")
Back to Journals » Vascular Health and Risk Management » Volume 18
Association of C-Terminal Pro-Endothelin-1 with Mortality in the Population-Based KORA F4 Study
Authors Then C , Sujana C , Herder C , Then H , Heier M, Meisinger C, Peters A, Koenig W, Rathmann W, Maalmi H, Ritzel K, Roden M, Stumvoll M, Thorand B, Seissler J
Received 26 February 2022
Accepted for publication 22 April 2022
Published 3 May 2022 Volume 2022:18 Pages 335—346
DOI https://doi.org/10.2147/VHRM.S363814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Daniel Duprez
Cornelia Then,1,2 Chaterina Sujana,2– 4 Christian Herder,5– 7 Holger Then,8 Margit Heier,3,9 Christa Meisinger,10,11 Annette Peters,3,12 Wolfgang Koenig,12– 14 Wolfgang Rathmann,5,15 Haifa Maalmi,5,7 Katrin Ritzel,1 Michael Roden,5– 7 Michael Stumvoll,16 Barbara Thorand,2,3 Jochen Seissler1,2
1Department of Internal Medicine IV, University Hospital of Ludwigs-Maximilians-University Munich, Munich, Germany; 2German Center for Diabetes Research (DZD), Partner Munich-Neuherberg, Munich, Germany; 3Institute of Epidemiology, Helmholtz Zentrum Munich – German Research Center for Environmental Health (GmbH), Neuherberg, Germany; 4Institute for Medical Information Processing, Biometry, and Epidemiology, Pettenkofer School of Public Health, Ludwigs-Maximilians-University Munich, Munich, Germany; 5German Center for Diabetes Research (DZD), Munich, Germany; 6Department of Endocrinology and Diabetology, Medical Faculty and University Hospital of the Heinrich-Heine-University Düsseldorf, Düsseldorf, Germany; 7Institute of Clinical Diabetology, German Diabetes Center, Leibniz Center for Diabetes Research at Heinrich-Heine-University Düsseldorf, Düsseldorf, Germany; 8Freie Waldorfschule Augsburg, Augsburg, Germany; 9KORA Study Centre, University Hospital Augsburg, Augsburg, Germany; 10Independent Research Group Clinical Epidemiology, Helmholtz Zentrum Munich – German Research Center for Environmental Health (GmbH), Neuherberg, Germany; 11Chair of Epidemiology, University Hospital Augsburg, Augsburg, Germany; 12DZHK (German Centre for Cardiovascular Research), Partner Site Munich Heart Alliance, Munich, Germany; 13Institute of Epidemiology and Medical Biometry, University of Ulm, Ulm, Germany; 14German Heart Center Munich, Technical University of Munich, Munich, Germany; 15Institute of Biometrics and Epidemiology, German Diabetes Center, Leibniz Institute at Heinrich-Heine-University Düsseldorf, Düsseldorf, Germany; 16Department of Medicine, University of Leipzig, Leipzig, Germany
Correspondence: Cornelia Then, Medizinische Klinik und Poliklinik IV - Klinikum der Ludwig-Maximilians-Universität, Ziemssenstraße 1, München, 80336, Germany, Tel +4989440052111, Fax +4989440054956, Email [email protected]
Introduction: Endothelin-1 and its prohormone C-terminal pro-endothelin-1 (CT-proET-1) have been linked to metabolic alterations, inflammatory responses and cardiovascular events in selected study populations. We analyzed the association of CT-proET-1 with cardiovascular events and mortality, carotid intima-media-thickness as surrogate for early atherosclerotic lesions, biomarkers of subclinical inflammation and adipokines in a population-based study.
Methods: The cross-sectional and prospective analyses used data from the KORA F4 study with a median follow-up time of 9.1 (8.8– 9.4) years. Data on CT-proET-1 and mortality were available for 1554 participants, data on the other outcomes in subgroups (n = 596– 1554). The associations were estimated using multivariable linear regression and Cox proportional hazard models adjusted for sex, age, body mass index, estimated glomerular filtration rate, arterial hypertension, diabetes, low-density and high-density lipoprotein cholesterol, current and former smoking and physical activity. The Bonferroni method was used to correct for multiple testing.
Results: In the fully adjusted model, CT-proET-1 was associated with cardiovascular (hazard ratio (HR) per standard deviation increase: 1.66; 95% confidence interval (CI): 1.10– 2.51; p = 0.017) and all-cause mortality (HR: 2.03; 95% CI 1.55– 2.67; p < 0.001), but not with cardiovascular events, and was inversely associated with the intima-media thickness (β: − 0.09 ± 0.03; p = 0.001). CT-proET-1 was positively associated with five out of ten biomarkers of subclinical inflammation and with two out of five adipokines after correction for multiple testing. After inclusion of biomarkers of subclinical inflammation in the Cox proportional hazard model, the association of CT-proET-1 with all-cause mortality persisted (p < 0.001).
Conclusion: These results emphasize the complexity of endothelin-1 actions and/or indicator functions of CT-proET-1. CT-proET-1 is a risk marker for all-cause mortality, which is likely independent of vascular endothelin-1 actions, cardiovascular disease and inflammation.
Keywords: endothelin, CT-proET-1, mortality, cardiovascular events, subclinical inflammation, intima-media thickness
Introduction
Endothelin-1 (ET-1) is a vasoactive 21-amino acid peptide secreted by vascular endothelium smooth vascular muscle cells, epicardial cells and renal cells. ET-1 acts via different endothelin receptors (ETR) and mediates vasoconstrictive effects by targeting endothelial cells and vascular smooth muscle cells via ETRA.1 ET-1 targets capillary and arterial endothelial cells, potentially inducing pulmonary hypertension and systemic vasoconstriction.2 In contrast, ETRB mediates vascular smooth muscle relaxation and vasodilation via the release of prostaglandins and nitric oxide.3 Further ETRB effects include natriuresis4 and direct metabolic effects.5
ET-1 is instable and rapidly cleared from the circulation, preventing reliable measurements. Therefore, more recently, its prohormone C-terminal pro-endothelin-1 (CT-proET-1), which is cleaved from the respective precursor protein and secreted in equimolar concentrations, is used as a stable surrogate parameter.6
Due to vasoconstrictive and pro-inflammatory properties, ET-1 putatively plays a causal role in metabolic disturbances, atherosclerosis, cardiovascular events and mortality. ET-1 or its surrogate CT-proET-1 were associated with the metabolic syndrome and impaired glucose tolerance in the general population,7,8 and with increased inflammation, cardiovascular disease and mortality in studies involving critically ill patients,9 participants with heart failure,10,11 acute myocardial infarction12–14 and chronic kidney disease.15 However, these results were not confirmed by all studies,16–19 and the association of CT-proET-1 with cardiovascular events, mortality and (subclinical) inflammation is less well studied in the general population.
The aim of the current study was to investigate the association of CT-proET-1 with cardiovascular events and mortality, carotid intima-media-thickness (IMT) as surrogate for early atherosclerotic lesions, biomarkers of subclinical inflammation and adipokines in a large population-based cohort. We further examined whether biomarkers of subclinical inflammation confounded the association of CT-proET-1 with mortality.
Methods
Study Cohort and Definition of Variables
The KORA (Cooperative Health Research in the Region of Augsburg) F4 (2006–2008) study is a follow-up examination of the population-based KORA S4 study (1999–2001). The study was approved by the Ethics Committees of the Bavarian Medical Association (approval number 06068) in adherence to the declaration of Helsinki. All participants gave written informed consent. Recruitment and eligibility criteria for the KORA studies, study design, standardized sampling methods and data collection (medical history, medication, anthropometric and blood pressure measurements) have been described in detail elsewhere.20,21
CT-proET-1 was measured in the first consecutive 1596 participants of the KORA F4 study (out of a total of 3080 participants). All variables necessary for the analysis of the association of CT-proET-1 with mortality were available in 1554 participants. Measurements of white blood cell count and high-sensitivity C-reactive protein (hsCRP) were available in 1552 participants; leptin and retinol-binding protein-4 (RBP-4) in 1547 participants; chemerin, progranulin and vaspin in 1055 participants; interleukin-6 (IL-6), tumor necrosis factor-α (TNF-α), interleukin-18 (IL-18), soluble intercellular adhesion molecule-1 (sICAM-1), myeloperoxidase (MPO), superoxide dismutase-3 (SOD-3), interleukin-22 (IL-22) and interleukin-1 receptor antagonist (IL-1RA) were available in 596 participants aged ≥ 62 years.
The outcomes all-cause and cardiovascular mortality (ICD-9 codes 390–459 and 798) were ascertained by regularly checking the status of the participants through the population registries until 2016. Death certificates were obtained from the local health authorities. The median (1st; 3rd quartile) follow-up time was 9.1 (8.8; 9.4) years. Myocardial infarction and stroke at baseline were self-reported diagnoses. Incident myocardial infarction occurring until the age of 74 years (for cases occurring before 2009) and until the age of 84 years (for cases occurring since 2009) was assessed by surveillance through the local myocardial infarction registry. Incident non-fatal myocardial infarction occurring in participants >74 and > 84 years, respectively, depending on the year of occurrence, or residing outside the study area as well as non-fatal stroke were assessed by postal follow-up questionnaires. All self-reported incident stroke cases and myocardial infarction cases occurring outside the study area or in persons > 74 or 84 years (depending on the year of occurrence) and the date of diagnosis were validated using data from participants’ hospital records and their attending physicians. Stroke and myocardial infarction were pooled to a combined endpoint with only the first event taken into account in case of several events. Participants with prevalent stroke (n = 34) or prevalent myocardial infarction (n = 52) or missing data on incident stroke and myocardial infarction (n = 84) were excluded from the analyses regarding the outcome of incident stroke or myocardial infarction. The follow-up time (median (1st quartile; 3rd quartile)) was 8.6 (8.1; 9.0) years for incident stroke/myocardial infarction.
Criteria for diabetes mellitus were a validated medical diagnosis or current self-reported use of glucose-lowering agents. Participants without clinically diagnosed diabetes underwent a standard 75 g oral glucose tolerance test. Newly diagnosed diabetes was defined according to the World Health Organization diagnostic criteria (≥ 7.0 mmol/l fasting and/or ≥ 11.1 mmol/l 2-h glucose). Participants with a diabetes type other than type 2 or unknown glucose tolerance status (n = 25) were excluded from the analyses.
Arterial hypertension was defined as a systolic blood pressure ≥ 140 mmHg and/or a diastolic blood pressure ≥ 90 mmHg, and/or intake of anti-hypertensive medication, given that the participants were aware of being hypertensive.
Leisure-time physical activity was assessed with two separate questions concerning leisure time sports activity in winter and in summer (cycling included). Possible answers were (i) > 2 hours, (ii) 1–2 hours, (iii) < 1 hour and (iv) none per week. Participants who had a total score < 5, obtained by summing the numbers (i)-(iv) from the winter and summer questions, were classified as “physically active”.
Biochemical Measurements
Blood samples were collected after an overnight fast of at least eight hours. Plasma was separated immediately, serum after 30 min. Plasma and serum samples were assayed immediately or stored at −80°C. Plasma CT-proET-1 was measured by sandwich fluoro-immunoassay (BRAHMS, Hennigsdorf, Berlin, Germany) on an automated BRAHMS KRYPTOR system as previously described.8 The intra- and inter-assay coefficients of variation for CT-proET-1 were 4.8 and 6.9%. Serum creatinine was assayed with a modified Jaffe test (Krea Flex; Dade Behring, Deerfield, IL, USA). Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (2009) based on serum creatinine.22 Glucose levels were measured in serum using a hexokinase method (GLUFlex, Dade Behring). HbA1c was measured in hemolyzed whole blood using the cation-exchange high performance liquid chromatographic, photometric VARIANT II TURBO HbA1c Kit - 2.0 assay on a VARIANT II TURBO Hemoglobin Testing System (Bio-Rad Laboratories Inc., Hercules, USA). Plasma hsCRP was measured with a high-sensitivity latex-enhanced nephelometric assay on a BN II analyzer (Siemens, Erlangen, Germany). Serum levels of IL-6 and TNF-α were measured with Quantikine HS ELISA kits, IL-22, IL-1RA and sICAM-1 with Quantikine ELISA kits (R&D Systems, Wiesbaden, Germany).23–25 Serum levels of IL-18 were assayed using ELISA kits from MBL (Nagoya, Japan). Serum MPO concentrations were measured using the Human Myeloperoxidase Quantikine ELISA (R&D Systems, Wiesbaden, Germany). Serum SOD-3 concentrations were measured with an ELISA from Cloud‐Clone Corp. (Houston, TX, USA).26 Intra-assay coefficients of variation for hsCRP, IL-1RA, IL-22, sICAM-1, IL-6, TNF-α, IL-18, MPO and SOD-3 were 2.7, 2.8, 5.5, 3.5, 7.2, 6.3, 7.6, 3.2 and 7.1%, respectively. Interassay coefficients were 6.3, 7.0, 9.3, 6.4, 11.8, 14.4, 9.4, 5.6 and 7.1%, respectively. For IL-22, 204 (34%) of the sera yielded values below the limit of detection (LOD; 3.9 pg/mL). Values below LOD were assumed to be evenly distributed between 0 and LOD and were assigned a value of 0.5 × LOD. Leptin was measured by ELISA (Mercodia, Uppsala, Sweden) with intra‐ and inter‐assay coefficients of variation of < 10%. RBP-4 were measured by immunonephelometry using a BN II analyzer. Chemerin serum concentrations were measured using a commercially available ELISA kit (Human Chemerin ELISA, Biovendor, Heidelberg, Germany) with a sensitivity of 0.1 ng/mL and intra- and inter-assay coefficients of variation of 6.0% and 7.6%.27 Progranulin serum concentrations were analyzed using the Progranulin human ELISA Kit AdipoGen from AdipoGen (Seoul, Korea).27 Serum vaspin concentrations were quantified using a commercial enzyme-linked immunosorbent assay kit (AdipoGen) with a sensitivity of 12 pg/mL. The intra- and inter-assay coefficients of variation were 1.3–3.8% and 3.3–9.1%, respectively.27
Measurement of IMT
Ultrasound measurement (Sonoline G, 10-MHz transducer; Siemens Medical Solutions, Munich, Germany) of both common carotid arteries (CCA) was performed using a validated protocol28 as previously described.29 The average of the measurements of 3 frozen images from both the left and right CCA were used to calculate artery thickness of the distal CCA ((mean left + mean right)/2). One certified reader measured all IMT scans. Reproducibility studies for intersonographer (n = 30 IMT measurements) and inter-reader variability (n = 50 IMT measurements) revealed coefficients of variations of 1.9% and 3.0% with Spearman correlation coefficients of ≥ 0.89.
Statistical Analysis
Characteristics of the study participants were compared between survivors and non-survivors using t-tests in case of approximately normally distributed variables. Mann–Whitney U-tests were performed for variables with skewed distributions. Binomial proportions were compared with Chi-square tests. The associations of CT-proET-1 with all-cause and cardiovascular mortality were examined using Cox proportional hazard models. The cross-sectional associations of CT-proET-1 with IMT, biomarkers of subclinical inflammation, adipokines and with traditional cardiovascular risk factors were assessed using linear regression models. Categorical cardiovascular risk factors were analyzed with logistic regression models. Continuous variables were transformed to approach Gaussian distribution by the probability integral transformation followed by an inverse transform sampling and were used in calculations per one standard deviation. The associations of CT-proET-1 with the respective outcomes were examined in models without adjustments (Model 1) and with adjustments for the covariates sex, age, BMI, type 2 diabetes, hypertension, eGFR (continuous), LDL cholesterol (continuous), HDL cholesterol (continuous), physical activity (active/inactive), current smoking and former smoking (Model 2). For further analyses, models adjusted for IL-6 and sICAM-1 were calculated. Participants with missing data were excluded from the respective adjusted and crude analyses. The level of statistical significance was set at 5% (two-sided). The Bonferroni method was used to correct for multiple testing when appropriate. The calculations were performed using the statistical environment R, version 3.6.0 (R Development Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing; 2019).
Results
Clinical Characteristics of the Study Participants
Clinical characteristics of the study participants are shown in Table 1. CT-proET-1 was higher in non-survivors compared to survivors (Supplementary Figure 1).
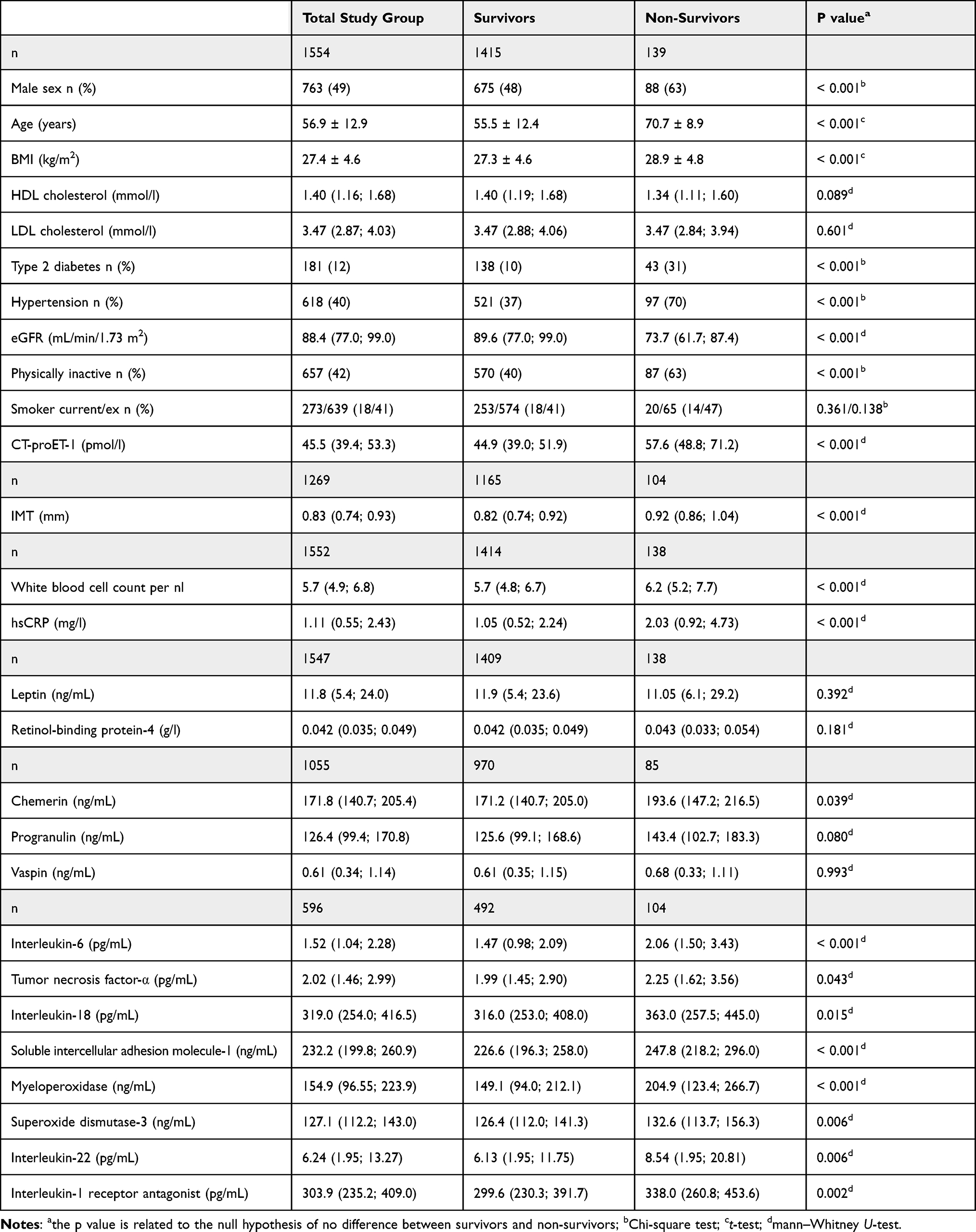 |
Table 1 Characteristics of the Study Participants at KOFA F4 Overall and Stratified by Survival Status (Mean ± Standard Deviation, Median (First Quartile; Third Quartile), or Number of Participants (Proportion in %)) |
Association of CT-proET-1 with Cardiovascular Risk Factors
CT-proET-1 was significantly positively associated with sex, age, BMI, type 2 diabetes, arterial hypertension, active and former smoking, and was inversely associated with LDL and HDL cholesterol, eGFR and physical activity. The strongest associations were observed with age, BMI, type 2 diabetes and inversely with the eGFR (Table 2). Scatterplots of CT-proET-1 in relation to age, BMI and eGFR are shown in Supplementary Figure 2.
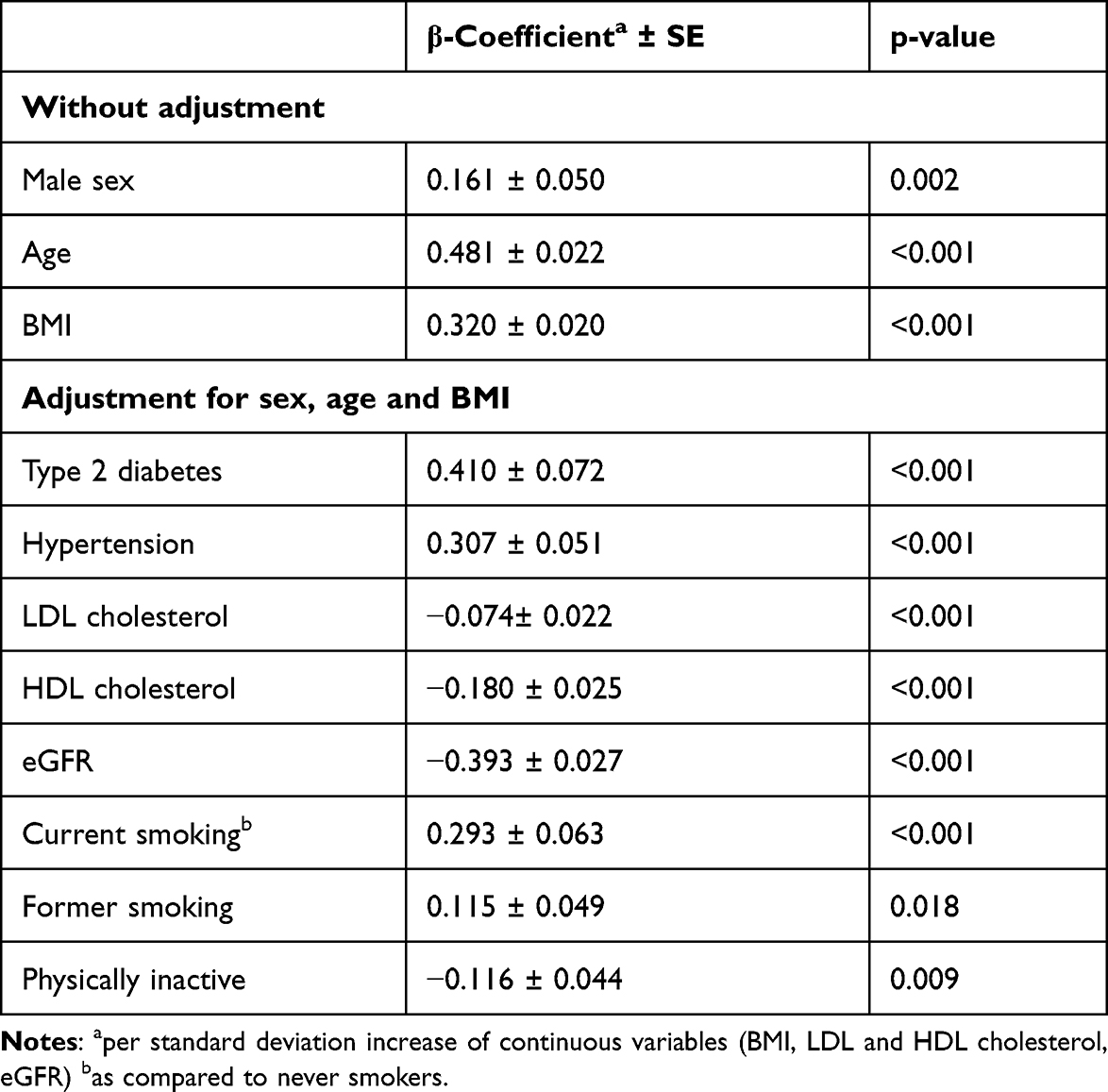 |
Table 2 Association of CT-proET-1 (as Dependent Variable) with Metabolic and Cardiovascular Risk Factors (as Independent Variables) |
Association of CT-proET-1 with Cardiovascular Complications and Mortality
CT-proET-1 was associated with stroke, myocardial infarction, the combined outcome of stroke and myocardial infarction, and with cardiovascular and all-cause mortality in the unadjusted model (Model 1).
After multivariable adjustment (Model 2), CT-proET-1 was no longer significantly associated with non-fatal or fatal stroke, non-fatal or fatal myocardial infarction or the combined endpoint of both outcomes (Table 3).
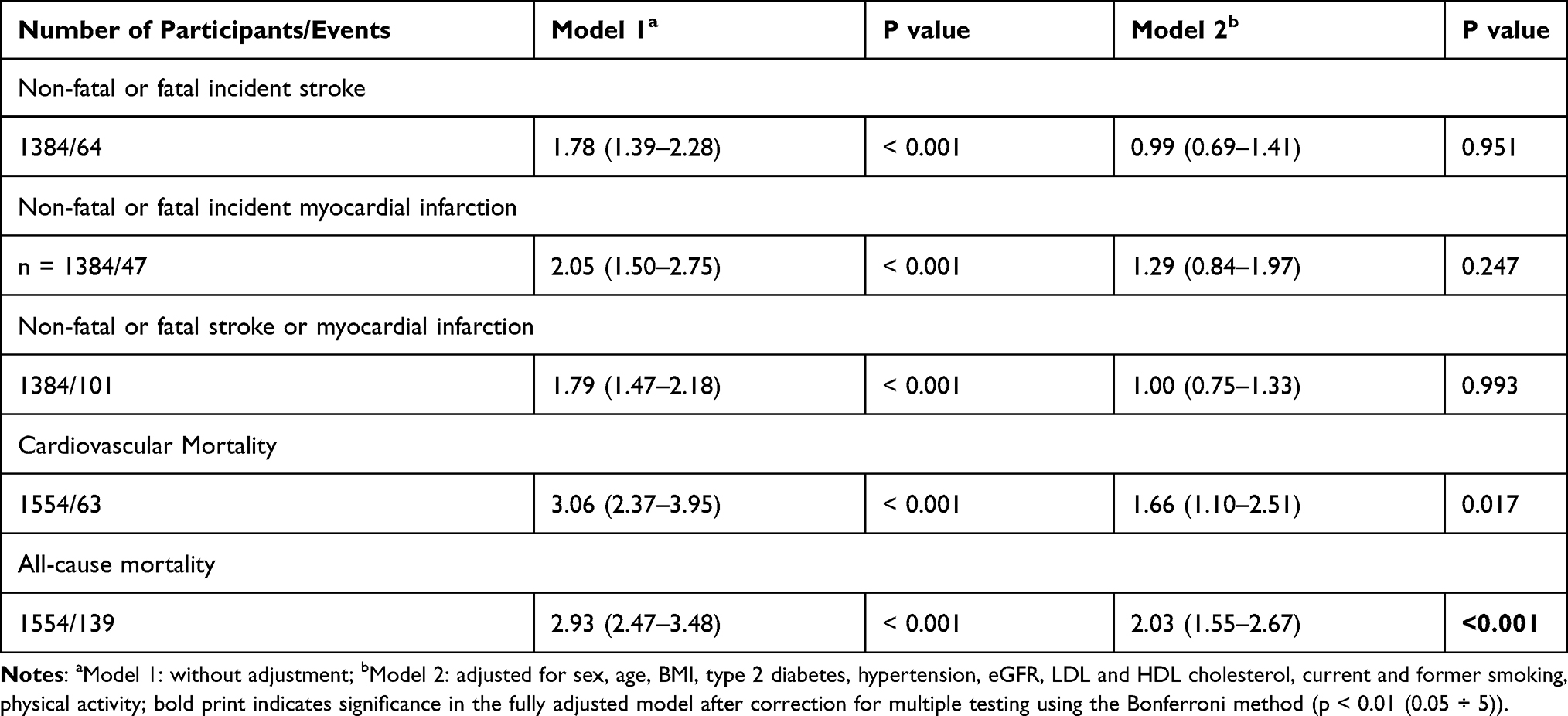 |
Table 3 Hazard Ratios (95% Confidence Interval) of the Association Between CT-proET-1 (per Standard Deviation) with Cardiovascular Outcomes and All-Cause Mortality |
CT-proET-1 was associated with cardiovascular mortality (HR per standard deviation: 1.66; 95% CI: 1.10–2.51; p = 0.017) and all-cause mortality (HR: 2.03; 95% CI: 1.55–2.67; p < 0.001) in the fully adjusted model. However, only the association with all-cause mortality met the corrected significance threshold (Table 3). Additional adjustment for stroke and myocardial infarction did not further attenuate the association of CT-proET-1 with cardiovascular mortality (HR: 1.70; 95% CI: 1.12–2.57; p = 0.013) and all-cause mortality (HR: 2.06; 95% CI: 1.57–2.71; p < 0.001).
Inverse Association of CT-proET-1 with IMT
In the crude model, CT-proET-1 was positively associated with the IMT (β per standard deviation: 0.29 ± 0.03; p < 0.001). Adjustment for age alone strongly attenuated this association (β: 0.005 ± 0.02; p = 0.83). After multivariable adjustment according to Model 2 (sex, age, BMI, type 2 diabetes, hypertension, eGFR, LDL and HDL cholesterol, current and former smoking, physical activity), the association between CT-proET-1 and IMT became inverse (β: −0.09 ± 0.03; p = 0.001).
Association of CT-proET-1 with Biomarkers of Subclinical Inflammation and Adipokines
CT-proET-1 was positively associated with the pro-inflammatory markers hsCRP, IL-6, TNF-α, IL-18, sICAM-1, MPO and with the anti-inflammatory marker IL-22. After correction for multiple testing, CT-proET-1 was still significantly associated with IL-6, TNF-α, IL-18, sICAM-1 and IL-22. No significant association was observed with white blood cell count and the anti-inflammatory markers SOD-3 and IL-1ra (Table 4).
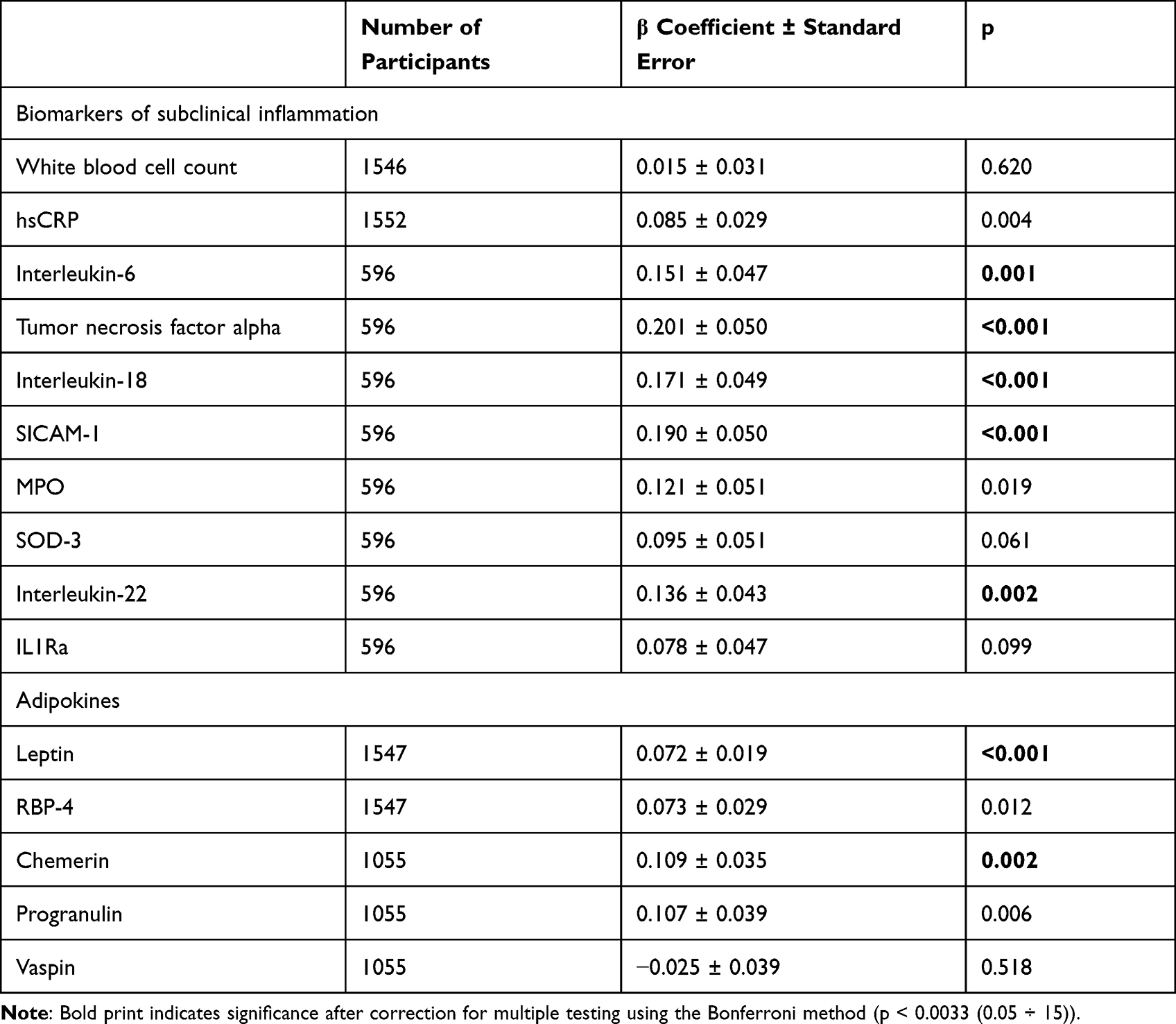 |
Table 4 Association of CT-proET-1 (per Standard Deviation) with Biomarkers of Subclinical Inflammation (per Standard Deviation): β Coefficients ± Standard Error from Linear Regression Models Adjusted for Sex, Age, BMI, eGFR, Hypertension, Type 2 Diabetes, LDL and HDL Cholesterol, Current and Former Smoking, Physical Activity (Model 2) |
Regarding adipokines, CT-proET-1 was significantly associated with the primarily pro-inflammatory adipokines leptin and chemerin after correction for multiple testing. The association with RBP-4 and the anti-inflammatory progranulin did not meet the corrected significance threshold. The anti-inflammatory vaspin was not significantly associated with CT-proET-1 (Table 4).
Exemplary scatterplots of CT-proET-1 in relation to IL-6, TNF-α, sICAM-1, leptin and chemerin are given in Supplementary Figure 2.
Among the biomarkers of subclinical inflammation and adipokines that were associated with CT-proET-1, only IL-6 and sICAM-1 were significantly associated with all-cause mortality after adjustment for sex and age (p < 0.001 for both). We included IL-6 and sICAM-1 in the unadjusted model (Model 1) and in the fully adjusted model (Model 2) of the association of CT-proET-1 with all-cause mortality and found that the association in Model 2 was modestly attenuated but remained significant. The attenuation was more pronounced when adding both markers to Model 2. Remarkably, adjustment for IL-6 alone in the otherwise unadjusted model resulted in a stronger attenuation as compared to full adjustment for traditional cardiovascular risk factors (Model 2; Table 5).
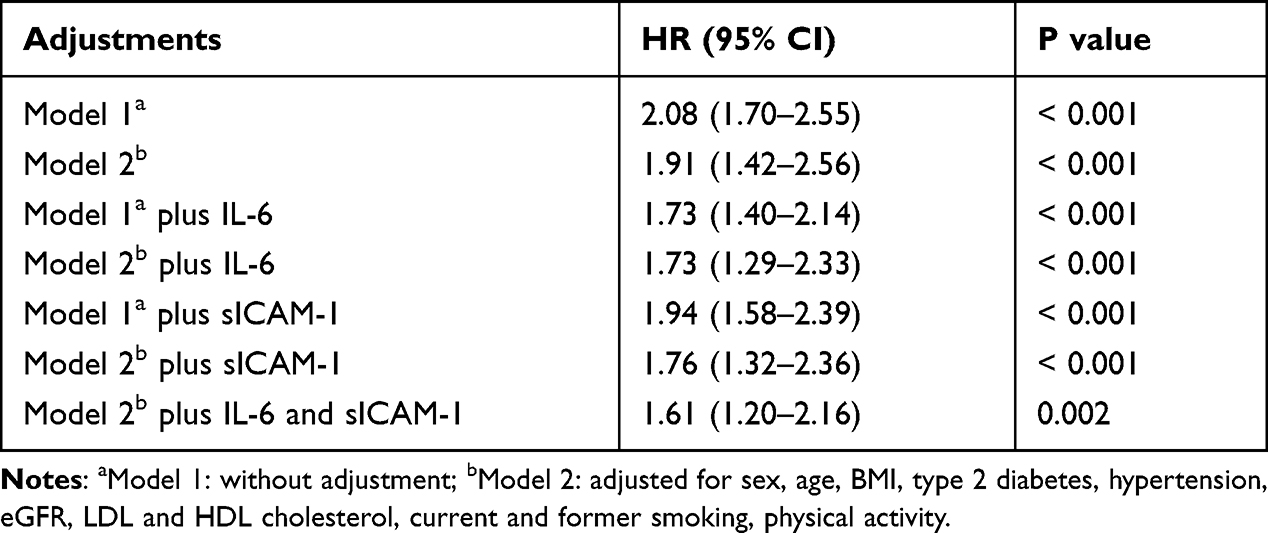 |
Table 5 Hazard Ratios (95% Confidence Interval) of the Association Between CT-proET-1 (per Standard Deviation) and All-Cause Mortality Adjusted for IL-6 and sICAM-1, Respectively. N = 596, Events = 104 |
Discussion
In the KORA F4 study, CT-proET-1 was associated with cardiovascular risk factors, all-cause mortality, biomarkers of subclinical inflammation and adipokines, but not with cardiovascular events. CT-proET-1 was inversely associated with IMT after multivariable adjustment.
Association of CT-proET-1 with Mortality
CT-proET-1 was associated with cardiovascular and all-cause mortality. The associations were largely independent of traditional cardiovascular risk factors. The association of CT-proET-1 with all-cause mortality was also largely independent of selected biomarkers of subclinical inflammation. The literature describes an association of ET-1/CT-proET-1 with cardiovascular and/or all-cause mortality in studies mostly including participants with high cardiovascular risk. In patients with acute myocardial infarction, CT-proET-1 offered additional prognostic information regarding mortality,12,13 and higher ET-1 was a predictor of a combined endpoint of major adverse clinical outcomes and mortality.14 Similarly, CT-proET-1 improved the risk stratification for mortality after acute ischemic stroke.30 In patients with systolic heart failure, CT-proET-1 was associated with adverse outcomes including mortality.10,11 Regarding population-based studies, CT-proET-1 was recently shown to be associated with all-cause mortality in a Swedish population.31
However, other studies showed no association of ET-1/CT-proET-1 with adverse outcomes after ischemic stroke,16 in patients on hemodialysis17 and in patients with heart failure,19 or even an inverse association of CT-proET-1 with mortality in heart failure patients,32 emphasizing the heterogeneity of the literature regarding the association of ET-1/CT-proET-1 with mortality.
In the present study, we observed no significant association between CT-proET-1 and incidence of cardiovascular events after adjustment for cardiovascular risk factors. Our study had a relatively low number of incident cardiovascular events and therefore may not be sufficiently powered to detect significant associations. However, regarding stroke and the combined endpoint, the hazard ratios were 0.99 and 1.00, indicating no association with CT-proET-1 in our study.
Previous studies on an association of ET-1/CT-proET-1 with prevalent cardiovascular disease and incident cardiovascular events were again mainly performed in high-risk populations and yielded mixed results. In a cross-sectional analysis of 961 older participants, ET-1 was associated with prevalent coronary heart disease in women, but in men only when aged > 75 years.33 In patients with type 2 diabetes, CT-proET-1 was associated with cardiovascular events and all-cause mortality in one study.34 However, in another study involving 781 patients with type 2 diabetes, CT-proET-1 was not an independent predictor for fatal/non-fatal cardiovascular events.18 In a study including participants referred for coronary angiography, ET-1 was not associated with the presence or severity of coronary artery disease, but with all-cause mortality.35 Thus, further studies with a larger sample size are needed to examine the association between CT-proET-1 with cardiovascular events.
Inverse Association of CT-proET-1 with IMT After Adjustment for Cardiovascular Risk Factors
In the current study, CT-proET-1 was positively associated with IMT in the crude model, but inversely after multivariable adjustment, which is an unexpected finding at a first glance. Previous data on the association of ET-1 or CT-proET-1 with IMT or intima-media thickness of peripheral arteries were mainly derived from small, selected cohorts and were inconsistent. Whereas ET-1 was positively associated with IMT in 61 older hypertensive patients (mean age 72.4 years),36 in a cohort of patients with chronic kidney disease, serum and tissue ET-1 was independent of the intima-media thickness of peripheral arteries.37 ET-1 infusion had no influence on extracerebral arteries or cerebral blood flow, suggesting that intravascular ET-1 does not have a direct cerebrovascular effect.38 Two small studies involving patients with type 2 diabetes39 and type 1 diabetes40 found an inverse association of ET-1 with the IMT.
Regarding measures of vascular function, CT-proET-1 was not associated with peripheral arterial tonometry in a population-based European study.41 Another study found a correlation between ET-1 and pulse pressure, which was, however, only present in Blacks and not in non-Hispanic Whites.42 Similarly, CT-proET-1 was associated with the ankle-brachial index only in hypertensive African Americans, but not in hypertensive non-Hispanic Whites.43 Therefore, as described for instance for aldosterone,44 ethnic differences may also play a role. The present study mainly included Western European participants and thus we were unable to test this hypothesis.
Our data suggest that in certain settings moderately increased CT-proET-1 concentrations may indicate a reduced risk of early carotid atherosclerotic lesions. A possible explanation are differential effects of ET-1 on different vascular beds. Similar findings were previously shown for the vasoconstrictive peptide copeptin45 and corroborated by experimental studies showing a vasodilatation of carotid arteries after vasopressin infusion in rats despite a systemic blood pressure increase.46 Thus, the net effect of circulating vasoconstrictive peptides may depend on the absolute hormone concentration and on the vascular bed. Whereas high levels may be proatherogenic or indirectly indicate an increased risk for vascular complications, intermediate concentrations may exert an inert or even protective effect on carotid vascular endothelium.
Association of CT-proET-1 with Biomarkers of Subclinical Inflammation and Adipokines
CT-proET-1 was associated with several biomarkers of subclinical inflammation as well as with adipokines. To our knowledge, the association of CT-proET-1 with a large number of biomarkers of subclinical inflammation and adipokines has been analyzed for the first time in a cohort of the general population. Previously, an association of CT-proET-1 with hsCRP, TNF-α and IL-6 has been described in patients with chronic heart failure.47 The association of ET-1 and markers of inflammation appears to be bi-directional and exhibits some inconsistencies in preclinical studies. ET-1 induces the production of IL-6, IL-13, IL-2 and granulocyte macrophage colony stimulating factor in pulmonary artery smooth muscle cells.48 Conversely, ET-1 release from endothelial cells is stimulated by TNF-α49 and IL-6.50 However, a dual ETRA and ETRB blocker had no effect on TNF-α, IL-6 and IL-10 plasma levels in a porcine model of sepsis,51 and differential effects of ETRA and ETRB activation depending on tissue are described.52 Interestingly, blocking of the ETRA was associated with an increase of the anti-inflammatory SOD activity in rats.53 In our study, CT-proET-1 was not significantly associated with SOD-3. However, we found a positive association with the anti-inflammatory cytokine IL-22, indicating that ET-1 may also exert immunomodulatory effects. The association of CT-proET-1 appeared to be stronger with primarily pro-inflammatory markers and adipokines than with anti-inflammatory markers, matching the putative pro-inflammatory properties of ET-1. The association of CT-proET-1 with all-cause mortality was attenuated by correction for IL-6 and sICAM-1 but remained statistically significant.
Limitations
The current data are based on a well-characterized large population-based study sample. Nevertheless, some of the null results might be due to insufficient power. The numbers of myocardial infarctions and cardiovascular mortality were relatively low, precluding definite conclusions regarding these outcomes. This may also hold true for the absence of differences after multiple testing for some of the biomarkers of subclinical inflammation and adipokines (e g MPO and progranulin). The study participants were mainly Western Europeans, limiting the generalizability of the results. The observational nature of the study precludes statements about causality.
Conclusions
CT-proET-1 was associated with all-cause mortality and with biomarkers of subclinical inflammation and adipokines. However, no significant association was detected regarding cardiovascular events. CT-proET-1 was even inversely associated with the IMT after multivariable adjustment. The results emphasize the complexity of ET-1 actions and/or indicator functions of CT-proET-1. Nevertheless, CT-proET-1 is an independent risk marker for all-cause mortality.
Abbreviations
CI, confidence interval; HR, hazard ratio; CT-proET-1, C-terminal pro-endothelin-1; CCA, common carotid artery; eGFR, estimated glomerular filtration rate; ET-1, endothelin-1; ETR, endothelin receptor(s); HDL, high density lipoprotein; hsCRP, high-sensitivity C-reactive protein; IMT, intima-media thickness; KORA, Cooperative Health Research in the Region of Augsburg; LDL, low density lipoprotein; LOD, limit of detection; MPO, myeloperoxidase; IL, interleukin; IL-1RA, interleukin-1 receptor antagonist; RBP-4, retinol-binding protein-4; sICAM-1, soluble intercellular adhesion molecule-1; SOD-3, superoxide dismutase-3; TNF-α, tumor necrosis factor-α.
Data Availability
The data are subject to national data protection laws and restrictions were imposed by the Ethics Committee of the Bavarian Chamber of Physicians to ensure data privacy of the study participants. Therefore, data cannot be made freely available in a public repository. However, data can be requested through an individual project agreement with KORA via the online portal KORA.passt (https://epi.helmholtz-muenchen.de/).
Acknowledgments
We gratefully acknowledge the contribution of all field staff members conducting the KORA F4 study and thank all study participants.
Funding
The study was supported by a research grant from the Virtual Diabetes Institute (Helmholtz Zentrum München) and the Clinical Cooperation Group Diabetes, Ludwig-Maximilians-University München and Helmholtz Zentrum München, and by the German Diabetes Center. The German Diabetes Center was supported by the Federal Ministry of Health (Berlin, Germany) and the Ministry of Culture and Science of the state North Rhine Westphalia (Düsseldorf, Germany). The KORA study was initiated and financed by the Helmholtz Zentrum München - German Research Center for Environmental Health, which is funded by the German Federal Ministry of Education and Research (BMBF) and by the State of Bavaria. This study was also supported by grants from the German Federal Ministry of Education and Research (BMBF) to the German Center for Diabetes Research e.V. (DZD). Further support was obtained from the Deutsche Diabetes Gesellschaft (DDG) and from the German Research Foundation (DFG, grant RA-45913/3-1). The funding sources had no role in in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Disclosure
CH received a research grant from Sanofi-Aventis. MR reports consulting fees from Eli Lilly, Terra Firma, Fishawack Group, Target-RWE, Bristol-Myers Squibb and Inventiva, and honoraria for lectures from Boehringer-Ingelheim Pharma, Sanofi US, Novo Nordisk. WR reports the receipt of consulting fees for attending educational sessions or advisory boards run by AstraZeneca, Boehringer Ingelheim and NovoNordisk and institutional research grants from NovoNordisk. WK reports consulting fees from AstraZeneca, Novartis, Pfizer, The Medicines Company, DalCor, Kowa, Amgen, Corvidia, Daiichi-Sankyo, Genentech, Novo Nordisk, Esperion, OMEICOS, speaker honoraria from Amgen, Novartis, Berlin-Chemie, Sanofi, and Bristol-Myers Squibb, grants and non-financial support from Abbott, Roche Diagnostics, Beckmann, and Singulex. The reported disclosures are outside of the topic of the current work. The other authors declare that they have no conflict of interest associated with this manuscript.
References
1. Kalani M. The importance of endothelin-I for microvascular dysfunction in diabetes. Vasc Health Risk Manag. 2008;4(5):1061–1068. doi:10.2147/VHRM.S3920
2. Comellas AP, Briva A. Role of endothelin-1 in acute lung injury. Transl Res. 2009;153(6):263–271. doi:10.1016/j.trsl.2009.02.007
3. Davenport AP, Hyndman KA, Dhaun N, et al. Endothelin. Pharmacol Rev. 2016;68(2):357–418. doi:10.1124/pr.115.011833
4. Ramseyer VD, Cabral PD, Garvin JL. Role of endothelin in thick ascending limb sodium chloride transport. Endothelin Renal Physiol Dis. 2011;172:76–83.
5. Roden M, Vierhapper H, Liener K, Waldhäusl W. Endothelin-1-stimulated glucose production in vitro in the isolated perfused rat liver. Metabolism. 1992;41(3):290–295. doi:10.1016/0026-0495(92)90273-D
6. Papassotiriou J, Morgenthaler NG, Struck J, Alonso C, Bergmann A. Immunoluminometric assay for measurement of the C-terminal endothelin-I precursor fragment in human plasma. Clin Chem. 2006;52(6):1144–1151. doi:10.1373/clinchem.2005.065581
7. Seissler J, Feghelm N, Then C, et al. Vasoregulatory peptides pro-endothelin-1 and pro-adrenomedullin are associated with metabolic syndrome in the population-based KORA F4 study. Eur J Endocrinol. 2012;167(6):847–853. doi:10.1530/EJE-12-0472
8. Sujana C, Seissler J, Jordan J, et al. Associations of cardiac stress biomarkers with incident type 2 diabetes and changes in glucose metabolism: KORA F4/FF4 study. Cardiovasc Diabetol. 2020;19(1). doi:10.1186/s12933-020-01117-1
9. Buendgens L, Yagmur E, Bruensing J, et al. C-terminal proendothelin-1 (CT-proET-1) is associated with organ failure and predicts mortality in critically ill patients. J Intensive Care. 2017;5(1). doi:10.1186/s40560-017-0219-y
10. Jankowska EA, Filippatos GS, von Haehling S, et al. identification of chronic heart failure patients with a high 12-month mortality risk using biomarkers including plasma C-terminal pro-endothelin-1. PLoS One. 2011;6(1):e14506. doi:10.1371/journal.pone.0014506
11. Zhang CL, Xie S, Qiao X, et al. Plasma endothelin-1-related peptides as the prognostic biomarkers for heart failure: a PRISMA-compliant meta-analysis. Medicine. 2017;96(50):e9342.
12. Haaf P, Zellweger C, Reichlin T, et al. Utility of C-terminal proendothelin in the early diagnosis and risk stratification of patients with suspected acute myocardial infarction. Can J Cardiol. 2014;30(2):195–203.
13. Khan SQ, Dhillon O, Struck J, et al. C-terminal pro-endothelin-1 offers additional prognostic information in patients after acute myocardial infarction. Leicester Acute Myocardial Infarction Peptide (LAMP) Study. Am Heart J. 2007;154(4):736–742.
14. Yip HK, Wu CJ, Chang HW, et al. Prognostic value of circulating levels of endothelin-1 in patients after acute myocardial infarction undergoing primary coronary angioplasty. Chest. 2005;127(5):1491–1497. doi:10.1378/chest.127.5.1491
15. Li P, Schmidt IM, Sabbisetti V, Tio MC, Opotowsky AR, Waikar SS. Plasma endothelin-1 and risk of death and hospitalization in patients undergoing maintenance hemodialysis. Clin J Am Soc Nephrol. 2020;15(6):784–793. doi:10.2215/CJN.11130919
16. Haapaniemi E, Tatlisumak T, Hamel K, et al. Plasma endothelin-1 levels neither increase nor correlate with neurological scores, stroke risk factors, or outcome in patients with ischemic stroke. Stroke. 2000;31(3):720–725.
17. Artunc F, Nowak A, Mueller C, et al. Plasma concentrations of the vasoactive peptide fragments mid-regional pro-adrenomedullin, C-terminal pro-endothelin 1 and copeptin in hemodialysis patients: associated factors and prediction of mortality. PLoS One. 2014;9(1):e86148. doi:10.1371/journal.pone.0086148
18. Maier C, Clodi M, Neuhold S, et al. Endothelial markers may link kidney function to cardiovascular events in type 2 diabetes. Diabetes Care. 2009;32(10):1890–1895. doi:10.2337/dc08-2168
19. Molvin J, Jujic A, Bachus E, et al. Cardiovascular biomarkers predict post-discharge re-hospitalization risk and mortality among Swedish heart failure patients. ESC Heart Failure. 2019;6(5):992–999. doi:10.1002/ehf2.12486
20. Rathmann W, Strassburger K, Heier M, et al. Incidence of Type 2 diabetes in the elderly German population and the effect of clinical and lifestyle risk factors: KORA S4/F4 cohort study. Diabet Med. 2009;26(12):1212–1219. doi:10.1111/j.1464-5491.2009.02863.x
21. Huth C, von Toerne C, Schederecker F, et al. Protein markers and risk of type 2 diabetes and prediabetes: a targeted proteomics approach in the KORA F4/FF4 study. Eur J Epidemiol. 2019;34(4):409–422. doi:10.1007/s10654-018-0475-8
22. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612. doi:10.7326/0003-4819-150-9-200905050-00006
23. Herder C, Bongaerts BWC, Rathmann W, et al. Differential association between biomarkers of subclinical inflammation and painful polyneuropathy: results from the KORA F4 study. Diabetes Care. 2015;38(1):91–96. doi:10.2337/dc14-1403
24. Herder C, De Las Heras Gala T, Carstensen-Kirberg M, et al. Circulating levels of interleukin 1-receptor antagonist and risk of cardiovascular disease: meta-analysis of six population-based cohorts. Arterioscler Thromb Vasc Biol. 2017;37(6):1222–1227. doi:10.1161/ATVBAHA.117.309307
25. Herder C, Kannenberg JM, Carstensen-Kirberg M, et al. Serum levels of interleukin-22, cardiometabolic risk factors and incident type 2 diabetes: KORA F4/FF4 study. Cardiovasc Diabetol. 2017;16(1). doi:10.1186/s12933-017-0498-6
26. Herder C, Kannenberg JM, Huth C, et al. Myeloperoxidase, superoxide dismutase-3, cardiometabolic risk factors, and distal sensorimotor polyneuropathy: the KORA F4/FF4 study. Diabetes Metab Res Rev. 2018;34(5):e3000. doi:10.1002/dmrr.3000
27. Ebert T, Gebhardt C, Scholz M, et al. Relationship between 12 adipocytokines and distinct components of the metabolic syndrome. J Clin Endocrinol Metab. 2018;103(3):1015–1023.
28. Touboul PJ, Hennerici MG, Meairs S, et al. Mannheim intima-media thickness consensus. Cerebrovasc Dis. 2004;18:346–349. doi:10.1159/000081812
29. Kowall B, Ebert N, Then C, et al. Associations between blood glucose and carotid intima-media thickness disappear after adjustment for shared risk factors: the KORA F4 study. PLoS One. 2012;7(12):e52590. doi:10.1371/journal.pone.0052590
30. Westphal LP, Schweizer J, Fluri F, et al. C-Terminal-Pro-Endothelin-1 Adds incremental prognostic value for risk stratification after ischemic stroke. Front Neurol. 2021;11:11.
31. Dakhel A, Engström G, Melander O, et al. Vasoactive biomarkers associated with long-term incidence of symptomatic peripheral arterial disease and mortality. Angiology. 2021;72(6):550–555. doi:10.1177/0003319720987739
32. Adlbrecht C, Hülsmann M, Strunk G, et al. Prognostic value of plasma midregional pro-adrenomedullin and C-terminal-pro-endothelin-1 in chronic heart failure outpatients. Eur J Heart Fail. 2009;11(4):361–366. doi:10.1093/eurjhf/hfp004
33. Kanaya AM, Barrett-Connor E, Wassel Fyr CL. Endothelin-1 and prevalent coronary heart disease in older men and women (the Rancho Bernardo study). Am J Card. 2007;99(4):486–490. doi:10.1016/j.amjcard.2006.09.096
34. Drion I, Kleefstra N, Landman GWD, et al. Plasma COOH-terminal proendothelin-1: a marker of fatal cardiovascular events, all-cause mortality, and new-onset albuminuria in type 2 diabetes? (ZODIAC-29). Diabetes Care. 2012;35(11):2354–2358. doi:10.2337/dc11-2526
35. Ibrahim NE, Gupta R, Lyass A, et al. Endothelin-1 measurement in patients undergoing diagnostic coronary angiography-results from the catheter sampled blood archive in cardiovascular diseases (CASABLANCA) study. Clin Chem. 2018;64(11):1617–1625. doi:10.1373/clinchem.2017.286385
36. Skalska AB, Grodzicki T. Carotid atherosclerosis in elderly hypertensive patients: potential role of endothelin and plasma antioxidant capacity. J Hum Hypertens. 2010;24(8):538–544. doi:10.1038/jhh.2009.97
37. Nezami N, Sepehrvand N, Mirchi M, et al. Serum and tissue endothelin-1 are independent from intima-media thickness of peripheral arteries in patients with chronic kidney disease. Vascular. 2015;23(4):382–390. doi:10.1177/1708538114551195
38. Hougaard A, Younis S, Iljazi A, et al. Cerebrovascular effects of endothelin-1 investigated using high-resolution magnetic resonance imaging in healthy volunteers. J Cereb Blood Flow Metab. 2020;40(8):1685–1694. doi:10.1177/0271678X19874295
39. Wang M, Sui J, Wang S, Wang X. Correlations of carotid intima-media thickness with endothelial function and atherosclerosis degree in patients with type 2 diabetes mellitus. Clin Hemorheol Microcirc. 2019;72(4):431–439. doi:10.3233/CH-180486
40. Cohen M, Yaseen H, Khamaisi M, et al. Endothelin‐1 levels are decreased in pediatric type 1 diabetes and negatively correlate with the carotid intima media thickness. Pediatr Diabetes. 2021;22(6):916–923. doi:10.1111/pedi.13237
41. Schnabel RB, Wild PS, Schulz A, et al. Multiple endothelial biomarkers and noninvasive vascular function in the general population: the Gutenberg health study. Hypertension. 2012;60(2):288–295. doi:10.1161/HYPERTENSIONAHA.112.191874
42. Du Plooy CS, Mels CMC, Huisman HW, Kruger R. Three-year change in endothelin-1 and markers of vascular remodelling in a bi-ethnic South African cohort: the SABPA study. J Hum Hypertens. 2017;31(11):708–714. doi:10.1038/jhh.2017.47
43. Habib A, Al-Omari MA, Khaleghi M, et al. Plasma C-terminal pro-endothelin-1 is associated with target-organ damage in African Americans with hypertension. Am J Hypertens. 2010;23(11):1204–1208. doi:10.1038/ajh.2010.149
44. Tu W, Eckert GJ, Hannon TS, et al. Racial differences in sensitivity of blood pressure to aldosterone. Hypertension. 2014;63(6):1212–1218. doi:10.1161/HYPERTENSIONAHA.113.02989
45. Then C, Kowall B, Lechner A, et al. Plasma copeptin levels are inversely associated with intima-media-thickness in men: the population-based KORA F4 study. Cardiovasc Diabetol. 2013;12(1):168. doi:10.1186/1475-2840-12-168
46. Rutschmann B, Evequoz D, Aubert JF, Brunner HR, Waeber B. Vasopressin dilates the rat carotid artery by stimulating V1 receptors. J Cardiovasc Pharmacol. 1998;32(4):637–641. doi:10.1097/00005344-199810000-00017
47. Gombos T, Förhécz Z, Pozsonyi Z, et al. Adrenomedullin and endothelin-1 are related to inflammation in chronic heart failure. Inflamm Res. 2009;58(6):298–305. doi:10.1007/s00011-008-8184-5
48. Yeager ME, Belchenko DD, Nguyen CM, Colvin KL, Ivy DD, Stenmark KR. Endothelin-1, the unfolded protein response, and persistent inflammation: role of pulmonary artery smooth muscle cells. Am J Respir Cell Mol Biol. 2012;46(1):14–22. doi:10.1165/rcmb.2010-0506OC
49. Hynynen MM, Khalil RA. The vascular endothelin system in hypertension–recent patents and discoveries. Recent Pat Cardiovasc Drug Discov. 2006;1(1):95–108. doi:10.2174/157489006775244263
50. Yamashita JI, Ogawa M, Nomura K, et al. Interleukin 6 stimulates the production of immunoreactive endothelin 1 in human breast cancer cells. Cancer Res. 1993;53(3):464–467.
51. Fenhammar J, Andersson A, Frithiof R, et al. The endothelin receptor antagonist tezosentan improves renal microcirculation in a porcine model of endotoxemic shock. Acta Anaesthesiol Scand. 2008;52(10):1385–1393. doi:10.1111/j.1399-6576.2008.01768.x
52. Kowalczyk A, Kleniewska P, Kolodziejczyk M, Skibska B, Goraca A. The role of endothelin-1 and endothelin receptor antagonists in inflammatory response and sepsis. Arch Immunol Ther Exp. 2015;63(1):41–52. doi:10.1007/s00005-014-0310-1
53. Briyal S, Philip T, Gulati A. Endothelin-a receptor antagonists prevent amyloid-β-induced increase in ETA receptor expression, oxidative stress, and cognitive impairment. J Alzheimers Dis. 2011;23(3):491–503. doi:10.3233/JAD-2010-101245
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.