Back to Journals » Infection and Drug Resistance » Volume 19
Artificial Intelligence for Antimicrobial Resistance Detection and Prediction in Klebsiella pneumoniae: A Systematic Review of Clinical Microbiology Applications
Authors Aggarwal RV ![]() , Shah N, Wong JJE
, Shah N, Wong JJE ![]() , Dajani Z
, Dajani Z
Received 3 April 2026
Accepted for publication 6 May 2026
Published 3 June 2026 Volume 2026:19 614240
DOI https://doi.org/10.2147/IDR.S614240
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Raghav Vinay Aggarwal,1 Nisarg Shah,2 Jolie Jin En Wong,3 Zaid Dajani4
1Imperial College Healthcare NHS Trust, London, UK; 2Department of Diabetes, Endocrinology and Metabolism, Hull Royal Infirmary, Hull, UK; 3School of Medicine, Cardiff University, Cardiff, UK; 4College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Raghav Vinay Aggarwal, Hammersmith Hospital, Imperial College Healthcare NHS Trust, Du Cane Road, London, W12 0HS, UK, Tel +447541192979, Email [email protected]
Background: Klebsiella pneumoniae is a WHO critical-priority pathogen associated with a substantial antimicrobial resistance (AMR) burden. Conventional microbiology workflows, including antimicrobial susceptibility testing, often require 36– 72 hours, prolonging empirical therapy and contributing to antibiotic overuse. Artificial intelligence (AI) has emerged as a promising approach for enhancing the detection and prediction of antimicrobial resistance.
Methods: We searched four databases (PubMed, EMBASE, MEDLINE, and CENTRAL) from 1 January 2010 to 3 January 2026 for peer-reviewed, original research studies evaluating AI methods for the detection and/or prediction of AMR in K. pneumoniae. Studies without K. pneumoniae-specific extractable outcomes were excluded. Data on study characteristics, input modalities, AI methods, performance, workflow gains, and validation methods were extracted and narratively synthesised. Risk of bias was assessed using PROBAST and QUADAS-2 according to study design.
Results: Fifty-seven studies were included, with publication output accelerating sharply in 2024– 2025 (27/57, 47.4%). Most studies originated from East Asia and predominantly aimed to classify resistance phenotypes from pre-AST data (37/57, 64.9%) using machine learning approaches. MALDI-TOF mass spectrometry was the most common input modality (27/57, 47.4%), followed by genomic sequencing and vibrational spectroscopy (12/57 each, 21.1%). Random forests were the most frequently studied model family (28/57, 49.1%), with high reported discrimination. Among AUROC/AUC-primary studies, 26/35 (74.3%) reported best-model performance ≥ 0.90; however, overall risk of bias was high, present in 45/57 studies (78.9%). Internally validated study designs predominated, with external validation reported in only 17/57 studies (29.8%), and prospective, real-world evaluation in 1/57.
Conclusion: AI-based AMR prediction and detection in K. pneumoniae is advancing rapidly, with MALDI-TOF-enabled approaches appearing most readily translatable to clinical microbiology workflows. However, the field remains dominated by retrospective, internally validated studies, often using imperfect automated susceptibility systems as reference standards. Progress now depends on rigorous external and prospective multicentre validation using geographically diverse datasets.
Plain Language Summary: Klebsiella pneumoniae is a bacterium that can cause serious infections, especially in people admitted to hospital. Many strains are now resistant to antibiotics, which means some medicines no longer work well. Standard laboratory tests to find the right antibiotic usually take 36 to 72 hours. During this time, doctors often need to start treatment with broad-spectrum antibiotics before the full results are ready, which can contribute to antibiotic resistance.
We reviewed published studies to understand whether artificial intelligence (AI) could help identify antibiotic resistance in Klebsiella pneumoniae more quickly. AI is a type of computer system that can look for patterns in complex data. We found 57 studies published between 2018 and 2025. Most looked at whether AI could use information already produced in the microbiology laboratory, especially from a common test called “MALDI-TOF mass spectrometry” (a test that identifies bacteria from their protein “fingerprint”), to predict resistance earlier than standard testing.
Studies predominantly originated from East Asia. Most reported good accuracy, and almost half said AI could provide faster results than usual laboratory methods. This means AI could help doctors choose better antibiotics sooner and reduce unnecessary use of broad-spectrum treatment.
However, we identified some important limitations. Most studies tested the AI on past data rather than in real-time patient care. In some studies, the AI learned from automated systems rather than the best available (“gold standard”) methods, meaning it may reproduce their weaknesses. More real-world studies across different hospitals are needed before AI can be used safely.
Keywords: Klebsiella, artificial intelligence, machine learning, deep learning, antimicrobial resistance, systematic review
Introduction
Antimicrobial resistance (AMR) is one of the most defining global health challenges of the 21st century, with recent projections estimating more than 39 million deaths attributable to AMR by 2050.1 Within this context, the World Health Organization (WHO) has designated the Enterobacteriaceae family, a clinically important group of pathogens that includes Klebsiella pneumoniae (K. pneumoniae; KP), as “Priority 1: Critical” for urgent research and development of new antibiotics. K. pneumoniae is a Gram-negative bacterium implicated in both hospital-acquired and community-acquired infections, and its marked capacity to acquire multidrug resistance mechanisms - particularly extended-spectrum β-lactamases (ESBLs) and carbapenemase enzymes such as KP carbapenemase (KPC), New Delhi metallo-β-lactamase (NDM) and oxacillinase-48 (OXA-48) - has contributed to substantial morbidity and mortality worldwide.2,3
Antibiotic selective pressure is a major driver of the evolving multidrug resistance profile of KP.4 Appropriate antibiotic prescribing is therefore a critical strategy for limiting the emergence and spread of resistance.5 However, efforts to reduce inappropriate antibiotic use and reliance on empirical therapy are frequently hindered by time-consuming, conventional pathogen identification and antimicrobial susceptibility testing (AST).6 Key rate-limiting steps include primary specimen culture for bacterial growth and isolation (6–18 hours), followed by phenotypic susceptibility testing by broth microdilution for minimum inhibitory concentration (MIC) determination or Kirby-Bauer disc diffusion, with clinically actionable results often only available 36–72 hours after sample collection.7 Collectively, these time-dependent processes underscore the need for more rapid diagnostics and innovative approaches to resistance detection and susceptibility prediction that could improve clinical microbiology workflows and support antimicrobial stewardship.8
Recent advances in machine learning (ML) and deep learning (DL) have accelerated interest in artificial intelligence (AI)-enabled diagnostics across healthcare, including AMR detection and susceptibility prediction.9 ML refers to data-trained algorithms that can identify patterns and support prediction or decision-making without being explicitly programmed for each rule.10 One example is the application of ML to MALDI-TOF mass spectrometry data to predict antimicrobial susceptibility in Staphylococcus aureus, enabling earlier resistance inference from routinely generated spectra, with strong reported discrimination.11 In contrast, deep learning is a subtype of ML that uses multilayer “neural networks” to analyse larger or more complex data and learn more detailed patterns automatically. For example, a recent experimental, proof-of-concept deep learning study used single-cell image analysis to enable rapid phenotypic susceptibility assessment in Escherichia coli within 30 minutes.12 Limitations to the implementation of AI technologies are also increasingly recognised, including insufficient model explainability, lack of prospective and external validation, under-representation of diverse populations in model development and evaluation datasets, and substantial heterogeneity across study designs, inputs, outcomes and reference standards.13,14
Given the pace of AI model development and the clinical urgency posed by drug-resistant K. pneumoniae, there is a clear need to synthesise and critically evaluate the emerging literature on AI-driven AMR detection and prediction in this pathogen. This species is of particular interest for AI-related research because it combines substantial genomic diversity, frequent acquisition of resistance determinants, and increasingly large publicly available genomic and routine microbiology datasets, creating information-rich patterns that may be well suited to AI-based AMR detection and prediction.15,16 This systematic review therefore aims to evaluate the contemporary evidence base in this area, with three key objectives: (i) to characterise the AI methods being used and the input data modalities on which they rely, (ii) to identify the best-performing approaches across antimicrobial resistance detection tasks (such as resistance mechanism detection or accelerated phenotypic AST) and prediction tasks (such as resistance phenotype inference or MIC prediction from pre-AST data), and (iii) to critically appraise validation practices, generalisability, and study design to judge clinical readiness. By mapping this field, we aim to inform future research priorities and identify the steps needed to support the translation of credible AI tools into clinical microbiology workflows worldwide.
Methods
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (PRISMA checklist provided in Supplementary Material S2). The protocol for this systematic review was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) under registration number CRD420251238578. No post-registration changes materially altered the review question, eligibility criteria, search strategy, or planned approach to synthesis.
Information Sources
Electronic searches were conducted in PubMed, EMBASE (Ovid), MEDLINE (Ovid), and the Cochrane Central Register of Controlled Trials (CENTRAL) from database inception to the final search date (3 January 2026). To focus on contemporary AI applications, we restricted eligibility to studies published from 1 January 2010 to 3 January 2026. Only English-language articles were considered, with no restrictions by geography or clinical setting.
Search Strategy
The search strategy was developed around three core concepts combined with Boolean operators: (1) AI terminology, including common machine learning and deep learning terms, (2) Klebsiella pneumoniae, and (3) AMR detection and prediction terms, including resistance, susceptibility, AST/MIC and resistance mechanism-related terminology. Controlled vocabulary terms (eg., MeSH and Emtree) were combined with free-text keywords to maximise sensitivity. A broad Klebsiella MeSH-based strategy was used in PubMed to enhance capture of relevant records. The PubMed strategy was benchmarked against eight pre-identified studies (KP006, KP008, KP007, KP010, KP015, KP039, KP051, KP036) to confirm sensitivity. Full search strategies for each database are provided in Supplementary Material S1. The search strategy was developed by the primary reviewer and peer-reviewed by a senior researcher prior to execution.
Eligibility Criteria
Studies were eligible if they were peer-reviewed, original research articles evaluating an artificial intelligence model as the primary analytical approach for detecting and/or predicting antimicrobial resistance in KP, with direct relevance to hospital-based clinical microbiology workflows. For multi-organism datasets, studies were included only if K. pneumoniae-specific outcomes could be extracted. Eligible studies were also required to define antimicrobial resistance using a clearly stated reference standard, such as culture-based antimicrobial susceptibility testing or minimum inhibitory concentration determination, and to report quantitative performance metrics, including area under the receiver operating characteristic curve, sensitivity, specificity, accuracy, positive predictive value, or negative predictive value.
Studies were excluded if they were not peer-reviewed or did not present original research, including reviews, editorials, protocols, conference abstracts, theses, book chapters, and preprints. Studies were also excluded if they reported only pooled multi-species performance, if artificial intelligence was not the primary analytical method, or if they relied solely on conventional statistical approaches. Additional exclusions applied to studies focussed on population-level antimicrobial resistance surveillance, ecological or national trend modelling, clinical decision-support systems beyond the isolate or specimen level (eg., outbreak forecasting), pathogen identification without antimicrobial resistance detection or prediction, non-human health contexts, antimicrobial drug discovery, or genomic analyses without a clear translational link to routine clinical microbiology workflows. Studies lacking a clearly defined reference standard for resistance determination were also excluded.
Study Selection
The search yielded 1013 records. All retrieved records were imported into Rayyan for de-duplication and screening. After duplicate removal, 646 unique studies remained for assessment. Study selection was conducted in two stages: initial title and abstract screening followed by full-text review of eligible articles. Screening at both stages was performed independently by two reviewers (R.A. and N.S). Disagreements were resolved through discussion and consensus, with referral to a senior reviewer when necessary. The final number of included studies was fifty-seven (see PRISMA flow diagram, Figure 1), each assigned to a unique study identifier (KP001-KP057).
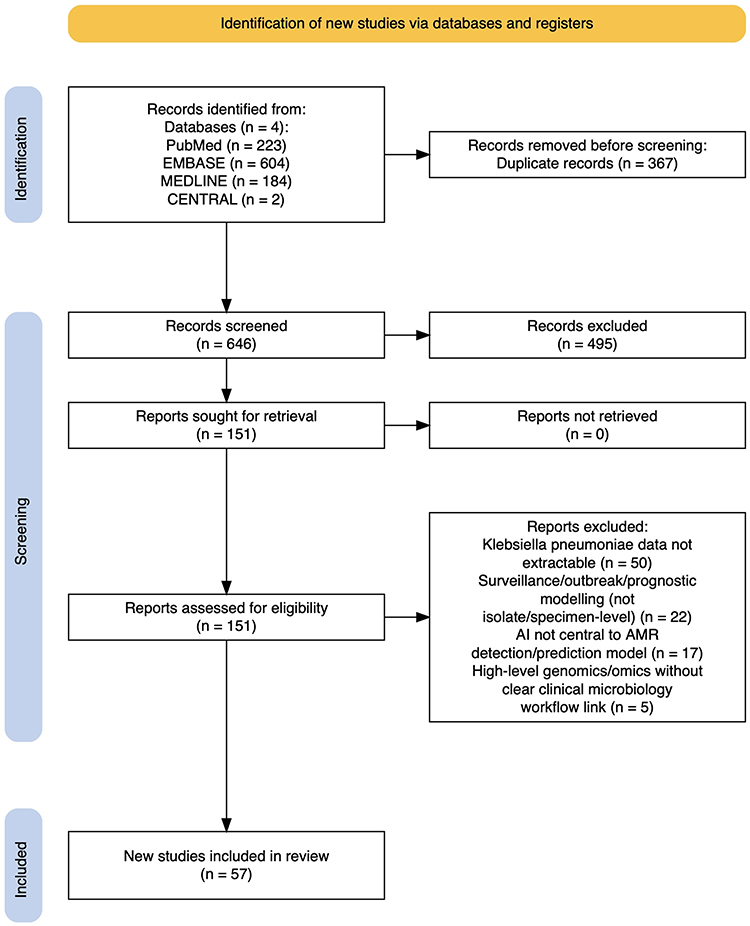 |
Figure 1 PRISMA 2020 flow diagram of study selection. Records were identified through four bibliographic databases (PubMed, EMBASE, MEDLINE and CENTRAL). Following de-duplication, 646 unique records remained and were screened by title and abstract. 495 were excluded. Full texts were sought for 151 reports; all were retrieved and assessed for eligibility. Ninety-four reports were excluded at full-text review, most commonly because KP-specific data were not extractable (n=50). Fifty-seven studies were included in the final review. Figure created using the PRISMA2020 Shiny app.17 |
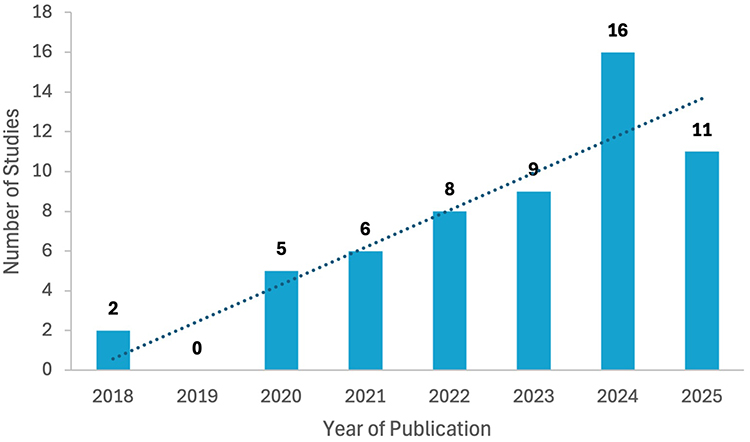 |
Figure 2 Annual publication of included studies. Bar chart showing the number of eligible studies published per year between 2018 and 2025. Values are annotated above bars; the dotted line indicates the linear publication trend. |
 |
Figure 3 Geographic distribution of dataset sources. Choropleth map showing the reported country of origin of datasets used for model training and/or validation. Multi-country datasets were disaggregated so that a single study could contribute counts to more than one country. Dataset origin was most frequently reported as China (n=16), Taiwan (n=10) and the USA (n=8). A minority of studies used international public datasets (n=5) or other unspecified public data sources (n=2) and so were not attributed to a specific country on the map. Figure created using Datawrapper (https://www.datawrapper.de). |
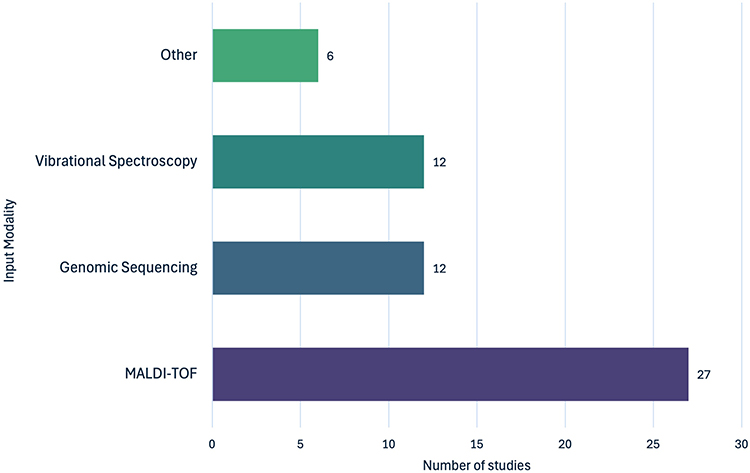 |
Figure 4 Primary input modalities used for AI modelling across included studies. Bar chart summarising the primary input modality reported in each study. The three dominant modalities were MALDI-TOF MS spectra, followed by genomic sequencing data (including whole-genome sequencing and metagenomic data) and vibrational spectroscopy (Raman or Fourier-transform infrared spectroscopy). The remaining studies were grouped as “other” (6/57), comprising image analysis (including disk diffusion antibiogram photographs and time-lapse single-cell imaging; n=2), nanomotion technology (n=2), flow cytometry (n=1) and MIC results from routine AST-derived data (n=1). |
Data Extraction and Risk of Bias Assessment
Data were extracted into a prespecified Excel framework developed by R.A., organised across five domains: (1) study characteristics, (2) study aims, (3) inputs, AI methods and reference standards, (4) performance outcomes, and (5) validation approaches and study conclusions. Extraction was performed by R.A. and independently verified by J.W.
For performance outcomes, where studies assessed multiple candidate algorithms, we extracted results for the authors’ prespecified primary model where stated. If no primary model was nominated, we selected the single best-performing model according to the study’s primary endpoint. Where multiple related metrics were reported without an explicitly defined primary endpoint, AUROC/AUC was prioritised for discrimination tasks, followed by accuracy, F1-based metrics, and categorical agreement; this rule was applied consistently across studies.
Risk of bias (RoB) and applicability concerns were assessed at the study level using validated tools selected according to study design and primary analytical aim. RoB and applicability assessments were treated as separate methodological judgements and were analysed independently. RoB assessed methodological validity, whereas applicability assessed relevance to the review question and intended clinical context. Studies developing or validating multivariable AI prediction models for antimicrobial resistance were appraised using PROBAST, whereas studies framed primarily as diagnostic test accuracy evaluations (index test versus reference standard) were assessed using QUADAS-2.18,19 Domain-level judgements were recorded as “low”, “high”, or “unclear” risk of bias. For PROBAST-assessed studies, risk of bias was evaluated across four domains - participants, predictors, outcome and analysis - with separate applicability judgements for participants, predictors and outcome. For QUADAS-2, risk of bias was evaluated across patient selection, index test, reference standard, flow and timing, with applicability assessed for patient selection, index test and reference standard. RoB and applicability assessments were conducted independently by N.S. and Z.D., with discrepancies resolved by consensus and R.A. adjudicating where required.
Given the anticipated heterogeneity in study designs, modelling approaches, target outcomes, and performance reporting, findings were synthesised narratively. To facilitate narrative synthesis, studies were grouped by primary clinical objective, input modality, AI model category, performance endpoint, validation approach, reference standard, and risk-of-bias tool assignment. Results were presented using descriptive summary tables and figures, including a publications-per-year plot, a geographic mapping of dataset sources, an input data modalities plot, and tabulated summaries of AI model categories, workflow time gains, and risk of bias judgements.
Results
Study Characteristics
A total of 57 studies, published between 2018 and 2025, were included.20–76 Publication output increased over time, with nearly half of all studies published in 2024–2025 (27/57, 47.4%; Figure 2). Dataset sources were geographically concentrated, particularly in East Asia (China and Taiwan), with limited representation from other high-AMR regions (Figure 3). Funding status was reported in 54 studies, of which 50 (92.6%) disclosed government, academic or hospital support.
Detailed study-level characteristics, primary objectives, input modalities, AI methods, reference standards, performance outcomes, validation approaches and study conclusions are provided in Supplementary Material S3.
Clinical Objectives & Input Modalities
Aims and Clinical Objectives
Primary clinical objectives were grouped into four categories. The most common objective was resistance phenotype classification from pre-AST data (37/57; 64.9%), in which models classified K. pneumoniae isolates as susceptible or resistant to specific antibiotics (most commonly carbapenems, ciprofloxacin, and colistin). Fewer studies focussed on resistance mechanism identification (10/57; 17.5%), including the detection of carbapenemase production, extended-spectrum β-lactamase (ESBL) production, or specific resistance determinants such as KPC, NDM and OXA-48. Rapid AST prediction and MIC prediction were each uncommon, with 5/57 studies each (8.8%). Rapid AST studies aimed to accelerate phenotypic susceptibility classification from AST-derived signals, whereas MIC prediction studies sought to estimate quantitative susceptibility values directly.
Antibiotics and Resistance Mechanisms
Carbapenems, particularly meropenem, imipenem and ertapenem, were the most frequently studied class, appearing as a primary target in 34/57 studies (59.6%). Other commonly studied antibiotics included ciprofloxacin (25 studies), colistin (11 studies), and third- or fourth-generation cephalosporins, such as ceftazidime and cefepime. Among studies targeting resistance mechanisms (n=10), primary targets included carbapenemase-producing KP (CPK), ESBL production, and carbapenemase-encoding genes, including blaKPC, blaNDM, and blaOXA-48.
Input Modalities
Three input modalities accounted for 89.5% of included studies (Figure 4). MALDI-TOF MS was the most common input modality (27/57 studies, 47.4%), followed by genomic sequencing data and vibrational spectroscopy (12/57 each, 21.1%).
AI Modelling Approaches
Most studies used machine learning (ML) methods alone (38/57; 66.7%), whereas deep learning (DL) alone was less common (9/57, 15.8%). A further nine studies evaluated both ML and DL in parallel, and one implemented a hybrid pipeline (autoencoder-SVM, KP056). Across algorithm families, random forests (RF) and gradient-boosting methods were the most frequently evaluated (Table 1). Overall, 41/57 studies (71.9%) compared more than one candidate model, with the number of distinct models per study ranging from 1 to 8 (mean 2.8 models; median 2 models per study).
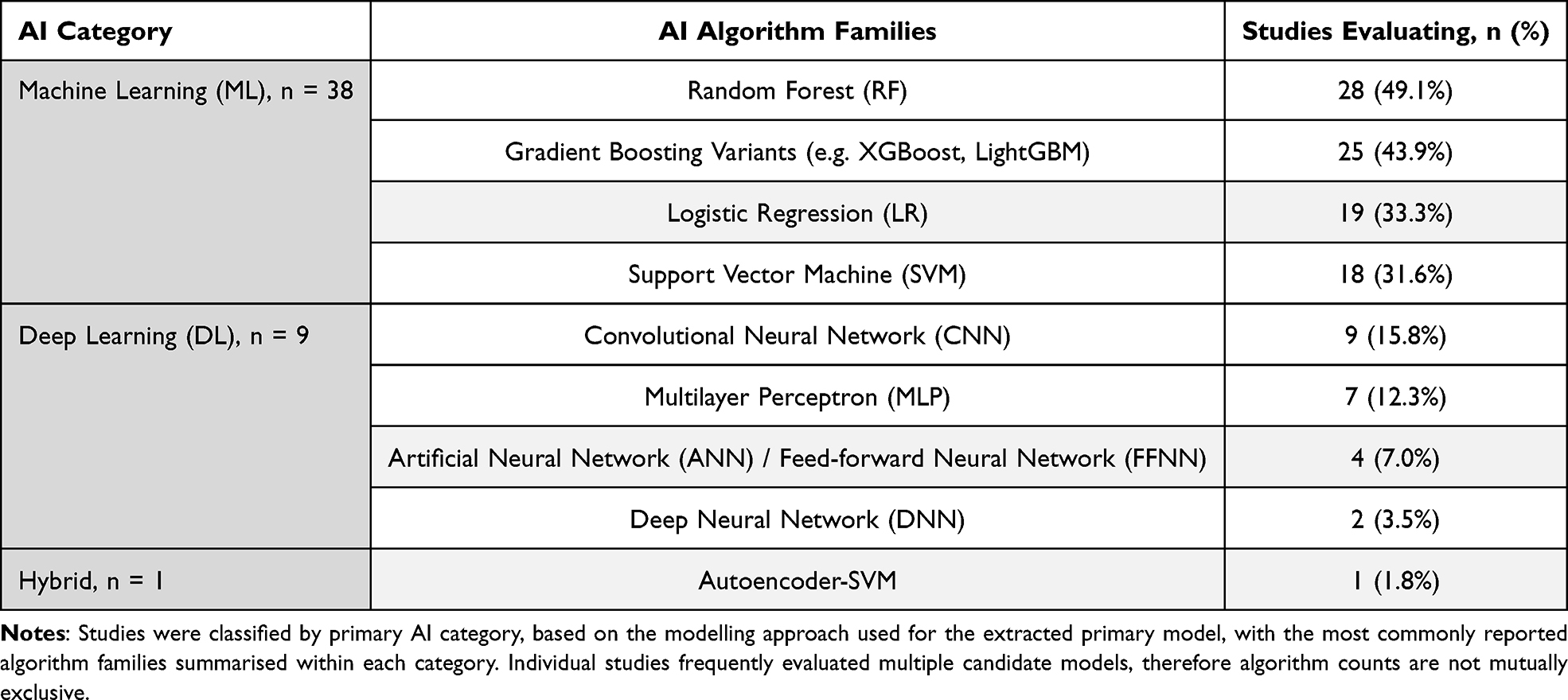 |
Table 1 AI Modelling Approaches and Commonly Evaluated Algorithm Families |
Model Performance, Validation and Reference Standards
Performance
Performance reporting was heterogeneous. AUROC/AUC was the primary endpoint in 35/57 studies (61.4%), whereas accuracy was primary in 16/57 (28.1%). Among AUROC/AUC-primary studies, 26/35 (74.3%) reported best-model performance of at least 0.90, and 21/35 (60.0%) reported performance of at least 0.95, although results varied across antibiotic targets. Random forest models were most often identified as best-performing (16/57 studies), followed by gradient-boosting methods (14/57 studies) and CNN-based models (9/57 studies).
Reported Workflow Time Improvements
Twenty-seven studies (47.4%) explicitly reported a workflow time advantage relative to conventional microbiology pathways. However, the analytical starting points for these comparisons were heterogeneous, ranging from urine sample receipt, initial culture, and blood culture positivity to post-species identification or post-sequencing data availability. Accordingly, time estimates should be interpreted as study-specific workflow improvements, rather than standardised sample-to-result turnaround times.
Thirteen studies reported time-to-result gains of less than 1 hour from their stated analytical start point (Supplementary Material S4), of which 6/13 (46.2%) used MALDI-TOF MS data as the input modality. A further three studies reported workflow improvements within 1–4 hours, including KP002 (AST results in 2–4h versus 24 hours with conventional AST), KP026 (reduced resistance detection time for KP to 1–2h using ML applied to MALDI-TOF MS data), and KP056 (culture incubation reduced to 4h versus 24 hours, corresponding to a 20h time benefit).
Where studies benchmarked against culture-based AST, the reported time advantage was typically framed as an approximately 24–48h-scale acceleration. Examples included up to 24 hours faster targeted antibiotic selection compared to conventional AST using an AI-clinical decision support system (KP001), AST results reported 1 day earlier than conventional routine diagnostics (KP037), and genotypic AST results with a mean turnaround time of 18.34 ± 0.87 h versus 60.15 ± 21.58 h for traditional culture-based AST (KP053).
Validation Reporting & Reference Standards
Internal validation was reported in 55/57 studies (96.5%), most commonly using k-fold cross-validation (typically 5–10 folds) in 36/55 studies, and, less often, hold-out train-test splitting alone (7/55). More rigorous approaches, such as nested cross-validation or bootstrapping, were rare. External validation using independent datasets was reported in 17/57 studies (29.8%), including evaluations using multi-site networks and public or previously published datasets such as the Database of Resistance Information on Antimicrobials and MALDI-TOF Mass Spectra (DRIAMS). One study reported a prospective, real-world diagnostic accuracy evaluation using newly collected samples (KP031). Temporal validation was described in 9/57 studies (15.8%), most often through chronological splits.
Reference standards for model training and validation were most often based on automated commercial systems such as VITEK 2 and BD Phoenix (29/57, 50.9%). The gold-standard broth microdilution (BMD) method was the primary reference in 9/57 studies (15.8%). The remaining studies relied on disk diffusion or gradient strips (n=7), unspecified MIC methods (n=6), or genotypic confirmation (n=4).
Risk of Bias
Across the fifty-seven included studies, overall risk of bias was judged high in 45/57 studies, and unclear in 12/57; no study met criteria for overall low risk. Among prediction-model studies assessed using PROBAST (n=24), high overall risk of bias was judged in 17/24 studies (7/24 unclear), driven mainly by the analysis domain (16/24 high) and participant selection (10/24 high), whereas the predictor domain was consistently low risk (24/24 low). Among diagnostic accuracy studies assessed using QUADAS-2 (n=33), 28/33 were rated high risk (5/33 unclear), predominantly due to patient selection (21/33 high) and index test (26/33 high). In contrast, the reference standard domain was generally low risk (24/33 low). Applicability concerns were also common, with high concern in 40/57 studies (PROBAST 17/24; QUADAS-2 23/33), low concern in 14/57 and unclear concern in 3/57.
Study-level domain judgements for PROBAST and QUADAS-2, including overall risk-of-bias and applicability assessments, are provided in Supplementary Material S5.
Discussion
The evidence base for artificial intelligence approaches to predicting and detecting antimicrobial resistance in Klebsiella pneumoniae has expanded rapidly. Across 57 studies published between 2018–2025, almost half appeared in 2024–2025, reflecting both accelerating technical capability and the growing urgency of drug-resistant KP as a global health priority. Notably, much of the recent work has pivoted towards machine learning applications for resistance phenotype prediction, leveraging routinely available hospital data streams such as MALDI-TOF mass spectrometry. However, this growth has not yet translated into demonstrable clinical readiness; although the best-performing models frequently reported high discrimination (AUROC commonly >0.90, with several exceeding 0.95), evaluation was dominated by internal resampling strategies, with relatively few studies undertaking independent external validation. This reliance on internal validation increases the risk of bias and raises concerns about the generalisability of these models across diverse clinical settings, laboratory platforms, and populations.
The predominance of MALDI-TOF MS as an input modality suggests a shift towards tools that can be embedded within existing microbiology workflows. By leveraging routinely generated data, MALDI-TOF-based models could, in principle, provide an early predictive layer of antimicrobial resistance prediction without additional wet-lab steps, equipment, or sample processing, offering a potentially low-cost route to earlier actionable information. This rationale is broadly supported by the time-to-result analyses reported in the literature: 27 studies explicitly quantified workflow acceleration, most commonly reporting an approximately 24-hour gain. However, these studies measured time gain from different starting points within the diagnostic pathway; therefore, the reported acceleration should be interpreted cautiously and in the context of each individual study, rather than as directly comparable end-to-end turnaround time reductions. Overall, the ability to extract clinically relevant proteomic or phenotypic signals from data already generated in the clinical laboratory suggests that MALDI-TOF-based prediction may represent one of the most readily implementable AI applications for earlier antimicrobial optimisation.
Beyond MALDI-TOF, the literature also explored alternative input modalities, including whole-genome sequencing (WGS), spectroscopic approaches (Raman/FTIR), and emerging phenotypic technologies such as nanomotion, many of which also reported strong discriminatory performance. Although some of these approaches offered ultra-rapid turnaround times in the range of minutes to hours, their translational pathway is complicated by limited existing infrastructure, such as dedicated nanomotion platforms and specialised analytical pipelines, and by a lack of demonstrable cost-effectiveness. While these studies provide a view of potentially rapid future diagnostic pathways, the uncertainty of the feasibility and scalability of these approaches means that MALDI-TOF-based strategies are likely to remain central to this research landscape in the near term. Of note, however, the single prospective, real-world diagnostic accuracy study identified in this review (KP031) evaluated a nanomotion-based platform rather than a MALDI-TOF-based approach. Given the emerging translational appeal of MALDI-TOF within existing laboratory workflows, prospective evaluation of MALDI-TOF-based AI models in routine clinical microbiology settings should now be considered a major priority for future research.
A central limitation of the current evidence base is the pronounced geographic skew in data sourcing, which raises concerns about the global transferability of the evaluated algorithms. Most datasets originated from East Asia, particularly China and Taiwan, with comparatively fewer studies from Europe and North America and a striking paucity of data from regions with a high AMR burden, such as sub-Saharan Africa and Latin America. This matters because K. pneumoniae is a genetically diverse pathogen, with geographically distinct high-risk clones and resistance determinants; for example, the ST11 sequence type predominates in much of Asia, whereas ST258 is more prominent in Europe and North America.77 As a result, models trained in settings dominated by specific high-risk clones or resistance determinants may underperform when lineage distributions or resistance mechanisms differ. This is particularly relevant to MALDI-TOF-based models, where spectra may exhibit clade-specific peak patterns; therefore, models trained on ST11-dominant datasets may generalise less well to ST258-predominant settings if resistance-associated peaks are lineage-dependent.42
Headline metrics may therefore reflect high performance within narrow epidemiological settings rather than robust discrimination across broader clinical contexts. Without external validation on geographically diverse cohorts, which was absent in nearly 70% of included studies, these models may remain overfitted to local epidemiology and thus unsuitable for broader deployment. Progressing from promising prototypes to deployable diagnostics will therefore require deliberate external validation across hospitals, regions, and time, using geographically diverse KP cohorts.
With respect to AI model types, we observed a preference for evaluating “traditional” machine learning models, most commonly random forests, which were both the most frequently studied and the most often reported as best-performing, alongside gradient-boosting variants and support vector machines. Importantly, however, random forests are also frequently used as comparator or benchmark models in applied ML studies; therefore, their apparent prominence in this review should not be taken to imply that they are inherently superior to other model classes across all translational settings. This pattern is nevertheless consistent with the characteristics of many routinely available microbiology input datasets; MALDI-TOF data are typically structured and often available in relatively modest sample sizes, conditions under which tree-based methods such as random forests can perform strongly while remaining less vulnerable than more complex models to overfitting.78–80 In contrast, deep learning approaches were used more selectively, with convolutional neural networks (CNNs) generally applied to more complex or less structured data types, such as SERS spectra (KP054) and raw nanomotion signals (KP002).
A critical translational consideration is whether these models are sufficiently interpretable to support safe clinical decision-making. Deep learning models, for example, are often described as “black-box” systems because the basis of their predictions may be difficult to interpret.81 In clinical settings where false susceptibility predictions could contribute to treatment failure, the interpretability of an algorithm therefore becomes an important determinant of trust and adoption of AI in healthcare.82 The growing emphasis on “explainable AI” may therefore favour simpler but more transparent machine learning approaches over deep learning in some clinical applications, despite the latter’s promise for accelerating microbiology workflows.
A central consideration for accurate antimicrobial resistance prediction is the quality of the “ground truth” labels used to train and evaluate models. Model performance is therefore constrained by the quality of the reference data on which those labels are based. A primary limitation of the current evidence base is the frequent use of imperfect automated commercial susceptibility systems, rather than reference-grade phenotypic methods, as the ground truth for model training and evaluation. In the reviewed literature, just over half of studies used automated commercial systems, particularly VITEK 2 and BD Phoenix, as the reference comparator. In contrast, only a minority employed the gold-standard, reference-grade broth microdilution (BMD) method. This distinction is important, as although automated systems are operationally more efficient, they have recognised limitations, including historical inaccuracies in identifying KPC-producing organisms and poor reliability for some targets such as colistin resistance in KP.83,84
Accordingly, when AI models are trained to reproduce the output of automated systems rather than reference-grade phenotypic methods such as BMD, they risk a form of diagnostic “mimicry” – a concept which can be defined as the reproduction of the comparator’s limitations within the model’s predictions. In clinical settings, this could have important downstream consequences if erroneous susceptibility predictions influence early treatment decisions. For AI to represent a genuine advance in diagnostic precision in KP, future model development should prioritise high-quality phenotypic reference data rather than highly performing models that function primarily as faster proxies for existing automated systems. Future studies should also specify whether the intended use of their AI approach is early approximation of routine AST for triage or stewardship support, or definitive reference-standard susceptibility inference. Validation and reporting should then be aligned accordingly, so that clinicians can judge how these tools might support practice without compromising patient safety.
Strengths and Limitations
This systematic review has several important strengths, including prospective registration on PROSPERO and rigorous adherence to PRISMA 2020 principles. Additionally, it is based on a comprehensive four-database search, with dual independent screening, structured data extraction (with full transparency of additional extracted variables provided in the Supplementary Material), and the use of validated risk-of-bias tools (PROBAST and QUADAS-2). Its pathogen-specific focus on K. pneumoniae and its translational emphasis on clinical microbiology workflows also enabled a more focussed and detailed synthesis of input modalities, validation practices, workflow claims and reference standards.
However, limitations of the study are also acknowledged. The evidence base was highly heterogeneous in study design, objectives, model types, outcomes, and reference standards, which precluded formal meta-analysis. The review was also constrained by the quality and completeness of reporting in the included studies. Finally, the exclusion of preprints, conference abstracts, and other forms of grey literature may act as a source of publication bias, potentially omitting very recent technical developments or studies with negative or non-significant results in this rapidly evolving field.
Conclusion
In summary, over the last decade, artificial intelligence approaches for Klebsiella pneumoniae AMR prediction and detection have emerged as promising strategies for accelerating the availability of clinically actionable susceptibility information. Many of the most promising models draw on signals already generated within routine microbiology workflows, particularly MALDI-TOF mass spectra, offering a plausible route to an early susceptibility layer at, or shortly after, species identification. If validated and implemented safely, AI-based approaches could substantially shorten diagnostic turnaround, reducing reliance on empirical therapy and enabling more timely de-escalation of antibiotics where appropriate, thus strengthening antimicrobial stewardship while conventional AST is pending.
Despite this progress, the evidence base remains dominated by retrospective, in silico prototyping, with relatively few studies progressing to the prospective, multicentre evaluation needed for safe clinical translation. Addressing this gap should now be a central priority for this field. Future work should shift from repeated model development towards rigorous external validation of the most promising approaches under realistic epidemiological shifts, laboratory platform variation and operational constraints. At the same time, stronger reference-standard integrity is essential: AI models intended for clinical translation should be trained and validated against reference-grade phenotypic comparators – ideally broth microdilution where appropriate – rather than imperfect automated systems, to reduce the risk of reproducing and amplifying existing diagnostic limitations. Broader international representation is also essential, particularly through inclusion of currently underrepresented high-AMR settings across African and Latin American healthcare systems, to improve transferability and avoid widening global inequities in diagnostic innovation. Priority should also remain with workflow-compatible strategies, especially MALDI-TOF-enabled approaches that can be embedded in existing laboratory pathways without requiring new, rate-limiting infrastructure. Finally, clearer intended-use framing is needed, explicitly distinguishing early approximation of routine AST for triage or stewardship support from definitive phenotypic susceptibility prediction, with validation and reporting aligned to that distinction.
Data Sharing Statement
The principal extracted study-level data and derived summary tables underlying this review are provided in the manuscript and Supplementary Information. Further extracted variables and supporting materials are available from the corresponding authors upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Naghavi M, Vollset SE, Ikuta KS, GBD 2021 Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. Lancet. 2024;404(10459):1199–15. doi:10.1016/S0140-6736(24)01867-1
2. Zheng S, Li S, Zhang D, et al. The mechanisms of antibiotic resistance and drug resistance transmission of Klebsiella pneumoniae. J Antibiot. 2025;78(12):704–716. doi:10.1038/s41429-025-00860-5
3. Navon-Venezia S, Kondratyeva K, Carattoli A. Klebsiella pneumoniae: a major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol Rev. 2017;41(3):252–275. doi:10.1093/femsre/fux013
4. Li J, Shi Y, Song X, Yin X, Liu H. Mechanisms of antimicrobial resistance in Klebsiella: advances in detection methods and clinical implications. Infect Drug Resist. 2025;18:1339–1354. doi:10.2147/IDR.S509016
5. Ha DR, Haste NM, Gluckstein DP. The role of antibiotic stewardship in promoting appropriate antibiotic use. Am J Lifestyle Med. 2017;13(4):376–383. doi:10.1177/1559827617700824
6. Edmondson R, Saeed K, Green S, O’Dwyer M. Improving turnaround times for routine antimicrobial sensitivity testing following European Committee on antimicrobial susceptibility testing methodology in patients with bacteraemia. Antibiotics. 2024;13(11):1094. doi:10.3390/antibiotics13111094
7. Burnham CD, Leeds J, Nordmann P, O’Grady J, Patel J. Diagnosing antimicrobial resistance. Nat Rev Microbiol. 2017;15(11):697–703. doi:10.1038/nrmicro.2017.103
8. Maurer FP, Christner M, Hentschke M, Rohde H. Advances in rapid identification and susceptibility testing of bacteria in the clinical microbiology laboratory: implications for patient care and antimicrobial stewardship programs. Infect Dis Rep. 2017;9(1):6839. doi:10.4081/idr.2017.6839
9. Li Y, Cui X, Yang X, Liu G, Zhang J. Artificial Intelligence in predicting pathogenic microorganisms’ antimicrobial resistance: challenges, progress, and prospects. Front Cell Infect Microbiol. 2024;14:1482186. doi:10.3389/fcimb.2024.1482186
10. Kufel J, Bargieł-łączek K, Kocot S, et al. What Is Machine Learning, Artificial Neural Networks and Deep Learning? Examples of Practical Applications in Medicine. Diagnostics. 2023;13(15):2582. doi:10.3390/diagnostics13152582
11. Zhang J, Wang Z, Wang H-Y, et al. Rapid antibiotic resistance serial prediction in Staphylococcus aureus based on large-scale MALDI-TOF data by applying XGBoost in multi-label learning. Front Microbiol. 2022;13:853775. doi:10.3389/fmicb.2022.853775
12. Zagajewski A, Turner P, Feehily C, et al. Deep learning and single-cell phenotyping for rapid antimicrobial susceptibility detection in Escherichia coli. Commun Biol. 2023;6(1):1164. doi:10.1038/s42003-023-05524-4
13. Pinto A, Pennisi F, Ricciardi GE, Signorelli C, Gianfredi V. Evaluating the impact of artificial intelligence in antimicrobial stewardship: a comparative meta-analysis with traditional risk scoring systems. Infectious Diseases Now. 2025;55(5):105090. doi:10.1016/j.idnow.2025.105090
14. Pinto A, Pennisi F, Odelli S, et al. Artificial Intelligence in the Management of Infectious Diseases in Older Adults: diagnostic, Prognostic, and Therapeutic Applications. Biomedicines. 2025;13(10):2525. doi:10.3390/biomedicines13102525
15. Holt KE, Wertheim H, Zadoks RN, et al. Genomic analysis of diversity, population structure, virulence, and antimicrobial resistance in Klebsiella pneumoniae, an urgent threat to public health. Proc Natl Acad Sci. 2015;112(27):E3574–E3581. doi:10.1073/pnas.1501049112
16. Spadar A, Perdigão J, Campino S, Clark TG. Large-scale genomic analysis of global Klebsiella pneumoniae plasmids reveals multiple simultaneous clusters of carbapenem-resistant hypervirulent strains. Genome Med. 2023;15(1). doi:10.1186/s13073-023-01153-y
17. Haddaway NR, Page MJ, Pritchard CC, McGuinness LA. PRISMA2020: an R package and Shiny app for producing PRISMA 2020-compliant flow diagrams, with interactivity for optimized digital transparency and open synthesis. Campbell Syst Rev. 2022;18(2):e1230. doi:10.1002/cl2.1230
18. Wolff RF, Moons KGM, Riley RD, et al. PROBAST: a tool to assess the risk of bias and applicability of Prediction model studies. Ann Intern Med. 2019;170(1):51–58. doi:10.7326/M18-1376
19. Whiting PF, Rutjes AWS, Westwood ME, et al. QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529–536. doi:10.7326/0003-4819-155-8-201110180-00009
20. Lin T-H, Chung H-Y, Jian M-J, et al. Accelerating antimicrobial stewardship: an AI-CDSS approach to combating multidrug-resistant pathogens in the era of increasing resistance. Clin Chim Acta. 2025;574:120336. doi:10.1016/j.cca.2025.120336
21. Sturm A, Jóźwiak G, Verge MP, et al. Accurate and rapid antibiotic susceptibility testing using a machine learning-assisted nanomotion technology platform. Nat Commun. 2024;15(1):2037. doi:10.1038/s41467-024-46213-y
22. Avershina E, Sharma P, Taxt AM, et al. Amr-Diag: neural network based genotype-to-phenotype prediction of resistance towards β-lactams in Escherichia coli and Klebsiella pneumoniae. Comput Struct Biotechnol J. 2021;19:1896–1906. doi:10.1016/j.csbj.2021.03.027
23. Gato E, Constanso IP, Candela A, et al. An improved matrix-assisted laser desorption ionization-time of flight mass spectrometry data analysis pipeline for the identification of carbapenemase-producing Klebsiella pneumoniae. J Clin Microbiol. 2021;59(7):e00800. doi:10.1128/JCM.00800-21
24. Rajaonison A, Le Page S, Maurin T, et al. Antilogic, a new supervised machine learning software for the automatic interpretation of antibiotic susceptibility testing in clinical microbiology: proof-of-concept on three frequently isolated bacterial species. Clin Microbiol Infect. 2022;28(9):1286. doi:10.1016/j.cmi.2022.03.035
25. Lin T-H, Chung H-Y, Jian M-J, et al. Artificial Intelligence-clinical decision support system for enhanced infectious disease management: accelerating ceftazidime-avibactam resistance detection in Klebsiella pneumoniae. J Infect Public Health. 2024;17(10):102541. doi:10.1016/j.jiph.2024.102541
26. Jian M-J, Lin T-H, Chung H-Y, et al. Artificial Intelligence-clinical decision support system in infectious disease control: combatting multidrug-resistant Klebsiella pneumoniae with machine learning. Infect Drug Resist. 2024;17:2899–2912. doi:10.2147/IDR.S470821
27. Zeng Y, Wang C, Ye Q, et al. Machine learning model of imipenem-resistant Klebsiella pneumoniae based on MALDI-TOF-MS platform: an observational study. Health Sci Rep. 2023;6(9):e1108. doi:10.1002/hsr2.1108
28. Guo G, Guo C, Qie X, et al. Correlation analysis between Raman spectral signature and transcriptomic features of carbapenem-resistant Klebsiella pneumoniae. Spectrochim Acta A Mol Biomol Spectrosc. 2024;308:123699. doi:10.1016/j.saa.2023.123699
29. Huang TS, Lee SSJ, Lee CC, Chang FC. Detection of carbapenem-resistant Klebsiella pneumoniae on the basis of matrix-assisted laser desorption ionization time-of-flight mass spectrometry by using supervised machine learning approach. PLoS One. 2020;15(2):e0228459. doi:10.1371/journal.pone.0228459
30. Abu-Aqil G, Suleiman M, Sharaha U, et al. Detection of extended-spectrum β-lactamase-producing bacteria isolated directly from urine by infrared spectroscopy and machine learning. Spectrochim Acta A Mol Biomol Spectrosc. 2023;295:122634. doi:10.1016/j.saa.2023.122634
31. Sharaha U, Suleiman M, Abu-Aqil G, et al. Determination of Klebsiella pneumoniae susceptibility to antibiotics using infrared microscopy. Anal Chem. 2021;93(40):13426–13433. doi:10.1021/acs.analchem.1c00734
32. Nguyen M, Brettin T, Long SW, et al. Developing an in silico minimum inhibitory concentration panel test for Klebsiella pneumoniae. Sci Rep. 2018;8(1):421. doi:10.1038/s41598-017-18972-w
33. Weis C, Cuénod A, Rieck B, et al. Direct antimicrobial resistance prediction from clinical MALDI-TOF mass spectra using machine learning. Nat Med. 2022;28(1):164–174. doi:10.1038/s41591-021-01619-9
34. Gato E, Arroyo MJ, Méndez G, et al. Direct detection of carbapenemase-producing Klebsiella pneumoniae by MALDI-TOF analysis of full spectra applying machine learning. J Clin Microbiol. 2023;61(6):e01751. doi:10.1128/jcm.01751-22
35. Yu J, Lin Y-T, Chen W-C, et al. Direct prediction of carbapenem-resistant, carbapenemase-producing, and colistin-resistant Klebsiella pneumoniae isolates from routine MALDI-TOF mass spectra using machine learning and outcome evaluation. Int J Antimicrob Agents. 2023;61(6):106799. doi:10.1016/j.ijantimicag.2023.106799
36. Liu W, Tang J-W, Lyu J-W, et al. Discrimination between carbapenem-resistant and carbapenem-sensitive Klebsiella pneumoniae strains through computational analysis of surface-enhanced Raman spectra: a pilot study. Microbiol Spectr. 2022;10(1):e02409. doi:10.1128/spectrum.02409-21
37. Nguyen QH, Ngo HH, Nguyen-Vo T-H, Do TTT, Rahardja S, Nguyen BP. Emic-AntiKP: estimating minimum inhibitory concentrations of antibiotics towards Klebsiella pneumoniae using deep learning. Comput Struct Biotechnol J. 2023;21:751–757. doi:10.1016/j.csbj.2022.12.041
38. Lu J, Chen J, Liu C, et al. Identification of antibiotic resistance and virulence-encoding factors in Klebsiella pneumoniae by Raman spectroscopy and deep learning. Microb Biotechnol. 2021;15(4):1270–1280. doi:10.1111/1751-7915.13960
39. Abu-Aqil G, Suleiman M, Lapidot I, Huleihel M, Salman A. Infrared spectroscopy-based machine learning algorithms for rapid detection of Klebsiella pneumoniae isolated directly from patients’ urine and determining its susceptibility to antibiotics. Spectrochim Acta A Mol Biomol Spectrosc. 2024;314:124141. doi:10.1016/j.saa.2024.124141
40. Ryu B, Jeon W, Kim D. Integrating genomic and molecular data to predict antimicrobial minimum inhibitory concentration in Klebsiella pneumoniae. Sci Rep. 2024;14(1):25951. doi:10.1038/s41598-024-75973-2
41. López-Cortés XA, Manríquez-Troncoso JM, Sepúlveda AY, Soto PS. Integrating machine learning with MALDI-TOF mass spectrometry for rapid and accurate antimicrobial resistance detection in clinical pathogens. Int J Mol Sci. 2025;26(3):1140. doi:10.3390/ijms26031140
42. Cai C, Zou M, Chen M, et al. Interpretable machine learning of clinical MALDI-TOF spectra discriminates carbapenem-resistant Klebsiella pneumoniae while revealing phylogenetic heterogeneity that limits model generalizability. J Mass Spectrom Adv Clin Lab. 2025;38:71–80. doi:10.1016/j.jmsacl.2025.11.003
43. Jaillard M, Palmieri M, van Belkum A, Mahé P. Interpreting k-mer–based signatures for antibiotic resistance prediction. GigaScience. 2020;9(10):giaa110. doi:10.1093/gigascience/giaa110
44. Wang C, Wang Z, Wang H-Y, et al. Large-scale samples based rapid detection of ciprofloxacin resistance in Klebsiella pneumoniae using machine learning methods. Front Microbiol. 2022;13:827451. doi:10.3389/fmicb.2022.827451
45. Xu X, Gao Y. Machine learning powered profiling: rapid identification of Klebsiella pneumoniae drug resistance from MALDI-TOF MS. J Microbiol Methods. 2025;238:107291. doi:10.1016/j.mimet.2025.107291
46. Tjandra KC, Ram-Mohan N, Roshardt M, et al. Growth independent morphometric machine learning workflow for single-cell antimicrobial susceptibility testing of Klebsiella pneumoniae to meropenem. Front Imaging. 2024;3:1418669. doi:10.3389/fimag.2024.1418669
47. Xu X. Modelling the rapid detection of carbapenemase-resistant Klebsiella pneumoniae based on machine learning and matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Diagn Microbiol Infect Dis. 2024;110(2):116467. doi:10.1016/j.diagmicrobio.2024.116467
48. López-Cortés XA, Manríquez-Troncoso JM, Hernández-García R, Peralta D. MSDEEPAMR: antimicrobial resistance prediction based on Deep Neural Networks and transfer learning. Front Microbiol. 2024;15:1361795. doi:10.3389/fmicb.2024.1361795
49. Astudillo CA, López-Cortés XA, Ocque E, Manríquez-Troncoso JM. Multi-label classification to predict antibiotic resistance from raw clinical MALDI-TOF mass spectrometry data. Sci Rep. 2024;14(1):31283. doi:10.1038/s41598-024-82697-w
50. Caruana G, Kritikos A, Vocat A, et al. Nanomotion-based technology for rapid antibiotic susceptibility testing among adult patients admitted to a tertiary-care hospital with Gram-negative bacteraemia: a prospective, single arm, comparative diagnostic accuracy study. Clin Microbiol Infect. 2026;32(2):299–305. doi:10.1016/j.cmi.2025.10.016
51. Fondrie WE, Liang T, Oyler BL, et al. Pathogen identification direct from polymicrobial specimens using membrane glycolipids. Sci Rep. 2018;8(1):15857. doi:10.1038/s41598-018-33681-8
52. Jian M-J, Lin T-H, Chung H-Y, et al. Pioneering Klebsiella pneumoniae antibiotic resistance prediction with artificial intelligence-clinical decision support system-enhanced matrix-assisted laser desorption/ionization time-of-flight mass spectrometry: retrospective study. J Med Internet Res. 2024;26:e58039.
53. Nguyen M, Olson R, Shukla M, VanOeffelen M, Davis JJ. Predicting antimicrobial resistance using conserved genes. PLoS Comput Biol. 2020;16(10):e1008319. doi:10.1371/journal.pcbi.1008319
54. Aytan-Aktug D, Nguyen M, Clausen PTLC, et al. Predicting antimicrobial resistance using partial genome alignments. mSystems. 2021;6(3):e00185. doi:10.1128/mSystems.00185-21
55. Macesic N, Bear Don’t Walk OJ, Pe’er I, Tatonetti NP, Peleg AY, Uhlemann A-C. Predicting phenotypic polymyxin resistance in Klebsiella pneumoniae through machine learning analysis of Genomic Data. mSystems. 2020;5(3):e00656. doi:10.1128/msystems.00656-19
56. Wiesmann N, Enders D, Westendorf A, Koch R, Schaumburg F. Prediction of antimicrobial resistance from MALDI-TOF mass spectra using machine learning: a validation study. J Clin Microbiol. 2025;63(12):e01186. doi:10.1128/jcm.01186-25
57. Zhou X, Yang M, Chen F, et al. Prediction of antimicrobial resistance in Klebsiella pneumoniae using genomic and metagenomic next-generation sequencing data. J Antimicrob Chemother. 2024;79(10):2509–2517. doi:10.1093/jac/dkae248
58. Condorelli C, Nicitra E, Musso N, et al. Prediction of antimicrobial resistance of Klebsiella pneumoniae from genomic data through machine learning. PLoS One. 2024;19(9):e0309333. doi:10.1371/journal.pone.0309333
59. Lin HH, Lin YT, Chen CH, et al. Prediction of methicillin-resistant Staphylococcus aureus and carbapenem-resistant Klebsiella pneumoniae from Raman spectra by Artificial Intelligent Raman Detection and Identification System (AIRDIS) with machine learning. Int J Antimicrob Agents. 2025;66(5):107587. doi:10.1016/j.ijantimicag.2025.107587
60. Yu J, Lin HH, Tseng KH, et al. Prediction of methicillin-resistant Staphylococcus aureus and carbapenem-resistant Klebsiella pneumoniae from flagged blood cultures by combining rapid SEPSITYPER MALDI-TOF mass spectrometry with Machine Learning. Int J Antimicrob Agents. 2023;62(6):106994. doi:10.1016/j.ijantimicag.2023.106994
61. Tan R, Yu A, Liu Z, et al. Prediction of minimal inhibitory concentration of meropenem against Klebsiella pneumoniae using metagenomic data. Front Microbiol. 2021;12:712886. doi:10.3389/fmicb.2021.712886
62. Xu X, Wang Z, Lu E, et al. Rapid detection of carbapenem-resistant Escherichia coli and carbapenem-resistant Klebsiella pneumoniae in positive blood cultures via MALDI-TOF MS and tree-based machine learning models. BMC Microbiol. 2025;25(1):44. doi:10.1186/s12866-025-03755-5
63. Wang J, Xia C, Wu Y, Tian X, Zhang K, Wang Z. Rapid detection of carbapenem-resistant Klebsiella pneumoniae using machine learning and MALDI-TOF MS platform. Infect Drug Resist. 2022;15:3703–3710. doi:10.2147/IDR.S367209
64. Suleiman M, Abu-Aqil G, Sharaha U, et al. Rapid detection of Klebsiella pneumoniae producing extended spectrum β lactamase enzymes by infrared microspectroscopy and machine learning algorithms. Analyst. 2021;146(4):1421–1429. doi:10.1039/D0AN02182B
65. Huang Y, Li J, Wang Q, Tang K, Li C. Rapid detection of kpc-producing Klebsiella pneumoniae in China based on MALDI-TOF MS. J Microbiol Methods. 2022;192:106385. doi:10.1016/j.mimet.2021.106385
66. Iskender S, Heydarov S, Yalcin M, et al. Rapid determination of colistin resistance in Klebsiella pneumoniae by MALDI-TOF peak based machine learning algorithm with MATLAB. Diagn Microbiol Infect Dis. 2023;107(4):116052. doi:10.1016/j.diagmicrobio.2023.116052
67. Ghouch YE, Schut MC, Sigaloff KCE, et al. Rapid extended-spectrum beta-lactamase-confirmation by using a machine learning model directly on routine automated susceptibility testing results. Front Microbiol. 2025;16:1582703. doi:10.3389/fmicb.2025.1582703
68. Ye Z, Zhu J, Liu Y, Lu J. Rapid identification and typing of carbapenem-resistant Klebsiella pneumoniae using MALDI-TOF MS and machine learning. Microb Biotechnol. 2025;18(6):e70184. doi:10.1111/1751-7915.70184
69. Kang H, Wang Z, Sun J, et al. Rapid identification of bloodstream infection pathogens and drug resistance using Raman spectroscopy enhanced by convolutional neural networks. Front Microbiol. 2024;15:1428304. doi:10.3389/fmicb.2024.1428304
70. Zhang Y-M, Tsao M-F, Chang C-Y, Lin K-T, Keller JJ, Lin H-C. Rapid identification of carbapenem-resistant Klebsiella pneumoniae based on matrix-assisted laser desorption ionization time-of-flight mass spectrometry and an artificial neural network model. J Biomed Sci. 2023;30(1):25. doi:10.1186/s12929-023-00918-2
71. Ye L, Sun Y, Liang X, et al. Rapid identification of carbapenemase subtypes in Klebsiella pneumoniae using MALDI-TOF MS combined with convolutional neural networks. Infect Microbes Dis. 2023;2023:10–97. Epub 2025 Aug 7.
72. Xu Y, Liu D, Han P, et al. Rapid inference of antibiotic resistance and susceptibility for Klebsiella pneumoniae by clinical shotgun metagenomic sequencing. Int J Antimicrob Agents. 2024;64(2):107252. doi:10.1016/j.ijantimicag.2024.107252
73. Lyu J-W, Zhang XD, Tang J-W, et al. Rapid prediction of multidrug-resistant Klebsiella pneumoniae through deep learning analysis of SERS spectra. Microbiol Spectr. 2023;11(2):e04126. doi:10.1128/spectrum.04126-22
74. Inglis TJJ, Paton TF, Kopczyk MK, Mulroney KT, Carson CF. Same-day antimicrobial susceptibility test using acoustic-enhanced flow cytometry visualized with supervised machine learning. J Med Microbiol. 2020;69(5):657–669. doi:10.1099/jmm.0.001092
75. Ciloglu FU, Hora M, Gundogdu A, Kahraman M, Tokmakci M, Aydin O. SERS-based sensor with a machine learning based effective feature extraction technique for fast detection of colistin-resistant Klebsiella pneumoniae. Anal Chim Acta. 2022;1221:340094. doi:10.1016/j.aca.2022.340094
76. Suleiman M, Abu-Aqil G, Lapidot I, Huleihel M, Salman A. Significant reduction of the culturing time required for bacterial identification and antibiotic susceptibility determination by infrared spectroscopy. Anal Methods. 2024;16(23):3745–3756. doi:10.1039/D4AY00604F
77. Duan Q, Wang Q, Sun S, et al. ST11 carbapenem-resistant Klebsiella pneumoniae clone harboring blaNDM replaced a blakpc clone in a tertiary hospital in China. Antibiotics. 2022;11(10):1373. doi:10.3390/antibiotics11101373
78. Singhal N, Kumar M, Kanaujia PK, Virdi JS. MALDI-TOF mass spectrometry: an emerging technology for microbial identification and diagnosis. Front Microbiol. 2015;6:791. doi:10.3389/fmicb.2015.00791
79. Fan S, Kind T, Cajka T, et al. Systematic error removal using random forest for normalizing large-scale untargeted lipidomics data. Anal Chem. 2019;91(5):3590–3596. doi:10.1021/acs.analchem.8b05592
80. Montesinos López OA, Montesinos López A, Crossa J. Overfitting, model tuning, and evaluation of prediction performance. In: Multivariate Statistical Machine Learning Methods for Genomic Prediction. Springer International Publishing; 2022:109–139.
81. Qamar T, Bawany NZ. Understanding the black-box: towards interpretable and reliable deep learning models. PeerJ Comput Sci. 2023;9:e1629. doi:10.7717/peerj-cs.1629
82. Cavallaro M, Moran E, Collyer B, McCarthy ND, Green C, Keeling MJ. Informing antimicrobial stewardship with explainable AI. PLOS Digit Health. 2023;2(1):e0000162. doi:10.1371/journal.pdig.0000162
83. Doern CD, Dunne WM, Burnham C-AD. Detection of Klebsiella pneumoniae carbapenemase (KPC) production in non-Klebsiella pneumoniae Enterobacteriaceae isolates by use of the Phoenix, Vitek 2, and disk diffusion methods. J Clin Microbiol. 2011;49(3):1143–1147. doi:10.1128/JCM.02163-10
84. Khurana S, Malhotra R, Mathur P. Evaluation of Vitek 2 performance for colistin susceptibility testing for Gram-negative isolates. JAC Antimicrob Resist. 2020;2(4):dlaa101. doi:10.1093/jacamr/dlaa101
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Systematic Review of Real-Time Deep Learning Methods for Image-Based Cancer Diagnostics
Sriraman H, Badarudeen S, Vats S, Balasubramanian P
Journal of Multidisciplinary Healthcare 2024, 17:4411-4425
Published Date: 9 September 2024
Radiomics and Deep Learning as Important Techniques of Artificial Intelligence — Diagnosing Perspectives in Cytokeratin 19 Positive Hepatocellular Carcinoma
Wang F, Yan C, Huang X, He J, Yang M, Xian D
Journal of Hepatocellular Carcinoma 2025, 12:1129-1140
Published Date: 5 June 2025
An Artificial Intelligence Pipeline for Hepatocellular Carcinoma: From Data to Treatment Recommendations
Zhang X, Yang L, Liu C, Yuan X, Zhang Y
International Journal of General Medicine 2025, 18:3581-3595
Published Date: 2 July 2025
Artificial Intelligence in Neuro-Ophthalmology for Optic Disc Pathologies and Neurodegenerative Disease
Ahuja AS, Paredes III AA, Eisel MLS, Miller C, Truong N, Falardeau J
Eye and Brain 2026, 18:555894
Published Date: 13 March 2026
Artificial Intelligence for Cardiovascular Risk Prediction: An Umbrella Review of Applications and Translational Challenges

Parizad R, Hatwal J, Brar A, Desai R, Batta A, Mohan B
Vascular Health and Risk Management 2026, 22:590502
Published Date: 28 March 2026