Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Artificial Intelligence in the Nutritional Management of Inflammatory Bowel Disease: A Scoping Review
Authors Qian X, Yu J ![]() , Zhang Q, Jia G, Guo J, Lin T
, Zhang Q, Jia G, Guo J, Lin T
Received 3 April 2026
Accepted for publication 22 June 2026
Published 14 July 2026 Volume 2026:19 614374
DOI https://doi.org/10.2147/JMDH.S614374
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Xia Qian, Jie Yu, Qun Zhang, Guanzhen Jia, Junjun Guo, Tianmei Lin
Department of Nursing, the Fourth Affiliated Hospital of School of Medicine, and International School of Medicine, International Institutes of Medicine, Zhejiang University, Yiwu, Zhejiang, 322000, People’s Republic of China
Correspondence: Jie Yu, Department of Nursing, the Fourth Affiliated Hospital of School of Medicine, and International School of Medicine, International Institutes of Medicine, Zhejiang University, Yiwu, Zhejiang, 322000, People’s Republic of China, Email [email protected]
Background: Diet is closely associated with the onset, progression, and prognosis of inflammatory bowel disease (IBD). In the absence of specific dietary and nutritional guidelines, nutritional management for IBD patients is fraught with challenges and uncertainties. Existing research indicates that artificial intelligence (AI) has great potential for application in the nutritional management of patients with chronic diseases; however, current research on its use in IBD patients is limited.
Methods: This scoping review was reported in strict accordance with the PRISMA-ScR checklist. A systematic search was conducted across 11 databases, including PubMed, Web of Science, and Scopus, covering the period from the inception of each database to February 2026, focusing on studies investigating the application of AI in the nutritional management of IBD patients.
Results: Of the 4,560 records initially screened, 16 studies met the inclusion criteria. The results indicate that AI applications primarily focus on: dietary pattern recognition, such as using clustering algorithms to identify an association between plant-based diets and lower inflammation risk; treatment response prediction, with machine learning models predicting the success rate of total parenteral nutrition and achieving 90% accuracy in distinguishing between Crohn’s disease and ulcerative colitis; personalized information support, where conversational AI such as ChatGPT answered nutritional questions with 83.0% accuracy, and smartphone apps can influence patients’ dietary behaviors; identifying patient needs, where Natural Language Processing and Latent Dirichlet Allocation (LDA) topic modeling identified key patient concerns such as treatment experiences, dietary advice, and psychological burden. Key technologies encompass traditional machine learning, deep learning, natural language processing, and multi-omics integrated analysis. AI applications have preliminarily demonstrated the ability to reduce inflammatory markers and improve gut microbiota; fecal metabolites have been confirmed as reliable indicators of disease.
Conclusion: AI holds promise for the nutritional management of IBD and has shown preliminary success in pattern recognition, prediction of treatment efficacy, and patient empowerment. However, existing studies are often limited by small sample sizes and insufficient generalizability, and the evidence remains preliminary and heterogeneous. Future efforts should focus on large-scale studies and multidisciplinary collaboration to advance AI from proof-of-concept to clinical practice.
Keywords: inflammatory bowel disease, crohn’s disease, ulcerative colitis, artificial intelligence, nutrition
Introduction
Inflammatory bowel disease (IBD), primarily comprising Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic, nonspecific, and recurrent inflammatory condition of the intestines,1,2 with a global prevalence that is rising year by year.3,4 The etiology of IBD is complex, involving interactions among multiple factors, including genetic susceptibility, environmental factors, gut microbiota dysbiosis, and abnormal immune responses.5 Among the various environmental factors, diet is not only a potential modifiable risk factor for IBD onset but also a critical component throughout the entire disease management process.6–8 For this reason, nutritional management plays a central role in IBD treatment. Its objectives extend beyond correcting and preventing malnutrition to directly modulating intestinal inflammation, alleviating symptoms, promoting mucosal healing, and optimizing the efficacy of pharmacological therapy through specific dietary patterns.9–12 However, due to limited evidence, current guidelines have not yet established a dietary pattern suitable for IBD patients,13 and traditional IBD nutritional management faces significant challenges. First, the effects of diet on the human body are highly individualized and influenced by multiple factors, including genetics,14 gut microbiota composition,15 disease phenotype,16 and lifestyle habits.17 The same food or dietary pattern may elicit vastly different responses in different patients. Second, traditional nutritional assessment tools, such as food frequency questionnaires and dietary diaries, often rely on patient recall, are subject to information bias, and struggle to quantify complex dietary exposures in real time and with precision.18,19
Furthermore, due to insufficient professional guidance and interference from non-specialized information, IBD patients face numerous nutritional issues, such as inadequate nutrient intake, avoidance of restrictive dietary behaviors, and blind adherence to dietary patterns.20 These nutritional issues increase patients’ risk of malnutrition, leading to adverse health outcomes such as increased risk of complications and surgery, prolonged hospital stays, and reduced immunity.19 Finally, in the absence of specific dietary recommendations, nutritional management for IBD patients is fraught with challenges and uncertainty,21,22 and some patients even develop a fear of eating.23 Therefore, extracting meaningful and actionable dietary guidance strategies for individual patients from vast, multidimensional datasets is a task that traditional statistical methods struggle to accomplish. Artificial Intelligence (AI), particularly the rapid advancements in technologies such as machine learning (ML), deep learning (DL), computer vision (CV), and natural language processing (NLP), offer entirely new possibilities for addressing these challenges.18
AI primarily refers to the theories, methods, technologies, and application systems that use computer algorithms to simulate, extend, and expand human intelligence, thereby enabling computers to perform a range of intelligent activities such as reasoning, task execution, and autonomous response.24 Its core capability lies in automatically learning patterns and regularities from complex, high-dimensional data and using them for prediction or classification.25 In the medical field, the potential of AI is gradually being tapped. AI technologies such as ML, CV, and NLP are widely applied and show great promise in the field of nutritional management. Not only can they provide patients with nutritional assessments, diagnoses, and screening and prediction of nutrition-related risks,26 but they can also offer personalized nutritional advice based on patients’ nutritional and physical conditions, enabling automated, scientific nutritional management.27 For example, using computer vision technology, AI can automatically analyze photos of food to estimate nutritional content and calories. This helps patients adjust their diets in real time.28 Through natural language processing, AI can interpret patients’ food diaries, identify unhealthy dietary habits, and provide recommendations for improvement.29 Combined with machine learning algorithms, AI can dynamically predict potential future nutritional risks in patients. This supports early intervention and personalized prevention strategies.30,31 Although research on AI in IBD nutritional management is increasing globally, the existing literature primarily focuses on the development of AI for specific applications, such as nutritional assessment32 and dietary pattern exploration,33 but few studies have classified these AI technologies or summarized their application outcomes. Therefore, this study aims to employ a scoping review methodology34 to systematically review and synthesize the literature on the application of AI technologies in the nutritional management of IBD patients, and to conduct a comprehensive analysis of AI applications in this field, to provide valuable references for future research and clinical practice.
Materials and Methods
Defining the Research Questions
The research questions addressed in this scoping review are as follows: (1) In which scenarios is AI primarily applied in the nutritional management of patients with IBD? (2) What technologies and methods are employed by AI in the nutritional management of patients with IBD? (3) What are the main outcomes or research findings associated with the application of AI in IBD nutritional management?
Methodology
This scoping review aims to systematically summarize the current status and characteristics of AI applications in the nutritional management of adult patients with IBD. The research methodology strictly adheres to the scoping review framework proposed by Arksey and O’Malley and its core methodological principles,34 while simultaneously following the PRISMA-ScR35 checklist for literature retrieval to ensure the transparency and integrity of the research report. This research process comprises four core stages: systematic literature search, preliminary title/abstract screening, application of inclusion/exclusion criteria, and final comprehensive analysis.36 Given that the primary objective of this study is to describe the characteristics of the existing literature rather than to assess the methodological quality of the included studies, we focused only on key methodological elements from the PRISMA checklist.35 The detailed PRISMA-ScR checklist is available in Supplementary Material S1.
Search Strategy
A systematic search was conducted in PubMed, Web of Science, Embase, the Cochrane Library, CINAHL, IEEE Xplore, the Association for Computing Machinery Digital Library, SinoMed, CNKI, Wanfang Data, VIP, and other Chinese databases to identify studies on the application of AI in the nutritional management of patients with IBD. The search period extended from the inception of each database to February 2026. Boolean operators, including AND and OR, were used. The database search strategy was optimized using the following Medical Subject Headings (MeSH) terms:
“Inflammatory Bowel Disease” OR “Ulcerative Colitis” OR “Crohn’s Disease”;
“food” OR “nutrition” OR “recipe” OR “diet” OR “dish”;
“ artificial intelligence ” OR “machine intelligence” OR “data mining” OR “fuzzy algorithms” OR “neural networks” OR “Bayesian networks” OR “text mining” OR “fuzzy logic” OR “knowledge representation” OR “machine learning” OR “deep learning” OR “natural language processing” OR “non-natural language processing” OR “random forests” OR “support vector machines” OR “algorithms”.
During the initial screening phase, studies that did not meet the inclusion criteria were excluded based on title and abstract screening. As shown in Table S1, this process was conducted independently by three reviewers (XQ, QZ, and GZJ) to ensure transparency and reduce uncertainty in the review findings. Any disagreements during the study screening process were resolved through consultation with a fourth reviewer (JY), who helped finalize the list of included studies.
Data Extraction and Analysis
First, duplicate studies were removed using the EndNote reference management tool. Subsequently, title and abstract screening was performed independently by three reviewers (XQ, QZ, GZJ) as described in Section 2.3. Full-text eligibility was assessed independently by two of these reviewers (XQ and QZ), with any disagreements resolved by consulting the third reviewer (GZJ) and, if necessary, the fourth reviewer (JY). The PRISMA flowchart (Figure 1) illustrates the step-by-step screening process, including the identification, screening, and inclusion stages.37 The characteristics of the included studies are summarized in three tables: Table 1 presents basic source characteristics (first author, year of publication, country, data source, and data volume); Table 2 presents technical and methodological details (first author, AI technologies, main application methods, and data types); and Table 3 presents outcomes and evaluation (first author, main research results, ethical issues, and technology stage).
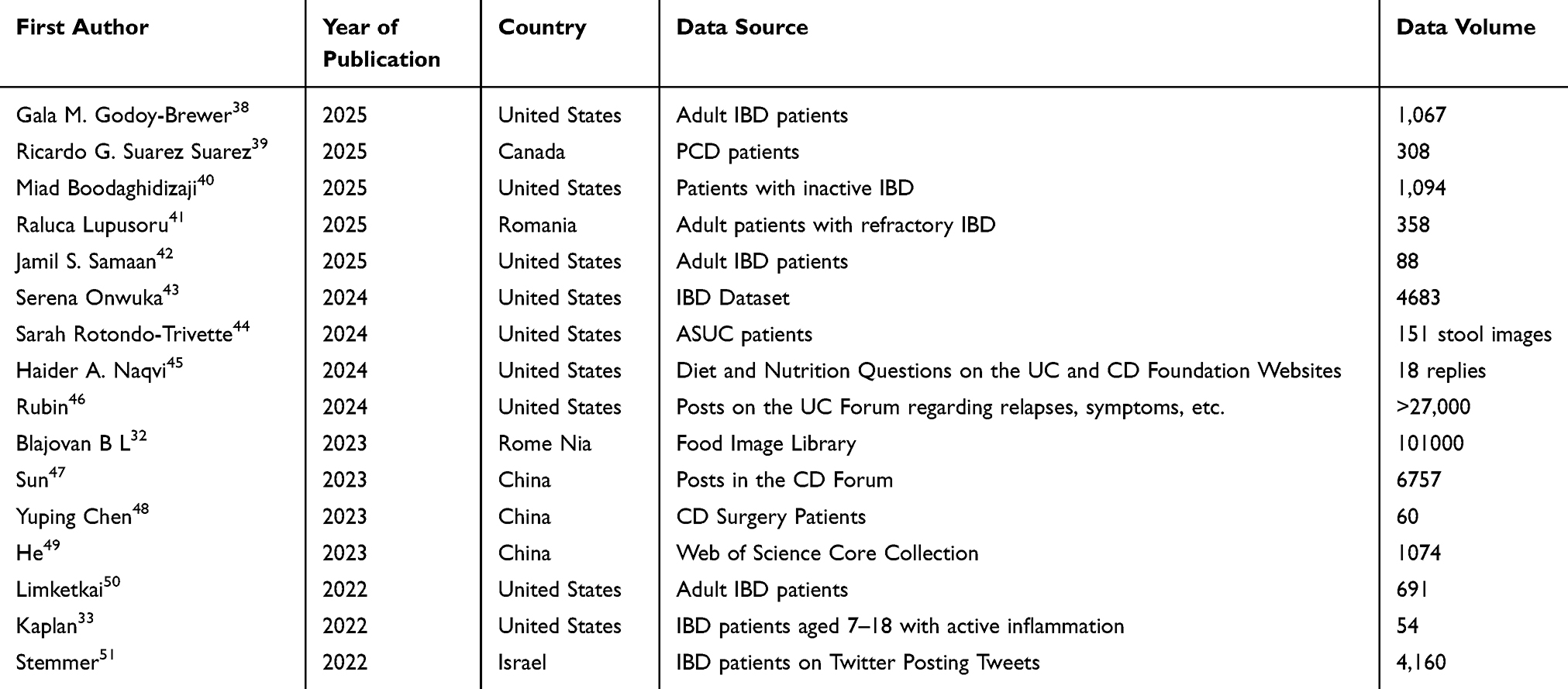 |
Table 1 Basic Characteristics of Included Studies |
 |
Table 2 Applied Artificial Intelligence Technologies and Data Types |
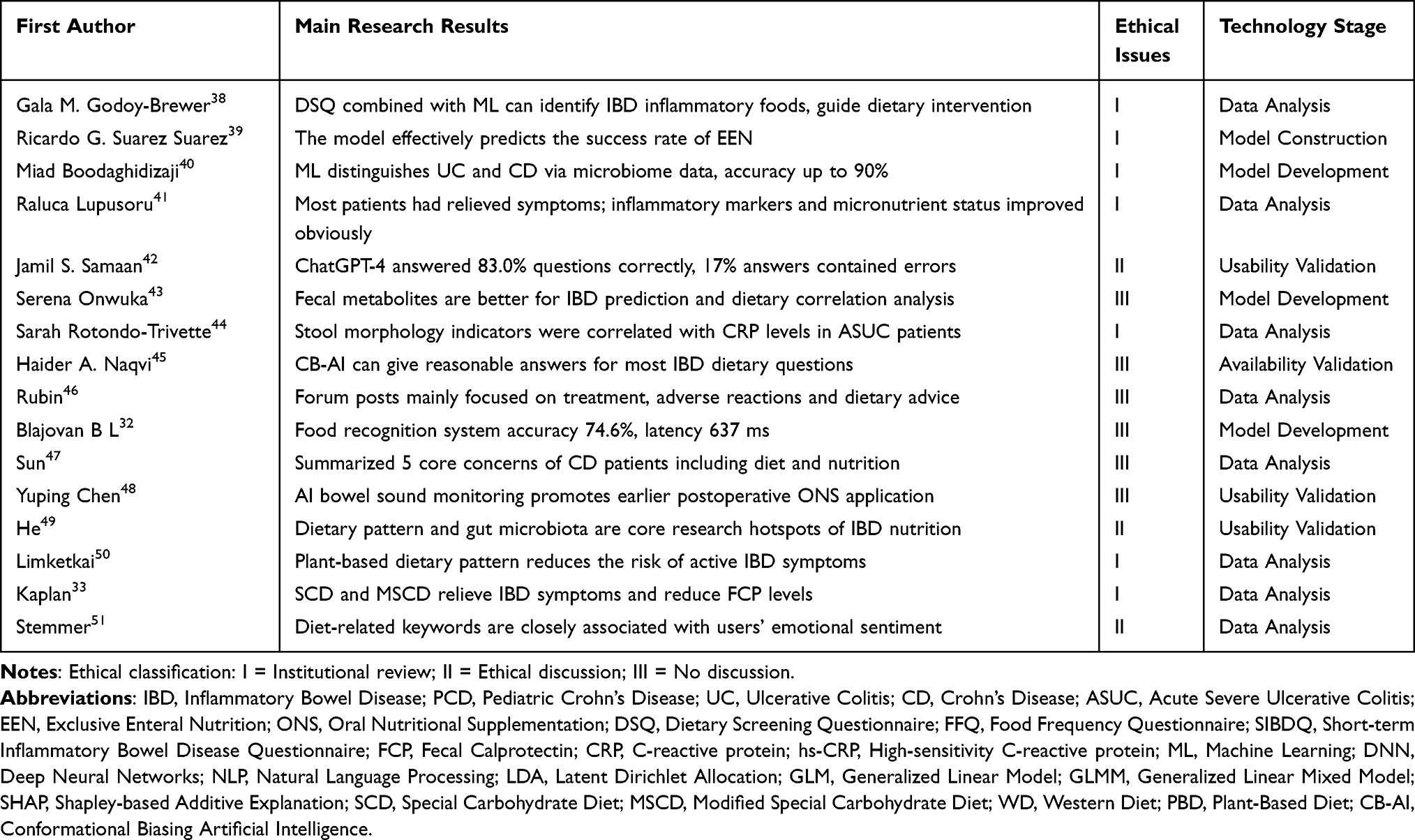 |
Table 3 Main Findings, Ethical Issues and Technology Stage |
 |
Figure 1 Flowchart for studies included in the scoping review. |
Inclusion and Exclusion Criteria
Inclusion criteria were determined based on the PCC principle,52][ which considers the study population, concept, and context. Inclusion criteria: (1) Study population included patients diagnosed with IBD; (2) Research content involved the application of AI in the field of nutritional management; (3) Studies included algorithm or model development, usability evaluation, or application research; (4) Full-text articles were accessible. Exclusion criteria: (1) Studies conducted in IBD that are unrelated to AI in nutritional knowledge or dietary behavior; (2) Studies without full-text access or conference abstracts without full-text availability; (3) Literature not in Chinese or English.
Risk of Bias Assessment
Given the exploratory nature of this scoping review, a formal risk-of-bias assessment was not conducted. However, study limitations were documented where applicable.
Study Registration
This study protocol has been registered on the Open Science Framework (OSF) platform (DOI: 10.17605/OSF.IO/X85MR).
Results
Basic Characteristics of Included Studies
A systematic literature search and screening process was conducted in accordance with the PRISMA statement. A total of 4,560 records were initially identified. After removal of duplicates and preliminary screening of titles and abstracts, 62 records were selected for full-text review. Of these, 46 records were excluded because they were not relevant to IBD diets, were not related to AI, were published in languages other than Chinese or English, lacked available full text, or represented duplicate Chinese and English versions of the same study.A total of 16 studies highly relevant to the research question were included. The included studies were primarily from the United States33,38,40,42–46,50 (n=9),33,38,40,42–46,50 China (n=3),47–49 Romania (n=2),32,41 Canada (n=1),39 and Israel (n=1),51 indicating that this topic is of interest in North America, Europe, and Asia. Data sources are diverse, including clinical patient data, social media/forum posts, public databases, and food image libraries. The volume of data varies widely, ranging from 54 cases to over 27,000 cases.
Application Scenarios of AI Technology in Nutrition Management
Across the included studies, AI technologies were primarily applied in five core scenarios: dietary pattern recognition, disease prediction, personalized support, patient sentiment analysis, and nutritional monitoring.
Dietary Pattern Recognition
Machine learning algorithms (eg, K-means clustering) were used to analyze Food Frequency Questionnaire (FFQ) data, successfully identifying specific dietary patterns (eg, plant-based diets) associated with IBD inflammatory activity. By comparing inflammatory marker levels across different clusters, these analyses provided a basis for personalized interventions.50
Disease Outcome Prediction
AI models demonstrated strong decision-support capabilities. For example, gradient-boosted decision trees integrated microbiome and clinical data to predict the success rate of EEN treatment.39 In addition, microbiome data were used to distinguish UC from CD with an accuracy as high as 90%.40
Personalized Dietary Recommendations and Informational Support
Large language models (eg, ChatGPT-4) answered IBD dietary questions with high accuracy (83.0%).42 Smartphone apps (eg, Dieta®) showed a positive guiding effect on dietary behaviors among specific populations (eg, male patients).44 Furthermore, smart devices assisted in initiating postoperative oral nutritional supplementation (ONS) through real-time monitoring of bowel sounds, outperforming traditional methods.48
Patient Sentiment Analysis
NLP techniques, including Latent Dirichlet Allocation (LDA) topic modeling and sentiment analysis, extracted key themes and emotional trends related to treatment experiences, peer support, and diet from large-scale social media data. These approaches revealed the impact of dietary factors on quality of life.51
Nutritional Assessment and Monitoring
DNNs were applied to food image recognition to evaluate nutrient intake. Using the Food101 dataset, the proposed model achieved an accuracy of 74.6% with ResNet50 and EfficientNet-B0, demonstrating the feasibility of on-device AI for dietary assessment in IBD patients and providing an objective basis for remote disease monitoring.32
Major AI Technologies and Methods Applied
The AI technologies applied across the included studies were diverse and encompassed multiple branches of machine learning. Traditional machine learning algorithms were the most widely used and were primarily applied to classification, regression, and clustering tasks. Classification and regression: Including Random Forests (RF), Support Vector Machines (SVM), XGBoost, LightGBM, and LASSO regression. These algorithms are commonly used to build predictive models39,43 (eg, predicting EEN success rates) and to identify important features (eg, through feature selection). Cluster Analysis: K-means clustering is a commonly used method for identifying patient dietary patterns.50 Probabilistic Models: Bayesian generalized linear models (GLMs) and generalized linear mixed models (GLMMs) are used to analyze patient-reported outcome data to evaluate treatment efficacy.33 Deep Learning Algorithms: These demonstrate advantages when processing images and complex text data. DNNs are primarily used to build food image recognition models.32 NLP is a core technology for processing and analyzing text data, including topic modeling (LDA), sentiment analysis, and keyword extraction.46,51 Large Language Models and Conversational AI: Represented by the ChatGPT series (including GPT-4, Bing Chat, and YouChat), research has focused on evaluating their accuracy, comprehensiveness, and reproducibility in providing IBD nutritional information.42,45 Multi-omics Integration and Explainable AI: Multi-omics Analysis: The NostraBiome platform is a prime example; by integrating metagenomic, metabolomic, transcriptomic, and clinical biomarker data and employing supervised ML (Gradient-Boosted Decision Trees) for comprehensive analysis, it provides patients with personalized microbiome and nutritional guidance. Lupusoru R et al41 found that fecal metabolites provide more reliable disease-prediction models than plasma metabolites. Explainable AI (XAI): A study employed a method based on Shapley additive explanations (SHAP) to interpret the predictions of ML classifiers, thereby enhancing the model’s transparency and credibility.43 Bibliometric Analysis Tools: The Bibliometrix R package was used to perform frequency analysis, network analysis, and geographical visualization of the literature in this field, revealing research hotspots (such as fatty acids and gut microbiota) and emerging trends.49
Key Findings and Effects of AI Applications
The application of AI in IBD nutritional management has preliminarily demonstrated its value and potential. Key research findings include: Feasibility of personalized dietary guidance: AI-based dietary screening tools (eg, DSQ) and predictive models can effectively identify inflammation-associated foods, providing practical tools for dietary assessment, guidance, and monitoring in clinical practice.38 A study by Raluca Lupusoru et al41 showed that, under AI guidance, the stool frequency of 358 participants decreased significantly, acute symptoms and rectal bleeding were alleviated in most patients, and over 70% of patients reported a “significant improvement” in their overall condition. Concurrently, inflammatory biomarkers (high-sensitivity C-reactive protein, fecal calprotectin) and micronutrient deficiencies (iron, zinc) improved, and beneficial gut microbiota (eg, Faecalibacterium prausnitzii, Bifidobacterium longum, and Akkermansia muciniphila) increased significantly. Comparison of the Efficacy of Specific Dietary Regimens: AI analysis provides data support for the efficacy of specific dietary regimens. The study found that the Special Carbohydrate Diet (SCD) and the Modified Special Carbohydrate Diet (MSCD) were superior to a standard diet in improving symptoms and reducing fecal calprotectin levels, with the SCD showing more pronounced effects.33 Unraveling the complex relationship between diet, microbiota, and host metabolism: Through multi-omics analysis, studies have confirmed the significant impact of IBD on the interactions between gut microbial metabolites and diet. Diet-related metabolites in feces demonstrated stronger and more population-specific disease associations than plasma metabolites, offering a new perspective for a deeper understanding of IBD pathogenesis.43 The Role of AI Tools in Patient Education and Behavior Change: Conversational AI can provide appropriate nutritional information to the majority of patients.45 Meanwhile, observational studies indicate that certain patient groups (such as men and Black patients) are more likely to adopt AI-driven dietary recommendations,44 suggesting that AI tools are subtly influencing patient behavior and are expected to drive the development of more precise and dynamic nutritional management models.
Discussion
From Macro-Level Pattern Recognition to Micro-Level Mechanism Exploration: AI Deepens Understanding of the “IBD Diet”
The overall landscape of AI applications in IBD nutritional management, including the core technologies, main application scenarios, key findings, and future directions, is summarized in Figure 2.The review found that the application of AI is reshaping our understanding of dietary management for IBD on two levels. At the macro level, through machine learning clustering algorithms, researchers can identify dietary patterns associated with different levels of inflammation risk (eg, plant-based diets vs Western diets) from complex dietary data.50 This approach addresses the limitations of traditional studies that focus on individual nutrients or foods and more effectively reflects the holistic and complex nature of real-world dietary patterns. It also provides stronger evidence for the development of generalizable dietary guidelines. At the micro level, multi-omics integration platforms such as NostraBiome combine AI with metagenomic and metabolomic data, not only validating the effects of specific dietary patterns on gut microbiota and inflammatory markers,41 but also revealing the unique value of fecal metabolites as predictors of disease.43 This suggests that future nutritional interventions may no longer be limited to “what to eat,” but will instead focus on “how ingested food is metabolized by an individual’s gut microbiota,” thereby achieving truly personalized nutrition.
 |
Figure 2 Conceptual framework of AI applications in the nutritional management of IBD. |
AI as a Bridge Between Clinical Endpoints and Patients’ Daily Experiences
Traditional IBD nutrition research has largely focused on clinical endpoints (such as disease activity indices and inflammatory markers). This review finds that AI, particularly NLP technology, is expanding the research perspective to patients’ daily lives. By mining vast amounts of text from social media and forums,46,47,51 researchers can capture patients’ most genuine concerns (such as worries about specific foods or a desire for peer support), emotional fluctuations, and unmet needs in real time and at low cost. The integration of patient-reported data with clinical data provides a foundation for a patient-centered, full-cycle care model. For example, the identification of food-related keywords associated with negative emotions not only reflects patients’ dietary concerns but may also indicate potential disease triggers, thereby providing new opportunities for clinical communication and health education.
Opportunities and Challenges of Conversational AI in Patient Empowerment
The emergence of large language models such as ChatGPT has provided patients with an immediate and convenient channel for accessing nutritional information. This review indicates that these models demonstrate a certain degree of accuracy and comprehensiveness in answering IBD-related nutritional questions45 and are expected to serve as a valuable supplement to traditional medical consultations. Particularly in settings with relatively scarce medical resources, they can effectively enhance patients’ self-management capabilities. However, the inadequate or outdated responses identified in the studies (17% in this review) also pose a challenge that cannot be ignored. Inaccurate information may mislead patients and lead to adverse consequences. Therefore, ensuring that medical information generated by chatbot-based AI (CB-AI) remains accurate and up-to-date, while clearly positioning it as a supplement rather than a substitute for professional medical decision-making, is a key challenge for future applications.
AI-Driven Behavior Change and Digital Health Equity
One included study found significant differences in the adoption of AI dietary recommendations among patients of different genders and races (with higher adoption rates among men and Black patients).44 This phenomenon warrants careful consideration. On the one hand, it confirms that AI tools can influence patients’ real-world behavior, offering hope of bridging the gap between standardized guidelines and individualized practice. On the other hand, it also serves as a wake-up call: the training data for AI algorithms, the design of user interfaces, and the selection of dissemination channels may inadvertently exacerbate or introduce new health inequities. Future research and applications must prioritize equity in digital health to ensure that AI-based nutrition tools benefit all IBD patient populations, rather than just specific subgroups.
Limitations of Existing Research and Future Prospects
Several important limitations of the current evidence base should be explicitly acknowledged. First, only 16 studies met the inclusion criteria, indicating that research at the intersection of AI, nutrition, and IBD remains at a very early stage. Second, the included studies were highly heterogeneous in terms of study design, including cross-sectional, retrospective, and proof-of-concept studies; AI technologies, including CNNs, random forests, NLP, and LLMs; data sources, including food images, dietary records, social media data, and electronic health records; and clinical contexts, including remission, active disease, and post-surgical settings. Third, none of the included studies performed external validation of their AI models, and no prospective or interventional studies were identified. Consequently, the current evidence should be interpreted as a preliminary mapping of an emerging research field, rather than as definitive evidence of the effectiveness of AI in improving nutritional management or clinical outcomes in IBD.
Beyond these field-wide limitations, several specific challenges warrant further attention. Most of the included studies were single-center studies with small sample sizes, which limits the generalizability of AI models to broader populations. Future large-scale, multicenter, prospective studies are needed to validate model stability and reliability. In addition, heterogeneity in AI technologies, data types, and outcome measures precludes direct comparisons across studies or meta-analyses; therefore, the field should gradually establish core data standards and a set of key outcome measures. With regard to AI explainability, although some studies incorporated methods such as SHAP, most models, particularly deep learning models, remain “black boxes,” which may hinder clinical trust. Future research should strengthen the use of explainable AI (XAI) to ensure that decision-making logic is understandable to clinicians. Finally, AI-based personalized dietary recommendations raise ethical and regulatory concerns, including data privacy, algorithmic bias, and liability, particularly when patients receive direct advice from conversational AI systems, such as CB-AI. Defining liability and ensuring safety are therefore urgent issues that require further discussion.
Looking ahead, the application of AI in IBD nutritional management is likely to evolve in the following directions: (1) Multimodal integration – combining clinical data, omics data, digital phenotypes (dietary images, bowel sounds, activity levels), and patient-reported data to build comprehensive personalized decision support systems; (2) Dynamic closed-loop management – shifting from static assessments to real-time monitoring via wearable devices and smart applications, enabling dynamic adjustments; (3) Precision nutritional intervention – leveraging multi-omic analysis to develop effective nutritional prescriptions for specific patient subgroups, including precise carbohydrate adjustments; and (4) Clinical decision support tools – integrating rigorously validated AI models into clinical workflows as auxiliary tools for physicians, not as substitutes.
Strengths and Limitations
The strengths of this study are primarily reflected in the following aspects. First, this review focuses on the emerging field of AI in the nutritional management of IBD. Methodologically, it strictly adheres to the PRISMA-ScR statement and the Arksey and O’Malley framework, and the study protocol was pre-registered on the OSF platform, thereby enhancing the rigor and reproducibility of the review process. Second, this study goes beyond the limitations of individual technologies or isolated application scenarios by systematically classifying and integrating 16 studies across multiple dimensions, including technology type, application scenario, data source, and research stage. It identifies five core application scenarios: dietary pattern recognition, treatment outcome prediction, personalized support, patient perspective analysis, and nutritional monitoring. It also systematically summarizes the application of AI technologies, including machine learning, deep learning, natural language processing, large language models, and multi-omics integration. In terms of results presentation, this study emphasizes an in-depth exploration of clinically relevant outcomes. Specifically, it summarizes preliminary evidence regarding the potential effects of AI-based approaches in reducing inflammatory markers, improving gut microbiota, and optimizing postoperative nutritional management. Particular attention is also given to the unique value of fecal metabolites as disease-related indicators, which may provide new insights for subsequent mechanistic research. Finally, based on the synthesis of existing evidence, this study identifies several areas that warrant further exploration, including model generalizability and interpretability, as well as data ethics and regulatory frameworks. To address these issues, we propose future directions such as multimodal data fusion, dynamic closed-loop management, and precision nutritional interventions, thereby providing guidance for future research in this field.
This review has several limitations. First, as a scoping review, it aimed to map the overall landscape of the research rather than to assess the methodological quality of individual studies; therefore, a formal risk-of-bias assessment of the included studies was not conducted. Second, although the search strategy was designed to be comprehensive, unpublished studies or studies published in languages other than Chinese or English may have been omitted. Finally, because this field is evolving rapidly, some of the most recent research findings may not have been captured.
Conclusion
In summary, the application of AI in the nutritional management of IBD represents a dynamic and emerging area of research. Current evidence suggests that AI technologies have considerable potential to identify personalized dietary patterns, predict treatment outcomes, capture patients’ real-world needs, and support self-management. However, this field still faces several challenges, including small sample sizes, limited model generalizability, poor interpretability, and underdeveloped ethical and regulatory frameworks. Future research should focus on multimodal data fusion, prospective interventional trials, strengthening explainable AI (XAI) research, and establishing appropriate ethical and regulatory frameworks to facilitate the translation of AI technologies from proof-of-concept studies into clinical practice, with the ultimate goal of improving the nutritional status and quality of life of patients with IBD. Specifically, future research should prioritize prospective, externally validated AI models that measure clinically relevant nutritional outcomes, such as remission rates and nutritional status biomarkers, in IBD populations, using standardized reporting guidelines such as CONSORT-AI.
Data Sharing Statement
Data available in a publicly accessible repository.
Acknowledgments
No formal effect measures were used, as this is a scoping review focused on mapping existing evidence. No data conversions or handling of missing statistics were performed, as this was a scoping review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Science and Technology Bureau of Yiwu City (Project Number: 24-3-156).
Disclosure
The authors declare no conflicts of interest.
References
1. Molodecky NA, S SI, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–13. doi:10.1053/j.gastro.2011.10.001
2. Yahui G, Weiwei N, Xiaolan Z. Consensus on the Diagnosis and Treatment of Inflammatory Bowel Disease. Beijing): Partial Interpretation of Crohn’s Disease; 2018. doi:10.3969/j.issn.1004-583x.2018.12.016
3. G KG. The global burden of IBD: from 2015 to 2025. Nat Rev Gastroenterol Hepatol. 2015;12(12):720–727. doi:10.1038/nrgastro.2015.150
4. C NS, K LW, Y SH, et al. Epidemiology of inflammatory bowel disease from 1981 to 2014: results from a territory-wide population-based registry in Hong Kong. Inflamm. Bowel Dis. 2016;22(8):1954–1960. doi:10.1097/MIB.0000000000000846
5. Guan Q. A comprehensive review and update on the pathogenesis of inflammatory bowel disease. J Immunol Res. 2019;16. doi:10.1155/2019/7247238
6. Levine A, M RJ, O LJ, et al. Dietary Guidance From the International Organization for the Study of Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol. 2020;18(6):1381–1392. doi:10.1016/j.cgh.2020.01.046
7. Park J, H CJ. Incidence and prevalence of inflammatory bowel disease across Asia. Yonsei Med J. 2021;62(2):99–108. doi:10.3349/ymj.2021.62.2.99
8. Qian Y, Tian T, Pengshuang S, et al. Visual study on the impact of food additives on the occurrence and development of inflammatory bowel disease. Chinese J Clin Nutr. 2022;30. doi:10.3760/cma.j.cn115822-20220905-00183
9. Raoul P, Cintoni M, Palombaro M, et al. Food Additives, a Key Environmental Factor in the Development of IBD through Gut Dysbiosis. Microorganisms. 2022;10(1):167. doi:10.3390/microorganisms10010167
10. N AA, N AA, Raman M. Diet in treatment of inflammatory bowel diseases. clinical gastroenterology and hepatology: the official clinical practice journal of the American gastroenterological association. Clin. Gastroenterol. Hepatol. 2021;19(3):425–435.e3. doi:10.1016/j.cgh.2019.11.054
11. Crooks B, McLaughlin J, Limdi J. Dietary beliefs and recommendations in inflammatory bowel disease: a national survey of healthcare professionals in the UK. Frontline Gastroenterol. 2022;13(1):25–31. doi:10.1136/flgastro-2020-101723
12. D LJ, T AM. Diet as a trigger or therapy for inflammatory bowel diseases. Gastroenterology. 2017;152(2):398–414.e6. doi:10.1053/j.gastro.2016.10.019
13. Bischoff SC, Bager P, Escher J, et al. ESPEN guideline on Clinical Nutrition in inflammatory bowel disease. Clin Nutr. 2023;42(3):352–379. doi:10.1016/j.clnu.2022.12.004
14. Glassner KL, Abraham BP, Quigley EMM. The microbiome and inflammatory bowel disease. J Allergy Clin Immunol. 2020;145(1):16–27. doi:10.1016/j.jaci.2019.11.003
15. T SP, B RSL, E RB, et al. Dysbiosis in inflammatory bowel disease: pathogenic role and potential therapeutic targets. Int J Mol Sci. 2022;23(7):3464. doi:10.3390/ijms23073464
16. E AT, Meyer M, Schwärzler J, et al. The metabolic nature of inflammatory bowel diseases. Nat Rev Gastroenterol Hepatol. 2022;19(12):753–767. doi:10.1038/s41575-022-00658-y
17. Crooks B, Misra R, Arebi N, et al. The dietary practices and beliefs of British South Asian people living with inflammatory bowel disease: a multicenter study from the United Kingdom. Intest. Res. 2022;20(1):53–63. doi:10.5217/ir.2020.00079
18. Barth I, L SC, Peters V, et al. Relative Validity of the Groningen IBD Nutritional Questionnaire (GINQ-FFQ): a Food Frequency Questionnaire Designed to Assess Nutritional Intake in Patients with Inflammatory Bowel Disease. Nutrients. 2025;17(2):239. doi:10.3390/nu17020239
19. Jabłońska B, Mrowiec S. Nutritional status and its detection in patients with inflammatory bowel diseases. Nutrients. 2023;15(8):1991. doi:10.3390/nu15081991
20. S DA, K YC, P CS, et al. Food avoidance, restrictive eating behaviour and association with quality of life in adults with inflammatory bowel disease: a systematic scoping review. Appetite. 2021;167:105650. doi:10.1016/j.appet.2021.105650
21. Rines J, Daley K, Loo S, et al. A patient-led, peer-to-peer qualitative study on the psychosocial relationship between young adults with inflammatory bowel disease and food. Health Expect. 2022;25(4):1486–1497. doi:10.1111/hex.13488
22. Li Y, Tu W, Yin T, et al. “Food doesn’t control me anymore!” psychosocial experiences during dietary management in adults with inflammatory bowel disease: a qualitative study. J Clin Nurs. 2024;33(10):4077–4089. doi:10.1111/jocn.17327
23. F ZH, Loftus P, Gibbons B, et al. “If I could survive without eating, it would be a huge relief”: development and initial validation of the Fear of Food Questionnaire. Appetite. 2022;169:105808. doi:10.1016/j.appet.2021.105808
24. Jarrahi MH, Lutz C, Newlands G. Artificial intelligence, human intelligence and hybrid intelligence based on mutual augmentation. Big Data Soc. 2022;9(2). doi:10.1177/20539517221142824
25. Voigtlaender S, Pawelczyk J, Geiger M, et al. Artificial intelligence in neurology: opportunities, challenges, and policy implications. J Neurol. 2024;271(5):2258–2273. doi:10.1007/s00415-024-12220-8
26. Zeevi D, Korem T, Zmora N, et al. Personalized nutrition by prediction of glycemic responses. Cell. 2015;163(5):1079–1094. doi:10.1016/j.cell.2015.11.001
27. Stefanidis K, Tsatsou D, Konstantinidis D, et al. PROTEIN AI advisor: a knowledge-based recommendation framework using expert-validated meals for healthy diets. Nutrients. 2022;14(20):4435. doi:10.3390/nu14204435
28. Yan R, Luo H, Lu J, et al. DietAI24 as a framework for comprehensive nutrition estimation using multimodal large language models. Communicat Med. 2025;5(1):458. doi:10.1038/s43856-025-01159-0
29. A KN, M MF, H OS, et al. MyDietCam: development and usability study of a food recognition integrated dietary monitoring smartphone application. Digital Health. 2023;9:20552076221149320. doi:10.1177/20552076221149320
30. Atwal K. Artificial intelligence in clinical nutrition and dietetics: a brief overview of current evidence. Nutr Clin Pract. 2024;39(4):736–742. doi:10.1002/ncp.11150
31. Varayil JE, Bielinski SJ, Mundi MS, et al. artificial intelligence in clinical nutrition: bridging data analytics and nutritional care. Curr. Nutr. Rep. 2025;14(1):91. doi:10.1007/s13668-025-00680-x
32. Blajovan BL, Chirilă OS, Stănescu D, et al. Food Medicine-android-based food recognition app for guiding patients with nutritional diseases[C]//2023
33. Kaplan HC, Opipari-Arrigan L, Yang J. Personalized research on diet in ulcerative colitis and Crohn’s disease:a series of N-of-1 diet trials. Am J Gastroenterol. 2022;117(6): 117(6):902–917. doi:10.14309/ajg.0000000000001800
34. Arksey H, O’Malley L. Scoping studies:towards amethodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
35. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and Explanation. Ann Internal Med. 2018;169(7):467–473. doi:10.7326/M18-0850
36. Page MJ, McKenzie JE, Bossuyt PM. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. 2021(372):71.
37. Truman E, Lane D, Elliott C. Defining food literacy: a scoping review. Appetite. 2017;116:365–371. doi:10.1016/j.appet.2017.05.007
38. Godoy-Brewer GM, Jiang C, Khakoo NS, et al. A short dietary screener captures food items and dietary patterns that associate with inflammation in inflammatory bowel disease. Crohn’s Colitis. 2025;7(4):otaf052. doi:10.1093/crocol/otaf052
39. Suarez RGS, McClement DG, Vega R, et al. Using machine learning to predict clinical remission with exclusive enteral nutrition in pediatric Crohn disease. J Pediatr Gastroenterol Nutr. 2025;82:465–476. doi:10.1002/jpn3.70299
40. Boodaghidizaji M, Jungles T, Chen T, et al. Machine learning based gut microbiota pattern and response to fiber as a diagnostic tool for chronic inflammatory diseases. BMC Microbiol. 2025;25(1):353. doi:10.1186/s12866-025-04072-7
41. Lupusoru R, C ML, Mare R, et al. AI-guided multi-omic microbiome modulation improves clinical and inflammatory outcomes in refractory ibd: a real-world study. Int J Mol Sci. 2025;27(1):201. doi:10.3390/ijms27010201
42. Samaan JS, Issokson K, Feldman E, et al. Examining the accuracy and reproducibility of responses to nutrition questions related to inflammatory bowel disease by generative pre-trained transformer-4. Crohn’s Colitis. 2025;7(1):otae077. doi:10.1093/crocol/otae077
43. Onwuka S, Bravo-Merodio L, V GG, et al. Explainable AI-prioritized plasma and fecal metabolites in inflammatory bowel disease and their dietary associations. iScience. 2024;27(7):110298. doi:10.1016/j.isci.2024.110298
44. Rotondo-Trivette S, C CV, Mathur K, et al. Artificial intelligence- and physician-interpreted stool image characteristics correlate with c-reactive protein among inpatients with acute severe ulcerative colitis: a pilot study. Crohn’s Colitis. 2024;6(3):otae043. doi:10.1093/crocol/otae043
45. Naqvi HA, Delungahawatta T, O AJ, et al. Evaluation of online chat-based artificial intelligence responses about inflammatory bowel disease and diet. Eur J Gastroenterol Hepatol. 2024;36(9):1109–1112. doi:10.1097/MEG.0000000000002815
46. T RD, Torres J, Dotan I, et al. An insight into patients’ perspectives of ulcerative colitis flares via analysis of online public forum posts. Inflamm. Bowel Dis. 2024;30(10):1748–1758. doi:10.1093/ibd/izad247
47. Sun S, Hu Y, Li H, et al. Patients’ perspectives on, experience with and concerns about crohn’s disease: insights from Chinese social media. BMC Gastroenterol. 2023;23(1):105. doi:10.1186/s12876-023-02747-x
48. Yuping C, Haili X, Dai Y, et al. Application research of artificial intelligence bowel sound monitoring in judging the timing of postoperative feeding in patients with crohn’s disease. Chinese J of General Sur. 2023;38(3):595–599.
49. He H, Liu C, Chen M, et al. Effect of dietary patterns on inflammatory bowel disease: a machine learning bibliometric and visualization analysis. Nutrients. 2023;15(15):3442. doi:10.3390/nu15153442
50. Limketkai BN, Hamideh M, Shah R, et al. Dietary patterns and their association with symptoms activity in inflammatory bowel diseases. Inflamm. Bowel Dis. 2022;28(11):1627–1636. doi:10.1093/ibd/izab335
51. Stemmer M, Parmet Y, Ravid G. Identifying patients with inflammatory bowel disease on twitter and learning from their personal experience: retrospective cohort study. J. Med. Internet Res. 2022;24(8):e29186. doi:10.2196/29186
52. Lockwood C, Dos Santos KB, Pap R. Practical guidance for knowledge synthesis: scoping review methods. Asian Nurs. Res. 2019;13(5):287–294. doi:10.1016/j.anr.2019.11.002
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Stem Cell Therapy in Inflammatory Bowel Disease: A Review of Achievements and Challenges

Tian CM, Zhang Y, Yang MF, Xu HM, Zhu MZ, Yao J, Wang LS, Liang YJ, Li DF
Journal of Inflammation Research 2023, 16:2089-2119
Published Date: 16 May 2023
A Multicentre Study of the Clinical and Epidemiological Profile of Inflammatory Bowel Disease in Northeast Brazil
Brito CAA, Celani LMS, Araújo MVTD, Lucena MT, Vasconcelos GBS, Lima GAS, Nóbrega FJF, Diniz GTN, Lucena-Silva N, Toneto GT, Falcão JVDC, Barbosa PM, Oliveira PRFD, Dantas LSX, Fernandes LKC, Araújo SAD, Martinelli VF
Clinical and Experimental Gastroenterology 2023, 16:87-99
Published Date: 21 June 2023
Cytomegalovirus Pneumonia in Inflammatory Bowel Disease: Literature Review and Clinical Recommendations
Ren K, Yong C, Wang Y, Wei H, Zhao K, He B, Cui M, Chen Y, Wang J
Infection and Drug Resistance 2023, 16:6195-6208
Published Date: 13 September 2023
Microbial Disruptions in Inflammatory Bowel Disease: A Comparative Analysis
Ma J, Wang K, Wang J, Zeng Q, Liu K, Zheng S, Chen Y, Yao J
International Journal of General Medicine 2024, 17:1355-1367
Published Date: 6 April 2024
Dissecting Innate and Adaptive Immunity in Inflammatory Bowel Disease: Immune Compartmentalization, Microbiota Crosstalk, and Emerging Therapies

Yue N, Hu P, Tian C, Kong C, Zhao H, Zhang Y, Yao J, Wei Y, Li D, Wang L
Journal of Inflammation Research 2024, 17:9987-10014
Published Date: 29 November 2024