comparing glucagon-like peptide-1 receptor agonists (GLP-1RAs) with other weight-loss medication. |
Secondary Outcomes
Compared with the control group, the GLP-1RA group was associated with lower risk of COPD exacerbation (HR, 0.79; 95% CI, 0.71–0.88), acute respiratory failure (HR, 0.55; 95% CI, 0.49–0.62), pneumonia (HR, 0.72; 95% CI, 0.64–0.81), and major adverse cardiovascular events (HR, 0.71; 95% CI, 0.64–0.79). The corresponding E-values were 1.9 (95% LCL, 1.5), 3.0 (95% LCL, 2.6), 2.1 (95% LCL, 1.8), and 2.2 (95% LCL, 1.9), respectively (Table 2).
Sensitivity Analyses
Landmark analyses consistently demonstrated robust associations between GLP-1RA use and reduced all-cause mortality (Table S5). The HRs remained stable across different time points: HR 0.38 (95% CI, 0.31–0.46) for 1-month to 1-year follow-up, and HR 0.41 (95% CI, 0.35–0.49) for 1-month to 2-year follow-up. Analysis of negative control outcomes showed no significant association between GLP-1RA use and acute appendicitis (HR, 1.54; 95% CI, 0.81–2.93; P = 0.181), supporting the specificity of our findings (Table S6).
Discussion
This large-scale, real-world comparative effectiveness study involving 10,487 matched pairs of patients with coexisting COPD and obesity revealed significant clinical benefits associated with GLP-1RA use compared with other weight loss medication. GLP-1RA therapy was associated with lower risks of all-cause mortality, COPD exacerbations, acute respiratory failure, pneumonia, and MACE. These associations remained consistent across multiple stratified analysis and sensitivity analyses using landmark approaches at different time points, demonstrating the robustness of our findings. Current management of this population focuses primarily on bronchodilators, corticosteroids, and general lifestyle modifications, yet outcomes remain suboptimal with persistent high rates of exacerbations and mortality. Our findings suggest that GLP-1RAs may offer a disease-modifying approach that extends beyond weight reduction to provide meaningful improvements in respiratory and cardiovascular outcomes.
Our findings align with and extend the emerging body of evidence suggesting respiratory benefits of GLP-1RAs across various patient populations, particularly for those with diabetes. Several large observational studies have demonstrated that GLP-1RA use in patients with T2D reduces the risk of COPD exacerbations.12–15,18,19 A population-based cohort study in the UK by Pradhan et al found that GLP-1RA use was associated with fewer COPD exacerbations compared with other glucose-lowering medications among patients with diabetes.12 Similarly, a recent US study by Ray et al showed that GLP-1RA use was associated with reduced risk of COPD exacerbations compared with DPP-4i in patients with T2D.13 Research in Taiwan by Yen et al demonstrated cardiopulmonary benefits of GLP-1RAs in patients with COPD compared to non-users,14 while Albogami et al reported reduced chronic lower respiratory disease exacerbations among patients with T2D receiving GLP-1RAs versus DPP-4i users.15 In contrast to prior research, our study is the first to specifically focus on patients with coexisting COPD and obesity without requiring concurrent diabetes, addressing a critical knowledge gap. While previous studies12–15,18,19 predominantly examined patients with T2D who also had COPD, our investigation targeted patients with COPD and obesity regardless of diabetic status. This approach provides novel insights into GLP-1RA effects in this previously understudied phenotype, representing a substantial and clinically relevant patient population.
The observed benefits of GLP-1RAs in patients with COPD and obesity likely involve multifactorial mechanisms affecting respiratory and systemic physiology. Weight reduction represents the most apparent pathway. Obesity impairs respiratory mechanics through increased chest wall load, reduced functional residual capacity, and diminished diaphragmatic excursion, exacerbating COPD-related ventilatory limitations.20–22 GLP-1RA-induced weight loss reverses these mechanical disadvantages, improving lung volumes and reducing work of breathing. Supporting this, Altintas Dogan et al demonstrated that 40 weeks of treatment with liraglutide in patients with COPD and obesity improved forced vital capacity and carbon monoxide diffusion capacity.16 Beyond mechanical effects, GLP-1RAs exert anti-inflammatory actions particularly relevant to COPD’s chronic inflammatory state.23 GLP-1 receptors expressed in immune cells mediate reductions in inflammatory cytokines including interleukin-6, tumor necrosis factor-alpha, and C-reactive protein.23–25 In obesity-associated COPD, where metabolic inflammation compounds airway inflammation, these anti-inflammatory effects may reduce exacerbation frequency and severity.26 Additionally, improved insulin sensitivity and reduced visceral adiposity diminish the inflammatory burden of metabolic dysfunction.24,27 Cardiovascular protection likely contributes to mortality reduction. COPD patients face elevated cardiovascular risk, amplified by obesity. GLP-1RAs provide cardioprotective effects including improved endothelial function, reduced atherosclerotic progression, and favorable effects on blood pressure and lipid profiles.9,28,29 The lower risk of MACEs observed in our study demonstrates these mechanisms operate effectively in the COPD-obesity population. The convergence of these mechanical, metabolic, anti-inflammatory, and cardiovascular mechanisms likely explains the substantial clinical benefits observed across multiple outcomes. Further mechanistic studies are needed to elucidate the relative contributions of each pathway and identify potential targets for therapeutic optimization.
This study has several strengths. First, the large sample size of over 20,000 patients drawn from 96 healthcare organizations across a geographically diverse network provides substantial statistical power and enhances generalizability. Second, the active-comparator, new-user design strengthens causal inference by reducing confounding by indication and healthy user bias inherent in comparisons with untreated patients. Third, the consistency of findings across multiple subgroup and sensitivity analyses using landmark approaches at different time points supports the robustness of our results. Fourth, the negative control outcome analysis showing no association with acute appendicitis provides evidence against unmeasured confounding or surveillance bias systematically affecting our findings. Fifth, the calculation of E-values demonstrates that substantial unmeasured confounding would be necessary to explain away the observed associations, particularly for mortality and acute respiratory failure.
However, several limitations warrant consideration. First, as an observational study using real-world data, unmeasured confounding remains possible despite propensity score matching and sensitivity analyses. Factors such as disease severity indicators not fully captured in administrative data, smoking intensity and cessation efforts, exercise capacity, medication adherence, and socioeconomic factors could potentially influence outcomes. Second, the use of diagnostic codes to identify outcomes may introduce misclassification, although these codes generally have reasonable validity for the outcomes examined. Third, we lacked detailed information on dosing regimens, treatment duration, and actual weight loss achieved, limiting our ability to assess dose-response relationships or compare individual agents. Fourth, another notable limitation of the present study is the residual imbalance in BMI between groups following propensity score matching, with a mean BMI of 39.5 kg/m2 in the GLP-1RA group compared with 36.3 kg/m2 in the comparator group (SMD = 0.416). This degree of imbalance is substantial and indicates that propensity score matching did not fully balance this key clinical variable, which may introduce residual confounding. Importantly, given that higher BMI is associated with worse respiratory and cardiovascular outcomes in patients with COPD, this baseline difference would be expected to bias effect estimates against GLP-1RAs - that is, toward the null or toward harm. Accordingly, the observed clinical benefits of GLP-1RAs in our study may represent a conservative estimate of the true treatment effect. To evaluate the potential influence of this imbalance, we conducted BMI-stratified subgroup analyses across five BMI categories (≥40, 35–40, 30–35, ≥30, and <30 kg/m2), and the direction and magnitude of effect estimates remained consistent with the primary analysis across all strata, suggesting that the primary findings were not materially driven by the residual BMI difference between groups. Fifth, the magnitude of the observed effect sizes, particularly for all-cause mortality, is large for an observational database study and should be interpreted with caution. While such effect sizes may partly reflect genuine pharmacological benefits of GLP-1RAs, they may also be influenced by residual confounding, differences in healthcare-seeking behavior, unmeasured channeling bias, or other systematic differences between treatment groups that were not fully addressed by propensity score matching. We acknowledge that the sensitivity analyses conducted, while supportive of the primary findings, do not fully resolve concerns related to cohort definition, comparator heterogeneity, and residual imbalance, and therefore cannot rule out the possibility that bias contributed to the observed associations. These findings should be validated in future randomized controlled trials or studies with more granular clinical data. Sixth, the predominantly White population in our cohort may limit generalizability to other racial and ethnic groups. Finally, the observational nature precludes definitive conclusions about causality, and residual confounding by indication remains a concern.
Conclusion
This large-scale, real-world study demonstrates that GLP-1RA use in patients with coexisting COPD and obesity was associated with lower risks of all-cause mortality, COPD exacerbations, acute respiratory failure, pneumonia, and MACEs compared with other weight loss interventions. The consistency of these findings across multiple subgroup and sensitivity analyses suggests that GLP-1RA benefits extend beyond weight reduction alone to encompass meaningful improvements in both respiratory and cardiovascular outcomes. Given the observational design, however, cautious interpretation is warranted due to potential residual confounding, and validation through adequately powered randomized controlled trials specifically enrolling patients with COPD and obesity remains essential. As the global burden of both COPD and obesity continues to rise, identifying therapies that can simultaneously address both conditions represents a critical clinical priority. This study provides important preliminary evidence suggesting that GLP-1RAs may fulfill this therapeutic need in a vulnerable population with limited effective treatment options.
Statement on AI Assistance
The authors acknowledge the use of Claude (Anthropic) for English language editing and proofreading of this manuscript. The AI tool was used to improve grammar, clarity, and readability of the text. All scientific content, interpretations, and conclusions remain the sole responsibility of the authors.
Availability of Supporting Data
The aggregated datasets used in this study were derived from the TriNetX research platform. In accordance with TriNetX data-sharing policies, only de-identified, aggregated data were accessible for analysis; individual-level patient data were not available to the investigators. Access to the TriNetX database is restricted because it contains protected health information. Researchers who wish to obtain access may submit an application through the TriNetX platform. Approval generally requires verification of research credentials, a clearly defined study objective, and adherence to applicable privacy and data protection regulations. The review and approval process may take several weeks, depending on the applicant’s qualifications and the nature of the research proposal. Additional details regarding data access are available on the TriNetX website (https://trinetx.com) or by contacting TriNetX support at [email protected].
Ethical Approval and Consent to Participate
The Chi Mei Hospital institutional review board approved this TriNetX database study (approval number: 11402-E02) and waived the requirement for informed consent since the research used only aggregated statistical data from de-identified sources.
Acknowledgments
This research was conducted without external funding or financial support, ensuring full independence in study design, data collection, analysis, interpretation, and manuscript preparation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare no competing interests.
References
1. de Oca MM, Perez-Padilla R, Celli B, et al. The global burden of COPD: epidemiology and effect of prevention strategies. Lancet Respir Med. 2025;13(8):709–13. doi:10.1016/S2213-2600(24)00339-4
2. Zewari S, Hadi L, van den Elshout F, et al. Obesity in COPD: comorbidities with Practical Consequences? Copd. 2018;15(5):464–471. doi:10.1080/15412555.2018.1509951
3. Alqarni AA, Badr OI, Aldhahir AM, et al. Obesity prevalence and association with spirometry profiles, ICU admission, and comorbidities among patients with COPD: retrospective study in two tertiary centres in Saudi Arabia. Int J Chron Obstruct Pulmon Dis. 2024;19:111–120. doi:10.2147/COPD.S442851
4. García-Rio F, Soriano JB, Miravitlles M, et al. Impact of obesity on the clinical profile of a population-based sample with chronic obstructive pulmonary disease. PLoS One. 2014;9(8):e105220. doi:10.1371/journal.pone.0105220
5. Lambert AA, Putcha N, Drummond MB, et al. Obesity is associated with increased morbidity in moderate to severe COPD. Chest. 2017;151(1):68–77. doi:10.1016/j.chest.2016.08.1432
6. O’Donnell DE, Ciavaglia CE, Neder JA. When obesity and chronic obstructive pulmonary disease collide. Physiological and clinical consequences. Ann Am Thorac Soc. 2014;11(4):635–644. doi:10.1513/AnnalsATS.201312-438FR
7. Yao H, Zhang A, Li D, et al. Comparative effectiveness of GLP-1 receptor agonists on glycaemic control, body weight, and lipid profile for type 2 diabetes: systematic review and network meta-analysis. BMJ. 2024;384:e076410. doi:10.1136/bmj-2023-076410
8. Klen J, Dolžan V. Glucagon-like peptide-1 receptor agonists in the management of type 2 diabetes mellitus and obesity: the impact of pharmacological properties and genetic factors. Int J Mol Sci. 2022;23(7):3451. doi:10.3390/ijms23073451
9. Ussher JR, Drucker DJ. Glucagon-like peptide 1 receptor agonists: cardiovascular benefits and mechanisms of action. Nat Rev Cardiol. 2023;20(7):463–474. doi:10.1038/s41569-023-00849-3
10. Moiz A, Filion KB, Toutounchi H, et al. Efficacy and safety of glucagon-like peptide-1 receptor agonists for weight loss among adults without diabetes: a systematic review of randomized controlled trials. Ann Intern Med. 2025;178(2):199–217. doi:10.7326/ANNALS-24-01590
11. Zamanian N, Imani H, Talebi S, et al. The efficacy and safety of glucagon-like peptide-1 receptor agonists in non-diabetic adults with overweight/obesity: an umbrella review of systematic reviews and meta-analyses. Eur J Pharmacol. 2025;1003:177966. doi:10.1016/j.ejphar.2025.177966
12. Pradhan R, Lu S, Yin H, et al. Novel antihyperglycaemic drugs and prevention of chronic obstructive pulmonary disease exacerbations among patients with type 2 diabetes: population based cohort study. BMJ. 2022;379:e071380. doi:10.1136/bmj-2022-071380
13. Ray A, Paik JM, Wexler DJ, et al. Glucose-lowering medications and risk of chronic obstructive pulmonary disease exacerbations in patients with type 2 diabetes. JAMA Intern Med. 2025;185(4):399–410. doi:10.1001/jamainternmed.2024.7811
14. Yen FS, Hsu CC, Wei JC, et al. Glucagon-like peptide-1 receptor agonists may benefit cardiopulmonary outcomes in patients with COPD. Thorax. 2024;79(11):1017–1023. doi:10.1136/thorax-2023-221040
15. Albogami Y, Cusi K, Daniels MJ, Wei YJ, Winterstein AG. Glucagon-like peptide 1 receptor agonists and chronic lower respiratory disease exacerbations among patients with type 2 diabetes. Diabetes Care. 2021;44(6):1344–1352. doi:10.2337/dc20-1794
16. Altintas Dogan AD, Hilberg O, Hess S, et al. Respiratory effects of treatment with a glucagon-like peptide-1 receptor agonist in patients suffering from obesity and chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2022;17:405–414. doi:10.2147/COPD.S350133
17. Wilson JL, Betensky M, Udassi S, et al. Leveraging a global, federated, real-world data network to optimize investigator-initiated pediatric clinical trials: the TriNetX pediatric collaboratory network. JAMIA Open. 2024;7(3):ooae077. doi:10.1093/jamiaopen/ooae077
18. Foer D, Strasser ZH, Cui J, et al. Association of GLP-1 receptor agonists with chronic obstructive pulmonary disease exacerbations among patients with type 2 diabetes. Am J Respir Crit Care Med. 2023;208(10):1088–1100. doi:10.1164/rccm.202303-0491OC
19. Meng LC, Chuang HM, Lai HY, et al. Frailty-stratified effectiveness of SGLT2 inhibitors versus DPP-4 inhibitors and GLP-1 receptor agonists on pulmonary outcomes in type 2 diabetes: a nationwide cohort study. EClinicalMedicine. 2025;85:103332. doi:10.1016/j.eclinm.2025.103332
20. Cesanelli L, Cesanelli F, Degens H, Satkunskiene D. Obesity-related reduced spirometry and altered breathing pattern are associated with mechanical disadvantage of the diaphragm. Respir Physiol Neurobiol. 2024;325:104267. doi:10.1016/j.resp.2024.104267
21. Steier J, Lunt A, Hart N, Polkey MI, Moxham J. Observational study of the effect of obesity on lung volumes. Thorax. 2014;69(8):752–759. doi:10.1136/thoraxjnl-2014-205148
22. Rabec C, Janssens JP, Murphy PB. Ventilation in the obese: physiological insights and management. Eur Respir Rev. 2025;34(176):240190. doi:10.1183/16000617.0190-2024
23. Wong CK, Drucker DJ. Antiinflammatory actions of glucagon-like peptide-1-based therapies beyond metabolic benefits. J Clin Invest. 2025;135(21). doi:10.1172/JCI194751
24. Ngabea MA, Dimeji IY. GLP-1 receptor agonists and inflammatory pathway modulation: dual targeting of metabolic and immune dysfunction in insulin resistance. Biochem Biophys Res Commun. 2025;789:152822. doi:10.1016/j.bbrc.2025.152822
25. Huang J, Yi H, Zhao C, et al. Glucagon-like peptide-1 receptor (GLP-1R) signaling ameliorates dysfunctional immunity in COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:3191–3202. doi:10.2147/COPD.S175145
26. Wang W, Mei A, Qian H, et al. The role of glucagon-like peptide-1 receptor agonists in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2023;18:129–137. doi:10.2147/COPD.S393323
27. Szekeres Z, Nagy A, Jahner K, Szabados E. Impact of selected glucagon-like peptide-1 receptor agonists on serum lipids, adipose tissue, and muscle metabolism-a narrative review. Int J Mol Sci. 2024;25(15):8214. doi:10.3390/ijms25158214
28. Mullur N, Morissette A, Morrow NM, Mulvihill EE. GLP-1 receptor agonist-based therapies and cardiovascular risk: a review of mechanisms. J Endocrinol. 2024;263(1). doi:10.1530/JOE-24-0046
29. Battistoni A, Piras L, Tartaglia N, et al. Glucagon-like peptide-1 receptor agonists and the endothelium: molecular and clinical insights into cardiovascular protection. Front Med. 2025;12:1669685. doi:10.3389/fmed.2025.1669685
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of C-Terminal Pro-Endothelin-1 with Mortality in the Population-Based KORA F4 Study
Then C, Sujana C, Herder C, Then H, Heier M, Meisinger C, Peters A, Koenig W, Rathmann W, Maalmi H, Ritzel K, Roden M, Stumvoll M, Thorand B, Seissler J
Vascular Health and Risk Management 2022, 18:335-346
Published Date: 3 May 2022
Short-Term Oxygen Therapy Outcomes in COPD
Soumagne T, Maltais F, Corbeil F, Paradis B, Baltzan M, Simão P, Abad Fernández A, Lecours R, Bernard S, Lacasse Y
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1685-1693
Published Date: 28 July 2022
The Association of Renin-Angiotensin System Blockades and Mortality in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Acute Respiratory Failure: A Retrospective Cohort Study
Ruan Z, Li D, Hu Y, Qiu Z, Chen X
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2001-2011
Published Date: 1 September 2022
Patients with Chronic Obstructive Pulmonary Disease and Evidence of Eosinophilic Inflammation Experience Exacerbations Despite Receiving Maximal Inhaled Maintenance Therapy
Chen S, Miravitlles M, Rhee CK, Pavord ID, Jones R, Carter V, Emmanuel B, Alacqua M, Price DB
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2187-2200
Published Date: 9 September 2022
COPD Exacerbations, Costs, and Health Care Resource Utilization Before and After Initiation of Fluticasone Furoate/Umeclidinium/Vilanterol in Routine Care in the USA
Hanania NA, Bunner SH, Bengtson LGS, Ismaila AS, Bogart M
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:407-418
Published Date: 24 March 2023